Introduction
Sarcopenia is defined as a decrease in muscle
strength and physical function and skeletal muscle mass depletion
(1,2). Primary sarcopenia is caused by aging;
secondary sarcopenia is caused by malnutrition, sedentary behavior,
and various clinical conditions, such as inflammatory disease,
endocrine disease, and liver disease (3,4). The
prevalence of sarcopenia in patients with chronic liver disease
(CLD) is ranged from 10 to 70% in Japan (4,5).
Recent studies have revealed that sarcopenia exacerbates survival,
quality of life, and outcome after liver transplant in patients
with liver cirrhosis (LC) (6-12).
Since hepatocytes perform the function of glucose, lipid, and
protein metabolism, liver dysfunction causes a glycogen storage
dysfunction in the liver that facilitates the utilization of
glycogen and branched amino acid from skeletal muscle, resulting in
the progression of proteolysis (13,14).
Therefore, preventive treatment is needed to reduce the onset and
progression of sarcopenia due to skeletal muscle depletion in
patients with CLD.
Levocarnitine (L-carnitine) is an essential nutrient
that plays a pivotal role in fatty acid metabolism (15). L-carnitine is involved in
β-oxidation of fatty acids. It is a conditionally synthesized
nutrient from amino acids methionine and lysine in the brain,
liver, and kidney. Carnitine is obtained mainly from food; however,
one-fourth of carnitine is synthesized in the kidney and liver
(14,16). In other words, L-carnitine
deficiency occurs more frequently in patients with LC or CLD.
Several reports about L-carnitine administration in patients with
LC revealed that it improved muscle cramps, suppressed hepatic
encephalopathy, and improved hyperammonemia (17,18).
Furthermore, L-carnitine administration may improve sarcopenia in
patients with LC (14,19). However, enough evidence has not been
obtained in previous studies. Thus, this study aimed to clarify the
effect of L-carnitine administration on body composition [skeletal
muscle mass and bone mineral density (BMD)] in patients with
CLD.
Materials and methods
Study design and patients
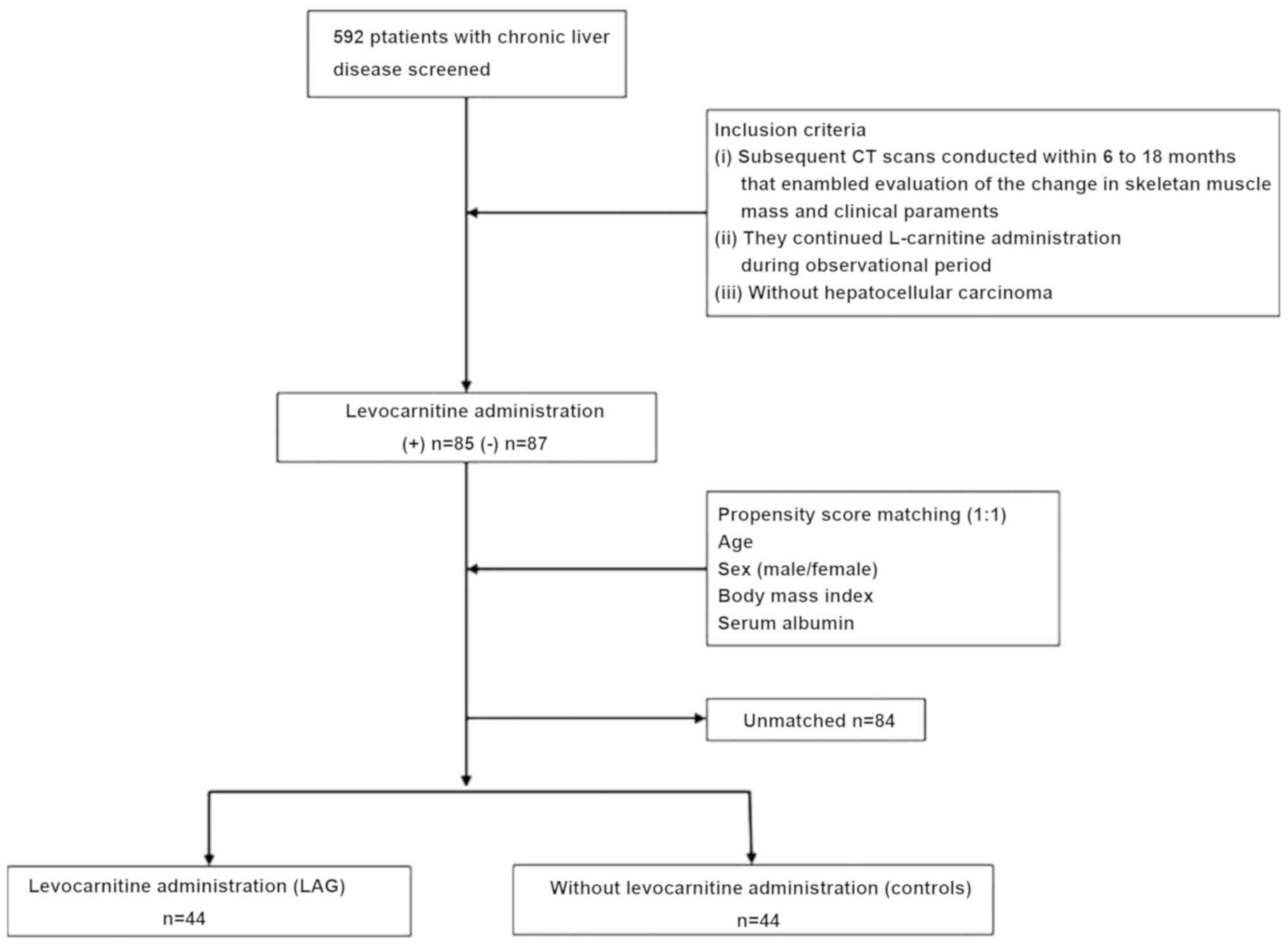
In this retrospective study, we reviewed 592
patients with CLD between 2015 and 2018 at Saiseikai Niigata
Hospital. Of those patients, 85 were treated with L-carnitine
(Otsuka Pharmaceutical, Tokyo, Japan) and underwent computed
tomography (CT) twice during L-carnitine administration. The
interval of CT scans was within 6-18 months. These 85 patients met
the following inclusion criteria: i) Subsequent CT scans were
conducted within 6-18 months that enabled evaluation of the change
in skeletal muscle mass and clinical parameters and BMD by dual
energy X-ray; and ii) they continued L-carnitine administration
during the observational period. Patients with hepatocellular
carcinoma (HCC) were excluded (Fig.
1). In this study, the L-carnitine dose ranged from 1,500 to
3,000 mg/day, and the dose was selected by the attending physician.
The reasons for L-carnitine administration were hepatic
encephalopathy, muscle cramps, hyperammonemia, hypoalbuminemia, or
combination of these conditions. We evaluated the effects of
L-carnitine on body composition in patients with CLD. Moreover, 87
patients with CLD who did not receive L-carnitine and underwent
paired CT scans to screen for HCC within 6-18 months were enrolled
as controls. Cases (patients who received L-carnitine) and controls
were matched for age, sex, body mass index (BMI), and serum
albumin, using propensity score matching.
Evaluation for skeletal muscle mass
and intramuscular adipose tissue content (IMAC)
Skeletal muscle mass was evaluated using the
skeletal muscle mass index (SMI) on CT scans. The SMI was
calculated as follows: The sum of the cross-sectional area of
skeletal muscles at the level of the third lumbar vertebra (L3) was
measured by a radiological technologist using a region of interest
(ROI) precisely traced with the use of commercially available image
analysis software (volume analyzer SYNAPSE VINCENT, Fujifilm
Medical Co., Ltd.), and this value was divided by height squared
(cm2/m2) (4).
To evaluate the yearly change in SMI, ΔSMI/year (%) was calculated
as follows: ΔSMI/year (%) = [(SMI on the second CT-SMI on the
initial CT)/SMI on the initial CT x100/interval between CT
(day)/365] (19). CT was typically
conducted in patients with CLD every 6-12 months according to the
guidelines of the Japan Society of Hepatology (20).
Muscle quality was examined as IMAC at the L3 level.
As previously described, IMAC was calculated by dividing the CT
attenuation value of the multifidus muscles by that of the
subcutaneous fat (21). To evaluate
the yearly change in IMAC, ΔIMAC/year was calculated as follows:
ΔIMAC/year = [IMAC on the second CT-IMAC on the initial
CT]/[interval between CT (day)/365].
Evaluation of BMD
All patients underwent scanning of the total lumbar
spine (L2-L4) BMD (LSBMD), and whole body BMD (WBBMD) by dual
energy X-ray absorptiometry (DEXA) at each CT. To evaluate the
yearly change in both BMD, ΔBMD/year (%) was calculated as follows:
ΔBMD/year (%) = [(BMD on the second DEXA-BMD on the initial
DEXA)/BMD on the initial DEXA x100/interval between DEXA
(day)/365].
Clinical and laboratory
assessment
Patients underwent blood tests and CT on the same
day. Clinical data were collected for the etiology of liver
disease, BMI, and blood test results (white blood cells, platelet
counts (Plt), serum albumin, aspartate aminotransferase (AST),
alanine aminotransferase (ALT), cholinesterase, and hemoglobin
A1c). The albumin-bilirubin (ALBI) score in each participant was
calculated by the following formula as reported previously: ALBI
score = [log10 total bilirubin (µmol/l) x 0.66] + [serum albumin
(g/l) x -0.085], while ALBI grade was classified into the
following: ALBI score ≤-2.60, grade 1; -2.60 <ALBI score ≤-1.39,
grade 2; and ALBI score >-1.39, grade 3 (22,23).
The fibrosis-4 index (FIB-4) in each participant was calculated by
the following formula as reported previously: FIB-4 = age (years) x
AST (IU/l) ÷ [platelets (109) x ALT (IU/l)] (24-26).
Statistical analysis
Continuous variables are presented as median and
interquartile range (IQR) and analyzed using the Mann-Whitney U
test. Categorical variables and nominal variables are presented as
frequency (percentage) and analyzed using Fisher's exact test. We
applied 1:1 propensity score matching to balance the assignment of
patients with L-carnitine administration. The variables were age,
sex, BMI, and serum albumin. Variables that affect sarcopenia were
selected. Clinical features of CLD patients with sarcopenia were
elderly, low BMI, and low albumin, and SMI depended on sex
(27). Values of P<0.05 were
considered statistically significant. All statistical analyses were
performed using EZR ver. 1.37 (Saitama Medical Center, Jichi
Medical University, Saitama, Japan) (28).
Results
Patient characteristics and body
composition at baseline and endpoint
We enrolled 85 patients with L-carnitine
administration and 87 control patients in this study and divided
these patients into two groups, namely, patients with L-carnitine
administration (LAG, n=44) and patients without L-carnitine
administration (controls, n=44), by using propensity score matching
for age, sex, BMI, and serum albumin. The overall characteristics
(32 men and 56 women) are shown in Table I. The median age was 69 years (IQR,
64.0, 75.0). The median SMI was 37.4 cm2/m2
(IQR, 34.01, 44.34). The etiology of CLD was hepatitis B virus
infection (n=10), hepatitis C virus infection (n=35), alcoholism
(n=8), nonalcoholic steatohepatitis and nonalcoholic fatty liver
disease (n=23), primary biliary cholangitis (n=5), autoimmune
hepatitis (n=5), and others (n=2). No significant difference in
variables were found between the LAG and controls at baseline as
well as at the endpoint (Table
II).
 | Table IComparison of clinical and
biochemical characteristics between the LAG and controls at
baseline. |
Table I
Comparison of clinical and
biochemical characteristics between the LAG and controls at
baseline.
| Factor | All patients
(IQR) | LAG (IQR) | Controls (IQR) | P-value |
|---|
| Number of
patients | 88 | 44 | 44 | |
| Age (years) | 69.00 (64.00,
75.00) | 70.50 (65.00,
75.25) | 68.00 (64.00,
75.00) | 0.523 |
| Sex | | | | 0.829 |
|
Male | 36 | 19 | 17 | |
|
Female | 52 | 25 | 27 | |
| Body mass index
(kg/m2) | 23.12 (20.71,
25.14) | 23.39 (19.96,
25.99) | 22.48 (21.43,
24.98) | 0.507 |
| Skeletal muscle
mass index (cm2/m2) | 37.40 (34.01,
44.34) | 37.74 (34.17,
43.58) | 37.16 (33.83,
44.34) | 0.67 |
| Intramuscular
adipose tissue content | -0.20 (-0.30,
-0.08) | -0.22 (-0.32,
-0.10) | -0.19 (-0.27,
-0.07) | 0.309 |
| Visceral fat area
(cm2) | 99.00 (61.79,
137.82) | 90.47 (53.98,
125.77) | 109.06 (77.08,
137.82) | 0.313 |
| Whole body bone
mineral density (g/cm2) | 0.94 (0.86,
1.04) | 0.94 (0.86,
1.04) | 0.95 (0.87,
1.02) | 0.914 |
| Lumber spine bone
mineral density (g/cm2) | 0.87 (0.75,
1.07) | 0.87 (0.74,
1.05) | 0.87 (0.78,
1.09) | 0.599 |
| Etiology | | | | 0.906 |
|
HBV | 10 | 4 | 6 | |
|
HCV | 35 | 17 | 18 | |
|
Alcohol | 8 | 4 | 4 | |
|
NASH and
NAFLD | 23 | 12 | 11 | |
|
PBC | 5 | 4 | 1 | |
|
AIH | 5 | 2 | 3 | |
|
Other | 2 | 1 | 1 | |
| ALBI score | -2.89 (-3.05,
-2.70) | -2.88 (-3.05,
-2.73) | -2.90 (-3.03,
-2.68) | 0.877 |
| ALBI grade
(1/2/3) | | | | 0.757 |
|
1 | 76 | 37 | 39 | |
|
2 | 12 | 7 | 5 | |
|
3 | 0 | 0 | 0 | |
| FIB-4 index | 2.30 (1.66,
3.14) | 2.62 (1.82,
3.51) | 2.23 (1.58,
2.74) | 0.123 |
| White blood cells
(x102/µl) | 55.00 (46.00,
62.25) | 55.50 (49.75,
63.50) | 53.50 (44.75,
61.00) | 0.251 |
| Platelet counts
(x104) | 18.65 (7.10,
43.40) | 17.95 (15.28,
21.38) | 20.00 (15.00,
23.38) | 0.307 |
| Albumin (g/dl) | 4.10 (3.98,
4.32) | 4.15 (4.00,
4.30) | 4.10 (3.90,
4.40) | 0.943 |
| Aspartate
aminotransferase (U/l) | 25.00 (21.00,
30.00) | 25.00 (21.00,
31.50) | 24.50 (19.00,
30.00) | 0.435 |
| Alanine
aminotransferase (U/l) | 17.00 (12.00,
25.00) | 17.00 (12.00,
23.50) | 17.00 (11.00,
25.00) | 0.947 |
| Cholinesterase
(U/l) | 297.00 (247.75,
340.00) | 282.00 (237.75,
332.25) | 297.50 (266.50,
353.25) | 0.346 |
| Triglyceride
(mg/dl) | 101.00 (73.00,
124.75) | 107.50 (71.75,
143.75) | 93.00 (73.25,
113.00) | 0.335 |
| γ-GTP (IU/l) | 17.50 (13.00,
32.75) | 18.00 (13.00,
35.50) | 17.00 (1300,
30.50) | 0.904 |
| Total cholesterol
(mg/dl) | 186.00 (161.25,
212.00) | 184.00 (161.75,
212.25) | 186.50 (161.00,
210.00) | 0.893 |
| Hemoglobin A1c
(%) | 5.80 (5.50,
6.20) | 5.80 (5.45,
6.20) | 5.80 (5.53,
6.10) | 0.711 |
| Observational
period (year) | 0.98 (0.85,
1.10) | 0.92 (0.74,
1.02) | 0.99 (0.90,
1.23) | 0.007 |
| Table IIComparison of clinical and
biochemical characteristics between the LAG and controls at
endpoint. |
Table II
Comparison of clinical and
biochemical characteristics between the LAG and controls at
endpoint.
| Factor | All patients
(IQR) | LAG (IQR) | Controls (IQR) | P-value |
|---|
| Number of
patients | 88 | 44 | 44 | |
| Skeletal muscle
mass index (cm2/m2) | 37.99 (32.98,
44.08) | 39.58 (34.63,
44.46) | 36.15 (32.43,
43.49) | 0.166 |
| Intramuscular
adipose tissue content | -0.20 (-0.30,
-0.07) | -0.22 (-0.33,
-0.08) | -0.19 (-0.26,
-0.08) | 0.367 |
| Visceral fat area
(cm2) | 102.48 (62.22,
137.26) | 92.38 (58.48,
147.07) | 114.33 (66.44,
135.65) | 0.404 |
| All bone mineral
density (g/cm2) | 0.93 (0.85,
1.03) | 0.93 (0.86,
1.04) | 0.93 (0.85,
1.02) | 0.764 |
| LS bone mineral
density (g/cm2) | 0.87 (0.76,
1.08) | 0.86 (0.74,
1.05) | 0.87 (0.78,
1.09) | 0.384 |
| ALBI score | -2.89 (-3.07,
-2.73) | -2.83 (-3.05,
-2.69) | -2.94 (-3.09,
-2.77) | 0.206 |
| ALBI grade | | | | 0.352 |
|
1 | 76 | 36 | 40 | |
|
2 | 12 | 8 | 4 | |
|
3 | 0 | 0 | 0 | |
| FIB-4 index | 2.20 (1.66,
2.88) | 2.50 (1.88,
2.95) | 2.12 (1.45,
2.73) | 0.115 |
| White blood cells
(x102/µl) | 58.00 (44.00,
70.25) | 57.00 (42.75,
68.00) | 59.00 (44.75,
70.50) | 0.907 |
| Platelet counts
(x104) | 19.65 (16.17,
23.30) | 19.10 (15.35,
21.77) | 20.20 (17.38,
25.72) | 0.139 |
| Albumin (g/dl) | 4.20 (4.00,
4.40) | 4.10 (3.90,
4.32) | 4.25 (4.00,
4.40) | 0.242 |
| Aspartate
aminotransferase (U/l) | 24.00 (20.75,
29.25) | 24.50 (21.00,
29.25) | 23.50 (19.75,
28.00) | 0.256 |
| Alanine
aminotransferase (U/l) | 16.00 (12.00,
22.25) | 17.00 (13.00,
23.25) | 15.00 (10.75,
21.25) | 0.171 |
| Cholinesterase
(U/l) | 288.50 (250.50,
350.25) | 282.00 (221.75,
332.50) | 293.00 (254.75,
351.25) | 0.138 |
| Triglyceride
(mg/dl) | 94.00 (72.00,
123.75) | 106.00 (72.00,
126.00) | 92.00 (71.75,
121.75) | 0.349 |
| γ-GTP (IU/l) | 16.00 (12.00,
32.00) | 16.50 (12.75,
29.00) | 16.00 (12.00,
32.25) | 0.691 |
| Total cholesterol
(mg/dl) | 180.00 (161.25,
206.75) | 179.00 (162.75,
203.25) | 181.00 (160.25,
212.00) | 0.99 |
| Hemoglobin A1c
(%) | 5.80 (5.50,
6.25) | 5.80 (5.50,
6.30) | 5.80 (5.70,
6.10) | 0.971 |
Comparison of change in SMI and body
composition between the LAG and controls
The initial CT showed similar median values of SMI
for the two groups [37.74 (34.17, 43.58) and 37.16 (33.83, 44.34),
P=0.67]. However, the median ΔSMI/year for the LAG and controls
were 0.95% (-3.07, 6.10) and -2.34% (-5.34, 0.53), respectively
(P<0.01) (Fig. 2A). The median
ΔIMAC/year for the LAG and controls were -0.00 (-0.03, 0.03) and
0.01 (-0.02, 0.04), respectively (P=0.46) (Fig. 2B). The median ΔWBBMD/year for the
LAG and controls were -0.24% (-1.20, 0.91) and -1.04% (-2.16,
0.47), respectively (P=0.04) (Fig.
2C). The median ΔLSBMD/year for the LAG and controls were
-0.67% (-2.87, 1.80) and -0.18% (-1.99, 2.99), respectively
(P=0.18) (Fig. 2D).
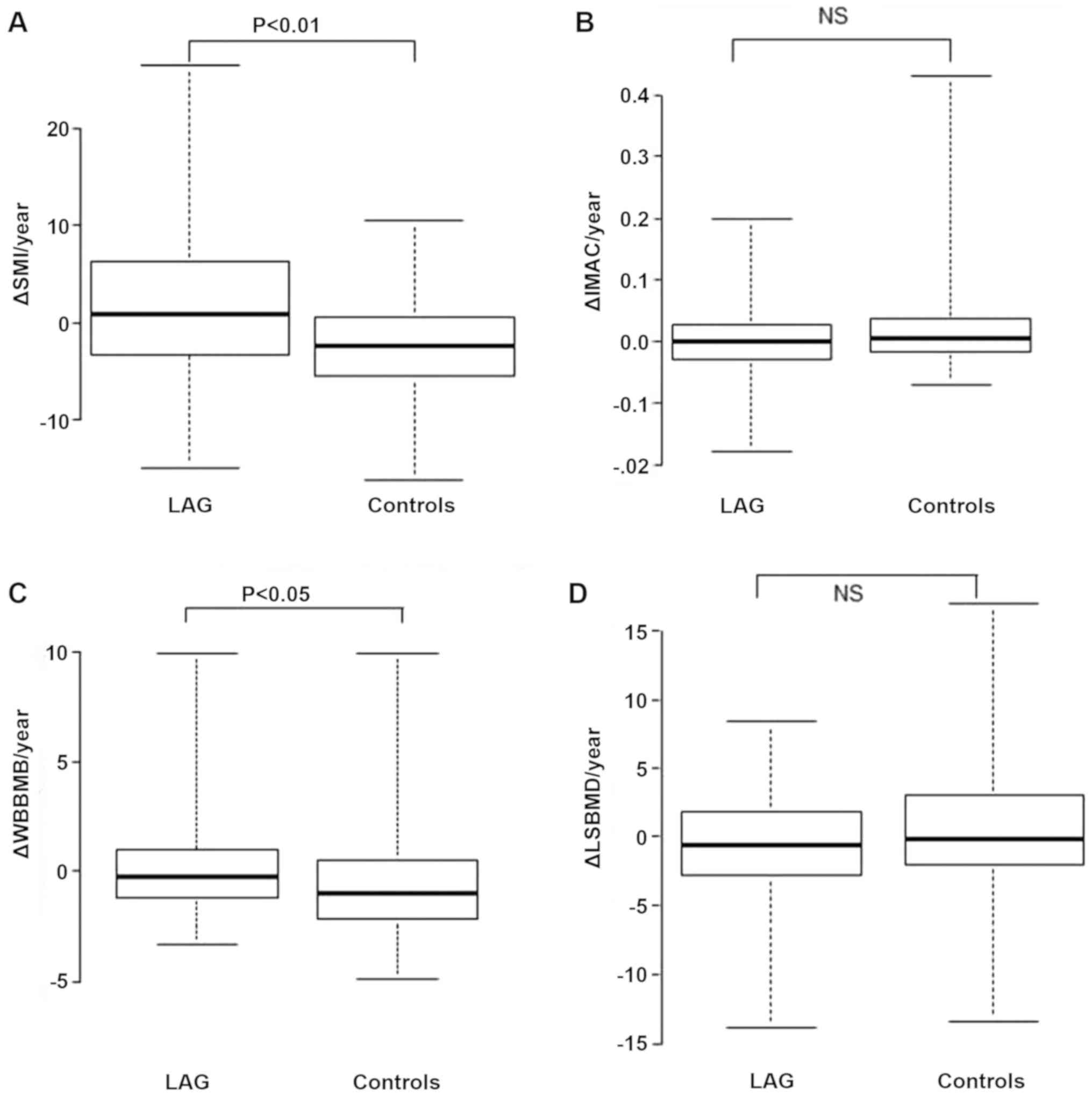 | Figure 2Comparison of ΔSMI/year, ΔIMAC/year,
ΔWBBMD/year, and ΔLSBMD in the LAG and controls. (A) Comparison of
ΔSMI/year in the LAG and controls. (B) Comparison of ΔIMAC/year in
the LAG and controls. (C) Comparison of ΔWBBMD/year in the LAG and
controls. (D) Comparison of ΔLSBMD in the LAG and controls. Data
were analyzed with the Mann-Whitney U test. Values of P<0.05
were considered statistically significant. LAG, levocarnitine
administration group; IMAC, intramuscular adipose tissue content;
NS, not significant; SMI, skeletal muscle mass index; IMAC,
intramuscular adipose tissue content; WBBMD, whole body bone
mineral density; LSBMD, lumbar spine bone mineral density. |
Discussion
Our results revealed that L-carnitine administration
prevents skeletal muscle mass loss and osteoporosis. To our
knowledge, this study is the first to report that L-carnitine may
improve both sarcopenia and osteoporosis. Thus, the results of this
study are of clinical significance for patients with CLD who have
sarcopenia and osteoporosis.
The median ΔSMI/year in our results was 0.69% for
all patients, 0.95% for the LAG and -2.34% for the controls.
Especially, the median ΔSMI/year of the LAG was significantly
better than that of the controls. According to previous studies,
ΔSMI/year or Δ skeletal muscle area/year of patients with LC ranged
from -2.2 to -0.22% (19,29). Our results show that skeletal muscle
loss is suppressed compared with the results of these reports. In
Japan, L-carnitine has been administered as a treatment for hepatic
encephalopathy, hypoalbuminemia, and muscle cramps in patients with
LC (17,18). Our study includes patients with CLD
who take L-carnitine for various purposes. However, the skeletal
muscle mass of the LAG was significantly increased, suggesting that
L-carnitine may prevent skeletal muscle mass loss.
There are multiple hypotheses that carnitine
administration suppresses skeletal muscle loss in patients with LC.
Carnitine plays a central role in transporting long-chain fatty
acids from the cytosol to the mitochondrial matrix. Carnitine binds
to the long-chain acyl coenzyme A and is converted to
acylcarnitine. Acylcarnitine is transported to the mitochondria and
degraded by β-oxidation (14,30).
Thus, carnitine administration improves energy metabolism disorders
in the mitochondria in the liver (31). Improvement of these energy
metabolism disorders is considered to suppress hyperammonemia in
patients with LC (32). This is
because the urea cycle, particularly localized in the liver, is a
metabolic system that requires a lot of energy. Hyperammonemia
activates myostatin and decreases muscle protein synthesis
(33). Therefore, preventing
hyperammonemia prevents skeletal muscle loss. Hiramatsu et
al (19) reported that
L-carnitine administration may suppress the progression of
sarcopenia in conjunction with the improvement of hyperammonemia.
The required dose of carnitine expected to inhibit the progression
of sarcopenia is ≥1,274 mg/day (19), and the carnitine dose administered
in this study (1,500-3,000 mg/day) exceeded that. However, since
this is a retrospective study, serum ammonia was not measured in
many cases. Prospective studies are needed to clarify the
relationship between formed ammonia levels and skeletal muscle
mass.
To date, carnitine administration has been suggested
to increase lipid utilization in the skeletal muscle during low
exercise and improve exercise performance (34). We considered that carnitine not only
increased skeletal muscle mass but also improved the quality and
examined changes in IMAC, the quality indicator of skeletal muscle
(21), but did not yield
significant results in our study. Studies reported that fatty
infiltration of the muscle (myosteatosis) exacerbates hepatic
encephalopathy in LC (35) and is a
prognostic factor for liver transplant patients (21,36).
Therefore, there is a need for treatments that improve not only
skeletal muscle mass but also muscle quality. However, since the
exercise and activity levels are not managed in this study, the
effect of carnitine on IMAC may be unclear. In the future, a
combination of carnitine and exercise may improve skeletal muscle
quality.
Furthermore, our study suggested that carnitine
administration may prevent BMD loss. The prevalence of osteoporosis
in patients with LC cirrhosis is ~12-55%, which is higher than in
healthy individuals (37). Along
with sarcopenia, it is one of the issues that have a major
influence on the health of patients with CLD. One of the mechanisms
of osteoporosis in patients with CLD has been shown to activate
osteoclasts by inflammatory cytokines (38). Because carnitine suppresses the
production of inflammatory cytokines (39), it may have prevented the decrease in
ΔWBBMD in our study. However, ΔLSBMD showed no significant effect.
Further research is needed to treat osteoporosis in patients with
CLD.
This study had several limitations. First, this was
a retrospective single-center study with a small sample size.
Moreover, the observation period was different for each patient.
Second, the purpose and dose of L-carnitine administration were
decided by the attending physician. Thus, prospective studies are
warranted to clarify the effects of L-carnitine on preventing
skeletal muscle loss in patients with liver disease.
In conclusion, we showed that L-carnitine
administration prevented the loss of skeletal muscle mass and BMD
in patients with CLD. L-carnitine administration can be a new
option for treating osteoporosis and sarcopenia. Further detailed
studies are needed to confirm this possibility.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed in this study are
included in this published article.
Authors' contributions
KO and TI designed the research; TI and TY conducted
the research; AH, TH evaluated SMI, IMAC and BMD. MS collected the
medication data. HN, HH, FK, MK, SH, and KS collected the clinical
and laboratory assessment data; KO, TI, and YM analyzed the data;
KO summarized the data; KO and TI wrote the manuscript. All authors
have read, checked, and approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki. Ethical approval was obtained from the
ethics committees of Saiseikai Niigata Hospital (approval no.
E17-27). Informed consent was obtained by the opt-out method on the
website.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cruz-Jentoft AJ, Landi F, Schneider SM,
Zúñiga C, Arai H, Boirie Y, Chen LK, Fielding RA, Martin FC, Michel
JP, et al: Prevalence of and interventions for sarcopenia in ageing
adults: A systematic review Report of the International Sarcopenia
Initiative (EWGSOP and IWGS). Age Ageing. 43:748–759.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chen LK, Liu LK, Woo J, Assantachai P,
Auyeung TW, Bahyah KS, Chou MY, Chou LY, Hsu PS, Krairit O, et al:
Sarcopenia in Asia: Consensus report of the Asian working group for
sarcopenia. J Am Med Dir Assoc. 15:95–101. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cruz-Jentoft AJ, Baeyens JP, Bauer JM,
Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y,
Schneider SM, et al: Sarcopenia: European consensus on definition
and diagnosis: Report of the European working group on Sarcopenia
in older people. Age Ageing. 39:412–423. 2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Nishikawa H, Shiraki M, Hiramatsu A,
Moriya K, Hino K and Nishiguchi S: Japan Society of Hepatology
guidelines for sarcopenia in liver disease (1st edition):
Recommendation from the working group for creation of sarcopenia
assessment criteria. Hepatol Res. 46:951–963. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ohashi K, Ishikawa T, Hoshi A, Suzuki M,
Mitobe Y, Yamada E, Abeywickrama HM, Seki N, Koyama C, Aoki H and
Koyama Y: Relationship between sarcopenia and both physical
activity and lifestyle in patients with chronic liver disease. J
Clin Med Res. 10:920–927. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hanai T, Shiraki M, Nishimura K, Ohnishi
S, Imai K, Suetsugu A, Takai K, Shimizu M and Moriwaki H:
Sarcopenia impairs prognosis of patients with liver cirrhosis.
Nutrition. 31:193–199. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Iritani S, Imai K, Takai K, Hanai T, Ideta
T, Miyazaki T, Suetsugu A, Shiraki M and Moriwaki H: Skeletal
muscle depletion is an independent prognostic factor for
hepatocellular carcinoma. J Gastroenterol. 50:323–332.
2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kim G, Kang SH, Kim MY and Baik SK:
Prognostic value of sarcopenia in patients with liver cirrhosis: A
systematic review and meta-analysis. PLoS One.
12(e0186990)2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hamaguchi Y, Kaido T, Okumura S, Kobayashi
A, Hammad A, Tamai Y, Inagaki N and Uemoto S: Proposal for new
diagnostic criteria for low skeletal muscle mass based on computed
tomography imaging in Asian adults. Nutrition. 32:1200–1205.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kaido T, Ogawa K, Fujimoto Y, Ogura Y,
Hata K, Ito T, Tomiyama K, Yagi S, Mori A and Uemoto S: Impact of
sarcopenia on survival in patients undergoing living donor liver
transplantation. Am J Transplant. 13:1549–1556. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fujiwara N, Nakagawa H, Kudo Y, Tateishi
R, Taguri M, Watadani T, Nakagomi R, Kondo M, Nakatsuka T, Minami
T, et al: Sarcopenia, intramuscular fat deposition, and visceral
adiposity independently predict the outcomes of hepatocellular
carcinoma. J Hepatol. 63:131–140. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ohashi K, Ishikawa T, Imai M, Suzuki M,
Hoshii A, Abe H, Koyama F, Nakano T, Ueki A, Noguchi H, et al:
Relationship between pre-sarcopenia and quality of life in patients
with chronic liver disease: A cross-sectional study. Eur J
Gastroenterol Hepatol. 31:1408–1413. 2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Moriwaki H, Miwa Y, Tajika M, Kato M,
Fukushima H and Shiraki M: Branched-chain amino acids as a protein-
and energy-source in liver cirrhosis. Biochem Biophys Res Commun.
313:405–409. 2004.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ohara M, Ogawa K, Suda G, Kimura M,
Maehara O, Shimazaki T, Suzuki K, Nakamura A, Umemura M, Izumi T,
et al: L-carnitine suppresses loss of skeletal muscle mass in
patients with liver cirrhosis. Hepatol Commun. 2:906–918.
2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Pekala J, Patkowska-Sokoła B, Bodkowski R,
Jamroz D, Nowakowski P, Lochyński S and Librowski T:
L-carnitine-metabolic functions and meaning in humans life. Curr
Drug Metab. 12:667–678. 2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kendler BS: Carnitine: An overview of its
role in preventive medicine. Prev Med (Baltim). 15:373–390.
1986.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Nakanishi H, Kurosaki M, Tsuchiya K,
Nakakuki N, Takada H, Matsuda S, Gondo K, Asano Y, Hattori N,
Tamaki N, et al: L-carnitine reduces muscle cramps in patients with
cirrhosis. Clin Gastroenterol Hepatol. 13:1540–1543.
2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Shiraki M, Shimizu M, Moriwaki H, Okita K
and Koike K: Carnitine dynamics and their effects on hyperammonemia
in cirrhotic Japanese patients. Hepatol Res. 47:321–327.
2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hiramatsu A, Aikata H, Uchikawa S, Ohya K,
Kodama K, Nishida Y, Daijo K, Osawa M, Teraoka Y, Honda F, et al:
Levocarnitine use is associated with improvement in sarcopenia in
patients with liver cirrhosis. Hepatol Commun. 3:348–355.
2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Clinical practice guidelines for
hepatocellular carcinoma differ between Japan, United States, and
Europe. Liver Cancer 4: 85-95, 2015.
|
|
21
|
Hamaguchi Y, Kaido T, Okumura S, Fujimoto
Y, Ogawa K, Mori A, Hammad A, Tamai Y, Inagaki N and Uemoto S:
Impact of quality as well as quantity of skeletal muscle on
outcomes after liver transplantation. Liver Transpl. 20:1413–1419.
2014.PubMed/NCBI View
Article : Google Scholar
|
|
22
|
Johnson PJ, Berhane S, Kagebayashi C,
Satomura S, Teng M, Reeves HL, O'Beirne J, Fox R, Skowronska A,
Palmer D, et al: Assessment of liver function in patients with
hepatocellular carcinoma: A new evidence-based approach-the ALBI
grade. J Clin Oncol. 33:550–558. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hiraoka A, Kumada T, Kudo M, Hirooka M,
Tsuji K, Itobayashi E, Kariyama K, Ishikawa T, Tajiri K, Ochi H, et
al: Albumin-Bilirubin (ALBI) grade as part of the evidence-based
clinical practice guideline for HCC of the Japan Society of
Hepatology: A comparison with the liver damage and child-pugh
classifications. Liver Cancer. 6:204–215. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Vallet-Pichard A, Mallet V, Nalpas B,
Verkarre V, Nalpas A, Dhalluin-Venier V, Fontaine H and Pol S:
FIB-4: An inexpensive and accurate marker of fibrosis in HCV
infection. Comparison with liver biopsy and fibrotest. Hepatology.
46:32–36. 2007.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Sumida Y, Yoneda M, Hyogo H, Itoh Y, Ono
M, Fujii H, Eguchi Y, Suzuki Y, Aoki N, Kaneyama K, et al:
Validation of the FIB4 index in a Japanese nonalcoholic fatty liver
disease population. BMC Gastroenterol. 12(2)2012.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Sterling RK, Lissen E, Clumeck N, Sola R,
Correa MC, Montaner J, Sulkowski MS, Torriani FJ, Dieterich DT,
Thomas DL, et al: Development of a simple noninvasive index to
predict significant fibrosis in patients with HIV/HCV coinfection.
Hepatology. 43:1317–1325. 2006.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Nishikawa H, Enomoto H, Yoh K, Iwata Y,
Sakai Y, Kishino K, Ikeda N, Takashima T, Aizawa N, Takata R, et
al: Association between sarcopenia and depression in patients with
chronic liver diseases. J Clin Med. 8(634)2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Hanai T, Shiraki M, Ohnishi S, Miyazaki T,
Ideta T, Kochi T, Imai K, Suetsugu A, Takai K, Moriwaki H and
Shimizu M: Rapid skeletal muscle wasting predicts worse survival in
patients with liver cirrhosis. Hepatol Res. 46:743–751.
2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Flanagan JL, Simmons PA, Vehige J, Willcox
MD and Garrett Q: Role of carnitine in disease. Nutr Metab (Lond).
7(30)2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sakai Y, Nishikawa H, Enomoto H, Yoh K,
Iwata Y, Hasegawa K, Nakano C, Kishino K, Shimono Y, Takata R, et
al: Effect of L-carnitine in patients with liver cirrhosis on
energy metabolism using indirect calorimetry: A pilot study. J Clin
Med Res. 8:863–869. 2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Malaguarnera M, Pistone G, Elvira R,
Leotta C, Scarpello L and Liborio R: Effects of L-carnitine in
patients with hepatic encephalopathy. World J Gastroenterol.
11:7197–7202. 2005.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Qiu J, Thapaliya S, Runkana A, Yang Y,
Tsien C, Mohan ML, Narayanan A, Eghtesad B, Mozdzak PE, McDobald C,
et al: Hyperammonemia in cirrhosis induces transcriptional
regulation of myostatin by an NF-κB-mediated mechanism. Proc Natl
Acad Sci USA. 110:18162–18167. 2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sawicka AK, Hartmane D, Lipinska P,
Wojtowicz E, Lysiak-Szydlowska W and Olek RA: L-carnitine
supplementation in older women. A pilot study on aging skeletal
muscle mass and function. Nutrients. 10(255)2018.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Bhanji RA, Moctezuma-Velazquez C,
Duarte-Rojo A, Ebadi M, Ghosh S, Rose C and Montano-Loza AJ:
Myosteatosis and sarcopenia are associated with hepatic
encephalopathy in patients with cirrhosis. Hepatol Int. 12:377–386.
2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hamaguchi Y, Kaido T, Okumura S, Kobayashi
A, Shirai H, Yao S, Yagi S, Kamo N, Okajima H and Uemoto S:
Proposal for new selection criteria considering pre-transplant
muscularity and visceral adiposity in living donor liver
transplantation. J Cachexia Sarcopenia Muscle. 9:246–254.
2018.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Patel N and Muñoz SJ: Bone disease in
cirrhosis. Clin Liver Dis (Hoboken). 6:96–99. 2015.PubMed/NCBI View
Article : Google Scholar
|
|
38
|
Tilg H, Moschen AR, Kaser A, Pines A and
Dotan I: Gut, inflammation and osteoporosis: Basic and clinical
concepts. Gut. 57:684–694. 2008.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Shakeri A, Tabibi H and Hedayati M:
Effects of L-carnitine supplement on serum inflammatory cytokines,
C-reactive protein, lipoprotein (a), and oxidative stress in
hemodialysis patients with Lp (a) hyperlipoproteinemia. Hemodial
Int. 14:498–504. 2010.PubMed/NCBI View Article : Google Scholar
|