Introduction
Pituitary adenoma (PA) is a common benign tumor in
neurosurgery that ranks third among brain tumors (1). Pituitary adenomas are overwhelmingly
of soft consistency; thus, typical methods of resection with
curettage and suction appear to be clinically efficient (2-5).
Tumors of the pituitary gland and sellar region account for 15% of
all brain tumors (6-8).
The most common tumors are by far pituitary adenomas and benign
neuroendocrine neoplasms confined to the sella (9). Early diagnosis of pituitary tumors is
highly significant and their proper classification is of paramount
importance for treatment and prognostic purposes (10). The initial treatment of pituitary
adenomas includes surgery and certain cases may require
chemotherapy with somatostatin analogs, cabergoline and/or
pegvisomant (11-13).
Compression of and invasion to surrounding structures by PA,
including the sella, optic chiasm, optic nerve, cavernous sinus,
skull base and brain-stem, may result in serious obstruction of the
corresponding organ functions. Tumor texture is considered an
important factor influencing the rate of surgical resection
(14,15).
In surgery, tumor consistency is one of the most
important factors that affect surgical difficulty and safety.
Therefore, accurately predicting tumor texture may preoperatively
guide surgeons in risk assessment and surgical planning (16). The soft and firm consistencies of
tumors directly affect the degree of tumor resection (17,18).
Previous studies indicated that preoperative MRI signals may
predict tumor consistency (18-20).
However, tumor consistency remains controversial and deserves
further investigation. A previous study demonstrated that low
signal intensity on T2-weighted imaging (T2-WI) MRI is correlated
with increased collagen content at pathologic diagnosis, and
therefore, fibrous consistency (3).
Pierallini et al (5) pointed out that signal intensity on
diffusion-weighted imaging (DWI) is associated with the collagen
content on pathologic examination. However, other studies indicated
no statistically significant correlation between consistency and
imaging (1,3,21,22).
Of note, collagen types I and III are highly
important in pituitary adenomas (21), while differences in collagen
composition between soft and firm pituitary tumors have remained
largely elusive.
In previous studies on the texture of pituitary
tumors, quantitative analysis with immunofluorescence was rarely
used for evaluating the collagen content. Furthermore, whether T2WI
is able to predict tumor texture has remained controversial
(20). Therefore, the present study
aimed to evaluate the levels of collagen types I and III in
pituitary adenomas with different consistencies using
immunofluorescence. In addition, the significance of T2-weighted
imaging (T2WI) sequences in predicting tumor consistency was
highlighted.
Materials and methods
Patients
In the present prospective study, 55 patients with
pituitary tumors, who were admitted to Beijing Tiantan Hospital,
Capital Medical University (Beijing, China) between September 2018
and March 2019, were recruited. The patients' demographic and
clinical data, including sex, age at surgery, clinical subtypes and
Knosp grade (23) were recorded.
All patients underwent transphenoidal or transcranial surgery.
During surgery, the consistency category (soft or firm) was
determined by two experienced neurosurgeons with >20 years of
experience in pituitary tumor surgery. Adenomas that were easily
removed in the standard fashion with curettage and suction were
considered soft tumors. Those resistant to removal by curettage or
requiring adjuvant methods were considered firm tumors. Patients
with microadenoma, tumor cysts or stroke were excluded. The study
was approved by the Ethics Committee of Beijing Tiantan Hospital,
Capital Medical University (Beijing, China) and informed consent
was obtained from each patient or their relatives.
Immunofluorescence
Tissue sections (thickness, 4-µm) were dewaxed in
xylene and dehydrated by an ethanol gradient. Citrate buffer (pH
6.0) was used for antigen retrieval by boiling for 2 min. After
incubation with 0.25% PBS containing Triton X for 15 min, sheep
serum (10%; ZLI-9021; OriGene Technologies, Inc.) was added for
blocking at 37˚C for 30 min, followed by successive incubations
with primary (overnight, 4˚C) and secondary (room temperature, 60
min in the dark) antibodies. Primary antibodies were for COLIII
(cat. no. ab23445) and COLI (cat. no. ab90395; both from Abcam).
The secondary antibody was goat anti-mouse fluorescein
isothiocyanate-labeled IgG (1:100; cat. no. ZF-0312; OriGene
Technologies, Inc.). Furthermore, 4',6-diamidino-2-phenylindole
(DAPI) was used for counterstaining. Fluorescence microscopy was
used for imaging and microscopic settings were kept stable
throughout the imaging. The intensity of green fluorescence signals
in each section was measured using Image-J software (v1.52;
National Institutes of Health). The contents of collagen types I
and III were determined as average optical density (AOD) values.
First, fluorescent micrographs were converted into 8-bit grayscale
images and inverted to white. Subsequently, measurements (set area,
integrated density and limit to the threshold) were set via
adjusting for thresholds (lower and upper threshold levels were set
to 2.71 and 0.01, respectively). Finally, the integrated density
and the sum of the original green fluorescence areas were measured.
The AOD was calculated by dividing the integrated optical density
(sum) by the area (sum).
MRI
All MRI examinations were performed on a Siemens 3.0
T MRI system (Siemens Healthineers AG). The parameters used for
conventional MRI were repetition time of 3000 msec and echo time of
98 msec. The OsiriX Lite system (v10.0; Pixmeo Sàrl) was used to
analyze MRI data. A region of interest (ROI) was selected within
the lesion for homogenous adenomas, while multiple ROIs were
selected for heterogeneous lesions and their mean intensity was
calculated. An ROI from the pons was selected and the mean
intensity was determined. The ratios of tumor to pons signal
intensities on T2WI were calculated. The maximum diameter of each
tumor was also determined by MRI preoperatively.
Statistical analysis
All statistical analyses were performed using SPSS
25.0 software (IBM Corp.). GraphPad Prism 7 (GraphPad Software,
Inc.) was used to plot figures and the receiver operating
characteristic (ROC) curve. Continuous variables were expressed as
the mean ± standard deviation or median with interquartile ranges.
Categorical variables were expressed as n (%). The two-samples
t-test or the Mann-Whitney U test was employed to determine
significant differences between the two groups for continuous data.
Pearson's χ2 and Fisher's exact tests were utilized to
assess the differences in proportions between groups. Pearson's
correlation analysis was used to investigate the relationship
between two individual variables. A two-sided P<0.05 was
considered to indicate statistical significance. The ROC curve was
plotted to evaluate the significance of signal intensity on T2WI
images to predict tumor consistency. An area under the ROC curve
(AUC) of >0.7 was considered to indicate a certain predictive
value.
Results
Demographics and clinical
characteristics
The intraoperative consistency of each tumor was
recorded based on resection characteristics and ease of adenoma
removal. There were 36 soft and 19 firm tumors and the patients
were grouped accordingly. The patients included 29 males and 26
females, with a mean age at diagnosis of 47.9±12.7 years (range,
17-72 years). Of the 55 patients, 12 had hypopituitarism prior to
surgery. In addition, 39 (71%) were categorized as Knosp grade 3-4,
while 16 (29%) were grade 0-2. There were 25 (45%) patients with
suprasellar extension, according to MRI findings. The clinical
manifestations and preoperative endocrinological examination
results indicated that 42 (76%) cases had non-functional pituitary
adenomas. The distribution of soft and firm tumors was different
between functional and non-functional pituitary adenomas (P=0.046).
The major clinical manifestations were visual disturbance (38.2%)
and visual field defect (32.7%). The detailed demographic and
clinical features are presented in Table I.
 | Table ICharacteristics of the patients with
soft and firm tumors. |
Table I
Characteristics of the patients with
soft and firm tumors.
| Item | Soft (n=36) | Firm (n=19) | P-value |
|---|
| Age (years) | 47.2±12.6 | 49.3±13.5 | 0.575 |
| Sex | | | 0.024 |
|
Male | 15 (41.7) | 14 (72.7) | |
|
Female | 21 (58.3) | 5 (26.3) | |
| Clinical
subtype | | | 0.046 |
|
Functional | 12 (33.3) | 1 (5.3) | |
|
Non-functional | 24 (66.7) | 18 (94.7) | |
|
Hypopituitarism | | | 0.733 |
|
Yes | 7 (19.4) | 5 (26.3) | |
|
No | 29 (80.6) | 14 (72.7) | |
| Knosp grade | | | 0.406 |
|
0 | 4 (11.1) | 0 (0.0) | |
|
1 | 4 (11.1) | 1 (5.3) | |
|
2 | 3 (8.3) | 4 (21.1) | |
|
3 | 15 (41.7) | 4 (21.1) | |
|
4 | 10 (27.8) | 10 (52.7) | |
| Suprasellar
extension | | | 0.057 |
|
Yes | 13 (36.1) | 12 (63.2) | |
|
No | 23 (63.9) | 7 (36.8) | |
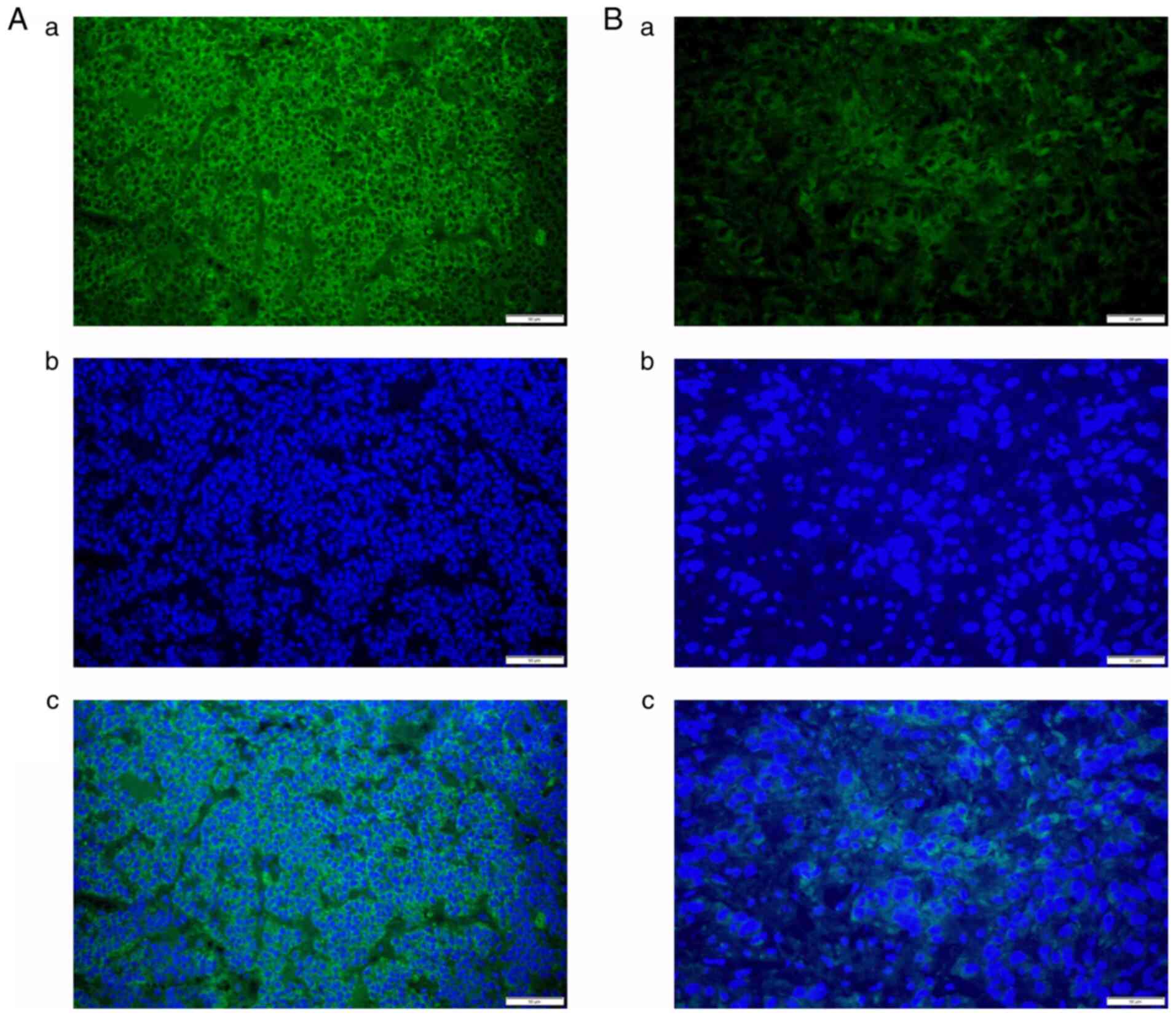
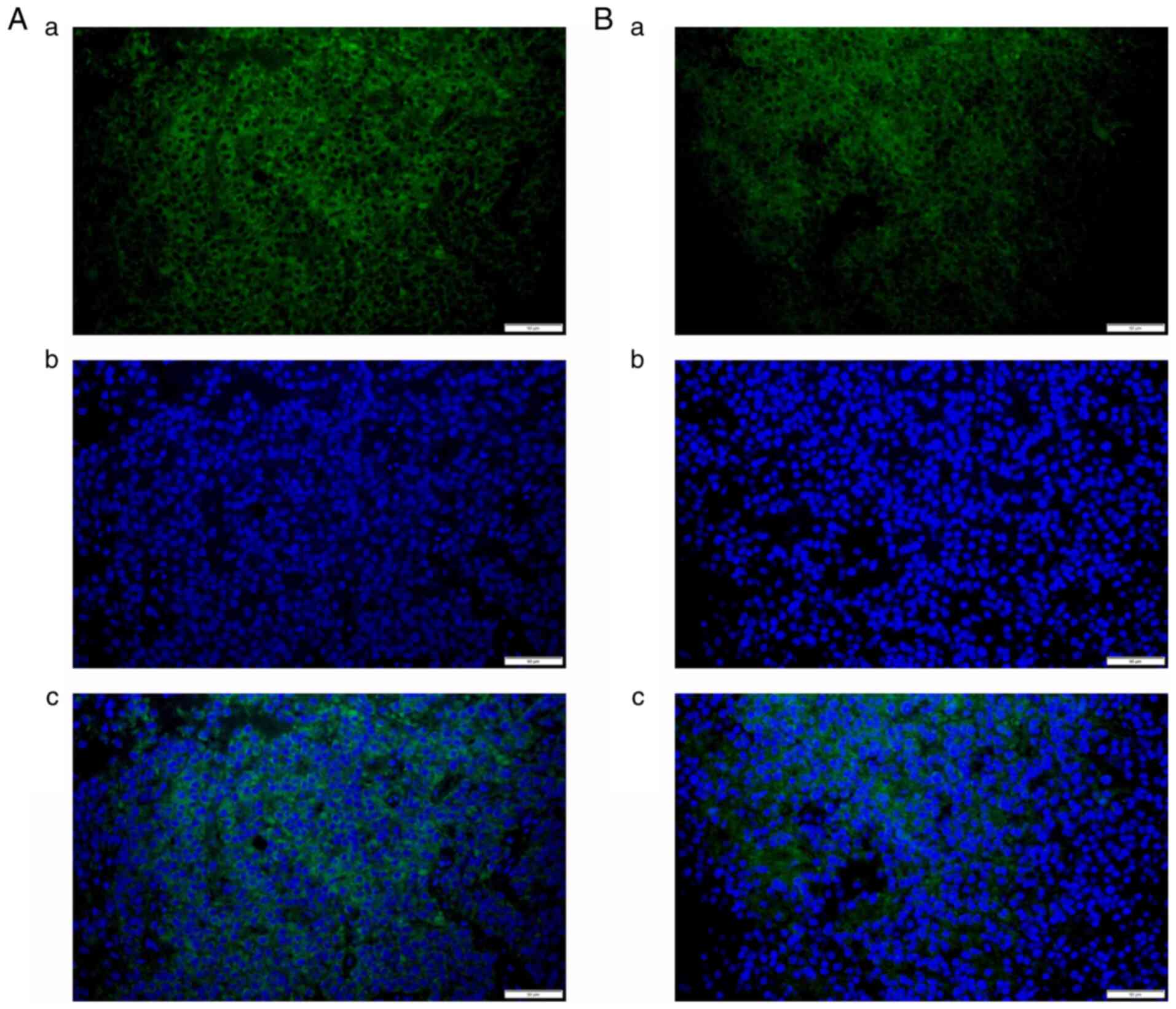
Expression levels of collagen types I
and III
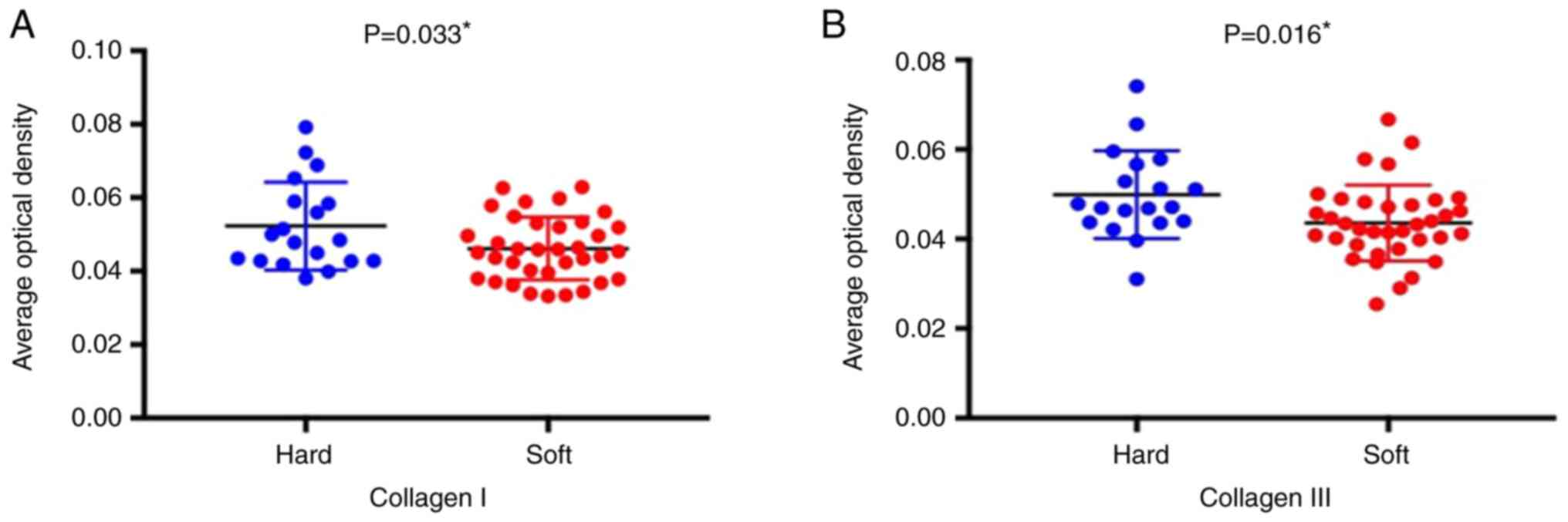
The contents of collagen types I (Fig. 1) and III (Fig. 2) were detected using staining in all
55 cases as green signals by immunofluorescence. AOD values for
collagen types I (0.046±0.008 vs. 0.052±0.012, P=0.033) and III
(0.044±0.008 vs. 0.050±0.010, P=0.016) were significantly lower in
the soft tumor group compared with those in the firm tumor group
(Fig. 3). AOD values for collagen
types I and III exhibited a significant correlation (P<0.001),
with a correlation coefficient of 0.986 (Fig. 3).
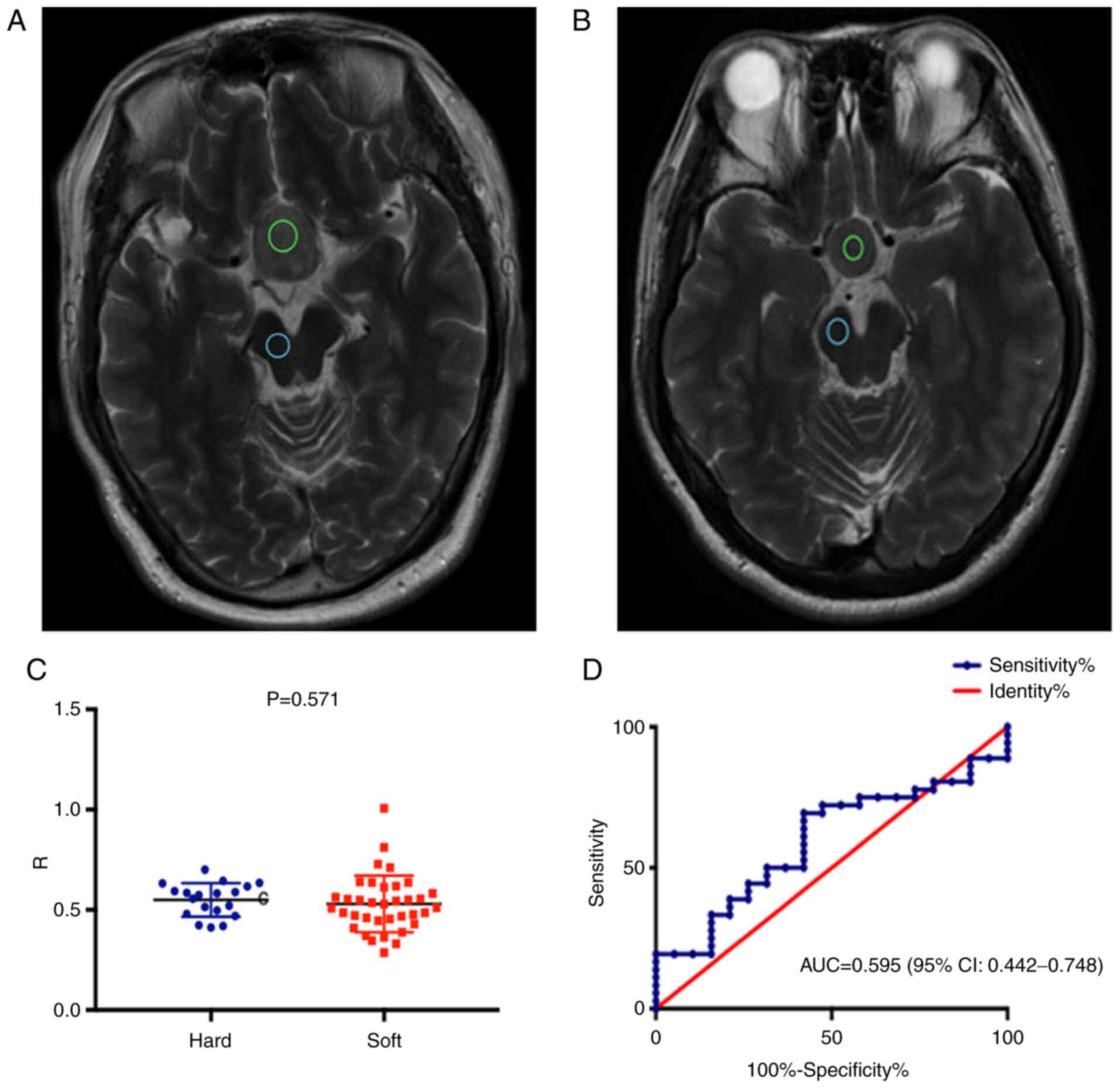
T2WI MRI signals are similar in the
soft and firm tumor groups
There was no significant difference in the ratio of
tumor to Pons' T2WI MRI signal intensities between the soft and
firm tumor groups. The ROC curve demonstrated no predictive value
for this ratio regarding tumor consistency [AUC=0.595 (95% CI:
0.442-0.748); P=0.250; Fig. 4]. The
median maximum tumor diameter was 2.82 (2.07, 3.25) cm. There was a
statistically significant difference in the maximum tumor diameter
between the soft [2.38 (2.01, 2.99) cm] and firm [3.25 (2.92, 3.68)
cm] tumor groups (P=0.001; Table
II).
| Table IITumor to Pons' signal intensities and
tumor diameters in the soft and firm tumor groups. |
Table II
Tumor to Pons' signal intensities and
tumor diameters in the soft and firm tumor groups.
| Item | Soft (n=36) | Firm (n=19) | P-value |
|---|
| Ratio of the tumor
to Pons' T2WI MRI signal intensities | 0.53±0.14 | 0.55±0.08 | 0.571 |
| Maximum diameter
(cm) | 2.38
(2.01,2.99) | 3.25
(2.92,3.68) | 0.001 |
Discussion
The present prospective study strongly suggested
that the levels of collagen types I and III were higher in the firm
tumor group compared with those in the soft tumor group. The size
of pituitary adenomas defined by T2WI may be associated with the
collagen content, while the ratio of tumor to Pons' signal
intensities on T2WI scans were not able to predict tumor
consistency.
Previous studies employed immunohistochemistry for
determining collagen content in tumors (3,24,25).
In the present study, immunofluorescence was applied and ImageJ
software was used to analyze the amounts of collagen types I and
III. Fibrillar collagen consists of types I, II, III, V and XI. Of
these, collagen types I, III and V are mainly detected in stromal
connective tissues, whereas collagen types II and XI are found in
cartilaginous tissues (21).
Type I collagen is the major component of the
extracellular matrix in the skin, bone and ligaments, while type
III collagen, an important structural protein, is one of the major
fibrillar collagens (26). The
expression of type III collagen was previously assessed in various
benign and malignant tumors by immunostaining (27). In the present study, collagen types
I and III were detected in all cases. Collagen types I and III are
at times detected in the same fibrils (28,29).
Increased expression of collagen type III is observed in several
human fibrotic diseases. Collagen type III is known to interact
with collagen types I and II in fibril formation and may regulate
fibril diameter (27).
The present results suggested that the expression
levels of collagen types I and III were higher in firm pituitary
adenomas compared with those in soft pituitary adenomas. These
results suggest that the collagen content may reflect the firmness
of adenomas detected during the operation. According to Pearson
correlation analysis, the maximum tumor diameter and collagen
content were significantly correlated. Consistent with previous
studies (27,29), the present study demonstrated that
fibrous tumors may have a larger volume than soft ones. To the best
of our knowledge, the secretion and architecture of collagens in
tumors are influenced by mutations in tumor suppressor genes
(30). Therefore, tumors with high
production of collagen may be larger. Various molecules in tumors
with high amounts of collagens are associated with cell activity
modulation toward more aggressive features (31-33).
Different types of cells, including immune cells and fibroblasts,
are also present within tumors and participate in the tumor's
immune escape and mutual feedback loops that may lead to cancer
recurrence (34,35). High collagen content in breast
cancer was reported to suppress the proliferation of T cells
(36). Therefore, tumors with high
amounts of collagens are not only larger and firmer compared with
adenomas, but also more likely to have aggressive features. This
should be considered in patient management on an individual basis.
Importantly, firm but small tumors may be easier to resect, as they
may be limited to the gland.
MRI T2WI signals have a significant role in
predicting tumor consistency prior to surgery. Although T2WI was
demonstrated to be able to predict the consistency and texture of
pituitary adenomas (3,16,21,37,38),
opposite results have been previously reported (18-20).
In the present prospective study, the ratios of the tumor to Pons'
signal intensities on T2WI scans were similar in the firm and soft
tumor groups. The present results were consistent with those
reported by Thotakura et al (39), who demonstrated that it was not
possible to reliably predict the consistency of pituitary adenomas
by preoperative MRI. In agreement with this, Mastorakos et
al (40) pointed out that the
ratio of tumor to cerebellar peduncle T2-WI intensity is not
associated with tumor consistency. Furthermore, Bahuleyan et
al (2) concluded that the
consistency of pituitary macroadenomas was not able to be
accurately predicted based on MRI signal intensity. However, MRI
sequences may provide more information. DWI may be used for
determining the texture of adenomas (16), as well as the Fast Imaging Employing
Steady-State Acquisition sequence (41). High-resolution MRI using high-power
magnetic fields was also reported to be predictive of texture
(42). In future studies, multiple
MRI sequences and their associations with collagen content and
adenoma consistency require to be assessed. A combination of those
sequences may assist in determining the consistency of tumors and
performing therapeutic management.
According to the MRI findings of the present study,
63.2% of patients with firm tumors had suprasellar extension
lesions vs. 36.1% in the soft tumor group. In the firm tumor group,
it was difficult to remove the lesions in the suprasellar region.
Koktekir et al (43)
described the successful use of a transventricular endoscope as an
adjunctive measure to remove giant pituitary adenomas by the
transsphenoidal approach. They concluded that this technique may be
safely used in selected cases. Case selection and surgical
strategies should be based on pre-operative MRI findings,
ventricular size and the availability of experienced surgeons.
The present study had a number of limitations.
First, it was a single-center trial with small sample size, and it
was not possible to adjust for important confounders in the
statistical analysis, e.g., sex. Thus, larger studies are required
to confirm the present findings. In addition, certain tumors had
uneven consistency and the specimens may not completely represent
the entire tumor. Furthermore, the results indicated that most of
the functional pituitary adenomas were soft and most of the
non-functional pituitary adenomas were firm. Studies with a larger
cohort size are also required to confirm the present results.
In conclusion, the present prospective study
demonstrated that the levels of collagen types I and III were
higher in pituitary tumors with firm consistency compared with
those with soft lesions. In addition, the size of pituitary
adenomas observed by MRI was correlated with the amounts of
collagen types I and III, and the ratio of tumor to Pons' signal
intensities on T2WI scans was not able to predict tumor
consistency.
Acknowledgements
The authors thank Professor Wang Jia from The
Department of Neurosurgery of Beijing Tiantan Hospital, Capital
Medical University (Beijing, China) for constructive comments and
suggestions.
Funding
Funding: The present study was supported by the Capital's Funds
for Health Improvement and Research (grant no. CFH2018-1-1071) and
National Natural Science Foundation of China (grant no.
NSFC82071996).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PL and DZ supervised the study. PL, WJ and PK
designed the experiments. PL, SM, BM and WZ performed the
experiments. CZ and JD provided new tools and reagents and
performed part of data analysis. XW, DZ and JP analyzed the data.
PL, YW and LY drafted the manuscript and acquired the clinical
data. DZ and WJ revised the manuscript. DZ and CZ confirm the
authenticity of all the raw data. All have authors read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
The study was approved by The Ethics Committee of
Beijing Tiantan Hospital, Capital Medical University (Beijing,
China) and informed consent was obtained from each patient or their
relatives.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jane JA Jr and Laws ER Jr: The surgical
management of pituitary adenomas in a series of 3,093 patients. J
Am Coll Surg. 193:651–659. 2001.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bahuleyan B, Raghuram L, Rajshekhar V and
Chacko AG: To assess the ability of MRI to predict consistency of
pituitary macroadenomas. Br J Neurosurg. 20:324–326.
2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Iuchi T, Saeki N, Tanaka M, Sunami K and
Yamaura A: MRI prediction of fibrous pituitary adenomas. Acta
Neurochir (Wien). 140:779–786. 1998.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mahmoud OM, Tominaga A, Amatya VJ, Ohtaki
M, Sugiyama K, Sakoguchi T, Kinoshita Y, Takeshima Y, Abe N,
Akiyama Y, et al: Role of PROPELLER diffusion-weighted imaging and
apparent diffusion coefficient in the evaluation of pituitary
adenomas. Eur J Radiol. 80:412–417. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Pierallini A, Caramia F, Falcone C,
Tinelli E, Paonessa A, Ciddio AB, Fiorelli M, Bianco F, Natalizi S,
Ferrante L and Bozzao L: Pituitary macroadenomas: Preoperative
evaluation of consistency with diffusion-weighted MR
imaging-initial experience. Radiology. 239:223–231. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sen A, Das C, Mukhopadhyay M, Mukhopadhyay
S, Deb S and Mukhopadhyay B: Cytohistological correlation in
pituitary tumor and immunological assessment with the help of
Ki-67. J Postgrad Med. 63:96–99. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bidari-Zerehpoosh F, Sharifi G, Novin K
and Mortazavi N: Invasive growth hormone producing pituitary
adenoma with lymphocytic infiltration: A case report and literature
review. Iran J Cancer Prev. 8(e3504)2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Jin G, Hao S, Xie J, Mi R and Liu F:
Collision tumors of the sella: Coexistence of pituitary adenoma and
craniopharyngioma in the sellar region. World J Surg Oncol.
11(178)2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Mete O and Lopes MB: Overview of the 2017
WHO classification of pituitary tumors. Endocr Pathol. 28:228–243.
2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lopes MB: Growth hormone-secreting
adenomas: Pathology and cell biology. Neurosurg Focus.
29(E2)2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Molitch ME: Diagnosis and treatment of
pituitary adenomas: A review. JAMA. 317:516–524. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Theodros D, Patel M, Ruzevick J, Lim M and
Bettegowda C: Pituitary adenomas: Historical perspective, surgical
management and future directions. CNS Oncol. 4:411–429.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Dai C, Liu X, Ma W and Wang R: The
treatment of refractory pituitary adenomas. Front Endocrinol
(Lausanne). 10(334)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zhao B, Wei YK, Li GL, Li YN, Yao Y, Kang
J, Ma WB, Yang Y and Wang RZ: Extended transsphenoidal approach for
pituitary adenomas invading the anterior cranial base, cavernous
sinus, and clivus: A single-center experience with 126 consecutive
cases. J Neurosurg. 112:108–117. 2010.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Han ZL, He DS, Mao ZG and Wang HJ:
Cerebrospinal fluid rhinorrhea following trans-sphenoidal pituitary
macroadenoma surgery: Experience from 592 patients. Clin Neurol
Neurosurg. 110:570–579. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wei L, Lin SA, Fan K, Xiao D, Hong J and
Wang S: Relationship between pituitary adenoma texture and collagen
content revealed by comparative study of MRI and pathology
analysis. Int J Clin Exp Med. 8:12898–12905. 2015.PubMed/NCBI
|
|
17
|
Zada G, Yashar P, Robison A, Winer J,
Khalessi A, Mack WJ and Giannotta SL: A proposed grading system for
standardizing tumor consistency of intracranial meningiomas.
Neurosurg Focus. 35(E1)2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Shiroishi MS, Cen SY, Tamrazi B, D'Amore
F, Lerner A, King KS, Kim PE, Law M, Hwang DH, Boyko OB and Liu CS:
Predicting meningioma consistency on preoperative neuroimaging
studies. Neurosurg Clin N Am. 27:145–154. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Tamrazi B, Shiroishi MS and Liu CS:
Advanced imaging of intracranial meningiomas. Neurosurg Clin N Am.
27:137–143. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Yao A, Pain M, Balchandani P and
Shrivastava RK: Can MRI predict meningioma consistency?: A
correlation with tumor pathology and systematic review. Neurosurg
Rev. 41:745–753. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Naganuma H, Satoh E and Nukui H: Technical
considerations of transsphenoidal removal of fibrous pituitary
adenomas and evaluation of collagen content and subtype in the
adenomas. Neurol Med Chir (Tokyo). 42:202–213. 2002.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hagiwara A, Inoue Y, Wakasa K, Haba T,
Tashiro T and Miyamoto T: Comparison of growth hormone-producing
and non-growth hormone-producing pituitary adenomas: Imaging
characteristics and pathologic correlation. Radiology. 228:533–538.
2003.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Knosp E, Steiner E, Kitz K and Matula C:
Pituitary adenomas with invasion of the cavernous sinus space: A
magnetic resonance imaging classification compared with surgical
findings. Neurosurgery. 33:610–618. 1993.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Wang H, Li W, Shi D, Ye Z, Qin F, Guo Y
and Yuan X: Expression of TGFbeta1 and pituitary adenoma fibrosis.
Br J Neurosurg. 23:293–296. 2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Yiping L, Ji X, Daoying G and Bo Y:
Prediction of the consistency of pituitary adenoma: A comparative
study on diffusion-weighted imaging and pathological results. J
Neuroradiol. 43:186–194. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ghosh AK: Factors involved in the
regulation of type I collagen gene expression: Implication in
fibrosis. Exp Biol Med (Maywood). 227:301–314. 2002.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Kuivaniemi H and Tromp G: Type III
collagen (COL3A1): Gene and protein structure, tissue distribution,
and associated diseases. Gene. 707:151–171. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Fleischmajer R, MacDonald ED, Perlish JS,
Burgeson RE and Fisher LW: Dermal collagen fibrils are hybrids of
type I and type III collagen molecules. J Struct Biol. 105:162–169.
1990.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Cameron GJ, Alberts IL, Laing JH and Wess
TJ: Structure of type I and type III heterotypic collagen fibrils:
An X-ray diffraction study. J Struct Biol. 137:15–22.
2002.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Xu S, Xu H, Wang W, Li S, Li H, Li T,
Zhang W, Yu X and Liu L: The role of collagen in cancer: From bench
to bedside. J Transl Med. 17(309)2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Discher DE, Smith L, Cho S, Colasurdo M,
Garcia AJ and Safran S: Matrix Mechanosensing: From scaling
concepts in ‘Omics data to mechanisms in the nucleus, regeneration,
and cancer. Annu Rev Biophys. 46:295–315. 2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Yamauchi M, Barker TH, Gibbons DL and
Kurie JM: The fibrotic tumor stroma. J Clin Invest. 128:16–25.
2018.PubMed/NCBI View
Article : Google Scholar
|
|
33
|
Oliveira-Ferrer L, Rößler K, Haustein V,
Schröder C, Wicklein D, Maltseva D, Khaustova N, Samatov T,
Tonevitsky A, Mahner S, et al: c-FOS suppresses ovarian cancer
progression by changing adhesion. Br J Cancer. 110:753–763.
2014.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Lambrechts D, Wauters E, Boeckx B, Aibar
S, Nittner D, Burton O, Bassez A, Decaluwé H, Pircher A, Van den
Eynde K, et al: Phenotype molding of stromal cells in the lung
tumor microenvironment. Nat Med. 24:1277–1289. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Kuczek DE, Larsen AMH, Thorseth ML,
Carretta M, Kalvisa A, Siersbaek MS, Simões AMC, Roslind A,
Engelholm LH, Noessner E, et al: Collagen density regulates the
activity of tumor-infiltrating T cells. J Immunother Cancer.
7(68)2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Suzuki C, Maeda M, Hori K, Kozuka Y,
Sakuma H, Taki W and Takeda K: Apparent diffusion coefficient of
pituitary macroadenoma evaluated with line-scan diffusion-weighted
imaging. J Neuroradiol. 34:228–235. 2007.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Musleh W, Sonabend AM and Lesniak MS: Role
of craniotomy in the management of pituitary adenomas and
sellar/parasellar tumors. Expert Rev Anticancer Ther. 6 (Suppl
9):S79–S83. 2006.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Thotakura AK, Patibandla MR, Panigrahi MK
and Mahadevan A: Is it really possible to predict the consistency
of a pituitary adenoma preoperatively? Neurochirurgie. 63:453–457.
2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Mastorakos P, Mehta GU, Chatrath A, Moosa
S, Lopes MB, Payne SC and Jane JA Jr: Tumor to cerebellar peduncle
T2-weighted imaging intensity ratio fails to predict pituitary
adenoma consistency. J Neurol Surg B Skull Base. 80:252–257.
2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Yamamoto J, Kakeda S, Shimajiri S,
Takahashi M, Watanabe K, Kai Y, Moriya J, Korogi Y and Nishizawa S:
Tumor consistency of pituitary macroadenomas: Predictive analysis
on the basis of imaging features with contrast-enhanced 3D FIESTA
at 3T. AJNR Am J Neuroradiol. 35:297–303. 2014.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Yao A, Rutland JW, Verma G, Banihashemi A,
Padormo F, Tsankova NM, Delman BN, Shrivastava RK and Balchandani
P: Pituitary adenoma consistency: Direct correlation of ultrahigh
field 7T MRI with histopathological analysis. Eur J Radiol.
126(108931)2020.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Koktekir E, Karabagli H and Ozturk K:
Simultaneous transsphenoidal and transventricular endoscopic
approaches for giant pituitary adenoma with hydrocephalus. J
Craniofac Surg. 26:e39–e42. 2015.PubMed/NCBI View Article : Google Scholar
|