Introduction
Uterine leiomyoma is the most common benign
condition of the uterus. The usual complications, such as
menorrhagia, dysmenorrhea, pelvic pain, and infertility, are well
known and fully covered by the literature. Although the tumors may
reach large dimensions, in extremely rare cases massive
haemoperitoneum can occur due to the rupture of an overlying
variceal vein. Rokitanski first described the complication,
following an autopsy report, in 1861 (1,2).
The real incidence is difficult to assess and the
reported cases are scarce. Performing an Embase, Scopus, and PubMed
search, the number of reported cases was identified at
approximately less than 100, including those occurring during
pregnancy. Saidi et al reported 50 cases before
1961(3), Akahira et al
reported 7 cases between 1961 and 1997(4), Jain et al reported no more than
7 cases from 1994 to 2004(5), and 9
cases were revealed by the search of the present authors between
2005 and 2020 (2,6-13).
The present case study included a 48-year-old woman
with massive haemoperitoneum caused by the rupture of a subserosa
vein overlying a uterine leiomyoma. To the best of our knowledge,
it is the first reported case in Romania, and through this, the
article aim is to raise awareness of this extremely rare, but
potentially fatal complication.
Case presentation
A 48-year-old G1P1 (one gestation, one parity) woman
was referred to the Gynaecology Department of the ‘Cuza-Voda’
University Hospital, Iasi, Romania presenting abdominal pain with
sudden onset, moderate genital bleeding, cold and sweat
extremities, hypotension, and tachycardia. The patient declared
that she has been diagnosed with uterine myoma 2 years before,
during a routine gynecologic examination. She had been asymptomatic
until hospital presentation. In addition, she was diagnosed 1 year
earlier with mild risk hypertension, being treated with β-blockers
since then. Clinical examination revealed a tender, distended
abdomen with dullness in flanks, skin pallor, cold and sweat
extremities, and tachycardia (124 beats/min). Blood pressure at
department admittance was 90/60 mmHg, 1 h later it had dropped to
70/40 mmHg. Initial haemoglobin level was 9.2 g/dl, dropping 1 h
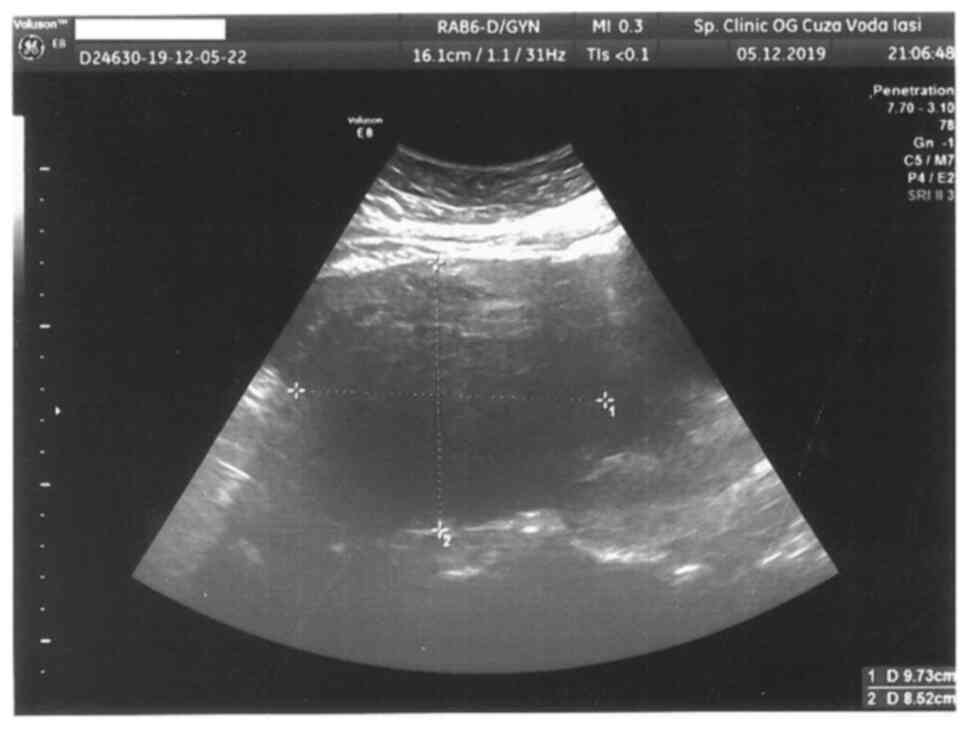
later to 7.1 g/dl. Transabdominal ultrasonography revealed a high
amount of free fluid within the peritoneal cavity, suggestive of
massive haemoperitoneum, and an enlarged uterus with an echogenic
mass of 97.3/85.2 mm cranially to the uterine fundus, with
posterior extension (Fig. 1).
Emergency enhanced computed tomography scan
confirmed the presence of a massive haemoperitoneum, the uterine
fundal tumor resembling a myoma (95/92/85 mm) and presenting
multiple venous dilatations with a maximum calibre of 6 mm,
overlying the tumor. No other pathologic findings were evident. Due
to the continuous reduction in blood pressure in spite of the
intense supportive treatment, an emergency laparotomy was decided.
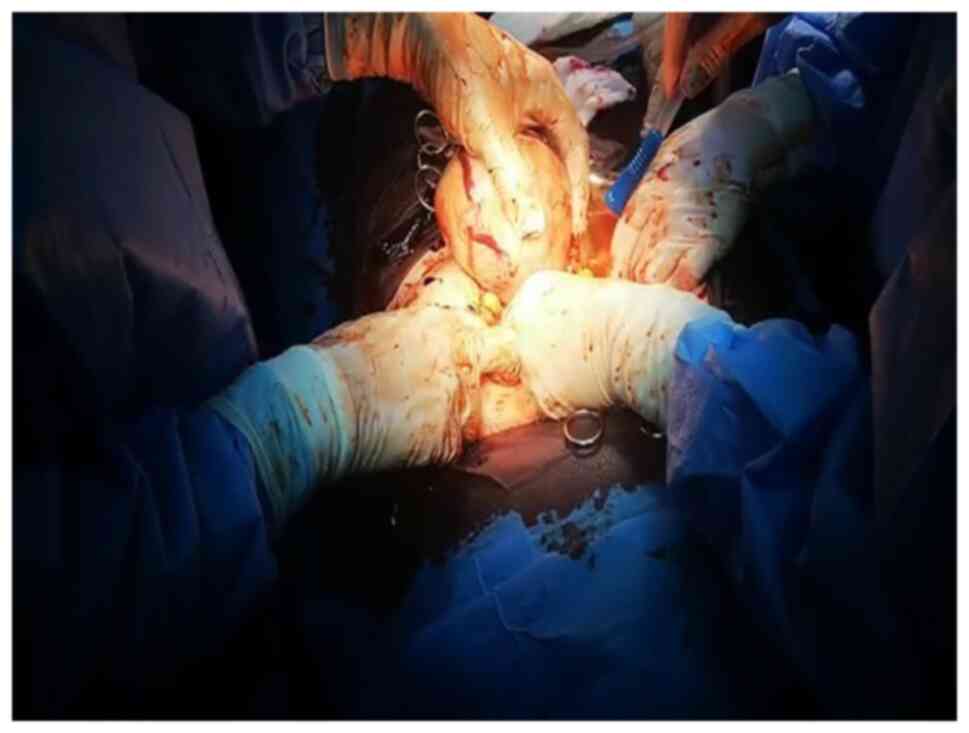
A sub-umbilical midline vertical incision was performed, and
approximately 2,000 ml of blood and clots (some of them having
impressive dimensions) were found. The uterus was enlarged, having
a fundal myoma of 10 cm in the maximum diameter. Multiple venous
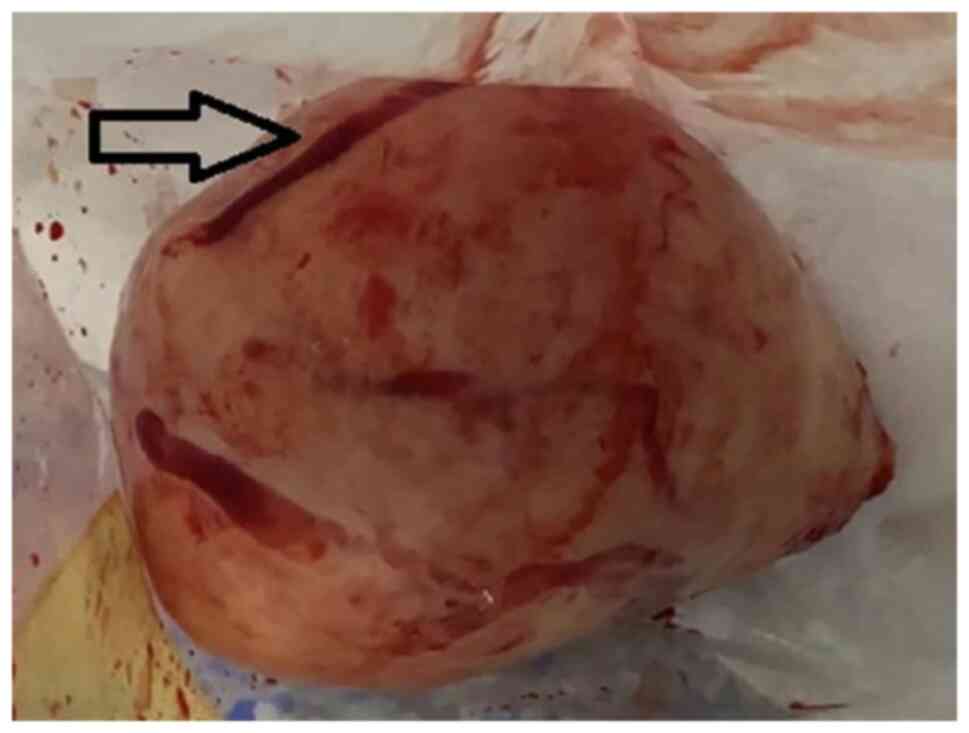
dilatations covered the posterior part of the tumor (Fig. 2). Due to the increased angulation of
the uterine arteries and subsequent reduction of uterine blood flow
produced by the exteriorization of the uterus from the abdominal
cavity, the bleeding source from a venous varicosity was
intermittent and minimal (Fig. 3).
The incision was extended laterally to the umbilicus, by a general
surgeon, to allow careful search in the superior compartment of the
abdomen for another source of bleeding. Since no other bleeding
source was found and the variceal tear continued to bleed when the
uterus was repositioned inside the abdominal cavity, the variceal
rupture was determined as the source of the massive
haemoperitoneum. Due to the altered hemodynamic status of the
patient and haemoglobin level of 5.2 g/dl during surgery, a
supracervical hysterectomy was performed in order to achieve quick
haemostasis. In the postoperative period, after the transfusion of
4 units of whole blood, the status of the patient consistently
improved and the recovery was uneventful.
This case report was conducted in accordance with
the World Medical Association Declaration of Helsinki. Patient
consent was obtained.
Discussion
Venous congestion plays an important role in
varicose venous formation. Increased abdominal pressure may lead to
the rupture of superficial dilated veins, which overlie a large
myoma of the uterus (5). Uterine
contractions during menstrual period can create a tension effect on
the blood vessels resulting in its rupture (14). Other predisposing factors for venous
congestion are pregnancy, large myoma (>10 cm) (6), nulliparity, age between 30 and 49
years, hormonal replacement therapy, and warfarin treatment
(15). Precipitating factors such
as constipation, intense physical activity, coughing, and sexual
intercourse (6) increase the
abdominal pressure in an acute manner and may have a catalytic
effect on the predisposing factors. Although the majority of
studies have assessed the theories regarding the predisposing
factors, Dahan and Ahmadi state that the risk of formation and
rupture of the varicose veins overlying a myoma is independent of
age, parity and size of the tumor (16).
In the majority of cases, patients present signs of
hypovolemic shock and abdominal pain with sudden onset. The
precipitating factors for the increase in abdominal pressure may be
present. In women of reproductive age, in these settings, the
rupture of an ectopic pregnancy or luteal cyst represents the most
common diagnosis to consider. Torsion of a subserous myoma, red
degeneration, avulsion and sarcomatous degeneration are common
causes of acute abdomen in patients with history of uterine
leiomyoma (11). Another cause of
non-gynecologic haemoperitoneum must be excluded. In most cases,
the actual cause of bleeding is often difficult to specify prior to
the surgical procedure (11,13).
Imaging techniques including ultrasonography,
magnetic resonance imaging (MRI) or computer tomography can
establish a positive diagnosis of haemoperitoneum and uterine
myoma, in rare cases it can reveal the site of bleeding (13). Contrast-enhanced 3-dimensional MRI
allows an accurate diagnosis regarding the site of the bleeding,
but often it is not available in emergency settings (13,17).
An acute haemoperitoneum represents an absolute
emergency. In a hemodynamic unstable patient the treatment is
intensive, both supportive and surgical. Blood transfusions and
intravenous fluids should be administered (13). Intravascular disseminated
coagulopathy is common in severe cases and for an improved outcome,
it is advisable to consider the administration of recombinant
factor VIIa. In our case, performing a supracervical hysterectomy
decreased the operative time and blood loss, the administration of
recombinant factor VIIa not being necessary. The main disadvantage
of an emergency supracervical hysterectomy is represented by the
impossibility of having a Pap test result prior to the surgical
intervention and the patient must be included in a careful cervical
screening following the procedure. Therapeutic laparoscopic
approach has not described in any case report, thus far. Some
authors recommend an exploratory laparoscopy in cases of acute
abdomen with uncertain etiology (6). In young patients, the preservation of
fertility is the main objective, but it may not be achieved in all
cases (4). Hemostatic suture or
myomectomy should be attempted as a first choice in women of
reproductive age. However, in cases of fertility-sparing
procedures, large myomas can cause serious problems regarding
hemostasis. Myomectomy presents a considerable risk of persistent
or recurrent bleeding from the site of myometrial repair, and in
patients with important bleeding prior to surgery, this procedure
may worsen their hemodynamic status (17). In cases of menopausal women,
hysterectomy is advisable due to a better hemostasis and a shorter
operative time. In all cases with conscious patients, they should
be informed that the intraoperative findings and the hemodynamic
status during surgery are essential in choosing the type of
surgical procedure.
The current case is of a premenopausal patient of
low parity (1P), with a positive history of uterine myoma, without
any predisposing and precipitating factors. Jenayah et al
mentioned that myomas >10 cm have an increased risk for
subserosal variceal development (6). In our case the maximum size of the
tumor was 9.5 cm, close below the limit. Of note was the fast
degradation of the hemodynamic status within 1 h from admittance.
Intraoperatively, the angulation of uterine arteries caused by
uterine exteriorization from the abdominal cavity significantly
reduces the blood flow of the uterus and the bleeding point from
the variceal tear may be difficult to observe. Repositioning the
uterus can facilitate the proper assessment of the varicosities and
possible bleeding points. In case of fundal and posterior location
of a large fibroid, which tends to deeply impact the uterus within
the sacral concavity, as in the case in the present study,
disimpaction manoeuvres of a less mobile uterus can modify the
uterine artery flow and momentarily stop the bleeding. A careful
inspection followed by saline irrigation of the abdominal cavity,
is recommendable for the exclusion of other possible bleeding
sites. The presented case of a massive haemoperitoneum caused by
the rupture of a subserosa vein overlying a uterine leiomyoma is,
to the best of our knowledge, the first reported in Romania, and
through this article the aim is to raise awareness of this
extremely rare, but potentially fatal complication.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The data used and/or analyzed during the current
study are available from the corresponding author on reasonable
request. Supplementary data are available from the corresponding
author.
Authors' contributions
RP, MG, and AP designed the study and wrote the
manuscript. PZ, MM, BR, DCA, RM, and LMH performed the literature
research and interpreted the data. All authors have read and agreed
to the published version of the manuscript. RP, AP and MG confirm
the authenticity of all the raw data.
Ethics approval and consent to
participate
This case report was conducted in accordance with
the World Medical Association Declaration of Helsinki. Patient
consent was obtained.
Patient consent for publication
Not applicable.
Authors' information
Loredana Maria Himiniuc: https://orcid.org/0000-0002-4721-4642.
Competing interests
The authors declare that there are no competing
interests.
References
|
1
|
Buttery BW: Spontaneous haemoperitoneum
complicating uterine fibromyoma. Aust N Z J Obstet Gynaecol.
12:210–213. 1972.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Porpora MG, Musacchio L, Piacenti I,
D'Alessandris N, Pecorini F, Iafrate F and Benedetti Panici P:
Massive haemoperitoneum caused by uterine leiomyoma: A case report.
J Obstet Gynaecol. 40:735–736. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Saidi F, Constable JD and Ulfelder H:
Massive intraperitoneal hemorrhage due to uterine fibroids. Am J
Obstet Gynecol. 82:367–374. 1961.PubMed/NCBI
|
|
4
|
Akahira J, Ito K, Nakamura R and Yajima A:
Massive intraperitoneal hemorrhage and hypovolemic shock due to
rupture of a coronary vessel of a uterine leiomyoma: A report of
two cases. Tohoku J Exp Med. 185:217–222. 1998.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jain P, Pradhan P, Cietak KA and Anyanwu
L: Acute abdomen following spontaneous variceal rupture overlying
uterine leiomyoma. J Obstet Gynaecol. 24(589)2004.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jenayah AA, Saoudi S, Sferi N, Skander R,
Marzouk SB, Cherni A, Sfar E, Chelli D and Boudaya F: Spontaneous
subserosal venous rupture overlying a uterine leiomyoma in a young
woman. Pan Afr Med J. 28(205)2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ihama Y, Miyazaki T and Fuke C:
Hemoperitoneum due to rupture of a subserosal vein overlying a
uterine leiomyoma. Am J Forensic Med Pathol. 29:177–180.
2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Althobaiti FA, Alsaadi KK and Althobaiti
AA: A case of hemoperitoneum due to spontaneous bleeding from a
uterine leiomyoma. Am J Case Rep. 20:167–170. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Rokhgireh S, Kashi AM, Kermansaravi M,
Tajbakhsh B, Allahqoli L, Alkatout I and Khodaverdi S:
Hemoperitoneum due to bleeding from a vein overlying a subserous
uterine myoma: A case report. J Med Case Rep. 14(55)2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Elkbuli A, Shaikh S, McKenney M and Boneva
D: Life-threatening hemoperitoneum secondary to rupture of a
uterine leiomyoma: A case report and review of the literature. Int
J Surg Case Rep. 61:51–55. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Dasari P and Maurya DK: Hemoperitoneum
associated with fibroid uterus. J Obstet Gynecol India. 55:553–554.
2005.
|
|
12
|
Sneha S, Munikrishna M and Sheela SR: A
rare case of hemoperitoneum due to rupture of vessels over the
surface of leiomyoma. J Clin Biomed Sci. 9:23–24. 2019.
|
|
13
|
Aydin C, Şen Selim H, Eriş S and Yalçin Y:
Haemoperitoneum: An extremely rare complication of leiomyoma. J
Obstet Gynaecol. 35:109–110. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Horowitz E, Dekel A, Feldberg D and
Rabinerson D: Massive hemoperitoneum due to rupture of an artery
overlying a uterine leiomyoma: A case report. Acta Obstet Gynecol
Scand. 84:408–409. 2005.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Tang A, Rao S and Cawdell G: Massive
intra-abdominal haemorrhage due to spontaneous bleeding from
fibroids in a post-menopausal woman. J Obstet Gynaecol. 28:244–245.
2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Dahan MH and Ahmadi R: Spontaneous
subserosal venous rupture overlying a uterine leiomyoma. A case
report. J Rep Med. 47:419–420. 2002.PubMed/NCBI
|
|
17
|
Kassegne I, Kolani K, Tchangai B,
Kanassoua K, Adabra K, Alassani F, Amavi AK and Dosseh EDJ:
Myomectomies for massive hemoperitoneum from spontaneous bleeding
of a uterine myoma. J Surg Case Rep. 2017(rjx127)2017.PubMed/NCBI View Article : Google Scholar
|