Introduction
Chronic hepatitis B (CHB) is a major health problem
worldwide. In China, although the prevalence of hepatitis B virus
(HBV) infection in the general population was reduced to 7.2% by
2006, it was estimated that there were ~93 million people who were
chronic HBV surface antigen (HBsAg) carriers, of which ~20 million
were patients with chronic hepatitis B (1,2).
Furthermore, in 2014, a seroepidemiological survey of HBV infection
among people aged 1–29 in China revealed that the detection rates
of HBsAg in people aged 1–4, 5–14 and 15–29 years were 0.32%, 0.94%
and 4.38% respectively (2). Most
patients with CHB require long-term therapy. The primary goal of
CHB treatment is to reduce the risk of chronic liver disease and
the associated complications, and improve the quality of life and
survival (2).
Anti-viral therapy, which aims to reduce the HBV DNA
levels as much as possible, is key in the management of CHB. In
this regard, nucleos(t)ide analogues (NAs) are commonly used to
treat CHB patients. Tenofovir disoproxil fumarate (TDF) and
entecavir (ETV) are the most potent HBV inhibitors and have a high
genetic barrier to resistance (3,4).
According to current guidelines, they are the recommended
first-line therapeutic agents for CHB (5–7).
Compared to adefovir, TDF displayed superior virological and
biochemical outcomes in NA-naïve patients in a randomized
controlled trial (3). TDF is able to
sustain its suppressive effects on HBV replication without the
occurrence of drug-resistant mutants after up to 8 years of
continuous therapy (8). Furthermore,
TDF has been reported to be efficacious and safe for CHB patients
with multi-drug resistance (9).
Another study reported that TDF is effective for achieving complete
viral suppression in HBeAg-positive, NA-naïve CHB patients with HBV
DNA levels of >6 log10 IU/ml (10,11).
However, in real life, an increasing number of
patients are experiencing treatment failure with different NA
treatment regimens due to poor compliance or/and financial
barriers. Lovett et al (12)
observed the long-term treatment outcomes of tenofovir therapy in
treatment-naïve and -experienced CHB patients in a real-world
Australian population. They observed that the rates of complete
virological suppression (defined as plasma HBV DNA levels <20
IU/ml) were 70, 87 and 100% at 12, 24 and 36 months, respectively.
However, they did not perform any hierarchical analysis according
to baseline HBV DNA levels. Furthermore, currently available data
on virological response (VR) to long-term continuous TDF therapy in
patients with a high viral load and partial VR (PVR) in the
clinical setting are limited. Therefore, the present study was
performed to provide objective real-life data for the clinical use
of TDF.
The aims of the present retrospective study were to
i) evaluate the long-term efficacy of TDF treatment in NA-naïve CHB
patients with a high viral load in real life and ii) assess the
efficacy of continuous TDF therapy in patients who failed to
achieve VR at 24 weeks.
Patients and methods
Study population
The present retrospective study was performed using
the data of consecutive patients encountered at the Department of
Infectious Diseases of The Third Affiliated Hospital of Sun Yat-sen
University (Guangzhou, China) between February 2012 and July 2017.
All CHB patients were diagnosed on the basis of the Guidelines for
the Prevention and Treatment for Chronic Hepatitis B (2015)
(9) and were treated with TDF 300
mg/day monotherapy. All of the patients were followed up once at
least every 3 months to collect their serum samples. The patients
were carefully examined at each follow-up visit and requested to
report any adverse events. The study protocol conformed to the
ethical guidelines of the Declaration of Helsinki and was approved
by the Ethics Committee of the Third Affiliated Hospital of Sun
Yat-sen University (Guangzhou, China). Informed consent was
obtained from each patient involved in the follow-up study.
The inclusion criteria were as follows: Age, 18–65
years; presence of detectable hepatitis B surface antigen (HBsAg)
levels for 6 months; HBV DNA levels >2,000 IU/ml; alanine
aminotransferase (ALT) levels >2 upper limit of normal; duration
of TDF monotherapy, at least 12 weeks. Patients were excluded if
they had HIV or other hepatitis virus infections, or evidence of
alcoholic hepatitis, autoimmune hepatitis or drug-induced liver
disease. Pregnant and breast-feeding women were also excluded.
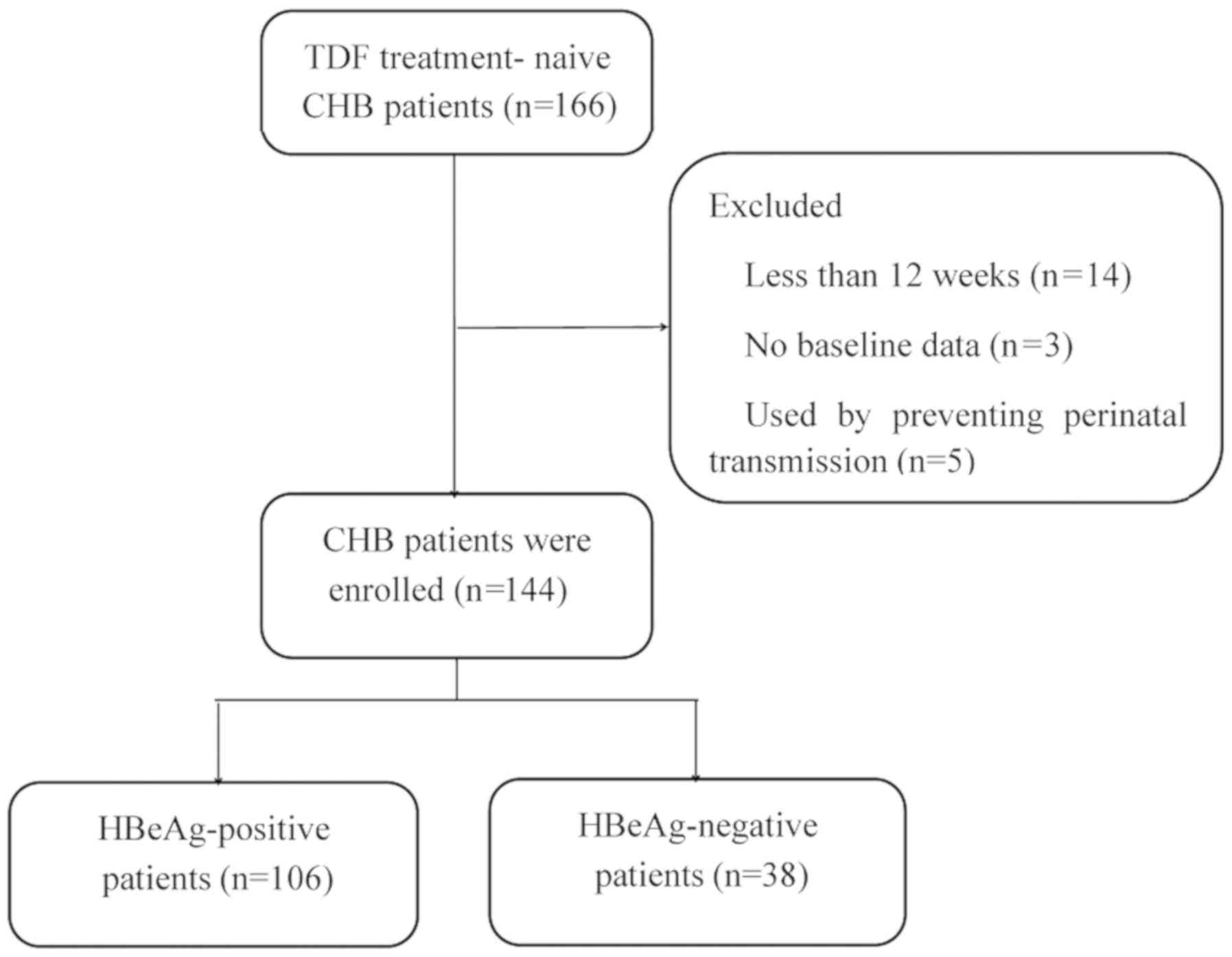
Among the 166 patients treated with TDF at 300
mg/day, 22 were excluded for the following reasons: Duration of TDF
monotherapy for <12 months (n=14), incomplete data at baseline
(n=3) and prevention of mother-to-child transmission (n=5). A total
of 144 patients were eligible for this analysis. A flowchart
depicting the patient enrollment process is provided in Fig. 1.
Laboratory measurements
Routine hematologic analysis, serologic analysis and
assessments of hepatobiliary enzymes, HBV DNA, hepatic synthetic
function, creatine kinase, blood urea nitrogen, creatinine and
blood lactate were performed at baseline and every 3–6 months
thereafter. A 2-ml blood sample was collected at each follow-up
examination for future assessment. The diagnosis of cirrhosis was
based on the results of histological or ultrasound
examinations.
Definitions of response
VR was defined as undetectable serum HBV DNA levels
(<100 IU/ml). PVR was defined as a decrease in HBV DNA level by
>2.0 log10 IU/ml, but detectable HBV DNA in a
real-time PCR assay (≥100 IU/ml) at 24 weeks of TDF treatment
(11). Virological breakthrough was
defined as a >1 log10 IU/ml increase in serum HBV DNA
levels from the nadir in two consecutive measurements. Virological
relapse was defined as serum HBV DNA levels of >2,000 IU/ml in
two tests with a 1-month interval after withdrawing the anti-viral
drug in patients who experienced VR. An ALT level of 5–40 U/l was
considered normal.
Clinical endpoints
The primary endpoint measures were the proportions
of patients achieving VR at 12, 24 and 48 weeks (year 1), 96 weeks
(year 2), 144 weeks (year 3), 192 weeks (year 4) and 240 weeks
(year 5). The secondary endpoints were HBeAg loss and
seroconversion, and ALT normalization.
Assay methods
Liver function assessments and other biochemical
assays were performed using automated techniques. Serum HBV DNA
levels were measured using a real-time quantitative PCR assay (DAAN
Gene Co., Ltd) with a lower detection limit of 100 IU/ml. The HBsAg
(cat. no. 11820532122), HBsAb (cat. no. 11820524122), HBeAg (cat.
no. 11820583122) and HBeAb (cat. no. 11820613122) were measured
using commercially available chemiluminescence assay kits purchased
from Roche Diagnostic Systems.
Statistical analysis
Data were analyzed using the SPSS software package
version 19.0 (IBM Corp.). Quantitative data were expressed as the
mean ± standard deviation. Categorical data were presented as
counts and percentages. HBV DNA levels were presented as
log-transformed values. Student's t-test was used for quantitative
data. Pearson's chi-square and Fisher's exact tests were used for
categorical variables. The associations between sex, age, presence
of cirrhosis, interferon experience, baseline HBV DNA, baseline
HBeAg status, baseline ALT level and end of follow-up of
virological suppression and PVR to TDF monotherapy were tested
using Cox proportional hazards regression analysis. The cumulative
rates of complete viral suppression were analyzed using the
Kaplan-Meier method. A two-tailed P<0.05 was considered to
indicate a statistically significant difference.
Results
Baseline characteristics of
patients
In total, 144 patients were included in the present
study, of whom 106 were HBeAg-positive and 38 were HBeAg-negative.
Overall, 55.6% of the patients (n=80) were male, and 25 patients
(17.4%) had cirrhosis. Five patients had undergone interferon
therapy: 2 had been treated with pegylated interferon and the other
3 had received conventional interferon. One patient received
treatment <3 months due to poor compliance, and 3 patients
finally exhibited virological relapse after cessation of interferon
therapy. One patient did not continue interferon therapy due to
side effects and switched to TDF. The 144 patients enrolled had
good compliance and took medication on time, Although 19 patients
were not followed up every three months, these patients were
followed up at intervals of 4 or 6 months. At each follow-up
time-point, the clinicians communicated with the patients by
telephone, and patients were urged to visit a doctor and receive
timely education to improve treatment adherence. The mean HBV DNA
level in the cohort was 6.7 log10 IU/ml. The mean
patient age was 34 years and the median follow-up period for the
whole study population was 120 weeks (range, 12–264) weeks. The
baseline characteristics of the study population are presented in
Table I.
 | Table I.Characteristics of patients at
baseline. |
Table I.
Characteristics of patients at
baseline.
| Parameter | Total (n=144) | HBeAg-positive
(n=106) | HBeAg-negative
(n=38) | P-value |
|---|
| Male gender
(%) | 80 (55.6) | 52 (49.1) | 28 (73.7) | 0.032 |
| Age (years) | 34±7 | 33±6 | 38±9 | 0.005 |
| Follow-up
(weeks) | 120
(12–264) | 144
(12–264) | 90
(12–240) | 0.363 |
| Presence of
cirrhosis (%) | 25 (17.4) | 7 (6.6) | 18 (47.4) | <0.001 |
| Interferon
experience | 5 (3.5) | 3 (2.8) | 2 (5.3) | 0.781 |
| ALT (U/l) |
172.5±276.6 |
169.0±175.2 |
182.5±456.5 | 0.967 |
| HBV DNA
(log10 IU/ml) |
6.7±1.5 |
7.1±1.3 |
5.6±1.5 | <0.001 |
VR
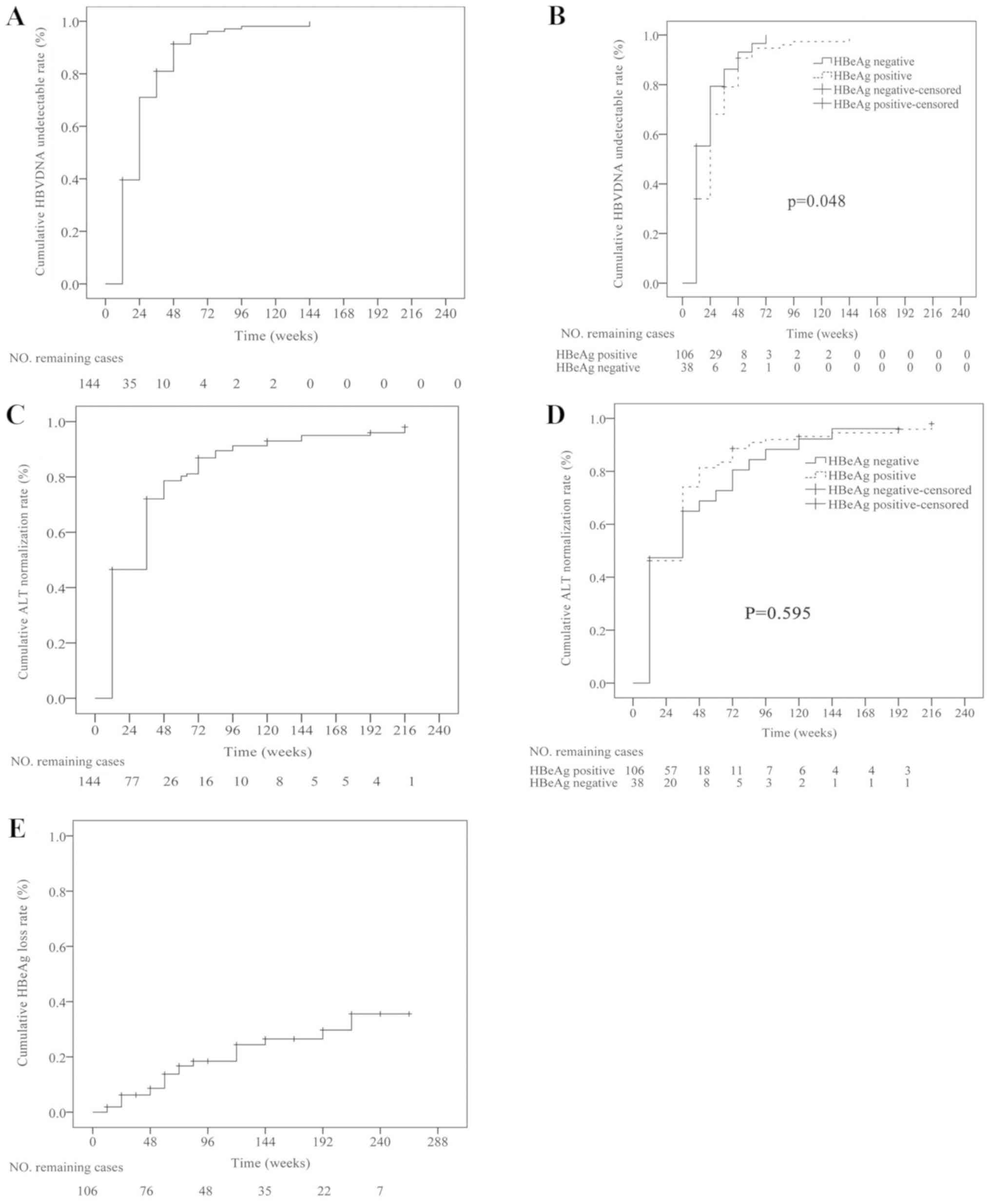
To analyze the suppression of HBV DNA, a
Kaplan-Meier plot was used to visualize the cumulative probability
of achieving complete viral suppression at each follow-up
time-point (Fig. 2). The cumulative
probability of achieving VR at 24, 48, 96, 144, 192 and 240 weeks
was 71, 91.3, 98.1, 100, 100 and 100%, respectively. A transient
elevation of the viral load was observed in 6 patients, which had
an elevation of HBV DNA levels by <1 log10 IU/ml.
However, in the subsequent second test, the HBV DNA level dropped
below the detection limit. Among these patients, HBV DNA levels in
one case rose from below the limit of detection at 36 weeks to 205
U/l at 48 weeks, HBV DNA levels in four cases increased
respectively from below the limit of detection at 60 weeks to 591,
656, 787 and 574 IU/ml at 72 weeks, and HBV DNA levels in one case
rose from below the limit of detection at 84 weeks to 839 U/l at 96
weeks. The proportion of patients exhibiting undetectable HBV DNA
levels at 144 weeks of treatment was higher among patients with
HBeAg-negative status at baseline than among those with
HBeAg-positive status (Fig. 2). Cox
regression analysis demonstrated that the baseline HBV DNA level
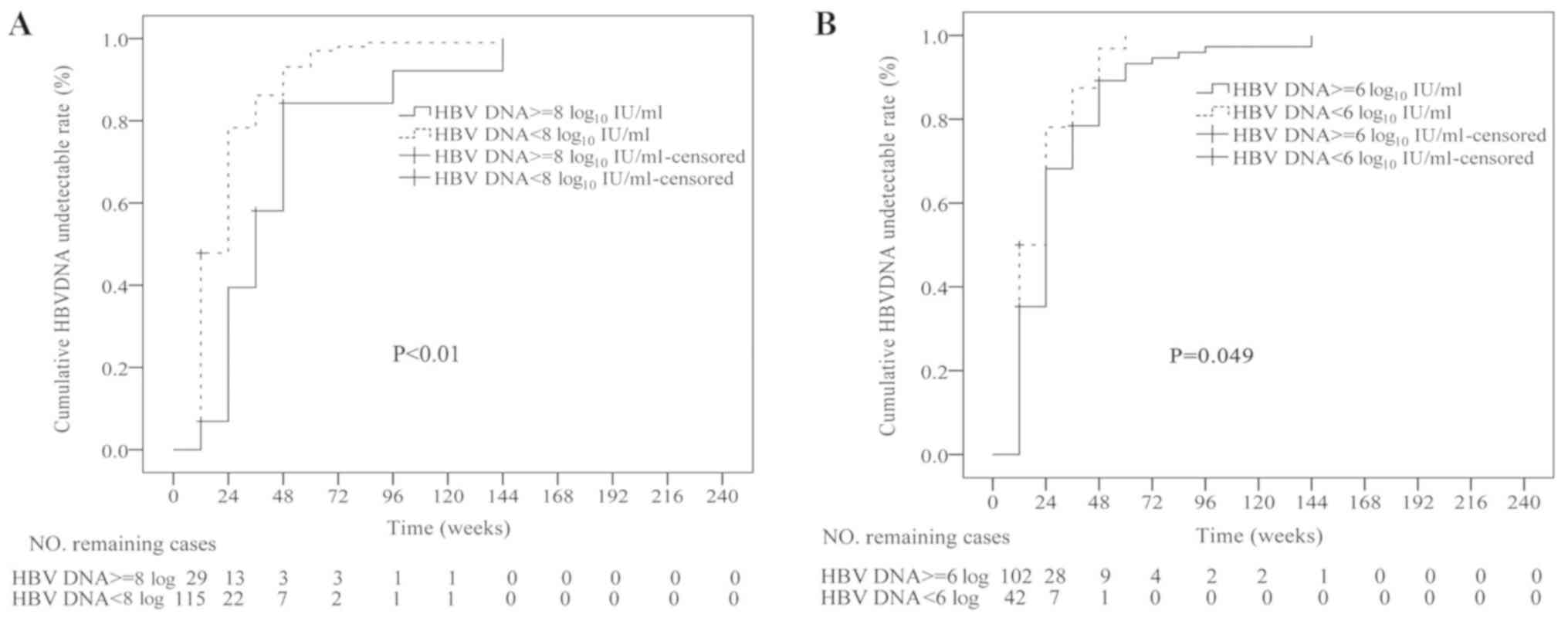
was a significant predictor of VR (P=0.012; Table II). The VR rate was also compared
between patients with baseline HBV DNA levels of ≥8 vs. <8
log10 IU/ml at different time-points. The
characteristics of patients stratified by their baseline HBV DNA
levels are presented in Table III.
The 29 patients with HBV DNA levels of ≥8 log10 IU/ml at
baseline achieved VR during the follow-up period. However, the
cumulative VR rate was higher in patients with baseline HBV DNA
levels of <8 log10 IU/ml than in those with baseline
HBV DNA levels of ≥8 log10 IU/ml (P<0.01; Fig. 3). When patients were divided into
groups with HBV DNA levels of ≥6 and <6 log10 IU/ml,
the VR was revealed to be different between the two groups
(P<0.05).
| Table II.Cox regression analysis for
identification of independent variables predictive of virological
response. |
Table II.
Cox regression analysis for
identification of independent variables predictive of virological
response.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| Sex (males vs.
females) | 0.915
(0.644–1.301) | 0.621 |
|
|
| Age (years) | 1.011
(0.987–1.036) | 0.378 |
|
|
| Presence of
cirrhosis | 1.099
(0.686–1758) | 0.695 |
|
|
| History of
interferon treatment prior to TDF | 1.692
(0.687–4.166) | 0.252 |
|
|
| HBeAg state at
baseline (positive vs. negative) | 0.739
(0.497–1.099) | 0.135 |
|
|
| ALT (U/l) | 1.000
(1.000–1.001) | 0.103 |
|
|
| HBV DNA at baseline
(log10 IU/ml) | 0.866
(0.770–0.974) | 0.016 | 0.808
(0.685–0.954) | 0.012 |
| Table III.Characteristics of patients at
baseline stratified by HBV DNA level. |
Table III.
Characteristics of patients at
baseline stratified by HBV DNA level.
| Parameter | HBV DNA ≥8
log10 IU/ml (n=29) | HBV DNA <8
log10 IU/ml (n=115) | P-value |
|---|
| Male gender
(%) | 20 (69) | 60
(52.2) | 0.104 |
| Age (years) | 32±6 | 35±7 | 0.502 |
| Presence of
cirrhosis (%) | 1
(3.4) | 24
(20.9) | 0.027 |
| Interferon
experienced | 0
(0.0) | 5
(4.3) | 0.583 |
| HBeAg-positive
(%) | 29
(100) | 77 (67) | <0.001 |
| ALT (U/l) | 156.6±172.0 | 176.6±278.8 | 0.722 |
| HBV DNA at baseline
(log10 IU/ml) | 8.3±0.2 | 6.3±1.3 | <0.001 |
Factors predictive of PVR at 24
weeks
The baseline demographics and disease
characteristics of those patients who exhibited a PVR at week 24
are summarized in Table IV. Cox
regression analysis demonstrated that baseline HBV DNA levels and
VR at 12 weeks were significant predictors of PVR (P=0.002;
Table V). A total of 35 cases
(26.9%) exhibited a PVR at 24 weeks. With continued therapy, 21
patients (60%) with PVR at 24 weeks achieved VR at 48 weeks. At 96
weeks, 28 patients (80%) had achieved VR. Another 2 patients
achieved VR at 144 weeks, with HBV DNA remaining at a low level
(<3 log10 IU/ml) prior to that. The remaining 5
patients did not achieve VR at the end of the study as the samples
were detected only every three months, however, they were still
included in the follow-up study.
| Table IV.Baseline demographics of patients who
exhibited a VR or PVR at 24 weeks. |
Table IV.
Baseline demographics of patients who
exhibited a VR or PVR at 24 weeks.
| Parameter | Total (n=130) | VR (n=95) | PVR (n=35) | P-value |
|---|
| Male gender
(%) | 72 (55.4) | 53 (55.8) | 19 (54.3) | 0.878 |
| Age (years) | 34.1±6.7 | 34.1±6.8 | 34.0±6.6 | 0.771 |
| Presence of
cirrhosis (%) | 20 (15.4) | 14 (14.7) | 6
(17.1) | 0.736 |
| Interferon
experienced | 4 (3.1) | 4 (4.2) | 0 (0.0) | 0.218 |
| HBeAg-positive | 98 (75.4) | 68 (71.6) | 30 (85.7) | 0.097 |
| ALT (U/l) | 175.9±287.6 | 202.7±325.5 | 103.4±116.5 | 0.052 |
| HBV DNA at baseline
(log10 IU/ml) | 6.7±1.4 | 6.5±1.4 | 7.3±1.4 | 0.652 |
| Table V.Cox analyses of host and viral
factors associated with undetectable levels of HBV DNA at 24
weeks. |
Table V.
Cox analyses of host and viral
factors associated with undetectable levels of HBV DNA at 24
weeks.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| Sex (males vs.
females) | 0.936
(0.624–1.404) | 0.750 |
|
|
| Age (years) | 1.002
(0.974–1.031) | 0.888 |
|
|
| Presence of
cirrhosis | 0.913
(0.518–1.610) | 0.754 |
|
|
| Interferon
experienced | 0.715
(0.457–1.118) | 0.404 |
|
|
| HBeAg status at
baseline (positive vs. negative) | 1.532
(0.562–4.172) | 0.141 |
|
|
| ALT (U/l) | 1.000
(1.000–1.001) | 0.112 |
|
|
| HBV DNA at baseline
(log 10 IU/ml) | 0.853
(0.747–0.975) | 0.020 | 0.760
(0.641–0.901) | 0.002 |
Biochemical response
The proportions of patients who exhibited ALT
normalization at 24, 48, 96, 144, 192 and 240 weeks were 72.1,
78.6, 91.2, 95, 96 and 100%, respectively. These proportions were
not significantly different between patients with HBeAg-positive
and HBeAg-negative status at baseline (P=0.595; Fig. 2).
Serological response
The proportion of patients who were HBeAg-positive
at baseline and exhibited HBeAg loss at 24, 48, 96, 144, 192 and
240 weeks was 6.2, 8.6, 18.4, 26.5, 29.7 and 35.6%, respectively
(Fig. 2). Furthermore, 2 patients
achieved HBeAg seroconversion at week 48 and 60, respectively. In
addition, 1 patient exhibited HBsAg loss at 120 weeks and the HBsAg
titer at baseline was 160.5 IU/ml, lower than that of
HBeAg-positive patients.
Safety
No severe adverse events were reported during the
present study. Transient elevations in creatine kinase levels were
detected in 42 patients. All of them exhibited no muscle pain
during the follow-up period. Of note, those patients performed a
great deal of physical exercise. After they reduced the amount of
exercise, creatine kinase was restored to normal. Serum creatinine
level and estimated creatinine clearance were evaluated. Estimated
creatinine clearance was calculated using the Modification of Diet
in Renal Disease formula (13). The
creatinine levels in a subset of 141 patients with an available
baseline creatinine level were analyzed. A slightly elevated
creatinine level (153 µmol/l) at week 12 was observed in one
patient, but this reverted to the normal range (31.6–116 µmol/l) at
36 weeks. This patient took part in long-distance running and
physical exercise at the gymnasium prior to the examination. After
the patient was instructed to stop exercising, the level of
creatinine gradually returned to normal. The median estimated
glomerular filtration rate (eGFR) at baseline and at 48, 96, 144,
192 and 240 weeks was 131.96, 122.66, 119.35, 121.25, 113.93 and
117.43 ml/min/1.73m2, respectively (Table VI). The eGFR decreased slightly from
baseline to 240 weeks, but did not reach <90 ml/min/1.73
m2. Serum calcium levels were normal in all patients
throughout the study period. Serum phosphorus levels decreased
slightly among 3 patients, but after another 12 weeks' follow-up
with continuous TDF administration, they reverted to the normal
range (0.74–1.52 mmol/l).
| Table VI.Change in eGFR in tenofovir
treatment-naïve chronic hepatitis B patients. |
Table VI.
Change in eGFR in tenofovir
treatment-naïve chronic hepatitis B patients.
| Time (weeks) | eGFR (ml/min/1.73
m2) |
|---|
| Baseline | 131.96
(58.51–292.75) |
| 48 | 122.66
(73.49–200.86) |
| 96 | 119.35
(80.79–203.08) |
| 144 | 121.25
(79.43–193.43) |
| 192 | 113.93
(80.9–196.32) |
| 240 | 117.43
(88.41–214.3) |
Discussion
TDF is an oral NA and a potent and selective
inhibitor of HBV DNA polymerase/reverse transcriptase in
vitro. The safety and efficacy of TDF in the treatment of
chronic HBV infection have been confirmed in phase 3 clinical
trials that enrolled patients with HBeAg-positive and
HBeAg-negative CHB, respectively (3,10). In
the present study, the cumulative VR rate in TDF-naïve patients
gradually increased throughout the treatment for up to 5 years in
real life. Within the cohort, >95% of the patients had
undetectable HBV DNA levels after 96 weeks, all patients had
undetectable HBV DNA levels after 144 weeks, and another 13
patients who were followed up until 240 weeks achieved complete VR.
This result further confirmed the potent effectiveness of TDF in
inhibiting HBV in real life.
Long-term treatment of CHB with TDF monotherapy has
been reported to maintain effective suppression of HBV DNA over 8
years, with no evidence of TDF resistance or accumulation of
polymorphic or conserved site changes (8). Therefore, TDF is recommended as the
first-line therapeutic agent for CHB in clinical practice
guidelines. In a previous study, the cumulative rate of VR in
TDF-naïve CHB patients with a high viral load (HBV DNA level ≥6
log10 IU/ml) at 24 months was 92.8 and 98.2% in
HBeAg-positive and HBeAg-negative patients, respectively (14). In another study, 7–24% of patients
receiving TDF monotherapy for 48 weeks were reported to exhibit PVR
(15). A 3-year, prospective,
real-world study in France demonstrated VR in 90% of the patients
after 12 weeks, irrespective of HBeAg status, age or prior
treatment history (16). Another
real-world study from Australia reported sustained complete
virological suppression (defined as plasma HBV DNA level <20
IU/ml) in 70% of subjects (29/44) at 12 months, 87% (26/30) at 24
months and 100% (18/18) at 36 months (12). In the present study, the cumulative
rate of complete VR (defined as plasma HBV DNA level <100 IU/ml)
at 24, 48, 96 and 144 weeks was determined as 71, 91.3 98.1 and
100%. This result appears to be superior to the VR obtained in the
Australian study (12). This may be
due to the high lower detection limit of the HBV DNA undetectable
status applied in the present study. The results of the current
study, obtained in the clinical practice setting, are similar to
results previously reported in clinical trials.
In the present study, a transient elevation of the
viral load was observed in 6 patients, comprising an elevation of
the HBV DNA level by <1 log. However, in the subsequent second
test, the HBV DNA level dropped below the detection limit. These
patients had good medication adherence, and the transient elevation
of viral load did not manifest as antiviral drug resistance.
Hongthanakorn et al (17)
also observed this virological breakthrough (VBT) phenomenon, which
is defined as a >1 log10 IU/ml increase in serum HBV
DNA levels from the nadir in two consecutive measurements (18), VBT is common in patients with chronic
hepatitis B receiving nucleos(t)ide analogue treatment, but not all
VBTs are due to drug resistance. The accountability of other
reasons except for medication adherence is worth further
exploration.
In the present study, a Cox regression analysis
indicated that a high HBV DNA level at baseline was an independent
factor influencing VR (P<0.05). When the patients were divided
into two groups according to the baseline HBV DNA level (≥8 and
<8 log10 IU/ml), the rate of VR was significantly
different between the two groups (P<0.05). However, with
continued treatment, the VR rate in each group had reached 100%
after 144 weeks. At present, there is no clear definition of high
viral load, and certain studies regard HBV DNA levels of ≥6
log10 IU/ml as indicative of high viral load (11). Therefore, in the present study, HBV
DNA levels of ≥6 and ≥8 log10 IU/ml were considered for
assessment. The patients were divided into two groups based on
baseline HBV DNA levels of ≥6 or <6 log10 IU/ml and
it was observed that the VR was different between the two groups
(P<0.05). This result provides further evidence that TDF is
highly effective for CHB patients with a high viral load. A
previous study by our group has demonstrated that TDF and ETV
rapidly inhibit HBV DNA replication in HBeAg-positive CHB patients
with high HBV DNA levels (19).
However, another study demonstrated that TDF is superior to ETV in
achieving complete viral suppression in HBeAg-positive CHB patients
with high HBV DNA levels (HBV DNA level >6 log10
IU/ml), with no significant difference in viral suppression in
HBeAg-negative patients (11). These
results provide a reference for the selection of anti-viral drugs
in patients with chronic HBV with a high viral load.
Previous studies reported that high baseline HBV DNA
and HBeAg positivity are independent risk factors for PVR (20,21). In
the present study, the e-antigen state at baseline appeared to have
no effect on the VR at 24 weeks in TDF-treated patients, as
indicated by Cox univariate and multivariate logistic regression
analysis. There may be several reasons for this observation. First,
the overall sample size of the present study was relatively small,
and the proportion of HBeAg-negative patients in the overall
population was <27%. Furthermore, the mean value of HBV DNA at
baseline was similar to that of HBeAg-negative and HBeAg-positive
patients.
The presence of PVR, particularly to treatment with
lamivudine, telbivudine and adefovir, is linked to the high risk of
resistance to long-term anti-HBV treatment in these patients
(22). Conversely, for drugs with a
high resistance barrier, including ETV and TDF, PVR is associated
with a lower risk of resistance to long-term monotherapy. A
previous study by our group suggests that adjustment of ETV
monotherapy may not be required in NA-naïve patients with a PVR at
1 year if no resistance to ETV has occurred by then; most patients
achieved VR if therapy was continued beyond 1 year (23).
In the present study, 35 cases (26.9%) achieved a
PVR at 24 weeks. With continued therapy, 21 patients (60%) with a
PVR at 24 weeks achieved VR at 48 weeks. After 3 years, >80% of
the patients had achieved VR. No virological breakthroughs were
observed during this process. A Korean study reported that 127 out
of 177 patients with PVR (71.8%) achieved VR during continuous
prolonged TDF therapy (20). It also
suggested that the vast majority of CHB patients with PVR achieved
VR through prolonged TDF therapy, and it was unnecessary to
urgently implement salvage therapy for TDF-naïve CHB patients with
PVR.
In addition to undetectable HBV DNA levels, the
disappearance of HBsAg and even the emergence of HBsAb are ideal
treatment goals for CHB patients. In the present study, only one
patient exhibited loss of HBsAg, and no serum conversion occurred.
Among the HBeAg-positive patients at baseline, 20 patients achieved
HBeAg loss until 192 weeks. Of those 20 patients, 2 achieved HBeAg
seroconversion at weeks 48 and 60. The proportion of patients
exhibiting HBeAg loss in the present study was lower than that
reported previously (35.6 vs. 45.0%) by Marcellin et al
(16). Novel drugs and strategies
should be developed to achieve the goal of HBsAg seroconversion
after VR, which remains a challenge.
No severe adverse events were reported in the
present study. The serum phosphorus levels decreased slightly in 3
patients and were restored to the normal range without
discontinuation of the treatment. The eGFR decreased slightly from
baseline to 144 weeks, but always remained >90 ml/min/1.73
m2. Until 144 weeks, the eGFR subsequently stabilized
gradually. Tsai et al (24)
reported that the eGFR decreased significantly in the TDF group
after a mean of 17 months of treatment, while Wang et al
(25) observed that the eGFR
decreased in patients with TDF treatment within 12 weeks. López
Centeno et al (26) indicated
no significant differences in terms of renal safety between CHB
patients treated with ETV and TDF. Another study reported no
significant differences in the eGFR in either the ETV- or
TDF-treated patients with compensated cirrhosis or decompensated
cirrhosis at week 96 (27). However,
adverse events, including Fanconi syndrome, asthenia,
hypophosphatemia and abdominal pain, have been reported to be
associated with TDF (12).
Therefore, regular follow-up examination is important and treatment
decisions should be based on individualized assessments of each
patient.
A relevant limitation of the present study is the
small sample size. It is regrettable that resistance was not
evaluated in patients with PVR at 24 weeks. In the majority of
patients, quantitative analysis of HBsAg was not detected.
In conclusion, long-term treatment with TDF for up
to 5 years significantly reduced HBV DNA levels in CHB patients,
regardless of high viral load at baseline. Adjustment of TDF
monotherapy in NA-naïve patients with PVR at 24 weeks may not be
required, and most patients achieved VR if therapy was
continued.
Acknowledgements
Not applicable.
Funding
This project was supported by the Natural Science
Foundation of Guangdong (grant nos. 2014A030313146, 2016A030313250
and 2016A030313302), the Tianhe District Science and Technology
Project (grant no. 201504KW032) and the Jiangxi Science and
Technology Project (grant no. 20151BBG70163).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JL, XYL and XY wrote the manuscript. YC, JL, XYL and
ZL designed the study. JL, XY, ZL, XYL, YW, JG, YJ, XHL, SX, ZZ, YZ
and DX collected the patient data. JL, XY, ZL and XYL analyzed the
data and revised the manuscript. All authors read and approved the
final manuscript.
Ethical approval and consent to
participate
The present study was approved by the Ethics
Committee of the Third Affiliated Hospital of Sun Yat-sen
University (Guangdong, China). Written informed consent was
obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CHB
|
chronic hepatitis B
|
|
PVR
|
partial virological response
|
|
TDF
|
tenofovir disoproxil fumarate
|
|
ETV
|
entecavir
|
|
NAs
|
nucleos(t)ide analogues
|
References
|
1
|
Wang FS, Fan JG, Zhang Z, Gao B and Wang
HY: The global burden of liver disease: The major impact of China.
Hepatology. 60:2099–2108. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chinese Society of Hepatology and Chinese
Society of Infectious Diseases, Chinese Medical Association, . The
Guideline of Prevention and Treatment for Chronic Hepatitis B (2015
Version). J Clin Hepatol. 31:1941–1960. 2015.
|
|
3
|
Marcellin P, Heathcote EJ, Buti M, Gane E,
de Man RA, Krastev Z, Gemanidis G, Lee SS, Flisiak R, Kaita K, et
al: Tenofovir disoproxil fumarate versus adefovir dipivoxil for
chronic hepatitis B. N Engl J Med. 359:2442–2455. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Buti M, Tsai N, Petersen J, Flisiak R,
Gurel S, Krastev Z, Aguilar Schall R, Flaherty JF, Martins EB,
Charuworn P, et al: Seven-year Efficacy and safety of treatment
with tenofovir disoproxil fumarate for chronic hepatitis B virus
infection. Dig Dis Sci. 60:1457–1464. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sarin SK, Kumar M, Lau GK, Abbas Z, Chan
HL, Chen CJ, Chen DS, Chen HL, Chen PJ, Chien RN, et al:
Asian-Pacifc clinical practice guide-lines on the management of
hepatitis B: A 2015 update. Hepatol Int. 10:1–98. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Terrault NA, Bzowej NH, Chang KM, Hwang
JP, Jonas MM, Murad MH; American Association for the Study of Liver
Diseases, ; et al: AASLD guidelines for treatment of chronic
hepatitis B. Hepatology. 63:261–283. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lampertco P, Maini M and Papatheodoridis
G: Optimal management of hepatitis B virus infection-EASL special
conference. J Hepatol. 63:1238–1253. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu Y, Corsa AC, But M, Cathcart AL,
Flaherty JF, Miller MD, Kitrinos KM, Marcelin P and Gane EJ: No
detectable resistance to tenofovir disoproxil fumarate in HBeAg+
and HBeAg−patents with chronic hepatts B afer 8 years of treatment.
J Viral Hepat. 24:68–74. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lim YS, Lee YS, Gwak GY, Byun KS, Kim YJ,
Choi J, An J, Lee HC, Yoo BC and Kwon SY: Monotherapy with
tenofovir disoproxil fumarate for multiple drug-resistant chronic
hepatitis B: 3-year trial. Hepatology. 66:772–783. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gordon SC, Krastev Z, Horban A, Petersen
J, Sperl J, Dinh P, Martins EB, Yee LJ, Flaherty JF, Kitrinos KM,
et al: Efficacy of tenofovir disoproxil fumarate at 240 weeks in
patients with chronic hepatitis B with high baseline viral load.
Hepatology. 58:505–513. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gao L, Trinh HN, Li J and Nguyen MH:
Tenofovir is superior to entecavir for achieving complete viral
suppression in HBeAg-positive chronic hepatitis B patients with
high HBV DNA. Aliment Pharmacol Ther. 39:629–637. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lovett GC, Nguyen T, Iser DM, Holmes JA,
Chen R, Demediuk B, Shaw G, Bell SJ, Desmond PV and Thompson AJ:
Efficacy and safety of tenofovir in chronic hepatitis B: Australian
real world experience. World J Hepatol. 9:48–56. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y,
Xu JS, Huang SM, Wang LN, Huang W, et al: Modified glomerular
filtration rate estimating equation for Chinese patients with
chronic kidney disease. J Am Soc Nephrol. 17:2937–2944. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wu IT, Hu TH, Hung CH, Lu SN, Wang JH, Lee
CM and Chen CH: Comparison of the efficacy and safety of entecavir
and tenofovir in nucleos(t)ide analogue-naive chronic hepatitis B
patients with high viraemia: A retrospective cohort study. Clin
Microbiol Infect. 23:464–469. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lampertico P: Partial virological response
to nucleos(t)ide analogues in naïve patients with chronic hepatitis
B: From guidelines to field practice. J Hepatol. 50:644–647. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Marcellin P, Zoulim F, Hezode C, Causse X,
Roche B, Truchi R, Pauwel A, Ouzan D, Dumortier J, Pageaux GP, et
al: Effectiveness and safety of tenofovir disoproxil fumarate in
chronic Hepatitis B: A 3-year, prospective, real-world study in
France. Dig Dis Sci. 61:3072–3083. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hongthanakorn C, Chotiyaputta W,
Oberhelman K, Fontana RJ, Marrero JA, Licari T and Lok AS:
Virological breakthrough and resistance in patients with chronic
hepatitis B receiving nucleos(t)ide analogues in clinical practice.
Hepatology. 53:1854–1863. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
European Association For The Study Of The
Liver. Electronic address, . easloffice@easloffice.eu; European
Association for the Study of the Liver: EASL 2017 Clinical Practice
Guidelines on the management of hepatitis B virus infection. J
Hepatol. 67:370–398. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shi H, Huang M, Lin GL, Li X, Wu Y, Jie Y
and Chong Y: Efficacy comparison of tenofovir and entecavir in
HBeAg-positive chronic hepatitis B patients with high HBV DNA.
Biomed Res Int. 2016:67250732016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Du Jeong I, Jung SW, Park BR, Lee Bu, Park
JH, Kim BG, Bang SJ, Shin JW and Park NH: Clinical course of
partial virologic response with prolonged Tenofovir therapy in
Nuclos(t)ides-naive patients with chronic hepatitis B. Dig Dis Sci.
62:2908–2914. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zoutendijk R, Reijnders JG, Brown A,
Zoulim F, Mutimer D, Deterding K, Petersen J, Hofmann WP, Buti M,
Santantonio T, et al: Entecavir treatment for chronic hepatitis B:
Adaptation is not needed for the majority of naive patients with a
partial virological response. Hepatology. 54:443–451. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
European Association for the Study of the
Liver, . EASL clinical practice guide-lines: Management of chronic
hepatitis B. J Hepatol. 50:227–242. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Luo J, Li X, Wu Y, Lin G, Pang Y, Zhang X,
Ao Y, Du Z, Zhao Z and Chong Y: Efficacy of entecavir treatment for
up to 5 years in Nucleos(t)ide-naïve chronic hepatitis B patients
in real life. Int J Med Sci. 10:427–433. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tsai MC, Chen CH, Tseng PL, Hung CH, Chiu
KW, Wang JH, Lu SN, Lee CM, Chang KC, Yen YH, et al: Comparison of
renal safety and efficacy of telbivudine, entecavir and tenofovir
treatment in chronic hepatitis B patients: Real world experience.
Clin Microbiol Infect. 22:95.e1–e7. 2016. View Article : Google Scholar
|
|
25
|
Wang HM, Hung CH, Lee CM, Lu SN, Wang JH,
Yen YH, Kee KM, Chang KC, Tseeng PL, Hu TH and Chen CH: Three-year
efficacy and safety of tenofovir in nucleos(t)ide analog-naïve and
nucleos(t)ide analog-experienced chronic hepatitis B patients. J
Gastroenterol Hepatol. 31:1307–1314. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
López Centeno B, Collado Borrell R, Pérez
Encinas M, Gutierrez Garcia ML and Sanmartin Fenollera P:
Comparison of the effectiveness and renal safety of tenofovir
versus entecavir in patients with chronic hepatitis B. Farm Hosp.
40:279–286. 2016.PubMed/NCBI
|
|
27
|
Park J, Jung KS, Lee HW, Kim BK, Kim SU,
Kim DY, Ahn SH, Han KH and Park JY: Effects of entecavir and
tenofovir on renal function in patients with hepatitis B
virus-related compensated and decompensated cirrhosis. Gut Liver.
11:828–834. 2017. View
Article : Google Scholar : PubMed/NCBI
|