Introduction
In recent years, the number of individuals with
obesity has increased worldwide because of changes in social
environments and lifestyles, including dietary habits (1). In treating primary obesity, it is
essential to understand the cause of excessive energy intake
through dietary surveys and to reduce one's weight by correcting
the energy balance. Since underreporting occurs in dietary surveys,
it is necessary to obtain information individually (2-5).
Generally, the degree of underreporting is assessed using the ratio
of reported energy intake to the basal metabolic rate (EI/BMR)
(2,6,7). It
has been found that overweight and obese individuals, including
those in Japan, have a lower EI/BMR value than individuals without
obesity, and a large proportion of these are underreported
(2,8-11).
However, data on obese Japanese individuals are lacking.
Furthermore, we have occasionally observed dietary survey data that
may reflect not only mere underreporting but also extreme
energy-restricted diets challenged by obese individuals for short
periods of time. Therefore, some of those judged to be
underreported with low EI/BMR may include those with energy
deficits due to such extreme diets; distinguishing between these
may be useful in accurately determining the diet that led to
obesity in each patient and to provide appropriate dietary therapy
based on the findings. However, there is no established way to
distinguish between or screen for these factors. Because ketone
bodies are evaluated in terms of energy shortage (12), it may be possible to distinguish
between the two reporter types by combining EI/BMR and ketone
bodies.
Accordingly, the purpose of this study was to
examine the relationship between EI/BMR, body mass index (BMI), and
ketone bodies in obese Japanese women to improve the quality of
dietary surveys in the treatment of obesity.
Materials and methods
Participants
This institutional cohort study is an ongoing
epidemiological study that began in 1994, primarily targeting women
with obesity. This was a retrospective study using data previously
collected for a cohort study database.
The participants of this study were those with
obesity with a BMI ≥25 kg/m2 (13) who participated in the baseline
survey of the institutional cohort study between 2006 and 2015 and
underwent anthropometric measurements, blood tests, and a 3-day
dietary survey. All measurements were performed by a trained
investigator at the research facility. Because obesity is a complex
pathology related to the pre-stage of various diseases, the
following exclusion criteria were set to exclude obesity-related
conditions in advance, and to target as much as possible, purely
obese participants: 1) age >65 years; 2) BMI less than 25
kg/m2; 3) medication or history of hypertension,
dyslipidemia, or diabetes; and 4) missing data. In addition, to
exclude the effect of glucose metabolism on ketone bodies,
participants with 5) fasting glucose levels of 140 mg/dl or higher
or HbA1C levels of 6.5% or higher were excluded.
Anthropometric measurements, blood pressure measurements, and blood
tests were performed on those fasting after 22:00 on the day prior
and without having had breakfast.
Anthropometric measurements
Fasting measurements of height, body weight, and
abdominal circumference were conducted while lightly dressed
without shoes or socks, after urinary excretion. Height and body
weight measurements were recorded as 0.1 cm and 0.1 kg,
respectively, and 1 kg was subtracted from the recorded body weight
to adjust for the weight of clothes (14). BMI was calculated using the
following formula: weight (kg)/height (m2). The
abdominal circumference was measured using a measuring tape around
the navel in 0.1 cm increments, with both feet shoulder-width apart
and arms hanging naturally, and with the participants lightly
exhaled and relaxed (13).
Blood pressure measurement
The cuff was kept at heart level, and blood pressure
was measured in a resting upright sitting position three times at
1-min intervals. The recorded blood pressure was the mean value of
three consecutive measurements, with differences between
measurements below 10 mmHg. It was re-evaluated if there was a
difference of >10 mmHg between the three measurements (14). An upper arm-cuff sphygmomanometer
(BP8800; Colin Co., Ltd.) was used for blood pressure
measurements.
Blood test
Blood collection and measurement for each blood test
item were sourced from SRL Co., Ltd. The inspection items used in
this study were as follows. Blood cells were measured for white
blood cells (automated method), red blood cells (automated method),
and hemoglobin levels (automated method). Blood lipid,
triglyceride, total cholesterol, and high-density lipoprotein (HDL)
cholesterol levels were measured. Low-density lipoprotein
cholesterol levels were calculated using the Friedewald equation
(15). Glucose metabolism-related
parameters were measured using fasting blood glucose (enzymatic
colorimetric method), HbA1C (enzymatic colorimetric
method), and insulin (chemiluminescent enzyme immunoassay) levels.
Homeostasis model assessment-insulin resistance (HOMA-R) was
calculated using fasting blood glucose and insulin values (16). In addition, acetoacetic acid and
3-hydroxybutyric acid were measured as organic acids in the fasting
state using an enzymatic colorimetric method, and the sum was
considered the level of ketone bodies in the blood. Researchers
with expertise in ketones agree that a ketone body level <0.5
mmol is normal and that a ketone body level in excess of 1.0 mmol
is considered hyperketonemic (17,18).
In this study, those with abnormally high ketone body levels (≥1.0
mmol/l) were defined as having short-term energy deficiencies.
Dietary survey
The dietary survey was conducted on three
consecutive days (one day on the weekends and on two weekdays),
using a food recording method combined with photographic recording.
We asked participants to be careful not to omit the recording of
seasonings used, the parts of any meat consumed, favorite foods,
and beverages, and to maintain a normal diet without deliberately
making the meals luxurious or restricted. In addition, we asked
participants to take pictures of their meals as served before
eating, and when there were leftovers, we asked them to record and
photograph the percentage of food left. When measurements were
difficult, for example when eating out, we instructed them to
record the size and quantity of foods they ate in as much detail as
possible. The registered dietitian researchers carefully examined
all dietary records and photographs. If any omissions or erroneous
entries were suspected, the participant was contacted for
face-to-face confirmation. If necessary, additions or corrections
were made before energy and nutrient intakes were calculated. The
energy and nutrient intakes in this study were analyzed using the
Standard Tables of Food Composition in Japan (19,20)
for an average of three days.
Assessment of underreporting by
determining the ratio of energy intake to basal metabolic rate
(EI/BMR)
EI/BMR was calculated by dividing the energy intake
obtained from the dietary survey via the basal metabolic rate
estimated using the National Institute of Health and Nutrition
formula (Ganpule's formula) (11,21,22).
The Ganpule formula was developed based on the BMR values of 137
Japanese men and women aged 20-74 years (66 women) (21), and its validity was confirmed by
comparison with the measured BMR values of 365 Japanese men and
women aged 18-79 years (202 women, BMI range: 16.5 to 36.4
kg/m2). Thus, compared to other estimation formulas, the
BMR estimation value obtained from the Ganpule formula is less
affected by age and body weight, and it has been reported that it
can be applied to individuals of all ages and whose status range
from thin to obese (22). The
cutoff value of EI/BMR for estimating underreporting was set at
1.35 and the value is the minimum cutoff value for energy intake
required to lead a normal life, as shown in previous studies using
the basic principles of energy physiology (6). This cutoff value was derived from
nine studies (n=207) that examined energy balance using whole-body
calorimeter measurements and doubly-labelled water measurements,
the gold standard of energy expenditure measurement, and is
considered reliable. This cutoff value has also been used in
large-scale studies investigating the relationship between
underreporting and weight and lifestyle (8), as well as in a recent study of
Japanese participants (23).
Thus, to accurately estimate the status of
underreporters or energy-restricted reporters in this study, we
defined 1) those with EI/BMR <1.35 and a ketone body level
<1.0 mmol/l as underreporters, 2) those with EI/BMR <1.35 and
a ketone body level ≥1.0 mmol/l as energy-restricted reporters, and
3) those with EI/BMR ≥1.35 as no underreporting.
Statistical analysis
Data are shown as mean ± standard deviation.
Pearson's correlation coefficient was used to determine the
relationship between EI/BMR and each variable, and a stepwise
multiple regression analysis was used. BMI, triglycerides, insulin,
HOMA-R, and ketone bodies, which were not normally distributed,
were analyzed after a log transformation. Comparisons of multiple
groups were performed using one-way ANOVA variance and evaluated
using Dunnett's post-hoc test with underreporters as controls,
where differences were significant (vs. energy-restricted reporters
and non-underreporters). Statistical Package for the Social
Sciences (SPSS) v27 (IBM Institute) was used, and a two-sided
p-value <0.05 was used to indicate statistical significance.
Ethical considerations
This study was approved by the ethical committee of
Nakamura Gakuen University (No. Rinri-13-015) and was performed in
accordance with the Declaration of Helsinki. In addition to aspects
of personal information protection, the following were explained:
the outline of the study, voluntary enrollment, no discrimination
when refusing enrollment, freedom to withdraw from the agreement of
participation with no discrimination, and that the results would be
made public at scientific conferences and in the literature.
Written informed consent documents were voluntarily supplied.
Results
Characteristics of the participants
included in the final analysis
A total of 164 participants were enrolled in the
study, and 91 were included in the final analysis. Excluded
participants included 24 whose BMI was less than 25 kg/m²; 44 who
were taking medication for blood pressure, blood glucose, or serum
lipids, or who had a history of hypertension, diabetes, or
dyslipidemia; 3 who had missing data to be used for analysis; and 2
who had fasting blood glucose levels ≥126 mg/dl or HbA1c
levels ≥6.5%. The participants were 47±9 years of age, had a BMI of
29.8±3.9 kg/m², and had normal mean values of blood pressure, serum
blood glucose levels, and lipid levels (Table I). The mean value of the
participants' ketone bodies was 0.98±1.50 mmol/l, which was within
the normal range, but 25.3% of the participants exceeded 1.0
mmol/l, which was defined as the upper limit in this study. The
energy intake estimated from the participants' dietary survey was
1,911±449 kcal/day, and the mean value of the BMR estimated using
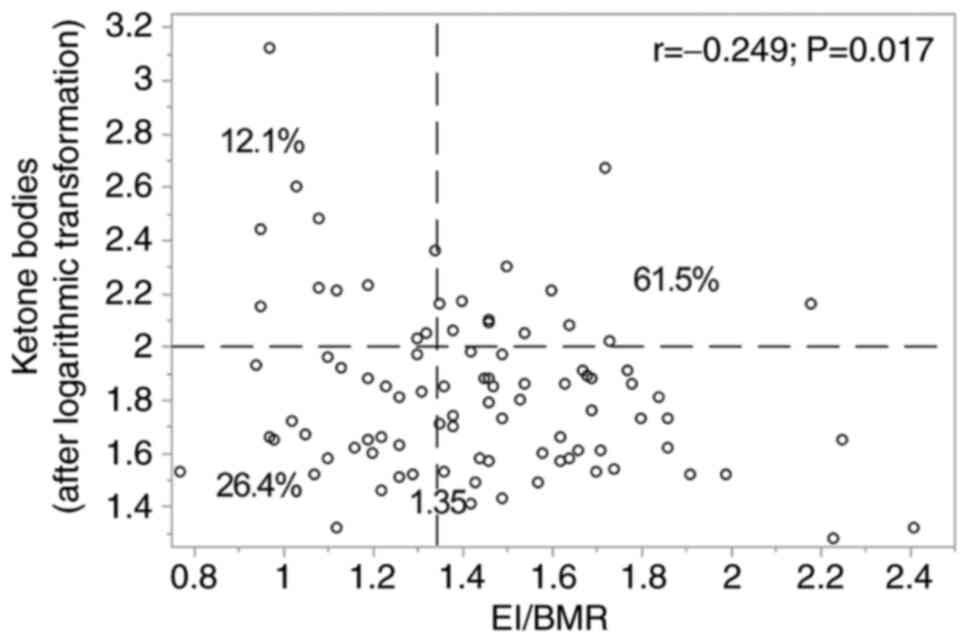
Ganpule's formula was 1,336±161 kcal/day (Table I). The mean value of EI/BMR
calculated by dividing these values was 1.44±0.32, and 38.5% of the
values were below the cutoff value of 1.35 (Fig. 1).
 | Table IParticipant characteristics and
clinical laboratory values. |
Table I
Participant characteristics and
clinical laboratory values.
| | Percentile |
|---|
| Characteristic | All | 25th | 50th | 75th |
|---|
| N | 91 | | | |
| Age (years) | 47±9 | 40 | 48 | 53 |
| Height (cm) | 157.0±5.2 | 153.9 | 156.8 | 160.0 |
| Weight (kg) | 73.5±11.2 | 65.9 | 70.9 | 80.3 |
| BMI
(kg/m2) | 29.8±3.9 | 26.7 | 28.9 | 31.3 |
| Waist circumference
(cm) | 97.6±8.8 | 91.1 | 96.8 | 103.2 |
| Energy intake | 1911±449 | 1,637 | 1,870 | 2,145 |
| BMR | 1336±161 | 1,213 | 1,327 | 1,414 |
| EI/BMR | 1.44±0.32 | 1.20 | 1.43 | 1.64 |
| Systolic blood
pressure (mmHg) | 124±15 | 111 | 122 | 134 |
| Diastolic blood
pressure (mmHg) | 74±10 | 67 | 74 | 81 |
| White blood cell
(/µl) | 5,746±1,400 | 4,800 | 5,600 | 6,800 |
| Red blood cell
(/µl) | 457±34 | 433 | 458 | 481 |
| Hemoglobin
(g/dl) | 13.2±1.1 | 12.5 | 13.3 | 14.1 |
| Total cholesterol
(mg/dl) | 215±41 | 188 | 210 | 235 |
| LDL cholesterol
(mg/dl) | 136±35 | 112 | 135 | 156 |
| HDL cholesterol
(mg/dl) | 58±12 | 50 | 56 | 67 |
| Triglyceride
(mg/dl) | 105±56 | 66 | 94 | 132 |
| Fasting blood
glucose (mg/dl) | 93±11 | 87 | 92 | 99 |
| HbA1c (%) | 5.3±0.4 | 5.1 | 5.3 | 5.5 |
| Insulin
(µU/ml) | 10.0±5.7 | 6.2 | 9.0 | 12.3 |
| HOMA-R | 2.3±1.5 | 1.3 | 2.0 | 2.9 |
| Ketone bodies
(µmol/l) | 0.98±1.50 | 0.40 | 0.63 | 1.04 |
Correlation between EI/BMR and each
variable
The correlations between EI/BMR and age, physical
measurements, and blood test values were measured. There was a
significant positive correlation between EI/BMR and log-transformed
triglyceride levels (r=0.208, P=0.047) and log-transformed ketone
body levels (r=-0.249, P=0.017). Multiple stepwise linear
regression analysis was performed with EI/BMR as the objective
variable and log-transformed triglycerides and log-transformed
ketone bodies, which showed significant correlations with age and
log-transformed BMI, as regulators and explanatory variables,
respectively. The standard partial regression coefficients from
each explanatory variable to the objective variable are shown in
Table II, and only
log-transformed ketone bodies are indicated as significant
explanatory variables.
| Table IIMultiple stepwise linear regression
analysis of factors associated with EI/BMR (N=91). |
Table II
Multiple stepwise linear regression
analysis of factors associated with EI/BMR (N=91).
| Factor | Partial regression
coefficient (β) | Standardized
partial regression coefficient (β) | P-value |
|---|
| Age (years) | 0.003 | 0.083 | 0.450 |
| BMI
(kg/m2)a | -0.012 | -0.148 | 0.179 |
| Ketone bodies
(µmol/l)a | -0.262 | -0.260 | 0.013 |
|
R2 | 0.100 | | |
| Adjusted
R2 | 0.069 | | 0.026 |
Comparison of proportions and
characteristics of underreporters, energy-restricted reporters and
those who did not underreport (non-underreporters) estimated by
EI/BMR and ketone bodies
We estimated the proportion of underreporters and
energy-restricted reporters, based on the association between
EI/BMR and ketone bodies. The results showed that 61.5% of the
participants did not underreport (EI/BMR ≥1.35), 26.4%
underreported (EI/BMR <1.35, ketone bodies <1.0 mmol/l), and
12.1% reported energy restriction (EI/BMR <1.35 and ketone
bodies ≥1.0 mmol/l) (Fig. 1).
Finally, the characteristics, energy and nutrient
intakes, and laboratory values were compared among the
underreporter, energy-restricted reporter, and no underreporting
groups. The results showed that underreporters were significantly
younger and had significantly higher weights and BMI than
non-underreporters. However, there were no significant differences
in reported energy intake, carbohydrate intake (g/day), and %
carbohydrate (%) between the underreporters and energy-restricted
reporters (Table III).
| Table IIIComparison of group characteristics,
clinical laboratory values and reported energy and reported energy
and nutrients intake between groups by EI/BMR and ketone
bodies. |
Table III
Comparison of group characteristics,
clinical laboratory values and reported energy and reported energy
and nutrients intake between groups by EI/BMR and ketone
bodies.
| Characteristic | Underreporters
(n=24) | Energy-restricted
reporters (n=11) | Non-underreporters
(n=56) | P-value |
|---|
| Age (years) | 43±10 | 49±9 | 48±8a | 0.032 |
| BMI
(kg/m2)b | 31.3±5.0 | 30.7±3.1 |
28.9±3.3a | 0.029 |
| Energy
(kcal/day) | 1,604±293 | 1,469±182 |
2,130±398a | <0.001 |
| Basal metabolic
rate | 1,408±189 | 1,315±96 |
1,309±150a | 0.036 |
| EI/BMR | 1.14±0.13 | 1.12±0.15 |
1.63±0.24a | <0.001 |
| Protein
(g/day) | 63.5±13.3 | 59.7±11.2 |
77.7±15.9a | <0.001 |
| % Protein (%) | 16.1±4.3 | 16.2±2.0 | 14.7±2.0 | 0.051 |
| Fat (g/day) | 52.4±12.2 | 46.9±14.2 |
72.3±18.1a | <0.001 |
| % Fat (%) | 29.5±4.7 | 28.3±6.2 | 30.5±5.0 | 0.385 |
| Carbohydrate
(g/day) | 208.7±51.2 | 197.5±24.1 |
279.8±59.8a | <0.001 |
| % Carbohydrate
(%) | 51.6±7.1 | 54.2±6.8 | 52.6±4.7 | 0.457 |
Discussion
This study is the first to demonstrate a
relationship between EI/BMR and ketone bodies in Japanese women
with obesity and aimed to distinguish between underreporters and
energy-restricted reporters to improve the quality of dietary
surveys in the treatment of obesity. Dietary surveys of individuals
with obesity show underreporting (2,8-11)
and a lack of energy due to the extreme energy-restricted diets.
EI/BMR can determine the presence and extent of underreporting, but
it cannot determine energy deficiency due to extreme dietary
restrictions. Conversely, ketone bodies can determine the presence
of energy deficits, but provide no information about
underreporting. However, the combination of the EI/BMR ratio and
ketone body levels can discriminate between or screen for both, and
through improved accuracy of dietary surveys, may lead to a better
understanding of the original diet that led to obesity in each
patient, which may lead to appropriate treatment.
The mean EI/BMR value of obese Japanese women in
this study was 1.44, which is lower than the mean EI/BMR value of
1.69 for Japanese women in representative studies using data from
the National Health and Nutrition Examination Survey (11). Underreporting was confirmed to be
frequent, as in previous studies conducted in Japan and abroad
(2,8-11).
Furthermore, 25.3% of the participants had
abnormally high levels of ketone bodies, indicating that
individuals with obesity undergoing dietary surveys should be
assumed to have extremely deficient energy intake (12) owing to excessive dietary
restriction. A significant negative correlation was found between
EI/BMR and ketone body levels, which was also a significant
variable in the multiple regression analysis. This suggests that
12.1% of those with an EI/BMR <1.35 and ketone body level ≥1.0
mmol/l included underreporters and those who reported extreme
energy restriction practices at the time of the dietary survey and
blood test. However, because ketone bodies are known to exhibit
diurnal variation (24), further
investigation is needed to determine the extent to which ketone
body values in a single blood sample reflect temporary energy
deficits in obese individuals. In recent years, ketone bodies have
been measured simply and accurately using small devices (25). Thus, evaluation of the quality of
dietary surveys combining EI/BMR and ketone bodies can be performed
in real time. This method is expected to improve the quality of
dietary surveys of individuals with obesity in clinical practice.
In addition, an extreme lack of carbohydrate intake was not
considered because there was no difference in the carbohydrate
intake (g/day), and % carbohydrate (%) between the group of
underreporters with ketone bodies in the normal range and the group
of energy-restricted reporters with abnormal ketone bodies.
In general, EI/BMR and BMI are negatively correlated
(8,10,11).
In addition, EI/BMR and age were reported to be negatively related
in previous studies conducted overseas (8,26)
and positively related in previous studies conducted in Japan
(10,11); thus, the results are conflicting.
This may be because the results are affected by differences in the
dietary survey methods between those used in previous studies in
Japan and overseas. In particular, previous studies conducted
overseas used the food intake frequency survey method (8) and 24-h recall method (26), whereas previous studies conducted
in Japan used semi-weighed dietary records (10,11).
In contrast, the present study was conducted with a relatively high
degree of accuracy, using a three-day food recording method
combined with photographic recording, as well as face-to-face
confirmation of dietary content by the examiner's registered
dietitian researchers. In this study, which included a special
population of only obese participants, underreporters with low
EI/BMR were younger and had a higher BMI than non-underreporters,
consistent with the results of previous studies. However, the small
number of subjects in this study makes generalization difficult and
further research is needed in the future.
In previous studies, several diet quality scores,
such as the Healthy Eating Index and the Mediterranean Diet Index,
were significantly associated with insulin resistance and indices
of inflammation (27). However, we
found no association between EI/BMR and the indices of glucose
metabolism or inflammation in the present study. We hypothesize
this is because the Healthy Eating Index and the Mediterranean Diet
Index systematically present the intake of various foods, whereas
the EI/BMR only considers the ratio of reported energy intake to
BMR.
This study had several limitations. First, EI/BMR
affects various factors such as smoking status, educational
history, recent weight changes, body composition, physical
activity, self-body image, health consciousness, and social
disability (2,3,8,28,29).
However, in this study, these data were not sufficiently available
and EI/BMR was not adjusted for various factors, which may have
affected the results. Furthermore, the participants were from a
relatively homogeneous population, with similar race, sex, BMI,
age, and health consciousness, and we hypothesize that the results
of this study provide informative results. In the future, based on
the results of this study, it would be valuable to conduct studies
that include several factors that may affect EI/BMR. Second, this
study did not accurately evaluate physical activity levels. In
addition, the target population was highly conscious of weight
loss, and there seemed to be an error in the proportion of
underreporters and energy-restricted reporters using the
relationship between EI/BMR and ketone bodies. Third, this study
targeted individuals who lived in specific areas, and the number of
participants and dietary survey days were relatively small.
However, few reports of careful collection and analysis of the
dietary content of Japanese individuals with obesity using the food
recording method combined with photographic recording exist in the
literature, and the findings of the present study are therefore
valuable. Fourth, there was a time lag of up to 10 years between
study participants, and there may have been an error in the
nutritional value due to repeated revisions of the Standard Tables
of Food Composition in Japan during this period. In addition, most
dietary surveys in this study were conducted between September and
October, which does not allow for seasonal variations in energy
intake (30). However, compared
with the underreporting of energy intake, the errors in energy
intake caused by food composition tables and seasonal variations
are quite small and are unlikely to have a significant impact on
the results of this study. Fifth, the BMR was not a measured value
but an estimated one using Ganpule's formula with reference to
previous studies (11). Therefore,
the EI/BMR ratio calculated based on the BMR estimates may contain
errors.
Furthermore, it has not been confirmed whether the
EI/BMR cutoff value used in this study is suitable for the Japanese
population. Therefore, the percentages of underreporters,
energy-limited reporters, and non-underreporters may also contain
errors. However, the combination of EI/BMR and ketone bodies is
useful for screening to reduce errors included in dietary surveys,
and the results of this study may lead to improvements in the
quality of dietary surveys of individuals with obesity.
Despite these limitations, we hypothesize that the
present study was highly significant because it showed the
relationship between EI/BMR, BMI, and age in Japanese women with
obesity and the possibility of estimating not only underreporting
but also energy deficiency associated with energy restriction in
the participants by combining EI/BMR and ketone body levels.
In conclusion, low EI/BMR was associated with high
ketone body levels in obese Japanese women. The combination of
EI/EMR and ketone body levels may distinguish between or screen for
underreporters and energy-restricted reporters at the time of the
dietary survey.
Acknowledgements
The authors wish to thank Dr Kenta Noguchi, Ms. Mana
Miya, Ms. Aiko Oniki and Ms Shoko Maeda at the Health Promotion
Center (Nakamura Gakuen University) for their technical
assistance.
Funding
Funding: This study was supported by Nakamura Gakuen
University.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KY, SN, MK and HK conceived, designed and supervised
the study. KY, RM, KI, SA, MO, HU, KW, SN and HK registered
subjects and collected data. IY and KY confirm the authenticity of
all the raw data. IY, KY and RM analyzed and interpreted the data.
RM, MO, MK and HK reviewed the manuscript. IY and KY wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethical Committee of
Nakamura Gakuen University (approval no. Rinri-13-015). Written
informed consent documents were provided voluntarily.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
World Health Organization (WHO): Obesity
and Overweight. WHO, Gemeva, 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Accessed June 9, 2021.
|
|
2
|
Livingstone MB and Black AE: Markers of
the validity of reported energy intake. J Nutr. 133 (Suppl
3):895S–920S. 2003.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Trabulsi J and Schoeller DA: Evaluation of
dietary assessment instruments against doubly labeled water, a
biomarker of habitual energy intake. Am J Physiol Endocrinol Metab.
281:E891–E899. 2001.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lichtman SW, Pisarska K, Berman ER,
Pestone M, Dowling H, Offenbacher E, Weisel H, Heshka S, Matthews
DE and Heymsfield SB: Discrepancy between self-reported and actual
caloric intake and exercise in obese subjects. N Engl J Med.
327:1893–1898. 1992.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Buhl KM, Gallagher D, Hoy K, Matthews DE
and Heymsfield SB: Unexplained disturbance in body weight
regulation: Diagnostic outcome assessed by doubly labeled water and
body composition analyses in obese patients reporting low energy
intakes. J Am Diet Assoc. 95:1393–1400; quiz 1401-2.
1995.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Goldberg GR, Black AE, Jebb SA, Cole TJ,
Murgatroyd PR, Coward WA and Prentice AM: Critical evaluation of
energy intake data using fundamental principles of energy
physiology: 1. Derivation of cut-off limits to identify
under-recording. Eur J Clin Nutr. 45:569–581. 1991.PubMed/NCBI
|
|
7
|
Black AE, Goldberg GR, Jebb SA,
Livingstone MB, Cole TJ and Prentice AM: Critical evaluation of
energy intake data using fundamental principles of energy
physiology: 2. Evaluating the results of published surveys. Eur J
Clin Nutr. 45:583–599. 1991.PubMed/NCBI
|
|
8
|
Johansson L, Solvoll K, Bjorneboe GE and
Drevon CA: Under- and overreporting of energy intake related to
weight status and lifestyle in a nationwide sample. Am J Clin Nutr.
68:266–274. 1998.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Rothenbreg E, Bosaeus I and Steen B:
Evaluation of energy intake estimated by a diet history in three
free-living 70 year old populations in Gothenburg, Sweden. Eur J
Clin Nutr. 51:60–66. 1997.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Okubo H, Sasaki S, Hirota N, Notsu A,
Todoriki H, Miura A, Fukui M and Date C: The influence of age and
body mass index on relative accuracy of energy intake among
Japanese adults. Public Health Nutr. 9:651–657. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Murakami K, Livingstone MBE, Okubo H and
Sasaki S: Prevalence and characteristics of misreporting of energy
intake in Japanese adults: The 2012 National Health and Nutrition
Survey. Asia Pac J Clin Nutr. 27:441–450. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Abdul Kadir A, Clarke K and Evans RD:
Cardiac ketone body metabolism. Biochim Biophys Acta Mol Basis Dis.
1866(165739)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Japan Society for the Study of Obesity:
Guidelines for the Management of Obesity Disease. Life Science
Publishing Company, Tokyo, 2016.
|
|
14
|
Yasutake K, Moriguchi R, Kajiyama T,
Miyazaki H, Abe S, Masuda T, Imai K, Iwamoto M, Tsuda H, Obe M, et
al: Interannual study of spot urine-evaluated sodium excretion in
young Japanese women. J Clin Hypertens (Greenwich). 19:653–660.
2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Friedewald WT, Levy RI and Fredrickson DS:
Estimation of the concentration of low-density lipoprotein
cholesterol in plasma, without use of the preparative
ultracentrifuge. Clin Chem. 18:499–502. 1972.PubMed/NCBI
|
|
16
|
Matthews DR, Hosker JP, Rudenski AS,
Naylor BA, Treacher DF and Turner RC: Homeostasis model assessment:
Insulin resistance and beta-cell function from fasting plasma
glucose and insulin concentrations in man. Diabetologia.
28:412–419. 1985.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Laffel L: Ketone bodies: A review of
physiology, pathophysiology and application of monitoring to
diabetes. Diabetes Metab Res Rev. 15:412–426. 1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Mitchell GA, Kassovska-Bratinova S,
Boukaftane Y, Robert MF, Wang SP, Ashmarina L, Lambert M, Lapierre
P and Potier E: Medical aspects of ketone body metabolism. Clin
Invest Med. 18:193–216. 1995.PubMed/NCBI
|
|
19
|
Council for Science and Technology:
Standard Tables of Food Composition in Japan, fifth revised and
enlarged edition 2010. National Printing Bureau, Tokyo, 2010.
|
|
20
|
Council for Science and Technology:
Standard Tables of Food Composition in Japan, 7th revised edition.
National Printing Bureau, Tokyo, 2015.
|
|
21
|
Ganpule AA, Tanaka S, Ishikawa-Takata K
and Tabata I: Interindividual variability in sleeping metabolic
rate in Japanese subjects. Eur J Clin Nutr. 61:1256–1261.
2007.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Miyake R, Tanaka S, Ohkawara K,
Ishikawa-Takata K, Hikihara Y, Taguri E, Kayashita J and Tabata I:
Validity of predictive equations for basal metabolic rate in
Japanese adults. J Nutr Sci Vitaminol. 57:224–232. 2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kagawa M and Hills AP: Preoccupation with
body weight and under-reporting of energy intake in female Japanese
Nutrition Students. Nutrients. 12(830)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Nakayama H, Tokubuchi I, Wada N, Tsuruta
M, Ohki T, Oshige T, Sasaki Y, Iwata S, Kato N, Ohtsuka Y, et al:
Age-related changes in the diurnal variation of ketogenesis in
patients with type 2 diabetes and relevance to hypoglycemic
medications. Endocr J. 62:235–241. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Moore AR, Holland-Winkler AM, Ansley JK,
Boone EDH and Schulte MKO: Reliability and diagnostic performance
of a new blood ketone and glucose meter in humans. J Int Soc Sports
Nut. 18(6)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Briefel RR, McDowell MA, Alaimo K,
Caughman CR, Bischof AL, Carroll MD and Johnson CL: Total energy
intake of the US population: The third National Health and
Nutrition Examination Survey, 1988-1991. Am J Clin Nutr. 62 (Suppl
5):1072S–1080S. 1995.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Fung TT, McCullough ML, Newby PK, Manson
JE, Meigs JB, Rifai N, Willett WC and Hu FB: Diet-quality scores
and plasma concentrations of markers of inflammation and
endothelial dysfunction. Am J Clin Nutr. 82:163–173.
2005.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Braam LA, Ocke MC, Bueno-de-Mesquita HB
and Seidell JC: Determinants of obesity-related underreporting of
energy intake. Am J Epidemiol. 147:1081–1086. 1998.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Johnson RK, Goran MI and Poehlman ET:
Correlates of over- and underreporting of energy intake in healthy
older men and women. Am J Clin Nutr. 59:1286–1290. 1994.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tokudome Y, Imaeda N, Nagaya T, Ikeda M,
Fujiwara N, Sato J, Kuriki K, Kikuchi S, Maki S and Tokudome S:
Daily, weekly, seasonal, within- and between-individual variation
in nutrient intake according to four season consecutive 7 day
weighed diet records in Japanese female dietitians. J Epidemiol.
12:85–92. 2002.PubMed/NCBI View Article : Google Scholar
|