Introduction
Viral myocarditis (VMC), a form of cardiac
inflammation caused by viral infections, is a common and fatal
disease, and one of the leading causes of dilated cardiomyopathy
(DCM) and sudden death, threatening millions of lives worldwide,
especially among children and young patients <40 years of age
(1,2). Enteroviruses have long been
recognized as the major etiological agents of VMC, accounting for
~25% of cases (3) and
coxsackievirus B3 (CVB3) is considered to be a major causative
virus (4). When a virus infects
the heart, it causes direct damage to cardiomyocytes by binding the
coxsackievirus and adenovirus receptor (CAR) and disrupting the
cytoskeleton (5). This also leads
to the activation of the immune system, the recruitment of immune
cells, such as T lymphocytes, and the release of a large number of
inflammatory factors, such as TNF-α, IL-1β and IL-6, which,
together with the virus, aggravate the myocardial injury (6). Although the effectiveness of
treatments for VMC, e.g., treatments targeting specific cytokines,
such as IL-1β, has been demonstrated in clinical experiments and
specific cases, 95% of patients receiving these treatments develop
various degrees of adverse reactions (7,8).
Inhibition of the inflammatory response to VMC is currently a valid
and reliable therapeutic approach (9). However, to the best of our knowledge,
safe and effective drugs to inhibit these inflammatory responses
are currently lacking.
Chinese herbal medicines are a major source of drugs
that can play primary or adjuvant therapeutic roles in a variety of
diseases (10). A previous
pharmacological study demonstrated that matrine can ameliorate
immunoinflammatory activity, and it has been shown to reduce the
levels of TNF-α and IL-1β in a rheumatoid arthritis model through
the NF-κB signaling pathway (11).
Panax quinquefolium saponins have also been shown to present
protective effects on cardiac injury, and improve cardiac fibrosis
and cardiac remodeling in rats with heart failure (12,13).
The main pharmacodynamic agents in Sophora flavescens are
Sophora flavescens alkaloids, while the main pharmacodynamic
agents in Panax quinquefolium are Panax quinquefolium
saponins, which were combined in the present study to investigate
the characteristics of this Chinese herbal medicine. KX, the drug
obtained by combining Sophora flavescens alkaloids and
Panax quinquefolium saponins, was previously shown to
ameliorate cardiac inflammation and myocarditis-induced fibrosis in
mice with autoimmune myocarditis (14). However, its role in the acute
inflammatory phase of VMC remains unclear. Therefore, in the
current study, we hypothesized that KX could ameliorate
CVB3-induced VMC in mice and the underlying mechanism was explored.
The present findings could provide an experimental basis for the
clinical application of KX in patients with VMC.
Materials and methods
Animals and CVB3
A total of 120 male BALB/c mice aged 6-8 weeks
(weight, 18-20 g) were purchased from Changchun Billion Laboratory
Animal Technology Co., Ltd. [license no. SCXK (Liao)-2020-0002].
The mice were housed in an SPF environment at a temperature of
23±2˚C, 60±10% humidity and under a 12-h light/dark cycle. All
animals had free access to food and water. The CVB3 strain was
maintained at the Department of Pathogen Biology, Jilin University
School of Basic Medical Sciences, Changchun, China. The virus was
passaged and propagated in Vero cells; the cells were lysed three
times through freeze-thawing, and their supernatants were harvested
by centrifugation at 200 x g, 4˚C for 5 min and stored at -70˚C
after aliquoting. Virus samples were serially diluted 10-fold. Then
equal volumes of viral fluids were taken to infect Vero cells,
respectively, and the number and proportion of cell wells
exhibiting cytopathic effect were observed for 3-4 days after viral
infection. Each dilution was assayed for its ability to induce
cytopathic changes. The TCID50 of the virus could then be
determined to be 106/ml by statistical analysis. The
present study was approved by the Animal Ethics Committee of Jilin
Academy of TCM (approval no. JLSZ KYDWLL2021-003; Changchun,
China).
Composition, ratio and concentration
selection of KX
Sophora flavescens alkaloids, consisting of
matrine (C15H24N2O) and oxymatrine
(C15H24N2O2) in a 1:1 ratio, were
pure (HPLC purity, ≥98%). Panax quinquefolium saponins
consisted of ginsenoside Rg1
(C42H72O14), ginsenoside Re
(C48H82O18) and ginsenoside Rb1
(C54H92O23), and their purity was
determined to be ≥70% by high-performance liquid chromatography.
These drugs were obtained from the new drug center of the Jilin
Academy of TCM. The optimal total matrine to total saponin ratio
from American ginseng was 1.1:1, as determined using an
experimental model of autoimmune myocarditis and the optimal
concentrations corresponding to high and low doses of KX were 275
and 138 mg/kg, respectively (14).
VMC induction and KX treatment
After 5 days of adaptive feeding, BALB/c mice were
randomly divided into the following groups based on body weight (30
mice/group): i) Control; ii) VMC; iii) KX-high (275 mg/kg); and iv)
KX-low (138 mg/kg). The specific grouping method is as follows:
Mice were sequentially arranged in cages according to body weight,
with the first round starting from the cage with the highest body
weight and ending with the cage with the lowest body weight or vice
versa. In the second round, the arrangement started from the second
cage until the last cage, with the first cage containing two mice.
In the third round, the arrangement started from the third cage
until the last cage, with the first two cages supplemented with
three mice. For the fourth round, the arrangement started from the
fourth cage until the last cage, with the first three cages
supplemented with four mice. This process was repeated starting
from the first cage until all the mice were separated into cages
with homogeneous body weights. All mice, except for those in the
control group, received intraperitoneal injections of 0.1 ml CVB3
virus with a TCID50 of 100, and KX or purified water 2 h
later.
High- and low-dose KX solutions were prepared by
dissolving 275 or 138 mg KX, respectively, in 10 ml distilled
water. Mice in the KX-high and KX-low groups were intragastrically
fed the experimental drug by gavage (10 ml/kg) daily from day 0
until sacrifice (day 7 or 21). Mice in the control and VMC groups
received an equal volume of distilled water. All animals were
anesthetized by intraperitoneal injection of sodium pentobarbital
(50 mg/kg) and then euthanized by cervical dislocation. Mice (a
total of 3 mice) that exhibited self-injuring behavior and
nonhealing wounds were anesthetized by intraperitoneal injection of
pentobarbital sodium (50 mg/kg), and then euthanasia was performed
through cervical dislocation. Death was confirmed by the absence of
breathing and heartbeat.
Histopathology
Mice were euthanized after 7 (40 mice; 10
mice/group) or 21 (40 mice; 10 mice/group) days and their body
weight (BW) and heart weight (HW) were measured to calculate the
cardiac index (HW/BW). The heart tissues were fixed in 15% formalin
at 23±2˚C for >48 h, embedded in paraffin and sectioned into
transverse sections (5 µm). Sections were stained with hematoxylin
and eosin (H&E) at 23±2˚C for 5-20 min. The H&E-stained
myocardial tissue sections were examined under a light microscope
at x400 magnification and the macroscopic score was measured using
the following five-point scale: 0, no inflammation; 1, limited
discoloration; 2, numerous small lesions; 3, diffused discoloration
not exceeding one-third of the heart surface; and 4, diffused
discoloration exceeding one-third of the heart surface (15).
Cytokine ELISA
After anesthetizing the mice, blood was collected
from the abdominal aorta. The whole blood was allowed to stand for
1 h at 23±2˚C, followed by centrifugation at 4˚C, 200 x g for 10
min, and then serum was obtained. Serum levels of creatine
kinase-myocardial band (CK-MB), lactate dehydrogenase (LDH),
cardiac troponin I (cTn-I), and the inflammatory markers IL-1β,
IL-6, TNF-α and high-sensitive C-reactive protein (hs-CRP), were
measured using the following mouse ELISA kits: (CK-MB; cat. no.
YX-031115M; LDH; cat. no.YX-120408M; cTn-I; cat. no. YX-201409M;
IL-1β; cat. no. YX-091203M; IL-6; cat. no. YX-091206M; TNF-α; cat
no. YX-201407M; hs-CRP; cat. no. YX-081903M; all from SINOBESTBIO,
Co., Ltd.). Standards (50 µl) were added into predefined wells of
the microplates. Samples (10 µl serum) and sample diluent (40 µl)
were added to the testing sample wells, while the blank wells were
left empty. In the wells for standards and samples, horseradish
peroxidase-labeled conjugates (100 µl) were added before sealing
the plates for incubation at 37˚C for 60 min. After washing the
plates five times, substrates A (50 µl) and B (50 µl) were added to
each well. After incubation at 37˚C for 15 min, a stop solution (50
µl) was added to each well, and the absorbance of each well was
measured at 450 nm within 15 min (cat. no. ELx800; BioTek
Instruments, Inc.).
Reverse transcription-quantitative
(RT-q)PCR
An appropriate amount of RNAiso plus (Takara Bio,
Inc.) was added to the myocardial tissue and allowed to stand for 5
min at a temperature of 23±2˚C. Subsequently, RNAiso plus and
one-fifth volume of chloroform were added and the solution was
centrifuged at 12,000 x g for 15 min at 4˚C. The supernatant was
then collected and pipetted into a new centrifuge tube. RNAiso plus
and an equal volume of isopropanol were added and allowed to stand
for 10 min at room temperature; thereafter, the solution was
centrifuged at 12,000 x g for 10 min at 4˚C. The supernatant was
removed and an equal volume of 75% ethanol to RNAiso plus was
added. The supernatant was carefully discarded after centrifugation
at 7,500 x g for 5 min at 4˚C and the samples were stored after
drying. The RNA was then reverse-transcribed into cDNA with the RT
Kit (GoScript™ Reverse Transcription; cat. no. A5001;
Promega Corporation), which was amplified via qPCR
(SystemGoTaq® qPCR Master Mix; cat. no. A6001; Promega,
Inc.). qPCR was performed using the following thermocycling
conditions: Initial denaturation at 95˚C for 10 min, followed by 40
cycles of 95˚C for 15 sec and 60˚C for 60 sec. The
2-ΔΔCq method was used to calculate the relative content
of mRNA using GAPDH as the internal reference gene (16). The following primer sequences were
used for qPCR: IκBα forward, 5'-ATCCTGACCTGGTTTCGCTC-3' and
reverse, 5'-TGGTAGGGGGAGTAGCCTTG-3'; NF-κB P65 forward,
5'-CCTCTGGCGAATGGCTTTAC-3' and reverse, 5'-TGCTTCGGCTGTTCGATGAT-3';
GAPDH forward 5'-TGGTGAAGGTCGGTGTGAAC-3', and reverse
5'-ACTGTGCCGTTGAATTTGCC-3'.
Western blotting
An appropriate amount of mouse myocardial tissue was
weighed and added to the RIPA lysis buffer (cat. no. CW2333S; CoWin
Biosciences) containing protease and phosphatase inhibitors in a
1:9 ratio. This was ground using a high-speed tissue grinder for 2
min, left to stand on ice for 20 min, centrifuged at 14,000 x g at
4˚C for 10 min and the supernatant stored in a -80˚C freezer. The
total protein concentration in the sample was measured according to
the instructions of the BCA protein concentration assay kit
(cat.no. P0012S, Beyotime Biotechnology, shanghai, china). Samples
containing 50 µg total protein were added to each lane to perform
electrophoresis. Proteins were separated by SDS-PAGE on a 10% gel
and transferred onto nitrocellulose membranes. After blocking in 5%
non-fat milk diluted in TBS-0.1% Tween-20 (CoWin Biosciences) in
the dark at 4˚C overnight, the membranes were incubated with
primary antibodies (Santa Cruz Biotechnology, Inc.) against
TGF-β-activated kinase 1 (TAK1)-binding protein 1 (TAB1; 1:100;
cat. no. sc-166138), NF-κB (1:200; cat. no. sc-8008),
phosphorylated (p)-NF-κB (1:200; cat. no. sc-136548), IκB (1:100;
cat. no. sc-74451), p-IκB (1:200; cat. no. sc-390622) or GAPDH
(1:100; cat. no. sc-365062) for 2 h at 37˚C. Subsequently, the
membranes were washed with TBS-0.1% Tween 20 and incubated with a
secondary HRP-conjugated antibody m-IgGκ (1:1,000; cat. no.
sc-516102) or m-IgG-Fc (1:1,000; cat. no. sc-525409; both from
Santa Cruz Biotechnology, Inc.) for 1.5 h at 37˚C. The membranes
were then washed again and visualized using an enhanced
chemiluminescence detection kit (cat. no. CW0049M, CoWin
Biosciences). The levels of target proteins were normalized to
those of GAPDH using a gel imaging system (ChemiDoc-It 510 Imager;
Ultra-Violet Products, Ltd.). Protein bands were analyzed using
ImageJ software (version 1.5.1; National Institutes of Health).
Statistical analysis
GraphPad Prism software (version 9.0 for Mac;
GraphPad Software; Dotmatics) was used to perform the statistical
analysis. Survival analysis was performed using Kaplan-Meier
analysis followed by the Log-rank test. When two variables were
being assessed, a two-way ANOVA with Bonferroni post hoc test was
performed, while other comparisons were performed using one-way
ANOVA followed by Tukey's post hoc test or Kruskal-Wallis test
followed by Dunn's post hoc test. The macroscopic scores were
presented as median ± interquartile range, while all other values
were presented as mean ± standard deviation. P<0.05 was
considered to indicate a statistically significant difference.
Results
Effects of KX on mouse survival and
cardiac index
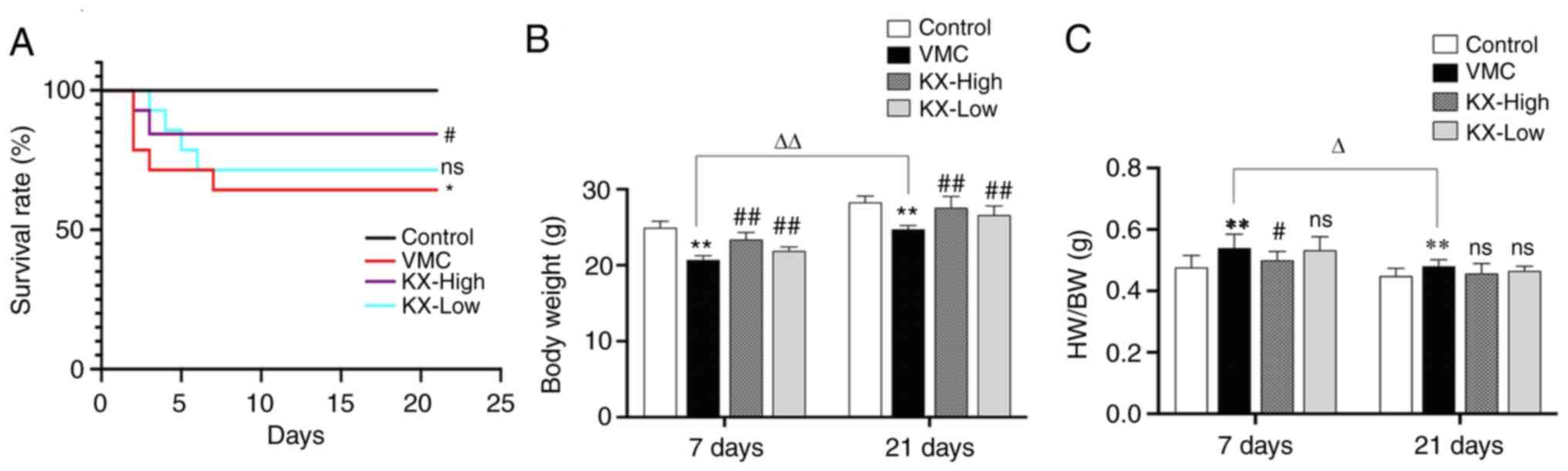
All mice developed symptoms such as apathy,
decreased activity, clumping, eating less and dull fur starting 2-3
days after virus injection and some of the mice developed
piloerection, which was progressively aggravated. The survival of
mice in the VMC group was significantly lower compared with that in
the control group (P<0.05; Fig.
1A); however, high-dose KX treatment significantly improved the
survival of mice in comparison with that in the VMC group
(P<0.05), while low-dose KX treatment had no significant effect
(P>0.05) (Fig. 1A). After 7
days, mice in the VMC group weighed significantly less than those
in the control group (P<0.01; Fig.
1B). In comparison with mice in the VMC group, mice that
received KX showed a significant increase in weight (P<0.01;
Fig. 1B). In comparison with that
in the VMC group, the high-dose KX group showed a significant
reduction in the cardiac index (P<0.05; Fig. 1C); however, the low-dose KX group
showed no significant changes in cardiac index (P>0.05; Fig. 1C).
After 21 days, mice in the VMC group weighed
significantly less compared with those in the control group
(P<0.01), while mice in the KX intervention groups showed a
significant increase in weight (P<0.01) (Fig. 1B). HW/BW in the VMC group was
significantly higher than that in the control group (P<0.01;
Fig. 1C); however, in comparison
with the VMC group, the KX intervention groups did not show
significant changes in HW/BW (P>0.05) (Fig. 1C). In comparison with the VMC mice
euthanized at 7 days, the VMC mice euthanized at 21 days showed
greater weight gain (P<0.05; Fig.
1A and B) and a lower HW/BW
(P<0.05; Fig. 1C).
Effects of KX on myocardial injury in
mice
After 7 days, the serum levels of LDH, CK-MB and
cTn-I were significantly increased in the VMC group compared with
those in the control group (P<0.01; Fig. 2A-C). In comparison with the VMC
group, the KX intervention groups showed significant reductions in
the serum levels of the aforementioned indicators (P<0.01;
Fig. 2A-C). H&E staining of
cardiac tissue showed significant inflammatory cell infiltration
and damage to cardiac tissue in the VMC group on day 7 (P<0.01),
while the inflammatory damage was significantly reduced after
KX-high-dose intervention (P<0.05; Fig. 2G).
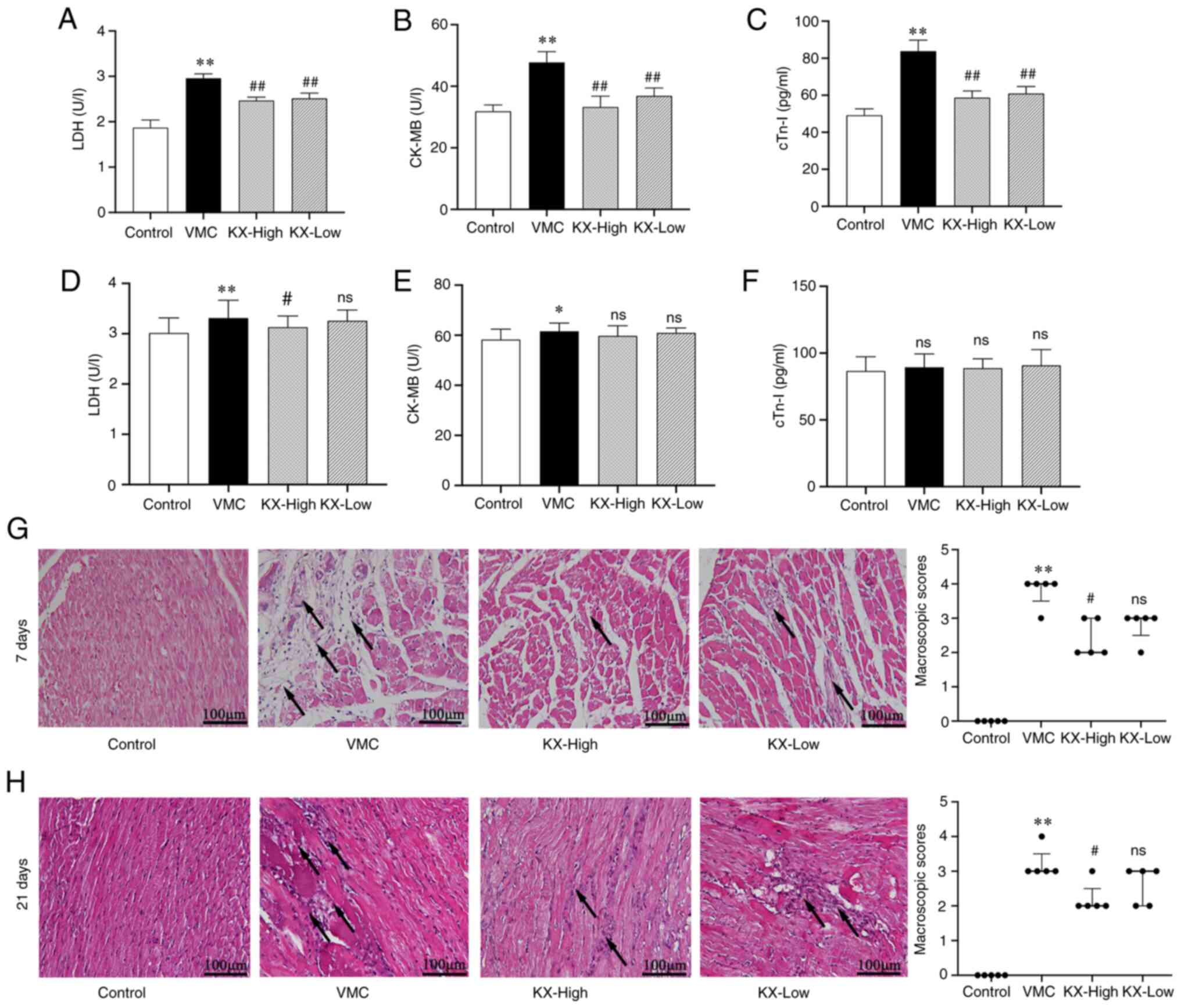 | Figure 2Effects of KX on myocardial injury in
mice with VMC. Changes in the serum levels of (A) LDH, (B) CK-MB
and (C) CTn-I after 7 days of KX treatment (Dunn's post hoc test).
Changes in the serum levels of (D) LDH, (E) CK-MB, and (F) cTn-I
after 21 days of KX treatment (One-way ANOVA and Tukey's post hoc
test). (G and H) Hematoxylin and eosin staining of the myocardium
(One-way ANOVA and Dunn's post-hoc test; n=5/group). Scale bars,
100 µm. Arrows indicate inflammatory cell infiltration (mainly
lymphocytes) and myocardial injury. Quantified data plots are shown
(macroscopic scores were compared among the groups).
*P<0.05 and **P<0.01 vs. control;
nsP>0.05, #P<0.05 and
##P<0.01 vs. VMC. KX, combination of Sophora
flavescens alkaloids and Panax quinquefolium saponins;
LDH, lactate dehydrogenase; CK-MB, creatine kinase-myocardial band;
cTn-I, cardiac troponin I; VMC, viral myocarditis; ns, not
significant. |
After 21 days, the serum CK-MB and LDH levels in the
VMC mice were significantly higher than those in the controls
(P<0.01 or P<0.05; Fig. 2D
and E). In comparison with the VMC
group, the KX-high-dose group showed a significantly lower LDH
level (P<0.05), while the KX-low-dose group showed no
significant change (P>0.05; Fig.
2D). Besides, KX had no significant effect on CK-MB (P>0.05;
Fig. 2E). cTn-I expression did not
differ significantly between the VMC and control groups (P>0.05;
Fig. 2F). H&E staining of
myocardial tissue showed inflammatory cell infiltration in the VMC
group at 21 days, but myocardial tissue damage and inflammation
were significantly reduced after KX-high-dose intervention in
comparison with the VMC group (P<0.05; Fig. 2H).
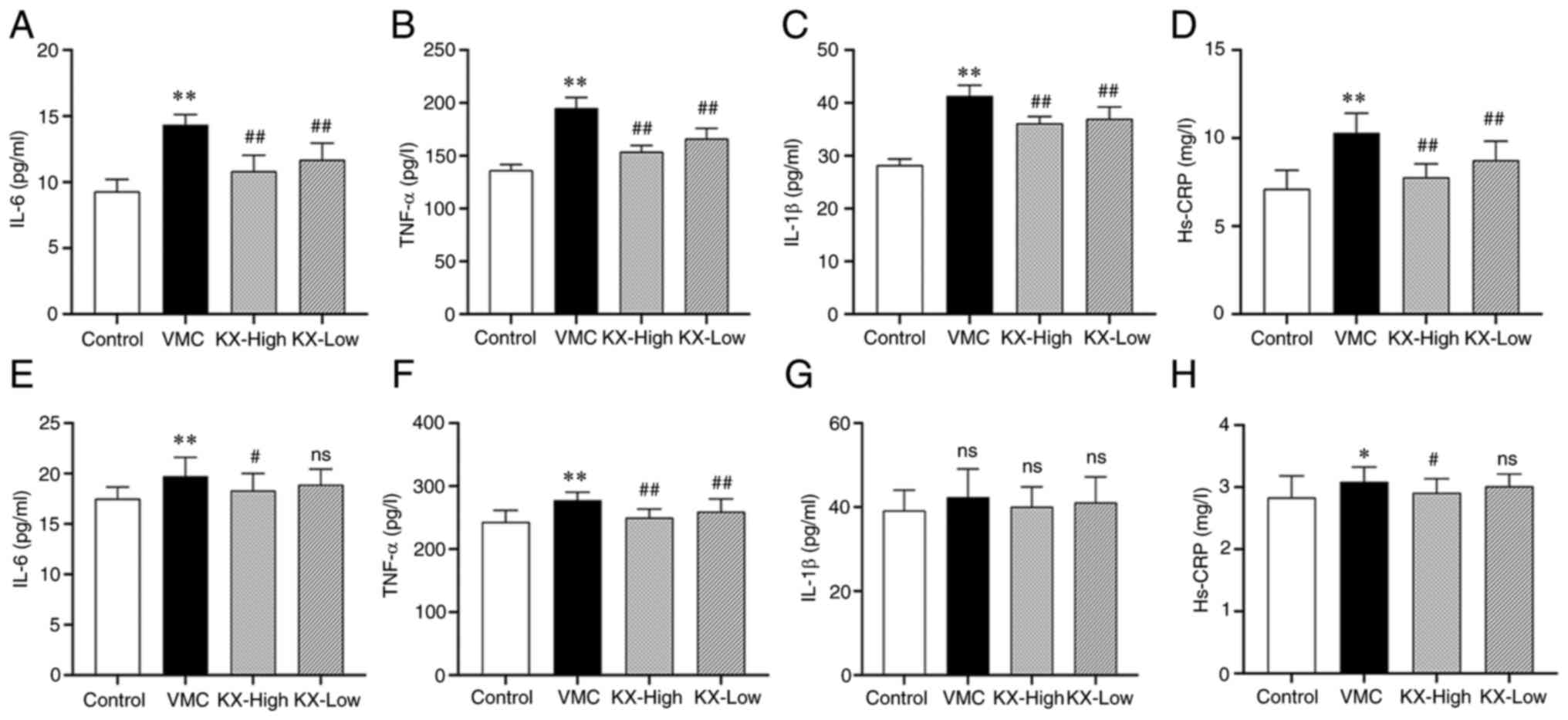
Effects of KX on inflammatory factors
in mouse serum
After 7 days, the levels of IL-6, IL-1β, TNF-α and
hs-CRP were significantly increased in the VMC group compared with
those in the control group (P<0.01; Fig. 3A-D). However, in comparison with
the VMC group, the KX intervention groups showed a significant
decrease in the levels of IL-6, IL-1β, TNF-α and hs-CRP (P<0.01;
Fig. 3A-D) with a dose-effect
relationship.
After 21 days, the levels of IL-6, TNF-α and hs-CRP
were significantly increased in the VMC group compared with those
in the control group (P<0.01 or P<0.05; Fig. 3E, F and H),
whereas IL-1β levels did not change significantly (P>0.05;
Fig. 3G). In comparison with the
VMC group, the high-dose KX group showed significantly lower levels
of IL-6, TNF-α and hs-CRP (P<0.01 or P<0.05; Fig. 3E, F and H),
while the low-dose KX group showed significantly decreased TNF-α
levels (P<0.01) but no significant changes in the IL-6, hs-CRP
and IL-1β levels (P>0.05) (Fig.
3E-H).
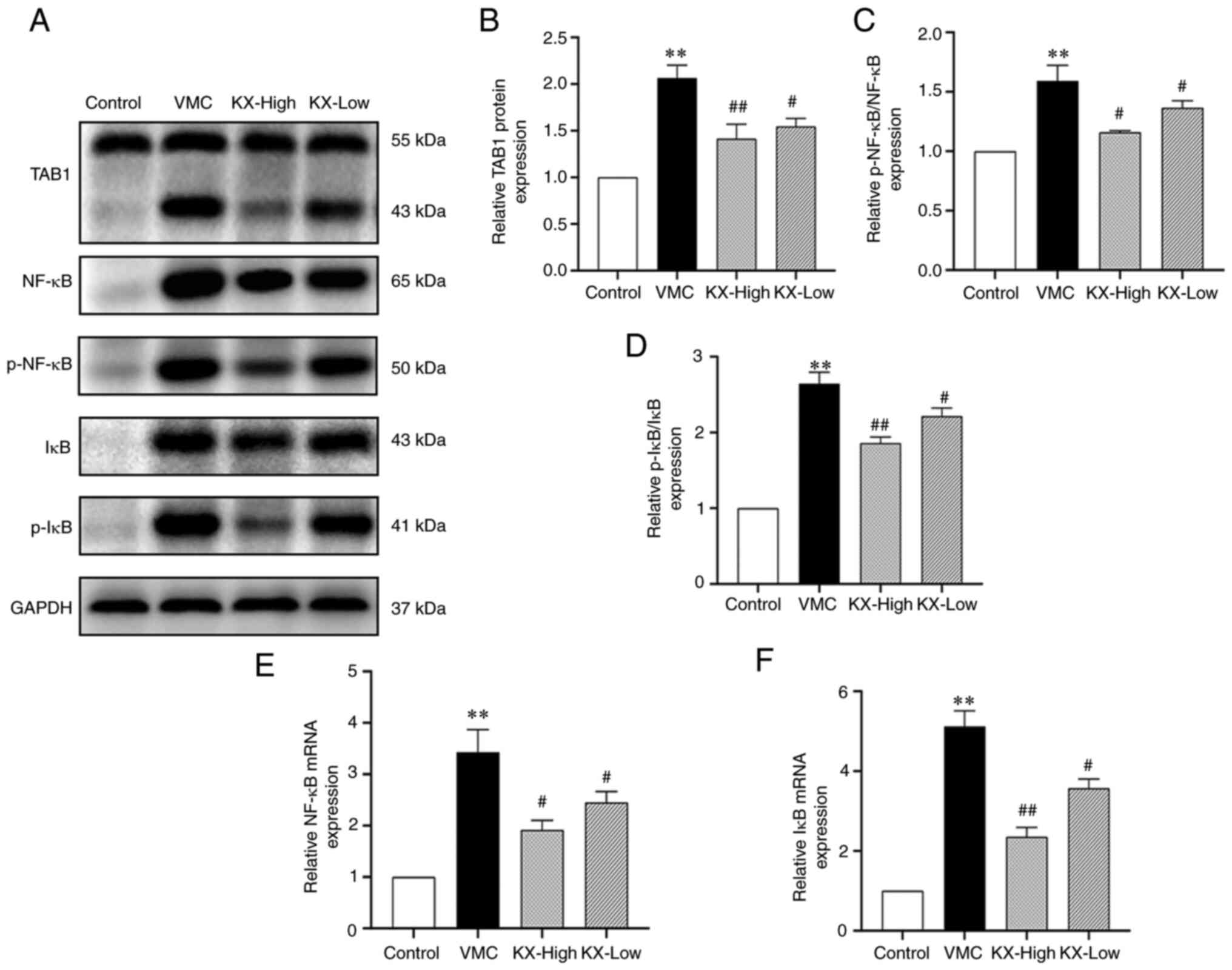
Effects of KX on the NF-κB pathway in
mouse myocardium
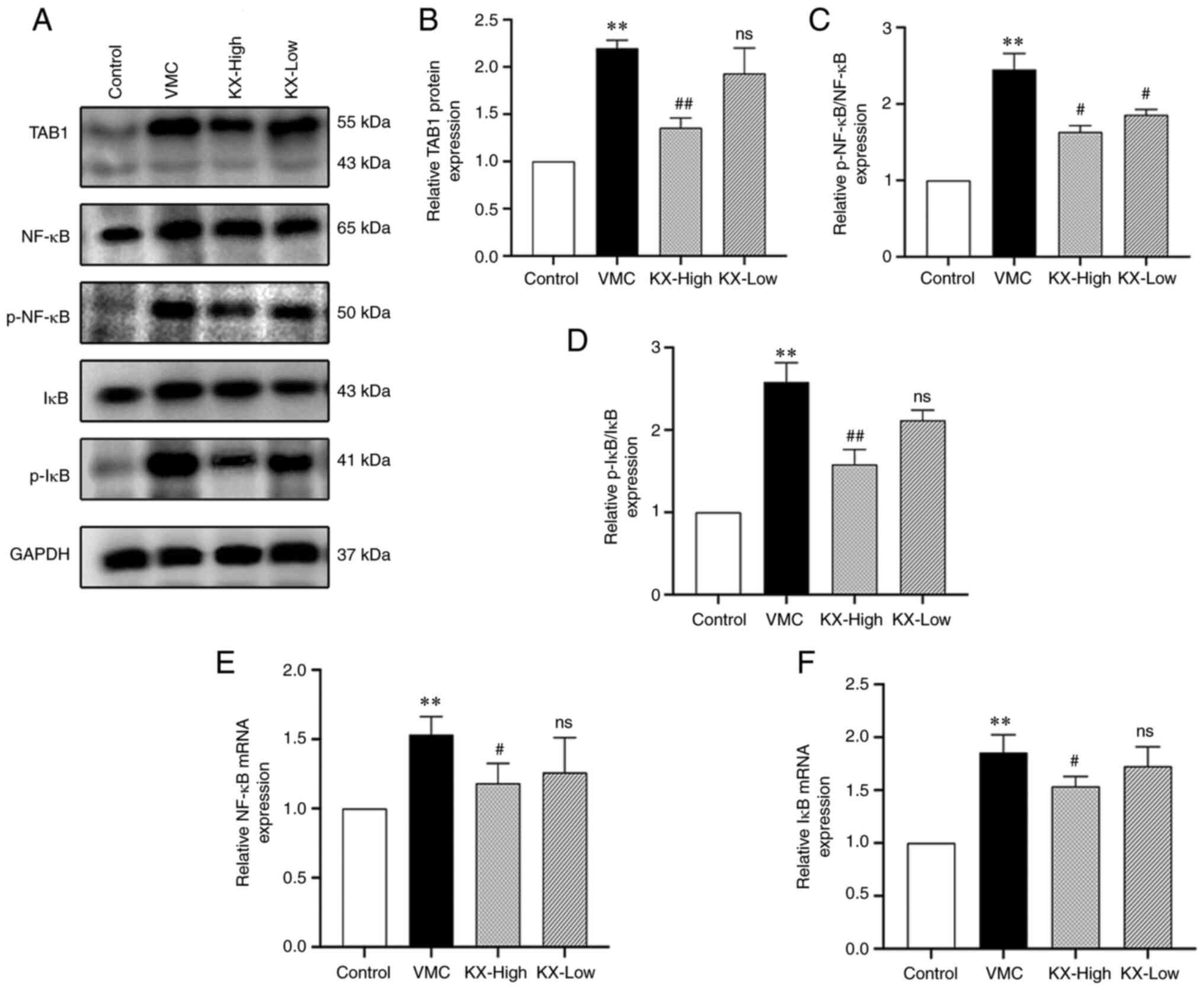
After 7 days, the protein expression levels of TAB1,
p-IκB/IκB and p-NF-κB/NF-κB in the myocardium of mice in the VMC
group were significantly increased compared with those in the
control group (P<0.01; Fig.
4A-D). KX intervention resulted in a significant decrease in
the myocardial levels of all of the aforementioned indicators
(P<0.01 or P<0.05; Fig.
4A-D) and the results showed a dose-dependent pattern. The mRNA
expression levels of NF-κB and IκB in the mouse myocardium were
significantly increased in the VMC group compared with those in the
control group (P<0.01) and their expression levels were
significantly decreased after KX intervention (P<0.01 or
P<0.05) (Fig. 4E and F), with the reduction showing a
dose-effect relationship.
After 21 days, the myocardial protein expression
levels of TAB1, p-IκB/IκB and p-NF-κB/NF-κB in the VMC group were
significantly increased compared with those in the control group
(P<0.01; Fig. 5A-D).
Nonetheless, the myocardial levels of all of the aforementioned
indicators were significantly decreased after high-dose KX
treatment (P<0.01 or P<0.05; Fig. 5A-D); by contrast, low-dose KX
treatment decreased the levels of p-NF-κB/NF-κB (P<0.05;
Fig. 5C), but had no significant
effect on TAB1 and p-IκB/IκB expression (P>0.05; Fig. 5B and D). Similarly, the mRNA expression levels
of NF-κB and IκB in the myocardium of the mice in the VMC group
were significantly increased compared with those in the control
group (P<0.01), whereas they were significantly reduced
(P<0.01 or P<0.05) after high-dose KX intervention but were
not affected by low-dose KX intervention (P>0.05) (Fig. 5E and F).
 | Figure 5Effects of KX on the NF-κB pathway in
mouse myocardium. (A) TAB1, NF-κB, p-NF-κB, IκB and p-IκB protein
expression levels in the murine myocardium after 21 days of KX
treatment. Western blot semi-quantification analysis (n=4/group) of
(B) TAB1, (C) p-NF-κB/NF-κB and (D) p-IκB/-IκB protein expression.
Expression of (E) NF-κB and (F) IκB mRNA in the mouse myocardium
after 21 days of KX treatment. One-way ANOVA and Dunn's post hoc
test comparisons, **P<0.01 vs. control;
nsP>0.05, #P<0.05 and
##P<0.01vs. VMC. TAB1, TGF-β-activated kinase
1-binding protein 1; VMC, viral myocarditis; KX, combination of
Sophora flavescens alkaloids and Panax quinquefolium
saponins; p-, phosphorylated. |
Discussion
VMC is characterized by an acute onset, and complex
and no specificity symptoms such as asthenia and shortness of
breath (17). According to the TCM
theory of treatment, the combination of Sophora flavescens
alkaloids and Panax quinquefolium saponins shows good
curative effects in the treatment of VMC, which displays the
characteristic of TCM, including synergistic effects and advantages
of drug combinations (14). KX has
recently been shown to be effective in alleviating chronic
inflammation and the degree of myocardial fibrosis in myocarditis
(14,18). To clarify whether the impact of KX
treatment on VMC extends throughout the entire pathological
development process, the present study established a CVB3-induced
acute VMC model and explored the effect of KX on acute inflammation
in VMC. The results showed that KX attenuated VMC-related injury
and inflammation levels possibly through the NF-κB pathway.
The CVB3-induced murine VMC model is commonly used
to study the reaction phase of acute inflammation in VMC (19). Viral infection of the heart results
in a series of pathological responses, which are mainly divided
into three phases: An acute inflammatory phase (1-7 days), a
subacute inflammatory phase (7-21 days) and a chronic inflammatory
phase (after ~21 days) (6,20). In the acute phase, CVB3 enters the
myocardium with the aid of a CAR, which damages cardiomyocytes
(21), and the host immune
response is subsequently induced. It has been shown that the
inflammatory response leads to the transmigration of macrophages, T
lymphocytes and natural killer cells to the site of injury, and the
production of high levels of proinflammatory factors, such as IL-6,
IL-1β and TNF-α. Together with the virus, these proinflammatory
factors further aggravate cardiac damage through the cleavage of
dystrophin by enteroviral protease 2A (22). In the subacute phase, viral
replication and myocardial inflammation are reduced under the
regulation of the autoimmune system (23); however, persistent myocardial
inflammation can lead to fibrosis and DCM (24,25).
Therefore, inhibition of myocardial inflammatory responses in the
acute and subacute phases is an important step in treating VMC.
Inhibition of TNF-α, IL-6 and IL-1β secretion was recently shown to
effectively attenuate myocardial inflammatory injury (26,27).
Simultaneous neutralization of TNF-α or IL-1β by antibodies or
soluble receptors could attenuate the inflammatory response in VMC
(28,29). In the present study, all mice
developed symptoms such as apathy, decreased activity, clumping,
eating less and dull fur starting 2-3 days after virus injection
and some of the mice developed piloerection, which was
progressively aggravated. Nonetheless, all the symptoms improved
significantly after KX treatment. Nearly all mice injected with the
virus were affected by VMC. In addition, significant myocardial
inflammation and damage appeared in the mice after 7 days and some
of the inflammation and damage persisted until day 21 under the
regulation of the autoimmune system, which is consistent with the
findings of a recent study (30).
After the treatment of mice in the VMC group with KX, the levels of
TNF-α, IL-6, IL-1β and hs-CRP were decreased in a dose-dependent
manner, which played an important role in attenuating myocardial
injury.
The NF-κB pathway is a classical proinflammatory
signaling pathway mainly based on the role of NF-κB in the
expression of proinflammatory genes, including cytokines,
chemokines and adhesion molecules (31). TAB1 is a protein activator of TAK1,
and the TAB1-TAK1 complex phosphorylates the IκB kinase complex,
which then induces phosphorylation of Ser32 and Ser36 residues in
IκB, leading to its degradation and the activation of NF-κB
(32). IL-1β, TNF-α and IL-6
overexpression can activate NF-κB via the TAB1 pathway. As a
transcription factor, the activated NF-κB translocates into the
nucleus to promote inflammation or the expression of inflammatory
cytokines (33), leading to a
cascade amplification of inflammatory cytokines and further
resulting in persistent necrosis of cardiomyocytes and infiltration
of inflammatory cells. Therefore, the TAB1/NF-κB pathway plays a
key role in regulating inflammation, and inhibition of TAB1 and
activation of the NF-κB pathway are effective in attenuating
inflammation in the myocardium (26,34-36).
Several studies have shown that Momordica charantia can act
through NF-κB signaling pathways to reduce the level of
inflammation in rheumatoid arthritis or models (11,37).
In the present study, KX intervention in VMC mice attenuated
myocardial injury in a dose-dependent manner and decreased TAB1
expression as well as the NF-κB pathway-related mRNA and protein
expression levels. Thus, the KX formula may act through the
TAB1/NF-κB pathway to reduce the level of inflammation and thereby
ameliorate myocardial injury.
The present findings indicated that KX could
effectively attenuate the inflammatory response in the acute and
subacute phases of VMC, thereby providing an experimental basis for
the clinical application of KX and indicating its effectiveness in
reducing the clinical symptoms of acute VMC. However, the present
study presented some limitations. The current study lacked a
positive control group. Although Astragalus membranaceus and
ribavirin were selected as positive drugs for VMC (38,39),
their effectiveness remains unclear, especially in the subacute
stage of VMC. Moreover, findings based on echocardiography, which
is critical for cardiac function assessment in mice, were not
obtained. Furthermore, it was difficult to identify which component
of KX was involved in inflammation at different stages of VMC. In
future work, the five components in KX could be isolated to perform
experiments in VMC mice at different stages to identify which of
them exert anti-inflammatory effects. Moreover, more accurate
experiments could be performed to determine inflammation and
protein expression localization of myocardium and determine if
there is any difference between the right and left ventricles in
the H&E staining or immunohistochemical methods.
Nevertheless, the present study suggested that KX
could act through the TAB1/NF-κB pathway to decrease the
inflammatory response in the acute and subacute phases of
CVB3-induced VMC and thereby alleviate pathological damage. These
findings partly embody the mechanism of action of KX in treating
VMC with multiple components and targets and represent the
synergistic effects and advantages of drug combinations of TCM
formulas in treating VMC.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Jilin Science
and Technology Development Plan Project (grant no.
20200403128SF).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TD made substantial contributions to the conception
and design of the study. ML and TD were responsible for the
experimental procedures, data acquisition, analysis and
interpretation, and confirmed the authenticity of all the raw data.
ML performed the drafting of the article and critically revised it
for important intellectual content.
were responsible for participating in the
experiments and confirm the authenticity of all the raw data. All
authors read and approved the final manuscript. All authors agree
to be accountable for all aspects of the work in ensuring that
questions related to the accuracy or integrity of the work are
appropriately investigated and resolved.
Ethics approval and consent to
participate
All experiments and animal care procedures were
approved by the Animal Ethics Committee of Jilin Academy of
Traditional Chinese Medicine (approval no. JLSZKYDWLL2021-003).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Putschoegl A and Auerbach S: Diagnosis,
evaluation, and treatment of myocarditis in children. Pediatr Clin
North Am. 67:855–874. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Doolan A, Langlois N and Semsarian C:
Causes of sudden cardiac death in young Australians. Med J Aust.
180:110–112. 2004.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Fairley CK, Ryan M, Wall PG and Weinberg
J: The organisms reported to cause infective myocarditis and
pericarditis in England and Wales. J Infect. 32:223–225.
1996.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Woodruff JF: Viral myocarditis. A review.
Am J Pathol. 101:425–484. 1980.PubMed/NCBI
|
|
5
|
He Y, Chipman PR, Howitt J, Bator CM,
Whitt MA, Baker TS, Kuhn RJ, Anderson CW, Freimuth P and Rossmann
MG: Interaction of coxsackievirus B3 with the full length
coxsackievirus-adenovirus receptor. Nat Struct Biol. 8:874–878.
2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pollack A, Kontorovich AR, Fuster V and
Dec GW: Viral myocarditis-diagnosis, treatment options, and current
controversies. Nat Rev Cardiol. 12:670–680. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Brucato A, Imazio M, Gattorno M, Lazaros
G, Maestroni S, Carraro M, Finetti M, Cumetti D, Carobbio A,
Ruperto N, et al: Effect of anakinra on recurrent pericarditis
among patients with colchicine resistance and corticosteroid
dependence: The AIRTRIP randomized clinical trial. JAMA.
316:1906–1912. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Scott IC, Hajela V, Hawkins PN and
Lachmann HJ: A case series and systematic literature review of
anakinra and immunosuppression in idiopathic recurrent
pericarditis. J Cardiol Cases. 4:e93–e97. 2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Tschöpe C, Ammirati E, Bozkurt B, Caforio
ALP, Cooper LT, Felix SB, Hare JM, Heidecker B, Heymans S, Hübner
N, et al: Myocarditis and inflammatory cardiomyopathy: Current
evidence and future directions. Nat Rev Cardiol. 18:169–193.
2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Li FS and Weng JK: Demystifying
traditional herbal medicine with modern approach. Nat Plants.
3(17109)2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Niu Y, Dong Q and Li R: Matrine regulates
Th1/Th2 cytokine responses in rheumatoid arthritis by attenuating
the NF-κB signaling. Cell Biol Int. 41:611–621. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zheng X, Wang S, Zou X, Jing Y, Yang R, Li
S and Wang F: Ginsenoside Rb1 improves cardiac function and
remodeling in heart failure. Exp Anim. 66:217–228. 2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Wang QW, Yu XF, Xu HL, Zhao XZ and Sui DY:
Ginsenoside re improves isoproterenol-induced myocardial fibrosis
and heart failure in rats. Evid Based Complement Alternat Med.
2019(3714508)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Liu M, Lin Y, Xu H, Li L and Ding T:
Combination of Sophora flavescens alkaloids and Panax
quinquefolium saponins modulates different stages of
experimental autoimmune myocarditis via the NF-κB and TGF-β1
pathways. Exp Ther Med. 24(570)2022.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Aretz HT: Myocarditis: The dallas
criteria. Hum Pathol. 18:619–624. 1987.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Sinagra G, Anzini M, Pereira NL, Bussani
R, Finocchiaro G, Bartunek J and Merlo M: Myocarditis in clinical
practice. Mayo Clin Proc. 91:1256–1266. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Liu M, Lin Y, Xu H, Wang X, Liu B, Fan M,
Ding T and Li L: Mechanism of the combination of KuShen and
XiYangShen on myocarditis based on network pharmacology and animal
experiments. Pharmacol Res-Mod Chin Med. 4(100141)2022.
|
|
19
|
Błyszczuk P: Myocarditis in humans and in
experimental animal models. Front Cardiovasc Med.
6(64)2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lasrado N and Reddy J: An overview of the
immune mechanisms of viral myocarditis. Rev Med Virol. 30:1–14.
2020.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Kandolf R, Ameis D, Kirschner P, Canu A
and Hofschneider PH: In situ detection of enteroviral genomes in
myocardial cells by nucleic acid hybridization: An approach to the
diagnosis of viral heart disease. Proc Natl Acad Sci USA.
84:6272–6276. 1987.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Badorff C, Lee GH, Lamphear BJ, Martone
ME, Campbell KP, Rhoads RE and Knowlton KU: Enteroviral protease 2A
cleaves dystrophin: Evidence of cytoskeletal disruption in an
acquired cardiomyopathy. Nat Med. 5:320–326. 1999.PubMed/NCBI View
Article : Google Scholar
|
|
23
|
Huber SA, Sartini D and Exley M:
Vgamma4(+) T cells promote autoimmune CD8(+) cytolytic T-lymphocyte
activation in coxsackievirus B3-induced myocarditis in mice: Role
for CD4(+) Th1 cells. J Virol. 76:10785–10790. 2002.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Izumi T, Takehana H, Matsuda C, Yokoyama
H, Kohno K, Suzuki K and Inomata T: Experimental autoimmune
myocarditis and its pathomechanism. Herz. 25:274–278.
2000.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Esfandiarei M and McManus BM: Molecular
biology and pathogenesis of viral myocarditis. Annu Rev Pathol.
3:127–155. 2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Liu T, Zhang M, Niu H, Liu J, Ruilian M,
Wang Y, Xiao Y, Xiao Z, Sun J, Dong Y and Liu X: Astragalus
polysaccharide from Astragalus Melittin ameliorates inflammation
via suppressing the activation of TLR-4/NF-κB p65 signal pathway
and protects mice from CVB3-induced virus myocarditis. Int J Biol
Macromol. 126:179–186. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Gu X, Li Y, Chen K, Wang X, Wang Z, Lian
H, Lin Y, Rong X, Chu M, Lin J and Guo X: Exosomes derived from
umbilical cord mesenchymal stem cells alleviate viral myocarditis
through activating AMPK/mTOR-mediated autophagy flux pathway. J
Cell Mol Med. 24:7515–7530. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kubota T, Bounoutas GS, Miyagishima M,
Kadokami T, Sanders VJ, Bruton C, Robbins PD, McTiernan CF and
Feldman AM: Soluble tumor necrosis factor receptor abrogates
myocardial inflammation but not hypertrophy in cytokine-induced
cardiomyopathy. Circulation. 101:2518–2525. 2000.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kraft L, Erdenesukh T, Sauter M, Tschöpe C
and Klingel K: Blocking the IL-1β signalling pathway prevents
chronic viral myocarditis and cardiac remodeling. Basic Res
Cardiol. 114(11)2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Yue-Chun L, Gu XH, Li-Sha G, Zhou DP, Xing
C, Guo XL, Pan LL, Song SY, Yu LL, Chen GY, et al: Vagus nerve
plays a pivotal role in CD4+ T cell differentiation during
CVB3-induced murine acute myocarditis. Virulence. 12:360–376.
2021.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sen R and Baltimore D: Multiple nuclear
factors interact with the immunoglobulin enhancer sequences. Cell.
46:705–716. 1986.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Shim JH, Xiao C, Paschal AE, Bailey ST,
Rao P, Hayden MS, Lee KY, Bussey C, Steckel M, Tanaka N, et al:
TAK1, but not TAB1 or TAB2, plays an essential role in multiple
signaling pathways in vivo. Genes Dev. 19:2668–2681.
2005.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Cheng Z, Taylor B, Ourthiague DR and
Hoffmann A: Distinct single-cell signaling characteristics are
conferred by the MyD88 and TRIF pathways during TLR4 activation.
Sci Signal. 8(ra69)2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Xue YL, Zhang SX, Zheng CF, Li YF, Zhang
LH, Hao YF, Wang S and Li XW: Silencing of STAT4 protects against
autoimmune myocarditis by regulating Th1/Th2 immune response via
inactivation of the NF-κB pathway in rats. Inflammation.
42:1179–1189. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Pan A, Tan Y, Wang Z and Xu G: STAT4
silencing underlies a novel inhibitory role of microRNA-141-3p in
inflammation response of mice with experimental autoimmune
myocarditis. Am J Physiol Heart Circ Physiol. 317:H531–H540.
2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zhu Z, Xueying L, Chunlin L, Wen X,
Rongrong Z, Jing H, Meilan J, Yuwei X and Zili W: Effect of
berberine on LPS-induced expression of NF-κB/MAPK signalling
pathway and related inflammatory cytokines in porcine intestinal
epithelial cells. Innate Immun. 26:627–634. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Hu J, Luo J, Zhang M, Wu J, Zhang Y, Kong
H, Qu H, Cheng G and Zhao Y: Protective effects of radix sophorae
flavescentis carbonisata-based carbon dots against ethanol-induced
acute gastric ulcer in rats: Anti-inflammatory and antioxidant
activities. Int J Nanomedicine. 16:2461–2475. 2021.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Liu ZL, Liu ZJ, Liu JP, Yang M and Kwong
J: Herbal medicines for viral myocarditis. Cochrane Database Syst
Rev. (CD003711)2010.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Matsumori A, Wang H, Abelmann WH and
Crumpacker CS: Treatment of viral myocarditis with ribavirin in an
animal preparation. Circulation. 71:834–839. 1985.PubMed/NCBI View Article : Google Scholar
|