1. Introduction
The first description of Guillain-Barré syndrome
(GBS) dates back to 1859, when Landry published a description of a
case with ascending paralysis (1).
The clinical and biological picture was later completed in 1916 by
French neurologists Georges Guillain, Jean-Alexandre Barré and
Andre Strohl (2).
GBS is an acute immune-mediated disease that reaches
maximum severity within 2-4 weeks. GBS affects the peripheral
nervous system and is characterized by progressive motor deficit in
the limbs with ascending sensory deficits, involvement of muscles
innervated by the cranial nerves, reduction or abolition of the
deep tendon reflexes, and possible impairment of the autonomic
nervous system, sometimes with respiratory failure and
albuminocytological dissociation (3). Due to the respiratory and autonomic
nervous dysfunction, the disease has the potential to be fatal even
when patients are treated at centers that provide optimal care.
From the neurophysiological point of view, the following phenotypes
of GBS are described: Acute inflammatory demyelinating
polyradiculoneuropathy (AIDP), Miller Fisher syndrome and acute
autonomic neuropathy (4) and the
axonal variants, acute motor sensory neuropathy (AMSAN) and acute
motor axonal neuropathy (AMAN). Axonal variants were first
recognized in northern China and then reported in other countries
(3,5). In North America and Europe the
incidence of AMAN is low (6,7).
The idea of molecular mimicry between pathogens and
autologous antigens has been proposed as a possible mechanism of
this autoimmune disease. In AIDP, the patient's immune system
generates antibodies that cross-react with shared epitopes against
myelin or the Schwann cell surface membrane (8).
Characteristic for AMAN is the association with
Campylobacter jejuni (C. jejuni) enteritis;
therefore, the antibodies against gangliosides are characteristic
(3,8-10).
The molecular mimicry and the structural similarity between
GM1/GD1a gangliosides and the lipo-oligosaccharides of C.
jejuni has been proven by numerous bacteriological,
immunological and pathological studies (8,11). The
immune response is mediated by antibodies against GM1 and GD1a that
are situated at the level of Ranvier nodes where the axolemma is
exposed and the sodium-channels are clustered (8,12).
Immunohistochemical studies from deceased patients
reveal antibody-mediated alteration of the motor axonal membrane,
suggesting that the immune response is primarily directed against
the motor axolemma (8,13). In AMAN, morphopathological
examination have shown deposits of IgG and complement in the
axolemma of the motor nerves at the Ranvier nodes, with minimal
demyelinating damage and mild lymphocytic infiltration, followed by
macrophage infiltration (2,14). The macrophages invade the axon at
the Ranvier nodes, where they insert between Schwann cells and the
axon without affecting the myelin sheath and produce nerve damage
and functional blockage of nerve transmission (15). After the complement activation the
development of the complement membrane attack complex occurs and
disrupts the sodium channels. The sodium channel dysfunction can
explain the changes in the nerve conduction studies, slowing the
motor conduction and producing variable degrees of conduction
blocks, due to the fact that saltatory conduction is critically
altered (8,12).
In advanced stages with ventral root involvement,
irreversible changes with severe axonal degeneration may occur
(16), if the underlying
pathophysiological mechanism is not controlled. Therefore, rapid
therapeutic interventions that trigger the neutralization of the
autoantibodies, easing the conduction blocks, may lead to a rapid
resolution of the symptoms. Contrary, a mediocre recovery is
expected if the axonal degeneration occurs at the level of the
nerve roots (8,17). The uncertainty is whether which type
of intervention may result in a better clinical evolution,
depending on the GBS subtype.
Although modern methods of treatment such as
therapeutic plasma exchange (TPE) and intravenous immunoglobulins
(IVIg) have significantly improved the prognosis, many patients
nevertheless experience significant neurological sequelae (5,18).
2. Practical applicability of
plasmapheresis: Case illustration
We report the case of a previously healthy
27-year-old man who had a mild viral respiratory tract infection 1
week prior to the onset of disease. Two days before admission to
our clinic, the patient experienced paresthesia in the lower limbs
with ascending character towards the upper limbs, followed by
progressive weakness with the same distribution as the paresthesia.
Neurological examination performed at admission did not reveal any
changes in the cranial nerves, but detected flaccid tetraparesis of
Medical Research Council (MRC) (19) grade 4/5 in the upper limbs and MRC
grade 3/5 in the lower limbs, diminished deep tendon reflexes in
the upper limbs and abolished deep tendon reflexes in the lower
limbs, without pyramidal signs, with no sensitivity disorders. The
evaluation performed after the Hughes functional grading scale
(HFGS) (20) at admission placed
the patient at grade 4. On the following day, the patient's
evolution was rapidly progressive, with worsening of the motor
deficit to MRC grade 2/5 in the upper and lower limbs with slight
swallowing difficulties and mild respiratory dysfunction, requiring
oxygen support. He also developed urinary retention, and a Foley
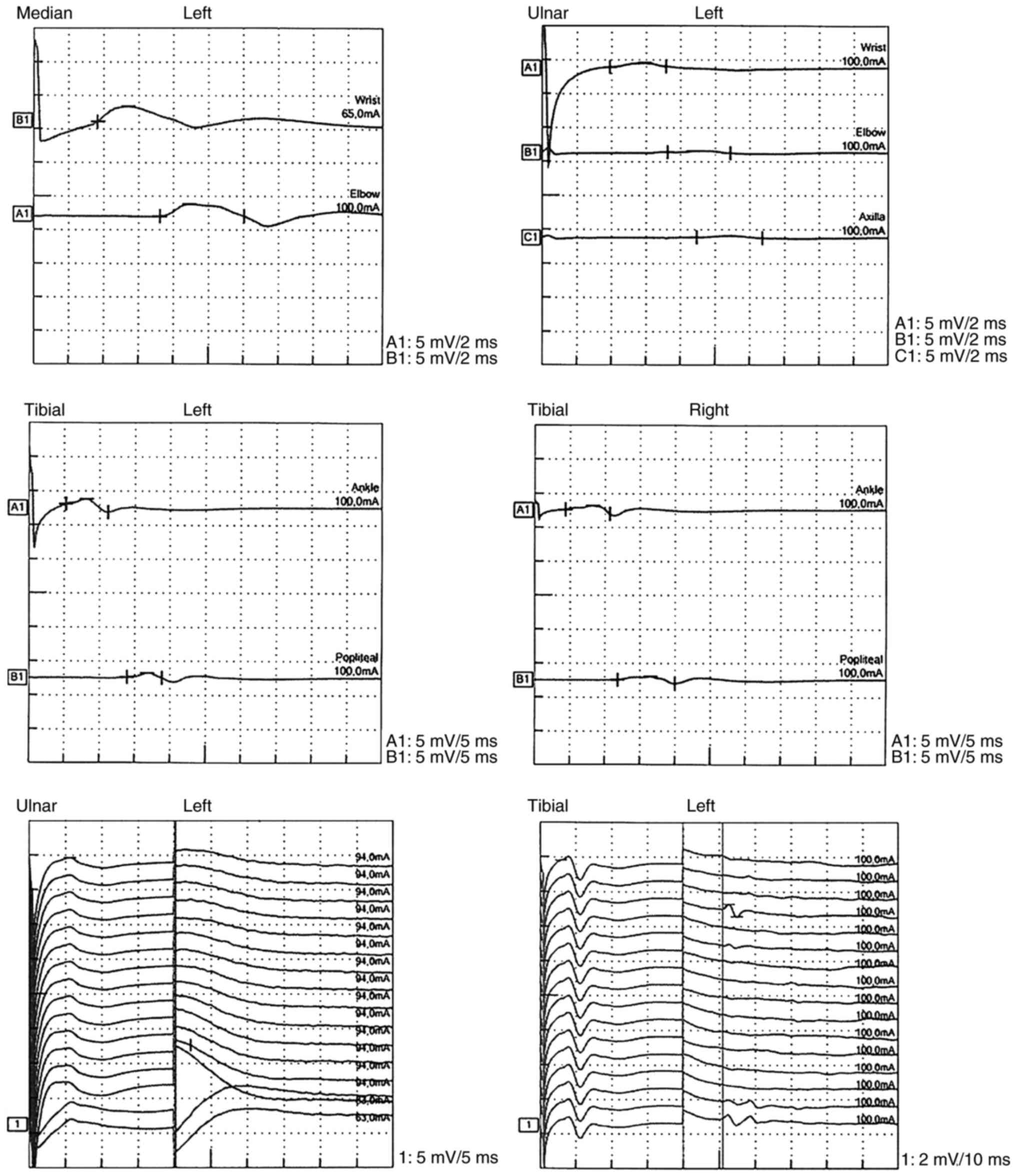
catheter was inserted. Nerve conduction studies (NCS) were
performed on the same day using conventional procedures, with motor
conduction studies on the medial, ulnar, peroneal and tibial nerves
bilaterally, and sensory conduction studies on the medial, ulnar
and sural nerves bilaterally. A low amplitude of compound muscle
action potential (CMAP) was detected in all motor nerves, aspects
that are characteristic for marked axonal loss. Examination of the
F wave showed a proximal conduction block of 100% at the level of
the median and ulnar nerves and a conduction block of 80-90% at the
level of the bilateral tibial nerve, suggesting proximal root
involvement (Fig. 1). The sensory
conduction was within normal limits. Following the NCS examination,
the diagnosis of the AMAN phenotypic variant of GBS was
established. The peripheral oxygen saturation measured by
pulsoximeter was 92%. The acid-base balance revealed a mild
respiratory acidosis with pH 7.27, PaO2 116 mmHg,
PaCO2 65 mmHg at a FiO2 0.4 with BE-1.2 mmol,
bicarbonate 24 mEq/l. Lumbar puncture with cortical spinal fluid
(CSF) examination was performed and was normal. Laboratory tests
ruled out infectious diseases [human immunodeficiency virus (HIV),
syphilis, hepatitis B and C, Lyme disease serology],
endocrinopathies and autoimmune diseases [anti-double stranded DNA
(anti-dsDNA), anti-nuclear antibodies (ANAs), antiphospholipid
antibodies were within normal limits]; serum protein
electrophoresis revealed no anomalies. His stool cultures were
negative; tests for anti-gangliosides antibody, Campylobacter
jejuni (C jejuni) and Mycoplasma pneumoniae
(M. peumoniae) antibody are not available in our hospital.
The patient also underwent a thoraco-abdominopelvic computed
tomography scan, which was within normal limits, to rule out a
paraneoplastic syndrome. He underwent cervical spine magnetic
resonance imaging (MRI), which excluded the possibility of
transverse myelitis.
On day 2 after admission and on day 4 after the
first symptoms, TPE was initiated immediately in hospital using a
commercially available system (Spectra Optia Apheresis, TerumoBCT).
The exchange fluid was a combination of fresh frozen plasma (FFP)
and 5% albumin solution with an Anticoagulant Citrate Dextrose,
SolutionA, (ACD-A) anticoagulant solution at 10:1 whole
blood:citrate ratio. The flow inlet rate varied between 30 and 70
ml/min according to the type of replacement fluid used and the
functioning of the peripheral venous approach. The procedure was
performed using the peripheral venous approach with two peripheral
catheters 16 Gauge diameter each placed at the antecubital veins on
both sides for the inlet and the outlet circuits. During TPE, the
patient received a prophylactic infusion of calcium supplementation
consisting of 10% calcium gluconate to prevent a symptomatic fall
in plasma ionized calcium due to citrate anticoagulation. After the
first TPE session, respiratory symptoms were significantly
improved, the peripheral oxygen saturation increased up to 96%,
therefore, subsequent arterial blood gases analyses were between
normal ranges.
In the first plasma exchange session, 1.1 plasma
volume (PV) was exchanged; in the second session, 1.2 PV was
exchanged. In the third session, only 0.5 PV was exchanged because
the patient developed an allergic reaction to plasma, with
generalized rash, pruritus and dyspnoea with hypo-oxygenation and
decreased oxygen saturation of 89%. The procedure was stopped
immediately, and 50 mg Ranitidine (Medochemie Ltd.) i.v., 200 mg
hydrocortisone hemisuccinate (HHS) (Zentiva) i.v. and 10 mg
Claritin (Schering Plough Labo NV, Belgium) orally were
administered with rapid allergic reaction regression. On the
following day, the fourth exchange was performed with 1.2 PV. Each
session was separated by 2 days, except for sessions 3 and 4, which
were held on two consecutive days, and a total of 4 PVs were
exchanged, and a combination of FFP and 5% albumin solution was
used as replacement. Following the initial allergic reaction, the
patient received 200 mg HHS (Zentiva) i.v. 2 h prior to TPE to
prevent other allergic reactions.
Laboratory testing was performed before the first
session of TPE, and then performed after each session to check the
complete blood count, calcium, magnesium, potassium, sodium,
glucose, creatinine and blood urea nitrogen. There were no
significant changes in the above parameters before the first TPE
and after the last TPE session (Table
I).
 | Table ILaboratory parameters during the
plasma exchange sessions. |
Table I
Laboratory parameters during the
plasma exchange sessions.
| | Before session
#1 | Before session
#2 | Before session
#3 | Before session
#4 |
|---|
| Hematocrit (%) | 46.5 | 48.5 | 53.2 | 51.1 |
| Platelet count
(/µl) | 297,000 | 346,000 | 344,000 | 314,000 |
| Total calcium
(mg/dl) | 2.14 | 2.43 | 2.38 | 2.3 |
| Magnesium
(mg/dl) | 0.99 | 0.9 | 1.03 | 0.95 |
| Potassium
(mmol/l) | 4.27 | 4.23 | 4.36 | 3.81 |
| Sodium
(mmol/l) | 141 | 140 | 141 | 137 |
| Creatinine
(mg/dl) | 0.70 | 0.80 | 0.69 | 0.67 |
| Blood urea nitrogen
(mg/dl) | 24.1 | 33.1 | 46.3 | 52 |
| Glucose
(mg/dl) | 101 | 96.9 | 95.0 | 88 |
The neurological evaluation performed after plasma
exchange session 4, i.e. on day 8 after admission, revealed
significant improvement, with regression of motor deficit in all
limbs at MRC grade 4/5, and he was able to pass urine, therefore
the Foley catheter was removed. He experienced no additional
TPE-related complications during or after the procedure and had no
difficulties related to peripheral venous access. We decided to
continue kinetotherapy and the supportive treatment with further
favorable evolution, and he was discharged 1 week later. The
patient was discharged with HFGS grade 2 with an improvement of 2
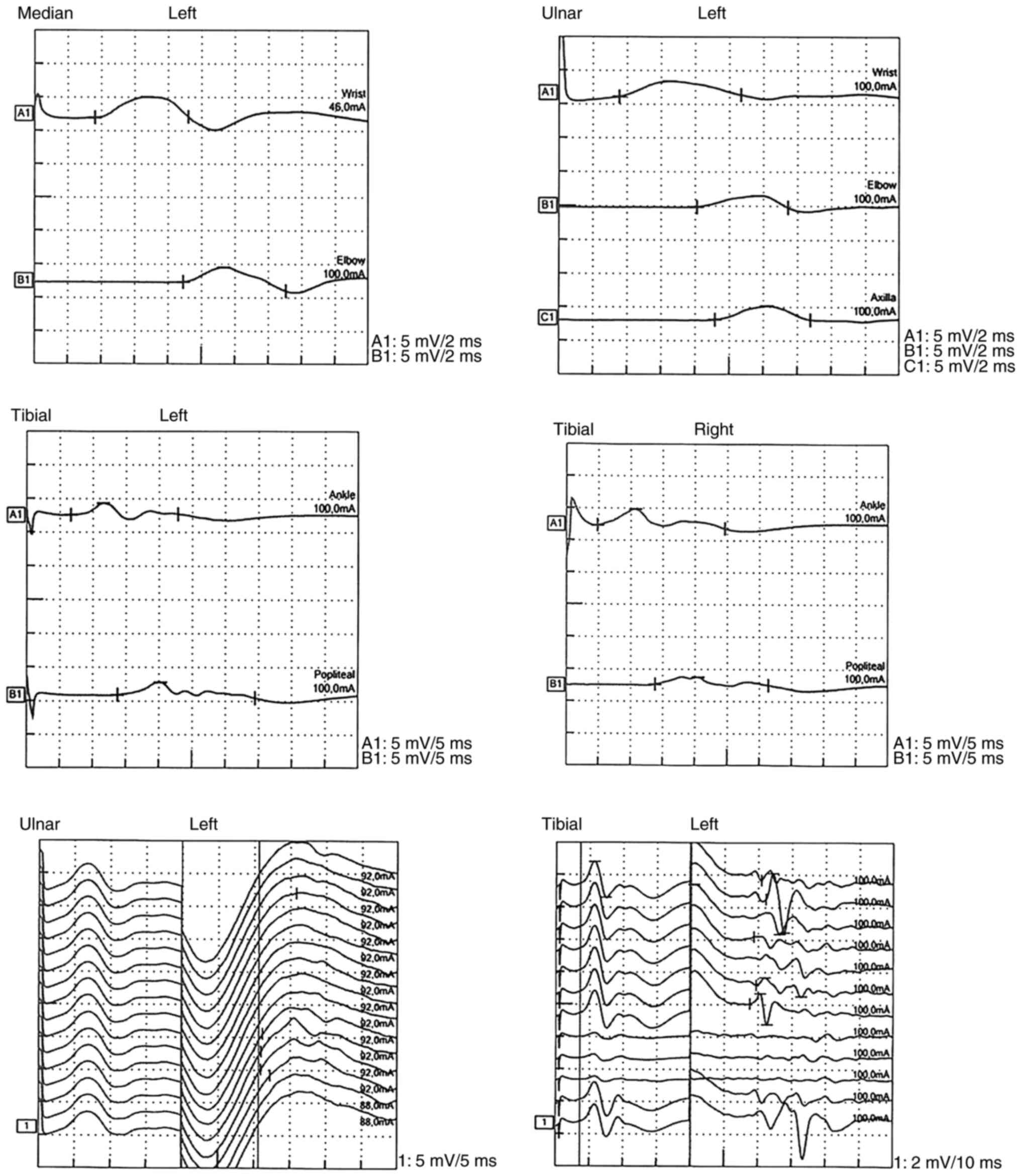
points compared with that at admission. NCS performed 2 weeks after
admission revealed also significant improvement (Fig. 2). One month later, the patient was
completely recovered, and the NCS no longer showed pathological
changes.
3. Discussion
The proportion of different GBS subtypes varies by
region. AMAN is more common in China, but there are also percentage
differences between northern and southern China (21-23).
In a study on the pediatric population, also conducted in China,
22% of patients with GBS had AMAN (21), while another study conducted in two
centers in France (Toulouse and Montpellier) that included children
showed that AMAN was present in 17 of the total 110 patients
included in the study (24). In
North America and Europe, the AIDP subtype is the most common, and
only 5% are axonal subtypes of GBS (25), where the incidence of AMAN subtype
is 1-3% (6,7).
Clinical and epidemiological observations show that
GBS is associated with a preceding illness, and 75% of patients
report acute enterocolitis or upper respiratory infection (26). The most frequent pathogens involved
are C. jejuni, cytomegalovirus (CMV), Epstein-Barr virus
(EBV), Zika, post-flu or other events involving immunization with
vaccines such as rabies vaccines (27,28),
surgery and anesthesia (5). In the
case of AMAN, the most frequently involved pathogen is C.
jejuni (15). Our patient had a
respiratory viral infection prior to the onset of the GBS that
could be considered the trigger of the immune process but specific
serological and immunological tests did not reveal infections
without having data concerning C. jejuni and M.
pneumoniae.
TPE using the Spectra Optia system involves
separating plasma from hematocrit by centrifugation, and removing
and replacing the patient's plasma with an equal volume of fluid
replacement consisting of FFP and 5% albumin solution to maintain
appropriate oncotic pressure while the remaining cells are
re-infused back to the patient (29). In GBS, this procedure alters the T
helper 1 cell (Th1) to Th2 ratio, alters B cell and T cell number
and activation, and helps to reduce the concentration of pathogenic
plasma components such as circulating autoantibodies, immune
complexes, complements, cytokines or other immunologically active
substances (29). The benefit of
TPE is increased if the treatment is initiated early, i.e. within 7
days from the disease onset, according to a recent Cochrane review
(30,31), but still has beneficial effect in
the first 4 weeks from disease onset (16,32).
According to the 2019 American Society of Aphaeresis
(ASFA) guidelines the primary use of TPE in GBS is an ASFA category
I indication (recommendation grade. 1A) (4). It is recommended to exchange 1-1.5 PV
per session, 5-6 times over 10-14 days in an every-other-day
regimen (4). A TPE procedure
usually removes 60-70% of the substances from the intravascular
compartment (4). The interval
between procedures is required to allow rebalancing of the
intravascular space and to reduce the risk of bleeding caused by
the depletion of the anticoagulation factors, of which the main
factor is fibrinogen (30-33).
In moderate cases, there was no difference between patients who
underwent four PV exchanges and those who underwent six exchanges
(16,34). Our patient underwent four exchanges
with a total of four PV exchanges. In moderate to severe groups,
four sessions are beneficial (34,35),
while severe cases require 5-6 TPE procedures (4,29).
The most common adverse effects associated with TPE
cited in the medical literature are allergic reactions to plasma
(chills, fever, rash, hives, dyspnea and stridor), chest pain,
dizziness, headache, abdominal pain, anxiety, hypotension, nausea
and vomiting; the incidence is approximately 11% compared to those
receiving 5% albumin solution as fluid replacement; another adverse
effect is symptoms of hypocalcaemia when citrate is used as an
anticoagulant as a result of calcium ion binding in the blood.
Albumin is especially associated with adverse effects such as
hypotension, nausea and vomiting due to the hypo-oncotic effect
(36).
Our patient had peripheral venous access and no
access-related complications. He was closely monitored, and the
onset of plasma allergy was detected immediately, with immediate
cessation of plasmapheresis, administration of Claritin
(loratadine, 10 mg tablet), which is a second-generation histamine
1 (H1) receptor antagonist used to treat allergies, and 50 mg of
Ranitidine i.v., a H2 receptor inhibitor that relieves the symptoms
of acute allergic reactions. It has been observed that the
combination of blocking both the H1 and H2 receptors may provide
better relief (37).
Geographical variation, clinical course and disease
severity probably differ due to gene polymorphism in populations
with different susceptibility to developing different types of GBS.
In a study conducted by Estrade et al, the mean follow-up
period was 300 days; 77% of the patients recovered with progressive
regression of symptoms, and the mean recovery time was estimated at
280 days. The presence of sequelae was correlated with the short
duration between symptom onset and hospitalization and with the
axonal form of GBS (AMSAN or AMAN), with 29% of children with the
axonal form having sequelae compared to 5% of those with AIDP. We
should mention that, in our French colleagues' study, most children
received IVIg, unlike our patient who underwent four courses of TPE
(24). Other studies report that
the axonal forms (AMAN and AMSAN) are correlated with a higher risk
of long-term sequelae (38,39), and other authors consider that
although the axonal form of GBS has a longer recovery period
compared to the demyelinating forms, there are no long-term
differences between them (40,41).
In a study published in 2015 in a Chinese
population, HFGS at nadir (grade 0, healthy; grade 1, minor signs
and symptoms, able to run; grade 2, able to walk independently at
least 5 meters; grade 3, able to walk with assistance; grade 4,
bedbound; grade 5, requires assisted ventilation; grade 6,
deceased) was significantly higher in patients in the AMAN subgroup
of GBS, and the necessity for mechanical ventilation was higher
than in the AIDP group (21,42).
Reports of GBS in the pediatric population also show that patients
with axonal involvement have more severe disease progression and a
higher rate of morbidity and mortality than patients with AIDP
(43). Our patient, diagnosed with
AMAN, had an HFGS score of 4 at nadir, which is quite high, and he
was close to being intubated, similar to the data reported in the
medical literature. In the above study, the patients with AMAN had
worse outcome at the 3- and 6-month follow-up than the patients
with AIDP (P=0.001, P=0.000 respectively) (21), unlike our patient, who presented a
favorable outcome after TPE.
Another UK study suggests that the pattern of axonal
injury is associated with poorer prognosis of recovery at 3 and 6
months (44). According to Zhang
et al, an HFGS score at onset of ≥3 and the presence of
dysautonomia are predictors of poor outcome at 6 months (21).
Generally, patients with AMAN are thought to have
poor prognosis compared with patients with AIDP (5), but some patients with AMAN often show
rapid recovery, and Hiraga et al described these patterns of
evolution in a study that included patients with GBS who received
immune treatments (3). Out of a
total of 35 patients with the AMAN phenotype of GBS who were
analyzed for neurological evolution, 19 had a 1 point improvement
on the HFGS at 4 weeks; in the other patients, the 1-point
improvement was delayed by >1 month (3). Low CMAP amplitudes or absent motor
responses on NCS are predictive criteria of poor outcome in adults
(43,45), and our patient presented these
criteria.
The explanation for patients with AMAN who reach
their nadir quickly and recover as quickly as patients with AIDP is
that the pathological process does not destroy the axon, but
produces a conduction block that is reversible without axonal
degeneration in the case of rapid elimination of the autoantibodies
directed against the sodium channel, or the degeneration that
occurs is located very distally (12,16).
A meta-analysis published in 2012 that included 649
patients enrolled in six trials showed that TPE decreased the need
for ventilation support compared with controls (RR: 0.53) and
reduced the time needed to regain the ability to walk (30 vs. 44
days) (29,46).
The combination between the HFGS and MRC scores
assessed at 1 and 2 weeks are good predictors and are correlated
with the outcome at 6 months (29,47).
Our patient had very good evolution, with improvement of 2 points
on the HFGS within 15 days, significantly higher compared to
previously reported data.
Autonomic impairment is common in GBS, especially in
cases where respiratory dysfunction is present, as happened with
our patient (2). Urinary
dysfunction is one manifestation and has been reported in 50% of
patients with axonal GBS, more frequently than in classic GBS
(21%), but the underlying mechanism is not well known and is
believed to be either bladder areflexia or a non-relaxing urethral
sphincter (43,48,49).
The CSF protein level is generally elevated, with
albuminocytological dissociation as a result of increased
blood-brain barrier (BBB) permeability if the protein level is
measured 2 or 3 weeks after onset, but in the first week of the
illness, it may be normal, as it was in our patient (43). Anti-ganglioside antibodies are
identified in many patients with GBS, but tests are expensive and
not always available (2).
We believe that our case presented rapid evolution
towards recovery with lack of neurological deficits 1 month after
discharge despite the presence of factors correlated with negative
evolution (short interval between symptom onset and admission,
presence of axonal form, low CMAP amplitude) due to the application
as the first-line treatment of plasmapheresis with the elimination
of autoantibodies, which prevented axonal degeneration, and to the
very short time elapsed between symptom onset and the first session
of plasmapheresis. The existence of good recovery potential,
evidenced by our patient's spectacular evolution with improvement,
suggests that axonal degeneration is not always the basis of the
changes found by NCS. It is possible that there is antibody-induced
blockade at the level of the Ranvier nodes in the motor fibers, and
in the case of rapid removal by plasmapheresis, axonal degeneration
does not recur, and this may explain our patient's favorable
evolution.
IVIg and TPE appear to have approximately equal
efficacy for treating GBS, but most studies have predominantly
included the AIDP subtype (15,50,51).
The therapeutic response to IVIg is good in the case of AIDP, but
is unsatisfactory in patients with the axonal forms (16,52);
Buzzigoli et al suggested that patients with GBS with axonal
involvement could have a better response to TPE, which should be
considered early (53), and Dada
and Kaplan also suggest that TPE may be superior to IVIg for
treating patients with severe forms of GBS and axonal involvement
(54). TPE is a therapeutic option
in the case of the AMAN phenotypic variant of GBS, with even higher
efficacy, when it is initiated earlier. Due to the increased
percentage of patients that become disabled, larger prospective
trials that include patients with the axonal form of GBS treated
with TPE and IVIg are needed.
Other favorable data for the use of TPE are
represented by a study conducted in Southern India and published in
2014, which compared the two treatments and did not show a
significant difference between the two groups in terms of
improvement rate, but found that IVIg costs more (USD 4250-5300)
compared to plasmapheresis (USD 2600-4100) (55). These data are similar to that
reported by Western European countries (56-58);
therefore, plasmapheresis could be the preferred method for
treating GBS in low-socioeconomic countries.
The main aim of the present article is to report the
efficacy of TPE in a severe and rapidly progressive AMAN subtype of
GBS. Another recently published case report showed the beneficial
effect of TPE after IVIg failed to improve the neurological
condition of a child diagnosed with the AMAN subtype of GBS
(59). Cases such as this may be
included in retrospective studies on the efficacy of different
treatments for the axonal forms of GBS.
The particularity of the presented case consists in
a good clinical resolution of the symptoms using TPE in the
presence of a severe disease with rapid onset and evolutionary
potential with severe nerve conduction impairment and respiratory
dysfunction, in a young patient with no associated
comorbidities.
4. Conclusions
The good evolution of our patient suggests that TPE
could be considered first choice treatment for the AMAN subtype of
GBS.
Close monitoring makes it easy to detect possible
complications, and prompt intervention makes it easy to treat them,
proving that, in these conditions, TPE is a relatively safe and
well-tolerated procedure.
The possibility of performing TPE in the neurology
clinic by the peripheral venous approach makes it possible to be
performed quickly from the moment of therapeutic indication, saving
precious time and relieving colleagues in intensive care units of
additional work.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Data and materials are available from the
corresponding author on reasonable request.
Authors' contributions
AS and GȘ performed the literature research and
drafted the manuscript. ZB, SA and OM analyzed and interpreted the
patient data regarding the neurological disease and treatment. AB
provided critical review for all aspects of the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable. Ethical approval was not required as
the patient was not included in a clinical study and did not
receive experimental treatment.
Patient consent for publication
Informed consent forms were signed by the patient
who agreed to the use of his medical records for publication.
Competing interests
The authors state that they have no competing
interests.
References
|
1
|
Afifi AK: The landry-guillain-barré strohl
syndrome 1859 to 1992 a historical perspective. J Family Community
Med. 1:30–34. 1994.PubMed/NCBI
|
|
2
|
Dash S, Pai AR, Kamath U and Rao P:
Pathophysiology and diagnosis of guillain-barré syndrome-challenges
and needs. Int J Neurosci. 125:235–240. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hiraga A, Mori M, Ogawara K, Hattori T and
Kuwabara S: Differences in patterns of progression in demyelinating
and axonal guillain-barre syndromes. Neurology. 61:471–474.
2003.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Padmanabhan A, Connelly-Smith L, Aqui N,
Balogun RA, Klingel R, Meyer E, Pham HP, Schneiderman J, Witt V, Wu
Y, et al: Guidelines on the use of therapeutic apheresis in
clinical practice-evidence-based approach from the writing
committee of the american society for apheresis: The eighth special
issue. J Clin Apher. 34:171–354. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Stoian A, Motataianu A, Bajko Z and Balasa
A: Guillain-Barré and acute transverse myelitis overlap syndrome
following obstetric surgery. J Crit Care Med (Targu Mures).
6:74–79. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Omejec G and Podnar S: Retrospective
analysis of slovenian patients with guillain-barré syndrome. J
Peripher Nerv Syst. 17:217–219. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kuwabara S: Axonal guillain-barré syndrome
is underestimated in Europe? J Neurol Neurosurg Psychiatry.
81(1063)2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kuwabara S and Yuki N: Axonal
guillain-barré syndrome: Concepts and controversies. Lancet Neurol.
12:1180–1188. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yuki N, Taki T, Inagaki F, Kasama T,
Takahashi M, Saito K, Handa S and Miyatake T: A bacterium
lipopolysaccharide that elicits Guillain-Barré syndrome has a GM1
ganglioside-like structure. J Exp Med. 178:1771–1775.
1993.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ho TW, Willison HJ, Nachamkin I, Li CY,
Veitch J, Ung H, Wang GR, Liu RC, Cornblath DR, Asbury AK, et al:
Anti-GD1a antibody is associated with axonal but not demyelinating
forms of guillain-barré syndrome. Ann Neurol. 45:168–173.
1999.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ang CW, Jacobs BC and Laman JD: The
guillain-barré syndrome: A true case of molecular mimicry. Trends
Immunol. 25:61–66. 2004.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kuwabara S, Bostock H, Ogawara K, Sung JY,
Kanai K, Mori M, Hattori T and Burke D: The refractory period of
transmission is impaired in axonal guillain-barré sindromes. Muscle
Nerve. 28:683–689. 2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hafer-Macko C, Hsieh ST, Li CY, Ho TW,
Sheikh K, Cornblath DR, McKhann GM, Asbury AK and Griffin JW: Acute
motor axonal neuropathy: An antibody-mediated attack on axolemma.
Ann Neurol. 40:635–644. 1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kalita J, Misra UK and Das M:
Neurophysiological criteria in the diagnosis of different clinical
types of guillain-barre syndrome. J Neurol Neurosurg Psychiatry.
79:289–293. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
van den Berg B, Walgaard C, Drenthen J,
Fokke C, Jacobs BC and van Doorn PA: Guillain-Barré syndrome:
Pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol.
10:469–482. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hughes RA and Cornblath DR: Guillain-Barré
syndrome. Lancet. 366:1653–1666. 2005.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kuwabara S, Asahina M, Koga M, Mori M,
Yuki N and Hattori T: Two patterns of clinical recovery in
guillain-barré syndrome with IgG anti-GM1 antibody. Neurology.
51:1656–1660. 1998.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Stoian A, Moțățăianu A, Bărcuțean L, Maier
S, Bazko Z, Voidăzan S, Fărcaș A and Bălașa R: Understandig the
mechanism of action of intravenous immunoglobulins: A ten years
experience in treating guillain-barré syndrome. Farmacia.
68:426–435. 2020.
|
|
19
|
Kleyweg RP, van der Meché FG and Schmitz
PI: Interobserver agreement in the assessment of muscle strength
and functional abilities in guillain-barré syndrome. Muscle Nerve.
14:1103–1109. 1991.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hughes RA, Newsom-Davis JM, Perkin GD and
Pierce JM: Controlled trial prednisolone in acute polyneuropathy.
Lancet. 2:750–753. 1978.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhang G, Li Q, Zhang R, Wei X, Wang J and
Qin X: Subtypes and prognosis of guillain-barré syndrome in
Southwest China. PLoS One. 10(e0133520)2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ho TW, Mishu B, Li CY, Gao CY, Cornblath
DR, Griffin JW, Asbury AK, Blaser MJ and McKhann GM: Guillain-Barre
syndrome in northern China Relationship to Campylobacter
jejuni infection and anti-glycolipid antibodies. Brain.
118:597–605. 1995.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ye Y, Wang K, Deng F and Xing Y:
Electrophysiological subtypes and prognosis of guillain-barré
syndrome in northeastern China. Muscle Nerve. 47:68–71.
2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Estrade S, Guiomard C, Fabry V, Baudou E,
Cances C, Chaix Y, Cintas P, Meyer P and Cheuret E: Prognostic
factors for the sequelae and severity of guillain-barré syndrome in
children. Muscle Nerve. 60:716–723. 2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Hadden RD, Cornblath DR, Hughes RA,
Zielasek J, Hartung HP, Toyka KV and Swan AV: The plasma
exchange/sandoglobulin guillain-barré syndrome trial group.
electrophysiological classification of guillain-barré syndrome:
Clinical associations and outcome. Ann Neurol. 44:780–788.
1998.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Winer JB, Hughes RA, Anderson MJ, Jones
DM, Kangro H and Watkins RP: A prospective study of acute
idiopathic neuropathy. II. Antecedent events. J Neurol Neurosurg
Psychiatry. 51:613–618. 1998.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hemachudha T, Griffin DE, Chen WW and
Johnson RT: Immunologic studies of rabies vaccination-induced GBS.
Neurology. 38:375–378. 1998.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Lasky T, Terracciano GJ, Magder L, Koski
CL, Ballesteros M, Nash D, Clark S, Haber P, Stolley PD,
Schonberger LB and Chen RT: The guillain-barre´ syndrome and the
1992-1993 and 1993-1994 influenza vaccines. N Engl J Med.
339:1797–1802. 1998.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kozanoglu I, Yerdelen D, Buyukkurt N,
Yeral M, Boga C and Ozdogu H: A retrospective study on patients
with guillain-barré syndrome treated with therapeutic plasma
exchange and other treatment options-a centre's experience. Eur
Neurological Rev. 10:81–84. 2015.
|
|
30
|
Huy PP and Schwartz J: Therapeutic plasma
exchange in guillain-barré syndrome and chronic inflammatory
demyelinating polyradiculoneuropathy. Presse Med. 48:338–346.
2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Chevret S, Hughes RA and Annane D: Plasma
exchange for guillain-barré syndrome. Cochrane Database Syst Rev.
2(CD00179)2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
McKhann GM, Griffin JW, Cornblath DR,
Mellits ED, Fisher RS and Quaskey SA: Plasmapheresis and
guillain-barré syndrome: Analysis of prognostic factors and the
effect of plasmapheresis. Ann Neurol. 23:347–353. 1998.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Derksen RH, Schuurman HJ, Meyling FH,
Struyvenberg A and Kater L: The efficacy of plasma exchange in the
removal of plasma components. J Lab Clin Med. 104:346–354.
1984.PubMed/NCBI
|
|
34
|
Appropriate number of plasma exchanges in
Guillain-Barré syndrome. The French Cooperative Group on plasma
exchange in Guillain-Barré syndrome. Appropriate number of plasma
exchanges in Guillain-Barré syndrome. Ann Neurol. 41:298–306.
1997.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Espérou H, Jars-Guincestre MC, Bolgert F,
Raphaël JC and Durand-Zaleski I: French cooperative group on plasma
exchange in guillain-barré syndrome. Cost-effectiveness of plasma
exchange therapy for the treatment of guillain-barré syndrome.
Intensive Care Med. 26:1094–1100. 2000.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Shemin D, Briggs D and Greenan M:
Complications of therapeutic plasma exchange: A prospective study
of 1,727 procedures. J Clin Apher. 22:270–276. 2007.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Dhanya NB, Rai R and Srinivas CR:
Histamine 2 blocker potentiates the effects of histamine 1 blocker
in suppressing histamine-induced wheal. Indian J Dermatol Venereol
Leprol. 74:475–477. 2008.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ogawara K, Kuwabara S, Mori M, Hattori T,
Koga M and Yuki N: Axonal guillain-barré syndrome: Relation to
anti-ganglioside antibodies and Campylobacter jejuni
infection in Japan. Ann Neurol. 48:624–631. 2000.PubMed/NCBI
|
|
39
|
Paradiso G, Tripoli J, Galicchio S and
Fejerman N: Epidemiological, clinical, and electrodiagnostic
findings in childhood guillain-barré syndrome: A reappraisal. Ann
Neurol. 46:701–717. 1999.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Chareyre J, Hully M, Simonnet H, Musset L,
Barnerias C, Kossorotoff M, Quijano-Roy S, Desguerre I and Gitiaux
C: Acute axonal neuropathy subtype of guillain barré syndrome in a
French pediatric series: Adequate follow-up may require repetitive
electrophysiological studies. Eur J Paediatr Neurol. 21:891–897.
2017.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Tekgul H, Serdaroglu G and Tutuncuoglu S:
Outcome of axonal and demyelinating forms of guillain-barré
syndrome in children. Pediatr Neurol. 28:295–299. 2003.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Zhang Y, Zhao Y and Wang Y: Prognostic
factors of guillain-barré syndrome: A 111-case retrospective
review. Chin Neurosurg J. 14:1–9. 2018.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Akbayram S, Doğan M, Akgün C, Peker E,
Sayιn R, Aktar F, Bektaş MS and Caksen H: Clinical features and
prognosis with guillain-barré syndrome. Ann Indian Acad Neurol.
14:98–102. 2011.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Gonzalez-Suarez I, Sanz-Gallego I,
Rodriguez de Rivera FJ and Arpa J: Guillain-Barre syndrome: Natural
history and prognostic factors: A retrospective review of 106
cases. BMC Neurol. 13(95)2013.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Bradshaw DY and Jones HR Jr:
Guillain-Barré syndrome in children: Clinical course,
electrodiagnosis, and prognosis. Muscle Nerve. 15:500–506.
1992.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Raphaël JC, Chevret S, Hughes RA and
Annane D: Plasma exchange for guillain-barré syndrome. Cochrane
Database Syst Rev. 7(CD001798)2012.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Walgaard C, Lingsma HF, Ruts L, van Doorn
PA, Steyerberg EW and Jacobs BC: Early recognition of poor
prognosis in guillain-barre syndrome. Neurology. 76:968–975.
2011.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Lee JH, Sung IY and Rew IS: Clinical
presentation and prognosis of childhood guillain-barré syndrome. J
Paediatr Child Health. 44:449–454. 2008.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Sakakibara R, Hattori T, Kuwabara S,
Yamanishi T and Yasuda K: Micturitional disturbance in patients
with guillain-barre syndrome. J Neurol Neurosurg Psychiatr.
63:649–653. 1997.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Sharshar T, Chevret S, Bourdain F and
Raphaël JC: French cooperative group on plasma exchange in
guillain-barré syndrome. Early predictors of mechanical ventilation
in guillain-barré syndrome. Crit Care Med. 31:278–283.
2003.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Van Doorn PA, Ruts L and Jacobs BC:
Clinical features, pathogenesis, and treatment of guillain-barré
syndrome. Lancet Neurol. 7:939–950. 2008.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Van Doorn PA, Kuitwaard K, Walgaard C, van
Koningsveld R, Ruts L and Jacobs BC: IVIG treatment and prognosis
in guillain-barré syndrome. J Clin Immunol. 30 (Suppl):S74–S78.
2010.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Buzzigoli SB, Genovesi M, Lambelet P, Logi
C, Raffaelli S and Cattano D: Plasmapheresis treatment in
guillain-barré syndrome: Potential benefit over intravenous
immunoglobulin. Anaesth Intensive Care. 38:387–389. 2010.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Dada MA and Kaplan AA: Plasmapheresis
treatment in guillain-barré syndrome: Potential benefit over IVIg
in patients with axonal involvement. Ther Apher Dial. 8:409–412.
2004.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Chaudhuri JR, Alladi S, Mridula KR, Boddu
DB, Rao MV, Hemanth C, Dhanalaxmi V, Reddy JM, Rao SM, Balaraju B,
et al: Clinical outcome of Guillain-Barré syndrome with various
treatment methods and cost effectiveness: A study from tertiary
care center in South India: Yashoda GBS Registry. Neurol Asia.
19:263–270. 2014.
|
|
56
|
Nagpal S, Benstead T, Shumak K, Rock G,
Brown M and Anderson DR: Treatment of guillain-barré syndrome: A
cost-effectiveness analysis. J Clin Apher. 14:107–113.
1999.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Winters JL, Brown D, Hazard E, Chainani A
and Andrzejewski C Jr: Cost-Minimization analysis of the direct
costs of TPE and IVIg in the treatment of guillain-barré syndrome.
BMC Health Serv Res. 11(101)2011.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Balasa R: Therapeutic plasma exchange: An
indispensable therapy for severe neurological condition. J Crit
Care Med (Targu Mures). 6:89–90. 2020.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Al Hamdani S, Aljanabi FY, Abdulrasool MI
and Salman AH: Child with guillain-barré syndrome responding to
plasmapheresis: A case report. Case Rep Acute Med. 3:4–11.
2020.PubMed/NCBI View Article : Google Scholar
|