Introduction
It is already well known that genetic thrombophilia
risk factors such as mutations in the Factor V Leiden and the
prothrombin genes have contributed to the understanding of the
environment-gene interaction in the development of thrombosis
(1). Data emerging from the
extensive studies from the past two decades identify abnormal
Factor V Leiden activity as the most common coagulation abnormality
in patients with cerebral venous thrombosis, with a prevalence of
20 to 25% (2-4).
Otogenic lateral sinus thrombosis is an intracranial, potentially
life-threatening complication frequently associated with acute and
chronic otitis media (5), but also
observed in other ear-associated pathologies such as cholesteatoma
(6). Thrombotic manifestations are
extremely heterogeneous, with the diagnosis often being made in
acute and complicated clinical circumstances.
The case of a young patient with lateral sinus
thrombosis is presented, complicated with unilateral sudden
sensorineural hearing loss (SSHL) and facial palsy, caused by
genetically-inherited thrombophilia.
Case report
A 27-year-old female was admitted, August 2018, to
the Department of Otorhinolaryngology (‘Venart’ Clinic,
Cluj-Napoca, Romania) for unilateral hearing loss in the left ear,
facial asymmetry of sudden onset, tinnitus, and dizziness
associated with progressive left hemi-cranial pain which appeared
in the 24 h preceding her admission, having increasing intensity.
Prior to admission, she presented subfebrile and febrile states,
with temperature values ranging from 37.5 to 39˚C.
Anamnesis revealed a history of recurrent left
otitis. The patient had undergone surgical treatment for left ear
cholesteatoma two years prior to the current admission. It is
important to note that the patient also had a history of two
spontaneous abortions in the first trimester of pregnancy, but
their etiology had not been thoroughly investigated at the time.
Her family history revealed the presence of three family members
(mother, maternal aunt, maternal grandfather) diagnosed with
life-threatening cerebral ischemic thrombotic vascular events.
Following physical examination at the Department of
Otorhinolaryngology, the patient was diagnosed with left peripheral
facial palsy. The otoscopic examination revealed a small
post-surgical scar in the left ear with no signs of infection and
inflammation. Audiometry revealed unilateral severe neuro-sensorial
hypoacusis in the left ear. The neurological consult described the
patient as alert and oriented with no signs of confusion or
lethargy. Kernig's and Brudzinski's signs were negative and there
were no signs of meningeal syndrome. Other than the minor facial
asymmetry, the patient exhibited no motor deficits in the upper and
lower limbs or incoordination. The fundoscopic eye exam revealed
mild papilledema (Fig. 1).
Laboratory investigations included complete blood
count, erythrocyte sedimentation rate, blood chemistry,
electrolytes, lipid profile, C-reactive protein, fibrinogen protein
C, protein S, antiphospholipid panel including lupus anticoagulant,
cardiolipin and beta-2 glycoprotein 1. Results were all within the
normal range.
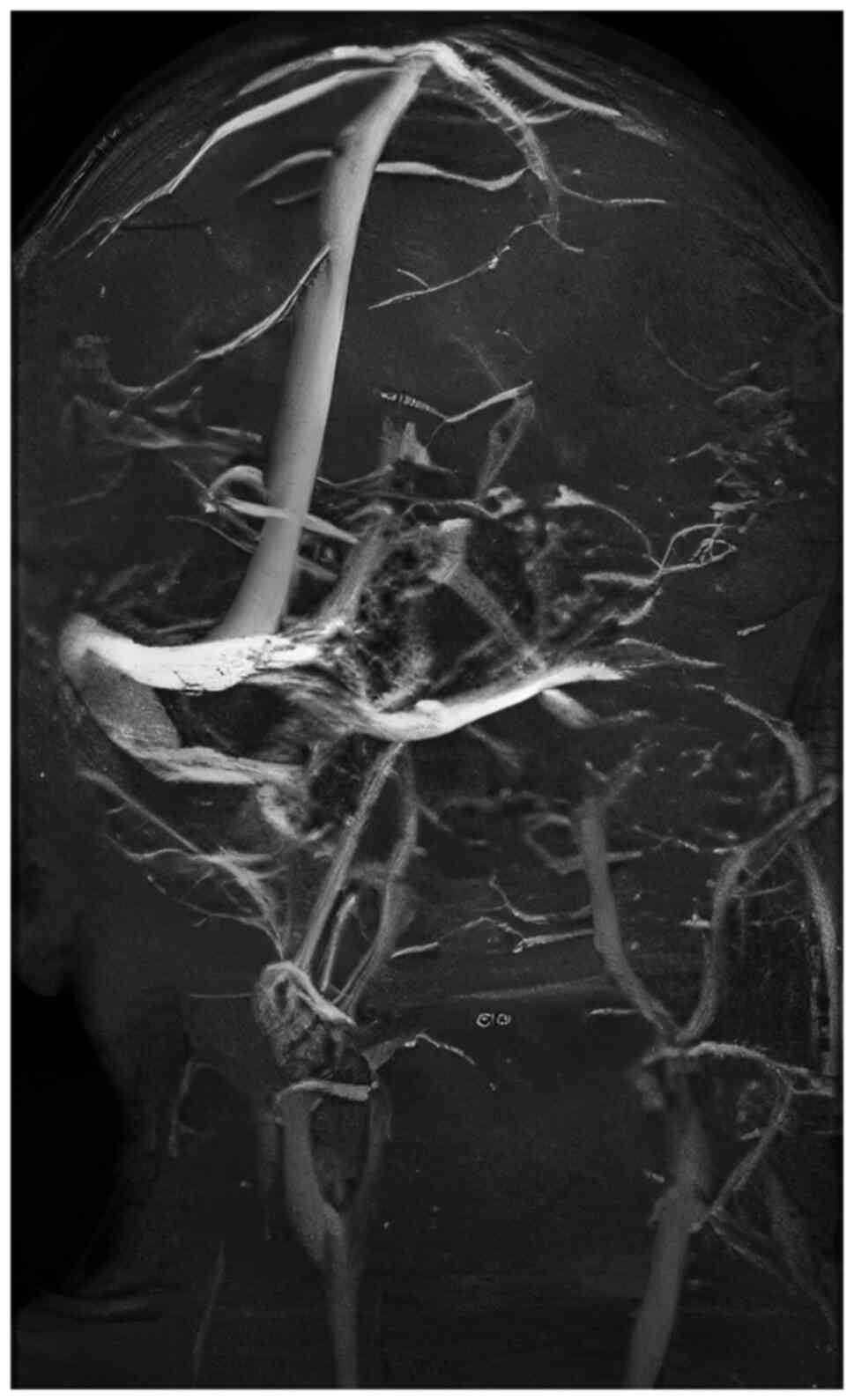
The computed tomography (CT) angiography highlighted
lateral sinus thrombosis, affecting the internal auditory meatus
and nerve.
Corroborating the clinical findings, the audiometry
and CT angiography results with the personal and family history of
thrombotic events, the hypothesis of genetic thrombophilia was
formulated, and genetic testing was recommended. The Multiplex PCR
Strip Assay, which allows the simultaneous detection of 13
different DNA targets in a single PCR reaction, followed by strip
hybridization for the further described gene variants linked to
thrombosis, (Screening trombofilico kit; Nuclear Laser Medicine
srl.) included the analysis of the following variants: Factor V
Leiden, V 4070 A>G (Hr2), prothrombin G202210A, MTHFR
C677T, MTHFR A1298C, CBS 844ins68, PAI-1
4G/5G, glycoprotein IIIa T156C (HPA01a/b), ACE-DEL/INS,
ApoE<AGT M235T, ATR-1 A1166C, fibrinogen-455 G>A and
Factor XIII Val34Leu (7).
Three mutant genotypes were identified: homozygous V
Leiden, homozygous MTHFR A1298C, and heterozygous
MTHFR C677T. These results confirmed the diagnosis of
genetic thrombophilia.
Intensive anti-inflammatory, antithrombotic and
antibiotic treatment was initiated (low-molecular weight heparin
7.5 mg daily, dexamethasone 4 mg every 8 h, and ceftriaxone 2 g
daily), and under this course of therapy, the evolution of the
patient was favourable. The hearing significantly improved, and
according to the statement of the patient, within 14 days following
admission, normal bilateral hearing had been regained. A control CT
angiography on the 7th day during therapy did not reveal any
detectable signs of cerebral vascular thrombosis.
The patient provided written informed consent for
the publication of this case report.
Discussion
SSHL is defined as rapid onset of hearing impairment
developing in one or both ears over 72 h (8). It is considered an
otorhinolaryngological emergency since it requires prompt
management to rapidly detect a potentially life-threatening
condition, although the majority of cases remain of idiopathic
nature (9,10).
SSHL is usually unilateral, with most cases being
idiopathic, and patients usually regain hearing spontaneously. In a
minority of cases, the etiology lies within the broad group of
autoimmune, vascular, metabolic, infectious, neoplastic, traumatic,
or inflammatory conditions, and in these circumstances, recovery is
usually incomplete or even unachievable (11,12).
Cerebral venous thrombosis (CVT) is extremely
heterogenous and its wide spectrum of clinical presentations
includes headache, dizziness, seizures, various focal neurological
deficits including cranial nerve involvement causing ipsilateral
facial palsy, blepharoptosis, blurry vision or diplopia, vertigo,
and hearing loss (2-4).
In our case, the patient only presented with sudden onset
unilateral hearing loss associated with headache and ipsilateral
peripheral facial palsy.
CT angiography revealed left lateral sinus
thrombosis; a complication most frequently associated with other
intracranial and extracranial pathologies, especially middle and
inner ear infections when thrombophlebitis can spread through the
emissary veins without bony erosion. Our patient had a personal
history of cholesteatoma, a cystic-like structure of keratinizing
stratified squamous epithelium that is well known to have a high
destructive and erosion potential of neighbouring structures
(13). Cholesteatoma has also been
revealed to be associated with lateral sinus thrombosis as a
complication. The auricular exam did not reveal any signs of
inflammation or infection that could suggest the diagnosis of
recurrent cholesteatoma, and thus, the episode of thrombosis was
unlikely to be a consequence of ear pathology (14). However, thorough examination is
recommended.
As far as molecular diagnosis is concerned, and
despite clear guidelines (15), in
Romania, testing for inherited thrombophilia remains deficient in
numerous departments of different specialties in the national
health system, and is not commonly suggested in clinical practice.
Although in certain branches such as obstetrics and haematology,
molecular testing for thrombophilia is frequently used (16); in others, such as
otorhinolaryngology it is completely absent.
In our case, thrombophilia was diagnosed in a young
patient with unilateral SSHL caused by lateral sinus thrombosis.
Despite the patient's personal history of two spontaneous abortions
in the first trimester of pregnancy, and despite a positive and
significant family history of thrombotic events, both representing
clear indications for thrombophilia testing according to current
guidelines (17), the diagnosis of
thrombophilia was only made following the occurrence of high-risk
cerebral thrombotic complications.
Venous thromboembolism (VTE) represents a complex
disease, the result of gene-gene and gene-environment interactions.
It is well known that the clinical manifestations of hereditary
thrombophilia are relatively heterogeneous, as far as severity and
age of onset are concerned, due to the incomplete clinical
penetrance of genotypes and to the additive and synergistic effect
of multiple genotypes (2,4).
It may appear trivial but having a family history of
VTE suggests that it is possible to find carrier relatives who may
present higher risk for this condition. When there is also a
positive history for thrombotic events in the proband, testing
becomes mandatory. Although the etiology of miscarriage often
remains idiopathic, it can be confidently affirmed that in the case
of our patient, enough evidence exists to support hereditary
thrombophilia as the cause of the two spontaneous abortions in her
history.
The mutations found in our patient affect the Factor
V Leiden and methylenetetrahydrofolate reductase. Mutations causing
defects in Factor V Leiden are linked to resistance to activated
protein C, leading to thrombophilia. Numerous studies have revealed
an association between Factor V Leiden defects and CVT development
(2,4,18).
Although multiple studies were performed and some even show a
higher prevalence of MTHFR pathological variants in patients with
CVT, there is not enough conclusive data yet to clearly correlate
the two conditions (2,19).
Current guidelines identify heterozygous and
homozygous genotypes for several variants in the Factor V Leiden
and prothrombin genes as significant etiological factors for
spontaneous miscarriage in the first trimester of pregnancy. The
American College of Obstetricians and Gynaecologists (ACOG)
underlines the importance of targeted assessment for inherited
thrombophilia in patients with personal history of VTE, with or
without obvious risk factors, and no prior thrombophilia testing,
and in patients with family history highly suggestive for inherited
thrombophilia (20). Identification
of thrombophilia risk in a patient, with or without thrombotic
manifestations, could lead to the implementation of a specific
prophylaxis which aims to lower the risk of occurrence of such
potentially life-threatening events (21).
In conclusion, since management of patients with
acute thrombotic events can be difficult in the context in which it
represents a major medical emergency, rigorous, guideline-based
identification of individuals at high risk for such manifestations
remains mandatory.
Acknowledgements
Not applicable.
Funding
Funding: Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AC and MSM contributed to genetic consulting and
counselling. ZCB and IVP interpreted the genetic testing. IVC
completed the ENT exam and OG the imaging exam. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient has provided written informed consent
for this material to appear in Experimental and Therapeutic
Medicine.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Colucci G and Tsakiris DA: Thrombophilia
screening revisited: An issue of personalized medicine. J Thromb
Thrombolysis. 49:618–629. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Di Paola JA: Cerebral venous thrombosis:
Incidence in prothrombotic states. Semin Cerebrovasc Dis Stroke.
2:102–110. 2002.
|
|
3
|
Cohen W, Castelli C, Suchon P, Bouvet S,
Aillaud MF, Brunet D, Barthet MC, Alessi MC, Trégouët DA and
Morange PE: Risk assessment of venous thrombosis in families with
known hereditary thrombophilia: The MARseilles-NImes prediction
model. J Thromb Haemost. 12:138–146. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Wu O, Robertson L, Twaddle S, Lowe G,
Clark P, Walker I, Brenkel I, Greaves M, Langhorne P, Regan L, et
al: Screening for thrombophilia in high-risk situations: A
meta-analysis and cost-effectiveness analysis. Br J Haematol.
131:80–90. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Raja K, Parida PK, Alexander A and
Surianarayanan G: Otogenic lateral sinus thrombosis: A review of
fifteen patients and changing trends in the management. Int Arch
Otorhinolaryngol. 22:208–213. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Viswanatha B and Naseeruddin K: Lateral
sinus thrombosis in otology: A review. Mediterr J Hematol Infect
Dis. 2(e2010027)2010.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Heit JA, Sobell JL, Li H and Sommer SS:
The incidence of venous thromboembolism among Factor V Leiden
carriers: A community-based cohort study. J Thromb Haemost.
3:305–311. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Stachler RJ, Chandrasekhar SS, Archer SM,
Rosenfeld RM, Schwartz SR, Barrs DM, Brown SR, Fife TD, Ford P,
Ganiats TG, et al: Clinical practice guideline: Sudden hearing
loss. Otolaryngol Head Neck. 146 (Suppl 3):S1–S35. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Rauch SD: Clinical practice. Idiopathic
sudden sensorineural hearing loss. N Engl J Med. 359:833–840.
2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ishak MN, Nik-Abdul-Ghani NM and Mohamad
I: Sudden bilateral sensorineural hearing loss secondary to
cerebral venous thrombosis. Iran J Otorhinolaryngol. 30:113–116.
2018.PubMed/NCBI
|
|
11
|
Haberkamp TJ and Tanyeri HM: Management of
idiopathic sudden sensorineural hearing loss. Am J Otol.
20:587–595. 1999.PubMed/NCBI
|
|
12
|
Kim SH, Kim SJ, Im H, Kim TH, Song JJ and
Chae SW: A trend in sudden sensorineural hearing loss: Data from a
population-based study. Audiol Neurotol. 22:311–316.
2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Heilbrun ME, Salzman KL, Glastonbury CM,
Harnsberger HR, Kennedy RJ and Shelton C: External auditory canal
cholesteatoma: Clinical and imaging spectrum. AJNR Am J
Neuroradiol. 24:751–756. 2003.PubMed/NCBI
|
|
14
|
Baráth K, Huber AM, Stämpfli P, Varga Z
and Kollias S: Neuroradiology of cholesteatomas. AJNR Am J
Neuroradiol. 32:221–229. 2011.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Stevens SM, Woller SC, Bauer KA, Kasthuri
R, Cushman M, Streiff M, Lim W and Douketis JD: Guidance for the
evaluation and treatment of hereditary and acquired thrombophilia.
J Thromb Thrombolysis. 41:154–164. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Liu N, Vigod SN, Farrugia MM, Urquia ML
and Ray JG: Venous thromboembolism after induced abortion: A
population-based, propensity-score-matched cohort study in Canada.
Lancet Haematol. 5:e279–e288. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Baglin T, Gray E, Greaves M, Hunt BJ,
Keeling D, Machin S, Mackie I, Makris M, Nokes T, Perry D, et al:
Clinical guidelines for testing for heritable thrombophilia. Br J
Haematol. 149:209–220. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Dentali F, Crowther M and Ageno W:
Thrombophilic abnormalities, oral contraceptives, and risk of
cerebral vein thrombosis: A meta-analysis. Blood. 107:2766–2773.
2006.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Habib G, Zahra S, Shahram S and Soltanpour
MS: Association study of methylenetetrahydrofolate reductase A1298C
mutation with cerebral venous thrombosis risk in an Iranian
population. Int J Appl Basic Med Res. 5:172–176. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Moll S: Thrombophilia: Clinical-practical
aspects. J Thromb Thrombolysis. 39:367–378. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Schünemann HJ, Cushman M, Burnett AE, Kahn
SR, Beyer-Westendorf J, Spencer FA, Rezende SM, Zakai NA, Bauer KA,
Dentali F, et al: American Society of Hematology 2018 guidelines
for management of venous thromboembolism: Prophylaxis for
hospitalized and nonhospitalized medical patients. Blood Adv.
2:3198–3225. 2018.PubMed/NCBI View Article : Google Scholar
|