Introduction
Traumatic brain injury (TBI) is a leading cause of
death and disability in young adults (1). The majority of TBI is due to a blow to
the head resulting from sports-related concussion, being hit by
falling objects, or traffic accidents (2). Mild brain injury may lead to temporary
brain disorders (3), while severe
brain injury may cause tissue tears, bruises and even death
(4). TBI has also a mental impact
(5). Statistical research has shown
that in 2013, ~2.8 million TBI-related emergency department visits,
hospitalizations, and deaths occurred in the United States,
including ~2.5 million TBI-related emergency department visits,
~282,000 TBI-related hospitalizations, and ~56,000 TBI-related
deaths (6). Hydrocephalus is a
commonly encountered secondary brain disorder to TBI (7), whose pathogenesis is very complicated.
Hydrocephalus is characterized by abnormal flow and absorbance of
cerebrospinal fluid (CSF), which leads to dilated ventricles
(8). When hydrocephalus occurs,
there is a massive accumulation of CSF within the brain (9), causing increased pressure inside the
skull. As a result, a series of neurological symptoms may develop.
A surgical procedure, called ventriculoperitoneal (VP) shunting,
can be performed to improve the brain symptoms (10).
A VP shunt is a medical device that consists of an
implantable one-way valve to relieve the pressure in the brain. The
excessive CSF can be shunted from the ventricle to the abdominal
cavity for absorption (11). A VP
shunt is suitable for all patients with hydrocephalus of different
causes (12). It has been reported
that VP shunting can reduce hydrocephalus mortality and morbidity
(13,14). However, complications such as
postoperative infection, shunt obstruction, excessive drainage,
shunt migration, and subdural hemorrhage may occur (15). When treating TBI with VP shunting,
the shunt which consists of a one-way valve can be used to treat
hydrocephalus with either normal intracranial pressure or high
intracranial pressure (16). As
medical technologies are advancing, treatment techniques of
hydrocephalus are also maturing. So far, VP shunting has become the
most common treatment option in clinical practice (17). In the present study, we explored the
clinical application of VP shunting in treating TBI.
Patients and methods
Patients
In total, 100 patients who had hydrocephalus due to
TBI and were admitted to Shanxian Central Hospital (Heze, China)
from February 2012 to June 2016 were recruited to this study. The
patients were separated into two groups according to the different
treatment methods: 50 patients in the experimental group and 50
patients in the control group. Patients in the experimental group
underwent VP shunting, while patients in the control group
underwent lumboperitoneal (LP) shunting. There were 31 males and 19
females in the experimental group. Their ages were 20–60 years and
their average age was 37.5±6.8 years. In the control group, there
were 28 males and 22 females. Their ages were 21–64 years and their
average age was 36.9±7.2 years. Using the ventricular/biparietal
(V/BP) ratio as a scale of assessing the severity of hydrocephalus,
the patients in the experimental group were further separated into
three subgroups: 18 in the mild hydrocephalus subgroup, 17 in the
moderate hydrocephalus subgroup and 15 in the severe hydrocephalus
subgroup. All enrolled subjects were diagnosed with hydrocephalus
in the Shanxian Central Hospital. Patients who had the following
conditions were excluded from the study: i) severe impairment in
cognitive function or mental function; ii) cardiovascular diseases;
iii) liver or kidney dysfunction; or iv) endocrine system
disorders. The study was approved by the Ethics Committee of
Shanxian Central Hospital and written informed consents were
obtained by the patients and/or guardians.
Methods
All patients received a routine examination before
surgery. The procedures were done under general anesthesia after
the hydrocephalus lesion was localized. Patients in the
experimental group underwent VP shunting surgery using a shunt
system (programmable pressure shunt system) manufactured by
Medtronic. An arc-shaped hole was made in the skull 4–5 cm behind
the right auricle. The size of the hole depended on the size of the
reservoir base. Dura mater was cut, and the front end of a
ventricular catheter was passed into the anterior horn of the
ventricle. The catheter was cut to suitable length and connected to
a reservoir. The reservoir was placed into the hole in the skull
and secured to the dura, followed by suture of the incision. The
outlet of the reservoir was connected to the valve in a pump. The
arrow on the pump chamber was adjusted to point to the direction in
which the CSF was shunted. The second step was to create a
subcutaneous tunnel to run the second catheter from the incision in
the head to the upper abdominal region through the neck and the
chest. A subcutaneous tunnel was created in three segments.
Incisions were made at the posterior mastoid, below the clavicle,
and on the right upper abdomen below the xiphoid process. Then,
using a blunt metal as a guide, each segment of the subcutaneous
tunnel was opened by deep subcutaneous separation of tissue. The
third step was to install the abdominal catheter. The proximal end
of the catheter was connected to the valve outlet. The distal end
was passed through the subcutaneous tunnel to arrive at the right
upper abdominal incision. The fourth step was to suture the
peritoneum and abdominal wall layer-by-layer, following securing
the catheter.
Patients in the control group underwent LP shunting
surgery using a shunt system (programmable pressure shunt system).
Patients were placed in the left lateral position. The preoperative
and postoperative cares were the same as those for patients in the
experimental group. In order to prevent any infection, patients in
both groups were given antibacterial drugs once after surgery.
Indicators observed and assessment
Grading scale for hydrocephalus
(18)
The V/BP ratio was used to grade the severity of
hydrocephalus. The grading scale is listed in Table I.
 | Table I.Grading scale of hydrocephalus. |
Table I.
Grading scale of hydrocephalus.
| Classification | V/BP value |
|---|
| Mild | 0.26–0.40 |
| Moderate | 0.41–0.60 |
| Severe | >0.60 |
Outcome assessment (19)
The following standards were established for the
outcome assessment. An excellent outcome was achieved, if the CT
results were all within the normal range and the patient's motor
function was totally recovered. A satisfactory outcome was
achieved, if significant improvements were observed in clinical
symptoms and the patient's motor function, as well as in the CT
results. An unsatisfactory outcome was achieved, if the conditions
were not improved at all or became worse. The total effective rate
was calculated using the formula: Total effective rate = (cases of
excellent outcome + cases of satisfactory outcome)/total number of
cases ×100%.
Postoperative neurological deficit
scoring (20)
A neurological deficit scoring system was designed
to assess the patient's language function, response and awareness.
The total score was 40 points. The higher the score, the more
severe the neurological deficit. A patient with a score >25
points was regarded to have neurological deficits; 1–15 points
indicated mild neurological deficit; 16–25 points indicated
moderate neurological deficit; 25–40 points indicated severe
neurological deficit.
Statistical analysis
All data acquired in this study were analyzed using
the SPSS 19.0 statistical software (IBM Corp.). Count data were
expressed as n (%), and Chi-square test was used for their
comparison. Measurement data were expressed as the mean ± standard
deviation. Paired t-test was used for the comparison of the data
between the experimental and the control group, before and after
surgery. Repeated measures ANOVA with Least Significant Difference
post hoc test were used for multiple comparisons. P<0.05 was
considered to indicate a statistically significant difference.
Results
General clinical records
There were no significant differences in age, sex,
body weight, time of injury, cause of injury, Glasgow Outcome Scale
(GOS) score at admission, and severity of hydrocephalus between the
two groups (P>0.05). This indicated that the baselines of
patients in the two groups were comparable. The general clinical
records of the patients are listed in Table II.
| Table II.General clinical records of the
patients. |
Table II.
General clinical records of the
patients.
| Variable | Experimental group
(n=50) | Control group
(n=50) | t or
χ2 | P-value |
|---|
| Age (years) |
|
>30 | 24 | 27 | 0.360 | 0.548 |
| ≤30 | 26 | 23 |
|
|
| Sex |
| Male | 31 | 28 | 0.372 | 0.542 |
|
Female | 19 | 22 |
|
|
| Body weight (kg) |
|
>50 | 22 | 26 | 0.641 | 0.423 |
| ≤50 | 28 | 24 |
|
|
| Time of injury
(h) | 56.84±27.55 | 58.24±30.45 | 0.241 | 0.810 |
| Cause of injury |
| Traffic
accident | 15 | 13 | 0.264 | 0.967 |
| Blow to
the head | 16 | 17 |
|
|
| Falling
object | 10 | 10 |
|
|
|
Other | 9 | 10 |
|
|
| GOS score at
admission | 2.95±0.68 | 3.12±0.75 | 1.187 | 0.238 |
| Severity of
hydrocephalus |
|
Severe | 18 | 20 | 0.467 | 0.792 |
|
Moderate | 17 | 18 |
|
|
| Mild | 15 | 12 |
|
|
Outcome comparison between the two
groups
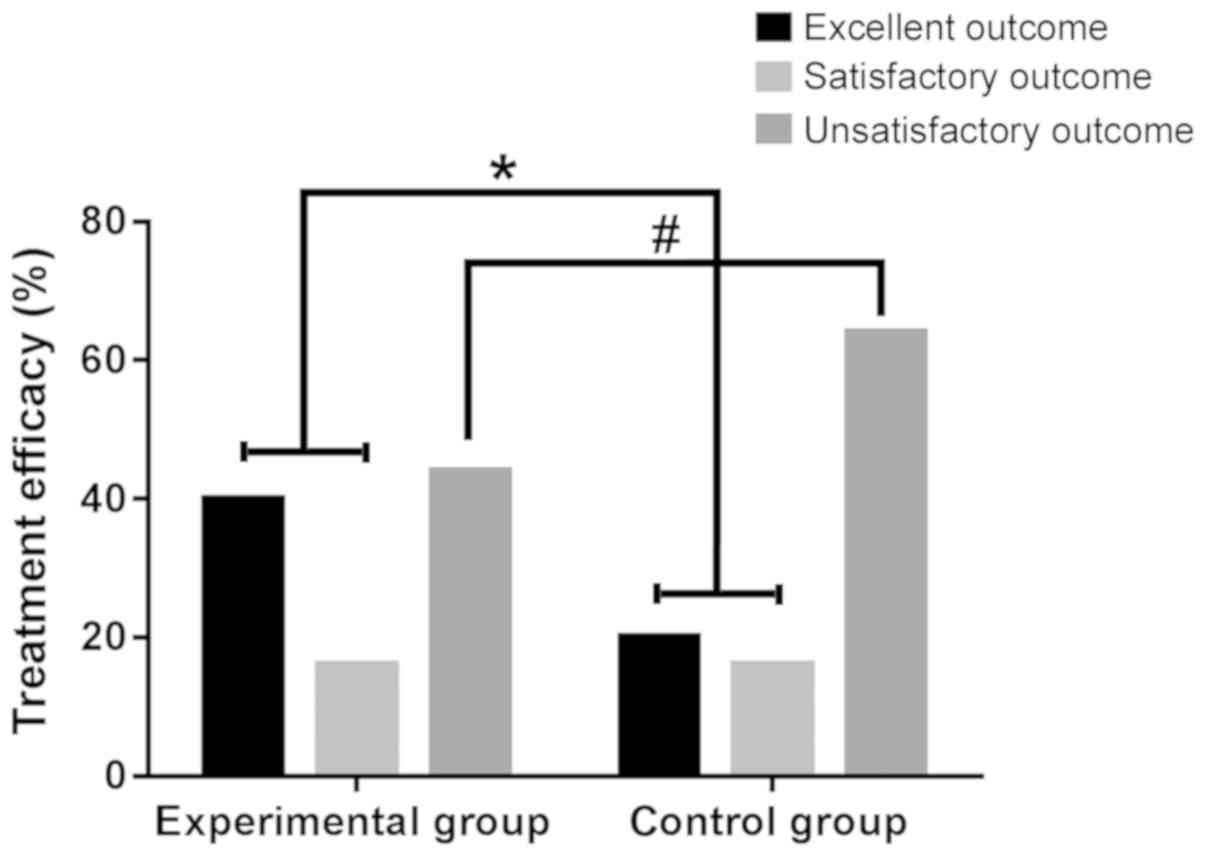
As shown in Fig. 1,
the effective rate in the experimental group (56.00%) was
significantly higher than that in the control group (36.00%), and
the difference was statistically significant (χ2=6.341,
P<0.05). The unsatisfactory outcome rate in the experimental
group was significantly lower than that in the control group
(P<0.05).
Outcome comparison among the subgroups
of the experimental group
As shown in Table
III, the effective rates in the severe, the moderate and the
mild hydrocephalus subgroups were 33.33, 76.47 and 94.44%,
respectively. The effective rate in the mild hydrocephalus subgroup
was significantly higher than that in the severe hydrocephalus
subgroup, and the difference was statistically significant
(P<0.05). The effective rate in the moderate hydrocephalus
subgroup was significantly higher than that in the severe
hydrocephalus subgroup, and the difference was statistically
significant (P<0.05) (Table
III).
| Table III.Outcome comparison among the subgroups
within the experimental group [n (%)]. |
Table III.
Outcome comparison among the subgroups
within the experimental group [n (%)].
| Subgroup | Excellent | Satisfactory | Unsatisfactory | Total effective
rate |
|---|
| Mild (n=18) | 10 (55.55) | 7 (38.89) | 1 (5.56) | 17
(94.44)a |
| Moderate (n=17) | 8 (47.06) | 5 (29.41) | 4 (23.53) | 13
(76.47)a |
| Severe (n=15) | 1 (6.67) | 4 (26.66) | 10 (66.67) | 5 (33.33) |
| χ2
value | – | – | – | 15.06 |
| P-value | – | – | – |
0.001 |
Incidence of complications in the two
groups
Patients in the control group underwent LP shunting
surgery. Among the 13 cases of complications that were observed in
this group, there were 4 cases of postoperative infection, 2 cases
of shunt obstruction, 3 cases of excessive drainage, 2 cases of
shunt migration, and 2 cases of subdural hemorrhage (Table IV). The incidence of complications
was 26.00%. Patients in the experimental group underwent VP
shunting surgery. Among the 6 cases of complications that were
observed in this group, there were 2 cases of postoperative
infection, 1 case of shunt obstruction, 2 cases of excessive
drainage, and 1 case of shunt migration. The incidence of
complications was 12.00%. Apparently, the incidence of
complications in patients undergoing LP shunting surgery (26.00%)
was significantly higher than that in patients undergoing VP
shunting surgery (12.00%). The difference was statistically
significant (χ2=66.04, P<0.05).
| Table IV.Incidence of complications in the two
groups [n (%)]. |
Table IV.
Incidence of complications in the two
groups [n (%)].
| Complication | Control group
(n=50) | Experimental group
(n=50) |
|---|
| Postoperative
infection | 4 (8.00) | 2 (4.00) |
| Shunt
obstruction | 2 (4.00) | 1 (2.00) |
| Excessive
drainage | 3 (6.00) | 2 (4.00) |
| Shunt
migration | 2 (4.00) | 1 (2.00) |
| Subdural
hemorrhage | 2 (4.00) | 0 (0) |
| Incidence | 13 (26.00) | 6
(12.00)a |
Neurological deficit scores before and
after treatment in the two groups
The neurological deficit scores before and after
treatment in the experimental group were 28.63±8.90 and 15.42±5.23,
respectively, while the neurological deficit scores before and
after treatment in the control group were 28.59±8.57 and
22.54±6.84, respectively (Table V).
There was no significant difference in neurological deficit score
between the two groups before surgery (t=0.023, P=0.982). However,
the difference in neurological deficit score between the two groups
was statistically significant after surgery (t=5.847,
P<0.05).
| Table V.Neurological deficit scores before
and after surgery in the two groups. |
Table V.
Neurological deficit scores before
and after surgery in the two groups.
|
| Neurological
deficit score |
|---|
|
|
|
|---|
| Group | Before surgery | After surgery |
|---|
| Experimental group
(n=50) | 28.63±8.90 | 15.42±5.23 |
| Control group
(n=50) | 28.59±8.57 |
22.54±6.84a |
Discussion
TBI is a brain dysfunction caused by an external
force, such as a violent blow to the head or concussion of the head
and body (21). TBI has a certain
impact on thinking and language abilities, as well as emotion
(22). In severe cases, it may lead
to permanent brain damage or death. Hydrocephalus is one of the
common symptoms of TBI, which often leads to aggravation of the
disease, affecting the patient's prognosis (23). It has been reported that
hydrocephalus is a devastating disease (24). If not treated in time, hydrocephalus
will not heal automatically. Therefore, surgical intervention is
very important for the recovery of brain tissue.
In this study, 50 patients with hydrocephalus after
TBI, who underwent VP shunting in Shanxian Central Hospital, were
assigned to the experimental group. Another 50 patients with
hydrocephalus after TBI, who underwent LP shunting, were assigned
to the control group. Therapeutic outcomes were first compared
between the experimental and the control group. The effective rate
in the experimental group (56.00%) was significantly higher than
that in the control group (36.00%), and the difference was
statistically significant (P<0.05). Up to our knowledge, this is
the first report in this regard. This result reveals that the
therapeutic outcome using VP shunting is much better than that
using LP shunting in treating TBI. Using the V/BP ratio as a scale
of assessing the severity of hydrocephalus, the patients in the
experimental group were further separated into three subgroups,
i.e., the mild, the moderate and the severe hydrocephalus
subgroups, and the clinical outcomes were compared among them. It
turned out that the effective rates in the severe, the moderate and
the mild hydrocephalus subgroups were 33.33, 76.47 and 94.44%,
respectively. The effective rate in the moderate hydrocephalus
subgroup was significantly higher than that in the severe
hydrocephalus subgroup, and the difference was statistically
significant (P<0.05). The effective rate in the mild
hydrocephalus subgroup was significantly higher than that in the
severe hydrocephalus subgroup, and the difference was statistically
significant (P<0.05). These findings suggest that VP shunting
can better benefit patients with mild or moderate hydrocephalus
than patients with severe hydrocephalus. The aforementioned results
of the present study are consistent with a previous report
(25). Also, as numerous
complications have been reported after a ventricular shunting
surgery (26), the incidence of
complications was also assessed in this study. The incidence of
complications following LP shunting surgery (26.00%) was
significantly higher than that following VP shunting surgery
(12.00%), and the difference was statistically significant
(χ2=66.04, P<0.05). Due to the use of shunt cannulas
in VP shunting surgery, the chance of a shunt obstruction and the
incidence of complications were low. The infection rate in the LP
group (8.00%) was higher than VP group (4.00%) in this experiment,
which may be related to the indications of LP, the patient's
personal condition, medical level, and surgical disadvantages. It
has been reported that the ventricular shunting effect can be
directly adjusted, leading to a low incidence of complications
(15), which is in accordance with
the results of this study. In the present study, preoperative and
postoperative neurological deficit scores were obtained to assess
the impact of ventricular shunting surgeries on patients'
awareness, response, and language. The neurological deficit scores
before and after treatment in the experimental group were
28.63±8.90 and 15.42±5.23, respectively, while the neurological
deficit scores before and after treatment in the control group were
28.59±8.57 and 22.54±6.84, respectively. There was no significant
difference in neurological deficit score between the two groups
before surgery (t=0.023, P=0.982). However, the difference in
neurological deficit score between the two groups was statistically
significant after surgery (t=5.847, P<0.05). These findings
suggest that VP shunting surgery has less negative impact on
postoperative neurological function, and this is consistent with a
literature report (27). We followed
up the patient's clinical efficacy to obtain satisfactory
outcomes.
Due to the small sample size in this study, the
results may contain certain biased findings. Therefore, more
subjects will be enrolled for future studies.
In summary, VP shunting provides more benefits than
LP shunting in patients with hydrocephalus after TBI, including low
incidence of complications and better quality of life. Also, a
better outcome is achieved when the patient has milder
hydrocephalus. Therefore, patients with hydrocephalus should be
early diagnosed and timely treated with VP shunting.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FM drafted the manuscript. FM and HW were
responsible for the assessment of indicators. FM and SY performed
the LP shunting surgery. SY assisted with statistical analysis. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Shanxian Central Hospital (Heze, China) and written informed
consents were obtained by the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hyder AA, Wunderlich CA, Puvanachandra P,
Gururaj G and Kobusingye OC: The impact of traumatic brain
injuries: A global perspective. NeuroRehabilitation. 22:341–353.
2007.PubMed/NCBI
|
|
2
|
Ommaya AK and Gennarelli TA: Cerebral
concussion and traumatic unconsciousness. Correlation of
experimental and clinical observations of blunt head injuries.
Brain. 97:633–654. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
McCrea M, Iverson GL, McAllister TW,
Hammeke TA, Powell MR, Barr WB and Kelly JP: An integrated review
of recovery after mild traumatic brain injury (MTBI): Implications
for clinical management. Clin Neuropsychol. 23:1368–1390. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Graham DI, Adams JH and Doyle D: Ischaemic
brain damage in fatal non-missile head injuries. J Neurol Sci.
39:213–234. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bryant RA, O'Donnell ML, Creamer M,
McFarlane AC, Clark CR and Silove D: The psychiatric sequelae of
traumatic injury. Am J Psychiatry. 167:312–320. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Taylor CA, Bell JM, Breiding MJ and Xu L:
Traumatic brain injury-related emergency department visits,
hospitalizations, and deaths - United States, 2007 and 2013. MMWR
Surveill Summ. 66:1–16. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ommaya AK, Goldsmith W and Thibault L:
Biomechanics and neuropathology of adult and paediatric head
injury. Br J Neurosurg. 16:220–242. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang J, Williams MA and Rigamonti D:
Genetics of human hydrocephalus. J Neurol. 253:1255–1266. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bering EA Jr and Sato O: Hydrocephalus:
Changes in formation and absorption of cerebrospinal fluid within
the cerebral ventricles. J Neurosurg. 20:1050–1063. 1963.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dixon GR, Friedman JA, Luetmer PH, Quast
LM, McClelland RL, Petersen RC, Maher CO and Ebersold MJ: Use of
cerebrospinal fluid flow rates measured by phase-contrast MR to
predict outcome of ventriculoperitoneal shunting for idiopathic
normal-pressure hydrocephalus. Mayo Clin Proc. 77:509–514. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Battal B, Kocaoglu M, Bulakbasi N, Husmen
G, Tuba Sanal H and Tayfun C: Cerebrospinal fluid flow imaging by
using phase-contrast MR technique. Br J Radiol. 84:758–765. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schoenbaum SC, Gardner P and Shillito J:
Infections of cerebrospinal fluid shunts: Epidemiology, clinical
manifestations, and therapy. J Infect Dis. 131:543–552. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reddy GK, Bollam P, Caldito G, Willis B,
Guthikonda B and Nanda A: Ventriculoperitoneal shunt complications
in hydrocephalus patients with intracranial tumors: An analysis of
relevant risk factors. J Neurooncol. 103:333–342. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang J, Qu C, Wang Z, Wang C, Ding X, Pan
S and Ji Y: Improved ventriculoatrial shunt for cerebrospinal fluid
diversion after multiple ventriculoperitoneal shunt failures. Surg
Neurol. 72 (Suppl 1):S29–S34. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Grosfeld JL, Cooney DR, Smith J and
Campbell RL: Intra-abdominal complications following
ventriculoperitoneal shunt procedures. Pediatrics. 54:791–796.
1974.PubMed/NCBI
|
|
16
|
Murtagh F and Lehman R: Peritoneal shunts
in the management of hydrocephalus. JAMA. 202:1010–1014. 1967.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Limbrick DD Jr, Baird LC, Klimo P Jr,
Riva-Cambrin J and Flannery AM; Pediatric Hydrocephalus Systematic
Review and Evidence-Based Guidelines Task Force, : Pediatric
hydrocephalus: systematic literature review and evidence-based
guidelines. Part 4: Cerebrospinal fluid shunt or endoscopic third
ventriculostomy for the treatment of hydrocephalus in children. J
Neurosurg Pediatr. 14 (Suppl 1):30–34. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hebb AO and Cusimano MD: Idiopathic normal
pressure hydrocephalus: A systematic review of diagnosis and
outcome. Neurosurgery. 49:1166–1186. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Constine LS, Konski A, Ekholm S, McDonald
S and Rubin P: Adverse effects of brain irradiation correlated with
MR and CT imaging. Int J Radiat Oncol Biol Phys. 15:319–330. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cao M and Wu JI: Camk2a-Cre-mediated
conditional deletion of chromatin remodeler Brg1 causes perinatal
hydrocephalus. Neurosci Lett. 597:71–76. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Walker WC and McDonald SD: Does neurologic
examination during inpatient rehabilitation help predict global
outcome after nonpenetrating traumatic brain injury? PM R. 3:6–12.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
McDonald S and Flanagan S: Social
perception deficits after traumatic brain injury: Interaction
between emotion recognition, mentalizing ability, and social
communication. Neuropsychology. 18:572–579. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yang XF, Wen L, Shen F, Li G, Lou R, Liu
WG and Zhan RY: Surgical complications secondary to decompressive
craniectomy in patients with a head injury: A series of 108
consecutive cases. Acta Neurochir (Wien). 150:1241–1248. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rekate HL: A contemporary definition and
classification of hydrocephalus. Semin Pediatr Neurol. 16:9–15.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chumas PD, Armstrong DC, Drake JM,
Kulkarni AV, Hoffman HJ, Humphreys RP, Rutka JT and Hendrick EB:
Tonsillar herniation: The rule rather than the exception after
lumboperitoneal shunting in the pediatric population. J Neurosurg.
78:568–573. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chung JJ, Yu JS, Kim JH, Nam SJ and Kim
MJ: Intraabdominal complications secondary to ventriculoperitoneal
shunts: CT findings and review of the literature. AJR Am J
Roentgenol. 193:1311–1317. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pudenz RH and Foltz EL: Hydrocephalus:
Overdrainage by ventricular shunts. A review and recommendations.
Surg Neurol. 35:200–212. 1991. View Article : Google Scholar : PubMed/NCBI
|