Introduction
Currently, laser-assisted in situ
keratomileusis (LASIK) is the default choice for refractive
surgical procedures, as it can address a wide spectrum of high and
complex ametropias (1-5).
There are numerous previous reports of hyperopic LASIK showing
various safety, efficiency and predictability percentages (6-32).
The new femtosecond laser technology to perform LASIK flaps avoids
many complications of the mechanical microkeratome (free caps,
incomplete, irregular or displaced flaps), being presently
preferred by many surgeons (1,2,33). In
this study, we evaluated the safety, efficacy, predictability and
accuracy of the refractive results of Femtosecond-LASIK
(Femto-LASIK) procedure using the
VisuMax®-MEL® 80 platform for hyperopia with
or without astigmatism.
Patients and methods
Data collection
We performed a retrospective, noncomparative
consecutive case series study on eyes with hyperopia and hyperopic
astigmatism that underwent Femto-LASIK surgery. Patients were
operated on by the same refractive surgeon (HTS) at the Europe
Eye-Metropolitan Hospital in Bucharest, Romania between June 2011
and June 2017. All surgeries were performed using the same
femtosecond laser-excimer laser platform
VisuMax®-MEL® 80 (Carl Zeiss Meditec).
Inclusion and exclusion criteria
The inclusion criteria for the surgery were:
Patients of age ≥22 years, no refractive change for at least 2
years before surgery, stable peripheral retina (normal or already
treated by laser photocoagulation if at-risk peripheral lesions
were present), central endothelial density ≥2,000
cells/mm2 and good compliance (1,3,33,34).
The refractive inclusion criteria were: Manifest
hyperopia up to 6.00 diopter (D) with or without astigmatism up to
5.00 D and spherical equivalent +6.00 D at most. Patients outside
these limits were referred for intraocular surgery, either phakic
intraocular lenses or refractive lens exchange, according to
patient age and ocular biometric considerations (35-37).
We considered the following exclusion criteria for
surgery: Eyes with corneal inadequate parameters (evidence or
suspect of ectasia, thinnest point on pachymetry ≤500 µm, estimated
postoperative steep keratometry >50 D, insufficient corneal
thickness for laser ablation-estimated residual thickness of the
stromal bed after treatment ≤300 µm) (1,3,33),
eyes with anterior segment pathology (eg. severe dry eye syndrome,
ocular inflammation or infection) (1,3,33),
patients with eye-related conditions which might interfere with
visual acuity (eg. cataract, congenital or acquired macular
pathology, optic nerve pathology or retinal vascular pathology)
(1,38-44),
patients with previous ocular trauma or any previous ocular
procedures (eg. scleral, vitreo-retinal surgery, glaucoma laser
procedures or glaucoma surgery) (1,45-47)
and patients taking medication with potential ocular side effects
(eg. isotretinoin, amiodarone) (1,3,33).
Patients with very deep-set eyes were also excluded,
as well as patients with narrow palpebral fissures or periocular
tumors (1,48-50),
as normal orbital anatomy is important in order to permit the
proper suction cup positioning.
We also excluded patients with systemic diseases
with risk of postoperative low visual acuity due to possible
vascular complications including ischemic optic neuropathy or
vascular occlusion (eg. cardiovascular diseases, severe systemic
hypertension, severe dyslipidemia) (1,51-54)
and patients with systemic diseases that could interfere with the
wound-healing process (eg. autoimmune disorders, diabetes mellitus)
(1,33,55).
Pregnancy or lactation were exclusion criteria for
the surgery (1,3,33).
Patients unable to understand the perioperative
management, patients with unreasonable expectations or patients
unable to sign the informed consent were excluded as well (1,33).
Preoperative assessment
Preoperative ocular examination included: Corrected
and uncorrected distance visual acuity, manifest, fogging and
cycloplegic refractions, keratometry, ultrasound corneal
pachymetry, corneal topography and tomography (Scheimpflug),
non-contact tonometry, pupillometry, white-to-white corneal
diameter, quantification of corneal endothelial cell density,
slit-lamp examination of the anterior segment and retina assessment
with pharmacological mydriasis.
Patients were asked not to wear soft contact lenses
2 weeks prior to preoperative investigations and then 2 weeks prior
to surgery.
All patients signed an informed written consent form
in accordance with the Declaration of Helsinki after being fully
informed about the benefits and risks of the procedure. The study
was approved by the Ethics Committee of ‘Carol Davila’ University
of Medicine and Pharmacy of Bucharest, Romania (no.
16-02-06-2011).
Surgical technique
All surgeries were performed by the same refractive
surgeon (HTS), with the same femtosecond laser-excimer laser
platform (VisuMax®-MEL® 80; Carl Zeiss
Meditec), using the same protocol and technique.
Surgical steps included the following: Topical
anesthesia, sterilization of the eyelids with 10% povidone-iodine
solution, draping of the eyelids, positioning of the eye to be
treated under the femtosecond laser surgical microscope, docking of
the eye and proper suction, femtosecond laser assisted cutting of
the corneal flap, repositioning of the eye under the excimer laser
surgical microscope, lifting the flap, drying the corneal bed,
excimer laser ablation, lavage of the debris with saline solution,
repositioning of the flap, bandage contact lens application and
instillation of topical antibiotic and artificial tears.
The flap position, the flap regularity and the
interface clarity were examined before patient discharge.
Postoperative care
Postoperative treatment consisted of topical eye
drops: Antibiotic, steroid and non-steroid anti-inflammatory and
artificial tears. The bandage contact lens was removed on the first
day of postoperative visit.
The follow-up visits were carried out at 1, 3, 6 and
12 months. For each examination, a slit-lamp examination of the
anterior segment and several investigations were performed which
included: Manifest refraction, uncorrected distance visual acuity,
corneal topography and tomography (Scheimpflug) and non-contact
tonometry. Corrected distance visual acuity and cycloplegic
refraction were performed for the eyes in which a residual
refraction was determined or the visual acuity was uncorrelated
with the manifest refraction.
Data analysis and statistics
Patient data were centralized into an
Excel® (ver.14.0, Microsoft Corp.) database after
being collected on case forms. Statistical analysis was performed
using Statistical Package for the Social Sciences (SPSS) software
(ver. 20, IBM® SPSS® Statistics; IBM Corp.).
Normality of continuous variables distribution was checked by the
Shapiro-Wilk test, the statistically significance being set at a
P-value <0.05. Preoperative and postoperative refractive
data are presented as mean ± standard deviation and range.
Refractive outcome analysis was performed according
to the Standard Graphs for Reporting Refractive Surgery (56,57).
Thus, we compared the preoperative data with the 1-, 3-, 6- and
12-month postoperative results and we analyzed the safety, the
efficacy, the predictability, the accuracy and the stability of the
Femto-LASIK procedure.
Results
Patient demographics and operative
data
A total of 593 eyes (290 right eyes and 303 left
eyes) from 373 patients (294 males and 79 females) were available
for evaluation 12 months after laser surgery and were reviewed for
statistical analysis in our retrospective interventional
consecutive case series study. The mean patient age at the time of
surgery was 33.20±8.098 years (range, 22-49 years). A total of 224
patients (448 eyes) had bilateral Femto-LASIK, while 153 patients
were anisometropic cases, being operated in one single eye. A total
of 163 eyes (27.49%) were amblyopic, having a visual acuity between
20/60 and 20/30. The preoperative manifest and cycloplegic
refraction data are presented in Table
I.
 | Table IPreoperative manifest and cycloplegic
refraction data. |
Table I
Preoperative manifest and cycloplegic
refraction data.
| Parameter | Diopters (mean ±
SD, range) |
|---|
| Manifest
sphere | +3.9532±1.5282,
+1.25 to +6.00 |
| Manifest
cylinder | +2.6316±1.2208,
+0.50 to +5.00 |
| Manifest SEQ | +4.0780±1.5723,
+1.50 to +6.00 |
| Cycloplegic
sphere | +5.7198±1.4351,
+3.25 to +6.75 |
| Cycloplegic
cylinder | +3.1320±1.4829,
+0.50 to +5.00 |
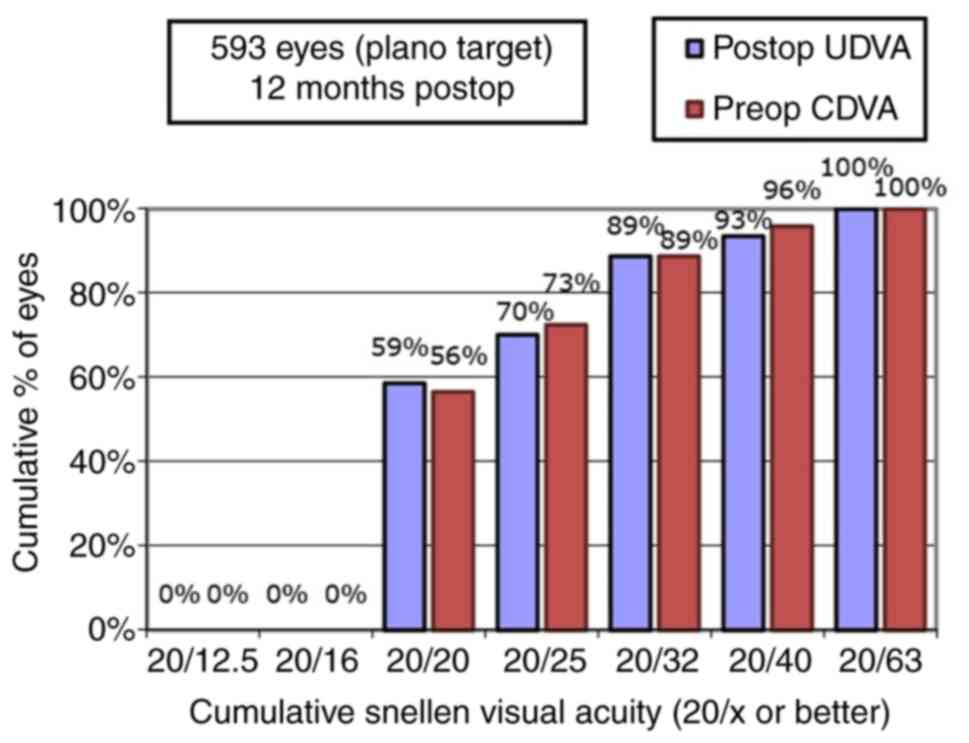
Visual and refractive results
The efficacy was defined as the ratio of the
uncorrected distance visual acuity (UDVA) at the end of the
follow-up period (12 months) and the preoperative corrected visual
acuity (CDVA). Fig. 1 shows that
all eyes reached a UDVA of 20/63 or better 12 months after
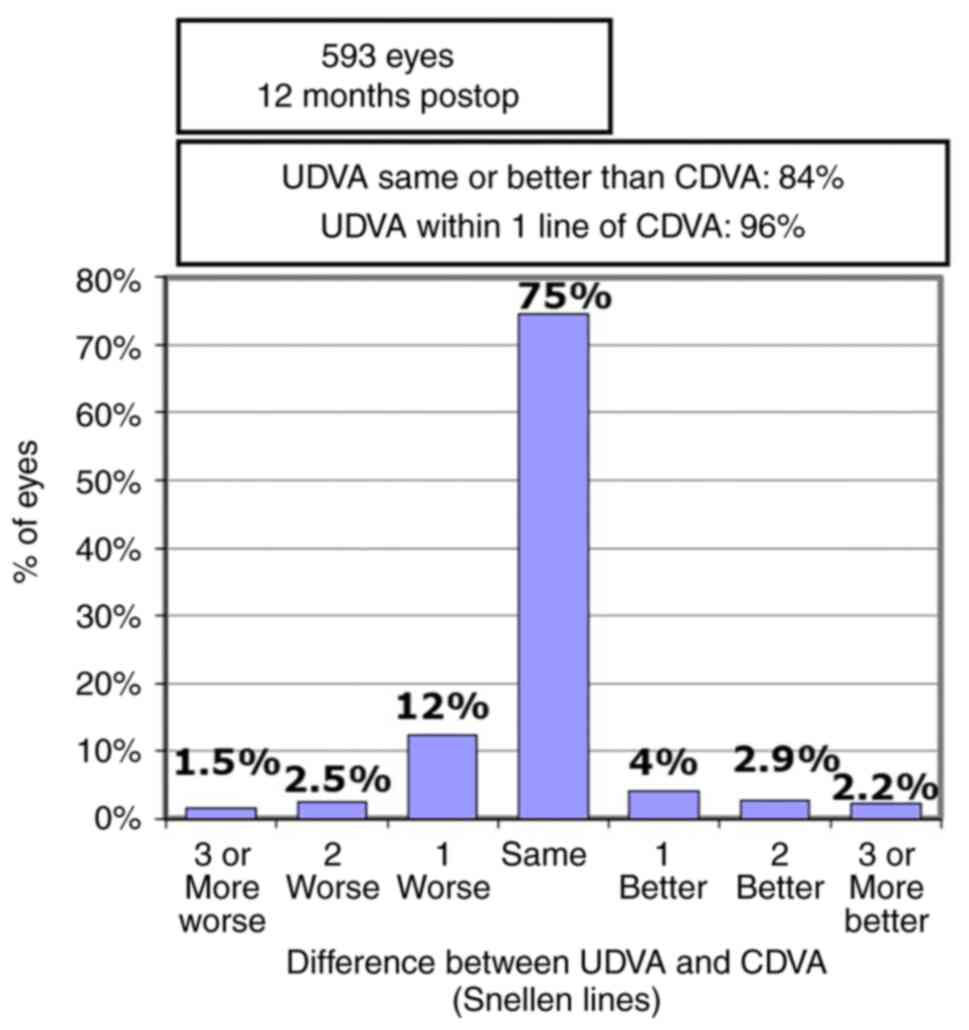
Femto-LASIK surgery. As shown in Fig.
2, for 84.1% of the eyes, the postoperative 12-month UDVA was
the same or better than the preoperative CDVA.
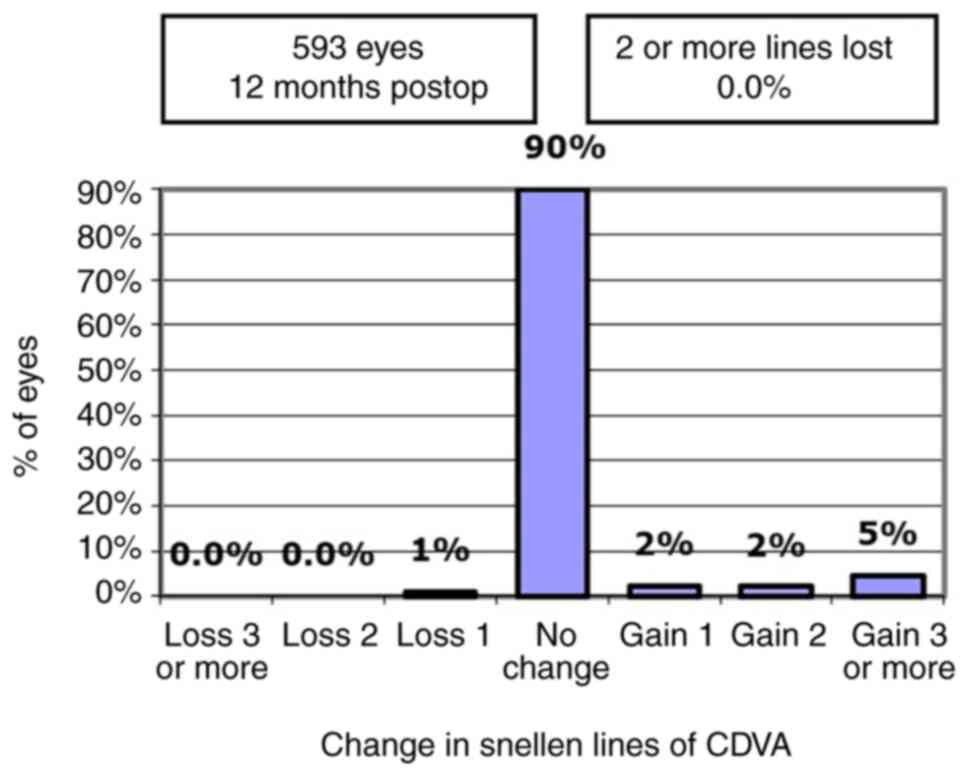
Safety, defined as no loss of two or more Snellen
lines of CDVA, was excellent. Twelve months after Femto-LASIK
surgery, no eye lost 2 lines and 6 eyes (1.012%) lost one Snellen
line of CDVA (Fig. 3).
Contrariwise, we found several amblyopic eyes that gained at least
one line of visual acuity, reflecting potential benefit of the
refractive surgery, possibly explained by reduction or elimination
of optical aberrations of the hyperopic magnifying correction
lenses.
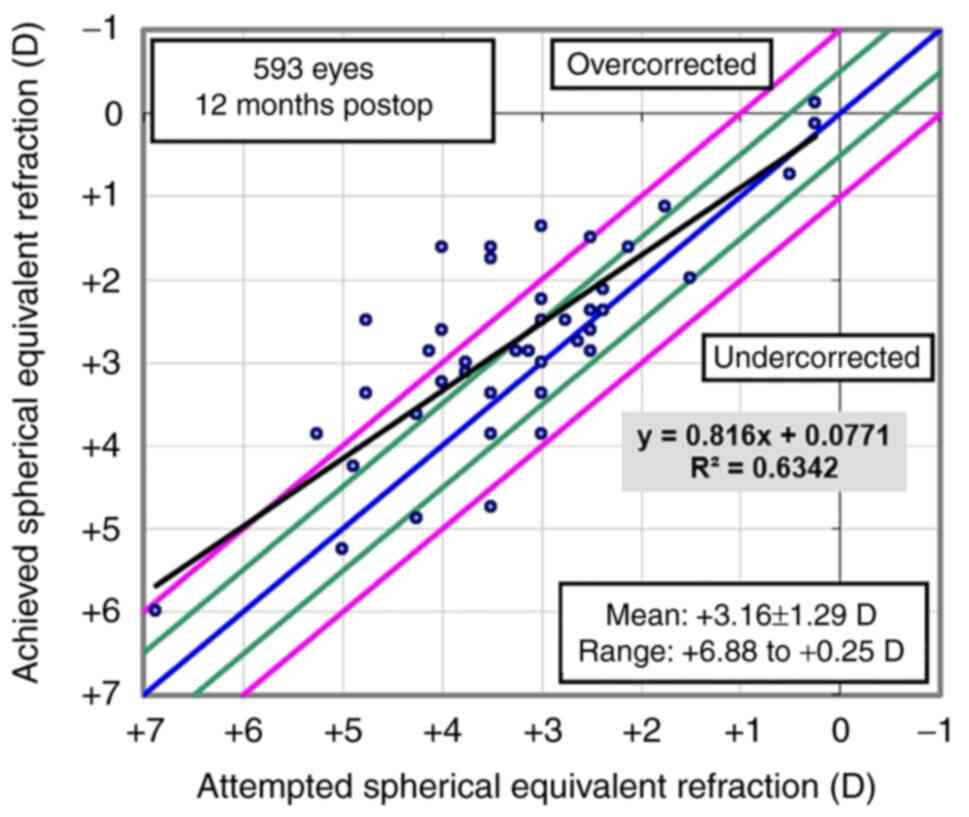
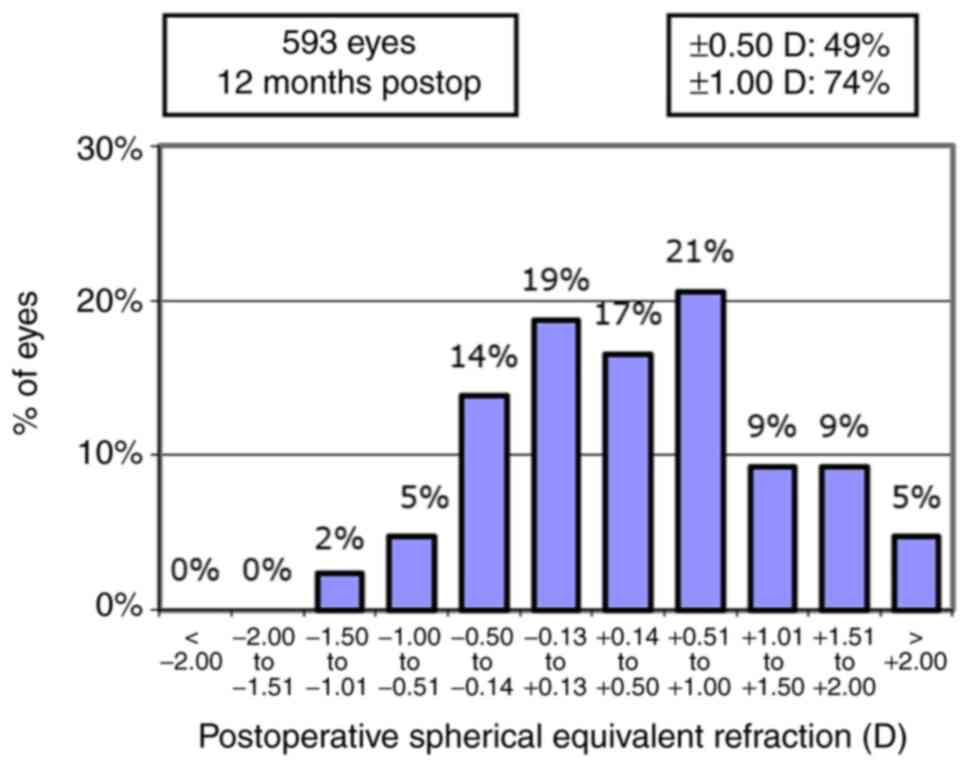
The scatterplot of the attempted spherical
equivalent refraction (SEQ) against the achieved refractive change
is shown in Fig. 4. At the
postoperative 12 months follow-up visit, the mean sphere was
+0.887±0.8746 D, the mean cylinder was +0.766±0.5797 and the mean
SEQ was +0.5042±0.8336. The accuracy of SEQ at 12 months was 49%
within ±0.50 D and respectively 74% within ±1.00 D of emmetropia
(Fig. 5). Lower predictability and
accuracy of SEQ was found for the eyes with high preoperative
refractive errors.
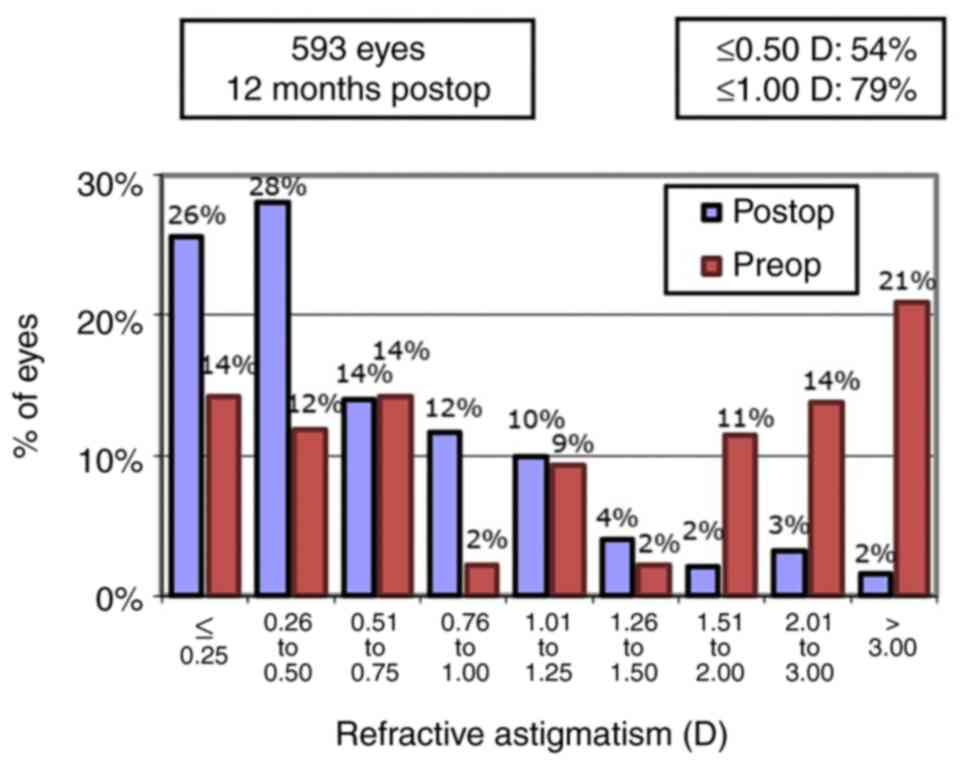
Regarding the mean refractive manifest astigmatism
at the last postoperative visit, 54 and 79% were <0.50 D and
≤1.00 D, respectively. Fig. 6 also
shows the comparison between the preoperative and the 12-month
postoperative refractive astigmatism.
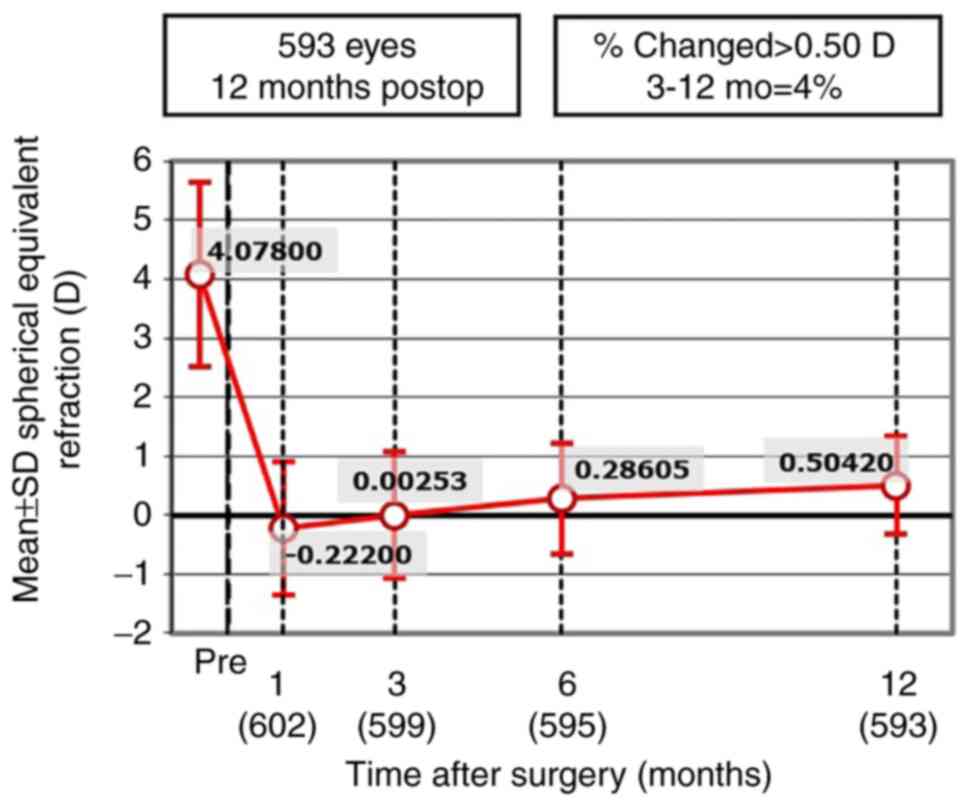
Fig. 7 shows the
excellent evolution of SEQ after the surgery and its stability in
time over the 12-month follow-up period. The postoperative
refraction data at 1, 3, 6 and 12 months postoperative are
presented in Table II. There were
no intraoperative or postoperative complications during the
follow-up period.
| Table IIPostoperative refraction data. |
Table II
Postoperative refraction data.
| | Postoperative
visit |
|---|
| | 1 month | 3 months | 6 months | 12 months |
|---|
| Parameter | Diopters (mean ±
SD, range) |
|---|
| Manifest
sphere | +0.233±1.1409,
-1.50 to +3.25 | +0.4393±1.1563,
-1.25 to +3.75 | +0.667±0.9742,
-1.00 to +2.50 | +0.887±0.8746,
-1.00 to +2.75 |
| Manifest
cylinder | +0.91±0.739, +0.00
to +3.00 | +0.8735±0.6021,
+0.25 to +2.75 | +0.7618±0.54706,
+0.00 to +2.75 | +0.766±0.5797,
+0.25 to +3.25 |
| Manifest SEQ | -0.222±1.1320,
-2.50 to +3.00 | +0.00253±1.079,
-1.50 to +3.375 | +0.28605±0.9382,
-1.25 to +2.50 | +0.5042±0.8336,
-1.00 to +3.00 |
Discussion
Laser-assisted in situ keratomileusis (LASIK)
is currently the most frequently practiced laser refractive
procedure worldwide as it can correct large diopter limits of all
types of refractive errors (1-4,6-33).
However, laser refractive surgery is challenging for eyes with
hyperopia or hyperopic astigmatism, especially when refractive
error is high (1,6-32,58).
Hyperopic correction has several difficulties.
Hyperopic patients are frequently under-corrected in regards to
glass prescriptions prior to preoperative evaluation and have
accommodation reserve of different degrees or accommodation spasm
(1,6). Therefore, the integration of manifest
and cycloplegic refractions is difficult and latent hyperopia may
lead to increasing values of manifest refraction with age (1,6).
Accurate centration of the ablation is another difficult point as
hyperopic patients have a wide angle Kappa (6). Hyperopic correction induces central
corneal flattening, which may be limited by preoperative
keratometry (6). Another issue
concerning hyperopic and astigmatic patients is the higher risk of
de-centration of ablation due to the difficulty in fixation of the
near target point during laser correction (6). Considering all the above listed
features, the predictability and the accuracy of the refractive
results in hyperopia, with or without astigmatism, are lower when
compared to myopic refractive corrections (58).
Although some excimer lasers have been approved for
corrections up to +6.0 D (1,7) and
current technology using models with wide ablation and high
correction speed has greatly improved prognosis (1,8) [large
diameter optical areas being more resistant to epithelial
hyperplasia that is responsible for real regression (1,7)],
latent hyperopia is often the reason why refractive surgeons avoid
approaching cases of hyperopia and hyperopic astigmatism or limit
the surgeries to refractive errors below +3.0 D (1,8). Laser
refractive treatment is difficult to choose because ablation of
manifest refraction in hyperopia or hyperopic astigmatism may lead
postoperatively to recurrence of a degree of hyperopia, falsely
interpreted as regression of the laser procedure (1,6,7), while
ablation of cycloplegic refraction may lead to myopic refraction in
the immediate postoperative period, causing an unsatisfactory UDVA
(1). In order to compensate in part
for the latent hyperopia, Kanellopoulos proposed a nomogram that
involves full treatment in the case of the cylinder and the
ablation of the manifest refraction sphere with an addition of
+0.25 D for the dominant eye and up to +0.75 D for the non-dominant
eye (1,9).
There have been several reports of hyperopic-LASIK
and hyperopic astigmatism-LASIK in the past, using different
excimer laser platforms and using for the flap creation either the
microkeratome or the femtosecond laser (1,6-32).
Table III shows the follow-up
periods and the refractive reports of all of these studies either
with high (1,6-23,25-29)
and lower predictability and efficacy rates for high refractive
errors (1,6,24,30).
The safety of the procedure in these reports was reported as good;
the number of eyes that lost two lines of CDVA postoperatively
being either zero (1,6,8,25,29)
or ranging between 1.09 and 4.34% (1,20,27,28,30,32).
The reports in the literature mention that the improvement of the
ametropic error allowed the gain in CDVA of one line in 44.6% of
cases (1,9) and of two lines in 3.7 to 22.8% of
cases in various studies (1,8,28).
| Table IIIPredictability of the SEQ between
±0.5 D and ±1.0 D of the intended target, in several published
reports of LASIK interventions for hyperopia or hyperopic
astigmatism (1). |
Table III
Predictability of the SEQ between
±0.5 D and ±1.0 D of the intended target, in several published
reports of LASIK interventions for hyperopia or hyperopic
astigmatism (1).
| Authors (Ref.) | Refractive error of
the treated eyes | Follow-up period
(months) | ±0.5 D of the
intended target | ±1.0 D of the
intended target |
|---|
| Zadok et al
(20) | Hyperopia (SEQ
<+3) | 6 | | 88.9% |
| Salz and Stevens
(32) | Hyperopia | 6 | 65.0% | 87.4% |
| Pineda-Fernández
et al (30) | Low hyperopia | 6 | 54.5% | |
| Zadok et al
(20) | Hyperopia (SEQ
<+5) | 6 | | 51.8% |
| Pineda-Fernández
et al (30) | Medium
hyperopia | 6 | 40.0% | |
| Kanellopoulos et
al (25) | Hyperopia (SEQ
<+3) | 12 | 92.0% | |
| Salz and Stevens
(32) | Hyperopia | 12 | 74.1% | 91.4% |
| Roesler and Kohnen
(31) | Hyperopia | 12 | | 88.0% |
| Kanellopoulos et
al (25) | Hyperopia (SEQ
<+5) | 12 | 79.0% | |
| Ditzen et al
(27) | Hyperopia | 12 | 78.0% | |
| Kanellopoulos
(9) | Hyperopia and
Hyperopic astigmatism | 6 | 77.9% | 88.9% |
| El-Naggar and
Hovaghimian (6) | Hyperopia and
Hyperopic astigmatism | 12 | 95% | 100.0% |
| Kanellopoulos et
al (25) | Hyperopia (SEQ
>+5) and Hyperopic astigmatism | 12 | 71.0% | |
| Lian et al
(28) | Hyperopia and
Hyperopic astigmatism | 12 | 61.1% | 83.3% |
| Kanellopoulos
(9) | Hyperopia and
Hyperopic astigmatism | 24 | 75.5% | 94.4% |
| Pineda-Fernández
et al (30) | Hyperopic
astigmatism (SEQ <+3) | 6 | 50.0% | |
| Pineda-Fernández
et al (30) | Hyperopic
astigmatism (SEQ <+6) | 6 | 38.8% | |
| Salz and Stevens
(32) | Hyperopic
astigmatism | 6 | 60.5% | 88.7% |
| Salz and Stevens
(32) | Hyperopic
astigmatism | 12 | 73.0% | 89.2% |
| Ditzen et al
(27) | Hyperopic
astigmatism | 12 | 42.0% | |
In the present study, we assessed the refractive
outcomes of femtosecond assisted LASIK performed for the correction
of hyperopia up to 6 D without or with astigmatism up to 5 D, with
a spherical equivalent not exceeding +6 D. The refractive target
was emmetropia in all cases. The treatment plan was chosen
corroborating the manifest, fogging and cycloplegic refraction,
considering both the accommodative reserve and patient age.
Femtosecond-LASIK using the
VisuMax®-MEL® 80 platform was demonstrated to
be a suitable option to correct selected cases of hyperopia and
hyperopic astigmatism. The postoperative results after one year
demonstrated the Femto-LASIK procedure to be safe and effective.
The predictability at 12 months was 74% within ±1 D of emmetropia.
As both the sphere and the cylinder plus values were reduced and
the need for hyperopic correction lenses was minimal, the optical
aberrations and distortion of the retinal image were smaller,
allowing us to achieve a better postoperative CDVA with at least
one line in 9% of the eyes.
The retrospective pattern of this report and the
short period of follow-up of one year are limiting factors in our
study. A future prospective study and a longer follow-up period are
necessary for a better understanding of the procedure stability and
for elaboration of nomogram ablation profiles.
Acknowledgements
Professional editing, linguistic and technical
assistance was performed by Irina Radu, Individual Service
Provider.
Funding
No funding was received.
Availability of data and materials
The data that support the findings of this study are
available from the corresponding author (HTS), upon reasonable
request.
Authors' contributions
BT contributed to the conception and design of the
study, the acquisition, analysis and interpretation of the data of
the study. She also contributed to the drafting of the work and its
critical revision for important intellectual content. HTS
contributed to the conception and design of the study, the
acquisition, analysis and interpretation of the data of the study,
contributed to the drafting of the work and its critical revision
for important intellectual content. RAP contributed to the
acquisition, analysis and interpretation of data of the study,
contributed to the drafting of the work and its critical revision
for important intellectual content. SS contributed to the
conception and design of the study, contributed to the drafting of
the work and its critical revision for important intellectual
content. CD contributed to the conception and design of the study,
contributed to the drafting of the work and its critical revision
for important intellectual content. MM contributed to the
acquisition, the analysis and interpretation of data of the study,
to the drafting of the work and its critical revision for important
intellectual content. CR contributed to the analysis and
interpretation of data of the study, to the drafting of the work
and its critical revision for important intellectual content. ACT
contributed to the analysis and interpretation of data of the
study, to the drafting of the work and its critical revision for
important intellectual content. All authors read and approved the
final version of the manuscript and agreed to be accountable for
all aspects of the study in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
All participants signed an informed consent in
accordance with the Declaration of Helsinki. The study was approved
by the Ethics Committee of ‘Carol Davila’ University of Medicine
and Pharmacy of Bucharest, Romania.
Patient consent for publication
This manuscript does not contain case details,
personal information or images that may enable an individual to be
identified.
Competing interests
The authors have no financial or proprietary
interest to declare in any device presented in this article.
References
|
1
|
Tăbăcaru B: Femtosecond Laser-Excimer
Laser Platform for Ametropias Surgery, PhD thesis (no. TD 4697).
‘Carol Davila’ University of Medicine and Pharmacy, Bucharest,
Romania, 2019.
|
|
2
|
Shah R: History and results; indications
and contraindications of SMILE compared with LASIK. Asia Pac J
Ophthalmol (Phila). 8:371–376. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Stanca HT, Munteanu M, Jianu DC, Motoc AG,
Jecan CR, Tăbăcaru B, Stanca S and Preda MA: Femtosecond-LASIK
outcomes using the VisuMax®-MEL® 80 platform
for mixed astigmatism refractive surgery. Rom J Morphol Embryol.
59:277–283. 2018.PubMed/NCBI
|
|
4
|
Tabacaru B and Stanca HT: One year
refractive outcomes of femtosecond-LASIK in mild, moderate and high
myopia. Rom J Ophthalmol. 61:23–31. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tabacaru B and Stanca HT: Scheimpflug
topographical changes after femtosecond LASIK for mixed
astigmatism-theoretical aspects and case study. Rom J Ophthalmol.
61:69–75. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
El-Naggar MT and Hovaghimian DG:
Assessment of refractive outcome of femtosecond-assisted LASIK for
hyperopia correction. Electron Physician. 9:3958–3965.
2017.PubMed/NCBI View
Article : Google Scholar
|
|
7
|
Motwani M and Pei R: Treatment of
moderate-to-high hyperopia with the WaveLight Allegretto 400 and
EX500 excimer laser systems. Clin Ophthalmol. 11:999–1007.
2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Motwani M: Topographic-guided treatment of
hyperopic corrections with a combination of higher order aberration
removal with WaveLight® Contoura and wavefront-optimized
hyperopic treatment. Clin Ophthalmol. 12:1021–1029. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kanellopoulos AJ: Topography-guided
hyperopic and hyperopic astigmatism femtosecond laser-assisted
LASIK: Long-term experience with the 400 Hz eye-Q excimer platform.
Clin Ophthalmol. 6:895–901. 2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Suarez E, Torres F and Duplessie M: LASIK
for correction of hyperopia and hyperopia with astigmatism. Int
Ophthalmol Clin. 36:65–72. 1996.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Esquenazi S: Five-year follow-up of laser
in situ keratomileusis for hyperopia using the Technolas Keracor
117C excimer laser. J Refract Surg. 20:356–363. 2004.PubMed/NCBI
|
|
12
|
Zadok D, Raifkup F, Landau D and
Frucht-Pery J: Long-term evaluation of hyperopic laser in situ
keratomileusis. J Cataract Refract Surg. 29:2181–2188.
2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Jaycock PD, O'Brart DP, Rajan MS and
Marshall J: 5-year follow-up of LASIK for hyperopia. Ophthalmology.
112:191–199. 2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Varley GA, Huang D, Rapuano CJ, Schallhorn
S, Boxer Wachler BS and Sugar A: Ophthalmic Technology Assessment
Committee Refractive Surgery Panel, Ameican Academy of
Ophthalmology. LASIK for hyperopia, hyperopic astigmatism, and
mixed astigmatism: A report by the American academy of
ophthalmology. Ophthalmology. 111:1604–1617. 2004.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Spades L, Sabetti L, D'Alessandri L and
Balestrazzi E: Photorefractive keratectomy and LASIK for the
correction of hyperopia: 2-year follow-up. J Refract Surg.
22:131–136. 2006.PubMed/NCBI
|
|
16
|
Alió J, Galal A, Ayala MJ and Artola A:
Hyperopic LASIK with esiris/schwind technology. J Refract Surg.
22:772–781. 2006.PubMed/NCBI
|
|
17
|
Antonios R, Arba Mosquera S and Awwad ST:
Hyperopic laser in situ keratomileusis: Comparison of femtosecond
laser and mechanical microkeratome flap creation. J Cataract
Refract Surg. 41:1602–1609. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Desai RU, Jain A and Manche EE: Long-term
follow-up of hyperopic laser in situ keratomileusis correction
using the Star S2 excimer laser. J Cataract Refract Surg.
34:232–237. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
el-Agha MS, Johnston EW, Bowman RW,
Cavanagh HD and McCulley JP: Excimer laser treatment of spherical
hyperopia: PRK or LASIK? Trans Am Ophthalmol Soc. 98:59–66.
2000.PubMed/NCBI
|
|
20
|
Zadok D, Maskaleris G, Montes M, Shah S,
Garcia V and Chayet A: Hyperopic laser in situ keratomileusis with
the Nidek EC-5000 excimer laser. Ophthalmology. 107:1132–1137.
2000.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Davidorf JM, Eghbali F, Onclinx T and
Maloney RK: Effect of varying the optical zone diameter on the
results of hyperopic laser in situ keratomileusis. Ophthalmology.
108:1261–1265. 2001.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Rashad KM: Laser in situ keratomileusis
for the correction of hyperopia from +1.25 to +5.00 diopters with
the Technolas Keracor 117C laser. J Refract Surg. 17:113–122.
2001.PubMed/NCBI
|
|
23
|
Llovet F, Galal A, Benitez-del-Castillo
JM, Ortega J, Martin C and Baviera J: One-year results of excimer
laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg. 35:1156–1165. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Alió JL, El Aswad A, Vega-Estrada A and
Javaloy J: Laser in situ keratomileusis for high hyperopia (>5.0
diopters) using optimized aspheric profiles: Efficacy and safety. J
Cataract Refract Surg. 39:519–527. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kanellopoulos AJ, Conway J and Pe LH:
LASIK for hyperopia with the WaveLight excimer laser. J Refract
Surg. 22:43–47. 2006.PubMed/NCBI
|
|
26
|
Gil-Cazorla R, Teus MA, de Benito-Llopis L
and Mikropoulos DG: Femtosecond laser vs. mechanical microkeratome
for hyperopic laser in situ keratomileusis. Am J Ophthalmol.
152:16–21.e2. 2011.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ditzen K, Fiedler J and Pieger S: Laser in
situ keratomileusis for hyperopia and hyperopic astigmatism using
the Meditec MEL 70 spot scanner. J Refract Surg. 18:430–434.
2002.PubMed/NCBI
|
|
28
|
Lian J, Ye W, Zhou D and Wang K: Laser in
situ keratomileusis for correction of hyperopia and hyperopic
astigmatism with the Technolas 117C. J Refract Surg. 18:435–438.
2002.PubMed/NCBI
|
|
29
|
El-Agha MS, Bowman RW, Cavanagh D and
McCulley JP: Comparison of photorefractive keratectomy and laser in
situ keratomileusis for the treatment of compound hyperopic
astigmatism. J Cataract Refract Surg. 29:900–907. 2003.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Pineda-Fernández A, Rueda L, Huang D, Nur
J and Jaramillo J: Laser in situ keratomileusis for hyperopia and
hyperopic astigmatism with the Nidek EC-5000 excimer laser. J
Refract Surg. 17:670–675. 2001.PubMed/NCBI
|
|
31
|
Roesler C and Kohnen T: Changes of
functional optical zone after LASIK for hyperopia and hyperopic
astigmatism. J Refract Surg. 34:476–481. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Salz JJ and Stevens CA: LADARVision LASIK
Hyperopia Study Group. LASIK correction of spherical hyperopia,
hyperopic astigmatism, and mixed astigmatism with the LADARVision
excimer laser system. Ophthalmology. 109:1647–1658. 2002.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Tăbăcaru B, Stanca S, Mocanu V, Zemba M,
Stanca HT and Munteanu M: Intraoperative flap-related complications
in FemtoLASIK surgeries performed with Visumax®
femtosecond laser: A ten-year Romanian experience. Exp Ther Med.
20:2529–2535. 2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Stanca TH, Tabacaru B and Celea C:
Correlations between confocal microscopy and histological aspects
of normal cornea. Rom J Ophthalmol. 59:19–23. 2015.PubMed/NCBI
|
|
35
|
Schallhorn SC, Schallhorn JM, Pelouskova
M, Venter JA, Hettinger KA, Hannan SJ and Teenan D: Refractive lens
exchange in younger and older presbyopes: Comparison of
complication rates, 3 months clinical and patient-reported
outcomes. Clin Ophthalmol. 11:1569–1581. 2017.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Mălăescu M, Stanca HT, Tăbăcaru B, Stănilă
A, Stanca S and Danielescu C: Accuracy of five intraocular lens
formulas in eyes with trifocal lens implant. Exp Ther Med.
20:2536–2543. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Alió JL, Grzybowski A and Romaniuk D:
Refractive lens exchange in modern practice: When and when not to
do it? Eye Vis (Lond). 1(10)2014.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Stanca HT, Stanca S, Tabacaru B, Boruga M
and Balta F: Bevacizumab in Wet AMD treatment: A tribute to the
thirteen years of experience from the beginning of the anti-VEGF
era in Romania. Exp Ther Med. 18:4993–5000. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Goldberg I, Jay Katz L, Mansouri K,
Pakravan M and Yazdani S: A refractive surgery candidate with optic
nerve head cupping. J Ophthalmic Vis Res. 7:248–256.
2012.PubMed/NCBI
|
|
40
|
Stanca HT, Suvac E, Munteanu M, Jianu DC,
Motoc AGM, Roşca GC and Boruga O: Giant cell arteritis with
arteritic anterior ischemic optic neuropathy. Rom J Morphol
Embryol. 58:281–285. 2017.PubMed/NCBI
|
|
41
|
Moshirfar M, D Wagner W, H Linn S, W Brown
T, L Goldberg J, T Gomez A, C Ronquillo Y and C Hoopes P: Corneal
refractive surgery in patients with history of optic neuritis. J
Ophthalmic Vis Res. 14:436–441. 2019.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Munteanu M, Rosca C and Stanca H:
Sub-inner limiting membrane hemorrhage in a patient with Terson
syndrome. Int Ophthalmol. 39:461–464. 2019.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Arevalo JF: Managing retinal detachment
after refractive surgery: With current knowledge, we cannot
determine whether prophylactic treatment is indicated in candidates
for refractive surgery. Retina Today. 2017:36–40. 2017.
|
|
44
|
Vatsa S and Sood S: Macular dystrophy in a
post LASIK patient. DJO. 30:60–62. 2020.
|
|
45
|
Stanca HT, Munteanu M, Jianu DC, Motoc
AGM, Tăbăcaru B, Stanca S, Ungureanu E, Boruga VM and Preda MA: New
perspectives in the use of laser diode transscleral
cyclophotocoagulation. A prospective single center observational
cohort study. Rom J Morphol Embryol. 59:869–872. 2018.PubMed/NCBI
|
|
46
|
Donnenfeld ED: Correcting astigmatism
after glaucoma surgery. Glaucoma Today. 2011:29–32. 2011.
|
|
47
|
Preda MA, Karancsi OL, Munteanu M and
Stanca HT: Clinical outcomes of micropulse transscleral
cyclophotocoagulation in refractory glaucoma-18 months follow-up.
Lasers Med Sci. 35:1487–1491. 2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Chang JSM, Law AKP, Ng JCM and Cheng MSY:
Femtosecond laser in situ keratomileusis flap creation in narrow
palpebral fissure eyes without suction. Case Rep Ophthalmol.
8:341–348. 2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Boruga O, Bălăşoiu AT, Giuri S, Munteanu
M, Stanca HT, Iovănescu G and Preda MA: Caruncular late-onset
junctional nevus: Apropos of an anatomo-clinical observation. Rom J
Morphol Embryol. 58:1461–1464. 2017.PubMed/NCBI
|
|
50
|
Moshirfar M, Shah TJ, Skanchy DF, Linn SH,
Kang P and Durrie DS: Comparison and analysis of FDA reported
visual outcomes of the three latest platforms for LASIK: Wavefront
guided Visx iDesign, topography guided WaveLight allegro contoura
and topography guided Nidek EC-5000 CATz. Clin Ophthalmol.
11:135–147. 2017.PubMed/NCBI View Article : Google Scholar
|
|
51
|
J Shah T, Moshirfar M and C Hoopes P:
Safety of the excimer laser in LASIK and PRK for patients with
implantable cardiac devices: Our clinical experience in the past
two decades. J Ophthalmic Vis Res. 14:530–531. 2019.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Stanca HT, Petrović Z and Munteanu M:
Transluminal Nd:YAG laser embolysis-a reasonable method to
reperfuse occluded branch retinal arteries. Vojnosanit Pregl.
71:1072–1077. 2014.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Cobo-Soriano R, Beltrán J and Baviera J:
LASIK outcomes in patients with underlying systemic
contraindications: A preliminary study. Ophthalmology.
113:1118.e1–e8. 2006.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Savoiu Balint G, Iovanescu G, Stanca H,
Popoiu CM, Boia E, Popovici RA and Bolintineanu SL: The protective
effect of HDL-cholesterol in patients with essential hypertension.
Rev Chim. 68:949–952. 2017.
|
|
55
|
Spadea L and Paroli MP: Laser refractive
surgery in diabetic patients: A review of the literature. Clin
Ophthalmol. 6:1775–1783. 2012.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Reinstein DZ, Archer TJ and Randleman JB:
JRS standard for reporting astigmatism outcomes of refractive
surgery. J Refract Surg. 30:654–659. 2014.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Waring GO III: Standard graphs for
reporting refractive surgery. J Refract Surg. 16:459–466.
2000.PubMed/NCBI
|
|
58
|
Spierer O, Mimouni M, Nemet A, Rabina G
and Kaiserman I: Hyperopic laser keratorefractive surgery: Do steep
corneas have worse outcomes? Int Ophthalmol. 40:1885–1895.
2020.PubMed/NCBI View Article : Google Scholar
|