Introduction
Chronic cough (CC) is a common clinical condition
that may disrupt the everyday activities of affected patients,
including their work. The prevalence of CC among the adult
population has been reported to range between 13 and 32% (1). By definition, CC is a cough lasting
for >8 weeks in patients who have a normal chest radiograph, are
not receiving therapy with angiotensin-converting enzyme inhibitors
and have not been exposed to environmental irritants (1,2).
According to the data reported in the literature, cough variant
asthma (CVA), upper airway cough syndrome (UACS), allergic cough
(AC), eosinophilic bronchitis (EB) and gastroesophageal
reflux-related cough (GERC) are the major causes of CC, accounting
for ~70-95% of the causes in Chinese patients (3,4).
Certain patients may have more than one of these conditions.
However, in a significant number of patients, the cause of the
cough may remain elusive, or the cough may be refractory to
treatment, despite extensive investigations and therapeutic trials.
Unexplained chronic cough (UCC) is a major health concern that
occurs in up to 5-10% of the Chinese population (5,6).
Furthermore, although the aetiology may be identified in certain
patients, there is no effective treatment method or there may be no
treatment response, leading to persistent cough (7). Collectively, UCC and persistent cough
with poor therapeutic response are referred to as chronic
refractory cough (CRC), which occurs in up to 12-42% of cases
(8).
Chronic persistent cough may interrupt patients'
sleep, leading to exhaustion. Affected patients experience a marked
decline in their quality of life. They frequently seek medical help
at various hospitals throughout China, are repeatedly subjected to
a variety of examinations and receive a number of different drugs,
suffer from various adverse drug reactions and carry a heavy
financial burden (9). Furthermore,
persistent respiratory symptoms, particularly in young adults, are
associated with an accelerated decline in lung function, an
increased incidence of obstructive and restrictive physiological
conditions and an elevated risk of future lung diseases (10).
Helicobacter pylori (a H. pylori) is a
slow-growing, microaerophilic, gram-negative bacterium; its most
striking biochemical characteristic is the abundant production of
urease. The prevalence of a H. pylori positive state varies
from <40% in developed countries to >70% in developing
countries (11). a H. pylori
positive state is causally associated with various health
conditions, including chronic active gastritis, peptic ulcer
disease and gastric cancer (12).
Over the past few years, a variety of extradigestive disorders,
particularly respiratory system diseases, including chronic
bronchitis, bronchiectasis, pulmonary tuberculosis, asthma, chronic
obstructive pulmonary disease (COPD) and idiopathic pulmonary
fibrosis (IPF), have been reported to be associated with a H.
pylori positive state (13,14).
In addition, a H. pylori has been detected in the
tracheobronchial aspirates of mechanically ventilated patients and
the possibility that it may cause ventilator-associated pneumonia
has been raised. Furthermore, previous studies have investigated a
potential role for a H. pylori positive state in several
clinical conditions (15). Their
results demonstrated that a H. pylori positive state may be
associated with several clinical manifestations (16-18),
including chronic persistent cough. However, the exact underlying
mechanisms have remained elusive. The current retrospective study
was performed to investigate the role of a H. pylori
positive state in CC.
Materials and methods
Patients and selection criteria
A total of 278 adult patients referred to the
respiratory clinic of Shaoxing People's Hospital (Shaoxing, China)
due to chronic persistent cough over a 2-year enrolment period
(June 2016-May 2018), including outpatients and inpatients, were
enrolled in the present study. The control group was recruited from
the Physical Examination Centre of Shaoxing People's Hospital
(Shaoxing, China) and included 148 age- and sex-matched subjects
with no history of CC, of whom 87 were females and 61 were males
(female/male ratio, 1.4:1), with a mean age of 48.6 years (95% CI:
46.53-50.75). The CC group included 176 females and 102 males
(female/male ratio, 1.7:1), with a mean age of 48.2 years (95% CI:
34.86-61.46).
The patients with different types of cough were
required to meet the following inclusion and exclusion criteria: i)
Τhe major or only clinical symptom is a cough lasting for >8
weeks. ii) No exposure to environmental irritants. iii) Normal or
near-normal chest radiographs or chest CT scans (no or minor stable
inconsequential scarring). iv) No treatment with
angiotensin-converting enzyme inhibitors. v) No response to
antibiotic therapy. vi) Exclusion of chronic bronchitis,
bronchiectasis, typical asthma, COPD and interstitial lung disease.
vii) Exclusion of combination of two or more causes of CC.
Diagnosis
The diagnostic criteria according to Guidelines for
diagnosis and treatment of cough (version 2015) (19) for the different types of cough are
described below.
CRC
Persistent CC despite thorough investigation and
conventional treatment according to published practice
guidelines.
CVA
i) CC, usually irritating cough at night. ii) A
positive result through bronchial provocation tests or bronchial
dilation test or lung function mean diurnal peak expiratory flow
(PEF) variation rate index >10% (continuous detection for at
least 7 days). iii) Cough improved significantly or even
disappeared following anti-asthmatic treatments.
AC
i) CC, usually irritating dry cough. ii) Normal
pulmonary ventilation and a negative result through bronchial
provocation tests. iii) Normal numbers of sputum eosinophils. iv) A
positive result in detection of atopy or total serum immunoglobulin
(Ig) E levels or a history of allergic diseases or exposure to
allergenic substances. v) Cough improved significantly or even
disappeared after glucocorticoid or anti-histamine treatments.
UACS
i) Paroxysmal or persistent cough occurring more
frequently in the daytime, with disappearance or decrease during
sleep. ii) Clinical manifestation and medical history of nasal or
pharyngeal diseases. iii) Adjunctive examination supporting the
diagnosis of nasal or pharyngeal diseases. iv) Cough improved
significantly or even disappeared after treatment of the nasal or
pharyngeal diseases.
GERC
i) CC occurring mainly in the daytime, associated
with typical reflux symptoms (e.g. chest pain) or food intake. ii)
Symptom index ≥45% or DeMeester score ≥12.7 (24 h ambulatory
oesophageal pH monitoring) or symptom association probability ≥80%.
iii) Cough improved significantly or even disappeared after
anti-reflux therapy.
EB
i) CC, usually irritating dry cough, or cough with a
small amount of phlegm. ii) Normal pulmonary ventilation, no airway
hyperresponsiveness and normal lung function mean diurnal PEF
variation rate index. iii) Percentage of sputum eosinophils ≥2.5%.
iv) Exclusion of other diseases characterised by eosinophil
infiltration and proliferation. v) Cough improved significantly or
even disappeared after oral or inhaled glucocorticoid
treatment.
Other rare causes
i) Psychogenic cough: a) CC occurring only in the
daytime with disappearance during sleep or while focusing on
something. b) CC aggravated by a variety of psychological factors.
c) A negative result following thorough investigation of CC. d)
Exclusion of other causes of CC. e) Cough improved significantly or
even disappeared after psychotherapy, anti-anxiety or
anti-depressant therapy. ii) Post-infectious cough: a) CC
persisting after the disappearance of acute symptoms of respiratory
infections, usually irritating dry cough or with a small amount of
phlegm. b) Normal or near-normal (no more than stable
inconsequential scarring) chest radiographs or chest CT scans; c)
Exclusion of other causes of CC; d) Cough improved significantly or
even disappeared after anti-tussive, anti-histamine or decongestant
treatment.
Evaluation of cough severity
A self-administered symptom telephone questionnaire
was used to evaluate cough severity and its effect on the quality
of life on a ranking scale, with scores of 1, 2, 3 and 4 indicating
mild, moderate, severe and highly severe complaints with high
impairment of life quality, respectively.
Occasional cough was graded as mild (cough symptom
score, 1).
Intermittent cough without affecting the quality of
life (including the quality of sleep) was graded as moderate (cough
symptom score, 2).
Intermittent cough with a mild impairment of life
quality (including the quality of sleep) was graded as severe
(cough symptom score, 3).
Persistent cough with a serious impairment of life
quality (including the quality of sleep) was graded as highly
severe (cough symptom score, 4).
Clinical examination
The medical history of patients with CC frequently
provided important initial clues. The history of the patients
included in the present study was thoroughly recorded, including
meticulous assessment of the symptoms, by using telephone
interviews. The concurrent symptoms may suggest a suitable
diagnosis. At the Shaoxing People's Hospital, CC is diagnosed
strictly according to the diagnostic criteria outlined above.
Subsequently, the necessary examinations and experimental
treatments may be performed to make an accurate diagnosis and
clearly determine the causes of the CC.
Clinical examinations were performed, including
chest X-ray or CT, lung function measurements, including the
bronchodilatation test or bronchial provocation test,
esophagogastroduodenoscopy or 24-h ambulatory oesophageal pH
monitoring, nasal endoscopy, laryngoscopy, paranasal sinus X-ray or
CT, induced sputum eosinophils, bronchoscopy and detection of
atopy, total serum IgE levels, C-reactive protein (CRP),
erythrocyte sedimentation rate (ESR) and eosinophil (EO) count in
the peripheral blood. IgE levels >200 IU/ml were considered
positive. A a H. pylori positive state was assayed using the
13C or 14C urea exhalation test (01 tester;
Shenzhen Zhonghe Headway Biological Technology Co. Ltd.). All the
participants were examined on an empty stomach in the morning.
Certain patients with a H. pylori positive
state received a bismuth-containing quadruple therapy consisting of
amoxicillin (1 g twice daily), clarithromycin (500 mg twice daily)
and omeprazole (20 mg twice daily) for 14 days (20). The a H. pylori status was
followed up for 6 weeks after the completion of treatments. a H.
pylori eradication treatment was offered based on the
gastroenterologists' discretion according to the American College
of Gastroenterology Clinical Guidelines (version 2017) (21).
Statistical analysis
SPSS (version 20.0; IBM Corp.) statistical software
was used for data analysis. Multivariate analysis was used to
investigate the independent association of a H. pylori and
CC. Comparisons of log-transformed CRP and ESR values, blood EO
count, lung function indices [forced expiratory volume in 1 sec
(FEV1), forced vital capacity (FVC), maximal vital capacity
(VCmax)] as well as body height, body weight and body mass index
(BMI) between groups were performed by an unpaired Student's
t-test. The χ2 test was used to compare the prevalence
of a H. pylori positive state, symptom improvement rate,
atopy, serum IgE levels and other data including sex, age,
educational background and smoking status among groups. P<0.05
was considered to indicate a statistically significant
difference.
Results
Patient characteristics
The present study included a total of 426 subjects,
which were divided into two groups. The study group included 278
patients with chronic persistent cough, who were then subdivided
into 7 subgroups according to the causes of CC as described above
(CC: Cough lasting for >8 weeks in patients who exhibited a
normal chest radiograph, are not receiving therapy with
angiotensin-converting enzyme inhibitors and have not been exposed
to environmental irritants such as occupational dust and chemical
substances).
The control group recruited from the Physical
Examination Centre of Shaoxing People's Hospital included 148 age-
and sex-matched subjects with no history of CC or other respiratory
diseases. No significant difference in sex, age, body height, body
weight, BMI, educational background or smoking status was present
between the CC and control groups (P>0.05). In the CC group,
there was also no significant difference in sex, age, height,
weight, BMI, educational background and smoking status between a
H. pylori positive and negative cases (P>0.05). However,
patients with a H. pylori positive (Tables I, II and III).
 | Table IPatient characteristics. |
Table I
Patient characteristics.
|
Characteristics | CC group
(n=278) | Control group
(n=148) | P-value |
|---|
| Sex,
female/male | 176/102 | 87/61 | 0.36 |
| Age, years | 48.16±13.30 | 48.64±13.00 | 0.289 |
| Body height,
cm | 162.91±7.63 | 162.85±7.27 | 0.942 |
| Body weight,
kg | 62.38±9.92 | 59.88±11.00 | 0.018 |
| BMI,
kg/m2 | 23.44±2.86 | 22.48±3.19 | 0.22 |
| Education,
years | 9.80±4.20 | 10.21±3.72 | 0.517 |
| Smoking | | | |
| Pack years | 2.73±8.12 | 4.43±11.06 | 0.089 |
| Time since smoking
cessation, years | 0.24±1.60 | 0.21±1.24 | 0.502 |
| Table IICC patient characteristics. |
Table II
CC patient characteristics.
| Variable | H. pylori
positive | H. pylori
negative | P-value |
|---|
| Number | 170 | 108 | |
| Sex
(male/female) | 68/102 | 34/74 | 0.15 |
| Age | 46.54±12.42 | 50.71±14.27 | 0.07 |
| Heigh (cm) | 163.45±7.54 | 162.06±7.71 | 0.14 |
| Weight (Kg) | 62.53±10.60 | 62.13±8.80 | 0.74 |
| BMI | 23.31±2.95 | 23.64±2.73 | 0.35 |
| Education
(Years) | 9.49±4.38 | 10.27±3.83 | 0.06 |
| Smoking status Pack
years | 2.87±8.03 | 2.51±8.30 | 0.25 |
| Table IIIControl group patient
characteristics. |
Table III
Control group patient
characteristics.
| Variable | H. pylori
positive | H. pylori
negative | P-value |
|---|
| Number | 65 | 83 | |
| Sex
(male/female) | 30/35 | 31/52 | 0.28 |
| Age | 48.45±13.67 | 48.80±12.54 | 0.84 |
| Heigh (cm) | 163.06±7.36 | 162.69±7.23 | 0.76 |
| Weight (Kg) | 58.69±9.98 | 60.81±11.71 | 0.25 |
| BMI | 22.01±2.93 | 22.86±3.35 | 0.11 |
|
Education(years) | 9.12±3.75 | 11.11±3.36 | 0.02 |
| Smoking status Pack
years | 5.61±12.05 | 3.50±10.20 | 0.06 |
H. pylori positivity
The rate of H. pylori positivity was 170/278
(61.2%) in the CC group and 65/148 (43.9%) in the control group.
The difference was indicated to be statistically significant
(P<0.05). Furthermore, there were 42/61 (68.9%) a H.
pylori-positive cases in the CRC group (P<0.05), 69/113
(61.1%) in the CVA group (P<0.05), 16/26 (61.5%) in the AC group
(P>0.05), 13/20 (65%) in the UACS group (P>0.05) and 22/37
(59.5%) in the GERC group (P>0.05) compared with the control
group. The remaining two groups were not analysed due to
insufficient numbers of patients. The results are presented in
Table IV.
| Table IVPrevalence of H. pylori
positivity. |
Table IV
Prevalence of H. pylori
positivity.
| Group | H. pylori
(+), n/totals (%) | H. pylori
(-), n/totals (%) | P-value |
|---|
| CC | 170/278 (61.2) | 108/278 (38.8) | 0.001 |
| CRC | 42/61 (68.9) | 19/61 (31.1) | 0.001 |
| CVA | 69/113 (61.1) | 44/113 (38.9) | 0.006 |
| AC | 16/26 (61.5) | 10/26 (38.5) | 0.097 |
| UACS | 13/20 (65.0) | 7/20 (35.0) | 0.076 |
| GERC | 22/37 (59.5) | 15/37 (40.5) | 0.09 |
| EB | 5/11 (45.5) | 6/11 (54.5) | 0.921 |
| Other rare
reasons | 5/10 (50.0) | 5/10 (50.0) | 0.708 |
| Control | 65/148 (43.9) | 83/148 (56.1) | |
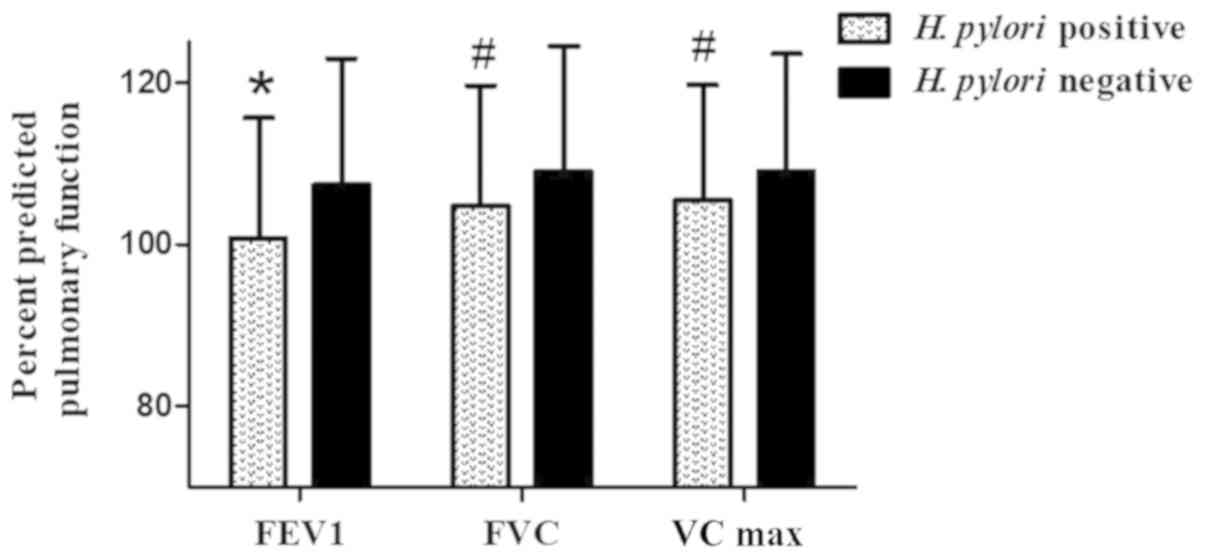
Pulmonary function
Patients with CC exposed to a H. pylori
exhibited lower lung function as compared with those who were not,
with a decrease in FEV1 by 84 ml, a decrease in FVC by 53 ml and a
decrease in VCmax by 46 ml (P>0.05). Although the difference did
not reach statistical significance, it became statistically
significant after adjusting for height, weight, age, sex and
ethnicity (the adjusted value was expressed as percent predicted
pulmonary function, P<0.05). There was no significant difference
in the aforementioned pulmonary function indices between a H.
pylori-positive and -negative cases in the control group
(P>0.05; Table VI).
| Table VIPredicted pulmonary function (%). |
Table VI
Predicted pulmonary function (%).
| | FEV1 | FVC | VCmax |
|---|
| Group | H. pylori
(+) | H. pylori
(-) | H. pylori
(+) | H. pylori
(-) | H. pylori
(+) | H. pylori
(-) |
|---|
| CC |
100.79±14.80a | 107.32±15.56 |
104.78±14.85a | 109.00±15.48 |
105.41±14.30a | 109.00±14.50 |
| CRC |
102.24±8.33a | 115.23±10.82 |
106.06±10.65a | 115.82±10.81 |
106.51±10.45a | 115.62±10.87 |
| CVA | 96.15±15.02 | 101.05±16.26 | 101.85±14.39 | 104.52±15.96 | 102.37±14.05 | 104.61±14.40 |
| AC | 106.11±18.73 | 108.41±15.62 | 106.00±21.00 | 106.50±13.66 | 107.32±18.93 | 107.42±14.05 |
| UACS |
98.01±13.10a | 112.19±11.32 | 103.68±16.93 | 114.30±15.83 | 102.48±17.18 | 112.06±14.48 |
| GERC | 110.58±15.32 | 109.12±13.68 | 111.94±15.40 | 110.15±17.97 | 113.74±13.74 | 109.61±17.76 |
| Control | 105.80±12.10 | 107.58±16.28 | 107.18±15.36 | 109.46±16.09 | 107.69±13.88 | 108.78±15.76 |
Furthermore, a subgroup analysis was performed.
Patients in the CRC group exposed to a H. pylori exhibited
lower lung function compared with those who were not, with a
decrease in FEV1 by 395 ml (P<0.05), a decrease in FVC by 335 ml
(P>0.05) and a decrease in VCmax by 314 ml (P>0.05). After
adjusting for height, weight, age, sex and ethnicity, effect
modification was observed for the association between a H.
pylori positive state and pulmonary function in the CRC group
(P<0.05). The percent predicted pulmonary function was
calculated using a prediction formula according to epidemiological
survey data of the East China area from Shanghai Zhongshan
Hospital, Fudan University (22).
The results are presented in Tables
V and VI and Figs. 1 and 2.
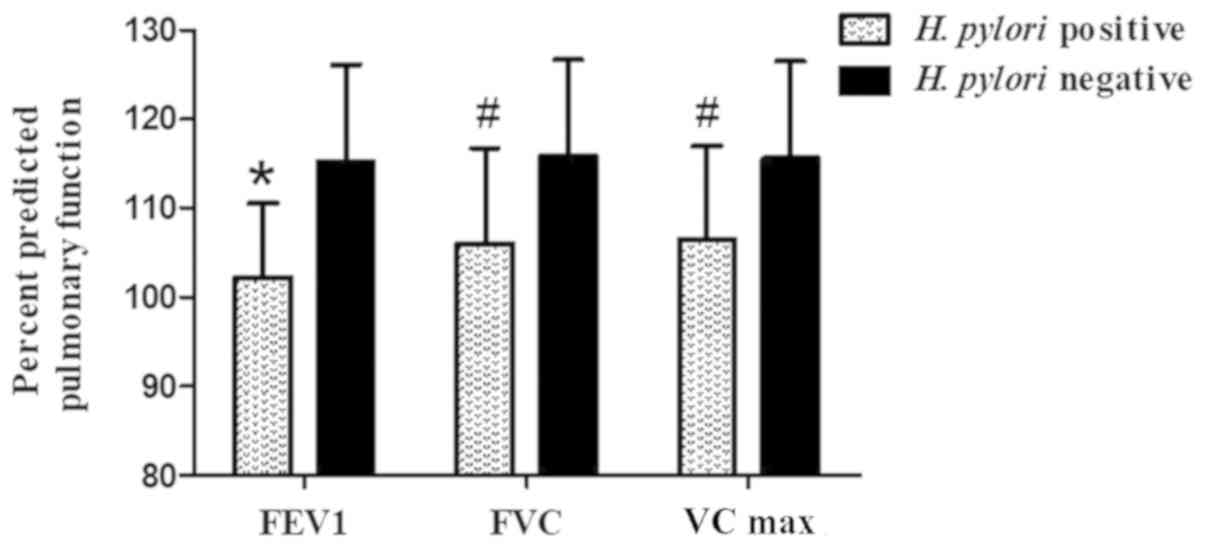 | Figure 2Predicted pulmonary function in the
chronic refractory cough group. Patients in the chronic refractory
cough group exposed to a H. pylori had lower lung function
than those who were not after adjusting for factors including
height, weight, age, sex and ethnicity. The adjusted value was
expressed as percent predicted pulmonary function. Values: A,
102.24±8.3 (P<0.001); B, 115.23±10.8; C, 106.06±10.6 (P=0.002);
D, 115.82±10.8; E, 106.51±10.4 (P=0.003); F, 115.62±10.9.
*P<0.001 and #P<0.05 vs. negative
group. FEV1, forced expiratory volume in 1 sec; FVC, forced vital
capacity; VCmax, maximal vital capacity. |
| Table VPulmonary function. |
Table V
Pulmonary function.
| | FEV1, l | FVC, l | VCmax, l |
|---|
| Group | H. pylori
(+) | H. pylori
(-) | H. pylori
(+) | H. pylori
(-) | H. pylori
(+) | H. pylori
(-) |
|---|
| CC | 2.85±0.74 | 2.93±0.84 | 3.59±0.89 | 3.65±0.99 | 3.70±0.91 | 3.75±0.99 |
| CRC |
2.98±0.61a | 3.37±0.85 | 3.74±0.69 | 4.08±1.04 | 3.86±0.72 | 4.17±1.01 |
| CVA | 2.62±0.71 | 2.80±0.90 | 3.37±0.85 | 3.56±1.04 | 3.46±0.86 | 3.68±1.06 |
| AC | 2.92±0.58 | 2.82±0.86 | 3.59±0.89 | 3.40±1.09 | 3.74±0.86 | 3.51±1.08 |
| UACS | 2.91±0.91 | 2.89±0.71 | 3.69±1.12 | 3.59±0.90 | 3.76±1.18 | 3.61±0.88 |
| GERC | 3.25±0.86 | 2.97±0.75 | 4.04±1.03 | 3.66±0.96 | 4.20±1.03 | 3.73±0.99 |
| Control | 2.94±0.69 | 2.92±0.78 | 3.63±0.85 | 3.63±0.95 | 3.75±0.87 | 3.71±0.96 |
Atopy and total IgE
Patients with CC who were a H.
pylori-positive had fewer allergic conditions compared with
those who were a H. pylori-negative, as evaluated by
determination of atopy and total serum IgE levels (P<0.05).
There was no statistically significant association between a H.
pylori exposure and allergic conditions in the CVA and AC
groups. However, the subgroup analysis according to age revealed an
inverse association between a H. pylori positive state and
allergic conditions in those patients. The allergic status differed
significantly according to age between a H. pylori-positive
and -negative cases in the CVA and AC groups. Among the patients
aged <40 years, a H. pylori-positive patients had a lower
prevalence of atopy compared with a H. pylori-negative cases
(46.9 vs. 81.8%, P<0.05). After defining serum IgE levels
>200 IU/ml as positives, there was a significantly reduced
number of IgE-positive patients in the H. pylori-positive
subgroup among patients aged <40 years (37.5 vs. 72.7%,
P<0.05). The results are provided in Table VII.
| Table VIIAssociation between H. pylori
exposure and allergic conditions. |
Table VII
Association between H. pylori
exposure and allergic conditions.
| Groups | Atopy (+), n/total
(%) | P-value | IgE, n/total
(%) | P-value |
|---|
| Chronic cough | | | | |
|
H.
pylori (+) | 46/170 (27.1) | <0.05 | 46/170 (27.1) | <0.05 |
|
HP (-) | 43/108 (39.8) | | 44/108 (40.7) | |
| CVA and AC | | | | |
|
H.
pylori (+) | 60/88 (68.2) | >0.05 | 44/88 (50.0) | >0.05 |
|
H.
pylori (-) | 35/53 (66.0) | | 33/53 (62.3) | |
| Age <40 years
(CVA and AC) | | | | |
|
H.
pylori (+) | 15/32 (46.9) | <0.05 | 12/32 (37.5) | <0.05 |
|
H.
pylori (-) | 9/11 (81.8) | | 8/11 (72.7) | |
| Control group | | | | |
|
H.
pylori (+) | 9/65 (13.8) | >0.05 | 4/65 (6.2) | >0.05 |
|
H.
pylori (-) | 9/83 (10.8) | | 6/83 (7.2) | |
CRP, ESR and EO in the peripheral
blood
There was no significant association between H.
pylori status and CRP, ESR or EO count in the peripheral blood
following the log-transformation (P>0.05). The results of the
subgroup analysis according to the cause of CC were consistent
(P>0.05; Data not shown). The results are presented in Table VIII.
| Table VIIIAssociation between H. pylori
exposure and systemic inflammation. |
Table VIII
Association between H. pylori
exposure and systemic inflammation.
| Group | H. pylori
(+), n (%) | H. pylori
(-), n (%) | P-value |
|---|
| Chronic cough | | | |
|
CRP | 2.24±6.54 | 3.43±10.68 | 0.309 |
|
Log CRP | -0.01±0.46 | 0.03±0.51 | 0.511 |
|
ESR | 10.35±8.31 | 11.78±13.42 | 0.419 |
|
Log ESR | 0.88±0.36 | 0.88±0.40 | 0.943 |
|
EO | 0.16±0.18 | 0.16±0.32 | 0.914 |
|
Log EO | -0.94±0.36 | -1.01±0.40 | 0.175 |
| Control group | | | |
|
CRP | 4.58±11.19 | 3.02±6.23 | 0.316 |
|
Log CRP | 0.13±0.66 | 0.05±0.60 | 0.486 |
|
ESR | 13.68±24.04 | 13.91±18.10 | 0.962 |
|
Log ESR | 0.88±0.30 | 0.88±0.35 | 0.996 |
|
EO | 0.13±0.11 | 0.11±0.10 | 0.326 |
|
Log EO | -1.02±0.38 | -1.10±0.41 | 0.263 |
Effect of a H. pylori eradication
Patients with CC exposed to H. pylori had
higher cough symptom scores and poorer therapeutic responses (cough
symptom score: 2.92±0.93 in H. pylori-positives vs.
2.50±0.92 in H. pylori-negatives; P<0.001). The patients
with CRC were followed up. A total of 29 patients with CRC received
H. pylori eradication treatment, 19 of whom exhibited an
improvement in the cough and the cough-specific quality of life at
1-2 months after successful eradication (improvement was defined as
a reduction in the ranking scores of the evaluated symptoms of at
least 1). However, a long-term follow-up study is required to fully
elucidate the effect of H. pylori eradication on pulmonary
function. The results are presented in Table IX.
| Table IXCough symptom score in chronic cough
and CRC groups (a H. pylori positive vs. a H. pylori
negative). |
Table IX
Cough symptom score in chronic cough
and CRC groups (a H. pylori positive vs. a H. pylori
negative).
| Group | H. pylori
positive | H. pylori
negative | P-value |
|---|
| Cough symptom
score | | | |
|
Chronic
cough | 2.92±0.93 | 2.50±0.92 | P<0.001 |
|
CRC | 3.19±0.86 | 2.26±0.87 | P<0.001 |
Discussion
Since Warren and Marshall (23) reported on the culture of a spiral
bacterium from the stomach in 1983, subsequently named a H.
pylori, the causative role of this gram-negative bacterium in
various upper-gastrointestinal-tract diseases has been increasingly
recognized (24,25). With advancing research, several
studies focused on the association between a H. pylori
positive state and extra digestive diseases, including respiratory
system diseases (26,27). It was reported by scholars from
Alexandria University that a H. pylori positive state may
lead to several clinical manifestations of respiratory-tract
diseases (15). Furthermore, a
H. pylori has been identified in the tracheobronchial
aspirates of mechanically ventilated patients and may cause
ventilator-associated pneumonia (28). This prompted us to investigate the
possible association between a H. pylori positive state and
CC, particularly CRC.
The present study revealed that a high percentage
(up to 61.2%) of patients with CC suffered from active a H.
pylori infection (29),
particularly those with CRC (up to 68.9%). This was significantly
higher compared with the percentage of active a H. pylori
positive state among controls without cough (43.9%). Subsequently,
a follow-up study was performed by telephone interviews. The
results revealed that 65.5% (19/29) of patients with CRC who had
received a H. pylori eradication treatment exhibited an
improvement in their cough and the cough-associated quality of life
at 1-2 months after successful eradication. Thus, it may be
inferred from the results that there may be a potential association
between a H. pylori positive state and CC. The results of
the present study are consistent with those reported by a study
from the Alexandria University (15).
While the pathogenetic mechanisms underlying the
effects of a H. pylori on airway disorders remain to be
determined, they may involve chronic inflammation promoted by
persistent infection with a H. pylori (30,31).
It is well-known that a H. pylori colonization of the
gastric mucosa stimulates the release of various pro-inflammatory
factors, including cytokines and eicosanoids. The
neutrophil-activating protein of a H. pylori is a major
pro-inflammatory factor that not only has a key role in driving
T-helper type 1 (Th1) inflammation, but is also able to inhibit
Th2-mediated bronchial inflammation (32,33).
Talaat et al (15) suggested
that continuous release of inflammatory mediators by a H.
pylori may result in direct or indirect effects on the
oesophageal mucosa, which increased its sensitivity to acid and
affected the motility of the oesophageal sphincter. As a result,
exposure of the lower oesophagus to comparably short-term reflux
episodes, through vagally mediated reflexes, may result in
persistent cough.
Furthermore, a H. pylori is capable of
adhering to epithelial cell lines originally derived from different
organs, including respiratory tract epithelial cells. a H.
pylori was recently identified in the tracheobronchial
aspirates of mechanically ventilated patients and there may be an
association between a H. pylori and ventilator-associated
pneumonia (28). A study from Japan
demonstrated that a H. pylori VacA, the major exotoxin of a
H. pylori, was present in the human lung and induced
inflammatory factor production by human lung cells (34). It is possible that a H.
pylori is aspirated into the respiratory tract from the
oropharynx or the gastric reservoir, thereby causing chronic
persistent cough. This chronic microaspiration may be involved in
chronic inflammatory injuries of the airway epithelia, as well as a
systemic immune response that affects the respiratory system in
susceptible patients. VacA may exert a local immunosuppressive
effect. VacA inhibits the production of interleukin (IL)-2, which
is required for T-cell viability and proliferation, and
downregulates the surface expression of IL-2 receptor-α (32). In addition, it was reported that
VacA induced apoptosis by release of cytochrome c from mitochondria
and activation of caspase-3, which may lead to airway injury
(35).
A clinical study from the Nottingham City Hospital
demonstrated that individuals with a H. pylori positive
state exhibited decreased lung function, with FEV1 being lower by
53 ml and FVC by 83 ml in their cross-sectional analysis, although
this association was not independent of body height or the
socioeconomic status (36). Similar
results were reported by a Canadian study, which demonstrated that
patients who were seropositive for a H. pylori had lower
FEV1 values compared with individuals who were seronegative for a
H. pylori; however, the significance of the association
between FEV1 and a H. pylori seropositivity disappeared when
FEV1 percent predicted values were used (37). Furthermore, previous studies
demonstrated that a H. pylori positive state was associated
with reduced lung function in patients with COPD and IPF, which is
most likely due to the effect of the bacterium on lung growth
earlier in life (38,39). Systemic inflammation may also be a
contributing factor.
The present study investigated the effect of a H.
pylori positive state on lung function, as well as the systemic
inflammation as evaluated by CRP, ESR, IgE and peripheral blood EO
count in patients with CC. The results demonstrated that patients
exposed to a H. pylori in the CC group had a lower percent
predicted lung function compared with those who were negative for
H. pylori. The difference was even more obvious in the CRC
group. Furthermore, there was no association between a H.
pylori status and lung function in the control group.
Therefore, it may be inferred that in patients with CC, a H.
pylori positive state is associated with decreased lung
function, although further studies and a long-term follow-up are
required to confirm this potential association. However, no
significant association was observed between a H. pylori
positive state and systemic inflammation markers, including CRP,
ESR, IgE and EO count.
Persistent airway injury and inflammation cause
airway remodelling and a progressive impairment of lung function,
leading to chronic airway diseases. Studies have demonstrated that
in young adults, persistent respiratory symptoms, including
persistent cough, were associated with an accelerated decline in
lung function, incidence of obstructive and restrictive physiology
and a higher risk of future radiographic emphysema (10,40).
The potential association between a H. pylori positive state
and CC indicates that the presence of cough-associated respiratory
symptoms and persistent airway inflammation induced by a H.
pylori may serve as a prognostic marker for accelerated decline
in lung function and future lung diseases. This association was
more obvious in patients with CRC.
A meta-analysis demonstrated that a H. pylori
positive state was associated with an estimated 18% reduction in
the risk of atopy, as estimated by allergen skin tests and specific
IgE (41). Whether a H.
pylori positive state is inversely associated with allergic
diseases remains controversial (42-45).
An experimental study demonstrated that oral immunomodulators with
a H. pylori extract prevented airway hyperresponsiveness,
bronchoalveolar eosinophilia, pulmonary inflammation and Th2
cytokine production, which are hallmarks of allergen-induced
asthma, in mice (44). Similar
results were also obtained in a recent study (45). Furthermore, several large
cross-sectional and case-control studies demonstrated an inverse
association between a H. pylori positive state and allergic
diseases, including inflammatory airway diseases (44). However, others reported no
association or a weak inverse association (41). In the present study, patients with
CC who were a H. pylori-positive had fewer allergic
conditions compared with those who were a H.
pylori-negative, as evaluated by determination of atopy and
total serum IgE levels. However, there was no statistically
significant association between H. pylori exposure and
allergic conditions in the CVA and AC groups. Of note, the subgroup
analysis according to age revealed an inverse association between a
H. pylori positive state and allergic conditions in those
patients. Among those aged <40 years, a H.
pylori-positive patients had a lower prevalence of atopy and
serum IgE levels compared with a H. pylori-negative cases.
The present results were in line with Korean studies, according to
which the association of IgE hypersensitivity and allergic diseases
with a H. pylori positive state differed depending on age
(44,46). Another study observed that early
exposure to H. pylori was inversely associated with allergic
conditions, which was possibly linked to infection with
CagA+ strains of H. pylori (41).
The gradual loss of the human indigenous microbiota
may be implicated in the increasing trend in the prevalence of
allergic diseases (42). H.
pylori, as a bacterial pathogen, is a constituent of the normal
gastric microbiota, which may partly explain the inverse
association between a H. pylori positive state and allergic
conditions in patients with CVA and AC aged <40 years (42). According to the ‘decreasing
microbiota hypothesis’, the intestinal microbiota affects the
immune system and commensal bacteria regulate the Th1/Th2
equilibrium. H. pylori, an ancient indigenous microbe, is
expected to affect the immune system by shifting the cytokine
balance toward the Th1 type, which suppresses Th2-dominated
allergic diseases. It has been reported that H. pylori
alters the T-cell response by inducing the expression of IL-12,
tumour necrosis factor-α and interferon-γ by T-cells. In the
present study, an inverse association between H. pylori and
allergic conditions in patients with CVA and AC aged <40 years,
but not in those aged >40 years was identified. The reason for
this remains elusive; however, it may be associated with the
pathophysiological processes of CVA and AC, which also require
further study. In addition, this is complicated by the fact that
certain children may change back from a positive to a negative
status of H. pylori positivity. In a population-based birth
cohort in Ethiopia, 17% of children with evidence of a H.
pylori positive state at the age of 3 years ceased to be
negative at the age of 5 years (47). The issue of the fluctuating exposure
status remains a major challenge.
Patients with chronic persistent cough experience a
significant reduction in their quality of life, particularly
patients with refractory chronic persistent cough. Persistent cough
in young adults was associated with accelerated decline in lung
function, which was associated with a greater risk of future
development of lung diseases, including COPD. Therefore, it is
crucial to develop an effective treatment. The present study raised
the possibility that H. pylori may be a cause of chronic
cough, and that eradication of this pathogen may resemble a
potential treatment. In certain patients with CRC, including those
with unexplained chronic cough, the symptoms subsided after a
successful H. pylori eradication, which may prevent the
decline in lung function and airway remodelling. In addition, a
vaccination for preventing or treating a H. pylori infection
may be of value, particularly during childhood. Since a recent
mouse study demonstrated that the protective effect of H.
pylori against allergic diseases did not require live bacteria,
treatment with an extract of H. pylori in neonates may
prevent the development of airway allergic diseases (48,49).
The application of H. pylori extract, particularly in early
life, may be an effective prevention and treatment measure for CVA
and AC (43). Of note, the present
study had certain limitations. A larger sample size and multicentre
prospective clinical trials are required to verify the
effectiveness of this novel potential clinical therapeutic
strategy.
In conclusion, the results of the present study
support the theory of a potential association between a H.
pylori positive state and CC, including CRC, CVA and AC. In
addition, HPI may be associated with the accelerated decline of
lung function in patients with chronic persistent cough, which may
lead to irreversible airway remodelling and even the future
development of chronic airway diseases. However, there is an
inverse association between HPI and allergic diseases, including
CVA and AC. Thus, H. pylori may be a promising target for
the treatment of chronic persistent cough. However, further
research is required.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from Department of
Health of Zhejiang Province, China (grant no. 2019KY226) and
Shaoxing Bureau of Science and Technology, Zhejiang Province, China
(grant no. 2018C30097). It was also supported by Zhejiang
Provincial Natural Science Foundation of China under Grant No.
LQ20H010001.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MH and KT designed the research and did most of the
work. JS was mainly responsible for the interpretation of data, and
also revised it critically for the important intellectual content.
AM and YZ were mainly responsible for the acquisition and analysis
of data. CZ, YY and HW were mainly accountable for ensuring the
questions related to the accuracy or integrity of the work to be
appropriately investigated and resolved, and performed the
experiments. YC and MX also performed some of the experiments. All
the authors read and approved the final manuscript.
Ethics approval and consent to
participate
This article does not contain any prospective
studies with human participants or animals performed by any of the
authors. It was approved by leaders of Shaoxing People's Hospital
and registered and approved by the ethics committee of Shaoxing
People's Hospital (Shaixing, China). Informed consent was obtained
from all individual participants included in the study by telephone
interviews.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Smith JA and Woodcock A: Chronic cough. N
Engl J Med. 376:183–184. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chung KF: IFN-γ: A driver of cough
hypersensitivity pathways in chronic cough. Am J Respir Crit Care
Med. 198:827–828. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Herregods TVK, Pauwels A, Jafari J, Sifrim
D, Bredenoord AJ, Tack J and Smout AJPM: Determinants of
Reflux-induced chronic cough. Gut. 66:2057–2062. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Song WJ, Kim HJ, Shim JS, Won HK, Kang SY,
Sohn KH, Kim BK, Jo EJ, Kim MH, Kim SH, et al: Diagnostic accuracy
of fractional exhaled nitric oxide measurement in predicting
cough-variant asthma and eosinophilic bronchitis in adults with
chronic cough: A systematic review and meta-analysis. J Allergy
Clin Immunol. 140:701–709. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Gibson P, Wang G, McGarvey L, Vertigan AE,
Altman KW and Birring SS: Treatment of Unexplained Chronic Cough:
CHEST guideline and expert panel report. Chest. 149:27–44.
2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Millqvist E: The problem of treating
unexplained chronic cough. Chest. 149:613–614. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Abdulqawi R, Dockry R, Holt K, Layton G,
McCarthy BG, Ford AP and Smith JA: P2X3 receptor antagonist
(AF-219) in refractory chronic cough: A randomised, Double-blind,
Placebo-controlled phase 2 study. Lancet. 385:1198–1205.
2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gopal AK, Schuster SJ, Fowler NH, Trotman
J, Hess G, Hou JZ, Yacoub A, Lill M, Martin P, Vitolo U, et al:
Ibrutinib as treatment for patients with relapsed/refractory
follicular lymphoma: Results from the open-label, multicenter,
phase II DAWN study. J Clin Oncol. 36:2405–2412. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Smith JA, Haines J and Yorke J: Taming
chronic cough. Thorax. 72:103–104. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kalhan R, Dransfield MT, Colangelo LA,
Cuttica MJ, Jacobs DR Jr, Thyagarajan B, Estepar RSJ, Harmouche R,
Onieva JO, Ash SY, et al: Respiratory symptoms in young adults and
future lung disease The CARDIA lung study. Am J Respir Crit Care
Med. 197:1616–1624. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Choi IJ, Kim YI and Park B:
Helicobacter pylori and prevention of gastric cancer. N Engl
J Med. 378:2244–2245. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Abbasi J: Barry marshall and MD: H
pylori 35 Years Later. JAMA. 317:1400–1402. 2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ehrlich D, Naini B and Mukewar S: A rare
cause of gastric wall thickening. Gastroenterology. 154:e18–e20.
2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Koch KN, Hartung ML, Urban S, Kyburz A,
Bahlmann AS, Lind J, Backert S, Taube C and Müller A: Helicobacter
urease-induced activation of the TLR2/NLRP3/IL-18 Axis protects
against asthma. J Clin Invest. 125:3297–302. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Talaat M, Gad MS, Magdy EA, Aggag SM and
Nour YA: Helicobacter pylori infection and chronic,
persistent cough: Is there an association. J Laryngol Otol.
121:962–7. 2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wang L, Guan Y, Li Y, Liu X, Zhang Y, Wang
F, Kong L and Guo Q: Association between chronic respiratory
diseases and Helicobacter pylori: A meta-analysis. Arch
Bronconeumol. 51:273–278. 2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kreuter M, Kirsten D, Bahmer T, Penzel R,
Claussen M, Ehlers-Tenenbaum S, Muley T, Palmowski K, Eichinger M,
Leider M, et al: Screening for Helicobacter pylori in
idiopathic pulmonary fibrosis lung biopsies. Respiration. 91:3–8.
2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hong L, Li S, Feng Q, Feng X, Jin Y, Zhao
Q and Zhang H: H. pylori infection may cause sleep-related
laryngospasm for a patient in climacteric. J Pain Symptom Manage.
39:e6–e7. 2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kefang Lai, et al: Guidelines for
diagnosis and treatment of cough (2015). Chinese Journal of
Tuberculosis and Respiratory Diseases: 323-354, 2016.
|
|
20
|
Liou JM, Fang YJ, Chen CC, Bair MJ, Chang
CY, Lee YC, Chen MJ, Chen CC, Tseng CH, Hsu YC, et al: Concomitant,
bismuth quadruple, and 14-day triple therapy in the First-line
treatment of Helicobacter pylori: A multicentre, Open-label,
randomised trial. Lancet. 388:2355–2365. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Chey WD, Leontiadis GI, Howden CW and Moss
SF: ACG Clinical Guideline: Treatment of Helicobacter pylori
Infection. Am J Gastroenterol. 112:212–239. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Zhao RY, Zhu L, Li L, Chen Q and Yang YJ:
The applicability of the 1988 version of the prediction equations
for adult normal lung function in Shanghai. Zhonghua Jie He He Hu
Xi Za Zhi. 34:586–589. 2011.PubMed/NCBI(In Chinese).
|
|
23
|
Parsonnet J:
Clinician-discoverers-Marshall, Warren, and H. pylori. N
Engl J Med. 353:2421–2423. 2005.
|
|
24
|
Lanas A and Chan FKL: Peptic ulcer
disease. Lancet. 390:613–624. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kim IJ, Lee J, Oh SJ, Yoon MS, Jang SS,
Holland RL, Reno ML, Hamad MN, Maeda T, Chung HJ, et al:
Helicobacter pylori Infection modulates host cell metabolism
through VacA-dependent inhibition of mTORC1. Cell Host Microbe.
23:583–593.e8. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kariya S, Okano M and Nishizaki K: An
Association between Helicobacter pylori and upper
respiratory tract disease: Fact or fiction. World J Gastroenterol.
20:1470–1484. 2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
De Korwin JD, Ianiro G, Gibiino G and
Gasbarrini A: Helicobacter pylori infection and extragastric
diseases in 2017. Helicobacter: 22 (Suppl 1), 2017 doi:
10.1111/hel.12411.
|
|
28
|
Gülhan M, Ozyilmaz E, Tarhan G, Demirağ F,
Capan N, Ertürk A, Canbakan S, Ayaşlioğlu E, Gülhan E and Ahmed K:
Helicobacter pylori in bronchiectasis: A polymerase chain
reaction assay in bronchoalveolar lavage fluid and bronchiectatic
lung tissue. Arch Med Res. 38:317–321. 2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
El-Serag HB, Kao JY, Kanwal F, Gilger M,
LoVecchio F, Moss SF, Crowe SE, Elfant A, Haas T, Hapke RJ and
Graham DY: Houston consensus conference on testing for
Helicobacter pylori Infection in the United states. clin
gastroenterol hepatol. 16:992–1002.e6. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Rossi AF, Cadamuro AC, Biselli-Perico JM,
Leite KR, Severino FE, Reis PP, Cordeiro JA and Silva AE:
Interaction between inflammatory mediators and miRNAs in
Helicobacter pylori Infection. Cell Microbiol. 18:1444–1458.
2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Barrozo RM, Hansen LM, Lam AM, Skoog EC,
Martin ME, Cai LP, Lin Y, Latoscha A, Suerbaum S, Canfield DR, et
al: CagY is an Immune-sensitive regulator of the Helicobacter
pylori type iv secretion system. Gastroenterology.
151:1164–1175.e3. 2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
D'Elios MM, Montecucco C and de Bernard M:
VacA and HP-NAP, Ying and Yang of Helicobacter
pylori-associated gastric inflammation. Clin Chim Acta.
381:32–38. 2007.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ramachandran M, Jin C, Yu D, Eriksson F
and Essand M: Vector-encoded Helicobacter pylori
neutrophil-activating protein promotes maturation of dendritic
cells with Th1 polarization and Improved Migration. J Immunol.
193:2287–2296. 2014.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Nakashima S, Kakugawa T, Yura H, Tomonaga
M, Harada T, Hara A, Hara S, Nakano M, Yamasaki E, Sakamoto N, et
al: Identification of Helicobacter pylori vaca in human lung
and its effects on lung cells. Biochem Biophys Res Commun.
460:721–726. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Montecucco C and de Bernard M:
Immunosuppressive and proinflammatory activities of the VacA Toxin
of Helicobacter pylori. J Exp Med. 198:1767–1771.
2003.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Fullerton D, Britton JR, Lewis SA, Pavord
ID, McKeever TM and Fogarty AW: Helicobacter pylori and lung
function, asthma, atopy and allergic disease-a population-based
cross-sectional study in adults. Int J Epidemiol. 38:419–426.
2009.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Gencer M, Ceylan E, Yildiz ZF and Aksoy N:
Helicobacter pylori seroprevalence in patients with chronic
obstructive pulmonary disease and its relation to pulmonary
function tests. Respiration. 74:170–175. 2007.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Sze MA, Chen YW, Tam S, Tashkin D, Wise
RA, Connett JE, Man SP and Sin DD: The relationship between
Helicobacter pylori Seropositivity and COPD. Thorax.
70:923–929. 2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Fogarty AW: Does Helicobacter
pylori Infection modify lung development, height or simply
reflect shared environmental exposures. Thorax.
70(918)2015.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Wang C, Xu J, Yang L, Xu Y, Zhang X, Bai
C, Kang J, Ran P, Shen H, Wen F, et al: China pulmonary health
study group Prevalence and risk factors of chronic obstructive
pulmonary disease in China (the China Pulmonary Health [CPH]
study): A national Cross-sectional study. Lancet. 391:1706–1717.
2018.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Taye B, Enquselassie F, Tsegaye A,
Amberbir A, Medhin G, Fogarty A, Robinson K and Davey G:
Association between infection with Helicobacter pylori and
atopy in young ethiopian children: A longitudinal study. Clin Exp
Allergy. 47:1299–1308. 2017.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Engler DB, Reuter S, van Wijck Y, Urban S,
Kyburz A, Maxeiner J, Martin H, Yogev N, Waisman A, Gerhard M, et
al: Effective treatment of allergic airway inflammation with
Helicobacter pylori immunomodulators requires
BATF3-dependent dendritic cells and IL-10. Proc Natl Acad Sci USA.
111:11810–11815. 2014.PubMed/NCBI View Article : Google Scholar
|
|
43
|
van Wijck Y, de Kleijn S, John-Schuster G,
Mertens TCJ, Hiemstra PS, Müller A, Smits HH and Taube C:
Therapeutic application of an extract of Helicobacter pylori
ameliorates the development of allergic airway disease. J Immunol.
200:1570–1579. 2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Lim JH, Kim N, Lim SH, Kwon JW, Shin CM,
Chang YS, Kim JS, Jung HC and Cho SH: Inverse relationship between
Helicobacter pylori infection and asthma among adults
younger than 40 years: A cross-sectional study. Medicine
(Baltimore). 95(e2609)2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
van Wijck Y, John-Schuster G, van
Schadewijk A, van den Oever RL, Obieglo K, Hiemstra PS, Müller A,
Smits HH and Taube C: Extract of Helicobacter pylori
ameliorates parameters of airway inflammation and goblet cell
hyperplasia following repeated allergen exposure. Int Arch Allergy
Immunol. 180:1–9. 2019.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Lee SP, Lee SY, Kim JH, Sung IK, Park HS,
Shim CS and Moon HW: Correlation between Helicobacter pylori
Infection, IgE hypersensitivity, and allergic disease in korean
adults. Helicobacter. 20:49–55. 2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Amberbir A, Medhin G, Abegaz WE, Hanlon C,
Robinson K, Fogarty A, Britton J, Venn A and Davey G: Exposure to
Helicobacter pylori infection in early childhood and the
risk of allergic disease and atopic sensitization: A longitudinal
birth cohort study. Clin Exp Allergy. 44:563–571. 2014.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Leppold C, Tanimoto T, Ozaki A, Morita T
and Sari PV: Helicobacter pylori Vaccination. Lancet.
387:748–749. 2016.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Liu H, Liu W, Tan Z, Zeng Z, Yang H, Luo
S, Wang L, Xi T and Xing Y: Promoting immune efficacy of the oral
Helicobacter pylori Vaccine by HP55/PBCA nanoparticles
against the gastrointestinal environment. Mol Pharm. 15:3177–3186.
2018.PubMed/NCBI View Article : Google Scholar
|