Introduction
Thyroid carcinoma is the most common type of
malignant tumor of the endocrine system; in recent years, there has
been a gradual rise in associated morbidity and this has been
increasingly studied by clinicians and researchers (1), and exhibits the fastest increase in
incidence among all types of malignant tumors. The soaring rate of
thyroid carcinoma is primarily due to papillary carcinoma,
particularly in its earliest stages (i.e. microcarcinoma) (2). According to the latest Surveillance,
Epidemiology and End Results data, nearly 90% of thyroid carcinomas
are of the papillary type (3),
indicating the particular importance of studying thyroid papillary
microcarcinoma (PTMC). In addition, PTMC has a cervical lymph-node
metastasis rate that is as high as 30-70% (4-6).
Certain patients experience early postsurgical local recurrences or
even initially present with distant metastases to the lungs or bone
(4,5).
The BRAF V600E mutation is the most common mutation
identified in papillary thyroid carcinoma (PTC) (6), corresponding to 28-83% of all gene
mutations observed and accounting for ~90% of all BRAF mutations
(7-9),
but it has not been detected in normal thyroid tissues or benign
lesions (10-14).
The presence of the BRAF V600E mutation is closely associated with
papillary carcinoma recurrence and patient mortality. In addition,
numerous patients choose surgical treatment for PTMC due to the
high morbidity rate (15) However,
certain patients develop recurrent PTMC postoperatively (16). This study focused on BRAF V600E,
clinical pathology and imaging factors to explore their
associations with PTMC recurrence. According to the definition by
the World Health Organization, PTC with a maximal diameter of tumor
≤1 cm is considered PTMC (17).
Patients and methods
Research subjects
The independent ethics committee of China Medical
University (Shenyang, China) approved this study. In total, 506
patients were included who underwent surgery for a thyroid nodule
(maximal diameter ≤1.0 cm) and underwent preoperative BRAF V600E
testing at the Department of Thyroid Surgery of the First
Affi�liated Hospital of China Medical University between January
2014 and March 2016. The cohort comprised 420 females and 86 males
with an age range of 17-73 years (mean age, 39.6±2.6 years). All
patients were pathologically diagnosed with PTMC, including 359
patients diagnosed with a single nodule and 147 patients with two
and more nodules. The mean and median diameters of nodules were
0.63 cm [standard deviation (SD), 0.21 cm] and 0.6 cm (range,
0.41-1.00 cm). Partial thyroidectomy was performed for unilateral
nodules and total thyroidectomy for bilateral nodules. None of the
patients included had any contraindications for surgery and signed
informed consent forms. Patients with a history of other tumors
were excluded.
Procedures
Phillip iu22 and EPIQ7 color Doppler ultrasonic (US)
diagnosis systems (Philips Medical Systems, Inc.) with a probe
frequency of 5-12 MHz were used. Patients were placed in a supine
position. The thyroid glands were scanned preoperatively to
determine the size, number, position, border, shape and internal
echo of thyroid nodules and the presence or absence of lymph node
metastasis. Surgical treatment was performed after the diagnosis
was confirmed by cytopathological evaluation. Prior to surgical
resection of the thyroid nodules, BRAF V600E testing was performed
using the Amplification Refractory Mutation System method with the
human BRAF gene V600E mutation detection kit (Shanghai Yuanqi
Biological Co., Ltd.) and the manufacturer's protocol was strictly
followed. During the test, 5 µl of the standardized DNA template
was pipetted into 35 µl of the reaction mixture containing Taq
enzyme (40 µl of the PCR reaction system). Nodule positions were
classified as being in the central area or marginal area; the
marginal area included anterior, posterior, lateral and medial
borders and the isthmus of the thyroid gland and the central area
consisted of the remaining parts of the thyroid gland.
Follow-up
All patients underwent thyroid-stimulating hormone
(TSH)-suppressive therapy with levothyroxine postoperatively. At 3,
6, 12, 18, 24, 36, 48 and 60 months after the operation, each
patient was followed up, and US scan, thyroglobulin (TG) and
thyroid function tests (including serum TSH, FT4, FT3, and anti-TG
antibody) were performed to detect recurrence and metastasis. For
patients with suspected or proven elevation of TG, enhanced CT and
cytopathological examinations were performed to evaluate
metastasis, and emission computed tomography (ECT) or positron
emission tomography-CT (PET-CT) examination was performed as
necessary.
To assess serum TG levels, electrochemiluminescence
immunoassay using the Cobas e601 immunoassay analyzer (Roche
Diagnostics) was used. Functional sensitivity is defined as the
lowest analyte concentration that can be reproducibly measured with
a precision coefficient of variation (CV) of 20%; the functional
sensitivity was 0.1 ng per milliliter. Using a chemiluminescence
immunoassay with an automated immunoassay analyzer (Architect
i2000; Abbott Laboratories; reference range, 0.35-4.94 µIU/ml;
functional sensitivity, 0.01 µIU/ml), serum thyroid-stimulating
hormone (TSH) levels were measured.
A lymph node is defined as abnormal on
ultrasonography if it meets any of the following criteria (12): i) Loss of fatty hilum, ii) diffuse
or focal hyperechogenicity, iii) cystic changes, iv)
microcalcifications, v) round shape, or vi) disorganized or
peripheral vascularity. Any lymph nodes classified as abnormal
underwent cytopathological examination; those in which cancer cells
were detected were considered metastatic.
Recurrence
It was determined that there was no clinical
evidence of disease if the following criteria were satisfied: i)
Suppressed thyroglobulin (TG) <1 ng/ml, ii) stimulated TG <2
ng/ml, iii) no detectable anti-TG antibody, or iv) no evidence of
disease on ultrasonography, computed tomography (CT), MRI, positron
emission tomography-CT (PET-CT) or ECT at the final follow-up.
Persistence was defined as suppressed TG ≥1 ng/ml, stimulated TG ≥2
ng/ml, or any evidence of disease on ultrasonography, CT, MRI,
PET-CT or ECT after initial surgery and remnant ablation therapy
with radioiodine. Recurrence was defined as malignancy diagnosed
based on cytology results, elevated serum TG, or PET-CT, ECT in
patients with no clinical evidence of disease (18). For a suspected recurrent mass
detected on ultrasound, ultrasound-guided fine-needle aspiration
(FNA) was usually performed. Cytopathological results were then
obtained from the samples taken from the FNA and surgical
excision.
Statistical analysis
SPSS v21.0 software (IBM Corp.) was used for data
analysis. Measurement data are presented as the mean ± SD and
numerical data are expressed as n (%). The categorical variables
associated with the recurrent rate were compared among different
groups using univariate Cox linear regression analysis to screen
for protective and adverse factors influencing recurrence of PTMC.
Survival rates were calculated using the Kaplan-Meier method and
compared using a log-rank test. A multivariate Cox proportional
hazard regression model was used to estimate the mortality risk.
Subsequently, stepwise multivariate co-variant analysis of the
recurrence rates in different groups was performed using the Cox
proportional hazards regression model to explore risk factors of
recurrence. P<0.05 was considered to indicate statistical
significance.
Results
Follow-up findings
During the study, there was no case of death; 477
patients were followed up, 29 patients were lost to follow-up and
26 patients experienced recurrence; the 5-year recurrent rate was
5.45%. The follow-up time from initial treatment to final clinical
follow-up was 49.7 months (SD, 11.6 months; median, 48.5 months;
range, 36.0-60.0 months). During follow-up, there was no case of
recurrence at 3 and 6 months, 1 case of recurrence each at 12 and
18 months, 3 new cases of recurrence at 24 months, 5 new cases of
recurrence at 36 months and 8 new cases of recurrence at 48 and 60
months (Table I).
 | Table IThe recurrence time and number of
cases of papillary thyroid microcarcinoma. |
Table I
The recurrence time and number of
cases of papillary thyroid microcarcinoma.
| Recurrence time
(month) | 3 | 6 | 12 | 18 | 24 | 36 | 48 | 60 | Total |
|---|
| N | 0 | 0 | 1 | 1 | 3 | 5 | 8 | 8 | 26 |
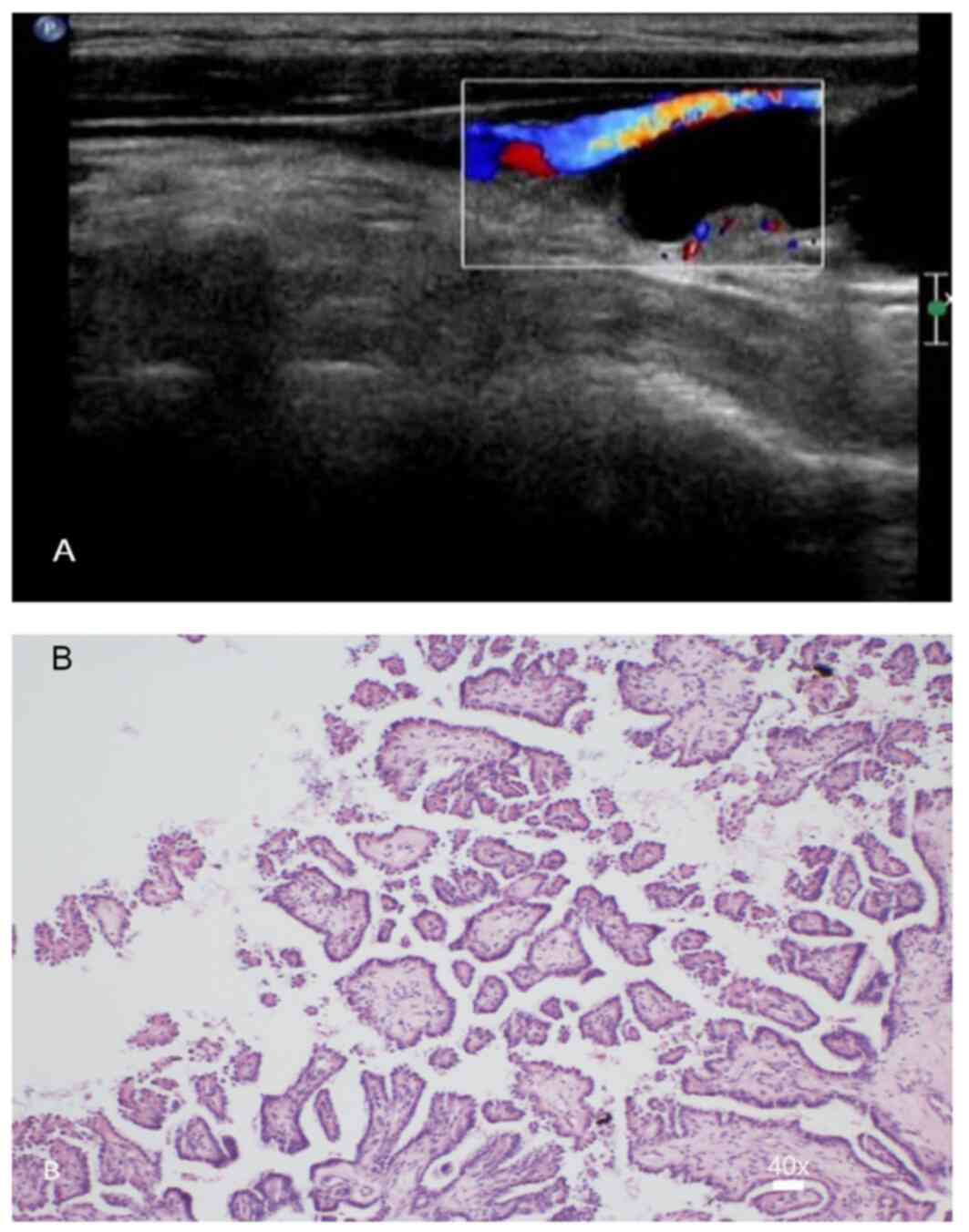
Recurrence parameters
Cases of structural recurrence accounted for 5.45%
(26/477) and all were lymph node metastasis without secondary
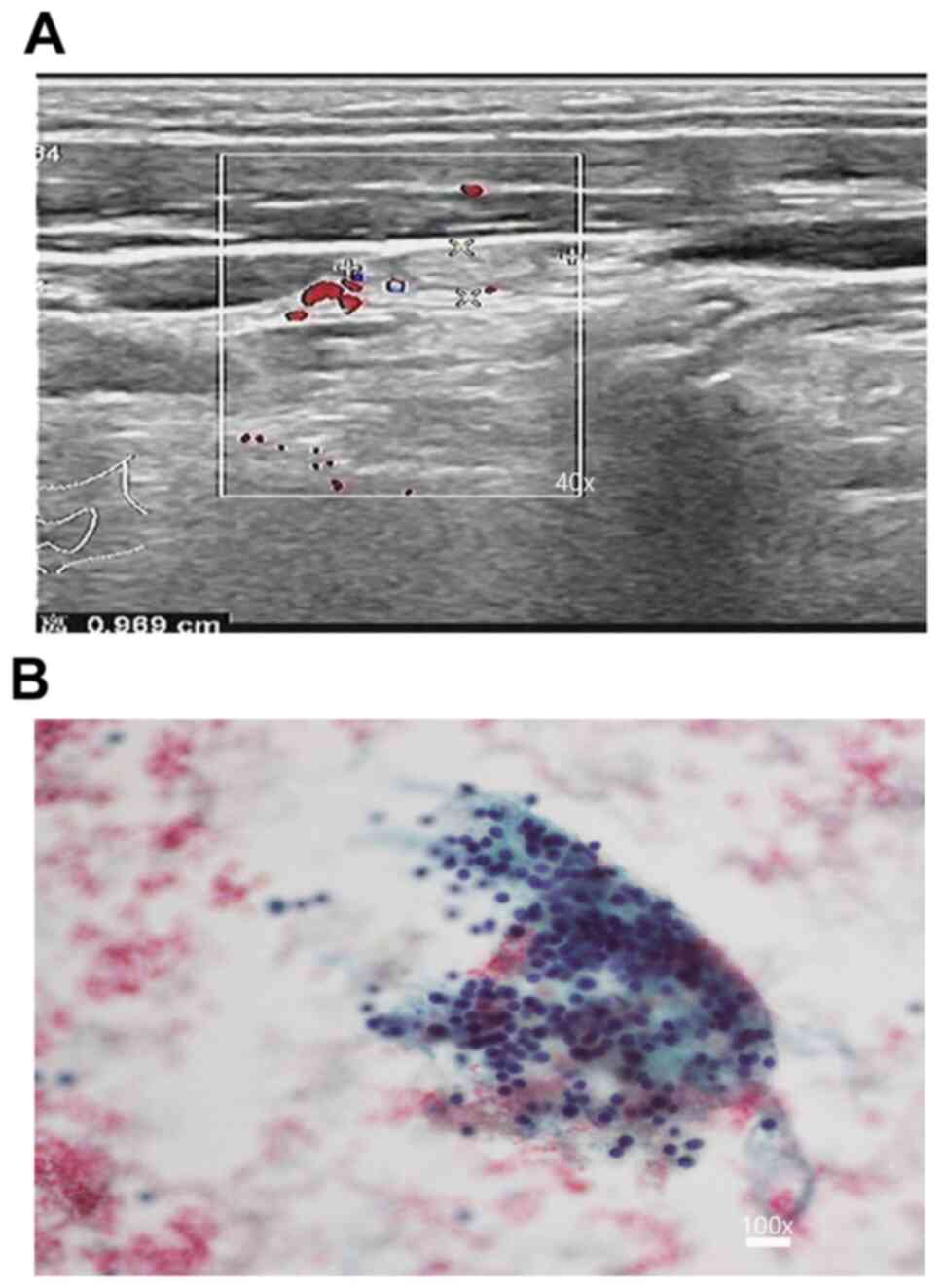
thyroid nodule or distant metastasis (Fig. 1); 1.26% (6/477) of cases exhibited
structural persistence (Fig. 2) and
biochemical recurrence accounted for 2.73% (13/477). Among the 26
patients with structural recurrence, 13 and 13 cases presented with
increased serum TG levels and normal serum TG levels, respectively;
all of these patients underwent surgery, including 2 cases
(increased TG) who underwent surgery for secondary recurrence (The
patient relapsed after undergoing a second operation following the
first recurrence) and were not indicated to have recurrence at the
second follow-up (Follow-up after the second operation). Out of the
6 patients with structural persistence, 2 cases underwent surgery
without apparent metastasis and recurrence at the last visit, and 4
cases were observed and determined to be without significant
enlargement of lymph nodes at the last follow-up (Table II).
| Table IIThe follow-up of lymph node structural
persistence. |
Table II
The follow-up of lymph node structural
persistence.
| Types of
follow-up | Lymph node
structural persistence |
|---|
| No recurrence after
surgery (N) | 2 |
| No change without
undergoing surgery (N) | 4 |
| Total | 6 |
Influencing factors of recurrence
Table III presents
details of the patients with PTMC, including the presence of BRAF
V600E, clinical pathology and imaging factors (e.g., sex, age,
lesion location, size and number, capsular invasion, metastasis
location, distant metastasis and operative approach). Univariate
Cox regression analysis indicated that recurrence of PTMC was
affected by BRAF V600E, sex, multifocality, capsular invasion and
lateral cervical lymph node metastasis (P<0.05), but not by age,
lesion location, size, single central lymph node metastasis,
distant metastasis and operative approach (P>0.05; Figs. S1 and S2).
| Table IIIAnalysis of the association of BRAF
V600E, clinical pathology and imaging factors with recurrence of
papillary thyroid microcarcinoma. |
Table III
Analysis of the association of BRAF
V600E, clinical pathology and imaging factors with recurrence of
papillary thyroid microcarcinoma.
| | | Recurrence, n
(%) | | |
|---|
| Factor | Cases (n) | Positive | Negative | HR (95% CI) | P-value |
|---|
| Location | | | | 0.451
(0.055-3.718) | 0.460 |
|
Marginal
region or near isthmus | 286 | 16 (5.59) | 270 (94.41) | | |
|
Central
region | 191 | 10 (5.24) | 181 (94.76) | | |
| Sex | | | | 1.689
(1.045-3.262) | 0.004 |
|
Female | 397 | 18 (4.53) | 379 (95.47) | | |
|
Male | 80 | 8 (10.00) | 72 (90.00) | | |
| Age (years) | | | | 1.065
(0.110-10.299) | 0.956 |
|
≥45 | 204 | 14 (6.86) | 190 (93.14) | | |
|
<45 | 273 | 12 (4.40) | 261 (95.60) | | |
| Anteroposterior
nodule size (cm) | | | | 0.444
(0.058-3.402) | 0.435 |
|
0.9-1.0 | 195 | 15 (7.69) | 180 (92.31) | | |
|
<0.9 | 282 | 11 (3.90) | 271 (96.10) | | |
| Nodule number | | | | 2.462
(1.192-5.086) | 0.015 |
|
Single | 338 | 12 (3.55) | 326 (96.45) | | |
|
Multifocal | 139 | 14 (10.07) | 125 (89.93) | | |
| BRAF V600E
testing | | | | 2.312
(1.254-4.074) | 0.022 |
|
Positive | 222 | 17 (7.66) | 205 (92.34) | | |
|
Negative | 255 | 9 (3.53) | 246 (96.47) | | |
| Capsular
invasion | | | | 1.244
(1.013-2.115) | 0.043 |
|
Yes | 77 | 7 (9.09) | 70 (90.91) | | |
|
No | 400 | 19 (4.75) | 381 (95.25) | | |
| Single central
lymph node metastasis | | | | 0.991
(0.863-1.137) | 0.894 |
|
Yes | 185 | 14 (7.57) | 171 (92.43) | | |
|
No | 292 | 12 (4.11) | 280 (95.89) | | |
| Lateral cervical
lymph node metastasis | | | | 1.899
(1.308-2.966) | 0.001 |
|
Yes | 72 | 9 (12.50) | 63 (87.50) | | |
|
No | 405 | 17 (4.20) | 88 (95.80) | | |
| Distant
metastasis | | | | 0.151
(0.009-2.529) | 0.189 |
|
Yes | 0 | 0 (0) | 0 (0) | | |
|
No | 477 | 26 (5.45) | 451 (94.55) | | |
| Operative
approach | | | | 1.012
(0.954-1.074) | 0.682 |
|
Total
thyroidectomy | 153 | 12 (7.84) | 141 (92.16) | | |
|
Unilateral
thyroidectomy | 324 | 14 (4.32) | 310 (95.68) | | |
As indicated by the stepwise multivariate Cox
proportional hazards regression model analysis of the significant
influencing factors for recurrent PTMC, sex, BRAF V600E,
multifocality and lateral cervical lymph node metastasis were
independent influencing factors for recurrence in patients with
PTMC, with a statistically significant difference (P<0.05;
Table IV).
| Table IVMultivariate stepwise Cox
proportional hazards regression model analysis of factors
influencing the recurrence of papillary thyroid microcarcinoma. |
Table IV
Multivariate stepwise Cox
proportional hazards regression model analysis of factors
influencing the recurrence of papillary thyroid microcarcinoma.
| Factor | HR (95% CI) | P-value |
|---|
| Sex (female vs.
male) | 2.340 (1.980,
5.585) | 0.032 |
| BRAF V600E
testing | 2.267 (1.311,
4.193) | 0.027 |
| Multifocality (yes
vs. no) | 3.043 (1.370,
6.759) | 0.019 |
| Capsular invasion
(yes vs. no) | 1.391
(0.702-3.906) | 0.504 |
| Lateral cervical
lymph node metastasis (yes vs. no) | 3.216
(2.393,6.634) | 0.009 |
Discussion
In recent years, the frequency of PTMC has rapidly
risen and its morbidity has markedly increased (16). Although the requirement for surgery
in the treatment of PTMC is debated, surgical management of nodal
metastasis of PTMC is undisputed and the rate of nodal metastasis
is high (16). For instance, the
reported rates of central lymph node metastasis alone range from 24
to 64% and its occurrence is associated with recurrence and death
rates (19,20). However, there is no expert consensus
on the susceptibility of PTMC types to recurrence. In the present
study, the risk of PTMC recurrence with respect to BRAF V600E,
clinical pathology factors and imaging factors was analyzed; this
analysis provided a detailed assessment of the biological behavior
and relapse rate associated with the BRAF mutation status.
Various studies have completed multi-year
postoperative follow-ups of patients with PTMC, but they have drawn
different conclusions. Hay et al (21) reported on 900 patients with PTMC
diagnosed and treated at the Mayo Clinic from 1945 to 2004, with an
average follow-up duration of 17.2 years; the 20-year and 40-year
tumor recurrence rates were 6 and 8%, respectively. Out of 281
patients with PTMC treated at the Gustave-Roussy Institute, 3.9% of
cases experienced local recurrence and 1 case developed pulmonary
metastasis (22). In a study on
patients with low-risk thyroid carcinoma (stage I or II), the
recurrence rate was 8.9% (23-28).
However, Nixon et al (29)
reported that PTMC had a low recurrence rate of only 0.6%. Durante
et al (30), confirmed that
none of their 312 patients with PTMC T1N0M0 experienced local
recurrence during a median 6-year follow-up. These conflicting
results may be due to different stages of primary carcinoma,
different FNA diagnostic criteria and a difference in the size
criterion of US-FNA used for suspected cervical lymph node lesions.
The 5-year recurrence rate in the present study was 5.45%, which is
similar to the 20-year follow-up results of the study by Hay et
al (21) and close to those
reported by the Gustave-Roussy Institute (22). However, the recurrence rate would
certainly increase with the prolongation of follow-up. Despite slow
growth, thyroid carcinoma has exhibited a high incidence rate in
recent years. Furthermore, as tumor heterogeneity is observed, the
importance of biological behaviors of PTMC should be
recognized.
The univariate analysis using univariate Cox
regression analysis indicated that BRAF V600E, sex, multifocality,
capsular invasion and lateral cervical lymph node metastasis
affected the recurrent rate of PTMC, according to the stepwise
multivariate Cox proportional hazards regression model analysis,
BRAF V600E, sex, multifocality and lateral cervical lymph node
metastasis were independent influencing factors for recurrence in
patients with PTMC (HR=2.267, 2.340, 3.043 and 3.216,
respectively), which was consistent with the results of several
previous studies (31-33).
Li et al (34), reported a
close association of BRAF V600E mutation with extracapsular
infiltration of PTC, lymph node metastasis and high TNM tumor
stage, and a subsequent higher capsular invasion rate (35). BRAF V600E-variant PTC has a
relatively higher risk of invasion, easily invades the tissues
surrounding the thyroid gland, and means that patients frequently
present at an advanced clinical stage (31,36,37)
and is associated with a worse prognosis (36,38,39).
Therefore, for patients with BRAF V600E-positive tumors, more
attention should be paid to US reexamination and TG and thyroid
function tests in order to avoid markedly elevated TSH levels. In
addition, surgery should be performed as soon as possible when BRAF
V600E-positive nodes are detected.
Sex, multifocality and lateral cervical lymph node
metastasis, as independent clinical pathology and imaging factors
influencing PTMC recurrence, are mainly associated with the
characteristics of PTMC. The incidence rate of PTMC in females is
markedly higher than that in males (up to 3.9-fold) (40), but the recurrence rate exhibits the
opposite trend, being higher in males (10.00%) than in females
(4.53%). However, a larger sample size is required to further
validate the accuracy of results because of the small number of
cases with recurrence. Multifocality, as an independent risk factor
for recurrence, contributes to the high morbidity (up to 25.7%) of
PTMC and is associated with BRAF V600E mutation (32). Therefore, regular US and TG
monitoring are required for patients with multifocality. Wada et
al (33), indicated that the
recurrence rate of patients with lateral cervical lymph node
metastasis was higher than that of patients with only central lymph
node metastasis and the difference was statistically significant;
this is comparable to the present results. The major cause for this
is that central lymph nodes are located in the VI area, the first
location of thyroid carcinoma metastasis, while lateral cervical
lymph nodes are located at the II, III and IV areas and are usually
the second location of metastasis; the lymph drainage generally
reaches the second location in the middle and advanced tumor
stages. In addition, patients with lateral cervical lymph node
metastasis are frequently at least stage T1N1bM0, and they are more
susceptible to recurrence and metastasis than patients with stage
T1N1aM0. In addition, the cutoff criterion of the thyroid nodule
size in the present study was 0.9 cm, mainly because if the nodule
size is >9 mm, its risk of metastasis increases, compared with
it risk decreasing if the size is <9 mm (41).
The present study has the following limitations.
First, it was a retrospective analysis and the exclusion of certain
cases was unavoidable. Furthermore, the sample size was relatively
small and a larger sample size is required. In addition, the
follow-up time was short and requires to be prolonged to further
validate the conclusion of the present study. In addition, the
imaging characteristics of nodules were not considered, which will
be investigated in future studies by our group.
In conclusion, PTMC has a low recurrence rate after
surgery; BRAF V600E, sex, multifocality and lateral cervical lymph
node metastasis are independent risk factors for recurrent
PTMC.
Supplementary Material
Figure S1. The survival curves of the
two capsular invasion groups were statistically significantly
different.
Figure S2. The survival curves of the
two single central lymph node metastasis groups were no
statistically significantly different.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
KH conceived this article, revised it critically for
important intellectual content and was responsible for the
interpretation of data. NG and PY made substantial contributions to
acquisition and analysis of data. DB and QZ constructed the figures
and involved in the acquisition of data. YZ collected the data
regarding the patients, drafted the manuscript and approved it for
publication. The final version of the manuscript has been read and
approved by all authors, and each author believes that the
manuscript represents honest work.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the First Affiliated Hospital of China Medical
University (Shenyang, Liaoning, China; no. AF-SOP-07-1.0-01).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Huang K, Bai Z, Bian D, Yang P, Li X and
Liu Y: Diagnostic accuracy of contrast-enhanced ultrasonography in
papillary thyroid microcarcinoma stratified by size. Ultrasound Med
Biol. 46:269–274. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chen AY, Jemal A and Ward EM: Increasing
incidence of differentiated thyroid cancer in the United States,
1988-2005. Cancer. 115:3801–3807. 2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Davies L and Welch HG: Increasing
incidence of thyroid cancer in the United States, 1973-2002. JAMA.
295:2164–2167. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Xu YH, Song HJ, Qiu ZL and Luo QY: Brain
metastases with exceptional features from papillary thyroid
carcinoma: Report of three cases. Hell J Nucl Med. 14:56–59.
2011.PubMed/NCBI
|
|
5
|
Varsavsky M, Cortés Berdonces M, Alonso G,
García Martín A and Muñoz Torres M: Metastatic adenopathy from a
thyroid microcarcinoma: Final diagnosis of a presumed
paraganglioma. Endocrinol Nutr. 58:143–144. 2011.(In Spanish).
PubMed/NCBI View Article : Google Scholar
|
|
6
|
Xing M, Westra WH, Tufano RP, Cohen Y,
Rosenbaum E, Rhoden KJ, Carson KA, Vasko V, Larin A, Tallini G, et
al: BRAF mutation predicts a poorer clinical prognosis for
papillary thyroid cancer. J Clin Endocrinol Metab. 90:6373–6379.
2005.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kim SW, Lee JI, Kim JW, Ki CS, Oh YL, Choi
YL, Shin JH, Kim HK, Jang HW and Chung JH: BRAFV600E mutation
analysis in fine-needle aspiration cytology specimens for
evaluation of thyroid nodule: A large series in a
BRAFV600E-prevalent population. J Clin Endocrinol Metab.
95:3693–3700. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Min HS, Lee C and Jung KC: Correlation of
immunohistochemical markers and BRAF mutation status with
histological variants of papillary thyroid carcinoma in the Korean
population. J Korean Med Sci. 28:534–541. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kwak JY, Kim EK, Chung WY, Moon HJ, Kim MJ
and Choi JR: Association of BRAFV600E mutation with poor clinical
prognostic factors and US features in Korean patients with
papillary thyroid microcarcinoma. Radiology. 253:854–860.
2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Millington GW: Mutations of the BRAF gene
in human cancer, by Davies et al. (Nature 417: 949-954,
2002). Clin Exp Dermatol. 38:222–223. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
DeLuca AM, Srinivas A and Alani RM: BRAF
kinase in melanoma development and progression. Expert Rev Mol Med.
10(e6)2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Liu Z, Lv T, Xie C and Di Z: BRAF V600E
gene mutation is associated with bilateral malignancy of papillary
thyroid cancer. Am J Med Sci. 356:130–134. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kebebew E, Weng J, Bauer J, Ranvier G,
Clark OH, Duh QY, Shibru D, Bastian B and Griffin A: The prevalence
and prognostic value of BRAF mutation in thyroid cancer. Ann Surg.
246:466–471. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kim TH, Park YJ, Lim JA, Ahn HY, Lee EK,
Lee YJ, Kim KW, Hahn SK, Youn YK, Kim KH, et al: The association of
the BRAF(V600E) mutation with prognostic factors and poor clinical
outcome in papillary thyroid cancer: A meta-analysis. Cancer.
118:1764–1773. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Gschwandtner E, Klatte T, Swietek N, Bures
C, Kober F, Ott J, Schultheis A, Neuhold N and Hermann M: Increase
of papillary thyroid microcarcinoma and a plea for restrictive
treatment: A retrospective study of 1,391 prospective documented
patients. Surgery. 159:503–511. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yi D, Song P, Huang T, Tang X and Sang J:
A meta-analysis on the effect of operation modes on the recurrence
of papillary thyroid microcarcinoma. Oncotarget. 8:7148–7156.
2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Sobin LH: Histological typing of thyroid
tumours. Histopathology. 16(513)1990.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Yoon JH, Lee HS, Kim EK, Youk JH, Kim HG,
Moon HJ and Kwak JY: Short-term follow-up us leads to higher
false-positive results without detection of structural recurrences
in PTMC. Medicine (Baltimore). 95(e2435)2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Huang XP, Ye TT, Zhang L, Liu RF, Lai XJ,
Wang L, Yang M, Zhang B, Li XY, Liu ZW, et al: Sonographic features
of papillary thyroid microcarcinoma predicting high-volume central
neck lymph node metastasis. Surg Oncol. 27:172–176. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Ferris RL, Baloch Z, Bernet V, Chen A,
Fahey TJ III, Ganly I, Hodak SP, Kebebew E, Patel KN, Shaha A, et
al: American thyroid association statement on surgical application
of molecular profiling for thyroid nodules: Current impact on
perioperative decision making. Thyroid. 25:760–768. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Hay ID, Hutchinson ME, Gonzalez-Losada T,
McIver B, Reinalda ME, Grant CS, Thompson GB, Sebo TJ and Goellner
JR: Papillary thyroid microcarcinoma: A study of 900 cases observed
in a 60-year period. Surgery. 144:980–988. 2008.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Baudin E, Travagli JP, Ropers J, Mancusi
F, Bruno-Bossio G, Caillou B, Cailleux AF, Lumbroso JD, Parmentier
C and Schlumberger M: Microcarcinoma of the thyroid gland: The
Gustave-Roussy Institute experience. Cancer. 83:553–559.
1998.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Pacini F, Molinaro E, Castagna MG, Agate
L, Elisei R, Ceccarelli C, Lippi F, Taddei D, Grasso L and Pinchera
A: Recombinant human thyrotropin-stimulated serum thyroglobulin
combined with neck ultrasonography has the highest sensitivity in
monitoring differentiated thyroid carcinoma. J Clin Endocrinol
Metab. 88:3668–3673. 2003.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Torlontano M, Attard M, Crocetti U, Tumino
S, Bruno R, Costante G, D'Azzò G, Meringolo D, Ferretti E, Sacco R,
et al: Follow-up of low risk patients with papillary thyroid
cancer: Role of neck ultrasonography in detecting lymph node
metastases. J Clin Endocrinol Metab. 89:3402–3407. 2004.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Tuttle RM, Tala H, Shah J, Leboeuf R,
Ghossein R, Gonen M, Brokhin M, Omry G, Fagin JA and Shaha A:
Estimating risk of recurrence in differentiated thyroid cancer
after total thyroidectomy and radioactive iodine remnant ablation:
Using response to therapy variables to modify the initial risk
estimates predicted by the new American thyroid association staging
system. Thyroid. 20:1341–1349. 2010.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Leboulleux S, Girard E, Rose M, Travagli
JP, Sabbah N, Caillou B, Hartl DM, Lassau N, Baudin E and
Schlumberger M: Ultrasound criteria of malignancy for cervical
lymph nodes in patients followed up for differentiated thyroid
cancer. J Clin Endocrinol Metab. 92:3590–3594. 2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Pelttari H, Laitinen K, Schalin-Jäntti C
and Välimäki MJ: Long-term outcome of 495 TNM stage I or II
patients with differentiated thyroid carcinoma followed up with
neck ultrasonography and thyroglobulin measurements on T4
treatment. Clin Endocrinol (Oxf). 69:323–331. 2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Yoon JH, Kim JY, Moon HJ, Youk JH, Son EJ,
Kim EK, Han KH and Kwak JY: Contribution of computed tomography to
ultrasound in predicting lateral lymph node metastasis in patients
with papillary thyroid carcinoma. Ann Surg Oncol. 18:1734–1741.
2001.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Nixon IJ, Ganly I, Patel SG, Palmer FL,
Whitcher MM, Tuttle RM, Shaha A and Shah JP: Thyroid lobectomy for
treatment of well differentiated intrathyroid malignancy. Surgery.
151:571–579. 2012.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Durante C, Attard M, Torlontano M, Ronga
G, Monzani F, Costante G, Ferdeghini M, Tumino S, Meringolo D,
Bruno R, et al: Identification and optimal postsurgical follow-up
of patients with very low-risk papillary thyroid microcarcinomas. J
Clin Endocrinol Metab. 95:4882–4888. 2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Kim MH, Bae JS, Lim DJ, Lee H, Jeon SR,
Park GS and Jung CK: Quantification of BRAF V600E alleles predicts
papillary thyroid cancer progression. Endocr Relat Cancer.
21:891–902. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Shin DY, Kim KJ, Chang S, Kim H, Hwang S,
Kim W, Bae J, Park S, Kang SW, Chung WY and Lee EJ: Follicular
variant of papillary thyroid carcinoma with B-type Raf(V600E)
showing higher frequency of suspicious sonographic features and
multifocality. Head Neck. 37:1590–1595. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Wada N, Duh QY, Sugino K, Iwasaki H,
Kameyama K, Mimura T, Ito K, Takami H and Takanashi Y: Lymph node
metastasis from 259 papillary thyroid microcarcinomas: Frequency,
pattern of occurrence and recurrence, and optimal strategy for neck
dissection. Ann Surg. 237:399–407. 2003.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Li F, Chen G, Sheng C, Gusdon AM, Huang Y,
Lv Z, Xu H, Xing M and Qu S: BRAFV600E mutation in papillary
thyroid microcarcinoma: A meta-analysis. Endocr Relat Cancer.
22:159–168. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Guo L, Ma YQ, Yao Y, Wu M, Deng ZH, Zhu
FW, Luo YK and Tang J: Role of ultrasonographic features and
quantified BRAFV600E mutation in lymph node metastasis in Chinese
patients with papillary thyroid carcinoma. Sci Rep.
9(75)2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Xing M, Alzahrani AS, Carson KA, Viola D,
Elisei R, Bendlova B, Yip L, Mian C, Vianello F, Tuttle RM, et al:
Association between BRAF V600E mutation and mortality in patients
with papillary thyroid cancer. JAMA. 309:1493–1501. 2013.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lin KL, Wang OC, Zhang XH, Dai XX, Hu XQ
and Qu JM: The BRAF mutation is predictive of aggressive
clinicopathological characteristics in papillary thyroid
microcarcinoma. Ann Surg Oncol. 17:3294–3300. 2010.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Miccoli P and Basolo F: BRAF mutation
status in papillary thyroid carcinoma: Significance for surgical
strategy. Langenbecks Arch Surg. 399:225–228. 2014.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Durante C, Puxeddu E, Ferretti E, Morisi
R, Moretti S, Bruno R, Barbi F, Avenia N, Scipioni A, Verrienti A,
et al: BRAF mutations in papillary thyroid carcinomas inhibit genes
involved in iodine metabolism. J Clin Endocrinol Metab.
92:2840–2843. 2007.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Zafon C, Baena JA, Castellví J, Obiols G,
Monroy G and Mesa J: Differences in the form of presentation
between papillary microcarcinomas and papillary carcinomas of
larger size. J Thyroid Res. 2011(639156)2010.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Huang K, Gao N, Zhai Q, Bian D, Wang D and
Wang X: The anteroposterior diameter of nodules in the risk
assessment of papillary thyroid microcarcinoma. Medicine
(Baltimore). 97(e9712)2018.PubMed/NCBI View Article : Google Scholar
|