From December 29, 2019, when cluster cases of
pneumonia with unknown etiology (PUE) were first reported in Wuhan,
the capital of Hubei, China, the disease spread rapidly across the
city (1). On January 3, 2019,
researchers at the National Institute for Viral Disease Control and
Prevention (Beijing, China) combined the use of Sanger sequencing,
Illumina sequencing and nanopore sequencing on bronchoalveolar
lavage (BAL) fluid samples from a patient with PUE from Wuhan to
analyze the pathogen genome (2). A
new β genus coronavirus was identified for the first time and named
2019 novel coronavirus (2019-nCoV) (3). On February 11, 2020, the international
committee on taxonomy of viruses designated this novel discovery as
a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
(4). On the same day, the World
Health Organization (WHO) coined the name ‘COVID-19,’ meaning
coronavirus disease 2019(5). The
present review highlights the epidemiology, etiology, pathobiology,
clinical manifestations and treatment of COVID-19.
The initial four cases of PUE, with clinical
manifestations resembling viral pneumonia, were reported via the
domestic PUE surveillance system (6) on December 29, 2020, in Wuhan, Hubei,
China (1). At the end of December
2019, the number of reported cases escalated to ~27(7). In late December 2019, several patient
BAL samples were sent to sequencing companies for next-generation
sequencing (NGS) analysis and the results suggested a type of
coronavirus. On December 31, 2019, the China National Health
Commission (NHC) sent a team of experts to Wuhan to perform the
epidemiological investigation (8).
The complete genome sequence of the novel coronavirus was
determined by researchers from the Wuhan Institute of Virology,
Chinese Academy of Sciences, China (3). On January 5, 2020, the virus was
isolated, and further phylogenetic analysis of the sequencing data
confirmed the novel coronavirus is a new β genus coronavirus
(2,8). The first reported mortality from the
virus occurred on January 9, 2020(7). On January 11, 2020, a 69-year-old
brain surgery patient who had no respiratory symptoms prior to
surgery developed symptoms of fever and was confirmed to have novel
coronavirus pneumonia (NCP) (9). He
subsequently infected one doctor and 13 nurses in Wuhan Union
hospital, which was the first direct evidence of human-to-human
transmission. On the same day, Professor Zhang Yongzhen's team from
Fudan University in Shanghai first shared the sequence of the new
coronavirus genome on the Virological (https://virological.org) and GenBank (https://www.ncbi.nlm.nih.gov) websites. As the
reported number of cases from other provinces besides Hubei
continued to rise, on January 23, 2020, Wuhan city was locked down
by the local government to prevent the disease from spreading. At
the end of January 2020, 11,821 patients were confirmed to be
infected with COVID-19 worldwide, and there were 3,215 cases in
Wuhan (10). The government
renovated and built 86 designated hospitals and 16 mobile cabin
hospitals and provided more than 60,000 beds to effectively
facilitate the admission and treatment of several confirmed
patients as soon as possible in Wuhan (11). In addition, the government focused
research on detection reagents, and several nucleic acid detection
reagents, such as the BGI Group 2019-nCOV Nucleic Acid Detection
Kit, were approved for clinical application, which improved the
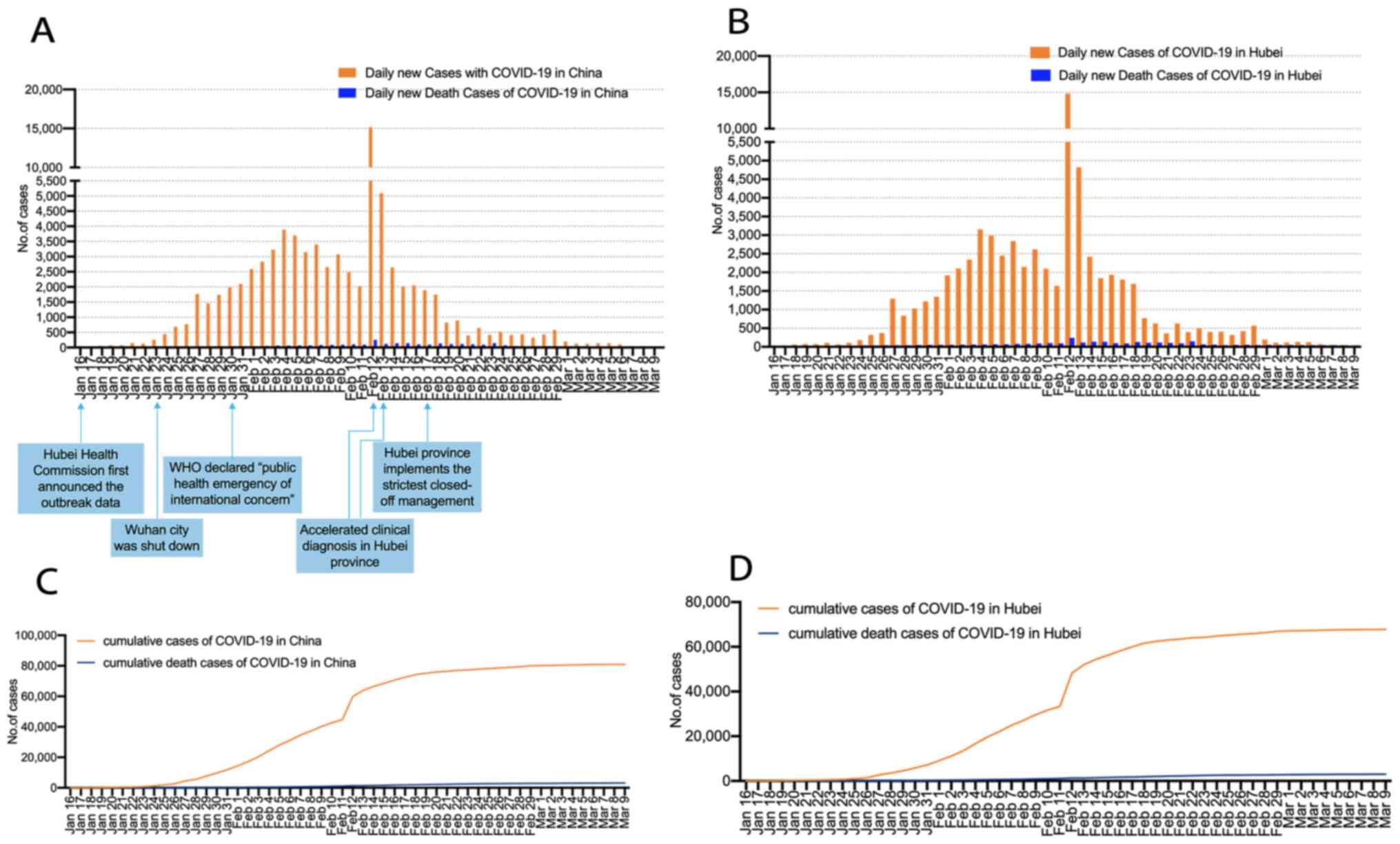
screening of suspected cases. Since strict joint prevention and
control measures were taken by the government, the outbreak of the
disease was rapidly restrained. The chronological incidence of
confirmed COVID-19 cases and COVID-19-associated mortalities are
presented in Fig. 1A-D. As of March
9, 2020, 80,924 cases have been confirmed in mainland China, with
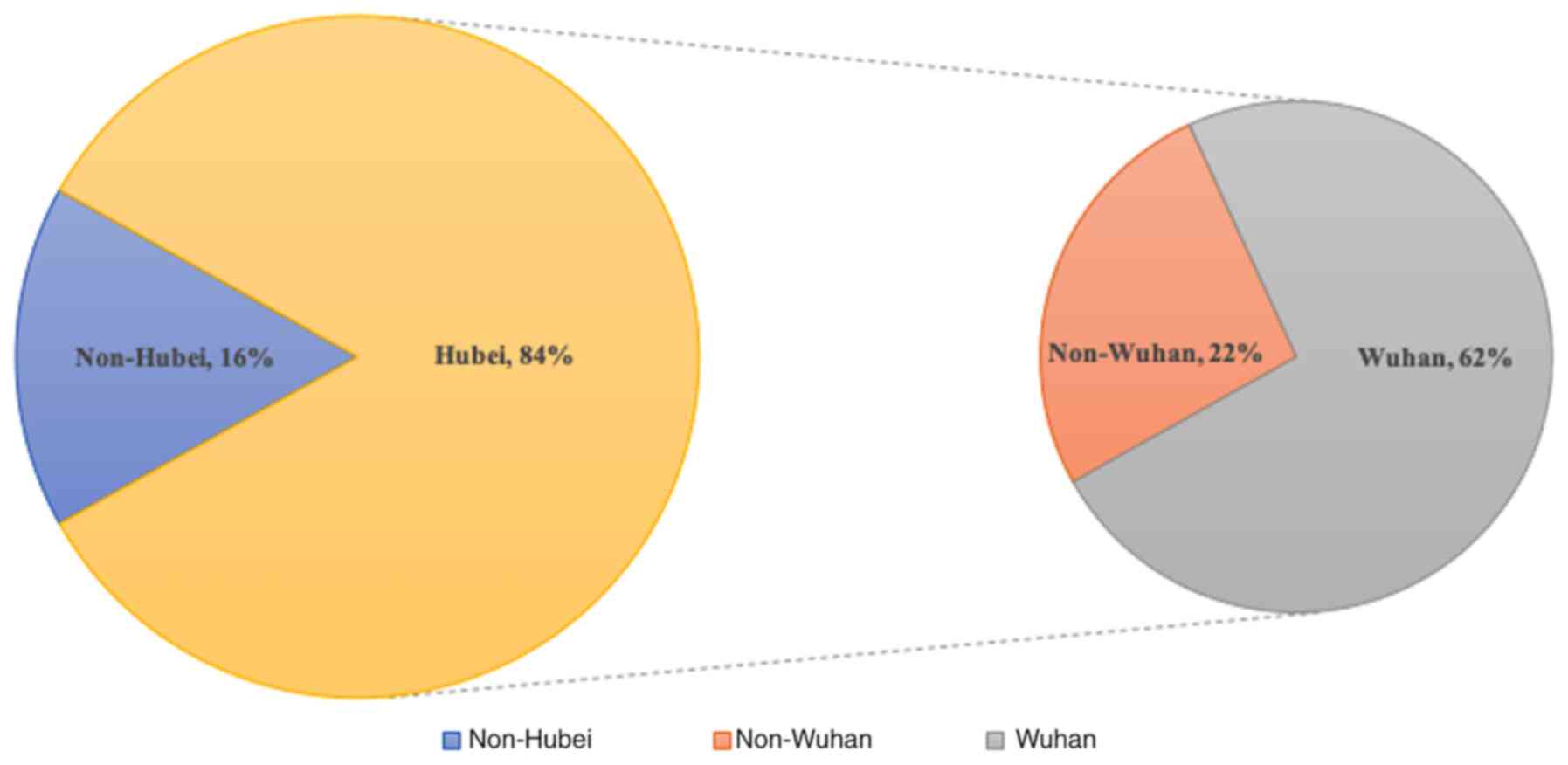
3,140 mortalities (10). A total of
84% of cases were in Hubei and Wuhan was the worst-hit area in
Hubei (Fig. 2). The case fatality
rate is 3.88% (3,140/80,924) worldwide, with 4.46% (3,024/67,760)
in Hubei and 4.81% (2,404/49,965) in Wuhan (10).
Early virus sequencing analysis of BAL samples from
five patients demonstrated that the genomes among these isolates
were almost identical, with 99.8-99.9% sequence identity (12). In another study, virus sequencing
was performed on BAL and pharyngeal swab samples from nine
patients, with 99.98% nucleotide identity (1). Further phylogenetic analysis of the
virus indicated that it belonged to the β genus coronavirus
(3). Its genome sequence was
dissimilar to the middle east respiratory syndrome coronavirus
(MERS-CoV), (51.8% identity) and SARS-CoV (79% identity) and was
closely associated with the bat SARS-like coronavirus RaTG13 (96.2%
identity) obtained from Rhinolophus affinis (3). Despite significant differences in
genome sequences, the SARS-CoV-2 spike (S)-protein and SARS-CoV
S-protein share an almost identical 3D structure in the receptor
binding domain (RBD), suggesting that they have the same
S-protein-angiotensin-converting enzyme 2 (ACE2) binding pathway
(13). In addition, in vitro
experiments have demonstrated that SARS-CoV-2 infects permissive
cells via ACE2 on the cell membrane (3,14-17).
The mechanism of transfer of the virus from its
natural hosts to other animals and humans remains unclear. With
regards to the search for reservoir hosts, a study proposed that a
species of snake may serve as the SARS-CoV-2 reservoir, based on
sequence analysis and relative synonymous codon usage bias
(18). An additional study
suggested that pangolins were the probable animal source of
SARS-CoV-2(19). Although reservoir
hosts are yet to be determined, these findings suggest the
importance of harmonious coexistence between humans and wildlife.
Recently, viral mutations during the epidemic have attracted
interest. A study analyzed 103 SARS-CoV-2 genomes and demonstrated
that these viruses evolved into two major types (L type and S type)
(20). The S type is an ancestral
and less aggressive type, which is less prevalent in Wuhan (Wuhan
vs. the rest of the world, 3.7% vs. 38.4%) (20). Conversely, the L type has evolved
from the S type, has a higher transmission rate compared with the S
type and is highly prevalent in Wuhan (Wuhan vs. the rest of the
world, 96.3 vs. 61.6%) (20).
Analysis suggests that government intervention may have prevented
the L type from spreading outwards (20). However, based on existing knowledge
of coronaviruses, this new RNA virus may still mutate and recombine
in the future, during which the virulence may be enhanced or
weakened.
The major immune characteristics in patients with
severe COVID-19 are as follows:
IL-6, secreted by monocytes, macrophages and
dendritic cells (DCs) has been reported to be a key driver of
inflammatory cytokine storms in patients with SARS-CoV or MERS-CoV
(24,25). Elevated IL-6 serum levels have also
been exhibited in patients with COVID-19 and are associated with
acute respiratory distress syndrome (ARDS), respiratory failure and
adverse clinical outcomes, including death (26). IL-6 has notable proinflammatory
characteristics. It acts on lymphocytes via cis signaling to
promote T helper 17 cell (Th17) and T follicular helper cell (Tfh)
differentiation, enhances CD8+T cytotoxic activity, and
promotes B-cell differentiation and proliferation (26). IL-6 also acts on vascular
endothelial cells via trans signaling to induce vascular
endothelial growth factor (VEGF) expression and decrease E-cadherin
expression on endothelial cells, resulting in increased vascular
permeability and leakage (26). It
also induces monocyte chemoattractant protein-1 (MCP-1) and IL-8
expression, to recruit monocytes and neutrophils into diseased
tissues (26).
Granulocyte-macrophage colony-stimulating factor (GM-CSF) is
another important cytokine in COVID-19 (27-29).
CD4+T lymphocytes activated by SARS-COV-2 become
pathogenic T helper (Th) 1 cells and serve as a source of GM-CSF
(27). GM-CSF activates mature
myeloid cells to a proinflammatory phenotype, with enhanced
cytokine and chemokine secretory capacity (28). Thus, GM-CSF is considered a primary
communication conduit between inflammatory lymphocytes and myeloid
cells (28). Patients with COVID-19
have been reported to have increased plasma concentrations of
GM-CSF and increased percentages of GM-CSF-expressing leukocytes
(29). Based on this, blocking the
IL-6 or GM-CSF pathway is expected to decrease the severity of the
cytokine storm in the lungs.
Unlike the immune process of other respiratory viral
infections, SARS-CoV-2 infection elicits delayed and lowered IFN-I
and IFN-III responses, while inducing elevated chemokine expression
(30,31). This delayed IFN secretion is not
conducive to early disease control, and instead induces more
chemokines and promotes systemic inflammation and lung injury
(23). This suggests that different
timing of IFN administration may lead to completely different
clinical effects.
On February 17, 2020, Dr Xu's team were the first to
publish the lung pathology of biopsy specimens obtained from an
elderly patient who had died of NCP (35). Subsequently, lung pathology from two
patients with NCP who underwent lobectomy for lung tumors was also
reported (36), which represented
early lung pathology. The first lung autopsy pathology of a patient
who had died of severe NCP was reported on February 27,
2020(37). Combined with the
pathological description in the COVID-19 guidelines in China
(38), the pathological changes can
be summarized as follows:
On gross examination, the lungs exhibited diffuse
congestion and hemorrhage, accompanied by partial hemorrhagic
necrosis (37). On the cut surface,
the bronchi were covered with mucus (38). Hemorrhage and necrosis were most
common at the margin zone of the lungs (37).
Histopathological findings included pulmonary
interstitial fibrosis, focal pulmonary hemorrhage and hemorrhagic
infarction (37). Serous or
fibromyxoid exudates and hyaline membranes were observed in the
alveolar cavity, and the exudated cells were predominantly
monocytes and macrophages (38-40).
Prominent hyperplasia of type II pneumocytes was observed, and some
type II pneumocytes desquamated (39,40).
Inclusion bodies were also observed in type II pneumocytes and
macrophages. Monocyte and lymphocyte infiltration were present in
the alveolar septa and the alveolar capillaries were congested,
accompanied by the formation of hyaline thrombus (38,39).
Inflammatory cell infiltrations, including lymphocytes, plasma
cells and monocytes, were exhibited in the pulmonary interstitium
(39). Some of the epithelial cells
in the bronchial mucosa were desquamated, and mucus plugs were
observed in the lumen (38). Some
alveoli were overinflated, and alveolar septa were ruptured or
accompanied by cystic cavity formation. Coronavirus particles were
seen in the cytoplasm of bronchial epithelial cells and type II
pneumocytes under electron microscopy (105x
magnification) (38,40). Immunohistochemical staining
demonstrated that some alveolar epithelium cells and macrophages
were positive for the novel coronavirus antigen (38,40).
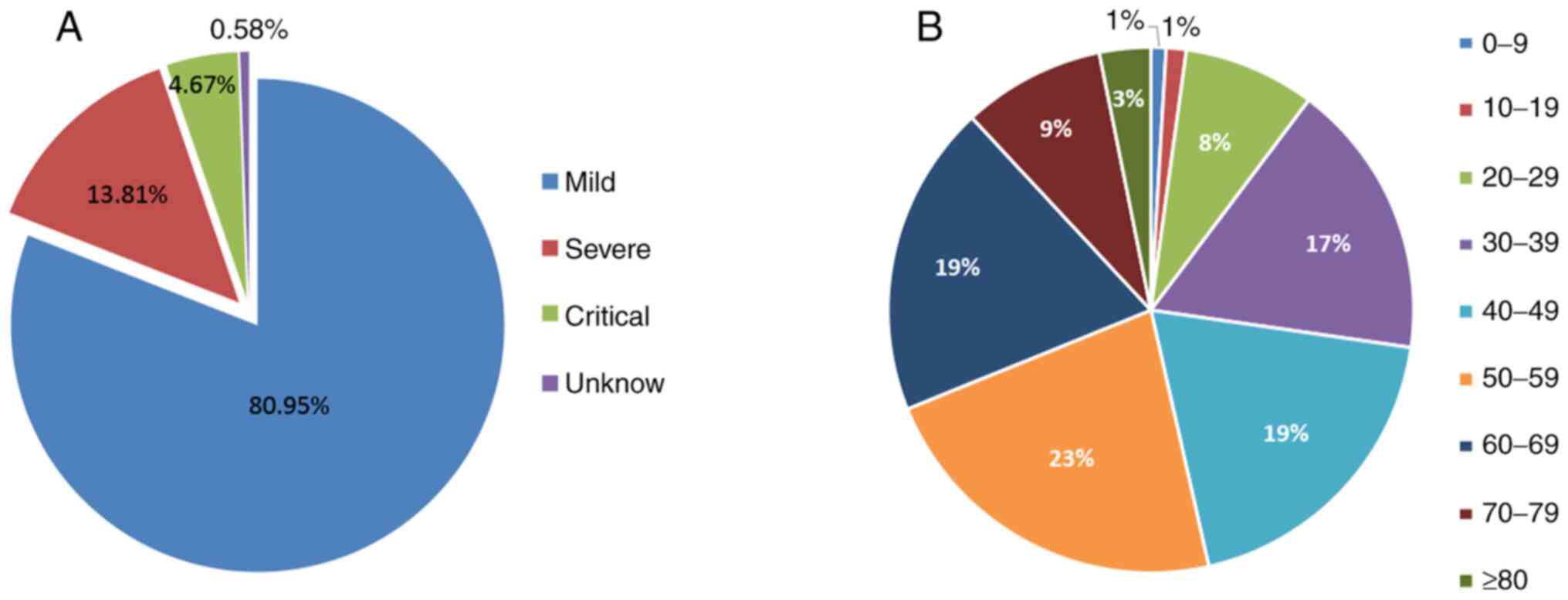
According to a statistical analysis of 44,672
confirmed patients in mainland China by the Chinese CDC
epidemiology team (43), 80.95% of
the patients had mild disease symptoms, 13.81% were severe cases
and 4.67% were critical (Fig. 3A).
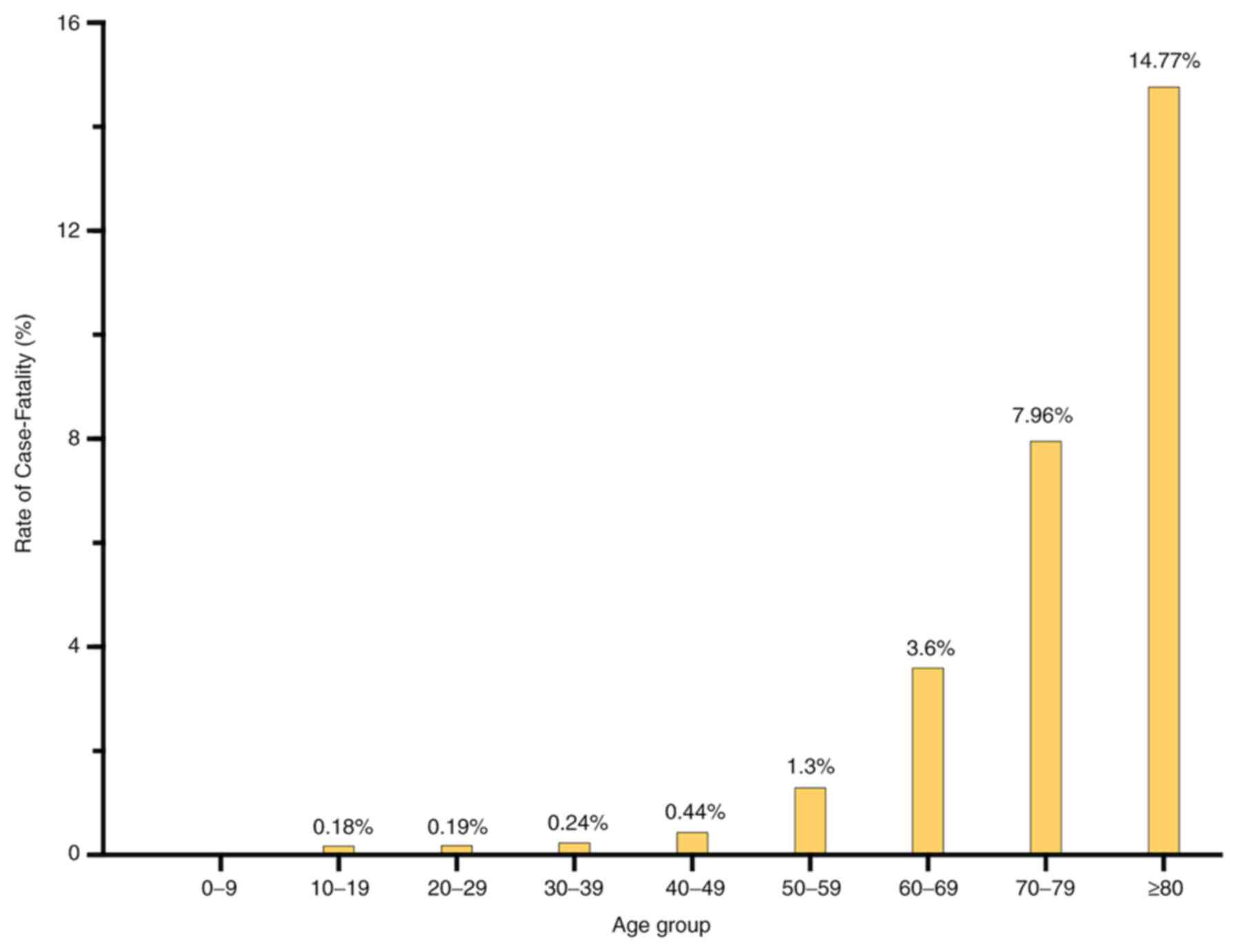
The age group with highest prevalence was 40-69 years (Fig. 3B). Statistical analysis demonstrated
that fatality rate increased with age (Fig. 4). In addition, the case fatality
rate was 0.9% in patients with no underlying disease, 6.0% in
patients with hypertension, 7.3% in patients with diabetes, 10.5%
in patients with other cardiovascular diseases, such as coronary
heart disease, 6.3% in patients with underlying respiratory
infections and 5.6% in patients with cancer (43). Analysis of this large sample data
indicated that the case fatality rate was closely associated with
patient age and whether there was any underlying disease.
According to the COVID-19 guidelines in China,
reverse-transcription polymerase chain reaction (RT-PCR) detection
and chest imaging examinations are considered the most important
methods for screening and diagnosing patients with NCP (38). Pathogen related tests include
qualitative detection of SARS-CoV-2 nucleic acids and screening of
serum antiviral antibodies. By March 16, 2020, the China National
Medical Products Administration had approved 11 SARS-CoV-2 nucleic
acid detection reagents and eight antibody detection reagents
(44). The methods used for PCR
detection of SARS-CoV-2 nucleic acids included nucleic acid
fluorescence PCR and nucleic acid sequencing (44). Currently, approved reagents detect
the novel gene segments of the coronavirus, including the open
reading frame 1ab (ORF1ab), envelope protein (E) and nucleocapsid
protein (N) coding region, and are classified as the single-target
detection (ORF1ab), double-target detection (ORF1ab, N protein) and
triple-target detection (ORF1ab, N protein and E protein). Viral
nucleic acids can be detected in nasopharyngeal swabs, sputum,
lower respiratory tract secretions, blood and feces via PCR or
sequencing analyses. Serum antibody screening can detect antiviral
antibodies IgM and IgG. The techniques used by these kits include
the immune colloidal gold technique, the magnetic particle-based
chemiluminescence enzyme immunoassay and the chemiluminescent
microparticle immunoassay (44).
The IgM antibodies against SARS-CoV-2 in serum usually appear
positive 3-5 days after the onset, which indicates a recent
infection, whereas IgG antibodies indicate convalescence or a past
infection (38).
The most common CT findings are ground-glass
opacification (GGO) and bilateral consolidative opacities (45). In the early stage of the disease,
the lung is characterized by single or multiple focal GGO and local
patchy shadows with a peripheral distribution (46). In the progressive stage, multiple
GGO, consolidative opacities, air bronchograms and interstitial
abnormalities are observed in both lungs (46). In severe and critical cases,
extensive consolidative opacities of both lungs are present
(46). Pleural and pericardial
effusion are less common. Although several cases of pulmonary
inflammatory lesions begin in peripheral areas, these CT findings
alone cannot easily distinguish them from other viral pneumonias
(47).
Effective antivirals and antiviral regimens are
important for combating COVID-19. IFN-α has been extensively used
in the treatment of viral infectious diseases (48). IFN, as an antiviral drug with an
exact curative effect, is limited to the treatment of hepatitis B
virus (HBV), hepatitis C virus (HCV), human herpes virus type 8
(HHV-8) and human papillomavirus infection (49). It is also used to treat other common
viral infectious diseases, including the common cold (50), influenza (50), and mumps (51); however, the curative effects have
not yet been proven in these diseases (50,52,53).
As early as the SARS epidemic, two studies reported the therapeutic
effect of IFN combined with glucocorticoids and/or ribavirin in
patients with SARS (54,55). However, a subsequent systematic
evaluation study revealed that there is no benefit from IIFN
treatment due to the complexity of clinical intervention measures
and lack of a suitable control group in the two studies (56). Although inhalation therapy with
IFN-α is recommended by the NHC guidelines (57), and several patients with COVID-19
underwent treatment with IFN-α during hospitalization in China, the
exact efficacy of interferon remains to be verified.
Lopinavir/ritonavir (LPV/r), an anti-HIV drug was
hypothesized to have effects on SARS and MERS (58), and was used in the treatment of
patients with COVID-19 (57,59).
However, a randomized, controlled, open label study from China
demonstrated that LPV/r treatment of patients with severe COVID-19
did not significantly change the clinical outcome, including the
mortality and oropharyngeal virus persistence time (60).
Remdesivir is a broad-spectrum antiviral that has
been reported to inhibit the replication of SARS-CoV and MERS-CoV
in vitro (8,61-64),
and has been successfully used to treat a US patient with NCP
(65). A report of 53 patients with
severe COVID-19 who were treated with compassionate-use remdesivir
demonstrated improvement in the oxygen-support status of 36
patients (68%) (66). However, the
results were limited by the lack of a control group and the small
sample size. In China, a double-blind, randomized,
placebo-controlled trial enrolling 237 patients with severe
COVID-19 demonstrated no clinical improvement in patients treated
with remdesivir (67). The trial
was originally scheduled to include 453 patients with COVID-19 but
failed to complete full enrollment due to the end of the outbreak
in China. Recently, another double-blind, randomized,
placebo-controlled study of remdesivir (Adaptive COVID-19 Treatment
Trial 1, ACTT-1) in 1,059 hospitalized patients with COVID-19
suggested that a 10-day course of remdesivir was superior compared
with placebo in shortening the time of recovery (median days, 11
vs. 15; P<0.001) (68). However,
given the high mortality in both groups, the report indicated that
monotherapy with an antiviral drug is not likely to be sufficient.
Thus, combined therapeutic approaches are urgently required to
further improve patient outcomes.
Favipiravir is a nucleoside analogue against the
RNA-dependent RNA polymerase of some viruses, including influenza A
and B (69). It has also been used
as post exposure prophylaxis and was evaluated in clinical trials
for Ebola virus (70-72).
An open-label control study from China assessed the efficacy and
safety of favipiravir on 80 patients with mild or moderate
COVID-19, whereby 35 patients were assigned to favipiravir and 45
were assigned to LPV/r. The results demonstrated that patients
treated with favipiravir had a shorter viral clearance time
(P<0.001) and better radiographic improvement (P<0.01)
compared with patients treated with LPV/r (73). Furthermore, a lower rate of adverse
events, such as nausea, was observed in the favipiravir group
(P<0.05). These preliminary clinical findings require further
research.
Chloroquine is an antimalarial drug.
Hydroxychloroquine is a superior analogue of chloroquine, which
possesses a more tolerable safety profile (74). Both exert anti-inflammatory effects
and are extensively used in the treatment of rheumatic diseases
(74). Previous in vitro
experiments have demonstrated that chloroquine inhibits the
replication of SARS-CoV by interfering with the binding of SARS-CoV
to the ACE2 receptor of the Vero E6 cell line (75). Recent in vitro studies
further supported the efficacy of chloroquine and
hydroxychloroquine in inhibiting MERS-CoV-2 (76-78).
Based on its antiviral effect in vitro and previous wide
clinical usage in patients with a safety track record, chloroquine
has been recommended for the treatment of patients with COVID-19 in
China (79). However, recent
clinical data seem to less promising for both chloroquine and
hydroxychloroquine in COVID-19(80). An open label, randomized controlled
trial from China (148 patients with mild to moderate COVID-19 and
two patients with severe COVID-19) demonstrated that the
probability of negative conversion of SARS-CoV-2 in the
hydroxychloroquine group was 85.4% by 28 days, which was similar to
81.3% in the standard treatment group (81). There was also no significant
difference between the two groups in the time to negative RT-PCR
test of SARS-CoV-2. A large observational study involving 1,376
patients with COVID-19, hospitalized in a medical center in New
York, also demonstrated that hydroxychloroquine administration did
not result in a significantly lowered or an increased risk of
intubation or mortality (82).
Another retrospective study analyzed the in-hospital mortality
among 1,438 hospitalized patients with COVID-19 in New York who
were treated with hydroxychloroquine, azithromycin, combined
hydroxychloroquine and azithromycin, or neither drug. The results
demonstrated that treatment with hydroxychloroquine, azithromycin,
or both, did not show a significant difference in in-hospital
mortality compared with neither treatment (83). In addition, hydroxychloroquine used
as post exposure prophylaxis for COVID-19 did not seem to offer
much hope either (84).
Mavrilimumab is a humanized monoclonal antibody
(mAb) (Ig4) targeting GM-CSF receptor α, which has demonstrated
efficacy and safety in phase I and phase II clinical trials in
rheumatoid arthritis (RA) (98).
GM-CSF is secreted by fibroblasts, macrophages, dendritic cells, T
cells, neutrophils, eosinophils and tumor cells (99). Analysis of serum cytokine levels in
41 patients with COVID-19 demonstrated that these patients had
higher GM-CSF levels compared with healthy controls (29). De Luca et al (99) recently performed a prospective study
on mavrilimumab in non-mechanically ventilated patients with
COVID-19 pneumonia and systemic hyperinflammation. The results
demonstrated that all 13 patients in the mavrilimumab treatment
group exhibited clinical improvement compared with 17/26 patients
(65%) in the control group, who received standard care (P=0.030),
and treatment of mavrilimumab was well tolerated.
Tocilizumab is a recombinant mAb against the IL-6
receptor (IL-6R) and has been approved for the treatment of RA and
giant cell arteritis (103). IL-6
is the main inducer of the acute phase response (104) and is classified as an important
infection-related marker (105-107).
Due to high levels of IL-6 observed in severely ill patients,
tocilizumab treatment in these patients may decrease lung damage
(27). In a recent report, 21
patients with severe or critical COVID-19 were treated with
tocilizumab and the clinical symptoms notably improved, with no
significant adverse events observed (108). However, the study's credibility
was limited by the lack of a control group. In China, tocilizumab
has been recommended for the treatment of severe COVID-19 pneumonia
with high IL-6 levels (38). As of
September 11, 2020, there are currently 38 clinical trials
involving tocilizumab for the treatment of COVID-19 registered at
clinicaltrials.gov. Sarilumab is another
humanized anti-IL-6R mAb approved for the treatment of RA (103). According to clinicaltrials.gov, eight clinical trials are underway
to assess the safety and efficacy of sarilumab in the treatment of
COVID-19.
Baricitinib, an approved drug for the treatment of
RA, is a reversible inhibitor of the intracellular signaling
molecule, JAK (109). Baricitinib
inhibits the production of multiple cytokines by suppressing the
JAK-signal transducer and activator of transcription (STAT)
signaling pathway, thus producing anti-inflammatory effects
(110). Another advantage of
baricitinib is its in vitro anti-coronavirus activity
(111-113),
which is mediated by suppressing endocytosis-associated enzymes
adaptor-associated kinase-1 (AAK1) and cyclin G-associated kinase
(GAK) (111). A recent open-label
pilot study demonstrated that baricitinib may significantly improve
clinical and laboratory parameters, including fever,
SPO2, Horowitz Index and CRP, in patients with moderate
COVID-19 pneumonia (114). The
ACTT-2 led by the US National Institute of Allergy and Infectious
Diseases is recruiting to assess the effectiveness and safety of
remdesivir and baricitinib in treating COVID-19(115). The trial is based on ACTT-1 to
determine whether JAK inhibitors can provide extra benefits to
patients, including decreasing mortality (116).
Convalescent plasma is collected from patients who
have recovered from COVID-19. In China, the time of blood donation
should be at least 3 weeks after the onset of COVID-19 symptoms.
Convalescent plasma contains virus-specific neutralizing
antibodies, which can directly bind the virus and eliminate it via
cellular cytotoxicity and phagocytosis (117). For those with coagulation
disorders, plasma transfusion can also replenish coagulation
factors (118). Thus, convalescent
plasma transfusion may be beneficial to patients with severe
COVID-19. Convalescent plasma has been used for treatment of viral
infectious diseases, such as SARS, H5N1 avian influenza, Ebola
hemorrhagic fever and MERS (119).
It has also been used in patients with severe COVID-19. Some
COVID-19 cases exhibited a clinical benefit, including improvement
in oxygenation, the sequential organ failure assessment (SOFA)
scores and other clinic status (120-123).
However, a recent open-label randomized clinical trial of 103
patients with severe COVID-19 given convalescent plasma did not
result in a significant improvement in time to clinical improvement
within 28 days compared with standard treatment alone (124). There are currently more than 70
ongoing registered clinical trials globally assessing the efficacy
of convalescence plasma in the treatment of COVID-19.
Given the persistence of the COVID-19 epidemic and
the inaccessibility of specific drugs, vaccine research is of great
significance for preventing further development and potential
future epidemic peaks. An optimal vaccine for SARS-CoV-2 would
elicit long-lasting antibody protective effects, an effective
T-cell response, simultaneously avoid generating antibody-dependent
enhancement (ADE) and a skewed Th2 immune response (125).
Currently, there are over 100 COVID-19 vaccines
under development worldwide. According to the design strategy,
these vaccines can be classified into four categories (126), as follows: i) virus vaccines; ii)
nucleic-acid vaccines; iii) viral-vector vaccines; and iv)
protein-based vaccines. The most common vaccines for SARS-COV-2 are
protein-based and adenovirus vectored vaccines, and most of these
vaccine trials are pre-clinical (126). The PiCoVacc and BBIBP-CorV
inactivated virus vaccine candidates have exhibited effective
protection against SARS-CoV-2 in animal experiments (127,128). Currently, there are eight
registered clinical phase I or II vaccine trials worldwide,
including Moderna's and BioNTech's mRNA COVID-19 vaccines, Inovio
Pharmaceuticals' DNA vaccine, three inactivated COVID-19 vaccines
manufactured by Sinovac (Wuhan and Beijing Institute of Biological
Products), University of Oxford's non-replicating chimpanzee
adenovirus vectored vaccine (also known as ChAdOx1 nCOV-19) and
CanSino's non-replicating adenovirus type 5 vectored vaccine
(Ad5-nCoV) (125,128). The phase I study of Ad5-nCoV has
been completed, and the results demonstrated that Ad5-nCoV has good
safety and can induce specific antibodies against the viral spike
proteins and specific T cell responses to SARS-CoV-2(128); however, it still requires
verification in phase II clinical trials.
Since the COVID-19 outbreak in Wuhan, the Chinese
government and Chinese people have made great efforts to control
the development and spread of the epidemic. These controls include:
Restricting and decreasing outdoor activities, home isolation,
banning gatherings, introducing population screening and education,
accelerating the admission and treatment of confirmed patients,
accelerating the supply of medical necessities, strengthening the
research and development of diagnostic reagents, and mobilizing all
citizens to participate in the prevention and control of the
epidemic.
Although the severity of the epidemic has greatly
decreased, a significant amount of work remains. Future endeavors
should aim to identify the origin of the coronavirus, clarify the
pathogenesis of COVID-19, hasten the research and development of
antiviral drugs and vaccines, and discuss how to establish a global
prevention and control system for emerging infectious diseases.
Not applicable.
The present study was partially supported by a
grant from the Sanming Project of Medicine in Shenzhen (grant no.
SZSM201612034).
All data generated or analyzed during the present
study are included in this published article.
HC drafted the initial manuscript. SW and XZ
revised the manuscript. All authors have read and approved the
final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Lu R, Zhao X, Li J, Niu P, Yang B, Wu H,
Wang W, Song H, Huang B, Zhu N, et al: Genomic characterisation and
epidemiology of 2019 novel coronavirus: Implications for virus
origins and receptor binding. Lancet. 395:565–574. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tan WJ, Zhao X, Ma XJ, Wang W, Niu P, Xu
W, Gao GF and Wu G: A novel coronavirus genome identified in a
cluster of pneumonia cases-Wuhan, China 2019-2020. China CDC
Weekly. 2:61–62. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhou P, Yang XL, Wang XG, Hu B, Zhang L,
Zhang W, Si HR, Zhu Y, Li B, Huang CL, et al: A pneumonia outbreak
associated with a new coronavirus of probable bat origin. Nature.
579:270–273. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Coronaviridae Study Group of the
International Committee on Taxonomy of Viruses. The species Severe
acute respiratory syndrome-related coronavirus: Classifying
2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 5:536–544.
2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
World Health Organization (WHO): Novel
coronavirus disease named COVID-19. WHO, Geneva, 2020. urihttps://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happensimplehttps://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen.
Accessed February 11, 2020.
|
|
6
|
Xiang N, Havers F, Chen T, Song Y, Tu W,
Li L, Cao Y, Liu B, Zhou L, Meng L, et al: Use of national
pneumonia surveillance to describe influenza A(H7N9) virus
epidemiology, China, 2004-2013. Emerg Infect Dis. 19:1784–1790.
2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
European Centre for Disease Prevention and
Control: Risk assessment: Outbreak of acute respiratory syndrome
associated with a novel coronavirus, Wuhan, China. urihttps://www.ecdc.europa.eu/sites/default/files/documents/Risk-assessment-pneumonia-Wuhan-China-22-Jan-2020.pdfsimplehttps://www.ecdc.europa.eu/sites/default/files/documents/Risk-assessment-pneumonia-Wuhan-China-22-Jan-2020.pdf.
Accessed January 22, 2020.
|
|
8
|
Zhu N, Zhang D, Wang W, Li X, Yang B, Song
J, Zhao X, Huang B, Shi W, Lu R, et al: A novel coronavirus from
patients with pneumonia in China, 2019. N Engl J Med. 382:727–733.
2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Cohen E: Super spreaders in coronavirus
outbreaks. CNN health, 2020. urihttps://edition.cnn.com/2020/01/23/health/wuhan-virus-super-spreader/index.htmlsimplehttps://edition.cnn.com/2020/01/23/health/wuhan-virus-super-spreader/index.html.
Accessed January 23, 2020.
|
|
10
|
China Centre for Disease Prevention and
Control: Distribution of COVID-19 outbreaks. urihttp://2019ncov.chinacdc.cn/2019-nCoVsimplehttp://2019ncov.chinacdc.cn/2019-nCoV.
|
|
11
|
Chutian Metropolis Daily: Central steering
group: Over 60,000 beds were completed in wuhan in one month,
equivalent to the construction of 60 tertiary hospitals. urihttp://news.cnhubei.com/content/2020-03/06/content_12823832.htmlsimplehttp://news.cnhubei.com/content/2020-03/06/content_12823832.html.
Accessed March 6, 2020.
|
|
12
|
Ren LL, Wang YM, Wu ZQ, Xiang ZC, Guo L,
Xu T, Jiang YZ, Xiong Y, Li YJ, Li XW, et al: Identification of a
novel coronavirus causing severe pneumonia in human: A descriptive
study. Chin Med J (Engl). 133:1015–1024. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Xu X, Chen P, Wang J, Feng J, Zhou H, Li
X, Zhong W and Hao P: Evolution of the novel coronavirus from the
ongoing Wuhan outbreak and modeling of its spike protein for risk
of human transmission. Sci China Life Sci. 63:457–460.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lan J, Ge J, Yu J, Shan S, Zhou H, Fan S,
Zhang Q, Shi X, Wang Q, Zhang L and Wang X: Structure of the
SARS-CoV-2 spike receptor-binding domain bound to the ACE2
receptor. Nature. 581:215–220. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shang J, Ye G, Shi K, Wan Y, Luo C, Aihara
H, Geng Q, Auerbach A and Li F: Structural basis of receptor
recognition by SARS-CoV-2. Nature. 581:221–224. 2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hoffmann M, Kleine-Weber H, Schroeder S,
Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH,
Nitsche A, et al: SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2
and is blocked by a clinically proven protease inhibitor. Cell.
181:271–280.e278. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wang Q, Zhang Y, Wu L, Niu S, Song C,
Zhang Z, Lu G, Qiao C, Hu Y, Yuen KY, et al: Structural and
functional basis of SARS-CoV-2 entry by using human ACE2. Cell.
181:894–904.e9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Ji W, Wang W, Zhao X, Zai J and Li X:
Cross-species transmission of the newly identified coronavirus
2019-nCoV. J Med Virol. 92:433–440. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
South China Agricultural University: Press
conference of scientific research on novel coronavirus pneumonia
outbreak. Guangzhou, 7 February, 2020.
|
|
20
|
Tang XL, Wu CC, Li X, Song YH, Yao XM, Wu
XK, Duan YG, Zhang H, Wng YR, Qian ZH, et al: On the origin and
continuing evolution of SARS-CoV-2. Natl Sci Rev. 7:1012–1023.
2020.
|
|
21
|
Khiali S, Khani E and Entezari-Maleki T: A
comprehensive review on tocilizumab in COVID-19 acute respiratory
distress syndrome. J Clin Pharmacol: June 18, 2020 (Epub ahead of
print).
|
|
22
|
Tay MZ, Poh CM, Rénia L, MacAry PA and Ng
LEP: The trinity of COVID-19: Immunity, inflammation and
intervention. Nat Rev Immunol. 20:363–374. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Vardhana S and Wolchok J: The many faces
of the anti-COVID immune response. J Exp Med.
217(e20200678)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Lew TW, Kwek TK, Tai D, Earnest A, Loo S,
Singh K, Kwan KM, Chan Y, Yim CF, Bek SL, et al: Acute respiratory
distress syndrome in critically Ill patients with severe acute
respiratory syndrome. JAMA. 290:374–380. 2003.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Drosten C, Seilmaier M, Corman VM,
Hartmann W, Scheible G, Sack S, Guggemos W, Kallies R, Muth D,
Junglen S, et al: Clinical features and virological analysis of a
case of Middle East respiratory syndrome coronavirus infection.
Lancet Infect Dis. 13:745–751. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Moore B and June C: Cytokine release
syndrome in severe COVID-19. Science. 368:473–474. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Zhou Y, Fu B, Zheng X, Wang D, Zhao C, Qi
Y, Sun R, Tian Z, Xu X and Wei H: Pathogenic T-cells and
inflammatory monocytes incite inflammatory storms in severe
COVID-19 patients. Natl Sci Rev. 7:998–1002. 2020.
|
|
28
|
Lang F, Lee K, Teijaro J, Becher B and
Hamilton J: GM-CSF-based treatments in COVID-19: Reconciling
opposing therapeutic approaches. Nat Rev Immunol. 20:507–514.
2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirus in Wuhan, China. Lancet.
395:497–506. 2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Blanco-Melo D, Nilsson-Payant B, Liu WC,
Uhl S, Hoagland D, Møller R, Jordan T, Oishi K, Panis M, Sachs D,
et al: Imbalanced host response to SARS-CoV-2 drives development of
COVID-19. Cell. 181:1036–1045.e9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Park A and Iwasaki A: Type I and Type III
interferons-induction, signaling, evasion, and application to
combat COVID-19. Cell Host Microbe. 27:870–878. 2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Guan W, Ni Z, Hu Y, Liang W, Ou C, He J,
Liu L, Shan H, Lei C, Hui DSC, et al: Clinical characteristics of
coronavirus disease 2019 in China. N Engl J Med. 382:1708–1720.
2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Cao X: COVID-19: Immunopathology and its
implications for therapy. Nat Rev Immunol. 20:269–270.
2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Chen X, Ling J, Mo P, Zhang Y, Jiang Q, Ma
Z, Cao Q, Hu W, Zou S, Chen L, et al: Restoration of leukomonocyte
counts is associated with viral clearance in COVID-19 hospitalized
patients. medRxiv: urihttps://doi.org/10.1101/2020.03.03.20030437simplehttps://doi.org/10.1101/2020.03.03.20030437.
|
|
35
|
Xu Z, Shi L, Wang Y, Zhang J, Huang L,
Zhang C, Liu S, Zhao P, Liu H, Zhu L, et al: Pathological findings
of COVID-19 associated with acute respiratory distress syndrome.
Lancet Respir Med. 8:420–422. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Tian S, Hu W, Niu L, Liu H, Xu H and Xiao
SY: Pulmonary pathology of early-phase 2019 novel coronavirus
(COVID-19) pneumonia in two patients with lung cancer. J Thorac
Oncol. 15:700–704. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Luo W, Yu H, Gou J, Li X, Sun Y, Li J and
Liu L: Clinical pathology of critical patient with novel
coronavirus pneumonia (COVID-19): Pulmonary fibrosis and vascular
changes including microthrombosis formation. Preprint: doi:
10.13140/RG.2.2.22934.29762.
|
|
38
|
General Office of National Health
Commission: Diagnosis and treatment of novel coronavirus pneumonia
(trial version seventh) (In Chinese). urihttp://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989/files/ce3e6945832a438eaae415350a8ce964.pdfsimplehttp://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989/files/ce3e6945832a438eaae415350a8ce964.pdf.
|
|
39
|
Carsana L, Sonzogni A, Nasr A, Rossi R,
Pellegrinelli A, Zerbi P, Rech R, Colombo R, Antinori S, Corbellino
M, et al: Pulmonary post-mortem findings in a series of COVID-19
cases from northern Italy: A two-centre descriptive study. Lancet
Infect Dis. 20:1135–1140. 2020.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Deshmukh V, Motwani D, Kumar A, Kumari C
and Raza K: Histopathological observations in COVID-19: A
systematic review. J Clin Pathol: Aug 18, 2020 (Epub ahead of
print).
|
|
41
|
Docherty A, Harrison E, Green C, Hardwick
H, Pius R, Norman L, Holden K, Read J, Dondelinger F, Carson G, et
al: Features of 20 133 UK patients in hospital with covid-19 using
the ISARIC WHO clinical characterisation protocol: Prospective
observational cohort study. BMJ. 369(m1985)2020.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Li L, Li R, Wu Z, Yang X, Zhao M, Liu J
and Chen D: Therapeutic strategies for critically ill patients with
COVID-19. Ann Intensive Care. 10(45)2020.PubMed/NCBI View Article : Google Scholar
|
|
43
|
The Novel Coronavirus Pneumonia Emergency
Response Epidemiology Team. The epidemiological characteristics of
an outbreak of 2019 novel coronavirus diseases (COVID-19)-China,
2020. China CDC Weekly. 2:113–122. 2020.PubMed/NCBI View Article : Google Scholar
|
|
44
|
China National Medical Products
Administration: Novel Coronavirus detection product is subject to
emergency approval by the China National Medical Products
Administration. urihttps://www.nmpa.gov.cn/zhuanti/yqyjzxd/yqyjxd/20200316153801928.htmlsimplehttps://www.nmpa.gov.cn/zhuanti/yqyjzxd/yqyjxd/20200316153801928.html.
Accessed March 16, 2020.
|
|
45
|
Shi H, Han X, Jiang N, Cao Y, Alwalid O,
Gu J, Fan Y and Zheng C: Radiological findings from 81 patients
with COVID-19 pneumonia in Wuhan, China: A descriptive study.
Lancet Infect Dis. 20:425–434. 2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Dong D, Tang Z, Wang S, Hui H, Gong L, Lu
Y, Xue Z, Liao H, Chen F, Yang F, et al: The role of imaging in the
detection and management of COVID-19: A review. IEEE Rev Biomed
Eng: Apr 27, 2020 (Epub ahead of print).
|
|
47
|
Dai W, Zhang H, Yu J, Xu H, Chen H, Luo S,
Zhang H, Liang L, Wu X, Lei Y, et al: CT imaging and differential
diagnosis of COVID-19. Can Assoc Radiol J. 71:195–200.
2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Wang N, Zhan Y, Zhu L, Hou Z, Liu F, Song
P, Qiu F, Wang X, Zou X, Wan D, et al: Retrospective multicenter
cohort study shows early interferon therapy is associated with
favorable clinical responses in COVID-19 patients. Cell Host
Microbe. 28:455–464.e2. 2020.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Balfour HH Jr: Antiviral drugs. N Engl J
Med. 340:1255–1268. 1999.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Bergman SJ, Ferguson MC and Santanello C:
Interferons as therapeutic agents for infectious diseases. Infect
Dis Clin North Am. 25:819–834. 2011.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Rüther U, Stilz S, Röhl E, Nunnensiek C,
Rassweiler J, Dörr U and Jipp P: Successful interferone-alpha 2 a
therapy for a patient with acute mumps orchitis. Eur Urol.
27:174–176. 1995.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Hayden FG, Kaiser DL and Albrecht JK:
Intranasal recombinant alfa-2b interferon treatment of naturally
occurring common colds. Antimicrob Agents Chemother. 32:224–230.
1988.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Grennan D: Mumps. JAMA.
322(1022)2019.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Loutfy MR, Blatt LM, Siminovitch KA, Ward
S, Wolff B, Lho H, Pham DH, Deif H, LaMere EA, Chang M, et al:
Interferon alfacon-1 plus corticosteroids in severe acute
respiratory syndromea preliminary study. JAMA. 290:3222–3228.
2003.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Zhao Z, Zhang F, Xu M, Huang K, Zhong W,
Cai W, Yin Z, Huang S, Deng Z, Wei M, et al: Description and
clinical treatment of an early outbreak of severe acute respiratory
syndrome (SARS) in Guangzhou, PR China. J Med Microbiol.
52:715–720. 2003.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Stockman LJ, Bellamy R and Garner P: SARS:
Systematic review of treatment effects. PLoS Med.
3(e343)2006.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Peng F, Tu L, Yang Y, Hu P, Wang R, Hu Q,
Cao F, Jiang T, Sun J, Xu G and Chang C: Management and treatment
of COVID-19: The Chinese experience. Can J Cardiol. 36:915–930.
2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Chen F, Chan KH, Jiang Y, Kao RY, Lu HT,
Fan KW, Cheng VC, Tsui WH, Hung IF, Lee TS, et al: In vitro
susceptibility of 10 clinical isolates of SARS coronavirus to
selected antiviral compounds. J Clin Virol. 31:69–75.
2004.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han
Y, Qiu Y, Wang J, Liu Y, Wei Y, et al: Epidemiological and clinical
characteristics of 99 cases of 2019 novel coronavirus pneumonia in
Wuhan, China: A descriptive study. Lancet. 395:507–513.
2020.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Cao B, Wang Y, Wen D, Liu W, Wang J, Fan
G, Ruan L, Song B, Cai Y, Wei M, et al: A Trial of
Lopinavir-Ritonavir in adults hospitalized with severe Covid-19. N
Engl J Med. 382:1787–1799. 2020.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Gordon CJ, Tchesnokov EP, Feng JY, Porter
DP and Götte M: The antiviral compound remdesivir potently inhibits
RNA-dependent RNA polymerase from Middle East respiratory syndrome
coronavirus. J Biol Chem. 295:4773–4779. 2020.PubMed/NCBI View Article : Google Scholar
|
|
62
|
de Wit E, Feldmann F, Cronin J, Jordan R,
Okumura A, Thomas T, Scott D, Cihlar T and Feldmann H: Prophylactic
and therapeutic remdesivir (GS-5734) treatment in the rhesus
macaque model of MERS-CoV infection. Proc Natl Acad Sci USA.
117:6771–6776. 2020.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Agostini M, Andres E, Sims A, Graham R,
Sheahan T, Lu X, Smith E, Case J, Feng J, Jordan R, et al:
Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is
mediated by the viral polymerase and the proofreading
exoribonuclease. mBio. 9:e00221–18. 2018.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Sheahan TP, Sims AC, Graham RL, Menachery
VD, Gralinski LE, Case JB, Leist SR, Pyrc K, Feng JY, Trantcheva I,
et al: Broad-spectrum antiviral GS-5734 inhibits both epidemic and
zoonotic coronaviruses. Sci Transl Med. 9(eaal3653)2017.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Holshue ML, DeBolt C, Lindquist S, Lofy
KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural
A, et al: First Case of 2019 Novel Coronavirus in the United
States. N Engl J Med. 382:929–936. 2020.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Grein J, Ohmagari N, Shin D, Diaz G,
Asperges E, Castagna A, Feldt T, Green G, Green ML, Lescure FX, et
al: Compassionate use of remdesivir for patients with severe
Covid-19. N Engl J Med. 382:2327–2336. 2020.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Wang Y, Zhang D, Du G, Du R, Zhao J, Jin
Y, Fu S, Gao L, Cheng Z, Lu Q, et al: Remdesivir in adults with
severe COVID-19: A randomised, double-blind, placebo-controlled,
multicentre trial. Lancet. 395:1569–1578. 2020.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Beigel JH, Tomashek KM and Dodd LE:
Remdesivir for the treatment of Covid-19-preliminary report. N Engl
J Med. 383(994)2020.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Coomes EA and Haghbayan H: Favipiravir, an
antiviral for COVID-19? J Antimicrob Chemother. 75:2013–2014.
2020.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Jacobs M, Aarons E, Bhagani S, Buchanan R,
Cropley I, Hopkins S, Lester R, Martin D, Marshall N, Mepham S, et
al: Post-exposure prophylaxis against Ebola virus disease with
experimental antiviral agents: A case-series of health-care
workers. Lancet Infect Dis. 15:1300–1304. 2015.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Bai CQ, Mu JS, Kargbo D, Song YB, Niu WK,
Nie WM, Kanu A, Liu WW, Wang YP, Dafae F, et al: Clinical and
virological characteristics of ebola virus disease patients treated
with favipiravir (T-705)-Sierra Leone, 2014. Clin Infect Dis.
63:1288–1294. 2016.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Sissoko D, Laouenan C, Folkesson E,
M'Lebing A-B, Beavogui A-H, Baize S, Camara A-M, Maes P, Shepherd
S, Danel C, et al: Experimental treatment with favipiravir for
ebola virus disease (the JIKI trial): A historically controlled,
single-arm proof-of-concept trial in Guinea. PLoS Med.
13(e1001967)2016.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Cai Q, Yang M, Liu D, Chen J, Shu D, Xia
J, Liao X, Gu Y, Cai Q, Yang Y, et al: Experimental treatment with
favipiravir for COVID-19: An open-label control study. Engineering
(Beijing): Mar 18, 2020. (Epub ahead of print).
|
|
74
|
Rainsford KD, Parke AL, Clifford-Rashotte
M and Kean WF: Therapy and pharmacological properties of
hydroxychloroquine and chloroquine in treatment of systemic lupus
erythematosus, rheumatoid arthritis and related diseases.
Inflammopharmacology. 23:231–269. 2015.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Keyaerts E, Vijgen L, Maes P, Neyts J and
Van Ranst M: In vitro inhibition of severe acute respiratory
syndrome coronavirus by chloroquine. Biochem Biophys Res Commun.
323:264–268. 2004.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Wang M, Cao R, Zhang L, Yang X, Liu J, Xu
M, Shi Z, Hu Z, Zhong W and Xiao G: Remdesivir and chloroquine
effectively inhibit the recently emerged novel coronavirus
(2019-nCoV) in vitro. Cell Res. 30:269–271. 2020.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Yao X, Ye F, Zhang M, Cui C, Huang B, Niu
P, Liu X, Zhao L, Dong E, Song C, et al: In vitro antiviral
activity and projection of optimized dosing design of
hydroxychloroquine for the treatment of severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 71:732–739.
2020.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Liu J, Cao R, Xu M, Wang X, Zhang H, Hu H,
Li Y, Hu Z, Zhong W and Wang M: Hydroxychloroquine, a less toxic
derivative of chloroquine, is effective in inhibiting SARS-CoV-2
infection in vitro. Cell Discovery. 6(16)2020.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Multicenter collaboration group of
Department of Science and Technology of Guangdong Province and
Health Commission of Guangdong Province for chloroquine in the
treatment of novel coronavirus pneumonia. Expert consensus on
chloroquine phosphate for the treatment of novel coronavirus
pneumonia. Zhonghua Jie He He Hu Xi Za Zhi. 43:185–188.
2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
80
|
Kupferschmidt K: Big studies dim hopes for
hydroxychloroquine. Science. 368:1166–1167. 2020.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Tang W, Cao Z, Han M, Wang Z, Chen J, Sun
W, Wu Y, Xiao W, Liu S, Chen E, et al: Hydroxychloroquine in
patients with mainly mild to moderate coronavirus disease 2019:
Open label, randomised controlled trial. BMJ.
369(m1849)2020.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Geleris J, Sun Y, Platt J, Zucker J,
Baldwin M, Hripcsak G, Labella A, Manson DK, Kubin C, Barr RG, et
al: Observational study of hydroxychloroquine in hospitalized
patients with Covid-19. N Engl J Med. 382:2411–2418.
2020.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Rosenberg ES, Dufort EM, Udo T,
Wilberschied LA, Kumar J, Tesoriero J, Weinberg P, Kirkwood J, Muse
A, DeHovitz J, et al: Association of treatment with
hydroxychloroquine or azithromycin with in-hospital mortality in
patients with COVID-19 in New York state. JAMA. 323:2493–2502.
2020.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Boulware DR, Pullen MF, Bangdiwala AS,
Pastick KA, Lofgren SM, Okafor EC, Skipper CP, Nascene AA, Nicol
MR, Abassi M, et al: A randomized trial of hydroxychloroquine as
postexposure prophylaxis for Covid-19. N Engl J Med. 383:517–525.
2020.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Fadel R, Morrison Austin R, Vahia A, Smith
ZR, Chaudhry Z, Bhargava P, Miller J, Kenney RM, Alangaden G and
Ramesh MS: Henry Ford COVID-19 Management Task Force: Early short
course corticosteroids in hospitalized patients with COVID-19. Clin
Infect Dis: May 19, 2020 (Epub ahead of print).
|
|
86
|
Shang L, Zhao J, Hu Y, Du R and Cao B: On
the use of corticosteroids for 2019-nCoV pneumonia. Lancet.
395:683–684. 2020.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Yazdanpanah F, Hamblin MR and Rezaei N:
The immune system and COVID-19: Friend or foe? Life Sciences.
256(117900)2020.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Kolilekas L, Loverdos K, Giannakaki S,
Vlassi L, Levounets A, Zervas E and Gaga M: Can steroids reverse
the severe COVID-19 induced ‘cytokine storm’? J Med Virol: Jun 12,
2020 (Epub ahead of print).
|
|
89
|
Taboada M, Caruezo V, Naveira A and
Atanassoff PG: Corticosteroids and the hyper-inflammatory phase of
the COVID-19 disease. J Clin Anesth. 66(109926)2020.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Russell CD, Millar JE and Baillie JK:
Clinical evidence does not support corticosteroid treatment for
2019-nCoV lung injury. Lancet. 395:473–475. 2020.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Li H, Chen C, Hu F, Wang J, Zhao Q, Gale
RP and Liang Y: Impact of corticosteroid therapy on outcomes of
persons with SARS-CoV-2, SARS-CoV, or MERS-CoV infection: A
systematic review and meta-analysis. Leukemia. 34:1503–1511.
2020.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Zha L, Li S, Pan L, Tefsen B, Li Y, French
N, Chen L, Yang G and Villanueva EV: Corticosteroid treatment of
patients with coronavirus disease 2019 (COVID-19). Med J Aust.
212:416–420. 2020.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Chen RC, Tang XP, Tan SY, Liang BL, Wan Z,
Fang JQ and Zhong N: Treatment of severe acute respiratory syndrome
with glucosteroids. Chest. 129:1441–1452. 2006.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Li H, Yang S, Gu L, Zhang Y, Yan X, Liang
Z, Zhang W, Jia H, Chen W, Liu M, et al: Effect of
low-to-moderate-dose corticosteroids on mortality of hospitalized
adolescents and adults with influenza A(H1N1)pdm09 viral pneumonia.
Influenza Other Respir Viruses. 11:345–354. 2017.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Villar J, Ferrando C, Martínez D, Ambrós
A, Muñoz T, Soler JA, Aguilar G, Alba F, González-Higueras E,
Conesa LA, et al: Dexamethasone treatment for the acute respiratory
distress syndrome: A multicentre, randomised controlled trial.
Lancet Respir Med. 8:267–276. 2020.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Zhao JP, Hu Y, Du RH, Chen ZS, Jin Y, Zhou
M, J Z, Qu JM and B C: Expert consensus on the use of
corticosteroid in patients with 2019-nCoV pneumonia. Zhonghua Jie
He He Hu Xi Za Zhi. 43(E007)2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
97
|
Gimeno J, Mestres-Truyol J, Ojeda-Montes
MJ, Macip G, Saldivar-Espinoza B, Cereto-Massagué A, Pujadas G and
Garcia-Vallvé S: Prediction of novel inhibitors of the main
protease (M-pro) of SARS-CoV-2 through consensus Docking and drug
reposition. Int J Mol Sci. 21(3793)2020.PubMed/NCBI View Article : Google Scholar
|
|
98
|
Burmester GR, Feist E, Sleeman MA, Wang B,
White B and Magrini F: Mavrilimumab, a human monoclonal antibody
targeting GM-CSF receptor-α, in subjects with rheumatoid arthritis:
A randomised, double-blind, placebo-controlled, phase I,
first-in-human study. Ann Rheum Dis. 70:1542–1549. 2011.PubMed/NCBI View Article : Google Scholar
|
|
99
|
De Luca G, Cavalli G, Campochiaro C,
Della-Torre E, Angelillo P, Tomelleri A, Boffini N, Tentori S,
Mette F, Farina N, et al: GM-CSF blockade with mavrilimumab in
severe COVID-19 pneumonia and systemic hyperinflammation: A
single-centre, prospective cohort study. Lancet Rheumatol.
2:e465–e473. 2020.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Vijayvargiya P, Esquer Garrigos Z,
Castillo Almeida NE, Gurram PR, Stevens RW and Razonable RR:
Treatment considerations for COVID-19: A critical review of the
evidence (or Lack Thereof). Mayo Clin Proc. 95:1454–1466.
2020.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Temesgen Z, Assi M, Shweta FNU, Vergidis
P, Rizza SA, Bauer PR, Pickering BW, Razonable RR, Libertin CR,
Burger CD, et al: GM-CSF neutralization with lenzilumab in severe
COVID-19 pneumonia: A case-control study. Mayo Clin Proc, 2020.
|
|
102
|
Temesgen Z, Assi M, Vergidis P, Rizza SA,
Bauer PR, Pickering BW, Razonable RR, Libertin CR, Burger CD,
Orenstein R, et al: First clinical use of lenzilumab to neutralize
GM-CSF in patients with severe COVID-19 pneumonia. medRxiv
2020.2006.2008.20125369, 2020.
|
|
103
|
Alijotas-Reig J, Esteve-Valverde E,
Belizna C, Selva-O'Callaghan A, Pardos-Gea J, Quintana A, Mekinian
A, Anunciacion-Llunell A and Miró-Mur F: Immunomodulatory therapy
for the management of severe COVID-19. Beyond the anti-viral
therapy: A comprehensive review. Autoimmun Rev.
19(102569)2020.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Garbers C, Heink S, Korn T and Rose-John
S: Interleukin-6: Designing specific therapeutics for a complex
cytokine. Nat Rev Drug Discov. 17:395–412. 2018.PubMed/NCBI View Article : Google Scholar
|
|
105
|
Pfäfflin A and Schleicher E: Inflammation
markers in point-of-care testing (POCT). Anal Bioanal Chem.
393:1473–1480. 2009.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Bloos F and Reinhart K: Rapid diagnosis of
sepsis. Virulence. 5:154–160. 2014.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Ma L, Zhang H, Yin Y, Guo W, Ma Y, Wang Y,
Shu C and Dong L: Role of interleukin-6 to differentiate sepsis
from non-infectious systemic inflammatory response syndrome.
Cytokine. 88:126–135. 2016.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Xu X, Han M, Li T, Sun W, Wang D, Fu B,
Zhou Y, Zheng X, Yang Y, Li X, et al: Effective treatment of severe
COVID-19 patients with tocilizumab. Proc Natl Acad Sci USA.
117:10970–10975. 2020.PubMed/NCBI View Article : Google Scholar
|
|
109
|
Taylor PC, Keystone EC, van der Heijde D,
Weinblatt ME, del Carmen Morales L, Reyes Gonzaga J, Yakushin S,
Ishii T, Emoto K, Beattie S, et al: Baricitinib versus Placebo or
Adalimumab in Rheumatoid Arthritis. N Engl J Med. 376:652–662.
2017.PubMed/NCBI View Article : Google Scholar
|
|
110
|
Bronte V, Ugel S, Tinazzi E, Vella A, De
Sanctis F, Canè S, Batani V, Trovato R, Fiore A, Petrova V, et al:
Baricitinib restrains the immune dysregulation in severe COVID-19
patients. J Clin Invest: 141772, 2020. Doi: 10.1172/JCI141772.
(Online ahead of print).
|
|
111
|
Stebbing J, Phelan A, Griffin I, Tucker C,
Oechsle O, Smith D and Richardson P: COVID-19: Combining antiviral
and anti-inflammatory treatments. Lancet Infect Dis. 20:400–402.
2020.PubMed/NCBI View Article : Google Scholar
|
|
112
|
Jorgensen SCJ, Ly Tse C, Burry L and
Dresser LD: Baricitinib: A review of pharmacology, safety and
emerging clinical experience in COVID-19. Pharmacotherapy.
40:843–856. 2020.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Richardson P, Griffin I, Tucker C, Smith
D, Oechsle O, Phelan A, Rawling M, Savory E and Stebbing J:
Baricitinib as potential treatment for 2019-nCoV acute respiratory
disease. Lancet. 395:e30–e31. 2020.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Cantini F, Niccoli L, Matarrese D,
Nicastri E, Stobbione P and Goletti D: Baricitinib therapy in
COVID-19: A pilot study on safety and clinical impact. J Infect.
81:318–356. 2020.PubMed/NCBI View Article : Google Scholar
|
|
115
|
National Institute of Allergy and
Infectious Diseases: Adaptive COVID-19 Treatment Trial 2.
urihttp://ClinicalTrials.govsimpleClinicalTrials.gov
Identifier: NCT04401579. urihttps://clinicaltrials.gov/ct2/show/NCT04401579?cond=ACTT-2&draw=2&rank=1simplehttps://clinicaltrials.gov/ct2/show/NCT04401579?cond=ACTT-2&draw=2&rank=1.
Last Updated August 13, 2020.
|
|
116
|
National Institute of Allergy and
Infectious Diseases: Adaptive COVID-19 treatment trial (ACTT).
urihttp://ClinicalTrials.govsimpleClinicalTrials.gov
Identifier: NCT04280705. urihttps://clinicaltrials.gov/ct2/show/study/NCT04280705simplehttps://clinicaltrials.gov/ct2/show/study/NCT04280705.
|
|
117
|
Wu R, Wang L, Kuo HD, Shannar A, Peter R,
Chou PJ, Li S, Hudlikar R, Liu X, Liu Z, et al: An update on
current therapeutic drugs treating COVID-19. Curr Pharmacol.
Rep:1–15. 2020.PubMed/NCBI View Article : Google Scholar
|
|
118
|
Roback JD and Guarner J: Convalescent
plasma to treat COVID-19: Possibilities and challenges. JAMA.
323:1561–1562. 2020.PubMed/NCBI View Article : Google Scholar
|
|
119
|
Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan
J, Wang F, Li D, Yang M, Xing L, et al: Treatment of 5 critically
ill patients with COVID-19 with convalescent plasma. JAMA.
323:1582–1589. 2020.PubMed/NCBI View Article : Google Scholar
|
|
120
|
Xia X, Li K, Wu L, Wang Z, Zhu M, Huang B,
Li J, Wang Z, Wu W, Wu M, et al: Improved clinical symptoms and
mortality among patients with severe or critical COVID-19 after
convalescent plasma transfusion. Blood. 136:755–759.
2020.PubMed/NCBI View Article : Google Scholar
|
|
121
|
Hegerova L, Gooley TA, Sweerus KA, Maree
C, Bailey N, Bailey M, Dunleavy V, Patel K, Alcorn K, Haley R, et
al: Use of convalescent plasma in hospitalized patients with
Covid-19: Case series. Blood. 136:759–762. 2020.PubMed/NCBI View Article : Google Scholar
|
|
122
|
Duan K, Liu B, Li C, Zhang H, Yu T, Qu J,
Zhou M, Chen L, Meng S, Hu Y, et al: Effectiveness of convalescent
plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci USA.
117:9490–9496. 2020.PubMed/NCBI View Article : Google Scholar
|
|
123
|
Li L, Zhang W, Hu Y, Tong X, Zheng S, Yang
J, Kong Y, Ren L, Wei Q, Mei H, et al: Effect of convalescent
plasma therapy on time to clinical improvement in patients with
severe and life-threatening COVID-19: A randomized clinical trial.
JAMA. 324:460–470. 2020.PubMed/NCBI View Article : Google Scholar
|
|
124
|
Sharpe HR, Gilbride C, Allen E,
Belij-Rammerstorfer S, Bissett C, Ewer K and Lambe T: The early
landscape of coronavirus disease 2019 vaccine development in the UK
and rest of the world. Immunology. 160:223–232. 2020.PubMed/NCBI View Article : Google Scholar
|
|
125
|
Callaway E: The race for coronavirus
vaccines: A graphical guide. Nature. 580:576–577. 2020.PubMed/NCBI View Article : Google Scholar
|
|
126
|
Gao Q, Bao L, Mao H, Wang L, Xu K, Yang M,
Li Y, Zhu L, Wang N, Lv Z, et al: Development of an inactivated
vaccine candidate for SARS-CoV-2. Science. 369:77–81.
2020.PubMed/NCBI View Article : Google Scholar
|
|
127
|
Wang H, Zhang Y, Huang B, Deng W, Quan Y,
Wang W, Xu W, Zhao Y, Li N, Zhang J, et al: Development of an
inactivated vaccine candidate, BBIBP-CorV, with potent protection
against SARS-CoV-2. Cell. 182:713–721.e9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
128
|
Zhu FC, Li YH, Guan XH, Hou LH, Wang WJ,
Li JX, Wu SP, Wang BS, Wang Z, Wang L, et al: Safety, tolerability,
and immunogenicity of a recombinant adenovirus type-5 vectored
COVID-19 vaccine: A dose-escalation, open-label, non-randomised,
first-in-human trial. Lancet. 395:1845–1854. 2020.PubMed/NCBI View Article : Google Scholar
|