Introduction
An adnexal tumour is defined as an enlarged
structure within the adnexa of the uterus (1). It represents a spectrum of benign and
malignant conditions that may originate from either gynaecological
or non-gynaecological sources (2).
The pathology is usually an incidental finding diagnosed during a
routine clinical examination or may be present in females with any
gynaecological complaint (3). Since
adnexal masses may present with a wide range of symptoms, it is
frequently difficult to differentiate benign tumours from other
malignant lesions such as ovarian cancer (2).
Cross-sectional imaging strategies have a major role
in managing patients with adnexal tumours, as they are able to
consistently differentiate between benign and malignant masses
affecting the fallopian tube and ovary. It is also helpful in
differentiating uterine and gastrointestinal pathologies from
adnexal abnormalities (1). Early
and accurate diagnosis of adnexal mass is essential for formulating
a treatment plan. The ability of the imaging modality to
differentiate between a benign and malignant nature of a lesion
further influences the decision for the requirement of expectant
management (cases with no symptoms or reproductive dysfunction) or
the requirement of surgery (for borderline or invasive tumours)
(4). Laparoscopic observation and
histopathological examination are considered the gold standard for
the specific diagnosis of adnexal mass (5). However, the invasive nature of the
procedure is a significant limitation for its use in routine
clinical practice.
Despite several advances and technological
advancements in the field of radiodiagnosis, simple transvaginal
ultrasound (TVUS) has been a standard procedure for the initial
diagnosis of patients with adnexal mass (6,7).
Several studies have reported that TVUS may also help in
discriminating between benign and malignant adnexal masses and also
to make a specific diagnosis (6,7). To
the best of our knowledge, there have been no systematic efforts to
perform a data synthesis to evaluate the diagnostic accuracy of
this method. Therefore, the purpose of the present study was to
perform a meta-analysis to evaluate the diagnostic accuracy of TVUS
for the differentiation of an adnexal mass as benign or
malignant.
Materials and methods
Inclusion criteria
All types of studies examining the diagnostic
accuracy of TVUS for a specific diagnosis of an adnexal mass and
comparing it with standard laparoscopic or histopathological
examination as the reference standard were considered. Studies were
to report on sensitivity and specificity or provide data to
calculate these values. Only full-text articles were included,
while unpublished data were excluded. Studies with a sample size of
<10 patients and case reports were also excluded.
Search strategy
An extensive and systematic electronic search was
performed in the Medline, Scopus, Cochrane Library and Embase
databases. Both medical subject headings along with free text terms
were utilized for the literature search. The search terms used were
as follows: ‘Validation studies’, ‘adnexal mass’, ‘pattern
recognition’, ‘transvaginal ultrasonography’, ‘benign adnexal
mass’, ‘malignant adnexal mass’, ‘gynaecological disorders’,
‘sensitivity’, ‘specificity’, ‘diagnosis’, ‘adnexal lesions’ and
‘diagnostic accuracy studies’. The time limit for the search was
from inception to November 2019 without any language restriction.
Reference lists of primary studies were hand-searched to find any
missed articles for inclusion in the review.
Selection of studies
Primary screening of title, keywords and abstracts
was performed by two authors independently (XZ and XM). Full-text
articles of the relevant entries were retrieved. These were further
screened independently by the two authors (XZ and XM) for final
inclusion in the review. Agreement between the two authors in
making decisions related to inclusion or exclusion of studies was
found to be excellent with a kappa value of 0.82. Disagreements
during the selection of studies were resolved by consulting the
third author (TD).
Data extraction and management
The primary investigator (XZ) performed data
extraction using a data-extraction form. The following details were
extracted: Study setting, study design, inclusion and exclusion
criteria, reference standards, index test, total participants,
comorbidities, mean age, sensitivity and specificity values. The
extracted data were entered into STATA software. They were
double-checked for correct entry by comparing the data in the
review and the study reports. The following outcome measures were
analysed in the review: Sensitivity, specificity, diagnostic odds
ratio (DOR), likelihood ratio positive (LRP) and likelihood ratio
negative (LRN).
Risk of bias assessment
The risk of bias for all of the included studies was
assessed by two authors (XZ and XM) independently using the Quality
Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool
(8). Studies were rated for patient
selection bias, conduct and interpretation of index test and
reference standard, as well as time interval (i.e. flow and timing)
of the outcome assessments. The studies were graded as having low,
high or unclear risk of bias for each domain.
Statistical analysis
The final estimate of sensitivity, specificity, LRN,
LRP and DOR for TVUS was obtained using the bivariate meta-analysis
method. The summary receiver operator characteristic curve was
constructed from which area under the curve (AUC) was obtained. An
AUC value closer to 1 was indicative of a better diagnostic
value.
Forest plots were used to graphically represent the
study-specific and pooled estimates of sensitivity and specificity.
The clinical value of the TVUS was determined by the LR
scattergram. The probability of a patient having a benign or
malignant adnexal mass was tested using the Fagan plot.
Heterogeneity was assessed graphically using bivariate boxplots and
tested using the chi-square test and I2 statistic. The
source of heterogeneity was explored with meta-regression using
study-related covariates such as the study design, year of
publication, sample size, study region and quality-related factors.
Publication bias was tested using Deek's test and graphically
depicted by a funnel plot. The analysis was performed using the
‘metandi’ command package in STATA 14.2 software (StataCorp).
Results
Selection of studies
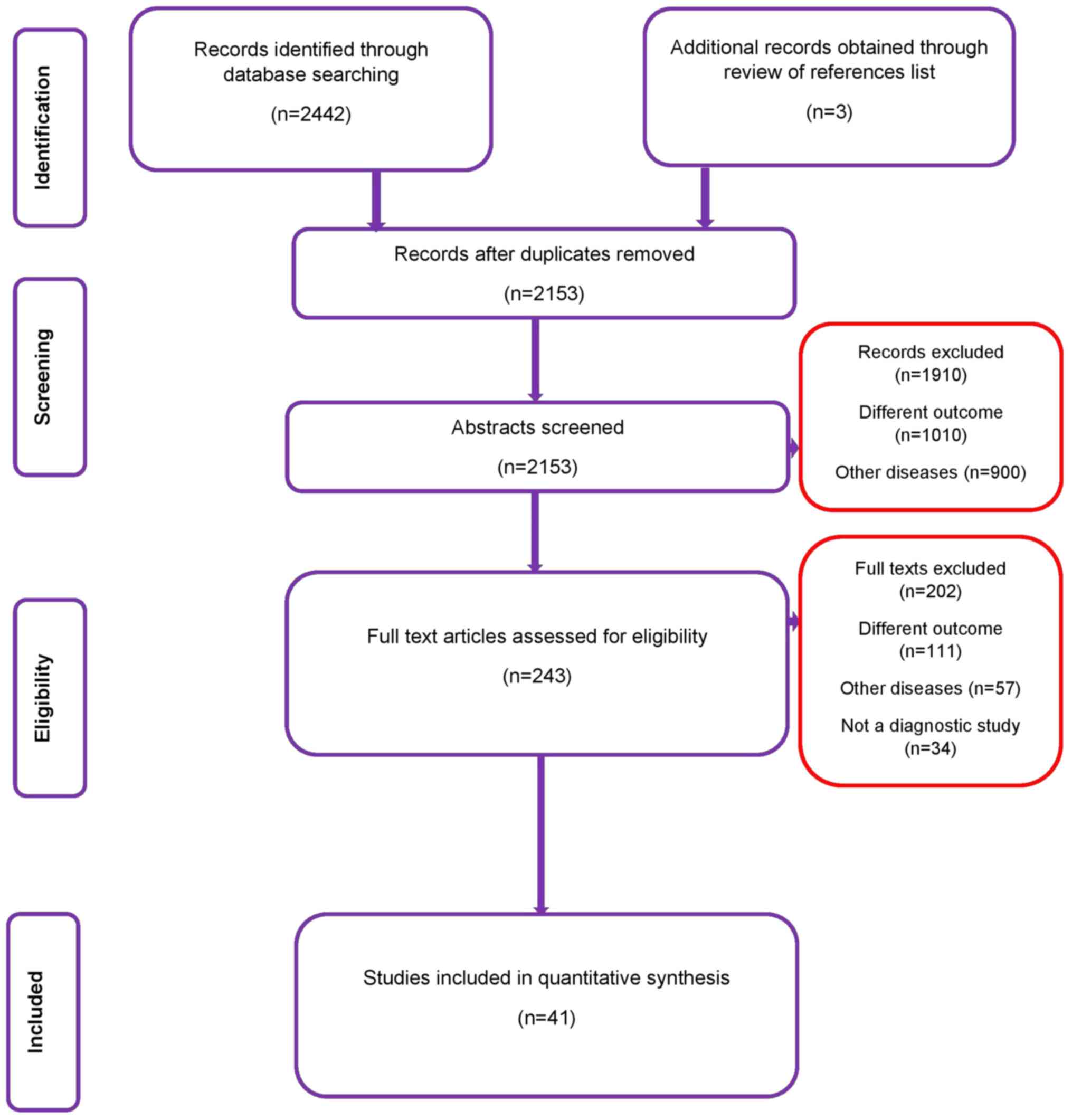
After database screening, a total of 2,442 records
were retrieved, of which 927 records were from Medline, 813 from
Scopus, 590 from Embase and 112 from the Cochrane library (Fig. 1). After the first stage of
screening, 243 relevant studies were retained. The full text of
these studies was examined against the eligibility criteria. In
total, 41 studies with 18,391 participants satisfying the inclusion
criteria were included in the present review (9-49).
Characteristics of included
studies
The characteristics of the included studies are
described in Table I. Of the
included studies, 35 were prospective studies. Most of the studies
were performed in high-income European countries such as the United
Kingdom, Italy, Belgium and Spain. The average age of the
participants ranged from 33.3 to 53.3 years. The sample size of the
studies varied from 37 to 2,403 patients. All of the included
studies used laparoscopy or laparotomy with histopathology as the
reference standard for comparing the diagnostic accuracy of TVUS.
The time interval between TVUS and the reference standard varied
from 24 h to 12 weeks.
 | Table ICharacteristics of the included
studies (n=41). |
Table I
Characteristics of the included
studies (n=41).
| First author and
year | Country | Study design | Sample size | Type of diagnostic
modality | Gold standard
comparator | Time interval
between index test and reference standard | Mean age
(years) | (Refs.) |
|---|
| Alcázar 2013 | Spain | Prospective | 340 | Simple TVUS-based
rules | Histopathology | 3 weeks | 42.1 | (9) |
| Daemen 2011 | 19 Ultrasound
centers in eight countries (Belgium, Canada, China, Czech Republic,
Italy, Poland, Sweden, UK) | Prospective | 1,938 | Subjective
assessment by grayscale TVUS | Histopathology | Not specified | Not specified | (10) |
| Ruiz de Gauna
2015 | Spain | Prospective | 247 | Simple TVUS-based
rules | Histopathology | 3 weeks | 43.6 | (11) |
| Fathallah 2011 | France | Prospective | 122 | Simple TVUS-based
rules | Histopathology | Not specified | Not specified | (12) |
| Granberg 1990 | Sweden | Prospective | 180 | Subjective
assessment by | Histopathology
grayscale TVUS | 1 week to 1
month | Not specified | (13) |
| Guerriero 2010 | Italy | Prospective | 2,148 | Subjective
assessment by | Histopathology
grayscale TVUS | Not specified | 42 | (14) |
| Hartman 2012 | Brazil |
Cross-sectional | 110 | Subjective
assessment by grayscale TVUS | Histopathology | Mean time
interval=64.4 days | Benign, 46.8
Malignant, 53.4 | (15) |
| Jain 1993 | United States of
America | Prospective
study | 37 | Endovaginal US | Surgery or
laparoscopy | 1-4 weeks | 41.5 | (16) |
| Jain 1994 | United States of
America | Prospective
study | 49 | Endovaginal US | Surgery or
laparoscopy | 1-5 days | 45 | (17) |
| Knafel 2013 | Poland | Prospective | 226 | Subjective
assessment | Histopathology by
TVUS | Not specified | 47 | (18) |
| Komatsu 1996 | Japan | Retrospective
study | 82 | TVUS | Histologic
examination | 2 weeks | 45.9 | (19) |
| Lucidarme 2010 | France | Prospective | 255 | TVUS | Histologic
examination | Not specified | Not specified | (20) |
| Mancuso 2004 | Italy | Retrospective | 125 | TVUS | Histologic
examination | Not specified | Not specified | (21) |
| Moszynski 2013 | Poland | Retrospective | 318 | TVUS | Histologic
examination | Not specified | Not specified | (22) |
| Nunes 2012 | United Kingdom | Prospective | 292 | TVUS | Histologic
examination | 120 days | 53.2 | (23) |
| Nunes 2013 | United Kingdom | Prospective | 303 | TVUS | Histologic
examination | 120 days | 51 | (24) |
| Radosa 2014 | Germany | Retrospective | 1,320 | Pattern recognition
by TVUS | Histopathology | Not specified | 33.3 | (25) |
| Romagnolo 2006 | Italy | Prospective | 221 | Subjective
assessment by TVUS | Histopathology | Not specified | Not specified | (26) |
| Roman 1997 | USA | Prospective | 226 | Grayscale TVUS | Histopathology | Not specified | Not specified | (27) |
| Salle 1995 | France | Prospective | 91 | Subjective
assessment by TVUS | Histopathology | Not specified | Not specified | (28) |
| Sayasneh 2013 | United Kingdom | Prospective
multicentric study | 255 | 2D grayscale
TVUS | Histopathology | 120 days | 46 | (29) |
| Sayasneh 2015 | United Kingdom | Prospective
multicentric study | 313 | 2D grayscale
TVUS | Histopathology | Not specified | 47 | (30) |
| Shetty 2017 | India | Prospective | 136 | Pattern recognition
by TVUS | Histopathology | Not specified | 40.5 | (31) |
| Shetty 2019 | India | Prospective | 183 | IOTA Simple rules
using TVUS | Histopathology | 12 weeks | 37.5 | (32) |
| Silvestre 2015 | Brazil | Prospective | 75 | IOTA Simple rules
using TVUS | Histopathology | 7 days | Not specified | (33) |
| Sohaib 2005 | United Kingdom | Prospective | 72 | Subjective
assessment by grayscale TVUS | Histopathology | Not specified | 53 | (34) |
| Sokalska 2009 | Nine European
centers | Retrospective | 860 | Grayscale TVUS | Histopathology | Not specified | 37 | (35) |
| Stein 1995 | USA | Prospective | 160 | Grayscale TVUS | Histopathology | Not specified | 114 patients were
premenopausal (mean, 33 years; range, 13-53), 39 were
perimenopausal or postmenopausal (mean, 57; range, 44-80) and eight
had undergone hysterectomy (mean, 44 years; range, 33-61) | (36) |
| Strigini 1996 | Italy | Prospective | 109 | TVUS | Laparotomy and
histopathology | 1 week | Median, 43 | (37) |
| Tantipalakorn
2014 | Thailand | Prospective | 398 | IOTA simple rules
using TVUS | Pathological or
operative findings | 24 h | 42.4 | (38) |
| Testa 2014 | 18 centres in six
countries (Sweden, Belgium, Italy, Poland, Spain and Czech
Republic) | Prospective | 2,403 | IOTA Logistic
regression model using TVUS | Histopathology | 120 days | Not specified | (39) |
| Timmerman 1999 | Belgium | Prospective | 300 | TVUS | Histopathology | Not specified | Premenopausal (mean
age, 40; range, 22-57); postmenopausal (mean age, 65; range,
47-93) | (40) |
| Timmerman 2010 | 19 centres in eight
European countries | Prospective | 1,501 | IOTA Simple rules
using TVUS | Histopathology | 120 days | 46 | (41) |
| Utrilla-Layna
2015 | Spain | Prospective | 367 | Pattern recognition
by TVUS | Histopathology | Not specified | 46.5 | (42) |
| Valentin 1999 | Sweden | Prospective | 173 | TVUS | Histopathology | 8 days | 98 were
premenopausal (median age, 37.5; range, 18-54), 70 were
postmenopausal (median age, 66; range, 51-88; median 15 years past
menopause with a range of 1-44 years), four had undergone
hysterectomy (median age, 51.5; range, 44-66) | (43) |
| Valentin 2009 | Nine European US
centres | Prospective | 534 | TVUS | Histopathology | 120 days | 48.8 | (44) |
| Van Calster
2007 | Nine European US
centres | Prospective | 809 | TVUS | Histopathology | Not specified | 49 | (45) |
| Van Gorp 2012 | Belgium | Prospective | 374 | Subjective
assessment by TVUS | Histopathology | Not specified | Patients with
benign disease: Mean age, 46.2; patients with malignant disease:
Mean age, 57.7 | (46) |
| Van Holsbeke
2009 | Belgium | Prospective | 507 | IOTA rules | Histopathology | Not specified using
TVUS | 40 | (47) |
| Van Trappen
2007 | United Kingdom | Prospective | 142 | TVUS | Histopathology | Not specified | 50 | (48) |
| Yamashita 1995 | Japan | Prospective | 80 | TVUS | Histopathology | 14 days | 43 | (49) |
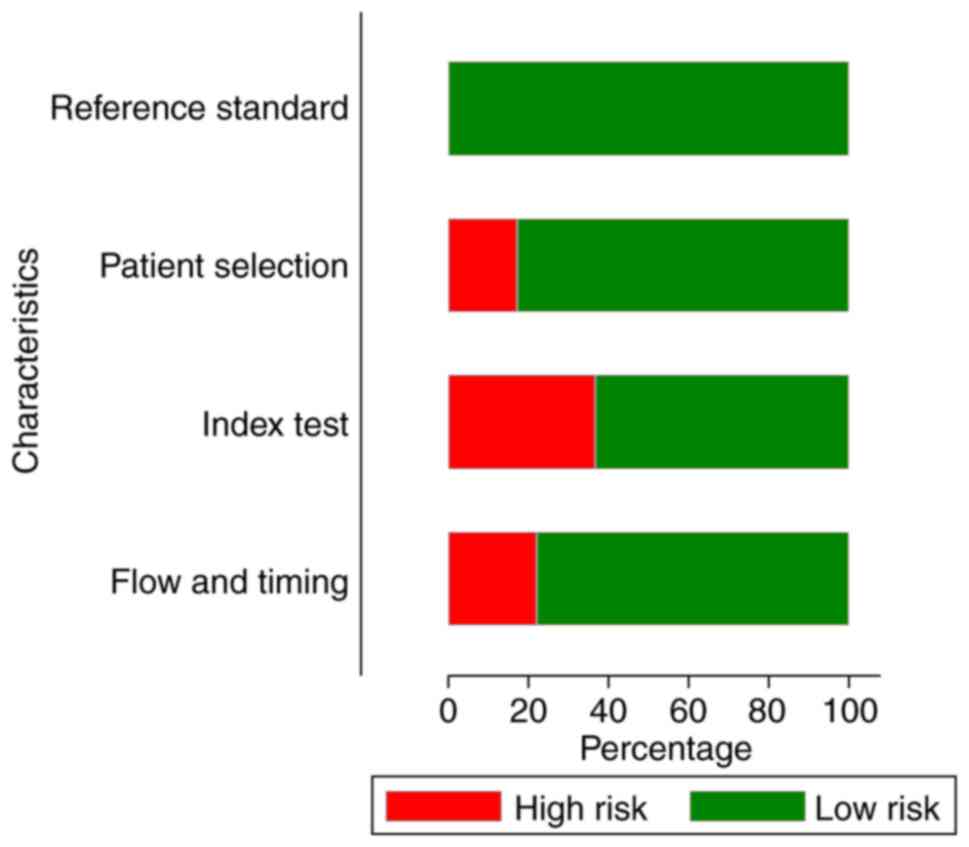
Risk of bias
The assessment of the risk of bias among the
included studies is presented in Fig.
2. Of the studies, 90% had a low risk of bias for ‘selection
bias’. Furthermore, out of the 41 studies, 26 had a low risk of
bias for ‘conduct and interpretation of index test’. All of the
studies had a low risk of bias for the ‘conduct of reference
standards test and interpretation’. A total of 32 studies had a low
risk of bias concerning ‘flow and interval between index and
reference standard test’ among the patients.
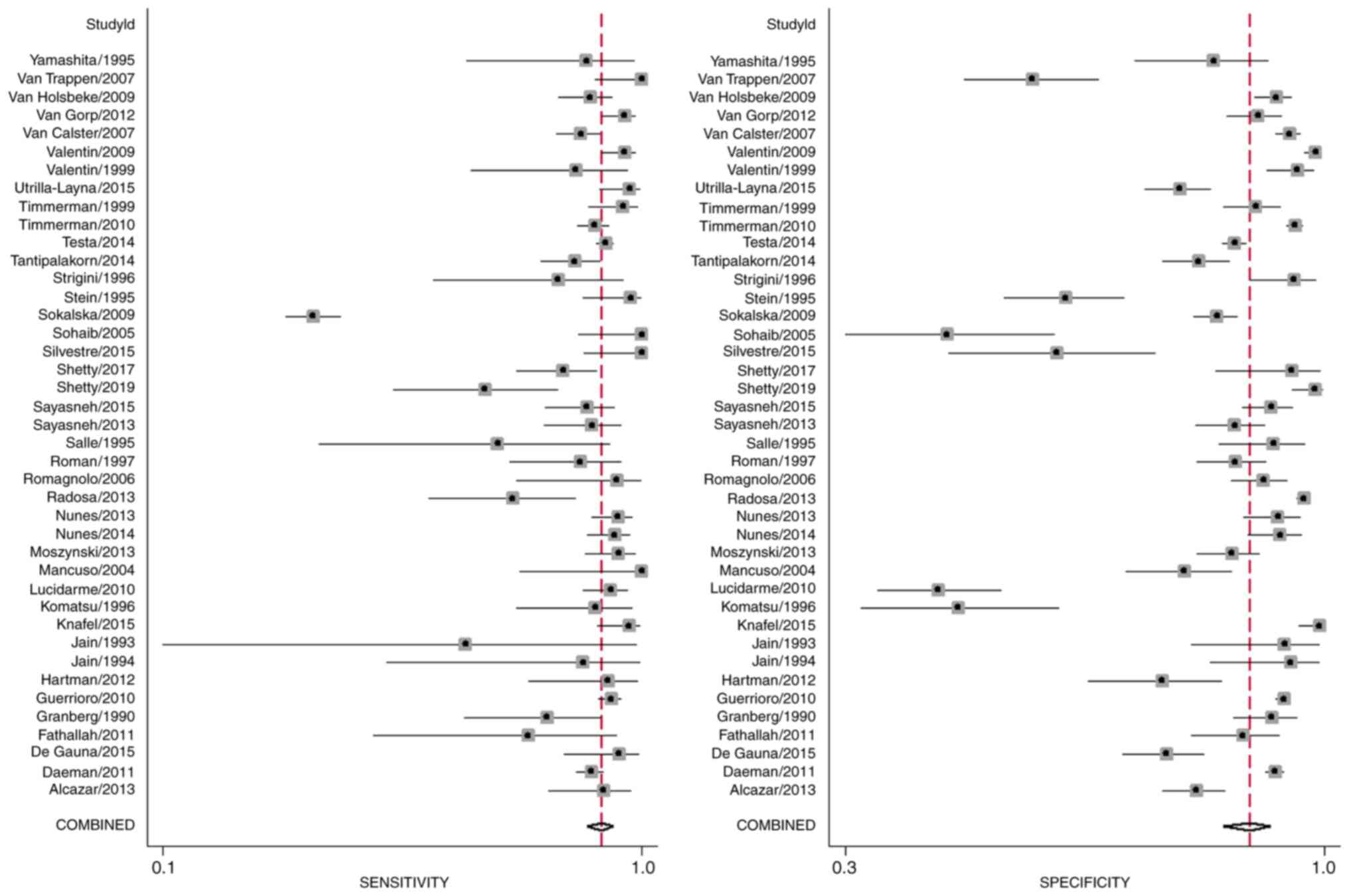
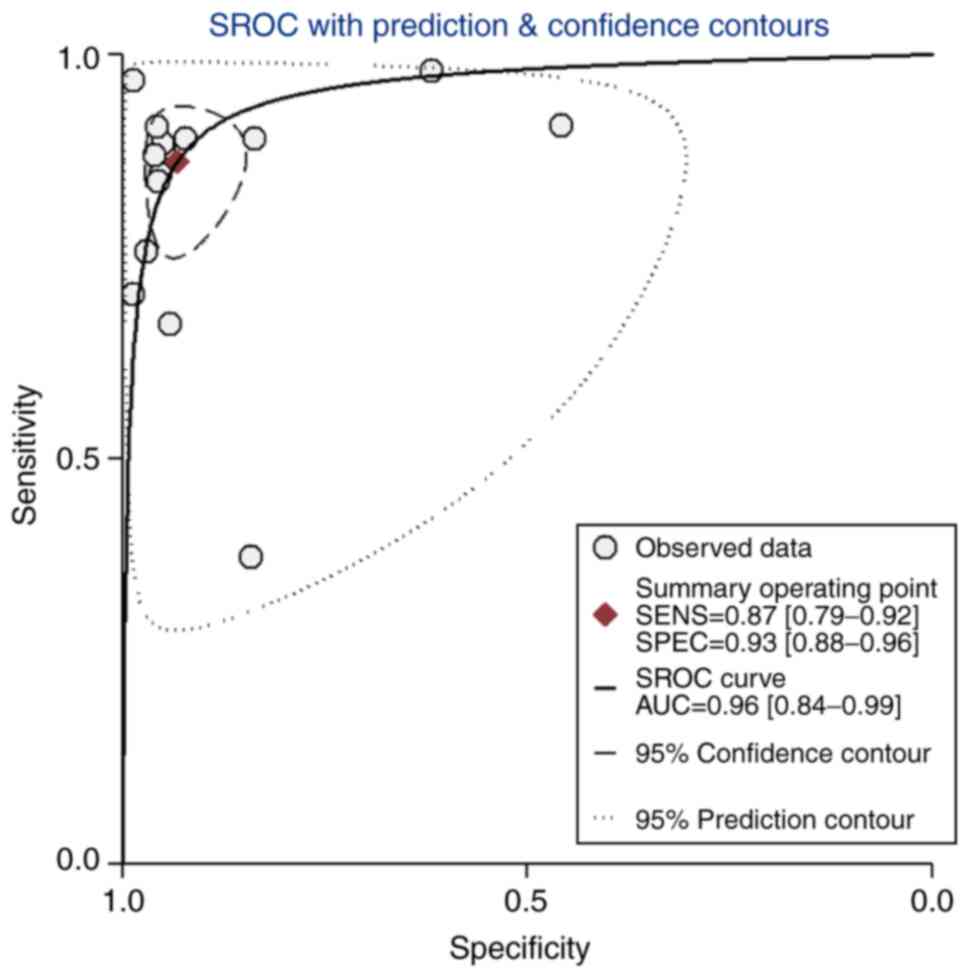
Diagnostic performance of TVUS
Analysis of data from the 41 studies provided a
pooled sensitivity and specificity of TVUS for differentiating
benign and malignant adnexal mass of 92% (95% CI: 90-94%) and 89%
(95% CI: 85-92%), respectively (Fig.
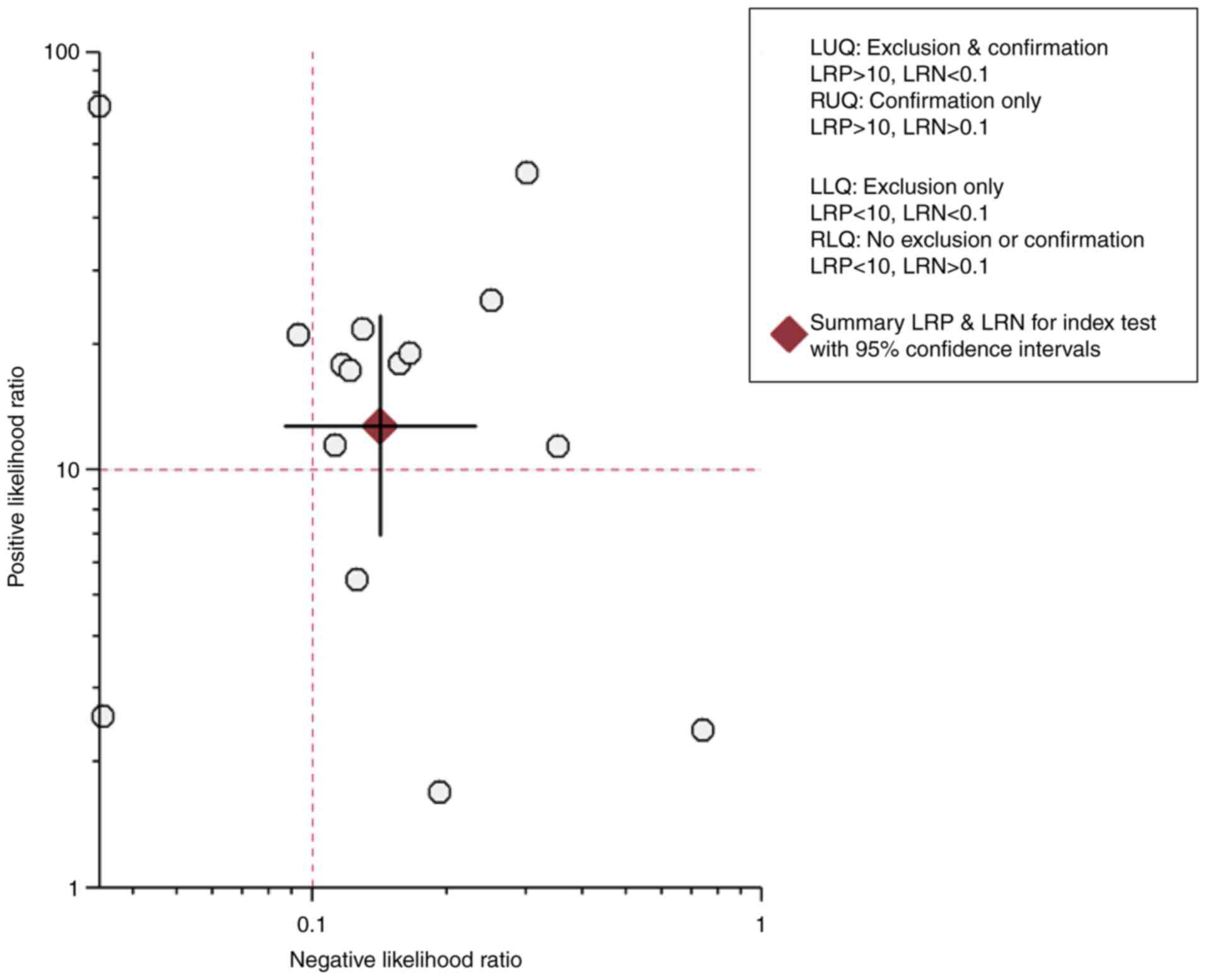
3). The DOR was 97 (95% CI: 65-147). The LRP was 8.3 (95% CI:
6.1-11.3) and the LRN was 0.09 (0.06-0.12). The upper right
quadrant in the LR scatter diagram was occupied by these values,
indicating that the TVUS may be used for confirmation only
(Fig. 4). The AUC was 0.96 (95% CI:
0.84-1.00) (Fig. 5), indicating a
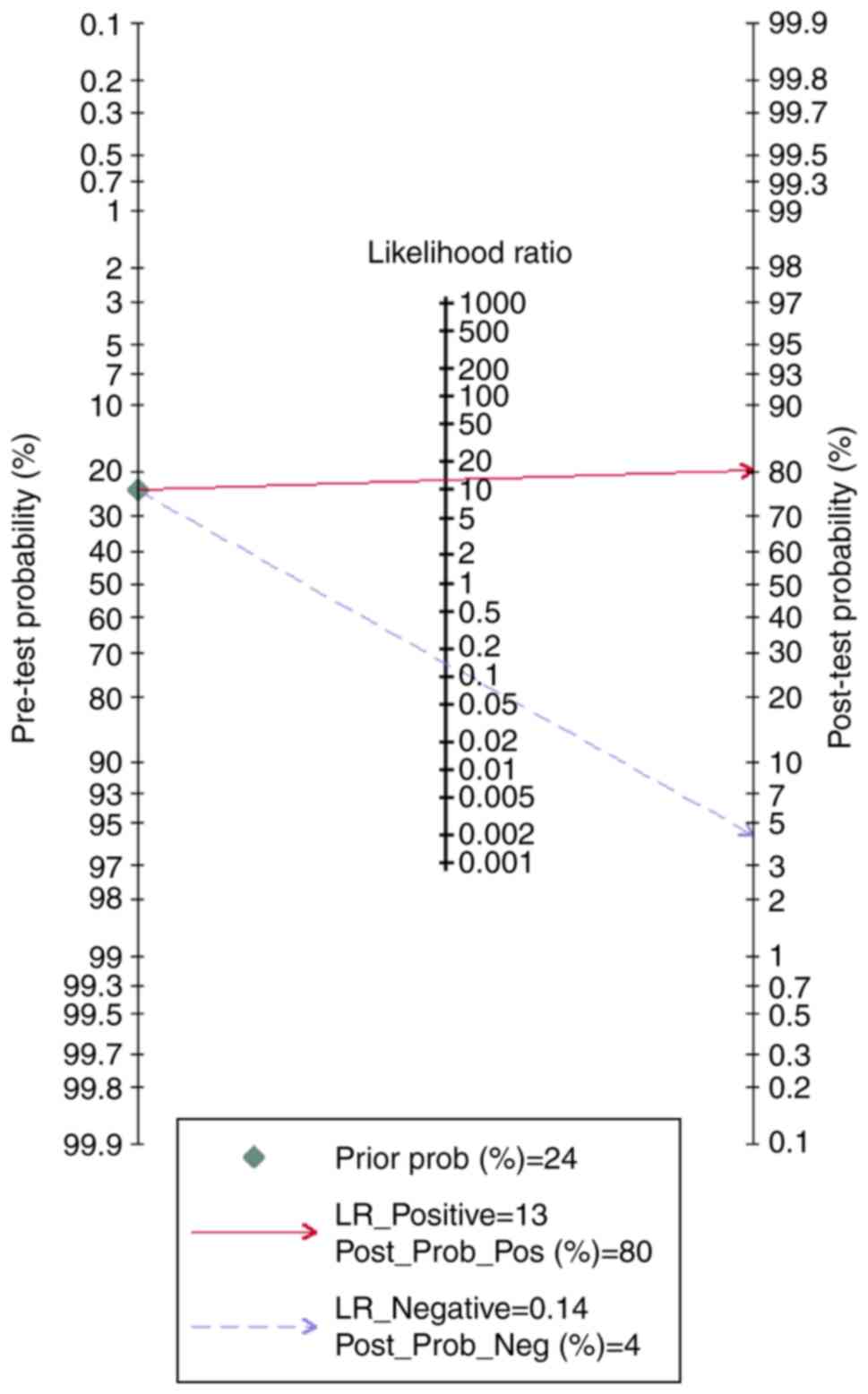
highdiagnostic value. TVUS for adnexal mass had a good clinical
value, as Fagan's nomogram had a significantly different post-test
probability (positive, 80%; negative, 4%) compared to the pre-test
probability (28%) (Fig. 6).
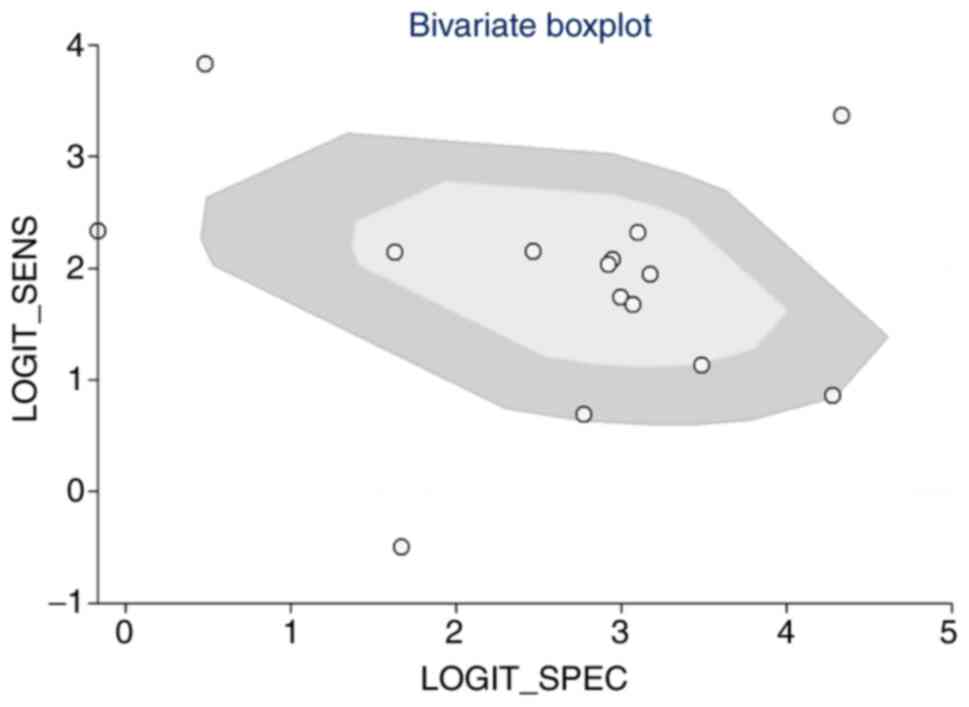
There was considerable heterogeneity with a
statistically significant chi-square test result (P<0.001) and
an I2 value of 99%. As indicated in the bivariate box
plot (Fig. 7), 4 studies were
outside the circle, demonstrating a possibility of inter-study
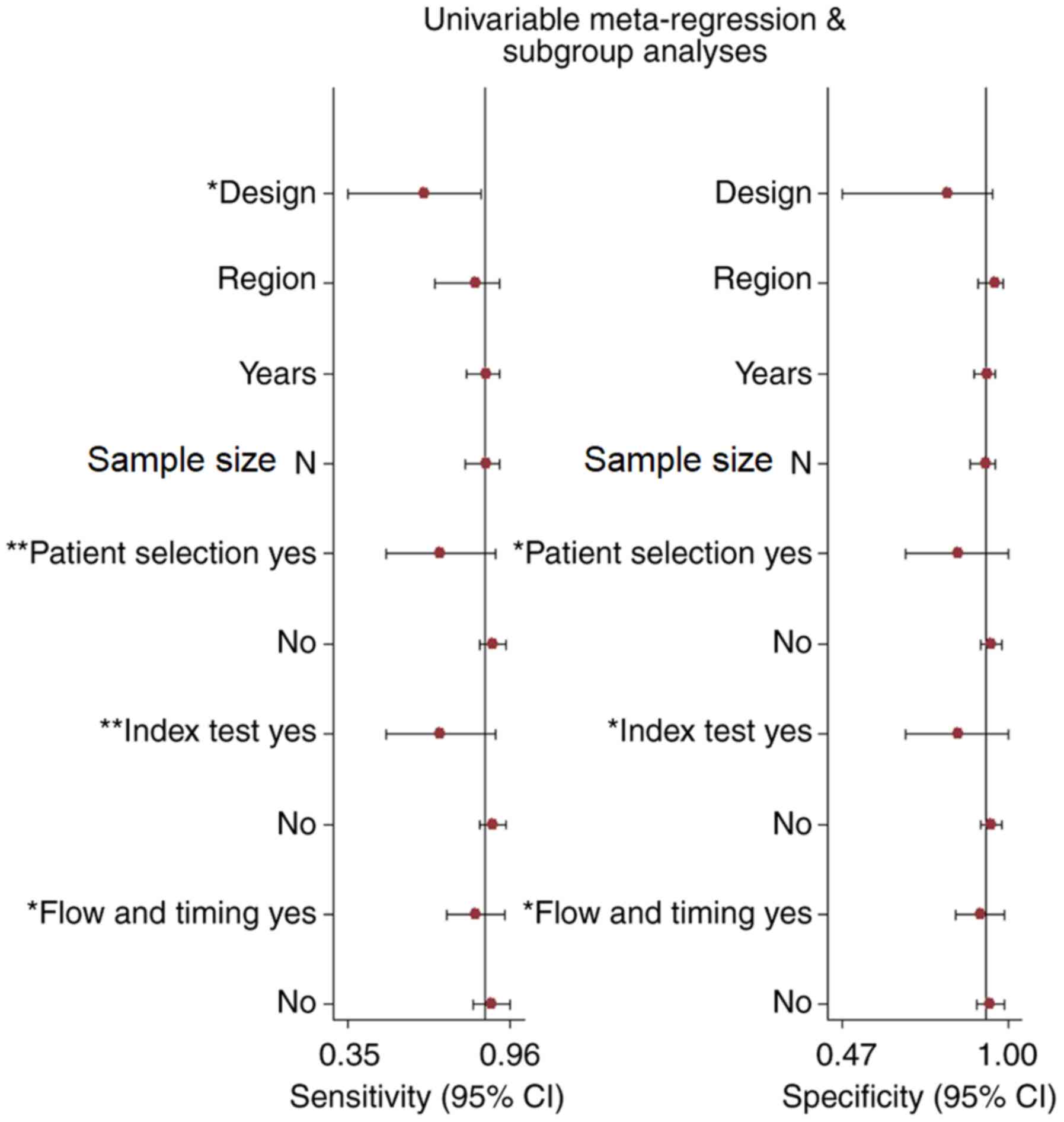
heterogeneity. Meta-regression for assessing the source of
heterogeneity suggested that the selection domain, standards of
index test conduct and study design were statistically significant
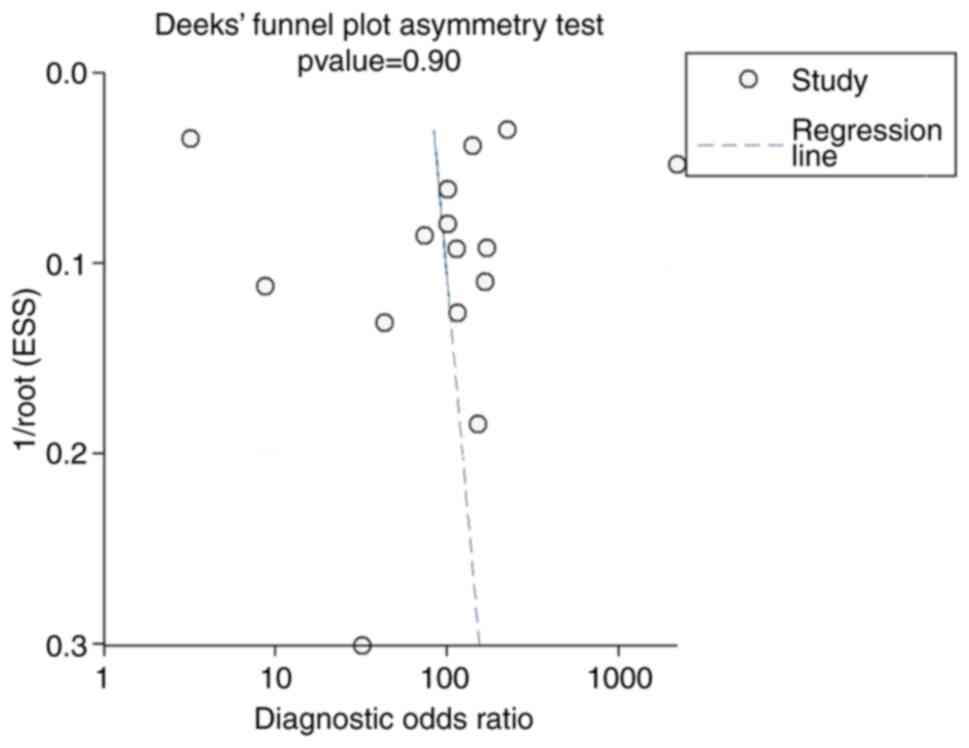
sources of heterogeneity (P<0.05; Fig. 8). The funnel plot for assessing the
publication bias was symmetrical and the low publication bias was
confirmed by non-significant Deek's test (P=0.90 Fig. 9).
Discussion
Several imaging modalities are available for making
a specific diagnosis among patients with adnexal mass (50). However, these modalities cannot
replace histopathology or biopsy as the gold standard for
diagnosis. Imaging modalities still have a major role in clinical
practice as these are non-invasive and are able to significantly
reduce the diagnostic delay and complications associated with
invasive diagnostic techniques (51). Since TVUS is a widely used imaging
tool for adnexal masses, it is important to evaluate the diagnostic
accuracy of this modality in differentiating between benign and
malignant adnexal mass.
In total, 41 studies with 18,391 participants met
the eligibility criteria of the review. The majority of the
included studies were prospective studies. Most of them were
performed in high-income countries such as the United Kingdom, the
USA, Italy and Sweden. The overall quality of evidence was high, as
most of the studies had a low risk of bias for all of the four
domains of the QUADAS tool.
The diagnostic accuracy of TVUS for differentiating
benign and malignant adnexal masses has not been evaluated in any
previous reviews, to the best of our knowledge. In the present
first meta-analysis, the pooled estimate of the sensitivity of TVUS
was 92% and the pooled specificity was 89% with a high diagnostic
performance (AUC=0.96). This diagnostic accuracy almost reached
that of other biomarkers and algorithms such as CA-125, human
epididymis protein 4, Risk of Malignancy Index and the Risk of
Ovarian Malignancy Algorithm (52-56).
In the LR scatter diagram, LRP and LRN occupied the
left lower quadrant, indicating that the TVUS should be used as the
test for confirmation only and not for exclusion. The clinical
value of TVUS for adnexal mass was also good, as Fagan's nomogram
indicated a significant increase in the post-test probability
compared to the pre-test probability. However, while inferring
these results, one must consider the quality and differences in
methodology of the included studies, which may have influenced the
study results. Hence, an analysis of inter-study heterogeneity
amongst the included studies was also performed. The present
analysis indicated significant inter-study heterogeneity with a
significant chi-square test result and I2 statistic. On
further exploration of the source of heterogeneity via
meta-regression, it was indicated that the study design,
publication year and quality-associated characteristics had a
significant influence on the inter-study variability. Deek's test
and the funnel plot indicated that there was no significant
publication bias among the studies reporting on the diagnostic
accuracy of TVUS.
The present study has the following strengths. A
comprehensive review was performed by including 41 studies with
18,391 patients to evaluate the diagnostic accuracy of TVUS in
differentiating adnexal masses. To the best of our knowledge, the
present study was the first to provide pooled estimates for the
specific diagnosis of adnexal mass using TVUS. Furthermore,
publication bias was determined to be insignificant, which adds
credibility to the results obtained in the present review. However,
the present study also has certain limitations. First, certain
studies had a high risk of bias, which may have influenced the
pooled estimates. Furthermore, there was significant inter-study
heterogeneity in the review. This limits the study's ability to
interpret the pooled results. However, it was attempted to overcome
this limitation by exploring the potential source of heterogeneity
among the included studies by a meta-regression analysis.
Despite these limitations, the present study
provided valuable insight regarding the diagnostic accuracy of
non-invasive techniques for differentiating benign and malignant
adnexal masses. While TVUS had good sensitivity and specificity, it
can only almost reach the SnNout triage test criteria for
sensitivity. It cannot meet the SpPin criteria for the specificity
of a diagnostic test (57). This
means that TVUS can rule out a adnexal mass to be free from
malignancy but cannot differentiate benign and malignant with
utmost certainty based on radiological evidence. These results are
in line with the international guidelines for the diagnosis of
adnexal masses, which suggests TVUS as a first-line imaging
modality to rule out malignancies such as ovarian cancer (6). However, it is not a replacement for
laparoscopic surgery and biopsy, which is still the gold standard
for the differentiation of adnexal masses.
In conclusion, the present study indicated that TVUS
may be a useful imaging modality for differentiating between benign
and malignant tumour among patients with adnexal mass with high
sensitivity and specificity. TVUS may be employed as an efficient
and rapid screening tool for suspected adnexal masses to rule out
malignancy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XZ designed the study. XZ, XM, TD and HS were
involved in literature search and data interpretation. XM and TD
were responsible for the data analysis. XZ prepared the manuscript.
HS edited the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Griffin N, Grant LA and Sala E: Adnexal
masses: Characterization and imaging strategies. Semin Ultrasound
CT MR. 31:330–346. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Givens V, Mitchell GE, Harraway-Smith C,
Reddy A and Maness DL: Diagnosis and management of adnexal masses.
Am Fam Physician. 80:815–820. 2009.PubMed/NCBI
|
|
3
|
Hakoun AM, AbouAl-Shaar I, Zaza KJ,
Abou-Al-Shaar H and A Salloum MN: Adnexal masses in pregnancy: An
updated review. Avicenna J Med. 7:153–157. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Fischerova D, Zikan M, Dundr P and Cibula
D: Diagnosis, treatment, and follow-up of borderline ovarian
tumors. Oncologist. 17:1515–1533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Curtin JP: Management of the adnexal mass.
Gynecol Oncol. 55:S42–S46. 1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
American College of Obstetricians and
Gynecologists: ACOG practice bulletin. Management of adnexal
masses. Obstet Gynecol 110: 201-214, 2007.
|
|
7
|
Coleman BG: Transvaginal sonography of
adnexal masses. Radiol Clin North Am. 30:677–691. 1992.PubMed/NCBI
|
|
8
|
Whiting PF, Rutjes AWS, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA and Bossuyt
PM: QUADAS-2 Group: QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Alcázar JL, Pascual MÁ, Olartecoechea B,
Graupera B, Aubá M, Ajossa S, Hereter L, Julve R, Gastón B, Peddes
C, et al: IOTA simple rules for discriminating between benign and
malignant adnexal masses: Prospective external validation.
Ultrasound Obstetr Gynecol. 42:467–471. 2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Daemen A, Valentin L, Fruscio R, Van
Holsbeke C, Melis GB, Guerriero S, Czekierdowski A, Jurkovic D,
Ombelet W, Rossi A, et al: Improving the preoperative
classification of adnexal masses as benign or malignant by
second-stage tests. Ultrasound Obstet Gynecol. 37:100–106.
2011.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Ruiz de Gauna B, Rodriguez D,
Olartecoechea B, Aubá M, Jurado M, Gómez Roig MD and Alcázar JL:
Diagnostic performance of IOTA simple rules for adnexal masses
classification: A comparison between two centers with different
ovarian cancer prevalence. Eur J Obstet Gynecol Reprod Biol.
191:10–14. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Fathallah K, Huchon C, Bats AS, Metzger U,
Lefrère-Belda MA, Bensaid C and Lécuru F: External validation of
simple ultrasound rules of Timmerman on 122 ovarian tumors. Gynecol
Obstet Fertil. 39:477–481. 2011.(In French). PubMed/NCBI View Article : Google Scholar
|
|
13
|
Granberg S, Norström A and Wikland M:
Tumors in the lower pelvis as imaged by vaginal sonography. Gynecol
Oncol. 37:224–229. 1990.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Guerriero S, Alcazar JL, Ajossa S, Galvan
R, Laparte C, García-Manero M, Lopez-Garcia G and Melis GB:
Transvaginal color Doppler imaging in the detection of ovarian
cancer in a large study population. Int J Gynecol Cancer.
20:781–786. 2010.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Hartman CA, Juliato CRT, Sarian LO, Toledo
MC, Jales RM, Morais SS, Pitta DD, Marussi EF and Derchain S:
Ultrasound criteria and CA 125 as predictive variables of ovarian
cancer in women with adnexal tumors. Ultrasound Obstet Gynecol.
40:360–366. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Jain KA, Friedman DL, Pettinger TW,
Alagappan R, Jeffrey RB Jr and Sommer FG: Adnexal masses:
Comparison of specificity of endovaginal US and pelvic MR imaging.
Radiology. 186:697–704. 1993.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jain KA: Prospective evaluation of adnexal
masses with endovaginal gray-scale and duplex and color Doppler US:
Correlation with pathologic findings. Radiology. 191:63–67.
1994.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Knafel A, Nocun A, Banas T, Wiechec M,
Jach R, Pietrus M and Pitynski K: IOTA simple ultrasound-based
rules; why do we inconclusive results? Int J Gynecol Cancer.
2013(8)2013.
|
|
19
|
Komatsu T, Konishi I, Mandai M, Togashi K,
Kawakami S, Konishi J and Mori T: Adnexal masses: Transvaginal US
and gadolinium-enhanced MR imaging assessment of intratumoral
structure. Radiology. 198:109–115. 1996.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lucidarme O, Akakpo JP, Granberg S, Sideri
M, Levavi H, Schneider A, Autier P, Nir D and Bleiberg H: Ovarian
HistoScanning Clinical Study Group: A new computer-aided diagnostic
tool for non-invasive characterisation of malignant ovarian masses:
Results of a multicentre validation study. Eur Radiol.
20:1822–1830. 2010.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mancuso A, De Vivo A, Triolo O and Irato
S: The role of transvaginal ultrasonography and serum CA 125 assay
combined with age and hormonal state in the differential diagnosis
of pelvic masses. Eur J Gynaecol Oncol. 25:207–210. 2004.PubMed/NCBI
|
|
22
|
Moszynski R, Szpurek D, Szubert S and
Sajdak S: Analysis of false negative results of subjective
ultrasonography assessment of adnexal masses. Ginekol Pol.
84:102–107. 2013.PubMed/NCBI View
Article : Google Scholar
|
|
23
|
Nunes N, Yazbek J, Ambler G, Hoo W,
Naftalin J and Jurkovic D: Prospective evaluation of the IOTA
logistic regression model LR2 for the diagnosis of ovarian cancer.
Ultrasound Obstet Gynecol. 40:355–359. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Nunes N, Ambler G, Hoo WL, Naftalin J, Foo
X, Widschwendter M and Jurkovic D: A prospective validation of the
IOTA logistic regression models (LR1 and LR2) in comparison to
subjective pattern recognition for the diagnosis of ovarian cancer.
Int J Gynecol Cancer. 23:1583–1589. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Radosa MP, Vorwergk J, Fitzgerald J,
Kaehler C, Schneider U, Camara O, Runnebaum IB and Schleußner E:
Sonographic discrimination between benign and malignant adnexal
masses in premenopause. Ultraschall Med. 35:339–344.
2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Romagnolo C, Trivella G, Bonacina M,
Fornalè M, Maggino T and Ferrazzi E: Preoperative diagnosis of 221
consecutive ovarian masses: Scoring system and expert evaluation.
Eur J Gynaecol Oncol. 27:487–489. 2006.PubMed/NCBI
|
|
27
|
Roman LD, Muderspach LI, Stein SM,
Laifer-Narin S, Groshen S and Morrow CP: Pelvic examination, tumor
marker level, and gray-scale and Doppler sonography in the
prediction of pelvic cancer. Obstet Gynecol. 89:493–500.
1997.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Salle B, Gaucherand P, Ecochard R and
Rudigoz RC: Role of pulsed color Doppler in the presurgical
evaluation of pelvic masses. J Gynecol Obstet Biol Reprod (Paris).
24:234–240. 1995.(In French). PubMed/NCBI
|
|
29
|
Sayasneh A, Wynants L, Preisler J, Kaijser
J, Johnson S, Stalder C, Husicka R, Abdallah Y, Raslan F, Drought
A, et al: Multicentre external validation of IOTA prediction models
and RMI by operators with varied training. Br J Cancer.
108:2448–2454. 2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sayasneh A, Kaijser J, Preisler J, Smith
AA, Raslan F, Johnson S, Husicka R, Ferrara L, Stalder C,
Ghaem-Maghami S, et al: Accuracy of ultrasonography performed by
examiners with varied training and experience in predicting
specific pathology of adnexal masses. Ultrasound Obstet Gynecol.
45:605–612. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Shetty J, Reddy G and Pandey D: Role of
sonographic gray-scale pattern recognition in the diagnosis of
adnexal masses. J Clin Diagn Res. 11:QC12–QC15. 2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Shetty J, Saradha A, Pandey D, Bhat R,
Pratap K and Bharatnur S: IOTA simple ultrasound rules for triage
of adnexal mass: Experience from South India. J Obstet Gynecol
India. 69:356–362. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Silvestre L, Martins WP and
Candido-dos-Reis FJ: Limitations of three-dimensional power Doppler
angiography in preoperative evaluation of ovarian tumors. J Ovarian
Res. 8(47)2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sohaib SA, Mills TD, Sahdev A, Webb JA,
Vantrappen PO, Jacobs IJ and Reznek RH: The role of magnetic
resonance imaging and ultrasound in patients with adnexal masses.
Clin Radiol. 60:340–348. 2005.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Sokalska A, Timmerman D, Testa AC, Van
Holsbeke C, Lissoni AA, Leone FP, Jurkovic D and Valentin L:
Diagnostic accuracy of transvaginal ultrasound examination for
assigning a specific diagnosis to adnexal masses. Ultrasound Obstet
Gynecol. 34:462–470. 2009.PubMed/NCBI View
Article : Google Scholar
|
|
36
|
Stein SM, Laifer-Narin S, Johnson MB,
Roman LD, Muderspach LI, Tyszka JM and Ralls PW: Differentiation of
benign and malignant adnexal masses: Relative value of gray-scale,
color Doppler, and spectral Doppler sonography. AJR Am J
Roentgenol. 164:381–386. 1995.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Strigini FA, Gadducci A, Del Bravo B,
Ferdeghini M and Genazzani AR: Differential diagnosis of adnexal
masses with transvaginal sonography, color flow imaging, and serum
CA 125 assay in pre- and postmenopausal women. Gynecol Oncol.
61:68–72. 1996.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Tantipalakorn C, Wanapirak C,
Khunamornpong S, Sukpan K and Tongsong T: IOTA simple rules in
differentiating between benign and malignant ovarian tumors. Asian
Pac J Cancer Prev. 15:5123–5126. 2014.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Testa A, Kaijser J, Wynants L, Fischerova
D, Van Holsbeke C, Franchi D, Savelli L, Epstein E, Czekierdowski
A, Guerriero S, et al: Strategies to diagnose ovarian cancer: New
evidence from phase 3 of the multicentre international IOTA study.
Br J Cancer. 111:680–688. 2014.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Timmerman D, Verrelst H, Bourne TH, De
Moor B, Collins WP, Vergote I and Vandewalle J: Artificial neural
network models for the preoperative discrimination between
malignant and benign adnexal masses. Ultrasound Obstet Gynecol.
13:17–25. 1999.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Timmerman D, Ameye L, Fischerova D,
Epstein E, Melis GB, Guerriero S, Van Holsbeke C, Savelli L,
Fruscio R, Lissoni AA, et al: Simple ultrasound rules to
distinguish between benign and malignant adnexal masses before
surgery: Prospective validation by IOTA group. BMJ.
341(c6839)2010.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Utrilla-Layna J, Alcázar JL, Aubá M,
Laparte C, Olartecoechea B, Errasti T, Juez L, Mínguez JÁ,
Guerriero S and Jurado M: Performance of three-dimensional power
Doppler angiography as third-step assessment in differential
diagnosis of adnexal masses. Ultrasound Obstet Gynecol. 45:613–617.
2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Valentin L: Prospective cross-validation
of Doppler ultrasound examination and gray-scale ultrasound imaging
for discrimination of benign and malignant pelvic masses.
Ultrasound Obstet Gynecol. 14:273–283. 1999.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Valentin L, Jurkovic D, Van Calster B,
Testa A, Van Holsbeke C, Bourne T, Vergote I, Van Huffel S and
Timmerman D: Adding a single CA 125 measurement to ultrasound
imaging performed by an experienced examiner does not improve
preoperative discrimination between benign and malignant adnexal
masses. Ultrasound Obstet Gynecol. 34:345–354. 2009.PubMed/NCBI View
Article : Google Scholar
|
|
45
|
Van Calster B, Timmerman D, Bourne T,
Testa AC, Van Holsbeke C, Domali E, Jurkovic D, Neven P, Van Huffel
S and Valentin L: Discrimination between benign and malignant
adnexal masses by specialist ultrasound examination versus serum
CA-125. J Natl Cancer Inst. 99:1706–1714. 2007.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Van Gorp T, Veldman J, Van Calster B,
Cadron I, Leunen K, Amant F, Timmerman D and Vergote I: Subjective
assessment by ultrasound is superior to the risk of malignancy
index (RMI) or the risk of ovarian malignancy algorithm (ROMA) in
discriminating benign from malignant adnexal masses. Eur J Cancer.
48:1649–1656. 2012.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Van Holsbeke C, Van Calster B, Testa AC,
Testa AC, Domali E, Lu C, Van Huffel S, Valentin L and Timmerman D:
Prospective internal validation of mathematical models to predict
malignancy in adnexal masses: Results from the international
ovarian tumor analysis study. Clin Cancer Res. 15:684–691.
2009.PubMed/NCBI View Article : Google Scholar
|
|
48
|
van Trappen PO, Rufford BD, Mills TD,
Sohaib SA, Webb JA, Sahdev A, Carroll MJ, Britton KE, Reznek RH and
Jacobs IJ: Differential diagnosis of adnexal masses: Risk of
malignancy index, ultrasonography, magnetic resonance imaging, and
radioimmunoscintigraphy. Int J Gynecol Cancer. 17:61–67.
2007.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Yamashita Y, Torashima M, Hatanaka Y,
Harada M, Higashida Y, Takahashi M, Mizutani H, Tashiro H, Iwamasa
J, Miyazaki K, et al: Adnexal masses: Accuracy of characterization
with transvaginal US and precontrast and postcontrast MR imaging.
Radiology. 194:557–565. 1995.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Karnik A, Tembey RA and Mani S: Value of
MRI in characterizing adnexal masses. J Obstet Gynaecol India.
65:259–266. 2015.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Kaijser J, Vandecaveye V, Deroose CM,
Rockall A, Thomassin-Naggara I, Bourne T and Timmerman D: Imaging
techniques for the pre-surgical diagnosis of adnexal tumours. Best
Pract Res Clin Obstet Gynaecol. 28:683–695. 2014.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Dochez V, Caillon H, Vaucel E, Dimet J,
Winer N and Ducarme G: Biomarkers and algorithms for diagnosis of
ovarian cancer: CA125, HE4, RMI and ROMA, a review. J Ovarian Res.
12(28)2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Ferraro S, Braga F, Lanzoni M, Boracchi P,
Biganzoli EM and Panteghini M: Serum human epididymis protein 4 vs
carbohydrate antigen 125 for ovarian cancer diagnosis: A systematic
review. J Clin Pathol. 66:273–281. 2013.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Wang J, Gao J, Yao H, Wu Z, Wang M and Qi
J: Diagnostic accuracy of serum HE4, CA125 and ROMA in patients
with ovarian cancer: A meta-analysis. Tumour Biol. 35:6127–6138.
2014.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Zhen S, Bian LH, Chang LL and Gao X:
Comparison of serum human epididymis protein 4 and carbohydrate
antigen 125 as markers in ovarian cancer: A meta-analysis. Mol Clin
Oncol. 2:559–566. 2014.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Li F, Tie R, Chang K, Wang F, Deng S, Lu
W, Yu L and Chen M: Does risk for ovarian malignancy algorithm
excel human epididymis protein 4 and CA125 in predicting epithelial
ovarian cancer: A meta-analysis. BMC Cancer. 12(258)2012.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Pewsner D, Battaglia M, Minder C, Marx A,
Bucher HC and Egger M: Ruling a diagnosis in or out with ‘SpPIn’
and ‘SnNOut’: A note of caution. BMJ. 329:209–213. 2004.PubMed/NCBI View Article : Google Scholar
|