Introduction
Sinonasal tumors are a rare pathological entity,
representing ~3% of upper respiratory tract tumors and being
characterized by marked anatomopathological diversity (1). The affected areas include the nasal
cavity and the paranasal sinuses and, in advanced cases, the tumors
may extend to involve the surrounding anatomical structures, with
no significant clinical symptoms until late in the course of the
disease (2,3). Their proximity to vital structures,
such as the optic nerves and brain, poses a challenge for surgeons
when proceeding with reconstructive treatment. The common extension
areas for this type of tumor are the cribriform plate, crista galli
and the roof of the ethmoid, the orbit and, occasionally, the
facial soft tissues (4). Performing
an extensive resection of the tumor with clear margins may result
in sizeable cranial and facial skin defects, which must then be
covered with the aid of a multidisciplinary team (5).
Currently, the improved craniofacial surgical
techniques, the advanced technology and equipment, high-quality
imaging and good interdisciplinary management may improve the
appearance of the face after surgery (6).
The main purpose of an efficient obstructive
prosthesis for a patient who has had the hard palate removed is to
create a barrier between the nasal cavity and the mouth,
maintaining good speaking and swallowing functions (4,6,7). The
defect can be repaired by using skin grafts, bone grafts, flaps and
even facial prostheses, in order to achieve satisfactory functional
and aesthetic results (4,7). The prostheses are designed and
adjusted by a maxillofacial prosthodontist, who is trained to
construct devices that replace the anatomical structures of the
head and neck, including those in the oral cavity, adapted to the
requirements of each patient (8).
Case report
We herein present the case of a 33-year-old male
patient, with no significant comorbidities, who was diagnosed with
sinonasal carcinoma treated with radical surgery in 2019 followed
by radiotherapy treatment, who required a complex surgical approach
and facial reconstruction.
This patient was admitted to the Department of
Otorhinolaryngology and Head and Neck Surgery from ‘Sf. Spiridon’
Clinical Hospital in September 2019 with complains of left
hemicrania, left nasal obstruction, left reflex otalgia, left clear
rhinorrhea and recurrent left epistaxis. These symptoms had
worsened during the last 5 months prior to hospitalization, with no
improvement following medical treatment for maxillary sinusitis.
Clinical examination at this stage revealed the following: Left
exophthalmy, and a tumor of reddish color and soft consistency that
occupied the entire left nasal cavity and was associated with an
extensive swelling in the left maxilla.
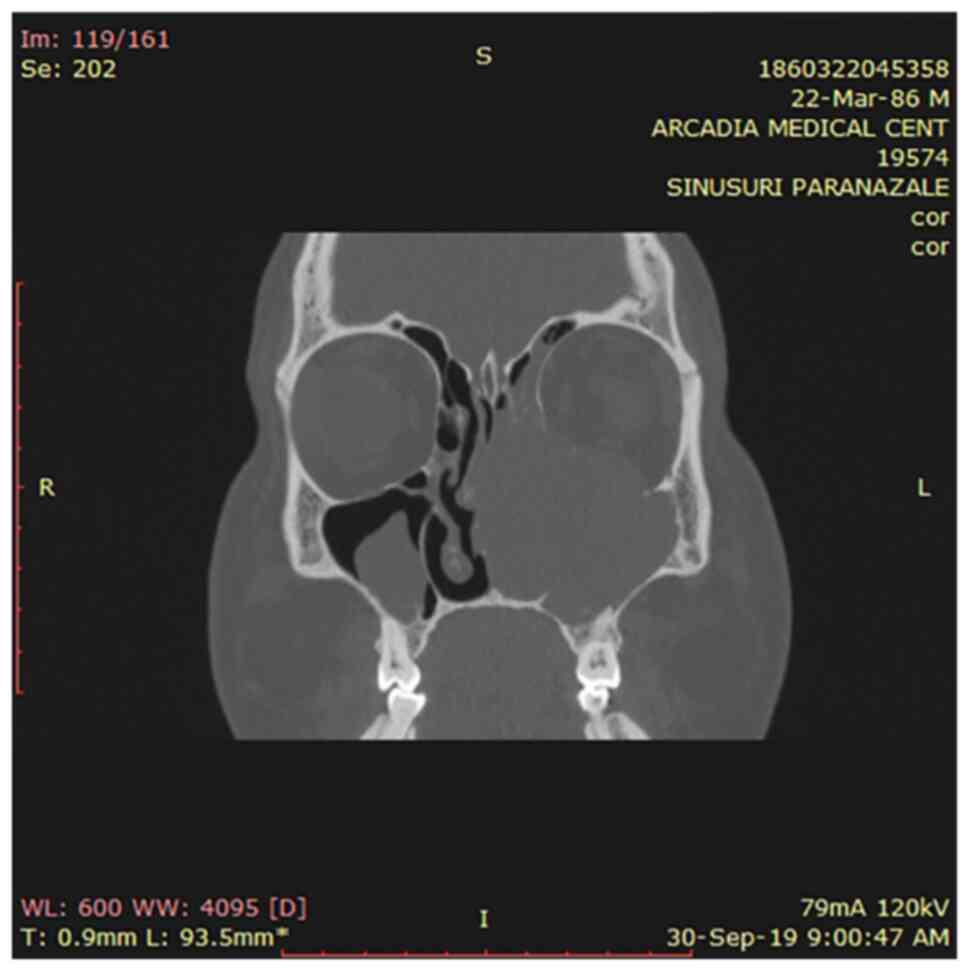
Another CT scan was performed followed by cranial
MRI examination that showed a large irregular tumor mass with
heterogeneous density filling the left nasal cavity and involving
the left paranasal sinuses. An expansive osteolytic bone
destruction pattern was observed in the ethmoid bone, medial and
lateral walls of the left maxillary sinus and orbital floor. Left
obstructive sinusitis and left exophthalmy were also present. The
lesion was isointense on T1 weighted images and exhibited mild
hypointensity on T2 weighted images (Fig. 1). There was no evidence of
metastasis on the total body scan.
The clinical diagnosis was a malignant tumor of
unknown type. A biopsy was performed, along with histopathological
examination, which concluded that the tumor was a sarcoma composed
of fusiform cells arranged in long intersected, irregular
fascicles. Tumoral proliferation with moderate cellularity was
observed, with non-homogeneous chromatin, elongated nuclei, some
nucleoli, with a homogeneous, moderately pleomorphic cell
population (9). Moderate mitotic
activity was observed, with no tumor necrosis, and a Ki-67 index of
50%.
The final diagnosis of grade 2 fibrosarcoma [score 3
according to the Fédération Nationale des Centres de Lutte Contre
Le Cancer (10)] was based on the
clinical, radiographic and histopathological characteristics and
immunohistochemistry examinations (smooth muscle actin was negative
in the tumor cells and positive in the vascular walls; S100 was
negative in the tumor cells and positive in the nerve fibers of the
mucosal chorion; CD34 was negative in tumor cells and positive in
the endothelial cells of intratumoral capillaries; CKAE1/3 was
negative in the tumor cells and positive in the mucosa and glands
of the chorion; and vimentin was positive in the tumor cells). The
stage was T4N0M0 and the treatment of choice was extended surgical
resection with facial reconstruction and radiotherapy.
The surgical strategy included radical maxillectomy
of the left side with removal of the left inferior orbital wall and
left nasal cavity, as well as left-side ethmoidectomy, in order to
ensure clear tumor resection margins (Fig. 2).
The inferior orbital wall was replaced by a titanium
mesh and a temporoparietal fascial flap was used to cover it,
elevated and transposed to the orbit through a subcutaneous tunnel.
An acrylic obturator prosthesis was especially designed and adapted
to the patient's postoperative defect.
Resection of the cervical lymph nodes in this case
was not deemed necessary.
Postoperatively, the patient underwent radiotherapy
treatment with Cobalt-60 using a linear accelerator at a total dose
of 50 Gy divided into 1.8-2 Gy per cycle of treatment over 5 weeks,
with good preservation of the covering flap. The patient
experienced no major side effects after the radiotherapy.
The patient was able to speak, eat and chew without
any problems after 5 days. In addition, there were no difficulties
with swallowing. The prosthesis allowed the patient to lead a
normal life. He was satisfied with the postoperative cosmetic
result and had no social problems or other complaints.
Control assessments were performed at 6 and 12
months postoperatively, showing no evidence of locoregional
recurrence, systemic metastases or distant complications. The last
check-up was in May 2021, revealing a good outcome for the
patient.
This procedure achieved optimal reconstruction of
the anterior wall of the left maxillary sinus and inferior orbital
wall. Moreover, it has greatly improved the aesthetic postoperative
outcomes (Fig. 3).
Discussion
Sinonasal fibrosarcoma is a rare malignant tumor,
with only 1% of fibrosarcomas occurring in the head and neck
region, whereas the majority are found at the extremities (11). Final diagnosis and staging are based
on histopathology, immunohistochemistry examination and on the
imaging evaluation (12).
Sinonasal fibrosarcomas are associated with a high
risk of local recurrence, but a low risk of distant metastasis
(12,13). The indicated treatment with the best
results is complete surgical resection of the tumor followed by
reconstruction and combined with postoperative radiotherapy
(11,12).
The biggest challenge of sinonasal reconstruction is
to repair a complex three-dimensional structure, with the varying
thickness of the tissue covering it, to restore its function and
aesthetic appearance to the greatest possible extent (14) and to achieve facial symmetry with a
good aesthetic outcome (15). The
prosthesis should provide a natural look adapted to the patient's
physiognomy, with no visible defects or scars (16), and with minimal risk of
complications. The local flap alone may not be able to fully
reestablish all the essential functions.
Particular cases, such as the present, highlight the
dilemma when selecting the appropriate method of reconstruction for
a young patient with a sizeable facial defect that may result after
radical surgery, which must be resolved to the greatest possible
extent. The combination of craniofacial prosthetic techniques with
temporoparietal flaps has been proven to be a successful technique
(17,18). However, this method may not be
suitable for all patients undergoing sinonasal cancer surgery, as
sometimes a simple flap alone may be a better option (for example,
in elderly patients or those who cannot adapt or do not have the
ability to remove the prosthesis) (19). Furthermore, certain activities, such
as speaking and swallowing, may be more difficult with a flap than
with an obturator prosthesis alone (20).
The reconstruction of the orbital floor is another
complex issue after an extensive surgical resection. It is
important to maintain the orbital contents in place, to prevent a
later dystopia, diplopia or the risk of a non-functional eye
(21). There must be enough soft
tissue coverage of the bone or titanium mesh, complete isolation of
sinonasal structures and an adequate orbital cavity depth in order
to achieve a realistic appearance and facial symmetry (19,22).
Another crucial factor that can change the
reconstructive strategy is the patient's history. For those with a
history of diabetes and tobacco use, there is a higher risk of skin
necrosis, which may require adaptation of the approach (5). In addition, the patient's expectations
and facial features may change the surgeon's perspective. For
example, older patients may not have the same appearance
expectations and tissue availability as younger patients (23). In order to achieve superior
aesthetic and functional results, a local flap with appropriate
tissue donor sources (14)
associated to an obturator prosthesis and a multilevel
reconstructive method may be the most viable option (22). The location, size and depth of the
surgical defect, and also adapting the technique to the patient's
particularities and needs, represent important variables in this
field (20). Moreover, it is
mandatory to ensure good postoperative care and follow-up in order
to optimize the final result. A compliant and well-informed patient
regarding the importance of postoperative care may significantly
improve the final cosmetic result (8).
Due to the complexity of the facial structures and
the surgical approach, the multidisciplinary team working on the
case must be experienced enough to elaborate the entire treatment
plan, to manage any potential intraoperative complications (for
example, the craniofacial area is highly vascular and there is a
high risk of hemorrhage, a large residual defect may be left after
resection, nerve injury may occur, etc.), as well as postoperative
complications. The nutritional status (24) is crucial for the healing process
(25,26), as the survival of the flap depends
on both the vascular supply and the local defense mechanisms. In
addition, all the steps involved in the management process must be
thoroughly explained to the patients, including surgery and
adjuvant therapy, to ensure proper compliance to treatment
(27), which may result in an
improved overall outcome.
In the present case, the patient was young, with no
remarkable medical history, and this allowed us to employ a
multimodal reconstructive technique with better functional outcomes
compared with either flap reconstruction or prosthesis alone. Good
communication and patient compliance were established early during
this process, which was also an important factor that allowed us to
implement improved solutions.
Overall, the management of large craniofacial
defects after advanced sinonasal cancer resection represents an
important challenge for the majority of surgeons. In order to
achieve satisfactory results, it is important to adapt the
technique to each patient's particularities, cosmetic expectations,
age and prognosis, while preserving vital functions. On the other
hand, these challenges allow us to implement improved
reconstructive techniques and methods, striving to preserve the
patient's quality of life to the greatest extent possible.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data presented and/or analysed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
All authors contributed to the acquisition of the
data and critical revision of manuscript for important intellectual
content. DOP and FA were responsible for the research design and
manuscript drafting. CP and MP were responsible for language
editing. VC and VA were responsible for editing the article and
photos. PZ contributed to the literature data analysis and the
critical interpretation and FM was a major contributor to the
writing of the manuscript. RH has reviewed the manuscript. DOP and
PZ confirm the authenticity of the raw data. All authors read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Signed written consent form was obtained from the
patient regarding the publication of the case details and
associated images.
Competing interests
All the authors declare that they have no competing
interests.
References
|
1
|
Banuchi V, Mallen J and Kraus D: Cancers
of the nose, sinus, and skull base. Surg Oncol Clin N Am.
24:563–577. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Haerle SK, Gullane PJ, Witterick IJ,
Zweifel C and Gentili F: Sinonasal carcinomas: Epidemiology,
pathology, and management. Neurosurg Clin N Am. 24:39–49.
2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kauke M, Safi AF, Grandoch A, Nickenig HJ,
Zöller J and Kreppel M: Sarcomas of the sinonasal tract. Head Neck.
40:1279–1286. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Suárez C, Ferlito A, Lund VJ, Silver CE,
Fagan JJ, Rodrigo JP, Llorente JL, Cantù G, Politi M, Wei WI and
Rinaldo A: Management of the orbit in malignant sinonasal tumors.
Head Neck. 30:242–250. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Na'ara S, Mukherjee A, Billan S and Gil Z:
Contemporary multidisciplinary management of sinonasal mucosal
melanoma. Onco Targets Ther. 13:2289–2298. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Eskander A, Kang SY, Teknos TN and Old MO:
Advances in midface reconstruction: Beyond the reconstructive
ladder. Curr Opin Otolaryngol Head Neck Surg. 25:422–430.
2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mello MC, Piras JA, Takimoto RM, Cervantes
O, Abraão M and Dib LL: Facial reconstruction with a bone-anchored
prosthesis following destructive cancer surgery. Oncol Lett.
4:682–684. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Paprocki GJ: Maxillofacial prosthetics:
History to modern applications. Part 1-obturators. Compend Contin
Educ Dent. 34:e84–e86. 2013.PubMed/NCBI
|
|
9
|
Stanciu AE, Zamfir-Chiru-Anton A, Stanciu
MM, Pantea Stoian A, Jinga V, Nitipir C, Bucur A, Pituru TS, Arsene
AL, Dragoi CM, et al: Clinical significance of serum melatonin in
predicting the severity of oral squamous cell carcinoma. Oncol
Lett. 19:1537–1543. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
National Cancer Institute (NCI): PDQ
Cancer Information Summaries [Internet]. NCI, Bethesda, MD,
2022.
|
|
11
|
Patel TD, Carniol ET, Vázquez A, Baredes
S, Liu JK and Eloy JA: Sinonasal fibrosarcoma: Analysis of the
surveillance, epidemiology, and end results database. Int Forum
Allergy Rhinol. 6:201–205. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ekinci A, Karataş D, Yetiş A, Erenler BH
and Ozcan M: Destructive fibrosarcoma of the maxillary sinus. J
Craniofac Surg. 29:e226–e228. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Plaza G, Ferrando J and Pinedo F:
Sinonasal fibrosarcoma: A case report. Eur Arch Otorhinolaryngol.
263:641–643. 2006.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gentile P, Nicoli F, Caruso R, Gravante G
and Cervelli V: Alternative strategy to reconstruct the nose after
excision: Extra-oral implant anchored to bone. Br J Oral Maxillofac
Surg. 47:50–51. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Summers BK and Siegle RJ: Facial cutaneous
reconstructive surgery: Facial flaps. J Am Acad Dermatol.
29:917–944. 1993.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Little SC, Hughley BB and Park SS:
Complications with forehead flaps in nasal reconstruction.
Laryngoscope. 119:1093–1099. 2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kim JYS, Buck DW II, Johnson SA and Butler
CE: The Temporoparietal fascial flap is an alternative to free
flaps for orbitomaxillary reconstruction. Plast Reconstr Surg.
126:880–888. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hu S, Arnaoutakis D, Kadakia S, Vest A,
Sawhney R and Ducic Y: Osseointegrated implants and prosthetic
reconstruction following skull base surgery. Semin Plast Surg.
31:214–221. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ali MM, Khalifa N and Alhajj MN: Quality
of life and problems associated with obturators of patients with
maxillectomies. Head Face Med. 14(2)2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hoasjoe DK, Stucker FJ and Aarstad RF:
Aesthetic and anatomic considerations for nasal reconstruction.
Facial Plast Surg. 10:317–321. 1994.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Santamaria E and Cordeiro PG:
Reconstruction of maxillectomy and midfacial defects with free
tissue transfer. J Surg Oncol. 94:522–531. 2006.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Gliklich RE, Rounds MF, Cheney ML and
Varvares MA: Combining free flap reconstruction and craniofacial
prosthetic technique for orbit, scalp, and temporal defects.
Laryngoscope. 108:482–487. 1998.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Burget GC and Menick FJ: The subunit
principle in nasal reconstruction. Plast Reconstr Surg. 76:239–247.
1985.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Nitipir C, Diaconu CC, Orlov C, Pantea
Stoian A, Hainarosie R, Slavu I, Suceveanu AI, Pituru A and Popa
AM: The necessity of nutritional intervention in the oncological
patient. What is the evidence? Conference: 35th Balkan Medical Week
on Healthy Ageing-An Endless Challenge, Proceedings of The 35th
Balkan Medical Week, pp133-137, 2018.
|
|
25
|
Drăgoi CM, Moroșan E, Dumitrescu IB,
Nicolae AC, Arsene AL, Drăgănescu D, Lupuliasa D, Ioniță AC, Pantea
Stoian A, Nicolae C, et al: Insight into chrononutrition: The
innermost interplay amongst nutrition, metabolism and the circadian
clock, in the context of epigenetic reprogramming. Farmacia.
67:557–571. 2019.
|
|
26
|
Rahnea-Nita G, Ciuhu AN, Pantea-Stoian AM,
Nitipir C, Popescu M, Badiu DC, Andronache LF, Mandu M and
Rahnea-Nita RA: Assessment of cachexia in cancer patients with
advanced disease. In: Proceedings if the 3rd International
Conference on Interdisciplinary Management of Diabetes Mellitus and
its Complications (INTERDIAB). INTERDIAB, Bucharest, pp139-147,
2017.
|
|
27
|
Țânțu MM, Stan GM, Rogozea L, Păunescu A,
Pleșa CF, Nemeș RM, Nicolae C and Bisoc A: Drug use, a valid
indicator for effective implementation of medical protocols.
Revista de Chimie-Bucharest-Original Edition. 70:859–862. 2019.
|