1. Introduction
Following the emergence of severe acute respiratory
syndrome (SARS) coronavirus (SARS-CoV) in 2003 and Middle East
respiratory syndrome coronavirus (MERS-CoV) in 2012, a novel
coronavirus pneumonia epidemic, named COVID-19 by the World Health
Organization (WHO) (1), resulted
from SARS-CoV-2 infection in Wuhan, China, and was identified in
late December 2019(2).
Subsequently, this disease spread rapidly to all parts of the
world. As the number of patients with SARS-CoV-2 infection
increased globally, the WHO declared COVID-19 a pandemic on 12th
March 2020(3). To date >37
million people have contracted this disease and as of 10th October
2020, the death toll stands at >1,070,355(4).
SARS-CoV-2 is a member of the nested viroid family
cornonaviridae and the coronavirus genus. It is the 7th
coronavirus known to infect humans and the third coronavirus known
to be transmitted from animal to animal, animal to human and human
to human (5,6). COVID-19 has been suggested to be a
disease of the nicotinic cholinergic system (7) and SARS-CoV-2 most commonly causes a
lower respiratory infection or pneumonia (8). High levels of mortality are noticed in
elderly individuals infected with SARS-CoV-2, with the risk of
death in individuals aged <65 years 15 to 100 fold lower
compared with that in older individuals in developed countries,
including Germany, Canada, France, Italy and the USA (9). Oxidative stress and inflammatory
cytokine production in elderly individuals cause a chronic low
level of inflammation and increase the severity of viral infections
(10). In view of the adverse
consequences of the current COVID-19 epidemic, it is necessary to
develop effective treatment strategies to deal with the lack of
effective drugs, high mortality and the possibility of further
epidemics caused by the virus. The present manuscript describes the
situation, clinical characteristics and current detection and
treatment methods for SARS-CoV-2 infection and discusses the
developing strategies for the treatment of COVID-19.
2. Virology
The first strain of SARS-CoV-2 was isolated from
Wuhan, China on 24th January 2020 after the outbreak of
COVID-19(11). In similarity to
other coronaviruses, SARS-CoV-2 consists of four structural
proteins, namely the spike (S), envelope, membrane/matrix (M) and
nucleocapsid proteins (12).
Non-structural proteins are produced after RNA genome expression in
the host cell during formation of new virus particles (12). On the surface of mature coronavirus,
the S protein usually forms a crown-like trimer, an important
morphological feature which differentiates coronaviruses from other
viruses (11). Similarly,
SARS-CoV-2 viruses isolated in South Korea have also been
identified by typical corona-like structure formed by the S protein
(13).
Based on phylogenetic analysis [Global Initiative on
Sharing All Influenza Data (GISAID) accession no. EPI_ISL_402124]
(14), SARS-CoV-2 is a lineage B
betacoronavirus and shares high sequence identity with SARS-CoV and
the bat SARS-like coronavirus (SL-CoV) (15). Like MERS-CoV and SARS-CoV,
SARS-CoV-2 is a positive-sense single-stranded RNA virus and shows
a similar pattern of infection (16). Using full-length genome sequencing,
SARS-CoV-2 and a bat coronavirus BatCoV RaTG13 were found to be 96%
identical (14), suggesting an
origin of the SARS-CoV-2 infection in bats. Comprehensive sequence
analysis with relative synonymous codon usage bias demonstrated
that SARS-CoV-2 may be derived from recombination between a bat
coronavirus and another coronavirus from snakes (17). Additionally, mink have been
suggested as a potential host of SARS-CoV-2(18). Interspecies transmissions of viruses
between animals and humans may result in unpredictable pathogenic
potential and transmissible COVID-19 disease (19).
3. Epidemiology
A cluster of patients with atypical pneumonia was
reported in Wuhan, China on December 31, 2019(20). During the subsequent 6 weeks,
several cases were reported in more than 37 countries, including
the USA, Japan, Iran and South Korea (1). The infection rapidly spread across the
globe, threatening global public health. Chinese authorities
locked-down Wuhan city and suspended transport to and from Wuhan to
control the spread (21). Imposing
mobility restrictions as fast as possible is thought to be an
effective way to avoid an outbreak (22). Numerous patients were diagnosed and
treated, and the epidemic situation in China has been gradually
controlled (23). Various countries
have instituted measures, such as practicing good hygiene (washing
hands), wearing a mask and quarantine (24). Meanwhile, understanding of the
epidemiological characteristics of COVID-19 have developed and
immunotoxicity of chemicals and drugs and immunodeficiency caused
by the environment and lifestyle are thought to contribute to
COVID-19(24). Nevertheless,
uncertainties remain regarding both the virus-host interaction and
the evolution of the epidemic, leaving the epidemic situation
worldwide severe.
4. Mechanism of SARS-CoV-2 infection
The SARS-Cov-2 virus binds to the
angiotensin-converting enzyme 2 (ACE2) on human cells via the
receptor binding domain (RBD) located on the S1 subunit of the S
protein-homotrimer of the S protein (25). This leads to clathrin-mediated
endocytosis (26,27), release of viral RNA and induction of
viral replication. The viral genome codes for non-structural
proteins containing polyproteins, nucleoproteins, RNA polymerase,
3-chymotrypsin-like protease, papain-like protease and helicase in
the host cell in order to form new virus particles (12). The newly manufactured virus emerges
via exocytosis where it binds again to ACE2, thus entering a
vicious cycle of infecting other cells (12).
As a glycoprotein, the S protein is generally
composed of 1,160-1,400 amino acid residues and contains multiple
N-glycosylation sites, which are important for proper folding and
modulating accessibility to host proteases. The S protein exists in
a metastable prefusion conformation, where the S1 and S2 subunits
remain noncovalently bound in the prefusion conformation (28). The S1 subunit, comprising the RBD on
the surface, is responsible for recognizing and binding to the
receptor of the host cell. The S2 subunit, embedded in the
envelope, mediates membrane fusion during viral assembly (29). It has been proposed that the S
protein is activated for membrane fusion via extensive irreversible
conformational changes (30,31).
When the S1 subunit binds to a susceptible cell receptor, S1/S2
cleavage is triggered, which enables the S1 RBD to undergo
hinge-like conformational movements and the S2 subunit transits to
a highly stable post fusion conformation. This S1/S2 cleaved site
harbors several arginine residues, rendering it multibasic
(32). SARS-CoV-2 S harbors a furin
cleavage site (33), a feature
conserved among the 144 SARS-CoV-2 isolates sequenced to date, but
not found in the closely related bat virus RaTG13 S (14), at the S1/S2 boundary, which is
processed during biosynthesis. It can be hypothesized that the
almost ubiquitous expression of furin-like proteases participates
in expanding SARS-CoV-2 cell and tissue tropism, relative to
SARS-CoV, and increases viral transmissibility and/or alters its
pathogenicity.
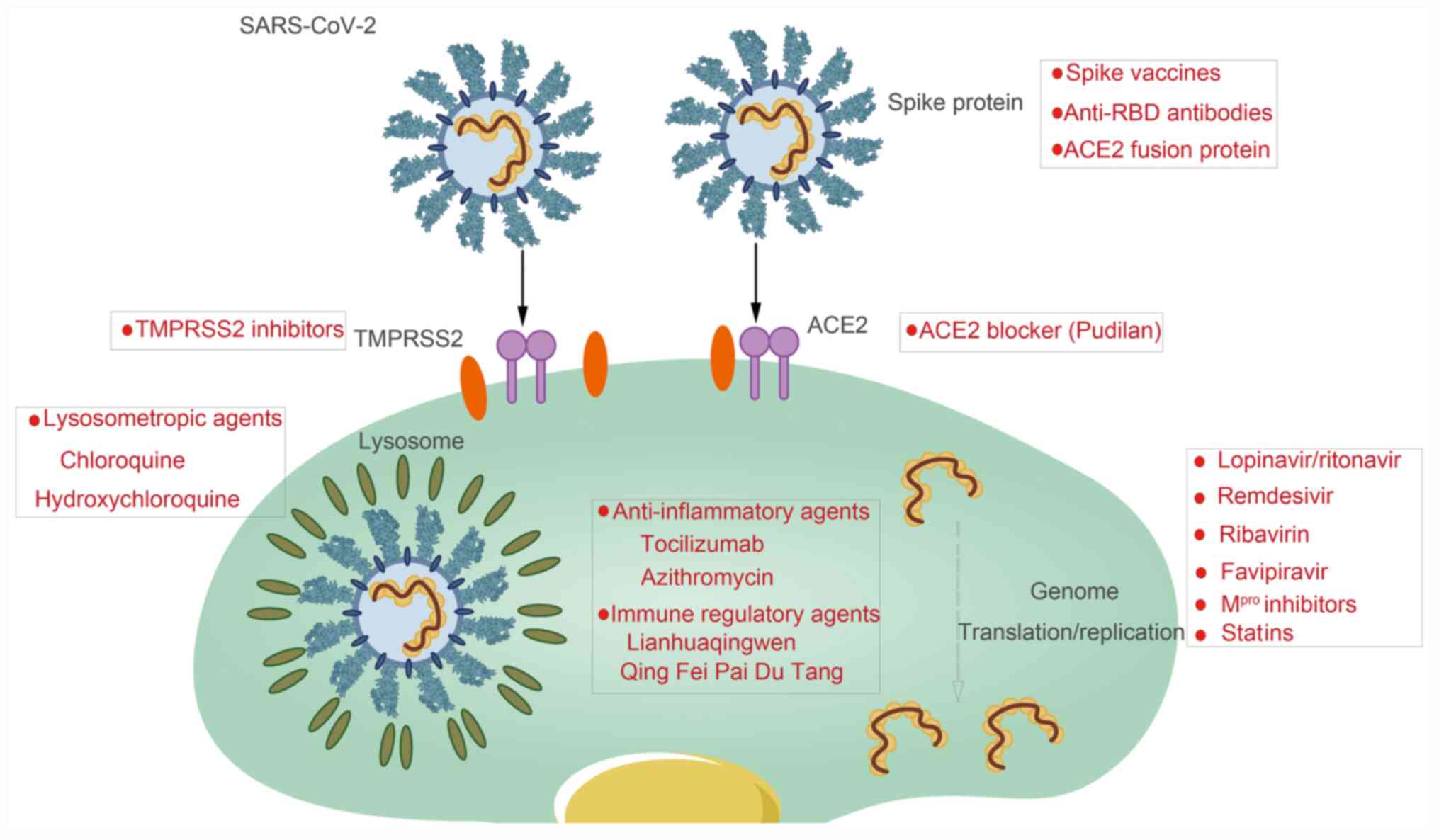
Proteases are necessary for host cell entry and
promoting virus-cell fusion (32,34).
When SARS-CoV-2 targets host cells (13), the serine protease transmembrane
protease serine 2 (TMPRSS2) is employed for S protein priming
(Fig. 1) (12,32,35).
Notably, all ACE2-expressing pulmonary cells are also
TMPRSS2-positive (35).
Similarly to SARS-CoV infection, the S protein of
SARS-CoV-2 binds to the human ACE2 receptor, which partially
explains the efficient transmission of SARS-CoV-2 in humans
(34). The binding ability of
SARS-CoV-2 S protein to ACE2 is stronger than that of SARS-CoV
(36), which may explain why
SARS-CoV-2 is more transmissible than SARS-CoV. The expression
level and tissue distribution of ACE2 determine the cell tropism
and pathogenicity of SARS-CoV-2(37). Coronavirus infection and the induced
cytokine storm are able to enhance the expression of ACE2 in host
cells, further accelerating infection and transmission of the virus
(38). The expression of ACE2 in
human lung cells was analyzed using single cell RNA sequencing
analysis technology and the results indicated that the expression
of ACE2 was concentrated in a small group of type II alveolar
epithelial cells in the lung (37),
suggesting that these cells may be the target of SARS-CoV-2. Recent
studies have also indicated that ACE2 is highly expressed not only
in lung cells, esophageal epithelium and stratified epithelial
cells, but also in the absorbing intestinal epithelial cells of the
ileum and colon (39), suggesting
that the digestive system is also a potential pathway for
SARS-CoV-2 infection.
5. Clinical manifestations and
diagnosis
Clinical manifestations
The most frequent clinical feature in patients
infected with SARS-CoV-2 appears to be pneumonia. Early COVID-19 is
characterized primarily by the symptoms of fever, myalgia, cough
and sore throat, all of which are common in other acute respiratory
virus infections (8). Most cases
appear to be mild, and most hospitalized patients have pneumonia
with bilateral infiltration upon chest imaging (8,40).
Notably, the period from infection to the appearance of symptoms
varies in patients with SARS-CoV-2 infection, and there are also
great differences in symptoms among individuals (41). There are patients with COVID-19 with
no detectable fever or other clinical symptoms (5).
SARS-CoV-2 is believed to be transmitted through
large respiratory droplets and close contact. Positive reverse
transcription (RT-PCR) results from stool specimens from patients
with COVID-19 suggested that stool or sewage might serve as another
vehicle for viral transmission (42).
PCR detection
Currently, the preferred method for detection of
COVID-19 is via molecular testing. Multiple specimen types are
recommended due to the unknown sensitivity and specificity of
tests. The PCR detection method was designed to detect a variety of
targets in SARS-CoV-2 genome and is the most widely used molecular
diagnostic method to analyze samples such as sputum, nasal swab,
pharyngeal swab, bronchoalveolar lavage and blood plasma (43,44). A
significant portion of suspected patients who have tested negative
for viral RNA indeed fit the diagnosis based on clinical and chest
CT findings (45). PCR detection
involves RNA extraction and preservation, and the degradation and
contamination of RNA samples could result in missed detection or
false positive results (46).
Moreover, the time, manpower and economic (advanced PCR equipment
and expensive reagents) costs are such that it is difficult to meet
the huge testing demand in the rapid outbreak of COVID-19(45).
Serological tests
Serological testing is method that is considered, at
the present time, as complementary to nucleic acid detection
(47). IgM testing has been
designed and validated, but currently limited information is
available about the performance of these tests (48). Some tests may produce inaccurate
results (49), suggesting gold
immunochromatography assay and ELISA methods should be used to
eliminate or reduce the impact of cross-reaction. Serological
testing is helpful for preliminary screening of suspected and
high-risk groups (50).
Previously, numerous methods for rapid detection and
diagnosis of coronavirus infection based on the S protein have been
developed. Thachil et al (51) established an indirect ELISA with the
S1 subunit of the S protein of porcine delta coronavirus as the
coating antigen, with a sensitivity of 91% and specificity of 95%
that was able to detect the specific IgG specific antibody against
porcine delta coronavirus in serum samples. Zhao et al
(52) established a set of ELISA
detection methods for antibodies against the S1 subunit of horse
coronavirus, which effectively diagnoses infection. Moreover,
Sunwoo et al (53) developed
a bispecific monoclonal antibody against the S1 antigen on the
surface of SARS-CoV, which can be used in clinical diagnosis of
suspected SARS patients. Since the S protein is the most important
antigenic determinant for coronavirus (54), ELISA methods based on the S protein
antigen-antibody reaction could be effective. Additionally, ELISA
detection is much faster and easier in comparison with PCR
detection (46). Therefore,
developing an effective ELISA kit for SARS-CoV-2 detection would be
helpful in the current epidemic.
6. Treatment
Overview
Numerous compounds have been proven effective
against SARS-CoV and MERS-CoV which have not been tested widely for
the newly emerged SARS-CoV-2. At present, drugs that inhibit the
process of virus replication, assembly and fusion with host cells
are under research.
Lopinavir/ritonavir
Lopinavir/ritonavir, protease inhibitors that have
been widely used for the treatment of human immunodeficiency
virus-1 infection (55), are
usually used in combination with azithromycin to increase the
half-life of lopinavir by inhibiting cytochrome P450. A previous
study suggested that patients with SARS treated with a combination
of lopinavir/ritonavir and ribavirin had lower risk of developing
acute respiratory distress syndrome or death (56). The combination of
lopinavir/ritonavir and interferon-β improved outcomes in MERS-CoV
infection (57). However, the
lopinavir/ritonavir combination provided little benefit in
improving the clinical outcomes in patients with mild and moderate
COVID-19(58). There were no
benefits of lopinavir/ritonavir beyond the standard treatment in a
trial performed on patients with severe COVID-19 in China, but a
slightly lower number of deaths was observed in the group receiving
lopinavir/ritonavir in the late stage of SARS-CoV-2 infection
compared with the standard-treatment group (59).
Remdesivir
As a new nucleoside analogue (60,61),
remdesivir has a broad-spectrum antiviral capacity against
filoviruses, paramyxoviruses, pneumoviruses, and human and bat
derived coronaviruses (62-65),
which makes it a promising agent for COVID-19 treatment. Against
the Ebola virus, remdesivir has completed the phase I clinical
trial, and the pharmacokinetics and safety in the human body have
relatively complete data (66). A
study reported that the replication of virus in human primary cell
was significantly inhibited (67,68),
because the triphosphate cannot be removed by non-structural
protein 14 N-terminal exoribonuclease (69). Remdesivir effectively reduced the
virus titer in the lungs of rhesus macaques infected with MERS-CoV
and it improved the degree of lung tissue damage in comparison with
that of the control group (70).
New England Journal of Medicine recently published a case of
SARS-CoV-2 infection in the United States treated with remdesivir
(71). A patient infected with
SARS-CoV-2 was administered remdesivir and the clinical status
improved within 24 h without any noticeable adverse effect
(71). It is worth noting that
uncertainties about adverse effects and clinical efficacy of
remdesivir have been reported recently, such as nausea, vomiting,
rectal hemorrhaging and hepatic toxicity (72).
Favipiravir
Favipiravir, which selectively and potently inhibits
RNA-dependent RNA polymerase (73-75),
has been administrated to patients infected with Ebola virus
(76) and has been approved in
Japan for influenza treatment and in China for the treatment of
COVID-19(77). Preliminary studies
on 80 patients with COVID-19 in China have demonstrated that
favipiravir exerts an antiviral action more potent than
lopinavir/ritonavir, and no serious adverse reactions have been
reported (77).
Chloroquine and
hydroxychloroquine
The antimalarial drugs chloroquine and
hydroxychloroquine are used in Korea and China for the treatment of
COVID-19 (78,79). Chloroquine presented an encouraging
anti-SARS-CoV-2 profile in early clinical trials (68,80).
Additionally, the chloroquine hydroxyl derivative
hydroxychloroquine (available as an antirheumatic drug under the
name ‘Plaquenil’) demonstrated a stronger in vitro
anti-COVID-19 effect than chloroquine (81,82). A
study found no evidence of clinical benefit of the combination of
hydroxychloroquine and azithromycin for the treatment of 11
patients with severe COVID-19(83).
However, patients with COVID-19 in France treated with
hydroxychloroquine (600 mg per day) were significant improved, even
in combination with azithromycin (84). In the wake of this evidence,
hydroxychloroquine was included in guidelines for COVID-19 therapy
in Belgium (85) and Italy
(86). Recently, chloroquine was
found not to inhibit human lung cancer cells infection with
SARS-CoV-2 although this study used human lung epithelial cells,
not the renal cell line selected in previous experiments with
TMPRSS2 protease (87). However,
chloroquine/hydroxychloroquine has an antiviral effect because
there is another enzyme, cathepsin L (catl), in renal cells that
can process the S protein of the novel coronavirus, and its
function is affected by cell pH (87). Chloroquine/hydroxychloroquine limits
the function of catl by regulating pH, thus indirectly inhibiting
the invasion of SARS-CoV-2(87).
Moreover, a study from French scientists indicated that
hydroxychloroquine cannot reduce viral load nor improve clinical
symptoms, prevent or treat COVID-19, regardless of the dosage and
timing (88). Thus, the application
of chloroquine/hydroxychloroquine requires further study.
Tocilizumab
When COVID-19 progresses from severe to critical,
patients may develop a cytokine storm immune reaction.
Consequently, the treatment of the cytokine storm is an important
part of rescuing severe patients (89). Since interleukin-6 (IL-6) is one of
the key cytokines involved in infection-induced cytokine storm, an
IL-6 receptor (IL-6R) antagonist would be a promising drug for
patients with COVID-19. Tocilizumab, a monoclonal antibody with
activity against the IL-6R was developed for the treatment of
rheumatoid arthritis (90) and has
been approved by the US FDA for the treatment of cytokine release
syndrome (91). For COVID-19, it
has been tested on 6 patients in Italy who experienced rapid
improvement in their health only 24-48 h after administration
(92). As tocilizumab blocks the
IL-6-mediated immune response in COVID-19, it was approved to treat
pneumonia and the severe cytokine release syndrome induced by the
immune system in patients with coronavirus as an ‘off label’ usage
in China (93).
Dexamethasone
Dexamethasone, a synthetic glucocorticoid with
anti-inflammatory and immunosuppressive properties, inhibits growth
of myeloma and lymphoma cells (94). Upon binding to the glucocorticoid
receptor, a ligand activated transcription factor, dexamethasone
regulates the expression of a diverse sets of genes, resulting in
resolution of inflammation. Dexamethasone inhibits the activity of
inflammatory cells, including neutrophils, macrophages and
lymphocytes, and suppresses pro-inflammatory cytokines, such as
tumor necrosis factor (TNF) and interleukins, and other genes such
as cyclooxygenase-2 and inducible nitric oxide synthase (95).
A randomized, controlled clinical trial in the
United Kingdom found that dexamethasone reduced deaths by about
one-third in patients with COVID-19 who were on ventilators
(96). Administered at a
low-to-moderate dose of 6 mg dexamethasone per day for 10 days
improved the clinical outcomes in patients on ventilators (96). Those who were receiving oxygen
therapy but were not on ventilators also saw improvement, but no
effect on patients who were not receiving oxygen therapy or
ventilation was observed. Some reports suggested that well-timed,
higher doses of 0.5-1.0 mg/kg methylprednisolone per day improved
outcomes in those patients with respiratory failure, severe
illness, and cytokine storm (97,98).
Notably, steroidal drugs can be associated with numerous adverse
effects, including diabetes/hyperglycemia, osteopenia, cataracts,
avascular necrosis, fluid retention, hypertension and infection
(94,99). A meta-analysis of 15 studies with
5,270 patients with SARS-CoV-2 indicated that corticosteroids were
associated with higher rates of bacterial infection, longer
hospital stay and higher mortality (100). These reports suggest that
high-dose steroidal agents may be beneficial in later stages of
severe SARS-CoV-2 infection and/or impending cytokine storm
(94,99). Therefore, patients with non-severe,
non-cytokine storm SARS-CoV-2 infection are not recommended for
dexamethasone treatment, and the possible side effects of
dexamethasone drug used must be considered.
Traditional Chinese medicine
(TCM)
Lianhua Qingwen (LH), is produced from a mixture of
herbs, including Forsythia suspensa, Lonicera japonica
Thunberg, Ephedra sinica, Prunus armeniaca, Isatis
indigotica, Dryopteridis crassirhizoma, Houttuynia cordata,
Pogostemon cablin, Rhodiola rosea and Glycyrrhiza
inflanta, along with menthol and a traditional Chinese mineral
medicine containing calcium sulfate, Gypsum Fibrosum. LH is used to
treat influenza and chronic obstructive pulmonary disease (101). Patients with influenza complicated
by bronchial pneumonia that received LH capsules displayed greater
symptom improvement than those in a control group (101). A prospective multicenter
open-label, randomized, controlled trial of LH in 284 patients with
COVID-19 (142 each in the treatment and control groups)
demonstrated that the recovery rate was significantly higher in the
treatment group who received the usual antiviral or antibiotics
treatments alone based on the protocol for diagnosis and treatment
of novel coronavirus pneumonia (4th edition) or in combination with
LH (4 capsules, three times per day) for 14 days, compared with
that in the control group (102).
Additionally, LH treatment shortened the time to symptom recovery,
and improved the recovery of chest radiologic abnormalities with no
adverse reactions observed, in comparison with that in the control
group (102). Though there were no
differences in the rate of conversion to severe cases or viral
assay findings, LH capsules may be beneficial in cases of COVID-19,
although this requires more randomized, controlled trials in a
larger patient population. LH combined with ribavirin, a guanosine
nucleoside analog, has been used in the treatment of viral upper
respiratory tract infection (103).
Qing Fei Pai Du Tang (QFPDT), a TCM containing 21
herbs, including Ephedra sinica, Bupleurum chinense,
Pogostemon cablin, Cinnamomum cassia and
Scutellaria baicalensis, is thought to act in the lung
(104,105). By regulating a series of proteins
co-expressed with ACE2 and signaling pathways closely related to
the occurrence and development of diseases, it may play a role in
reducing inflammation (104).
QFPDT may act as an antiviral agent by targeting ribosomal proteins
that are necessary for viral replication, thus inhibiting viral
mRNA translation and inhibiting a group of proteins that interact
with viral proteins (103). When
QFPDT was administered to 214 patients with COVID-19 in China, the
majority of patients (60%) displayed improved symptoms, where the
illness of the 30% patients were stabilized (106). An additional 701 patients with
COVID-19 were treated with QFPDT and, of these, 130 patients
(18.5%) were symptom free after treatment, 51 patients (7.27%)
recovered from their fever and cough, symptoms were improved in 268
patients (38.2%) and stabilized in 212 patients (30.2%) (106). Administration of QFPDT along with
Western medical therapy (the antiviral medicines interferon,
lopinavir or arbidol) revealed a tendency to mitigate the extent of
multiorgan impairment in 63 patients with confirmed
COVID-19(107), providing evidence
that QFPDT combined with antiviral drugs for the treatment of
COVID-19 may be beneficial.
Statins
Statins, used conventionally for lowering
cholesterol and for their anti-thrombotic properties, also have
anti-viral activity (108,109). Statins block the infectivity of
enveloped viruses through inhibition of glycoprotein processing.
Reiner et al (110)
performed docking studies, which revealed that statins interact
directly with the main protease enzyme of SARS-CoV-2. Among them,
promising statins, including pitavastatin, rosuvastatin, lovastatin
and fluvastatin, might be useful in COVID-19 treatment (110). A recent retrospective study
involving 13,981 patients with COVID-19 indicated a lower risk for
28-day all-cause mortality in the matched statin group of 1,219
patients, suggesting the safety of statins or the combination of a
statin with an angiotensin-converting enzyme (ACE)
inhibitor/angiotensin receptor blocker for treatment of patients
with COVID-19(111). As statins
may induce the expression of ACE2, resulting in an increased risk
of SARS-CoV-2 viral entrance (111), further research is urgently needed
to validate the utility of statins to combat the mortality of
COVID-19.
Viral main protease (Mpro)
inhibitors
Mpro, a key coronavirus enzyme playing an
important role in proteolytic maturation (110), has been investigated as a
potential protein target to prevent infection expansion (112).
Carmofur (1-hexylcarbamoyl-5-fluorouracil), an
antineoplastic agent used to treat colorectal cancer, breast,
gastric and bladder cancers, is shown to inhibit the SARS-CoV-2
Mpro. Carmofur inhibits viral replication in SARS-CoV-2
infected Vero E6 cells and shows promise for its successful use as
a new antiviral treatment for COVID-19(113).
Jin et al (114) identified 7 compounds (N3, ebselen,
disulfiram, tideglusib, carmofur, shikonin and PX-12) from
>10,000 compounds, including approved drugs, drug candidates in
clinical trials and other pharmacologically active compounds, that
could inhibit Mpro. Following further study, ebselen and
N3 demonstrated the strongest antiviral effects against SARS-CoV-2.
Among these, N3 is a mechanism-based inhibitor developed using
computer-aided drug design, which specifically inhibits
Mpro from multiple coronaviruses, including SARS-CoV and
MERS-CoV (114). Ebselen is an
organoselenium compound with anti-inflammatory, anti-oxidant and
cytoprotective properties and has previously been investigated for
the treatment of multiple diseases, including bipolar disorder and
has a low cytotoxicity (114).
Gupta et al (115) reported that, by using a
combination of molecular docking, scoring functions and molecular
dynamics simulations, C1
(1E,6E)-1,2,6,7-tetrahydroxy-1,7-bis(4-hydroxy-3-methoxyphenyl)hepta-1,6-diene-3,5-dione)
and C2
(4Z,6E)-1,5-dihydroxy-1,7-bis(4-hydroxyphenyl)hepta-4,6-dien-3-one,
identified from among 267 compounds in Curcuma longa L.
(Zingiberaceae family), bound strongly to the catalytic core
of the Mpro protein with higher efficacy than lopinavir,
a standard Mpro inhibitor.
RBD-targeting antibodies
As the S protein plays the most important role in
viral attachment, fusion and entry, much of the development of
monoclonal antibodies, entry inhibitors and vaccines are focused on
the S protein (28). Specifically,
the 193 amino acid length (N318-V510) receptor binding domain (RBD)
within the S protein is a critical target for neutralizing
antibodies (116). 206
RBD-specific monoclonal antibodies derived from single B cells of
eight SARS-CoV-2 infected individuals displayed potent
anti-SARS-CoV-2 neutralization activity but did not cross-react
with SARS-CoV or MERS-CoV RBDs (117), suggesting that anti-RBD antibodies
are viral species-specific inhibitors. According to a study by
Robbiani et al (118), most
convalescent plasma collected from individuals who recover from
COVID-19 does not contain high levels of neutralizing activity but
has anti-SARS-CoV-2 RBD antibodies, suggesting that humans are
intrinsically capable of generating potent anti-RBD antibodies that
neutralize SARS-CoV-2. In addition, 2 specific human monoclonal
antibodies, named CA1 and CB6, from a convalescent COVID-19 patient
demonstrated potent in vitro SARS-CoV-2-specific
neutralization activity against SARS-CoV-2(119).
ACE2-targeting agents
ACE2, identified as an important drug target for the
treatment of cardiovascular and kidney diseases, is a key
functional receptor for coronavirus infection (120). A fusion protein containing an ACE2
mutant with low catalytic activity, which has a high binding
affinity for the receptor-binding domains of SARS-CoV and
SARS-CoV-2, has broad neutralizing activity against SARS-CoV and
SARS-CoV-2 in vitro and exhibits desirable pharmacological
properties in mice (121),
suggesting that an ACE2 fusion protein have potential applications
in the development of vaccines for SARS-CoV-2 treatment.
Pudilan (PDL), a TCM including Isatis
indigotica, Corydalis bungeana, Taraxacum
mongolicum and Scutellaria baicalensis has been used as
an anti-SARS-CoV-2 agent in China (121). By conducting network pharmacology
analysis, PDL might also have therapeutic potential for COVID-19,
it may prevent SARS-CoV-2 entry into cells by blocking the ACE2
receptor and by regulating cytokines and chemokines to moderate the
immune response (121). However,
the targets predicted by bioinformatics and network pharmacology
tools require further investigation to confirm.
TMPRSS2 inhibitors
TMPRSS2 facilitates viral particle entry into host
cells and its inhibition blocks viral fusion with ACE2(32). Withanone (Wi-N), a natural compound
derived from Withania somnifera and used in Indian Ayurvedic
medicine, can bind and stably interact at the catalytic site of
TMPRSS2(122). Having strong
interactions with TMPRSS2 catalytic residues, Wi-N may decrease the
endogenous expression of TMPRSS2(122), suggesting that Wi-N probably
confers therapeutic effects against COVID-19 by blocking the entry
of SARS-CoV-2 into host cells.
TMPRSS2 targets were screened from the natural
compounds library Natural Product Activity and Species Source, a
freely accessible database containing 30,927 compounds, using a
ligand-based pharmacophore approach and a molecular docking-based
screen in the Molecular Operating Environment software (123). The 12 compounds with the most
favorable structural features were studied for physicochemical and
absorption, distribution, metabolism, excretion and toxicity
properties. The results suggested that the compound NPC306344, with
a low-molecular-weight, interacted significantly with the active
site residues of TMPRSS2(123).
However, in vitro and in vivo studies should be
conducted to confirm the preventive effect of NPC306344.
Probiotics
Several patients with COVID-19 experienced
dysbiosis, characterized by lower levels of Lactobacillus
and Bifidobacterium. Prebiotic and probiotic intake for
these patients reduces the risk of secondary infection due to
bacterial translocation (124),
suggesting that probiotics could be a promising strategy for the
treatment of SARS-CoV-2.
Scientific data supports the action of probiotics
that help maintain or restore the balance of the intestinal
microbiome, consequently enhancing the immune response to viral
infections, such as SARS-CoV and MERS-CoV, suggesting that
probiotics could be beneficial in the treatment of viral infections
(125,126). The regulatory role of probiotics
on the gut-lung axis and the mucosal immune system for the
potential antiviral mechanisms revolves around the competitive
inhibition of the growth of pathogenic bacteria. In addition, the
secretion of antimicrobial peptides, the action of metabolites, and
nucleosidase activity also is responsible for the potential
antiviral ability of probiotics (125,127).
Antibiotics
SARS-CoV-2 infection impairs the host immune system
via damaging lymphocytes, especially B cells, T cells and NK cells
(128), which may be the main
promoter for coinfection with bacteria and fungi (129,130). A single-center, retrospective case
series of 221 patients with COVID-19 suggested that the bacterial
coinfection rate was 7.7%, and the fungal coinfection rate was 3.2%
(131). A report of postmortem
needle autopsy in 10 COVID-19 cases indicated that the pulmonary
pathological changes of fatal COVID-19 include signs of diffuse
alveolar damage and, in some cases, bacteria and fungi were
detected (132), suggesting a
serious bacterial or fungal infection secondary to the diffuse
alveolar damage. In another 44 nasopharyngeal test samples, 38
varieties of bacteria and 9 varieties of fungi were found (133). A patient with COVID-19 recovered
after combination therapy against the virus, bacteria and fungi,
and respiratory support. Therefore, antibiotic treatment for
COVID-19 patients seemed to be a basic requirement (130,134).
Azithromycin, a macrolide antibiotic with excellent
tissue penetration and anti-inflammatory effects, downregulates
pathways involving serine proteases TMPRSS2 and TMPRSS11D required
for SARS-CoV-2 activation, indicating that azithromycin may hinder
SARS-CoV-2 infection (135). In
combination with hydroxychloroquine, azithromycin was shown to
inhibit the replication of SARS-CoV-2(136). As of 28th April 2020, there are 21
clinical trials registered on ClinicalTrials.gov for azithromycin related to
COVID-19(137).
However, the most appropriate antibacterial agent
must be chosen based on the clinical symptoms of patients with
COVID-19 and microbiological results; otherwise, clinicians must
halt the misapplication of antibiotics (138).
7. Vaccines
According to the latest WHO vaccine candidate
research and development report (139), as of 1st October, 2020, there were
187 global COVID-19 vaccines under development, including five
known types of vaccine: Inactivated vaccine, attenuated live
vaccine, recombinant protein vaccine, nucleic acid vaccine (RNA and
DNA vaccine) and virus vector vaccine. Of these vaccines, 38 are in
the human trial phase. The progress of vaccine research is
summarized in Table I.
 | Table IAnti-COVID-19 vaccines in clinical
evaluation (138,139). |
Table I
Anti-COVID-19 vaccines in clinical
evaluation (138,139).
| * | Immunization
strategy | Clinical Stage |
Advantages/limitations of the vaccine
platform |
|---|
| Vaccine
platform | Vaccine
developer | Schedule | Route | Phase I | Phase I/II | Phase II | Phase III |
|---|
| Inactivated
virus | Inactivated
virus | Sinovac Biotech
Ltd. | 2 doses | i.m | | NCT04383574 | | NCT04456595 669/
UN6.KEP/EC/2020 | Compared with the
live attenuated vaccines, the route is mature, the preparation is
simple and fast and has the pre-existing technology for
development. The immunization period is short but incidence of
serious adverse reactions is high. |
| NCT04352608 |
| NCT04551547 | |
| | Inactivated
virus | Wuhan Institute of
Biological Products Co., Ltd. | 2 doses | i.m | |
ChiCTR2000031809 |
ChiCTR2000034780 |
| | Inactivated
virus | Beijing Institute
of Biological Products Co., Ltd. | 2 doses | i.m | |
ChiCTR2000032459 |
ChiCTR2000034780 |
| | Inactivated
virus | Chinese Academy of
Medical Sciences Research Institute for Biological Safety Problems
(Republic of Kazakhstan) Bharat Biotech International Ltd. | 2 doses | i.m | NCT04412538 | NCT04470609 | |
| | Inactivated
virus | 2 doses | i.m | | NCT04530357 | |
| | Inactivated
virus | 2 doses | i.m | | NCT04471519 | |
| Virus-like
particles | Virus like
particle | Medicago, Inc. | 2 doses | i.m | NCT04450004 | | | | Its composition is
clear, safe and stable. It is produced only by sequence of
pathogens, and the manufacturing process is simple. It may be
integrated into the genome. |
| DNA | DNA plasmid
vaccine+ electroporation | Inovio
Pharmaceuticals, Inc./International Vaccine Institute Osaka
University/ AnGes, Inc./Takara Bio, Inc. | 2 doses | i.d | | NCT04447781 | | |
| | | | NCT04336410 | | |
| | | | | | |
| | | | | | | | |
| | DNA plasmid vaccine
+ Adjuvant | 2 doses | i.m | | NCT04463472 | | |
| | DNA plasmid
vaccine | Cadila Healthcare
Ltd. | 3 doses | i.d | |
CTRI/2020/07/026352 | | |
| NCT04527081 | | |
| | DNA vaccine | Genexine
Consortium | 2 doses | i.m | | NCT04445389 | | |
| RNA | LNP- encapsulated
mRNA | Moderna, Inc./
National Institute of Allergy and Infectious Diseases, National
Institutes of Health | 2 doses | i.m | NCT04283461 | | NCT04405076 | NCT04470427 | It is produced only
by sequence of pathogens and the manufacturing process is simple.
Instability. |
| | 3 LNP-mRNAs | BioNTech SE/
Shanghai Fosun Pharmaceutical Co., Ltd./Pfizer Inc. | 2 doses | i.m | | 2020-001038-36 | | NCT04368728 | |
| | | | | |
ChiCTR2000034825 | | | |
| | | | | | NCT04537949 | | | |
| | | | | | | | | |
| | mRNA | CureVac | 2 doses | i.m | NCT04449276 | | NCT04515147 | | |
| | mRNA | Arcturus | 2 doses | i.m | | NCT04480957 | | | |
| | | Therapeutics/
Duke-NUS Medical School | | | | | | | |
| | RNA | Imperial College
London | 2 doses | i.m | ISRCTN17072692 | | | | |
| | RNA | PLA Academy of
Military Sciences/ Walvax Biotech | 2 doses | i.m |
ChiCTR2000034112 | | | | |
| Viral vector-
based | Replicating viral
vector | Beijing Wantai
Biological Pharmacy/ Xiamen University | 2 doses | i.m |
ChiCTR2000037782 | | | | It induces strong
humoral and cellular immune responses. |
| | Replicating viral
vector | Institute Pasteur/
Themis/Univ, of Pittsburg CVR/Merck Sharp& Dohme | 1 dose | i.m | NCT04497298 | | | | The body will
interfere with the prestored immune response of the virus
vector. |
|
| | Non-replicating
viral vector | University of
Oxford/ AstraZeneca | 1 dose | i.m | |
PACTR202006922165132 | 2020-001228-32 | ISRCTN89951424 | |
| | 2020-001072-15 | | NCT04516746 | |
| | | | | | | | | NCT04520393 | |
| | Non-replicating
viral vector | CanSino Biological
Inc./Bejing Institute of Biotechnology | 1 dose | i.m |
ChiCTR2000030906 | |
ChiCTR2000031781 | NCT04526990 | |
| | NCT04540419 | |
| | Non-replicating
viral vector | Gamaleya Research
Institute of Epidemiology and Microbiology | 2 doses | i.m | NCT04436471 | | | NCT04530396 | |
| NCT04437875 | | | | |
| | Non-replicating
viral vector | Janssen
Pharmaceuticals Inc. | 2 doses | i.m | | NCT04436276 | | NCT04505722 | |
| | Non-replicating
viral vector | ReiThera Srl/
Leukocare AG/ Univercells SA | 1 dose | i.m | NCT04528641 | | | | |
| | Non-replicating
viral vector | Institute of
Biotechnology/PLA | 2 doses | i.m/ mucosal | NCT04552366 | | | | |
| | | Academy of Military
Sciences | | | | | | | |
| Protein subunit
vaccine | | Novavax, Inc. | 2 doses | i.m | | NCT04368988 | NCT04533399 | | It induces strong
humoral and cellular immune responses. |
| | Anhui Zhifei
Longcom | 2 doses or 3
doses | i.m | NCT04445194 | NCT04550351 | NCT04466085 | |
| | | Biologic Pharmacy
Co., Ltd./Institute of Microbiology (Chinese Academy of
Sciences) | | | | | | |
| The body will
interfere with the prestored immune response of the virus
vector. |
| | | Kentucky
Bioprocessing, Inc | 2 doses | i.m | | NCT04473690 | | |
| |
| | | Sanofi SA/
GlaxoSmithKline | 2 doses | i.m | | NCT04537208 | | | |
| | | Sichuan Clover
Biopharmaceuticals Inc./ GlaxoSmithKline/ Dynavax Technologies | 2 doses | i.m | NCT04405908 | | | | |
| | | Vaxine Pty Ltd./
Medytox, Inc. | 1 dose | i.m | NCT04453852 | | | | |
| | | University of
Queensland/CSL Ltd. | 2 doses | i.m |
ACTRN12620000674932p ISRCTN51232965 | | | | |
| | | Medigen Vaccine
Biologics Corporation/ National Institute of Health/Dynavax
Technologies | 2 doses | i.m | NCT04487210 | | | | |
| | | Instituto Finlay de
Vacunas (Cuba) | 2 doses | i.m | IFV/COR/04 | | | | |
| | | FBRI SRC VB VECTOR,
Rospotrebnadzor (Russia) | 2 doses | i.m | NCT04527575 | | | | |
| | | Sichuan
University | 2 doses | i.m |
ChiCTR2000037518 | | | | |
| | | University Hospital
Tübingen | 1 dose | sc | NCT04546841 | | | | |
| | | COVAX | 2 doses | i.m | NCT04545749 | | | | |
Inactivated viral vaccines
Inactivated vaccines use cell culture to create
virus particles and destroy pathogenicity, by physical or chemical
means, so that the viral particles retain only antigenicity
(140). The commonly used cell
lines for vaccine production are the canine renal epithelial (MDCK)
cells and the African green monkey kidney (Vero) cells (141). A SARS-CoV-2 candidate vaccine
PiCoVacc induced a specific neutralizing antibody against
SARS-CoV-2 in mice, rats and rhesus monkeys (142), where the inactivated vaccine was
safe and reliable. At present, there are nine inactivated vaccine
projects. Of these, four are in phase I or II clinical trials. The
blind clinical phase III trial of the Vero inactivated vaccine from
Sinopharm Group Co., Ltd. has started in Abu Dhabi (143). The results of completed phase I/II
suggested that there were no serious adverse reactions in the
vaccinated group and that the antibody positive rate reached 100%
according to the 0- and 28-day vaccination procedures. The clinical
phase I/II of CoronaVac inactivated vaccine developed by SinoVac
Biotech Ltd. (Beijing Kexing Zhongwei Biological Technology Co.,
Ltd.) also demonstrated no serious adverse reactions (144,145). The positive conversion rate of
neutralizing antibody was >90% after 14 days of whole
immunization.
Live attenuated viral vaccine
Live attenuated vaccine is obtained by passaging
several generations of the virus until it retains only weak
pathogenicity in the human host (139). There are three COVID-19 live
attenuated vaccine projects under research and development
(139): i) A recombinant live
attenuated vaccine jointly developed by Codagenix, Inc. and the
Serum Institute of India Pvt. Ltd.; ii) a vaccine developed by
Griffith University of Australia and India Immunologicals Ltd.
(ILL), and iii) the viral vector vaccine and attenuated measles
vaccine targeting the S protein and N protein developed by the
German Center for Infection Research (Deutsches Zentrum für
Infektionsforschung) and IDT Biologika GmbH. Due to the long
development time of live attenuated vaccine, the three projects
have not yet entered the clinical trial stage. Notably, a study
suggested that the live attenuated SARS vaccine could produce toxic
viral protein again after multiple generations of replication in
mice (146), indicating that the
live attenuated vaccine still has substantial safety concerns.
Recombinant protein vaccine
The recombinant protein vaccine, a genetically
engineered vaccine, is considered to be safe type of vaccine
(140). These vaccines are
produced by integrating specific antigen viral gene into expression
vectors and transforming the expression vectors into bacteria,
yeast or animal cells, inducing expression of antigen proteins
(140). However, due to the
selection of different cells as vectors, the expressed antigen may
be different from the natural antigen of the virus, so the
immunogenicity is weak (147).
There are two methods to solve this problem: Using virus like
particles and adding adjuvants (147). A vaccine candidate with M matrix
adjuvant of Novavax has entered clinical trial phase II (148). A vaccine developed by Clover
Biopharmaceuticals Inc./GSK/Dynavax with an S-trimer, a protein
highly similar to the SARS-CoV-2 S, developed using the patented
technology of trimer tag and genetic engineering, has been proven
to bind to the specific antibody in the serum of convalescent
patients (149). A phase I
clinical trial was also completed to evaluate the safety and
immunogenicity of the S-trimer candidate (149).
Nucleic acid vaccines
Nucleic acid vaccines are also known as gene
vaccines, including DNA and mRNA vaccines (150). These vaccines use intramuscular
injection of plasmid or naked DNA, RNA or mRNA gene of a certain
antigen to induce antigen protein expression in host body, thereby
eliciting an immune response (151,152). At present, there are no human
nucleic acid vaccines on the market, partially because of some of
the technical difficulties in delivering a precise and accurate
vaccine. A DNA vaccine may be integrated into the genome because it
needs to enter the nucleus to express the antigen (146). Although the mRNA can avoid the
risk of host genome integration, it has some disadvantages, such as
instability (152). Some methods
to improve the stability and protein production of mRNA and to
improve the delivery effect have academic focus on an mRNA vaccine
(152). These methods include the
use of modified nucleotides and the development of nanoparticle
delivery systems, which can stabilize mRNA, enhance cell uptake and
improve the bioavailability of mRNA after it enters the cell
(152).
The first COVID-19 vaccine approved
for clinical trial was the mRNA-1273 vaccine developed by Moderna,
Inc.,
which is currently in phase III clinical trials
(153). In addition, the mRNA
vaccine led by BioNTech SE is in phase III clinical trials
(154).
Viral vector
vaccines. A recombinant virus vector vaccine is a vaccine that
takes the replicative activity or non-replicating virus as a
carrier and recombines antigenic genes into the viral genome
(140). The adenovirus vector
(Ad5) vaccine developed by Beijing Institute of Biotechnology and
CanSino Biologics, Inc. has entered phase II clinical trials
(139). A total of 108 healthy
volunteers aged 18-60 were recruited to phase I clinical trials to
determine the human tolerance of different doses of the vaccine by
observing the safety of vaccine use (155). The results indicated that the Ad5
NCoV vaccine is well tolerated and can induce an immune response to
SARS-CoV-2(156). Compared with
the phase I clinical trials, the phase II clinical trials opened
the upper age limit, to further analyze and confirm the preliminary
efficacy and safety of the vaccine in the population, and to
determine the immune program and dose of the vaccine. In addition,
the ChAd0x1-s vector vaccine, led by Oxford University, has also
entered phase III of clinical trials (156).
8. Conclusions and outlook
SARS-CoV-2 is a new virus and its source,
transmission mode, pathogenesis and clinical manifestations are not
well-known. In addition, SARS-CoV-2 is highly infectious, creating
an outbreak that has spread rapidly to all parts of the world
(2). The novel coronavirus has been
prevalent all over the world since SARS-CoV-2 was first identified
in patients who were exposed at a seafood market in Wuhan City,
Hubei Province, China in December 2019(11). Similar to findings related to
SARS-CoV and MERS-CoV, SARS-CoV-2 is believed to have crossed
species and initiated primary human infections (5,6). As
SARS-CoV-2 will evolve through frequent recombination of its
genomes and through mutations (157), the propensity to infect multiple
species and the increasing human-animal interface presents unknown
problems.
Practicing good hygiene and wearing masks seem to
be effective methods to restrict the spread of COVID-19 (24,158).
However, prevention and treatment of COVID-19 with drugs remain
urgent issues to be resolved. Non-specific antiviral therapy
(oseltamivir, ganciclovir), antibacterial therapy (moxifloxacin,
ceftriaxone, azithromycin) and glucocorticoid therapy are being
improvised by combination with broad-spectrum antivirals such as
remdesivir, chloroquine, and lopinavir/ritonavir (159). Plasma therapy shows promise as a
beneficial treatment. The deliberate infection of healthy
volunteers with SARS-CoV-2 were proposed, as it may shorten the
time required for the development of COVID-19 vaccines (160).
During the current outbreak, the development of
clinical drugs against coronaviruses has been challenging, and the
recent advances in understanding the molecular mechanisms of
infection and transmission facilitate more rapid diagnoses and
treatment of COVID-19. Aside from traditional drug therapy during
the ongoing SARS-CoV-2 epidemic, vigorous efforts on the vaccine
development are urgently needed. Finding a short section or
sections of viral protein sequence suitable for a synthetic vaccine
and antagonists against COVID-19 can be useful for preliminary
design proposals. The S protein, a glycoprotein encoded by
coronavirus genome RNA that is usually cut into spherical S1
subunit and rod-shaped S2 subunit during virus assembly, is an
important component of coronavirus to recognize and infect host
cells. Thus, identification of immunogenic targets against the
important SARS-CoV-2 proteins, such as the S glycoprotein, will
provide crucial advances towards the development of sensitive
diagnostic tools and potential vaccine candidates. Moreover, the
therapeutic options currently under investigation, such as
inhibitors targeting the S protein, require confirmation in
clinical trials prior to recommendation. Moving forward there are
treatment options available that could be utilized clinically
during the ongoing SARS-CoV-2 epidemic, as these agents have shown
significant effects against COVID-19 in preclinical trials. Based
on knowledge of the mechanism of SARS-CoV-2 replication and
infection, a broad-range of combinational therapies should also be
evaluated. Computational techniques combined with the mechanistic
studies of SARS-CoV-2 can aid in the design and development of
predicted antiviral agents. Follow-up experimental studies will
test novel candidates for drug repurposing, which will be hopefully
be translated into clinical practice.
The present review summarizes the latest findings
related to the clinical features, diagnosis, and management of
COVID-19. The aim was to provide the most up-to-date understanding
of SARS-CoV-2, with ongoing guidance for COVID-19 prevention and
control. As there is a dynamic and a large volume of emerging
therapeutic approaches for COVID-19, only
articles/publications/translations from English (Pubmed database;
https://www.ncbi.nlm.nih.gov/) and
Chinese (China National Knowledge Infrastructure database;
https://www.cnki.net/) of the adult population
between December 2019 and September 2020, and realize that some
relevant international data might be missing.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the
National Natural Science Foundation of China (grant no. 81773271),
the Fund of Guangdong Provincial Education Department (grant nos.
2017KZDXM088 and 2018KQNCX284), the Joint Basic and Applied
Research Fund of Guangdong Province (grant no. 2019A1515110689) and
the National Science and Technology Major Project (grant no.
2018YFA0902702). The funders had no role in study design, data
collection and analysis, decision to publish or preparation of the
manuscript.
Availability of data and materials
Not Applicable.
Authors' contributions
RW prepared the draft manuscript. RW, XL, FL and SL
critically revised and edited the manuscript. All authors have read
and agreed to the published version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
World Health Organization. WHO
Director-General's remarks at the media briefing on 2019-nCoV on 11
February 2020. Available from: urihttps://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020simplehttps://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020.
|
|
2
|
Lu H, Stratton CW and Tang YW: Outbreak of
pneumonia of unknown etiology in Wuhan, China: The mystery and the
miracle. J Med Virol. 92:401–402. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
World Health Organization. WHO
Director-General's opening remarks at the media briefing on
COVID-19-11 March 2020. Available from: urihttps://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020simplehttps://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020.
|
|
4
|
World Health Organization. WHO
Director-General's opening remarks at the media briefing on
COVID-19-11 October 2020. Available from: urihttps://www.who.int/docs/default-source/coronaviruse/situation-reports/20201012-weekly-epi-update-9.pdf?sfvrsn=49dc56e1_4&download=truesimplehttps://www.who.int/docs/default-source/coronaviruse/situation-reports/20201012-weekly-epi-update-9.pdf?sfvrsn=49dc56e1_4&download=true.
|
|
5
|
Chan JF, Yuan S, Kok KH, To KK, Chu H,
Yang J, Xing F, Liu J, Yip CC, Poon RW, et al: A familial cluster
of pneumonia associated with the 2019 novel coronavirus indicating
person-to-person transmission: A study of a family cluster. Lancet.
395:514–523. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong
Y, Ren R, Leung KSM, Lau EHY, Wong JY, et al: Early transmission
dynamics in Wuhan, China, of novel coronavirus-infected pneumonia.
N Engl J Med. 382:1199–1207. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Farsalinos K, Niaura R, Le Houezec J,
Barbouni A, Tsatsakis A, Kouretas D, Vantarakis A and Poulas K:
Editorial: Nicotine and SARS-CoV-2: COVID-19 may be a disease of
the nicotinic cholinergic system. Toxicol Rep. 7:658–663.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirusin Wuhan, China. Lancet.
395:497–506. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ioannidis JPA, Axfors C and
Contopoulos-Ioannidis DG: Population-level COVID-19 mortality risk
for non-elderly individuals overall and for non-elderly individuals
without underlying diseases in pandemic epicenters. Environ Res.
188(109890)2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Nasi A, McArdle S, Gaudernack G, Westman
G, Melief C, Rockberg J, Arens R, Kouretas D, Sjölin J and Mangsbo
S: Reactive oxygen species as an initiator of toxic innate immune
responses in retort to SARS-CoV-2 in an ageing population, consider
N-acetylcysteine as early therapeutic intervention. Toxicol Rep.
7:768–771. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhu N, Zhang D, Wang W, Li X, Yang B, Song
J, Zhao X, Huang B, Shi W, Lu R, et al: A novel coronavirus from
patients with pneumonia in China, 2019. N Engl J Med. 382:727–733.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Amini Pouya M, Afshani SM, Maghsoudi AS,
Hassani S and Mirnia K: Classification of the present
pharmaceutical agents based on the possible effective mechanism on
the COVID-19 infection. Daru: Jul 30, 2020 (Epub ahead of print).
doi: 10.1007/s40199-020-00359-4.
|
|
13
|
Park WB, Kwon NJ, Choi SJ, Kang CK, Choe
PG, Kim JY, Yun J, Lee GW, Seong MW, Kim NJ, et al: Virus isolation
from the first patient with SARS-CoV-2 in Korea. J Korean Med Sci.
35(e84)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zhou P, Yang XL, Wang XG, Hu B, Zhang L,
Zhang W, Si HR, Zhu Y, Li B, Huang CL, et al: A pneumonia outbreak
associated with a new coronavirus of probable bat origin. Nature.
579:270–273. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tian X, Li C, Huang A, Xia S, Lu S, Shi Z,
Lu L, Jiang S, Yang Z, Wu Y and Ying T: Potent binding of 2019
novel coronavirus spike protein by a SARS coronavirus-specific
human monoclonal antibody. Emerg Microbes Infect. 9:382–385.
2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Meo SA, Alhowikan AM, Al-Khlaiwi T, Meo
IM, Halepoto DM, Iqbal M, Usmani AM, Hajjar W and Ahmed N: Novel
coronavirus 2019-nCoV: Prevalence, biological and clinical
characteristics comparison with SARS-CoV and MERS-CoV. Eur Rev Med
Pharmacol Sci. 24:2012–2019. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ji W, Wang W, Zhao X, Zai J and Li X:
Cross-species transmission of the newly identified coronavirus
2019-nCoV. J Med Virol. 92:433–440. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wang J, Liang J, Cheng J, Guo Y and Zeng
L: Deep learning based image reconstruction algorithm for
limited-angle translational computed tomography. PLoS One.
15(e0226963)2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sundararaman A, Ray M, Ravindra PV and
Halami PM: Role of probiotics to combat viral infections with
emphasis on COVID-19. Appl Microbiol Biotechnol. 104:8089–8104.
2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wang C, Hornby PW, Hayden FG and Gao GF: A
novel coronavirus outbreak of global health concern. Lancet.
395:470–473. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Business Daily: China locks down two
cities to curb virus outbreak. Available from: urihttps://www.businessdailyafrica.com/news/world/China-locks-down-two-cities-to-curb-virus-outbreak/4259366-5428676-xkv9uo/index.htmlsimplehttps://www.businessdailyafrica.com/news/world/China-locks-down-two-cities-to-curb-virus-outbreak/4259366-5428676-xkv9uo/index.html.
|
|
22
|
Goumenou M, Sarigiannis D, Tsatsakis A,
Anesti O, Docea AO, Petrakis D, Tsoukalas D, Kostoff R, Rakitskii
V, Spandidos DA, et al: COVID-19 in Northern Italy: An integrative
overview of factors possibly influencing the sharp increase of the
outbreak (Review). Mol Med Rep. 22:20–32. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Torequl Islam M, Nasiruddin M, Khan IN,
Mishra SK, Kudrat-E-Zahan M, Alam Riaz T, Ali ES, Rahman MS,
Mubarak MS, Martorell M, et al: A perspective on emerging
therapeutic interventions for COVID-19. Front Public Health.
8(281)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tsatsakis A, Petrakis D, Nikolouzakis TK,
Docea AO, Calina D, Vinceti M, Goumenou M, Kostoff RN, Mamoulakis
C, Aschner M and Hernández AF: COVID-19, an opportunity to
reevaluate the correlation between long-term effects of
anthropogenic pollutants on viral epidemic/pandemic events and
prevalence. Food Chem Toxicol. 141(111418)2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Del Rio C and Malani PN: COVID-19-New
insights on a rapidly changing epidemic. JAMA. 323:1339–1340.
2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lukassen S, Chua RL, Trefzer T, Kahn NC,
Schneider MA, Muley T, Winter H, Meister M, Veith C, Boots AW, et
al: SARS-CoV-2 receptor ACE2 and TMPRSS2 are primarily expressed in
bronchial transient secretory cells. EMBO J.
39(e105114)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Izaguirre G: The proteolytic regulation of
virus cell entry by furin and other proprotein convertases.
Viruses. 11(837)2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kirchdoerfer RN, Cottrell CA, Wang N,
Pallesen J, Yassine HM, Turner HL, Corbett KS, Graham BS, McLellan
JS and Ward AB: Pre-fusion structure of a human coronavirus spike
protein. Nature. 531:118–121. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Li F: Structure, function, and evolution
of coronavirus spike proteins. Annu Rev Virol. 3:237–261.
2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Walls AC, Tortorici MA, Snijder J, Xiong
X, Bosch BJ, Rey FA and Veesler D: Tectonic conformational changes
of a coronavirus spike glycoprotein promote membrane fusion. Proc
Natl Acad Sci USA. 114:11157–11162. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Park JE, Li K, Barlan A, Fehr AR, Perlman
S, McCray PB Jr and Gallagher T: Proteolytic processing of Middle
East respiratory syndrome coronavirus spikes expands virus tropism.
Proc Natl Acad Sci USA. 113:12262–12267. 2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Hoffmann M, Kleine-Weber H, Schroeder S,
Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH,
Nitsche A, et al: SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2
and is blocked by a clinically proven protease inhibitor. Cell.
181:271–280.e8. 2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Kawase M, Kataoka M, Shirato K and
Matsuyama S: Biochemical analysis of coronavirus spike glycoprotein
conformational intermediates during membrane fusion. J Virol.
93:e00785–19. 2019.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Walls AC, Park YJ, Tortorici MA, Wall A,
McGuire AT and Veesler D: Structure, function, and antigenicity of
the SARS-CoV-2 spike glycoprotein. Cell. 181:281–292.e6.
2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Heurich A, Hofmann-Winkler H, Gierer S,
Liepold T, Jahn O and Pohlmann S: TMPRSS2 and ADAM17 cleave ACE2
differentially and only proteolysis by TMPRSS2 augments entry
driven by the severe acute respiratory syndrome coronavirus spike
protein. J Virol. 88:1293–1307. 2014.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wrapp D, Wang N, Corbett KS, Goldsmith JA,
Hsieh CL, Abiona O, Graham BS and McLellan JS: Cryo-EM structure of
the 2019-nCoV spike in the prefusion conformation. Science.
367:1260–1263. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Zhao Y, Zhao Z, Wang Y, Zhou Y, Ma Y and
Zuo W: Single-Cell RNA expression profiling of ACE2, the receptor
of SARS-CoV-2. Am J Respir Crit Care Med. 202:756–759.
2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Wang PH and Chen Y: Increasing host
cellular receptor-angiotensin-converting enzyme 2(ACE2) expression
by coronavirus may facilitate 2019-nCoV infection. bioRxiv: Feb 27,
2020 (Epub ahead of print). doi: urihttps://doi.org/10.1101/2020.02.24.963348simplehttps://doi.org/10.1101/2020.02.24.963348.
|
|
39
|
Zhang H, Kang Z, Gong H, Xu D, Wang J, Li
Z, Cui X, Xiao J, Meng T, Zhou W, et al: The digestive system is a
potential route of 2019-nCov infection: A bioinformatics analysis
based on single-cell transcriptomes. bioRxiv: Jan 31, 2020 (Epub
ahead of print). doi: urihttps://doi.org/10.1101/2020.01.30.927806simplehttps://doi.org/10.1101/2020.01.30.927806.
|
|
40
|
Zu ZY, Jiang MD, Xu PP, Chen W, Ni QQ, Lu
GM and Zhang LJ: Coronavirus disease 2019 (COVID-19): A perspective
from China. Radiology. 296:E15–E25. 2020.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Zhang G, Zhang J, Wang B, Zhu X, Wang Q
and Qiu S: Analysis of clinical characteristics and laboratory
findings of 95 cases of 2019 novel coronavirus pneumonia in Wuhan,
China: A retrospective analysis. Respir Res. 21(74)2020.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Tang A, Tong ZD, Wang HL, Dai YX, Li KF,
Liu JN, Wu WJ, Yuan C, Yu ML, Li P and Yan JB: Detection of novel
coronavirus by RT-PCR in stool specimen from asymptomatic child,
China. Emerg Infect Dis. 26:1337–1339. 2020.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Corman VM, Landt O, Kaiser M, Molenkamp R,
Meijer A, Chu DK, Bleicker T, Brünink S, Schneider J, Schmidt ML,
et al: Detection of 2019 novel coronavirus (2019-nCoV) by real-time
RT-PCR. Euro Surveill. 25(2000045)2020.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Chu DK, Pan Y, Cheng SM, Hui KP, Krishnan
P, Liu Y, Ng DY, Wan CKC, Yang P, Wang Q, et al: Molecular
diagnosis of a novel coronavirus (2019-nCoV) causing an outbreak of
pneumonia. Clin Chem. 66:549–555. 2020.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Xiao SY, Wu Y and Liu H: Evolving status
of the 2019 novel coronavirus infection: Proposal of conventional
serologic assays for disease diagnosis and infection monitoring. J
Med Virol. 92:464–467. 2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Tahmasebi S, Khosh E and Esmaeilzadeh A:
The outlook for diagnostic purposes of the 2019-novel coronavirus
disease. J Cell Physiol. 235:9211–9229. 2020.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Liu R, Liu X, Yuan L, Han H, Shereen MA,
Zhen J, Niu Z, Li D, Liu F, Wu K, et al: Analysis of adjunctive
serological detection to nucleic acid test for severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2) infection
diagnosis. Int Immunopharmacol. 86(106746)2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Perera RA, Mok CK, Tsang OT, Lv H, Ko RL,
Wu NC, Yuan M, Leung WS, Chan JM, Chik TS, et al: Serological
assays for severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2), March 2020. Euro Surveill. 25(2000421)2020.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Vieira MA, Vieira CP, Borba AS, Melo MC,
Oliveira MS, Melo RM, Nunes VV, Santana WS and Aguiar YA:
Sequential serological surveys in the early stages of the
coronavirus disease epidemic: Limitations and perspectives. Rev Soc
Bras Med Trop. 53(e20200351)2020.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Wang Q, Du Q, Guo B, Mu D, Lu X, Ma Q, Guo
Y, Fang L, Zhang B, Zhang G and Guo X: A method to prevent
SARS-CoV-2 IgM false positives in gold immunochromatography and
enzyme-linked immunosorbent assays. J Clin Microbiol. 58:e00375–20.
2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Thachil A, Gerber PF, Xiao CT, Huang YW
and Opriessnig T: Development and application of an ELISA for the
detection of porcine deltacoronavirus IgG antibodies. PLoS One.
10(e0124363)2015.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Zhao S, Smits C, Schuurman N, Barnum S,
Pusterla N, Kuppeveld FV, Bosch BJ, Maanen KV and Egberink H:
Development and validation of a S1 protein-based ELISA for the
specific detection of antibodies against equine coronavirus.
Viruses. 11(1109)2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Sunwoo HH, Palaniyappan A, Ganguly A,
Bhatnagar PK, Das D, El-Kadi AO and Suresh MR: Quantitative and
sensitive detection of the SARS-CoV spike protein using bispecific
monoclonal antibody-based enzyme-linked immunoassay. J Virol
Methods. 187:72–78. 2013.PubMed/NCBI View Article : Google Scholar
|
|
54
|
He Y, Lu H, Siddiqui P, Zhou Y and Jiang
S: Receptor-binding domain of severe acute respiratory syndrome
coronavirus spike protein contains multiple conformation-dependent
epitopes that induce highly potent neutralizing antibodies. J
Immunol. 174:4908–4915. 2005.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Lu H: Drug treatment options for the
2019-new coronavirus (2019-nCoV). Biosci Trends. 14:69–71.
2020.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Chu CM, Cheng VC, Hung IF, Wong MM, Chan
KH, Chan KS, Kao RY, Poon LL, Wong CL, Guan Y, et al: Role of
lopinavir/ritonavir in the treatment of SARS: Initial virological
and clinical findings. Thorax. 59:252–256. 2004.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Chan JF, Yao Y, Yeung ML, Deng W, Bao L,
Jia L, Li F, Xiao C, Gao H, Yu P, et al: Treatment with
Lopinavir/Ritonavir or Interferon-β1b improves outcome of MERS-CoV
infection in a nonhuman primate model of common marmoset. J Infect
Dis. 212:1904–1913. 2015.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Tu YF, Chien CS, Yarmishyn AA, Lin YY, Luo
YH, Lin YT, Lai WY, Yang DM, Chou SJ, Yang YP, et al: A Review of
SARS-CoV-2 and the ongoing clinical trials. Int J Mol Sci.
21(2657)2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Cao B, Zhang D and Wang C: A trial of
lopinavir-ritonavir in covid-19. Reply. N Engl J Med.
382(e68)2020.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Warren TK, Jordan R, Lo MK, Ray AS,
Mackman RL, Soloveva V, Siegel D, Perron M, Bannister R, Hui HC, et
al: Therapeutic efficacy of the small molecule GS-5734 against
Ebola virus in rhesus monkeys. Nature. 531:381–385. 2016.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Gordon CJ, Tchesnokov EP, Feng JY, Porter
DP and Gotte M: The antiviral compound remdesivir potently inhibits
RNA-dependent RNA polymerase from Middle East respiratory syndrome
coronavirus. J Biol Chem. 295:4773–4779. 2020.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Sheahan TP, Sims AC, Graham RL, Menachery
VD, Gralinski LE, Case JB, Leist SR, Pyrc K, Feng JY, Trantcheva I,
et al: Broad-spectrum antiviral GS-5734 inhibits both epidemic and
zoonotic coronaviruses. Sci Transl Med. 9(eaal3653)2017.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Martinez MA: Compounds with therapeutic
potential against novel respiratory 2019 coronavirus. Antimicrob
Agents Chemother. 64:e00399–20. 2020.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Jean SS, Lee PI and Hsueh PR: Treatment
options for COVID-19: The reality and challenges. J Microbiol
Immunol Infect. 53:436–443. 2020.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Lo MK, Jordan R, Arvey A, Sudhamsu J,
Shrivastava-Ranjan P, Hotard AL, Flint M, McMullan LK, Siegel D,
Clarke MO, et al: GS-5734 and its parent nucleoside analog inhibit
Filo-, Pneumo-, and Paramyxoviruses. Sci Rep.
7(43395)2017.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Mulangu S, Dodd LE, Davey RT Jr, Tshiani
Mbaya O, Proschan M, Mukadi D, Lusakibanza Manzo M, Nzolo D,
Tshomba Oloma A, Ibanda A, et al: A randomized, controlled trial of
ebola virus disease therapeutics. N Engl J Med. 381:2293–2303.
2019.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Brown AJ, Won JJ, Graham RL, Dinnon KH
III, Sims AC, Feng JY, Cihlar T, Denison MR, Baric RS and Sheahan
TP: Broad spectrum antiviral remdesivir inhibits human endemic and
zoonotic deltacoronaviruses with a highly divergent RNA dependent
RNA polymerase. Antiviral Res. 169(104541)2019.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Wang M, Cao R, Zhang L, Yang X, Liu J, Xu
M, Shi Z, Hu Z, Zhong W and Xiao G: Remdesivir and chloroquine
effectively inhibit the recently emerged novel coronavirus
(2019-nCoV) in vitro. Cell Res. 30:269–271. 2020.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Jordan PC, Stevens SK and Deval J:
Nucleosides for the treatment of respiratory RNA virus infections.
Antivir Chem Chemother. 26(2040206618764483)2018.PubMed/NCBI View Article : Google Scholar
|
|
70
|
de Wit E, Feldmann F, Cronin J, Jordan R,
Okumura A, Thomas T, Scott D, Cihlar T and Feldmann H: Prophylactic
and therapeutic remdesivir (GS-5734) treatment in the rhesus
macaque model of MERS-CoV infection. Proc Natl Acad Sci USA.
117:6771–6776. 2020.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Holshue ML, DeBolt C, Lindquist S, Lofy
KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural
A, et al: First Case of 2019 Novel Coronavirus in the United
States. N Engl J Med. 382:929–936. 2020.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Available from urihttps://times.hinet.net/mobile/news/22831665simplehttps://times.hinet.net/mobile/news/22831665.
|
|
73
|
Furuta Y, Komeno T and Nakamura T:
Favipiravir (T-705), a broad spectrum inhibitor of viral RNA
polymerase. Proc Jpn Acad Ser B Phys Biol Sci. 93:449–463.
2017.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Du YX and Chen XP: Favipiravir:
Pharmacokinetics and concerns about clinical trials for 2019-nCoV
infection. Clin Pharmacol Ther. 108:242–247. 2020.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Shannon A, Selisko B, Le N, Huchting J,
Touret F, Piorkowski G, Fattorini V, Ferron F, Decroly E, Meier C,
et al: Favipiravir strikes the SARS-CoV-2 at its Achilles heel, the
RNA polymerase. bioRxiv: May 15, 2020 (Epub ahead of print). doi:
10.1101/2020.05.15.098731.
|
|
76
|
Nagata T, Lefor AK, Hasegawa M and Ishii
M: Favipiravir: A new medication for the Ebola virus disease
pandemic. Disaster Med Public Health Prep. 9:79–81. 2015.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Dong L, Hu S and Gao J: Discovering drugs
to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther.
14:58–60. 2020.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Korea Biomedical Review. Physicians work
out treatment guidelines for coronavirus. 2020. Available from:
urihttp://www.koreabiomed.com/news/articleView.html?idxno=7428simplehttp://www.koreabiomed.com/news/articleView.html?idxno=7428.
|
|
79
|
Notice on Adjusting the Usage and Dosage
of Chloroquine Phosphate in Treating COVID-19 Pneumonia. Available
from: urihttp://www.nhc.gov.cn/yzygj/s7653p/202002/0293d017621941f6b2a4890035243730.shtmlsimplehttp://www.nhc.gov.cn/yzygj/s7653p/202002/0293d017621941f6b2a4890035243730.shtml.
|
|
80
|
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J,
Wang B, Xiang H, Cheng Z, Xiong Y, et al: Clinical characteristics
of 138 hospitalized patients with 2019 novel coronavirus-infected
pneumonia in Wuhan, China. JAMA. 323:1061–1069. 2020.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Yao X, Ye F, Zhang M, Cui C, Huang B, Niu
P, Liu X, Zhao L, Dong E, Song C, et al: In vitro antiviral
activity and projection of optimized dosing design of
hydroxychloroquine for the treatment of severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 71:732–739.
2020.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Liu J, Cao R, Xu M, Wang X, Zhang H, Hu H,
Li Y, Hu Z, Zhong W and Wang M: Hydroxychloroquine, a less toxic
derivative of chloroquine, is effective in inhibiting SARS-CoV-2
infection in vitro. Cell Discov. 6(16)2020.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Molina JM, Delaugerre C, Le Goff J,
Mela-Lima B, Ponscarme D, Goldwirt L and de Castro N: No evidence
of rapid antiviral clearance or clinical benefit with the
combination of hydroxychloroquine and azithromycin in patients with
severe COVID-19 infection. Med Mal Infect. 50(384)2020.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Gautret P, Lagier JC, Parola P, Hoang VT,
Meddeb L, Mailhe M, Doudier B, Courjon J, Giordanengo V, Vieira VE,
et al: Hydroxychloroquine and azithromycin as a treatment of
COVID-19: Results of an open-label non-randomized clinical trial.
Int J Antimicrob Agents. 56(105949)2020.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Interim clinical guidance for patients
suspected of/confirmed with Covid-19 in Belgium. Availabe from:
urihttps://epidemio.wiv-isp.be/ID/Documents/Covid19/COVID-19_InterimGuidelines_Treatment_ENG.pdf?fbclid=IwAR2PP0GEhBHm2m3zH7c-simplehttps://epidemio.wiv-isp.be/ID/Documents/Covid19/COVID-19_InterimGuidelines_Treatment_ENG.pdf?fbclid=IwAR2PP0GEhBHm2m3zH7c-.
|
|
86
|
Azioni intraprese per favorire la ricerca
e l'accesso ai nuovi farmaci per il trat-tamento del COVID-19.
Availabe from: urihttps://www.aifa.gov.it/-/azioni-intraprese-per-favorire-la-ricerca-e-l-accesso-ai-nuovi-farmaci-per-il-trattamento-del-covid-19simplehttps://www.aifa.gov.it/-/azioni-intraprese-per-favorire-la-ricerca-e-l-accesso-ai-nuovi-farmaci-per-il-trattamento-del-covid-19.
|
|
87
|
Hoffmann M, Mösbauer K, Hofmann-Winkler H,
Kaul A, Kleine-Weber H, Krüger N, Gassen NC, Müller MA, Drosten C
and Pöhlmann S: Chloroquine does not inhibit infection of human
lung cells with SARS-CoV-2. Nature. 585:588–590. 2020.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Maisonnasse P, Guedj J, Contreras V,
Behillil S, Solas C, Marlin R, Naninck T, Pizzorno A, Lemaitre J,
Gonçalves A, et al: Hydroxychloroquine use against SARS-CoV-2
infection in non-human primates. Nature. 585:584–587.
2020.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Zhang S, Li L, Shen A, Chen Y and Qi Z:
Rational use of tocilizumab in the treatment of novel coronavirus
pneumonia. Clin Drug Investig. 40:511–518. 2020.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Scott LJ: Tocilizumab: A review in
rheumatoid arthritis. Drugs. 77:1865–1879. 2017.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Venkiteshwaran A: Tocilizumab. MAbs.
1:432–438. 2009.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Triestall News. Coronavirus, will
‘To-cilizumab’ be the drug of hope? Available from: urihttps://www.triesteallnews.it/2020/03/14/coronavirus-will-tocilizumab-be-the-drug-of-hope/64simplehttps://www.triesteallnews.it/2020/03/14/coronavirus-will-tocilizumab-be-the-drug-of-hope/64.
|
|
93
|
Costanzo M, De Giglio MAR and Roviello GN:
SARS-CoV-2: Recent reports on antiviral therapies based on
lopinavir/ritonavir, darunavir/umifenovir, hydroxychloroquine,
remdesivir, favipiravir and other drugs for the treatment of the
new coronavirus. Curr Med Chem. 7:4536–4541. 2020.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Marinella MA: Routine antiemetic
prophylaxis with dexamethasone during COVID-19: Should oncologists
reconsider? J Oncol Pharm Pract. 26:1482–1485. 2020.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Andreakos E, Papadaki M and Serhan CN:
Dexamethasone, pro-resolving lipid mediators and resolution of
inflammation in COVID-19. Allergy: Sep 21, 2020 (Epub ahead of
print). doi: org/10.1111/all.14595.
|
|
96
|
Ledford H: Coronavirus breakthrough:
Dexamethasone is first drug shown to save lives. Nature.
582(469)2020.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Shang L, Zhao J, Hu Y, Du R and Cao B: On
the use of corticosteroids for 2019-nCoV pneumonia. Lancet.
395:683–684. 2020.PubMed/NCBI View Article : Google Scholar
|
|
98
|
Mehta P, McAuley DF, Brown M, Sanchez E,
Tattersall RS and Manson JJ: HLH Across Speciality Collaboration,
UK. COVID-19: Consider cytokine storm syndromes and
immunosuppression. Lancet. 395:1033–1034. 2020.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Youssef J, Novosad SA and Winthrop KL:
Infection risk and safety of corticosteroid use. Rheum Dis Clin
North Am. 42:157–176, ix-x. 2016.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Yang Z and Liu J, Zhou Y, Zhao X, Zhao Q
and Liu J: The effect of corticosteroid treatment on patients with
coronavirus infection: A systematic review and meta-analysis. J
Infect. 81:e13–e20. 2020.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Dong L, Xia JW, Gong Y, Chen Z, Yang HH,
Zhang J, He J and Chen XD: Effect of lianhuaqingwen capsules on
airway inflammation in patients with acute exacerbation of chronic
obstructive pulmonary disease. Evid Based Complement Alternat Med.
2014(637969)2014.PubMed/NCBI View Article : Google Scholar
|
|
102
|
Hu K, Guan WJ, Bi Y, Zhang W, Li L, Zhang
B, Liu Q, Song Y, Li X, Duan Z, et al: Efficacy and safety of
Lianhuaqingwen capsules, a repurposed Chinese herb, in patients
with coronavirus disease 2019: A multicenter, prospective,
randomized controlled trial. Phytomedicine: May 16, 2020 (Epub
ahead of print) doi: 10.1016/j.phymed.2020.153242.
|
|
103
|
Chen S: Clinical observation of Lianhua
Qingwen capsule combined with ribavirin injection in the treatment
of viral upper respiratory tract infection. Chin Community Doctors.
13(170)2011.
|
|
104
|
Zhao J, Tian SS, Yang J, Liu JF and Zhang
WD: Investigating mechanism of Qing-Fei-Pai-Du-Tang for treatment
of COVID-19 by network pharmacology. Chin Trad Herbal Drugs.
4:829–835. 2020.(In Chinese).
|
|
105
|
Ding Y, Zeng L, Li R, Chen Q, Zhou B, Chen
Q, Cheng PL, Yutao W, Zheng J, Yang Z and Zhang F: The Chinese
prescription lianhuaqingwen capsule exerts anti-influenza activity
through the inhibition of viral propagation and impacts immune
function. BMC Complement Altern Med. 17(130)2017.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Yang Y, Islam MS, Wang J, Li Y and Chen X:
Traditional Chinese medicine in the treatment of patients infected
with 2019-new coronavirus (SARS-CoV-2): A review and perspective.
Int J Biol Sci. 16:1708–1717. 2020.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Xin S, Cheng X, Zhu B, Liao X, Yang F,
Song L, Shi Y, Guan X, Su R, Wang J, et al: Clinical retrospective
study on the efficacy of Qingfei Paidu decoction combined with
Western medicine for COVID-19 treatment. Biomed Pharmacother.
129(110500)2020.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Yende S, Milbrandt EB, Kellum JA, Kong L,
Delude RL, Weissfeld LA and Angus DC: Understanding the potential
role of statins in pneumonia and sepsis. Crit Care Med.
39:1871–1878. 2011.PubMed/NCBI View Article : Google Scholar
|
|
109
|
Chrusciel P, Sahebkar A, Rembek-Wieliczko
M, Serban MC, Ursoniu S, Mikhailidis DP, Jones SR, Mosteoru S,
Blaha MJ, Martin SS, et al: Impact of statin therapy on plasma
adiponectin concentrations: A systematic review and meta-analysis
of 43 randomized controlled trial arms. Atherosclerosis.
253:194–208. 2016.PubMed/NCBI View Article : Google Scholar
|
|
110
|
Reiner Z, Hatamipour M, Banach M, Pirro M,
Al-Rasadi K, Jamialahmadi T, Radenkovic D, Montecucco F and
Sahebkar A: Statins and the COVID-19 main protease: In silico
evidence on direct interaction. Arch Med Sci. 16:490–496.
2020.PubMed/NCBI View Article : Google Scholar
|
|
111
|
Zhang XJ, Qin JJ, Cheng X, Shen L, Zhao
YC, Yuan Y, Lei F, Chen MM, Yang H, Bai L, et al: In-Hospital use
of statins is associated with a reduced risk of mortality among
individuals with COVID-19. Cell Metab. 32:176–187.e4.
2020.PubMed/NCBI View Article : Google Scholar
|
|
112
|
Pillaiyar T, Manickam M, Namasivayam V,
Hayashi Y and Jung SH: An overview of severe acute respiratory
syndrome-coronavirus (SARS-CoV) 3CL protease inhibitors:
Peptidomimetics and small molecule chemotherapy. J Med Chem.
59:6595–6628. 2016.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Jin Z, Zhao Y, Sun Y, Zhang B, Wang H, Wu
Y, Zhu Y, Zhu C, Hu T, Du X, et al: Structural basis for the
inhibition of SARS-CoV-2 main protease by antineoplastic drug
carmofur. Nat Struct Mol Biol. 27:529–532. 2020.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Jin Z, Du X, Xu Y, Deng Y, Liu M, Zhao Y,
Zhang B, Li X, Zhang L, Peng C, et al: Structure of M(pro) from
SARS-CoV-2 and discovery of its inhibitors. Nature. 582:289–293.
2020.PubMed/NCBI View Article : Google Scholar
|
|
115
|
Gupta S, Singh AK, Kushwaha PP, Prajapati
KS, Shuaib M, Senapati S and Kumar S: Identification of potential
natural inhibitors of SARS-CoV2 main protease by molecular docking
and simulation studies. J Biomol Struct Dyn: Jun 11, 2020 (Epub
ahead of print). doi: 10.1080/07391102.2020.1776157.
|
|
116
|
Wong SK, Li W, Moore MJ, Choe H and Farzan
M: A 193-amino acid fragment of the SARS coronavirus S protein
efficiently binds angiotensin-converting enzyme 2. J Biol Chem.
279:3197–3201. 2004.PubMed/NCBI View Article : Google Scholar
|
|
117
|
Ju B, Zhang Q, Ge J, Wang R, Sun J, Ge X,
Yu J, Shan S, Zhou B, Song S, et al: Human neutralizing antibodies
elicited by SARS-CoV-2 infection. Nature. 584:115–119.
2020.PubMed/NCBI View Article : Google Scholar
|
|
118
|
Robbiani DF, Gaebler C, Muecksch F,
Lorenzi JCC, Wang Z, Cho A, Agudelo M, Barnes CO, Gazumyan A,
Finkin S, et al: Convergent antibody responses to SARS-CoV-2 in
convalescent individuals. Nature. 584:437–442. 2020.PubMed/NCBI View Article : Google Scholar
|
|
119
|
Shi R, Shan C, Duan X, Chen Z, Liu P, Song
J, Song T, Bi X, Han C, Wu L, et al: A human neutralizing antibody
targets the receptor binding site of SARS-CoV-2. Nature.
584:120–124. 2020.PubMed/NCBI View Article : Google Scholar
|
|
120
|
Lei C, Qian K, Li T, Zhang S, Fu W, Ding M
and Hu S: Neutralization of SARS-CoV-2 spike pseudotyped virus by
recombinant ACE2-Ig. Nat Commun. 11(2070)2020.PubMed/NCBI View Article : Google Scholar
|
|
121
|
Kong Q, Wu Y, Gu Y, Lv Q, Qi F, Gong S and
Chen X: Analysis of the molecular mechanism of Pudilan (PDL)
treatment for COVID-19 by network pharmacology tools. Biomed
Pharmacother. 128(110316)2020.PubMed/NCBI View Article : Google Scholar
|
|
122
|
Kumar V, Dhanjal JK, Bhargava P, Kaul A,
Wang J, Zhang H, Kaul SC, Wadhwa R and Sundar D: Withanone and
Withaferin-A are predicted to interact with transmembrane protease
serine 2 (TMPRSS2) and block entry of SARS-CoV-2 into cells. J
Biomol Struct Dyn: Jun 16, 2020 (Epub ahead of print). doi:
10.1080/07391102.2020.1775704.
|
|
123
|
Rahman N, Basharat Z, Yousuf M, Castaldo
G, Rastrelli L and Khan H: Virtual screening of natural products
against type ii transmembrane serine protease (TMPRSS2), the
priming agent of coronavirus 2 (SARS-CoV-2). Molecules.
25(2271)2020.PubMed/NCBI View Article : Google Scholar
|
|
124
|
Xu K, Cai H, Shen Y, Ni Q, Chen Y, Hu S,
Li J, Wang H, Yu L, Huang H, et al: Management of corona virus
disease-19 (COVID-19): The Zhejiang experience. Zhejiang Da Xue Xue
Bao Yi Xue Ban. 49:147–157. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
125
|
Morais AHA, Passos TS, Maciel BLL and da
Silva Maia JK: Can probiotics and diet promote beneficial immune
modulation and purine control in coronavirus infection? Nutrients.
12(1737)2020.PubMed/NCBI View Article : Google Scholar
|
|
126
|
Sharifi-Rad J, Rodrigues CF,
Stojanovic-Radic Z, Dimitrijević M, Aleksić A, Neffe-Skocińska K,
Zielińska D, Kołożyn-Krajewska D, Salehi B, Milton Prabu S, et al:
Probiotics: Versatile bioactive components in promoting human
health. Medicina (Kaunas). 56(433)2020.PubMed/NCBI View Article : Google Scholar
|
|
127
|
Infusino F, Marazzato M, Mancone M, Fedele
F, Mastroianni CM, Severino P, Ceccarelli G, Santinelli L,
Cavarretta E, Marullo AGM, et al: Diet supplementation, probiotics,
and nutraceuticals in SARS-CoV-2 infection: A scoping review.
Nutrients. 12(1718)2020.PubMed/NCBI View Article : Google Scholar
|
|
128
|
Wang M, Luo L, Bu H and Xia H: One case of
coronavirus disease 2019 (COVID-19) in a patient co-infected by HIV
with a low CD4+ T-cell count. Int J Infect Dis. 96:148–150.
2020.PubMed/NCBI View Article : Google Scholar
|
|
129
|
Luo Y, Xie Y, Zhang W, Lin Q, Tang G, Wu
S, Huang M, Yin B, Huang J, Wei W, et al: Combination of lymphocyte
number and function in evaluating host immunity. Aging (Albany NY).
11:12685–12707. 2019.PubMed/NCBI View Article : Google Scholar
|
|
130
|
Chen X, Liao B, Cheng L, Peng X, Xu X, Li
Y, Hu T, Li J, Zhou X and Ren B: The microbial coinfection in
COVID-19. Appl Microbiol Biotechnol. 104:7777–7785. 2020.PubMed/NCBI View Article : Google Scholar
|
|
131
|
Zhang G, Hu C, Luo L, Fang F, Chen Y, Li
J, Peng Z and Pan H: Clinical features and short-term outcomes of
221 patients with COVID-19 in Wuhan, China. J Clin Virol.
127(104364)2020.PubMed/NCBI View Article : Google Scholar
|
|
132
|
Wu JH, Li X, Huang B, Su H, Li Y, Luo DJ,
Chen S, Ma L, Wang SH, Nie X and Peng L: Pathological changes of
fatal coronavirus disease 2019 (COVID-19) in the lungs: Report of
10 cases by postmortem needle autopsy. Zhonghua Bing Li Xue Za Zhi.
49:568–575. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
133
|
Wang Z, Hu X, Li Z, Tu C, Wang Y, Pang P,
Zhang H, Zheng X, Liang Y, Shan H and Liu J: Effect of SARS-CoV-2
infection on the microbial composition of upper airway. Infect Drug
Resist. 13:2637–2640. 2020.PubMed/NCBI View Article : Google Scholar
|
|
134
|
Piva S, Filippini M, Turla F, Cattaneo S,
Margola A, De Fulviis S, Nardiello I, Beretta A, Ferrari L, Trotta
R, et al: Clinical presentation and initial management critically
ill patients with severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) infection in Brescia, Italy. J Crit Care. 58:29–33.
2020.PubMed/NCBI View Article : Google Scholar
|
|
135
|
Renteria AE, Endam Mfuna L, Adam D,
Filali-Mouhim A, Maniakas A, Rousseau S, Brochiero E, Gallo S and
Desrosiers M: Azithromycin downregulates gene expression of IL-1β
and pathways involving TMPRSS2 and TMPRSS11D required by
SARS-CoV-2. Am J Respir Cell Mol Biol. 63:707–709. 2020.PubMed/NCBI View Article : Google Scholar
|
|
136
|
Fanin A, Calegari J, Beverina A and
Tiraboschi S: Gruppo di Autoformazione Metodologica (GrAM).
Hydroxychloroquine and azithromycin as a treatment of COVID-19.
Intern Emerg Med. 15:841–843. 2020.PubMed/NCBI View Article : Google Scholar
|
|
137
|
Parra-Lara LG, Martinez-Arboleda JJ and
Rosso F: Azithromycin and SARS-CoV-2 infection: Where we are now
and where we are going. J Glob Antimicrob Resist. 22:680–684.
2020.PubMed/NCBI View Article : Google Scholar
|
|
138
|
Ardal C, Balasegaram M, Laxminarayan R,
McAdams D, Outterson K, Rex JH and Sumpradit N: Antibiotic
development-economic, regulatory and societal challenges. Nat Rev
Microbiol. 18:267–274. 2020.PubMed/NCBI View Article : Google Scholar
|
|
139
|
World Health Organization. Draft landscape
of COVID-19 vaccine candidates. Available from: urihttps://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccinessimplehttps://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines.
|
|
140
|
Krammer F: SARS-CoV-2 vaccines in
development. Nature. 586:516–527. 2020.PubMed/NCBI View Article : Google Scholar
|
|
141
|
Bai ZH, Li XR, Wang RB, LIU XR, et al:
Review of industrialized production technology of human inactivated
vaccine based on mammalian cell culture. Chin J Cell Biol.
41:1986–1993. 2019.
|
|
142
|
Gao Q, Bao L, Mao H, Wang L, Xu K, Yang M,
Li Y, Zhu L, Wang N, Lv Z, et al: Development of an inactivated
vaccine candidate for SARS-CoV-2. Science. 369:77–81.
2020.PubMed/NCBI View Article : Google Scholar
|
|
143
|
World's First Phase III clinical trial of
COVID-19 inactivated vaccine begins in UAE. Journal 2020. Available
from: urihttps://www.businesswire.com/news/home/20200717005085/en/simplehttps://www.businesswire.com/news/home/20200717005085/en/.
|
|
144
|
Sinovac. Safety and immunogenicity study
of inactivated vaccine for prophylaxis of SARS-CoV-2 infection
(COVID-19). 2020-04-20. Available from: urihttps://clinicaltrials.gov/ct2/show/NCT04352608?cond=COVID+vaccine&draw=2simplehttps://clinicaltrials.gov/ct2/show/NCT04352608?cond=COVID+vaccine&draw=2.
|
|
145
|
Sinovac. Safety and immunogenicity study
of inactivated vaccine for prophylaxis of SARS-CoV-2 infection
(COVID-19). 2020-05-12. Available from: urihttps://clinicaltrials.gov/ct2/show/NCT04383574simplehttps://clinicaltrials.gov/ct2/show/NCT04383574.
|
|
146
|
Wan Y, Shang J, Sun S, Tai W, Chen J, Geng
Q, He L, Chen Y, Wu J, Shi Z, et al: Molecular mechanism for
antibody-dependent enhancement of coronavirus entry. J Virol.
94:e02015–19. 2020.PubMed/NCBI View Article : Google Scholar
|
|
147
|
Guo ZY, Liu J and Liu X: Progress in
severe acute respiratory syndrome coronavirus 2 vaccine. Chin J
Viral Dis. 10:249–254. 2020.
|
|
148
|
A Study Looking at the Effectiveness and
Safety of a COVID-19 Vaccine in South African Adults. (2020-08-31).
Available from: urihttps://clinicaltrials.gov/ct2/show/NCT04533399?term=vaccine&cond=covid-19&draw=7simplehttps://clinicaltrials.gov/ct2/show/NCT04533399?term=vaccine&cond=covid-19&draw=7.
|
|
149
|
Clover Initiates Phase 1 Clinical Trial
for COVID-19 Vaccine Candidate. (2020-06-19). Available from:
urihttp://www.cloverbiopharma.com/index.php?m=content&c=index&a=show&catid=11&id=48&langId=1simplehttp://www.cloverbiopharma.com/index.php?m=content&c=index&a=show&catid=11&id=48&langId=1.
|
|
150
|
Geall AJ, Mandl CW and Ulmer JB: RNA: The
new revolution in nucleic acid vaccines. Semin Immunol. 25:152–159.
2013.PubMed/NCBI View Article : Google Scholar
|
|
151
|
Ferraro B, Morrow MP, Hutnick NA, Shin TH,
Lucke CE and Weiner DB: Clinical applications of DNA vaccines:
Current progress. Clin Infect Dis. 53:296–302. 2011.PubMed/NCBI View Article : Google Scholar
|
|
152
|
Mclvor RS: Therapeutic delivery of mRNA:
The medium is the message. Mol Ther. 19:822–823. 2011.PubMed/NCBI View Article : Google Scholar
|
|
153
|
Moderna Announces Phase 3 COVE Study of
mRNA Vaccine Against COVID-19 (mRNA-1273) Begins. (2020-07-27).
Available from: urihttps://investors.modernatx.com/news-releases/news-release-details/moderna-announces-phase-3-cove-study-mrna-vaccine-against-covidsimplehttps://investors.modernatx.com/news-releases/news-release-details/moderna-announces-phase-3-cove-study-mrna-vaccine-against-covid.
|
|
154
|
Study to Describe the Safety, Tolerability
Immunogenicity, Efficacy of RNA Vaccine Candidates Against COVID-19
in Healthy Adults. (2020-09-29). Available from: urihttps://clinicaltrials.gov/ct2/show/NCT04368728simplehttps://clinicaltrials.gov/ct2/show/NCT04368728.
|
|
155
|
COVID-19 vaccine developed by military
medical academy approved for clinical trials. Available from:
urihttp://www.chinadaily.com.cn/a/202003/17/WS5e70b732a31012821727fd62.htmsimplehttp://www.chinadaily.com.cn/a/202003/17/WS5e70b732a31012821727fd62.htm.
|
|
156
|
Zhu FC, Li YH, Guan XH, Hou LH, Wang WJ,
Li JX, Wu SP, Wang BS, Wang Z, Wang L, et al: Safety, tolerability,
and immunogenicity of a recombinant adenovirus type-5 vectored
COVID-19 vaccine: A dose-escalation, open-label, non-randomised,
first-in-human trial. Lancet. 395:1845–1854. 2020.PubMed/NCBI View Article : Google Scholar
|
|
157
|
Li X, Giorgi EE, Marichannegowda MH, Foley
B, Xiao C, Kong XP, Chen Y, Gnanakaran S, Korber B and Gao F:
Emergence of SARS-CoV-2 through recombination and strong purifying
selection. Sci Adv. 6(eabb9153)2020.PubMed/NCBI View Article : Google Scholar
|
|
158
|
Han G and Zhou YH: Possibly critical role
of wearing masks in general population in controlling COVID-19. J
Med Virol: Apr 15, 2020 (Epub ahead of print). doi:
10.1002/jmv.25886.
|
|
159
|
Rabaan AA, Al-Ahmed SH, Sah R, Tiwari R,
Yatoo MI, Patel SK, Pathak M, Malik YS, Dhama K, Singh KP, et al:
SARS-CoV-2/COVID-19 and advances in developing potential
therapeutics and vaccines to counter this emerging pandemic. Ann
Clin Microbiol Antimicrob. 19(40)2020.PubMed/NCBI View Article : Google Scholar
|
|
160
|
Calina D, Hartung T, Docea AO, Spandidos
DA, Egorov AM, Shtilman MI, Carvalho F and Tsatsakis A: COVID-19
vaccines: Ethical framework concerning human challenge studies.
Daru: Aug 27, 2020 (Epub ahead of print). doi:
10.1007/s40199-020-00371-8.
|