Melatonin (MT) is a hormone produced by the pineal
gland, which is superior to the third ventricle of the brain
(7). MT has the ability to diffuse
in and out of cells due to its chemical structure and low molecular
weight (8). MT is synthesized by
the pineal gland, in the bone marrow, the eyes and the
gastrointestinal tract. The synthesis of MT arises from
5-hydroxytryptamine and the rate-limiting enzyme in this reaction
is MT-N-acetyltransferase (9).
Certain researchers have indicated that MT can lighten mottled skin
by downregulating melanophores (10,11)
Moreover, MT regulates the human chronobiological
function known as the circadian rhythm (12). The suprachiasmatic nuclei (SCN)
located in the hypothalamus are responsible for maintaining the
circadian rhythm in mammals (13).
Sleep state and metabolism are activated by MT, which is stimulated
by the SCN (14). In the human 24-h
sleeping cycle, MT secretion changes periodically based on an
internal biological clock (15).
Apart from the central circadian clock, MT also modulates
peripheral tissues and organs, making MT the best marker of the
circadian rhythm (16). Generally,
MT secretion is highest between 11:00 p.m. and 2:00 a.m., and the
secretion decreases sharply after 7:00 a.m (17). Additionally, the level of MT is
affected by light intensity, age and other factors (18,19).
Notably, light during the night can severely disrupt MT production
and Circadian rhythms of patients in ICU in hospitals (20). MT administration and its receptor
agonists have advantages in preventing delirium by promoting
nocturnal sleep (21,22).
MT has three receptors: MT receptor-1 (MT1), MT2 and
MT3. MT1 and MT2 are G protein-coupled receptors, which are
involved in various cell signal transduction processes, such as the
regulation of the immune system and photosensitivity (23). Additionally, MT1 receptors are
located in the locus coeruleus and lateral hypothalamus (rapid eye
movement area), while MT2 receptors are located in the reticular
thalamus (non-rapid eye movement area) in selective MT1/MT2
receptor ligands and MT1/MT2 receptor knockout mice (23). Thus, MT1 is considered to establish
and maintain the circadian rhythm, mood, pain and sleep (24). Recently, certain researchers have
demonstrated that the structure of MT2 allowed for accurate mapping
of type 2 diabetes-related single-nucleotide polymorphisms
(23,25,26).
MT1, rather than MT2, has been implicated in circadian rhythm
regulation. It has been reported that MT1 receptors are involved in
Alzheimer's and Huntington's diseases, and patients with depression
(26). Moreover, the expression
level of MT1 and MT2 decreased as the cancer stage increased and
MT2 was an independent prognostic factor for survival rate in
patients with NSCLC (27).
Additionally, MT has an affinity for specific MT membrane
receptors, including retinoic acid receptor-related orphan nuclear
receptors (RORs) (28). The MT-RORα
axis serves as a novel endogenous protective signalling pathway in
the vasculature, regulates intraplaque inflammation and stabilizes
rupture-prone vulnerable plaques (29).
The summary was designed to critically review
scientific studies that demonstrate the therapeutic actions of
melatonin on lung injury. The molecular aspects of melatonin's
therapeutic potential is also discussed with due reference to
molecular targets and pharmacological effects.
The inflammation mechanism is a natural human
response to bodily injury from injection or chemical and physical
stimulation. Inflammatory cells (such as leukocytes, macrophages,
mast cells and endothelial cells), which release TNF-α, IL-1β and
IL-6, are involved in the process of inflammatory tissue repair
(30). Inhibition of the
inflammatory process is one of the essential strategies in
antagonizing chronic or acute inflammatory diseases, including
pneumonia, asthma and COPD (30-33).
Anti-inflammatory actions by MT are of particular clinical
significance in high-grade inflammation, such as sepsis-induced
lung injury, ischemia-reperfusion lung injury and brain injury
(34). Following tissue damage, MT
activates pro-inflammatory cytokines and other mediators (35). Additionally, MT administration
suppresses inflammatory processes, including nitric oxide (NO)
release, activation of cyclooxygenase-2, nucleotide-binding
oligomerization domain-like receptor protein 3 (NLRP3)
inflammasome, toll-like receptor 4 (TLR-4) and mTOR signalling, and
amyloid-β toxicity (36-39).
Additionally, previous studies proved that exogenous MT attenuated
the inflammatory response by increasing the expression of silent
information regulator 1 (SIRT1) activity, which exerts
anti-inflammatory effects (34,40).
Furthermore, the mechanisms contributing to
inflammatory effects are oxidative stress and oxidative-mediated
processes such as oxygen free radical reaction and lipid
peroxidation (41). Inflammatory
cells secrete numerous cytokines and chemokines including IL-1β,
TNF-α, MCP-1, which are responsible for the production of reactive
oxygen species (ROS) in phagocytic cells at the beginning of the
inflammation phase (42). ROS
adversely impact the action of neutrophils and macrophages, and
decrease the activation of apoptotic signals (43).
Concerning anti-inflammatory and molecular
mechanisms, various novel perspectives focus on the immune-pineal
axis, which serves as a negative feedback mechanism to mediate the
immune system (44). Moreover,
these pro-inflammatory cytokines including TNF-α, IL-1β and IL-6
have several detrimental effects on individual tissues, including
lung, liver and kidney, and manifest as endothelial cell damage,
vascular permeability changes, tissue degeneration and edema
(45,46).
MT serves as an antioxidant and rapidly disappears
from the blood and in the systemic circulation of mammals, once
they are under conditions of high oxidative stress (47). MT acts as an antioxidant either
directly or indirectly via the MT receptors MT1 and MT2(27). Novel research has indicated that MT
depleted ROS and increased glutathione (GSH) levels to inhibit the
development of lung cancer (48).
This result indicates that the unique indole composition has a
leading role in the antioxidant effect of MT due to its high
stability and electroactivity (49).
Moreover, MT O-methyl and N-acetyl residues are the
basis of its amphiphilicity, allowing the molecule to enter all
organs and subcellular compartments, and are the primary
facilitators of its antioxidant properties (50). A recent study reported that MT
significantly improved the tolerance of apple seedlings to
waterlogging stress as ROS are hypothesized to serve a critical
role in the response of the plant to waterlogging pressure
(51). MT administration increased
ascorbic acid levels and the activity of antioxidants, including
superoxide dismutase (SOD), catalase (CAT) and peroxidase in rats
(52). Numerous in vitro and
in vivo studies have demonstrated that exogenous MT
suppresses oxidative stress (53,54).
Another study reported that MT-loaded lipid-core nanocapsules
(Mel-LNC) increased the fluorescence intensity of Caenorhabditis
elegans that encodes the antioxidant enzyme SOD-3 to inhibit
lipid peroxidation (54). Treatment
with MT following CCl4 exposure in rats resulted in a
significant increase in the activity of lung tissue oxidized
proteins, including myeloperoxidase (MPO) and malondialdehyde (MDA)
(55). Additionally, the same
author indicated that MT upregulated the levels of intracellular
antioxidant enzymes, including SOD2 and glutathione peroxidase
1(56).
There is a plethora of clinical treatments targeting
the significant therapeutic role of MT against different diseases,
including lung disease, liver disease, kidney disease, diabetes,
Alzheimer's disease and Parkinson's disease (46,57,58). A
randomized, double-blinded, placebo-controlled trial indicated that
MT supplementation (2x5 mg/day for 12 weeks) significantly reduces
the sum of total antioxidant capacity, including GSH and MDA, in
patients with diabetic hemodialysis (59). MT administration substantially
minimized oxidative stress and directly acted on its membrane
receptors MT1 and MT2, which serve a vital role during the whole
gestational period in humans and animals (60). A previous study indicated that
cyclic 3-hydroxy-MT is a product that includes antioxidative
effects of MT and mediates its metabolite interaction with ROS
(61). Another study demonstrated
that administering a subcutaneous implant containing 18 mg of MT
with lamb model and ovine prepubertal cumulus cells, promoted
antioxidant capacity (SOD1, Glutathione peroxidase 4 and CAT) via
RORα in ovine prepubertal cumulus cells (62).
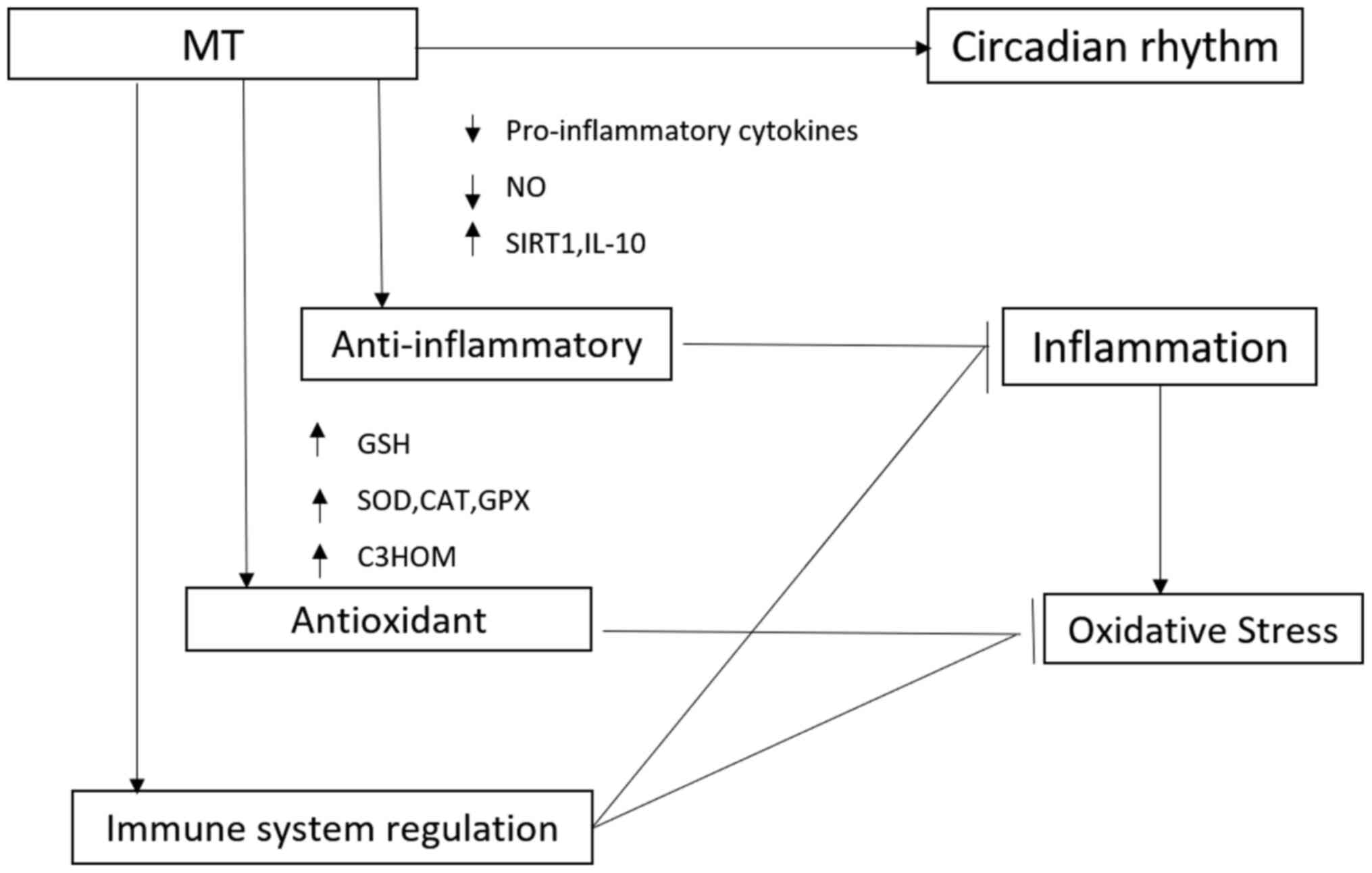
The regulatory effect of MT in the immune system is
not surprising, as a correlation has been demonstrated between
melatonin production and circadian in immune function, pinealectomy
has been shown to cause changes in the immune system, and in
vivo and in vitro administration of melatonin has been
shown to cause changes in immune functions (Fig. 1) (63). The immune system is notably complex,
which becomes evident with the multitude of participating cell
types and subtypes, as well as humoral factors, the flexible
regulatory network, the participation of non-immune cells in the
classic sense and in the short- and long-term temporal changes
(64). With regard to acute
inflammation, the immune system activates the required cellular and
humoral processes, later actively terminating them and initiating
healing (65).
Coronaviruses (CoVs) are RNA viruses that infect
both humans and animals. Infection involves the respiratory,
gastrointestinal and central nervous systems. Since the outbreak of
COVID-19 at the end of 2019, thousands of people have been infected
or succumbed to the disease (66).
Unfortunately, there is a lack of a specific treatment for
COVID-19. In Severe Acute Respiratory Syndrome-CoV- and Middle East
Respiratory Syndrome-CoV-infected animal models, marked
inflammatory and immune responses activate a ‘cytokine storm’ and
the apoptosis of epithelial cells and endothelial cells;
subsequently, vascular leakage and abnormal T cell and macrophage
responses ensue and induce ALI/acute respiratory distress syndrome
(ARDS) or even death (67).
Melatonin is effective in critical care patients by reducing vessel
permeability, anxiety, sedation use, and improving sleeping
quality, which might also be beneficial for better clinical
outcomes for COVID-19 patients (66).
MT can be classified as an immune stimulatory agent.
Notably, the effect of anti-inflammatory actions has been observed
in cells in the blood or other body fluids (68). Previous tudies have indicated that
MT administration had positive effects in alleviating ARDS-induced
by viruses, bacteria and radiation (37,69).
MT exerts regulatory actions on the immune system and directly
enhances the immune response by increasing the proliferation and
maturation of natural killing cells, T and B lymphocytes,
granulocytes and monocytes in the bone marrow and other tissues
(70).
ALI is a common clinical respiratory disease that
often develops into a more complex syndrome termed ARDS (71). It has multiple etiologies and often
results in severe respiratory failure and death (72). According to the World Health
Organization (WHO), ARDS was the leading cause of death in
Intensive Care Units from 50 Countries in 2014(73). Annually, ~2 million days in ICU and
75,000 deaths occur in the USA due to ARDS (74). The ‘Berlin definition’ was developed
in 2012 based on the clinical standards for ALI/ARDS (75). Therefore, preventing ARDS and its
complications is an urgent clinical problem for doctors. A high
number of clinical and experimental studies were dedicated to
prevention and diagnosis in order to improve the prognosis of
ARDS.
Lung ischaemia-reperfusion injury (LIRI), known as a
frequent and severe clinical complication, has a high mortality
after lung transplantation worldwide (80,81).
LIRI is a pathological process with the clinical feature of initial
restriction of blood supply to lung organs followed by the
restoration of perfusion, which involves oxidative stress (82). The primary cause of this may be the
imbalance of excessive oxygen free radical production and
insufficient antioxidant mechanisms (83). Ischemia/reperfusion (IR) injury is a
severe clinical event that may induce tissue injury, whose primary
underlying mechanisms include an inflammatory immune response, the
release of inflammatory mediators and the induction of apoptosis
(84).
Asthma has a high occurrence and is the most common
long-term inflammatory syndrome (85). It affects the lower airway mucosa by
producing IL-4, IL-13, IL-5 and IL-9(86). The typical clinical manifestations
including wheezing, breathlessness, coughing and difficulty
breathing, particularly at night or in the early morning (65). Certain researchers have indicated
that asthma, as a chronic inflammatory disorder of the airways, is
associated with numerous cells and cellular elements, including
mast cells, eosinophils, type 2 T helper cells, macrophages,
neutrophils and epithelial cells (87,88).
In asthma, type 2 T helper cells have a crucial role in producing
inflammatory cytokines, such as IL-4, IL-9, IL-10 and
IL-13(89). Additionally, oxidative
stress is another essential factor in stimulating inflammatory
responses in asthma (90).
According to WHO reports, in developed countries asthma affects 10%
of the population and people with asthma have an increased risk of
developing anxiety disorders (91).
Although the treatment strategies of asthma are diverse in
developing countries, its prevalence is still rapidly increasing
yearly (92). Wang et al
(93) demonstrated that MT
administration (10 mg/kg) significantly inhibited the expression of
NF-κβ and downregulated inducible NO synthase activity in lung
tissues and substantially reduced NO production in bronchoalveolar
lavage fluid (BALF) in a rat model of asthma.
Researchers have reported that TLR-9 is one of the
most extensively studied TLRs used to treat asthma. Wu et al
(94) reported that, compared with
wild-type (WT) mice, MT effectively inhibited airway inflammation
in an asthmatic mouse model induced by ovalbumin (OVA).
Additionally, the experimental results indicated that the protein
expression of immunoglobulin E (IgE) and MT levels in serum and
BALF were reduced in OVA-induced WT mice; however, TLR9(-/-) mice
significantly restored these decreases. SP600125, a JNK-specific
inhibitor, significantly deceased OVA-induced expression of TLR9
and reset the level of MT in OVA-treated WT mice. In summary, the
JNK-TLR9 signalling pathway mediated the airway inflammation
process via inhibiting MT biosynthesis. Furthermore, Shin et
al (95) reported that
intraperitoneal injection of MT (10 or 15 mg/kg daily)
significantly decreased the numbers of inflammatory cells, airway
inflammation, and IgE, IL-4, IL-5 and IL-13 expression levels in an
OVA-induced allergic asthma rat model. In vitro experiments
indicated that pro-inflammatory cytokine expression and matrix
metalloproteinase-9 activity were significantly suppressed by MT
administration in TNF-α-stimulated BEAS-2B cells. Further research
by the same authors revealed that MT notably suppressed chronic
airway inflammation, accompanied by a reduction in the expression
levels of mucin 5AC (MUC5AC) mRNA and protein (33). In an in vitro experiment, MT
treatment suppressed IL-6 production and MUC5AC expression in
EGF-stimulated H292 cells. The authors concluded that MT
significantly inhibited the expression of MUC5AC via the
downregulation of the MAPK signalling pathway in an OVA-induced
asthma murine model (96). A
double-blinded, randomized, placebo-controlled clinical research
trial included MT treatment (3 mg/day) or placebo for 4 weeks in 22
women with asthma and the Pittsburgh Sleep Quality Index, Epworth
Sleepiness Scale (97) and
pulmonary function were assessed (98). The results indicated that MT
significantly improved sleep quality in patients with asthma in
comparison with the placebo group.
COPD is a devastating lung disease that affects
alveolar structures and adversely impacts ventilation (99). Exposure to cigarette smoke is
considered to be the leading risk factor for COPD, as well as air
pollution and infection. Currently, COPD is a well-known lung
disease and an increasing global health problem (100). The main pathological feature of
COPD is chronic airway inflammation and an abnormal response to the
external environment, resulting in small airway and alveolar
restructuring, as reflected by a lack of ventilation function and
emphysema in COPD (101).
Mechanical ventilation is increasingly used in life
support and routine anesthesia; however, VILI has always
represented a challenging issue (104). Mechanical ventilation translates
into prolonged hospital stays, increased burden on the health care
system and increased treatment costs (105). The mechanisms responsible for VILI
are complex. Increased tidal volumes cause the lung tissues to
stretch, which is potentially problematic, as it induces a local
cytokine storm which is known to initiate VILI (106). A previous study reported that
obese patients may suffer fatal emphysema with high airway pressure
and postoperative pulmonary complications following intraoperative
ventilation (107). However, a
previous study revealed that obesity served a protective role in
VILI by alleviating pulmonary endothelial barrier injury and the
inflammatory response (108). A
previous study reported that MT administration significantly
decreased VILI by increasing the anti-inflammatory response (IL-10)
despite an unexpected increase in oxidative stress (6). However, the specific mechanism
underlying MT and VILI has not been elucidated.
Although the therapeutic role of MT for the clinical
treatment of VILI has not been assessed until now, it can be
hypothesized. Recently, protective lung ventilation strategies have
beneficial effects against VILI, including optimizing mechanical
ventilation by setting suitable positive end-expiratory pressure,
low tidal volume ventilation strategy, recruitment maneuvers and a
lax hypercapnia strategy (109).
Adherens and tight junctions are essential components in
maintaining the integrity of the alveolar epithelial barrier. Rho
belongs to the Ras superfamily of low molecular weight GTPases,
which have a key role in the formation of the alveolar epithelial
cell cytoskeleton, as well as Rho-associated coiled-coil forming
protein kinase (110). Sripathi
et al (111) reported that
MT treatment could be beneficial in protecting mitochondria under
oxidative stress and maintaining the structure of the cytoskeleton
in the retinal pigment epithelium. Moreover, p120 serves as an
essential protein in the regulation of cell junctions and protects
against VILI by regulating both adherens and tight junctions by
reducing the degradation of occludin via the inhibition of RhoA
activity (112). Finally, the
effect of MT on stabilizing cytoskeleton structure and the
activation of target genes may represent a novel way to alleviate
VILI.
Treatment with MT has been demonstrated to exert
positive effects on the alleviation of the aforementioned lung
injuries, including ALI/ARDS, LIRI, asthma, COPD and VILI. At a
molecular level, MT reduces lung injury via antioxidative effects
and upregulation of anti-inflammatory cytokines, profibrotic
cytokines and chemokines in lung tissues, which have a pivotal role
in the pathophysiology of lung injury.
In ALI/ARDS, MT serves as a crucial antioxidant and
anti-inflammatory vehicle that has vital roles in the alleviation
of oxidative stress and the excessive production of
pro-inflammatory cytokines and chemokines in lung tissues. In LIRI,
MT inhibits the activation of the JNK/p38 signalling pathway to
protect against lung injury. Additionally, MT decreases the
expression of MPO and NO in lung tissues. In asthma, MT improves
lung function by alleviating airway inflammation and reducing the
release of inflammatory cytokines via the downregulation of NF-κB.
Additionally, it can be hypothesized that MT reduces the severity
of chronic asthma via the inhibition of the JNK-TLR9 signalling
pathway. It is well known that there is systemic oxidative stress
in COPD and antioxidant therapeutic targets are required for the
improvement of lung function in patients with COPD (113). Additionally, the critical role of
SIRT1 in chronic inflammation cannot be ignored. In VILI, MT
reduces the severity of injury via its anti-inflammatory and
inhibitory actions on the expression levels of pro-inflammatory
cytokines. Notably, recent research has documented the positive
effects of MT in treating COVID-19-induced pneumonia and ALI
(66,114). Furthermore, the effects of MT on
stabilizing cytoskeletal structure and inhibiting the expression of
cytoskeletal proteins are areas of interests for the future
research of VILI.
Not applicable.
The present study was supported by the Yangzhou
International Cooperation Project: ‘Yangzhou Science and Technology
Plan Project’ (grant no. YZ2019145).
Not applicable.
WW reviewed literature and wrote the manuscript. JG
reviewed and revised the manuscript. JG gave final approval for
publication. Both authors read and approved the final version of
the manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Harhay MO and King CH: Global burden of
disease in young people aged 10-24 years. Lancet. 379:27–28; author
reply 28. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Habtemariam S, Daglia M, Sureda A,
Selamoglu Z, Gulhan MF and Nabavi SM: Melatonin and Respiratory
Diseases: A Review. Curr Top Med Chem. 17:467–488. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Rudan I, Tomaskovic L, Boschi-Pinto C and
Campbell H: WHO Child Health Epidemiology Reference Group. Global
estimate of the incidence of clinical pneumonia among children
under five years of age. Bull World Health Organ. 82:895–903.
2004.PubMed/NCBI
|
|
4
|
Rosenberg SR, Kalhan R and Mannino DM:
Epidemiology of Chronic Obstructive Pulmonary Disease: Prevalence,
Morbidity, Mortality, and Risk Factors. Semin Respir Crit Care Med.
36:457–469. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pedreira PR, García-Prieto E, Parra D,
Astudillo A, Diaz E, Taboada F and Albaiceta GM: Effects of
melatonin in an experimental model of ventilator-induced lung
injury. Am J Physiol Lung Cell Mol Physiol. 295:L820–L827.
2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lerner AB, Case JD, Takahashi Y, Lee TH
and Mori W: Isolation of melatonin, the pineal gland factor that
lightens melanocytes 1. J Am Chem Soc. 80(2587)1958.
|
|
8
|
Lapin V and Ebels I: Effects of some low
molecular weight sheep pineal fractions and melatonin on different
tumors in rats and mice. Oncology. 33:110–113. 1976.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Beñaldo FA, Llanos AJ, Araya-Quijada C,
Rojas A, Gonzalez-Candia A, Herrera EA, Ebensperger G, Cabello G,
Valenzuela GJ and Serón-Ferré M: Effects of Melatonin on the
Defense to Acute Hypoxia in Newborn Lambs. Front Endocrinol
(Lausanne). 10(433)2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Alvarez-Artime A, Cernuda-Cernuda R,
Francisco-Artime-Naveda Cepas V, Gonzalez-Menendez P, Fernadez-Vega
S, Quiros-Gonzalez I, Sainz RM and Mayo JC: Melatonin-Induced
Cytoskeleton Reorganization Leads to Inhibition of Melanoma Cancer
Cell Proliferation. Int J Mol Sci. 21(E548)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Andersson TPM, Filippini D, Suska A,
Johansson TL, Svensson SPS and Lundström I: Frog melanophores
cultured on fluorescent microbeads: Biomimic-based biosensing.
Biosens Bioelectron. 21:111–120. 2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Plaimee P, Weerapreeyakul N, Thumanu K,
Tanthanuch W and Barusrux S: Melatonin induces apoptosis through
biomolecular changes, in SK-LU-1 human lung adenocarcinoma cells.
Cell Prolif. 47:564–577. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Karimfar MH, Rostami S, Haghani K,
Bakhtiyari S and Noori-Zadeh A: Melatonin alleviates
bleomycin-induced pulmonary fibrosis in mice. J Biol Regul Homeost
Agents. 29:327–334. 2015.PubMed/NCBI
|
|
14
|
Zisapel N: New perspectives on the role of
melatonin in human sleep, circadian rhythms and their regulation.
Br J Pharmacol. 175:3190–3199. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Genovese T, Di Paola R, Mazzon E, Muià C,
Caputi AP and Cuzzocrea S: Melatonin limits lung injury in
bleomycin treated mice. J Pineal Res. 39:105–112. 2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Trivedi AK, Mishra I and Kumar V: Temporal
expression of genes coding for aryl-alkamine-N-acetyltransferase
and melatonin receptors in circadian clock tissues: Circadian
rhythm dependent role of melatonin in seasonal responses. Physiol
Behav. 207:167–178. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kurhaluk N and Tkachenko H: Melatonin and
alcohol-related disorders. Chronobiol Int. 37:781–803.
2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Sanchez-Hidalgo M, de la Lastra CA,
Carrascosa-Salmoral MP, Naranjo MC, Gomez-Corvera A, Caballero B
and Guerrero JM: Age-related changes in melatonin synthesis in rat
extrapineal tissues. Exp Gerontol. 44:328–334. 2009.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Erren TC and Reiter RJ: Melatonin: A
universal time messenger. Neuro Endocrinol Lett. 36:187–192.
2015.PubMed/NCBI
|
|
20
|
Bonmati-Carrion MA, Arguelles-Prieto R,
Martinez-Madrid MJ, Reiter R, Hardeland R, Rol MA and Madrid JA:
Protecting the melatonin rhythm through circadian healthy light
exposure. Int J Mol Sci. 15:23448–23500. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lewis SR, Pritchard MW, Schofield-Robinson
OJ, Alderson P and Smith AF: Melatonin for the promotion of sleep
in adults in the intensive care unit. Cochrane Database Syst Rev.
5(CD012455)2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mo Y, Scheer CE and Abdallah GT: Emerging
Role of Melatonin and Melatonin Receptor Agonists in Sleep and
Delirium in Intensive Care Unit Patients. J Intensive Care Med.
31:451–455. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Gobbi G and Comai S: Differential Function
of Melatonin MT1 and MT2Receptors in REM and NREM Sleep. Front
Endocrinol (Lausanne). 10(87)2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Comai S, Lopez-Canul M, De Gregorio D,
Posner A, Ettaoussi M, Guarnieri FC and Gobbi G: Melatonin MT1
receptor as a novel target in neuropsychopharmacology: MT1 ligands,
pathophysiological and therapeutic implications, and perspectives.
Pharmacol Res. 144:343–356. 2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Owino S, Buonfiglio DDC, Tchio C and
Tosini G: Melatonin Signaling a Key Regulator of Glucose
Homeostasis and Energy Metabolism. Front Endocrinol (Lausanne).
10(488)2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Hu JJ, Xiao LF, Song LL, Ge WB, Duan HW
and Jiang Y: The expression of melatonin receptors MT1 and MT2 is
regulated by E2 in sheep oviduct. Gen Comp Endocrinol.
286(113135)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Jablonska K, Nowinska K, Piotrowska A,
Partynska A, Katnik E, Pawelczyk K, Glatzel-Plucinska N,
Podhorska-Okolow M and Dziegiel P: Prognostic Impact of Melatonin
Receptors MT1 and MT2 in Non-Small Cell Lung Cancer (NSCLC).
Cancers (Basel). 11(E1001)2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Xu L, Su Y, Zhao Y, Sheng X, Tong R, Ying
X, Gao L, Ji Q, Gao Y, Yan Y, et al: Melatonin differentially
regulates pathological and physiological cardiac hypertrophy:
Crucial role of circadian nuclear receptor RORα signaling. J Pineal
Res. 67(e12579)2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ding S, Lin N, Sheng X, Zhao Y, Su Y, Xu
L, Tong R, Yan Y, Fu Y, He J, et al: Melatonin stabilizes
rupture-prone vulnerable plaques via regulating macrophage
polarization in a nuclear circadian receptor RORα-dependent manner.
J Pineal Res. 67(e12581)2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Puig Á, Rancan L, Paredes SD, Carrasco A,
Escames G, Vara E and Tresguerres JAF: Melatonin decreases the
expression of inflammation and apoptosis markers in the lung of a
senescence-accelerated mice model. Exp Gerontol. 75:1–7.
2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Peng Z, Zhang W, Qiao J and He B:
Melatonin attenuates airway inflammation via SIRT1 dependent
inhibition of NLRP3 inflammasome and IL-1β in rats with COPD. Int
Immunopharmacol. 62:23–28. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Chen J, Qian C, Duan H, Cao S, Yu X, Li J,
Gu C, Yan F, Wang L and Chen G: Melatonin attenuates neurogenic
pulmonary edema via the regulation of inflammation and apoptosis
after subarachnoid hemorrhage in rats. J Pineal Res. 59:469–477.
2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Shin I-S, Shin N-R, Park J-W, Jeon C-M,
Hong J-M, Kwon O-K, Kim J-S, Lee I-C, Kim J-C, Oh S-R, et al:
Melatonin attenuates neutrophil inflammation and mucus secretion in
cigarette smoke-induced chronic obstructive pulmonary diseases via
the suppression of Erk-Sp1 signaling. J Pineal Res. 58:50–60.
2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Hardeland R: Melatonin and
inflammation-Story of a double-edged blade. J Pineal Res.
65(e12525)2018.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Zhang Y, Li X, Grailer JJ, Wang N, Wang M,
Yao J, Zhong R, Gao GF, Ward PA, Tan D-X, et al: Melatonin
alleviates acute lung injury through inhibiting the NLRP3
inflammasome. J Pineal Res. 60:405–414. 2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Aguilar SA, Arias PV, Canquil I,
Ebensperger G, Llanos AJ, Reyes RV, González-Candia A and Herrera
EA: Melatonin modulates the expression of pulmonary prostanoids.
Rev Med Chil. 147:281–288. 2019.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
37
|
Wu X, Ji H, Wang Y, Gu C, Gu W, Hu L and
Zhu L: Melatonin Alleviates Radiation-Induced Lung Injury via
Regulation of miR-30e/NLRP3 Axis. Oxid Med Cell Longev.
2019(4087298)2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Pourhanifeh MH, Sharifi M, Reiter RJ,
Davoodabadi A and Asemi Z: Melatonin and non-small cell lung
cancer: New insights into signaling pathways. Cancer Cell Int.
19(131)2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Panmanee J, Nopparat C, Chavanich N,
Shukla M, Mukda S, Song W, Vincent B and Govitrapong P: Melatonin
regulates the transcription of βAPP-cleaving secretases mediated
through melatonin receptors in human neuroblastoma SH-SY5Y cells. J
Pineal Res. 59:308–320. 2015.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Hardeland R: Aging, Melatonin, and the
Pro- and Anti-Inflammatory Networks. Int J Mol Sci.
20(E1223)2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Wang M-L, Wei C-H, Wang W-D, Wang J-S,
Zhang J and Wang J-J: Melatonin attenuates lung
ischaemia-reperfusion injury via inhibition of oxidative stress and
inflammation. Interact Cardiovasc Thorac Surg. 26:761–767.
2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Sánchez A, Calpena AC and Clares B:
Evaluating the Oxidative Stress in Inflammation: Role of Melatonin.
Int J Mol Sci. 16:16981–17004. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Carrascal L, Nunez-Abades P, Ayala A and
Cano M: Role of Melatonin in the Inflammatory Process and its
Therapeutic Potential. Curr Pharm Des. 24:1563–1588.
2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Mańka S and Majewska E: Immunoregulatory
action of melatonin. The mechanism of action and the effect on
inflammatory cells. Postepy Hig Med Dosw. 70:1059–1067.
2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Dong Y-J, Ding C-H, Zhang Z, Gu W-W and Ma
Y-L: Protective effects of melatonin in acute lung injury rats
caused by LPS. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 26:481–484.
2010.PubMed/NCBI(In Chinese).
|
|
46
|
Chiu M-H, Su C-L, Chen C-F, Chen K-H, Wang
D and Wang J-J: Protective effect of melatonin on liver
ischemia-reperfusion induced pulmonary microvascular injury in
rats. Transplant Proc. 44:962–965. 2012.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Reiter RJ, Rosales-Corral S, Tan DX, Jou
MJ, Galano A and Xu B: Melatonin as a mitochondria-targeted
antioxidant: One of evolution's best ideas. Cell Mol Life Sci.
74:3863–3881. 2017.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Bhattacharya S, Patel KK, Dehari D,
Agrawal AK and Singh S: Melatonin and its ubiquitous anticancer
effects. Mol Cell Biochem. 462:133–155. 2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Tan D-X, Reiter RJ, Manchester LC, Yan MT,
El-Sawi M, Sainz RM, Mayo JC, Kohen R, Allegra M and Hardeland R:
Chemical and physical properties and potential mechanisms:
Melatonin as a broad spectrum antioxidant and free radical
scavenger. Curr Top Med Chem. 2:181–197. 2002.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Poeggeler B, Thuermann S, Dose A, Schoenke
M, Burkhardt S and Hardeland R: Melatonin's unique radical
scavenging properties - roles of its functional substituents as
revealed by a comparison with its structural analogs. J Pineal Res.
33:20–30. 2002.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Zheng X, Zhou J, Tan D-X, Wang N, Wang L,
Shan D and Kong J: Melatonin Improves Waterlogging Tolerance of
Malus baccata (Linn.) Borkh. Seedlings by Maintaining
Aerobic Respiration, Photosynthesis and ROS Migration. Front Plant
Sci. 8(483)2017.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Yildiz A, Vardi N, Karaaslan MG, Ates B,
Taslidere E and Esrefoglu M: The protective effect of melatonin in
lungs of newborn rats exposed to maternal nicotine. Biotech
Histochem. 93:442–452. 2018.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Reiter RJ, Mayo JC, Tan D-X, Sainz RM,
Alatorre-Jimenez M and Qin L: Melatonin as an antioxidant: Under
promises but over delivers. J Pineal Res. 61:253–278.
2016.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Charão MF, Goethel G, Brucker N, Paese K,
Eifler-Lima VL, Pohlmann AR, Guterres SS and Garcia SC:
Melatonin-loaded lipid-core nanocapsules protect against lipid
peroxidation caused by paraquat through increased SOD expression in
Caenorhabditis elegans. BMC Pharmacol Toxicol. 20 (Suppl
1)(80)2019.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Radovic M, Ristic L, Krtinic D, Rancic M,
Nickovic V, Vujnovic Zivkovic ZN, Zivkovic JB, Mirkovic MV, Toskic
DR and Sokolovic D: Melatonin treatment prevents carbon
tetrachloride-induced acute lung injury in rats by mitigating
tissue antioxidant capacity and inflammatory response. Bratisl Lek
Listy. 120:527–531. 2019.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Chen W, Chen X, Chen AC, Shi Q, Pan G, Pei
M, Yang H, Liu T and He F: Melatonin restores the
osteoporosis-impaired osteogenic potential of bone marrow
mesenchymal stem cells by preserving SIRT1-mediated intracellular
antioxidant properties. Free Radic Biol Med. 146:92–106.
2020.PubMed/NCBI View Article : Google Scholar
|
|
57
|
de Matos Cavalcante AG, de Bruin PFC, de
Bruin VMS, Nunes DM, Pereira EDB, Cavalcante MM and Andrade GM:
Melatonin reduces lung oxidative stress in patients with chronic
obstructive pulmonary disease: A randomized, double-blind,
placebo-controlled study. J Pineal Res. 53:238–244. 2012.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Chen D, Zhang T and Lee TH: Cellular
Mechanisms of Melatonin: Insight from Neurodegenerative Diseases.
Biomolecules. 10(E1158)2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Ostadmohammadi V, Soleimani A, Bahmani F,
Aghadavod E, Ramezani R, Reiter RJ, Mansournia MA, Banikazemi Z,
Soleimani M, Zaroudi M, et al: The Effects of Melatonin
Supplementation on Parameters of Mental Health, Glycemic Control,
Markers of Cardiometabolic Risk, and Oxidative Stress in Diabetic
Hemodialysis Patients: A Randomized, Double-Blind,
Placebo-Controlled Trial. J Ren Nutr. 30:242–250. 2020.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Carlomagno G, Minini M, Tilotta M and
Unfer V: From Implantation to Birth: Insight into Molecular
Melatonin Functions. Int J Mol Sci. 19(E2802)2018.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Tan D-X, Hardeland R, Manchester LC,
Galano A and Reiter RJ: Cyclic-3-hydroxymelatonin (C3HOM), a potent
antioxidant, scavenges free radicals and suppresses oxidative
reactions. Curr Med Chem. 21:1557–1565. 2014.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Fang Y, Zhang J, Li Y, Guo X, Li J, Zhong
R and Zhang X: Melatonin-induced demethylation of antioxidant genes
increases antioxidant capacity through RORα in cumulus cells of
prepubertal lambs. Free Radic Biol Med. 131:173–183.
2019.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Esteban MÁ, Cuesta A, Chaves-Pozo E and
Meseguer J: Influence of melatonin on the immune system of fish: A
review. Int J Mol Sci. 14:7979–7999. 2013.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Carrillo-Vico A, Guerrero JM, Lardone PJ
and Reiter RJ: A review of the multiple actions of melatonin on the
immune system. Endocrine. 27:189–200. 2005.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Lee J, Byun H, Madhurakkat Perikamana SK,
Lee S and Shin H: Current Advances in Immunomodulatory Biomaterials
for Bone Regeneration. Adv Healthc Mater.
8(e1801106)2019.PubMed/NCBI View Article : Google Scholar : Zhang R, Wang X,
Ni L, Di X, Ma B, Niu S, Liu C and Reiter RJ: COVID-19: Melatonin
as a potential adjuvant treatment. Life Sci 250: 117583, 2020.
|
|
66
|
Channappanavar R and Perlman S: Pathogenic
human coronavirus infections: Causes and consequences of cytokine
storm and immunopathology. Semin Immunopathol. 39:529–539.
2017.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Haldar C and Ahmad R:
Photoimmunomodulation and melatonin. J Photochem Photobiol B.
98:107–117. 2010.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Wu X, Ji H, Wang Y, Gu C, Gu W, Hu L and
Zhu L: Melatonin Alleviates Radiation-Induced Lung Injury via
Regulation of miR-30e/NLRP3 Axis. Oxid Med Cell Longev.
2019(4087298)2019.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Miller SC, Pandi-Perumal SR, Esquifino AI,
Cardinali DP and Maestroni GJM: The role of melatonin in
immuno-enhancement: Potential application in cancer. Int J Exp
Pathol. 87:81–87. 2006.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Butt Y, Kurdowska A and Allen TC: Acute
Lung Injury: A Clinical and Molecular Review. Arch Pathol Lab Med.
140:345–350. 2016.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Morales-Ortíz J, Deal V, Reyes F,
Maldonado-Martínez G, Ledesma N, Staback F, Croft C, Pacheco A,
Ortiz-Zuazaga H, Yost CC, et al: Platelet-derived TLT-1 is a
prognostic indicator in ALI/ARDS and prevents tissue damage in the
lungs in a mouse model. Blood. 132:2495–2505. 2018.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Bellani G, Laffey JG, Pham T, Fan E,
Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley
DF, et al: LUNG SAFE Investigators; ESICM Trials Group:
Epidemiology, Patterns of Care, and Mortality for Patients With
Acute Respiratory Distress Syndrome in Intensive Care Units in 50
Countries. JAMA. 315:788–800. 2016.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Rubenfeld GD, Caldwell E, Peabody E,
Weaver J, Martin DP, Neff M, Stern EJ and Hudson LD: Incidence and
outcomes of acute lung injury. N Engl J Med. 353:1685–1693.
2005.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Ranieri VM, Rubenfeld GD, Thompson BT,
Ferguson ND, Caldwell E, Fan E, Camporota L and Slutsky AS: ARDS
Definition Task Force. Acute respiratory distress syndrome: The
Berlin Definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Ozdinc S, Oz G, Ozdemir C, Kilic I,
Karakaya Z, Bal A, Koken T and Solak O: Melatonin: Is it an
effective antioxidant for pulmonary contusion? J Surg Res.
204:445–451. 2016.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Zhang Z, Gao L, Ding C-H, Ma W-Z, Gu W-W
and Ma Y-L: Protective function of melatonin to acute lung injury
and its mechanisms in rats caused by oleic acid. Zhongguo Ying Yong
Sheng Li Xue Za Zhi. 27:480–483. 2011.PubMed/NCBI(In Chinese).
|
|
77
|
Taslidere E, Esrefoglu M, Elbe H, Cetin A
and Ates B: Protective effects of melatonin and quercetin on
experimental lung injury induced by carbon tetrachloride in rats.
Exp Lung Res. 40:59–65. 2014.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Wu WS, Chou MT, Chao CM, Chang CK, Lin MT
and Chang CP: Melatonin reduces acute lung inflammation, edema, and
hemorrhage in heatstroke rats. Acta Pharmacol Sin. 33:775–782.
2012.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Huai J-P, Sun X-C, Chen M-J, Jin Y, Ye
X-H, Wu J-S and Huang Z-M: Melatonin attenuates acute
pancreatitis-associated lung injury in rats by modulating
interleukin 22. World J Gastroenterol. 18:5122–5128.
2012.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Zhang XH, Qi HX, Xu DS, Pang XC, Wang CY
and Yu WJ: Expression of proteinase-activated receptor-2 and
transient receptor potential A1 in vagal afferent nerve of rat
after lung schemia-reperfusion injury. J Biol Regul Homeost Agents.
33:1405–1413. 2019.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Fındık O, Yılmaz MY, Yazır Y, Rençber SF,
Sarıhan KK and Kunt AT: Investigation of the protective effect of
enoxaparin and ticagrelor pretreatment against ischemia-reperfusion
injury in rat lung tissue. Rev Assoc Med Bras (1992). 65:1193–1200.
2019.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Esteban-Zubero E, García-Gil FA,
López-Pingarrón L, Alatorre-Jiménez MA, Iñigo-Gil P, Tan D-X,
García JJ and Reiter RJ: Potential benefits of melatonin in organ
transplantation: A review. J Endocrinol. 229:R129–R146.
2016.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Banaei S, Ahmadiasl N and Alihemmati A:
Comparison of the Protective Effects of Erythropoietin and
Melatonin on Renal Ischemia-Reperfusion Injury. Trauma Mon.
21(e23005)2016.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Takhtfooladi H, Takhtfooladi M, Moayer F
and Mobarakeh S: Melatonin attenuates lung injury in a hind limb
ischemia-reperfusion rat model. Rev Port Pneumol. 21:30–35.
2015.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Lambrecht BN and Hammad H: The airway
epithelium in asthma. Nat Med. 18:684–692. 2012.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Ryzhov S, Goldstein AE, Matafonov A, Zeng
D, Biaggioni I and Feoktistov I: Adenosine-activated mast cells
induce IgE synthesis by B lymphocytes: An A2B-mediated process
involving Th2 cytokines IL-4 and IL-13 with implications for
asthma. J Immunol. 172:7726–7733. 2004.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Steurer-Stey C: Asthmamanagement:
Uberblick und neue Aspekte. Praxis (Bern 1994). 96:1951–1957.
2007.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
88
|
Woodruff Pg, Modrek B, Choy DF, Jia g,
Abbas AR, Ellwanger A, Koth LL, Arron JR and Fahy JV: T-helper Type
2–driven Inflammation Defines Major Subphenotypes of Asthma. Am J
Respir Crit Care Med. 180:388–395. 2009.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Brown V and Ennis M: T Cell Cytokine
Production in Childhood Asthma. CRMR. 1:1–6. 2005.
|
|
90
|
Huang W-C, Liu C-Y, Shen S-C, Chen L-C,
Yeh K-W, Liu S-H and Liou C-J: Protective Effects of Licochalcone A
Improve Airway Hyper-Responsiveness and Oxidative Stress in a Mouse
Model of Asthma. Cells. 8(E617)2019.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Cobham VE, Hickling A, Kimball H, Thomas
HJ, Scott JG and Middeldorp CM: Systematic Review: Anxiety in
Children and Adolescents With Chronic Medical Conditions. J Am Acad
Child Adolesc Psychiatry 59:. 59:595–618. 2019.PubMed/NCBI View Article : Google Scholar
|
|
92
|
To T, Stanojevic S, Moores G, Gershon AS,
Bateman ED, Cruz AA and Boulet L-P: Global asthma prevalence in
adults: Findings from the cross-sectional world health survey. BMC
Public Health. 12(204)2012.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Wang YT, Chen SL and Xu SY: Effect of
melatonin on the expression of nuclear factor-kappa B and airway
inflammation in asthmatic rats. Zhonghua Er Ke Za Zhi. 42:94–97.
2004.PubMed/NCBI(In Chinese).
|
|
94
|
Wu H-M, Shen Q-Y, Fang L, Zhang S-H, Shen
P-T, Liu Y-J and Liu R-Y: JNK-TLR9 signal pathway mediates allergic
airway inflammation through suppressing melatonin biosynthesis. J
Pineal Res. 60:415–423. 2016.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Shin I-S, Park J-W, Shin N-R, Jeon C-M,
Kwon O-K, Kim J-S, Kim J-C, Oh S-R and Ahn K-S: Melatonin reduces
airway inflammation in ovalbumin-induced asthma. Immunobiology.
219:901–908. 2014.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Shin I-S, Park J-W, Shin N-R, Jeon C-M,
Kwon O-K, Lee M-Y, Kim H-S, Kim J-C, Oh S-R and Ahn K-S: Melatonin
inhibits MUC5AC production via suppression of MAPK signaling in
human airway epithelial cells. J Pineal Res. 56:398–407.
2014.PubMed/NCBI View Article : Google Scholar
|
|
97
|
American Thoracic Society. Standardization
of Spirometry, 1994 Update. Am J Respir Crit Care Med.
152:1107–1136. 1995.PubMed/NCBI View Article : Google Scholar
|
|
98
|
Campos FL, da Silva-Júnior FP, de Bruin VM
and de Bruin PF: Melatonin improves sleep in asthma: A randomized,
double-blind, placebo-controlled study. Am J Respir Crit Care Med.
170:947–951. 2004.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Li Q, Qu HJ, Lv D, Yeh M-K, Sun S, Li L
and Liao Y: Drug-related problems among hospitalized patients with
COPD in mainland China. Int J Clin Pharm. 41:1507–1515.
2019.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Kc R, Shukla SD, Gautam SS, Hansbro PM and
O'Toole RF: The role of environmental exposure to non-cigarette
smoke in lung disease. Clin Transl Med. 7(39)2018.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Brandsma CA, Van den Berge M, Hackett TL,
Brusselle G and Timens W: Recent advances in chronic obstructive
pulmonary disease pathogenesis: From disease mechanisms to
precision medicine. J Pathol. 250:624–635. 2020.PubMed/NCBI View Article : Google Scholar
|
|
102
|
He B, Zhang W, Qiao J, Peng Z and Chai X:
Melatonin protects against COPD by attenuating apoptosis and
endoplasmic reticulum stress via upregulating SIRT1 expression in
rats. Can J Physiol Pharmacol. 97:386–391. 2019.PubMed/NCBI View Article : Google Scholar
|
|
103
|
Shin N-R, Ko J-W, Kim J-C, Park G, Kim
S-H, Kim M-S, Kim J-S and Shin I-S: Role of melatonin as an SIRT1
enhancer in chronic obstructive pulmonary disease induced by
cigarette smoke. J Cell Mol Med. 24:1151–1156. 2020.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Cherpanath TGV, Smeding L, Hirsch A,
Lagrand WK, Schultz MJ and Groeneveld ABJ: Low tidal volume
ventilation ameliorates left ventricular dysfunction in
mechanically ventilated rats following LPS-induced lung injury. BMC
Anesthesiol. 15(140)2015.PubMed/NCBI View Article : Google Scholar
|
|
105
|
Pandita A, Murki S, Oleti TP, Tandur B,
Kiran S, Narkhede S and Prajapati A: Effect of Nasal Continuous
Positive Airway Pressure on Infants With Meconium Aspiration
Syndrome: A Randomized Clinical Trial. JAMA Pediatr. 172:161–165.
2018.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Sutherasan Y, Vargas M and Pelosi P:
Protective mechanical ventilation in the non-injured lung: Review
and meta-analysis. Crit Care. 18(211)2014.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Ball L, Hemmes SNT, Serpa Neto A, Bluth T,
Canet J, Hiesmayr M, Hollmann MW, Mills GH, Vidal Melo MF, Putensen
C, et al: LAS VEGAS investigators; PROVE Network; Clinical Trial
Network of the European Society of Anaesthesiology: Intraoperative
ventilation settings and their associations with postoperative
pulmonary complications in obese patients. Br J Anaesth.
121:899–908. 2018.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Yu Q, Wang D, Wen X, Tang X, Qi D, He J,
Zhao Y, Deng W and Zhu T: Adipose-derived exosomes protect the
pulmonary endothelial barrier in ventilator-induced lung injury by
inhibiting the TRPV4/Ca2+ signaling pathway. Am J
Physiol Lung Cell Mol Physiol. 318:L723–L741. 2020.PubMed/NCBI View Article : Google Scholar
|
|
109
|
van der Zee P and Gommers D: Recruitment
Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in
Patients with ARDS. Crit Care. 23(73)2019.PubMed/NCBI View Article : Google Scholar
|
|
110
|
Alkasalias T, Alexeyenko A, Hennig K,
Danielsson F, Lebbink RJ, Fielden M, Turunen SP, Lehti K, Kashuba
V, Madapura HS, et al: RhoA knockout fibroblasts lose
tumor-inhibitory capacity in vitro and promote tumor growth in
vivo. Proc Natl Acad Sci USA. 114:E1413–E1421. 2017.PubMed/NCBI View Article : Google Scholar
|
|
111
|
Sripathi SR, Prigge CL, Elledge B, He W,
Offor J, Gutsaeva DR and Jahng WJ: Melatonin Modulates Prohibitin
and Cytoskeleton in the Retinal Pigment Epithelium. Int J Sci Eng
Res. 8:502–506. 2017.PubMed/NCBI View Article : Google Scholar
|
|
112
|
Gu C, Liu M, Zhao T, Wang D and Wang Y:
Protective role of p120-catenin in maintaining the integrity of
adherens and tight junctions in ventilator-induced lung injury.
Respir Res. 16(58)2015.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Ito K, Colley T and Mercado N:
Geroprotectors as a novel therapeutic strategy for COPD, an
accelerating aging disease. Int J Chron Obstruct Pulmon Dis.
7:641–652. 2012.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Giamarellos-Bourboulis EJ, Netea MG,
Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, Damoraki G,
Gkavogianni T, Adami M-E, Katsaounou P, et al: Complex Immune
Dysregulation in COVID-19 Patients with Severe Respiratory Failure.
Cell Host Microbe. 27:992–1000.e3. 2020.PubMed/NCBI View Article : Google Scholar
|