Introduction
Acute ischemic stroke (AIS) is one of the main
reasons for death and disability, particularly in an aging society
(1). In 61% of stroke patients,
administering intravenous thrombolysis with different agents
[medical management; urokinase (2.7%), streptokinase (36.8%) and
alteplase, recombinant tissue plasminogen activator] within 3-4.5 h
of symptom onset has a favorable outcome (2,3).
Furthermore, previous studies suggested that medical management is
safe and may benefit patients presenting mild AIS symptoms with a
low National Institutes of Health Stroke Scale (NIHSS) score (NIHSS
score ≤8) and who are also found to have an intracranial large
vessel occlusion (LVO) (4-6).
Endovascular thrombolysis (ET), focusing on
relieving vessel occlusion in stroke, has been developed as an
alternative for medical management or as an adjunct in
administration over the past few years (7,8).
However, there is limited knowledge about the role of ET in
patients with mild symptoms caused by LVO (9). Nonetheless, some studies also
proposed that ET may be favorable in patients with severe symptoms
(10).
Patients with mild AIS symptoms with an NIHSS score
≤8 also have an intracranial LVO presentation, requiring remarkably
complex therapeutic management (11). Unfortunately, LVO in those patients
is associated with poor outcomes; they present with mild deficits
(12) and because of weak
collateral conditions, they can worsen rapidly or progressively
(13). Thus, the need for any
acute management is often debated since these patients ‘only’ have
mild defects and any therapy has related risks (11).
Given these conflicting observational reports and
the lack of randomized data, the present study aimed to evaluate
the safety and effectiveness of medical management vs. ET therapy
among patients with mild AIS symptoms (NIHSS score ≤8) accompanied
by LVO.
Materials and methods
Search strategy
The study searched the comparative articles
involving mild AIS and LVO, thrombectomy, and medical management
through electronic databases, including the Cochrane Library,
Medline (1980-2022.12), PubMed (1980-2022.12), and EMBASE
(1980-2022.12). Preferred reporting items for systematic reviews
and meta-analyses were applied for establishing protocol and
manuscript design (14). The
keywords ‘mild acute ischemic stroke’, ‘large vessel occlusion’ and
‘thrombectomy/endovascular thrombolysis and medical management’,
which are present in the MeSH list, were used for database
search.
Selection of studies
Two of the reviewers (GF and VEG) independently
extracted data from the included articles, following the guidelines
of the epidemiology of meta-analysis. The following basic
information was captured: Main authors; year of publication; total
case number in the thrombectomy and medical management groups;
study type; outcome indicator; diabetes; hypertension; atrial
fibrillation; location; prior ischemic stroke; NIHSS of admission.
The extracted data were input into a table designed and
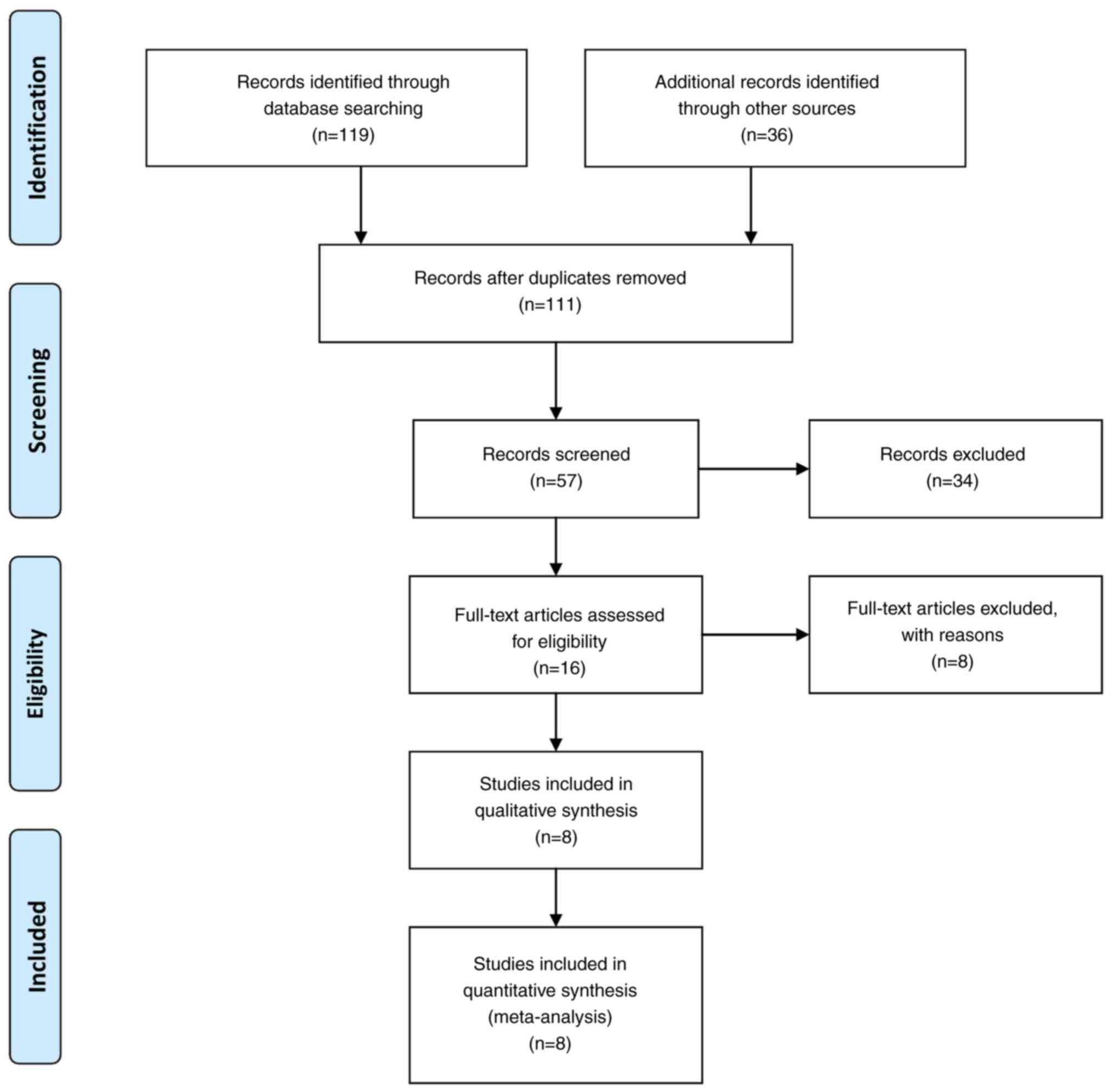
standardized according to the Cochrane Handbook. Fig. 1 depicts the flow of the study
selection process. In case of disagreement on the information to be
retained, another author with authority (this authority was decided
upon by all authors prior to commencing the research) had the final
say.
Inclusion and exclusion criteria. If an article
satisfied the following PICOS criteria, it was considered for
inclusion in the present meta-analysis: i) Population limited to
patients with mild acute ischemic stroke (NIHSS score ≤8) and LVO
on CT angiography [middle cerebral artery M1/M2, intracranial
carotid artery (ICA) or vertebrobasilar occlusion]; ii)
intervention limited to ET or medical management; iii) studies
comparing the outcomes between ET and medical management; iv) one
of the primary outcomes, such as morbidity and mortality, was
involved. To avoid publication bias, the final aim was to collect a
homogenous pool of manuscripts, including articles that compare
only two intervention modalities, i.e. ET and medical management.
Table I contains detailed data on
these articles.
 | Table IDesign and baseline characteristics
of the included trials. |
Table I
Design and baseline characteristics
of the included trials.
| | Sample size, n | Mean age
(years) | No. of males | Diabetes | Hypertension | Atrial
fibrillation | |
|---|
| First author/s,
year | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | (Refs.) |
|---|
| Urra et al,
2014 | 34 | 44 | 64 | 71 | 24 | 26 | 6 | 6 | 21 | 29 | 9 | 14 | (18) |
| Haussen et
al, 2016 | 10 | 22 | 60 | 68.2 | 5 | 15 | 2 | 4 | 6 | 13 | 3 | 8 | (19) |
| Haussen et
al, 2017 | 30 | 88 | 63.5 | 73 | 15 | 41 | 9 | 10 | 21 | 63 | 10 | 16 | (20) |
| Nagel et al,
2018 | 80 | 220 | 65.3 | 69.5 | 44 | 117 | 13 | 36 | 56 | 159 | 35 | 62 | (21) |
| Sarraj et
al, 2018 | 124 | 90 | 65.8 | 65.4 | 72 | 51 | 36 | 27 | 87 | 72 | NR | NR | (22) |
| Kastrup et
al, 2018 | 145 | 160 | 71 | 72 | 65 | 67 | 32 | 35 | 122 | 129 | 57 | 74 | (23) |
| Wang et al,
2020 | 23 | 24 | 53.9 | 64.4 | 17 | 17 | 4 | 6 | 17 | 17 | 2 | 2 | (24) |
| Xue et al,
2022 | 123 | 449 | 69 | 68 | 82 | 307 | 21 | 78 | 75 | 299 | 25 | 61 | (25) |
| | Location | |
| | Prior to ischemic
stroke | ICA | M1 | M2 |
Vertebrobasilar | NIHSS of
admission | |
| First author/s,
year | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | (Refs.) |
| Urra et al,
2014 | 5 | 2 | 0 | 1 | 13 | 13 | 7 | 16 | 12 | 12 | 4 | 3 | (18) |
| Haussen et
al, 2016 | 2 | 7 | 0 | 3 | 6 | 10 | 1 | 5 | 2 | 3 | 4 | 2 | (19) |
| Haussen et
al, 2017 | NR | NR | 2 | 17 | 11 | 17 | 9 | 17 | 7 | 11 | 4 | 3 | (20) |
| Nagel et al,
2018 | NR | NR | 10 | 26 | 33 | 48 | 23 | 108 | 6 | 15 | 4 | 3 | (21) |
| Sarraj et
al, 2018 | 22 | 12 | 21 | 12 | 68 | 21 | 33 | 44 | 0 | 0 | 4 | 3 | (22) |
| Kastrup et
al, 2018 | NR | NR | 32 | 19 | 62 | 76 | 51 | 65 | 0 | 0 | 8 | 7 | (23) |
| Wang et al,
2020 | 4 | 9 | 6 | 8 | 10 | 5 | 2 | 2 | 5 | 9 | 3 | 3 | (24) |
| Xue et al,
2022 | 19 | 77 | 34 | 110 | 59 | 213 | 20 | 83 | 12 | 12 | 3 | 3 | (25) |
| | mRS 0-2 after 3
months | Bleeding | Morbidity | Mortality | | | |
| First author/s,
year | | | Throm | Medic | Throm | Medic | Throm | Medic | Throm | Medic | | | (Refs.) |
| Urra et al,
2014 | | | 1 | 1 | 4 | 0 | 14 | 14 | 4 | 2 | | | (18) |
| Haussen et
al, 2016 | | | 10 | 17 | 0 | 0 | 1 | 5 | 0 | 3 | | | (19) |
| Haussen et
al, 2017 | | | 29 | 64 | 2 | 0 | NR | NR | NR | NR | | | (20) |
| Nagel et al,
2018 | | | 68 | 154 | 4 | 3 | 8 | 36 | 3 | 20 | | | (21) |
| Sarraj et
al, 2018 | | | 78 | 61 | 17 | 9 | 35 | 28 | 11 | 1 | | | (22) |
| Kastrup et
al, 2018 | | | 86 | 89 | NR | NR | 19 | 22 | NR | NR | | | (23) |
| Wang et al,
2020 | | | 16 | 18 | 2 | 0 | 12 | 5 | 1 | 1 | | | (24) |
| Xue et al,
2022 | | | 84 | 331 | 10 | 9 | NR | NR | 11 | 24 | | | (25) |
All prospective and retrospective studies that
evaluated at least one of the two modalities were included, whereas
editorials, reviews, case reports and articles focusing on the
pediatric population, unrelated outcomes, co-morbidities,
experimental techniques, or one of the two modalities from that
article pool, were excluded. In addition, in the case of studies
with mixed or unclear results, the corresponding information was
removed or was placed into groups accordingly, although without
affecting the ratio.
Outcomes' definition
The primary outcomes involved in the present study
included mortality and post-intervention morbidity (Karnofsky
Performance Score-KPS <80). In addition, to find out the
association between ET and medical management, the present
collected outcome measurements (secondary outcomes) such as the
rates of modified Rankin scale (mRS) scores 0-2 (indicating a good
outcome) at discharge and long-term follow-up (3 months for the
interventional cohort and bleeding after the intervention). The
outcomes reported in the included articles were assessed at least
three months after the ET or medical management for large vessel
occlusion strokes with minimal symptoms. Additionally, a quality
assessment tool was used to decrease the risk of bias in our poor
articles (Newcastle-Ottawa Scale; Table II) (15).
| Table IINOS quality assessment of final
article pool. |
Table II
NOS quality assessment of final
article pool.
| | NOS | |
|---|
| First author/s,
year | Study design | Selection | Comparability | Exposure | Total scores | (Refs.) |
|---|
| Urra et al,
2014 | Prosp | 3 | 3 | 3 | 9 | (18) |
| Haussen et
al, 2016 | Prosp | 3 | 3 | 3 | 9 | (19) |
| Haussen et
al, 2017 | Retro | 3 | 2 | 2 | 7 | (20) |
| Nagel et al,
2018 | Prosp | 3 | 3 | 3 | 9 | (21) |
| Sarraj et
al, 2018 | Retro | 3 | 2 | 2 | 7 | (22) |
| Kastrup et
al, 2018 | Retro | 3 | 2 | 2 | 7 | (23) |
| Wang et al,
2020 | Retro | 3 | 2 | 2 | 7 | (24) |
| Xue et al,
2022 | Retro | 3 | 2 | 2 | 7 | (25) |
Evaluation of the risk of bias
The Cochrane Collaboration tool was used by two
reviewers (GF and VEG) to assess the risk of bias in each study
(16). The evaluation included
random sequence generation, allocation concealment, blinding of
participants and assessors, blinding of outcome assessment,
incomplete outcome data, selective reporting and other biases (such
us criteria of ‘unclear risk’ of bias; this was in the case of
insufficient available information to assess whether an important
risk of bias exists or insufficient evidence that an identified
problem will introduce bias. The assessment results were classified
into low, high and unclear risk levels. The third reviewer
arbitrated any disagreements.
Data synthesis and assessment of
heterogeneity
All analyses were carried out using Review Manager
Software v5.4 (RevMan; https://training.cochrane.org/online-learning/core-software/revman).
Heterogeneity across trials was identified using I2
statistics; considering I2 >50% as high
heterogeneity, a meta-analysis was conducted using a random-effect
model according to the Cochrane Handbook for Systematic Reviews of
Interventions (v5.1.0) (17).
Otherwise, a meta-analysis using the fixed-effect model was
performed. The continuous outcomes were expressed as a weighted
mean difference with 95% confidence intervals (CIs). For
discontinuous variables, odds ratios (OR) with 95% CIs were applied
for the assessment. To test the sensitivity, the ‘leave out one’
model was used by removing one study at a time. P<0.05 was
considered to indicate a statistically significant difference.
Results
Articles meeting criteria
A total of eight articles met the eligibility
criteria (18-25).
The total number of patients was 569 who underwent ET and 1097 with
medical management for LVO strokes with minimal symptoms. The study
sample was based on eight studies (Table II). Among these, five were
retrospective and three were prospective observational studies.
Epidemiological and clinical
features
The mean age of the patients was 70.46 years (range,
53-72 years; 64.06 and 76.93 years for the ET and the medical
management sample, respectively). The male-to-female ratio was
1:1.7. Diabetes was diagnosed in 325/1666 (19.5%) of patients
(123/569 and 202/1097 in the ET and the medical management group,
respectively), hypertension in 1186/1666 (71.1%) of patients
(405/569 and 781/1097 in the ET and medical management groups,
respectively), and atrial fibrillation in 378/1666 (22.6%) of
patients (141/569 and 237/1097 in the ET and medical management
groups, respectively) (Table
I).
Diabetes mellitus
Information regarding diabetes mellitus was
available in eight articles (18-25)
and demonstrated no statistical result (OR 1.07, CI 95% 0.58-1.40;
P=0.61) with no heterogeneity (P=0.56 and I2=0%)
(Fig. S1). Diabetes mellitus was
found in 325 of the 1666 (19.5%) patients in the total group. In
the ET group, diabetes mellitus was diagnosed in 123 of 569 (21.6%)
patients, compared with 202 of 1097 (18.4%) in the medical
management group. Looking at the funnel plot of the same parameter,
no publication bias was found.
Hypertension
As regards hypertension, information was available
in eight articles (18-25)
and demonstrated no statistical result (OR 1.87, CI 95% 0.68-1.10;
P=0.23) with no heterogeneity (P=0.83 and I2=0%) (Fig. S2). Hypertension was found in 1186
of 1666 (71.1%) patients in the total group. In the ET group,
hypertension was diagnosed in 405 of 569 (71.1%) patients, compared
with 781 of 1097 (71.1%) in the medical management group. Looking
at the funnel plot of the same parameter, no publication bias was
found.
Atrial fibrillation
Atrial fibrillation data were available in eight
articles (18-25).
Atrial fibrillation was reported for 378 of the 1666 (22.6%)
patients in the total group and 141 of the 569 (28.2%) patients in
the ET group. The statistical analysis demonstrated no
statistically significant difference (OR 1.27, CI 95% 0.85-1.91;
P=0.24), but indicated heterogeneity (P=0.07 and I2=48%)
(Fig. 2A). By testing sensitivity
(Table III), after removing the
article by ‘Kastrup et al, 2018’ (23), a statistically significant
difference result was found (OR 1.61, CI 95% 1.18-2.21; P<0.05),
with no heterogeneity (P=0.52 and I2=0%) (Fig. 2B). The total sample size for this
combination was 247 (18.1%) out of 1361, of which 84 (19.8%) out of
424 were from the ET group and 163 (17.3%) out of 937 were from the
medical management group. Looking at the funnel plot of the same
parameter, it was found that the study results without the Karstup
et al, 2018 article (23)
displayed an improved dispersion with no publication bias (Fig. 2C and D).
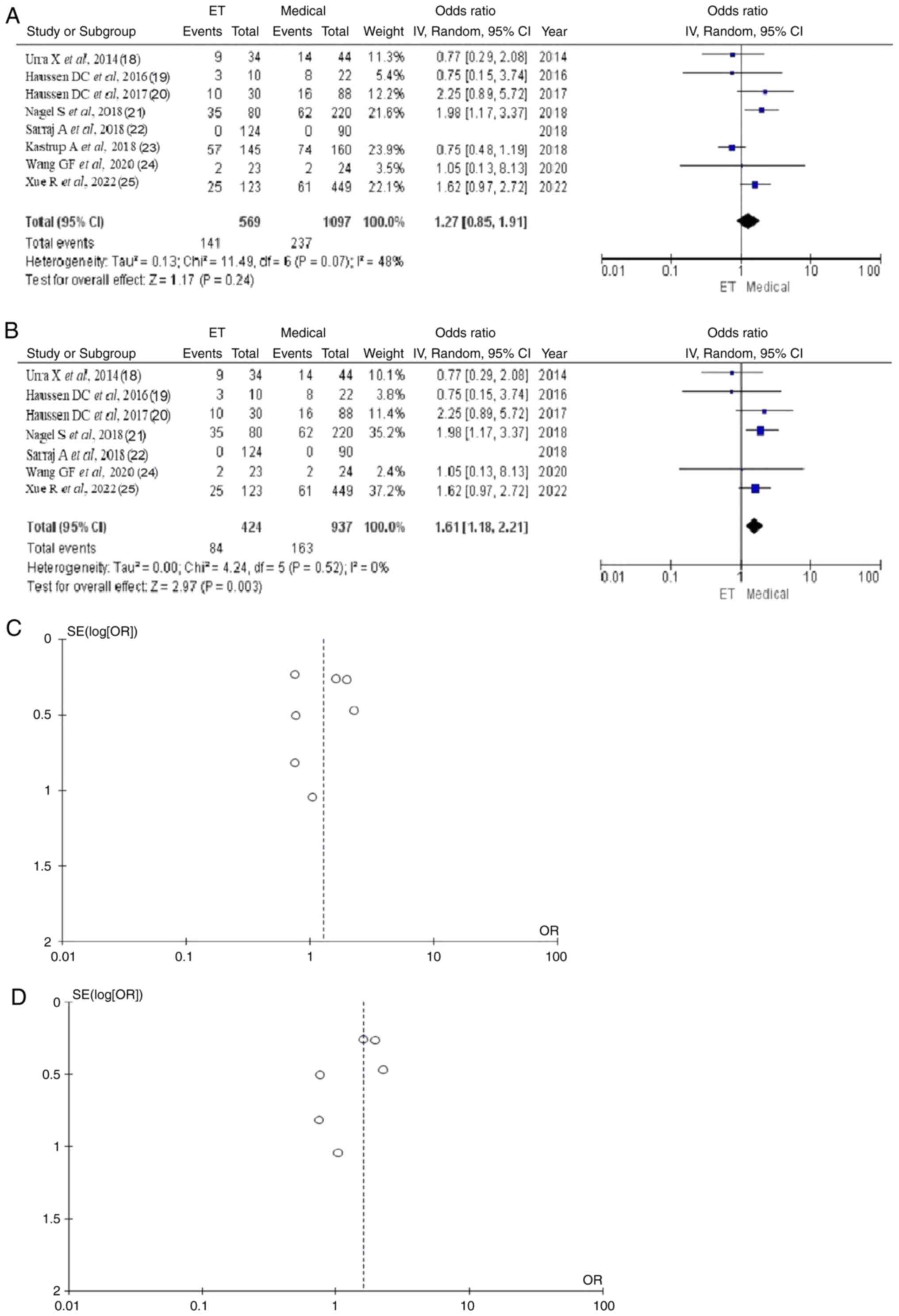 | Figure 2Atrial fibrillation ORs. (A) Forest
plot of atrial fibrillation ORs demonstrated no statistically
significant difference between the groups (total OR 1.27, CI 95%
0.85-1.91; P=0.24). (B) Forest plot of atrial fibrillation ORs
obtained by excluding the ‘Kastrup et al, 2018’ (23) article demonstrated a statistically
significant difference between the groups, (total OR 1.61, CI 95%
1.18-2.21; P<0.05). (C) Funnel plot of the atrial fibrillation
between groups, with ‘Kastrup A et al 2018’ (23) article and with heterogeneity
(P=0.07 and I2=48 %). (D) Funnel plot of the atrial
fibrillation between groups, without ‘Kastrup A et al, 2018’
(23) article and without
heterogeneity (P=0.52 and I2=0%). ET, endovascular
thrombolysis; medical, medical management; OR, odds ratio. |
| Table IIIMeta-analysis of clinical
parameters. |
Table III
Meta-analysis of clinical
parameters.
| | Groups | Overall effect | Heterogeneity | |
|---|
| Parameters | Excluded
trials | Trials, n | Throm | Medic | Effect
estimate | CI 95% | P-value | I2
(%) | P-value | (Refs.) |
|---|
| Atrial
fibrillation | None | 8 | 141 | 237 | 1.27 | 0.85-1.91 | 0.24 | 48 | 0.07 | (18-25) |
| | Urra et al,
2014 | 7 | 132 | 223 | 1.36 | 0.87-2.12 | 0.18 | 52 | 0.06 | (18) |
| | Haussen et
al, 2016 | 7 | 138 | 229 | 1.31 | 0.85-2.03 | 0.22 | 55 | 0.05 | (19) |
| | Haussen et
al, 2017 | 7 | 131 | 221 | 1.18 | 0.76-1.82 | 0.46 | 49 | 0.08 | (20) |
| | Nagel et al,
2018 | 7 | 106 | 175 | 1.13 | 0.73-1.73 | 0.58 | 36 | 0.17 | (21) |
| | Sarraj et
al, 2018 | 7 | 141 | 237 | 1.27 | 0.85-1.91 | 0.24 | 48 | 0.07 | (22) |
| | Kastrup et
al, 2018 | 7 | 84 | 163 | 1.61 | 1.18-2.21 | <0.05 | 0 | 0.52 | (23) |
| | Wang et al,
2020 | 7 | 139 | 235 | 1.28 | 0.83-1.98 | 0.26 | 56 | 0.04 | (24) |
| | Xue et al,
2022 | 7 | 116 | 176 | 1.19 | 0.72-1.97 | 0.50 | 51 | 0.07 | (25) |
| Prior to ischemic
stroke | None | 8 | 52 | 107 | 0.97 | 0.56-1.70 | 0.93 | 32 | 0.21 | (18-25) |
| | Urra et al,
2014 | 7 | 47 | 105 | 0.90 | 0.60-1.36 | 0.63 | 14 | 0.32 | (18) |
| | Haussen et
al, 2016 | 7 | 50 | 100 | 1.03 | 0.55-1.96 | 0.92 | 45 | 0.14 | (19) |
| | Haussen et
al, 2017 | 7 | 52 | 107 | 0.97 | 0.56-1.70 | 0.93 | 32 | 0.21 | (20) |
| | Nagel et al,
2018 | 7 | 52 | 107 | 0.97 | 0.56-1.70 | 0.93 | 32 | 0.21 | (21) |
| | Sarraj et
al, 2018 | 7 | 30 | 95 | 0.84 | 0.39-1.78 | 0.65 | 36 | 0.20 | (22) |
| | Kastrup et
al, 2018 | 7 | 52 | 107 | 0.97 | 0.56-1.70 | 0.93 | 32 | 0.21 | (23) |
| | Wang et al,
2020 | 7 | 48 | 98 | 1.10 | 0.68-1.80 | 0.69 | 14 | 0.32 | (24) |
| | Xue et al,
2022 | 7 | 33 | 30 | 1.01 | 0.41-2.49 | 0.99 | 46 | 0.13 | (25) |
| Diabetes
mellitus | None | 8 | 123 | 202 | 1.07 | 0.58-1.40 | 0.61 | 0 | 0.56 | (18-25) |
| Hypertension | None | 8 | 405 | 781 | 0.87 | 0.68-1.10 | 0.23 | 0 | 0.83 | (18-25) |
Prior ischemic stroke
As regards the prior ischemic stroke, the total
number of patients was 159 (9.5%) out of 1666 patients, of which 52
out of 569 (9.1%) were from the ET group and 107 out of 1097 (9.7%)
were from the medical management group. The statistical analysis
demonstrated no significant difference (OR 0.97, CI 95% 0.56-1.70;
P=0.93) but indicated heterogeneity (P=0.21 and I2=32%)
(Fig. S3A). By testing the
sensitivity (Table III), low
heterogeneity (P=0.32 or and I2=14%) was achieved only
after removing the articles by ‘Urra et al, 2014’ (18) or ‘Wang et al, 2020’
(24), as the combination with the
removed article by ‘Urra et al, 2014’ (18) was of higher quality because the
total sample was 152 compared with 146 in the combination without
the article by ‘Wang et al, 2020’ (24) (Table
III). However, it was found again no statistically significant
difference (OR 0.90, CI 95% 0.60-1.36; P=0.63) (Fig. S3B). Looking at the funnel plot of
the same parameter, it was found that the study results without the
‘Urra et al, 2014’ (18)
article displayed an improved dispersion with low publication bias
(Fig. S3C and D).
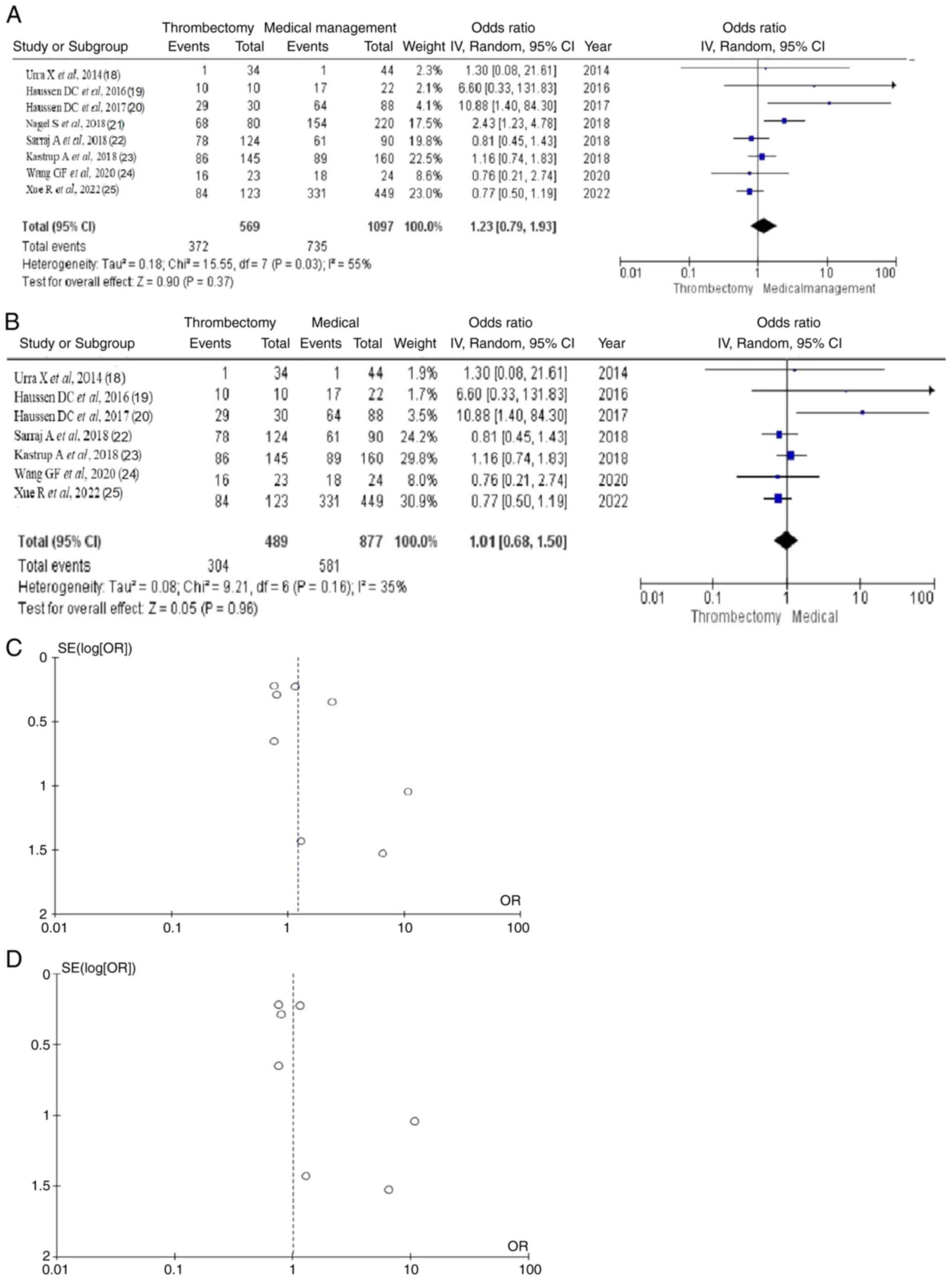
MRS 0-2 after 3 months
As regards the mRS 0-2 after 3 months, the total
number of patients was 1,107 (66.4%) out of 1,666 patients in the
total group, of which 372 (65.3%) out of 569 were from the ET group
and 735 (67.0%) out of 1097 patients were from the medical
management group. The statistical analysis demonstrated no
significant difference (OR 1.23, CI 95% 0.79-1.93; P=0.37) but
indicated some heterogeneity (P=0.03 and I2=55%)
(Fig. 3A). By testing the
sensitivity (Table IV), low
heterogeneity (P=0.16 and I2=35%) was achieved only
after removing the article by ‘Nagel et al, 2018’ (21) but it was found again no
statistically significant difference (OR 1.01, CI 95% 0.68-1.50;
P=0.96) (Fig. 3B). Looking at the
funnel plot of the same parameter, it was found that the study
results without the ‘Nagel S et al, 2018’ (21) article displayed an improved
dispersion with low publication bias (Fig. 3C and D).
| Table IVMeta-analysis of clinical
outcomes. |
Table IV
Meta-analysis of clinical
outcomes.
| | Groups | Overall effect | Heterogeneity | |
|---|
| Outcomes | Excluded
trials | Trials, n | Throm | Medic | Effect
estimate | CI 95% | P-value | I2
(%) | P-value | (Refs.) |
|---|
| mRS 0-2 | None | 8 | 372 | 735 | 1.23 | 0.79-1.93 | 0.37 | 55 | 0.03 | (18-25) |
| | Urra et al,
2014 | 7 | 371 | 734 | 1.24 | 0.77-1.99 | 0.37 | 61 | 0.02 | (18) |
| | Haussen et
al, 2016 | 7 | 362 | 718 | 1.18 | 0.76-1.85 | 0.46 | 58 | 0.03 | (19) |
| | Haussen et
al, 2017 | 7 | 343 | 671 | 1.10 | 0.75-1.61 | 0.63 | 43 | 0.10 | (20) |
| | Nagel et al,
2018 | 7 | 304 | 581 | 1.01 | 0.68-1.50 | 0.96 | 35 | 0.16 | (21) |
| | Sarraj et
al, 2018 | 7 | 294 | 674 | 1.40 | 0.81-2.42 | 0.23 | 58 | 0.03 | (22) |
| | Kastrup et
al, 2018 | 7 | 286 | 646 | 1.32 | 0.72-2.42 | 0.36 | 61 | 0.02 | (23) |
| | Wang et al,
2020 | 7 | 356 | 717 | 1.31 | 0.80-2.13 | 0.29 | 61 | 0.02 | (24) |
| | Xue et al,
2022 | 7 | 288 | 404 | 1.43 | 0.84-2.43 | 0.19 | 50 | 0.06 | (25) |
| Bleeding | None | 7 | 39 | 21 | 3.13 | 1.65-5.95 | <0.05 | 14 | 0.33 | |
| Mortality | None | 6 | 30 | 51 | 1.37 | 0.55-3.41 | 0.50 | 45 | 0.10 | (18,19,21-25) |
| | Urra et al,
2014 | 5 | 26 | 49 | 1.19 | 0.40-3.52 | 0.75 | 53 | 0.07 | (18) |
| | Haussen et
al, 2016 | 5 | 30 | 48 | 1.56 | 0.60-4.05 | 0.36 | 50 | 0.09 | (19) |
| | Sarraj et
al, 2018 | 5 | 19 | 50 | 1.07 | 0.46-2.48 | 0.87 | 33 | 0.20 | (20) |
| | Nagel et al,
2018 | 5 | 27 | 31 | 1.94 | 1.02-3.69 | 0.04 | 2 | 0.40 | (21) |
| | Wang et al,
2020 | 5 | 29 | 50 | 1.41 | 0.50-3.97 | 0.51 | 56 | 0.06 | (22) |
| | Xue et al,
2022 | 5 | 19 | 27 | 1.27 | 0.34-4.75 | 0.73 | 53 | 0.08 | (23) |
| Morbidity | None | 6 | 89 | 110 | 1.02 | 0.64-1.63 | 0.94 | 39 | 0.14 | (18,19,21-24) |
| | Urra et al,
2014 | 5 | 75 | 96 | 0.95 | 0.55-1.64 | 0.85 | 45 | 0.12 | (18) |
| | Haussen et
al, 2016 | 5 | 88 | 105 | 1.07 | 0.65-1.75 | 0.80 | 47 | 0.11 | (19) |
| | Sarraj et
al, 2018 | 5 | 70 | 88 | 1.07 | 0.56-2.01 | 0.84 | 51 | 0.08 | (22) |
| | Kastrup et
al, 2018 | 5 | 81 | 74 | 1.16 | 0.70-1.94 | 0.56 | 35 | 0.19 | (23) |
| | Nagel et al,
2018 | 5 | 54 | 82 | 1.10 | 0.58-1.09 | 0.78 | 50 | 0.09 | (21) |
| | Wang et al,
2020 | 5 | 77 | 105 | 0.87 | 0.61-1.24 | 0.45 | 0 | 0.57 | (24) |
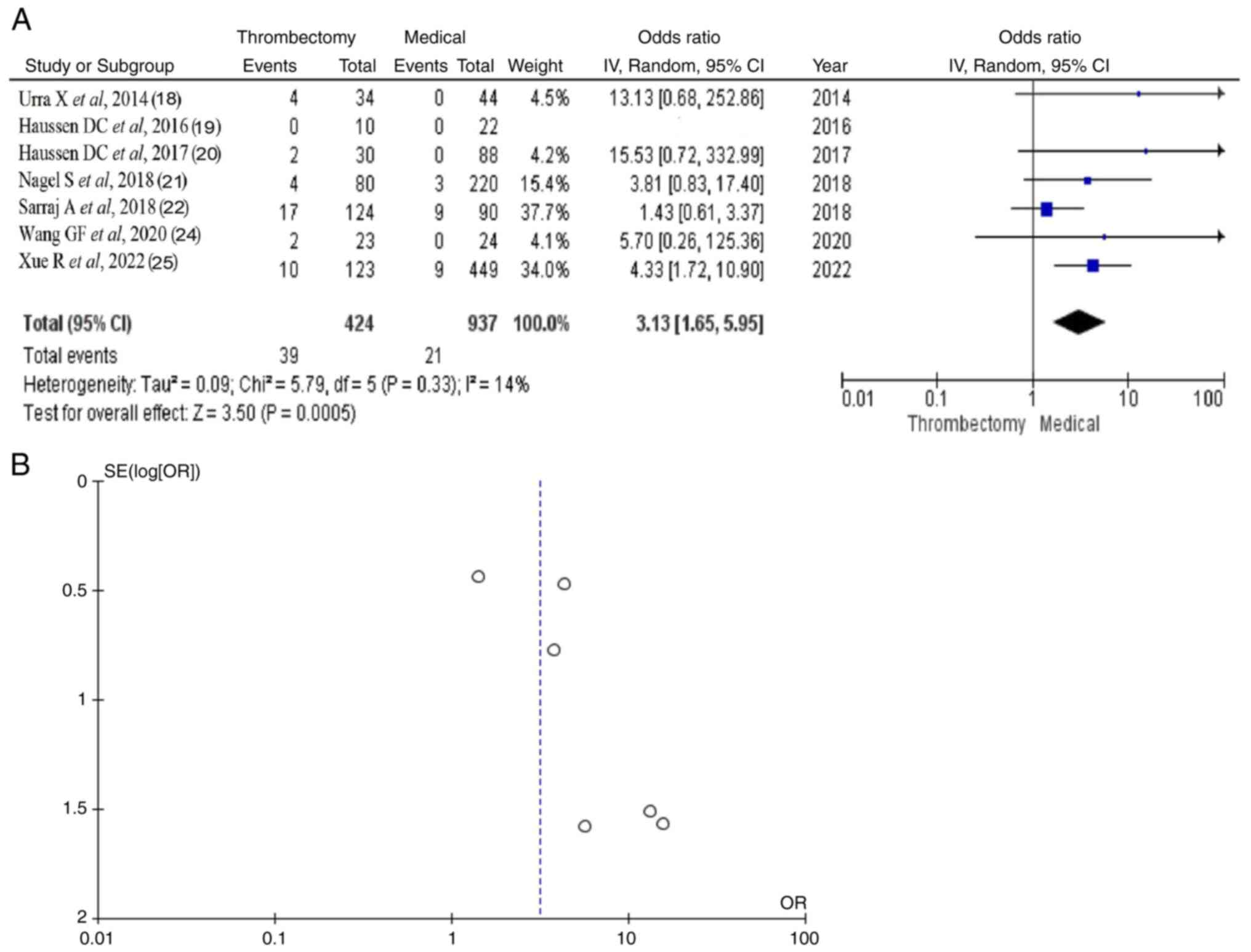
Bleeding
Information regarding bleeding was available in
seven out of eight articles (18-22,24,25)
and demonstrated a statistical result (OR 3.13, CI 95% 1.65-5.95;
P<0.05) with no heterogeneity (P=0.33 and I2=14%)
(Fig. 4). Bleeding was found in 60
out of 1666 (3.6%) patients in the total group. In the ET group,
bleeding was diagnosed in 39 out of 129 (30.2%) patients, compared
with 21 out of 1097 (1.9%) in the medical management group. Looking
at the funnel plot of the same parameter, it was found a very low
publication bias.
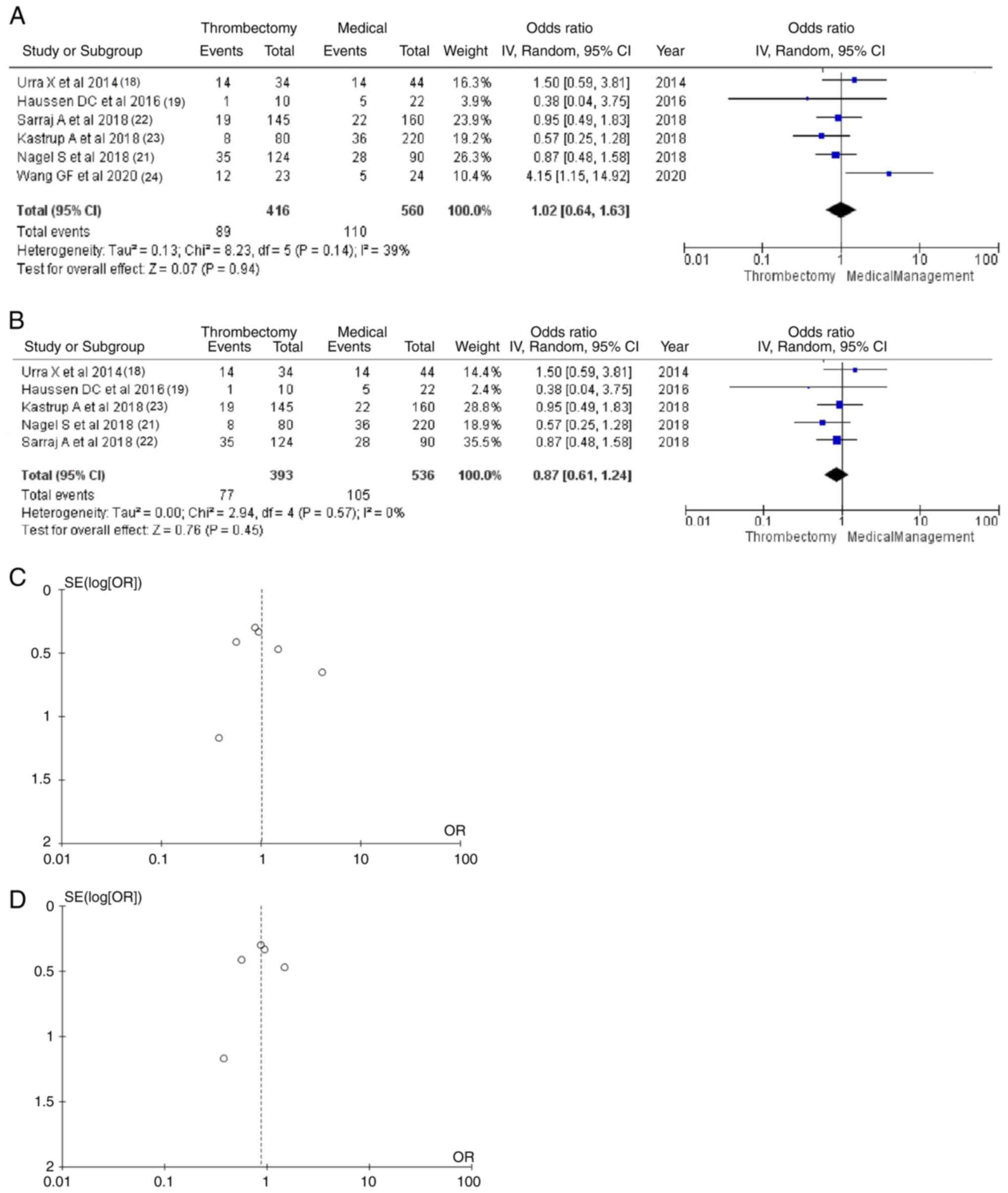
Morbidity
Morbidity data were available in six of the eight
articles (18,20-22,24,25):
A total of 199 (20.3%) from 976 included patients; and poor KPS in
89 (21.3%) of 416 patients from the ET group. The statistical
analysis demonstrated no significant difference (OR 1.02, CI 95%
0.64-1.63; P=0.94) and indicated heterogeneity (P=0.14 and
I2=39%) (Fig. 5A). By
testing the sensitivity (Table
IV), no heterogeneity (P=0.57 and I2=0%) was
achieved only after removing the article by ‘Wang et al,
2020’ (24) but again without a
statistically significant difference (OR 0.87, CI 95% 0.61-1.24;
P=0.45) (Fig. 5B). Looking at the
funnel plot of the same parameter, it was found that the study
results without the ‘Wang et al, 2020’ (24) article displayed an improved
dispersion with no publication bias (Fig. 5C and D).
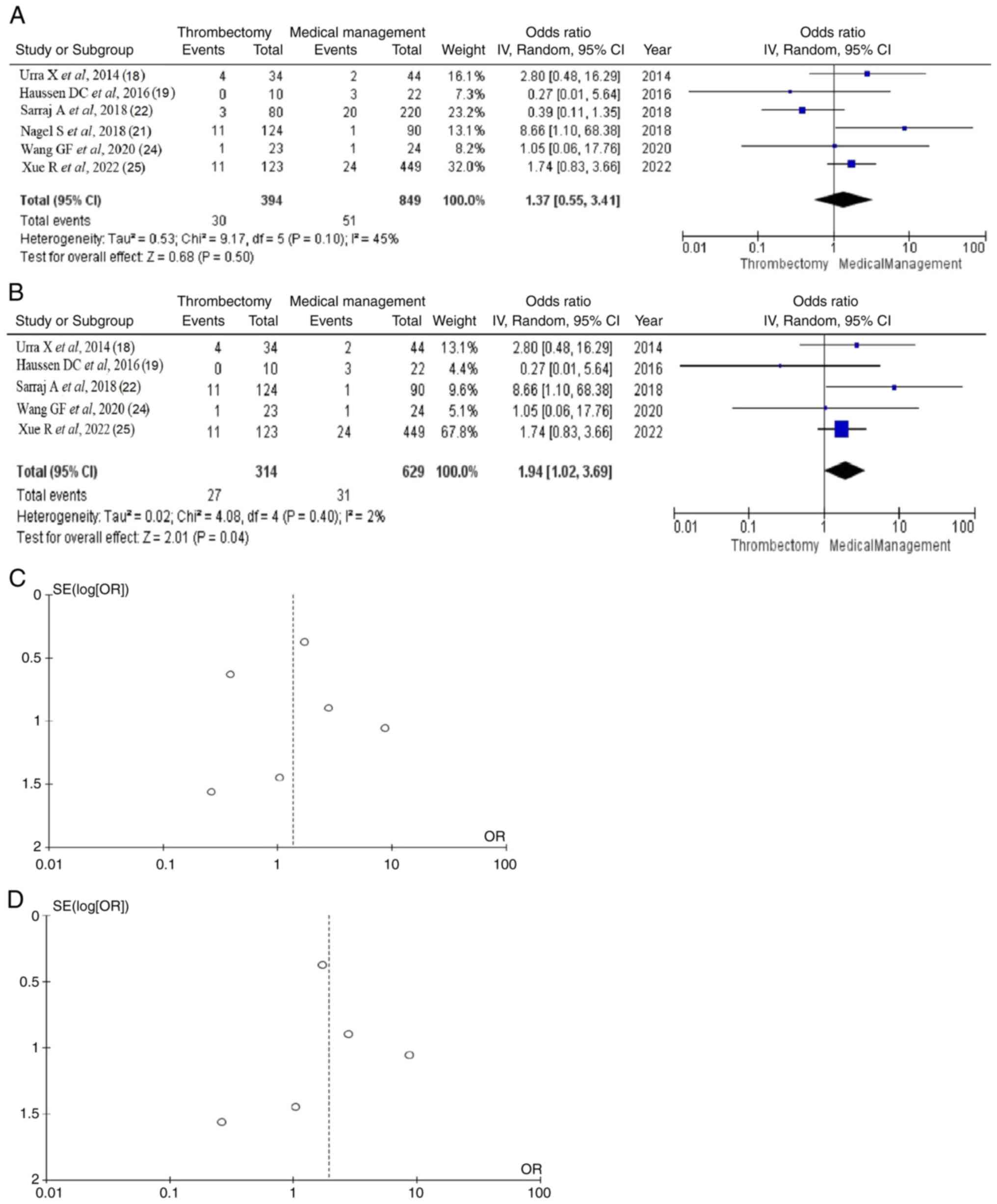
Mortality
Mortality data were available in six of the eight
articles (18,19,21,22,24,25):
A total of 81/1,243 (6.5%) patients, including 30 out of 394 (7.6%)
from the ET group and 51 (6.0%) out of 849 from the medical
management group. The statistical analysis demonstrated no
statistically significant difference (OR 1.37, CI 95 % 0,55-3.41;
P=0.50) but indicated heterogeneity (P=0.10 and I2=45 %)
(Fig. 6A). By testing the
sensitivity (Table IV), after
removing the article by ‘Nagel S et al, 2018’ (21), it was found a statistically
significant difference (OR 1.94, CI 95% 1.02-3.69; P<0.05) with
no heterogeneity (P=0.40 and I2=2%) (Fig. 6B). Looking at the funnel plot of
the same parameter, it was found that the study results without the
‘Nagel S et al, 2018’ (21)
article displayed an improved dispersion with very little
publication bias (Fig. 6C and
D).
Discussion
The present study suggested that medical management
for LVO strokes with minimal symptoms was associated with fewer
complications compared with ET intervention. More precisely, atrial
fibrillation was the only statistically significant parameter
related to bleeding and mortality in patients with LVO strokes with
minimal symptoms. Interestingly, the rates of the mRS score of 0-2
(indicating a good outcome) at discharge and the morbidity (KPS
<80) showed no association with medical management or ET therapy
in those patients.
The findings of the present meta-analysis pointed
out that ET therapy may be associated with a high risk of bleeding
and mortality in patients with LVO presenting with mild symptoms
(NIHSS score ≤8).
The absence of benefits from ET therapy is
consistent with the findings of several previous studies (26-29).
However, a multicenter observational study reported that ET therapy
was effective in recanalizing the occluded vessel but increased the
risk of serious bleeding significantly without improving the
functional outcome, suggesting that it was not justified routinely
in minor strokes (18). The
current study showed that ET therapy is related to a high risk of
bleeding and mortality in patients with LVO presenting mild
symptoms (NIHSS score ≤8). This may be attributed to several
reasons, such as the acceptable collateral condition that developed
in patients with LVO and mild symptoms, which predisposes to
bleeding and reduces the advantages of ET.
In addition, the recent meta-analysis showed that ET
therapy, compared with medical management alone, is associated with
higher rates of bleeding and mortality outcomes in patients with
atrial fibrillation. A possible explanation is the higher
proportion of atrial fibrillation in the ET group, an extensively
reported risk factor for intracerebral haemorrhage (30,31).
In agreement with previous cohorts of patients
presenting with mild symptoms, the treatment modality had a high
percentage of good early clinical outcomes and an excellent early
clinical outcome (23); however,
even after excluding patients with contraindications for an ET, the
clinical outcome was not significantly different between ET and
medical management in patients with an admission NIHSS ≤8. The
aforementioned results are similar to the ones shown in the present
study, with mRS 0-2 and morbidity having no association with
medical management or ET therapy in those patients.
Prior studies reported on outcomes achieved using ET
therapy in milder stroke patients but were limited because of a
single-center study design (20),
a small number of patients (18-20)
or the lack of a similar medical management group (32). These uncertain results highlight
the need for higher-quality data for this population.
There are several limitations in the present study.
First, most of the eligible reports that were included were
retrospective. These retrospective studies are affected by low
accuracy and data loss. Additionally, the study design differed
significantly among the included studies, e.g. the duration of
follow-up (e.g., 30-90 days).
In conclusion, the routine use of ET was not
significantly favorable for the early clinical or radiological
outcome in patients with mild strokes and LVO compared with medical
management alone. However, the present results suggested that ET
could be beneficial only in patients with NIHSS ≥8. It is also
undisputable that a randomized trial is needed to determine the
difference in outcome between these two treatment modalities in
these patients.
Supplementary Material
Diabetes mellitus ORs. (A) Forest plot
of diabetes mellitus ORs demonstrated no statistically significant
difference between the groups (total OR 1.07, CI 95% 0.58-1.40; p
0.61). (B) Funnel plot of the diabetes mellitus ORs demonstrated no
heterogeneity in the groups (P=0.56, and I2=0%). ET,
endovascular thrombolysis; medical, medical management; OR, odds
ratio.
Hypertension ORs. (A) Forest plot
hypertension ORs demonstrated no statistically significant results
(total OR 1.87, CI 95% 0.68-1.10; P=0.23). (B) Funnel plot of the
hypertension ORs demonstrated no heterogeneity in the groups
(P=0.83 and I2=0%). ET, endovascular thrombolysis;
medical, medical management; OR, odds ratio.
Prior ischemic stroke ORs. (A) Forest
plot of prior ischemic stroke ORs demonstrated no statistically
significant difference groups (total OR 0.97, CI 95% 0.56-1.70;
P=0.93). (B) Forest plot of prior ischemic stroke ORs without ‘Urra
et al 2014’ (18) article demonstrated no statistically
significant difference between the groups (total OR 0.90, CI 95%
0.60-1.36; P=0.63). (C) Funnel plot of the prior ischemic stroke
ORs between groups, with ‘Urra et al, 2014’(18) article and
with heterogeneity (P=0.21 and I2=32%). (D) Funnel plot
of the prior ischemic stroke ORs between groups, without ‘Urra
et al, 2014’(18) article, and very low heterogeneity (P=0.32
and I2=14%). Medical, medical management; OR, odds
ratio.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
GF and VEG conceptualized the study. VEG, IT, GF,
PP, ISA, DAS and NT analyzed the data and wrote and prepared the
draft of the manuscript. VEG and GF provided critical revisions.
All authors contributed to the manuscript revision. All authors
read and approved the final manuscript. GF and VEG confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this
article.
References
|
1
|
Feigin VL, Roth GA, Naghavi M, Parmar P,
Krishnamurthi R, Chugh S, Mensah GA, Norrving B, Shiue I, Ng M, et
al: Global burden of stroke and risk factors in 188 countries,
during 1990-2013: A systematic analysis for the global burden of
disease study 2013. Lancet Neurol. 15:913–924. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hacke W, Kaste M, Bluhmki E, Brozman M,
Dávalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, et
al: Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic
stroke. N Engl J Med. 359:1317–1329. 2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
IST-3 collaborative group. Effect of
thrombolysis with alteplase within 6 h of acute ischaemic stroke on
long-term outcomes [the third International Stroke Trial (IST-3)]:
18-month follow-up of a randomised controlled trial. Lancet Neurol.
12:768–776. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Strbian D, Piironen K, Meretoja A,
Sairanen T, Putaala J, Tiainen M, Artto V, Rantanen K, Häppölä O,
Kaste M, et al: Helsinki stroke thrombolysis registry group:
Intravenous thrombolysis for acute ischemic stroke patients
presenting with mild symptoms. Int J Stroke. 8:293–299.
2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Köhrmann M, Nowe T, Huttner HB, Engelhorn
T, Struffert T, Kollmar R, Saake M, Doerfler A, Schwab S and
Schellinger PD: Safety and outcome after thrombolysis in stroke
patients with mild symptoms. Cerebrovasc Dis. 27:160–166.
2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Baumann CR, Baumgartner RW, Gandjour J,
von Büdingen HC, Siegel AM and Georgiadis D: Good outcomes in
ischemic stroke patients treated with intravenous thrombolysis
despite regressing neurological symptoms. Stroke. 37:1332–1333.
2006.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Meyers PM, Schumacher HC, Connolly ES Jr,
Heyer EJ, Gray WA and Higashida RT: Current status of endovascular
stroke treatment. Circulation. 123:2591–2601. 2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Pierot L, Soize S, Benaissa A and Wakhloo
AK: Techniques for endovascular treatment of acute ischemic stroke:
From intra-arterial fibrinolytics to stent-retrievers. Stroke.
46:909–914. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Selim MH and Molina CA: Management of
acute stroke patients with rapidly resolving deficits and
persistent vascular occlusion: A real clinical equipoise. Stroke.
41:3007–3008. 2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Broderick JP, Palesch YY, Demchuk AM,
Yeatts SD, Khatri P, Hill MD, Jauch EC, Jovin TG, Yan B, Silver FL,
et al: Endovascular therapy after intravenous t-PA versus t-PA
alone for stroke. N Engl J Med. 368:893–903. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Cerejo R, Cheng-Ching E, Hui F, Hussain
MS, Uchino K, Bullen J and Toth G: Treatment of patients with mild
acute ischemic stroke and associated large vessel occlusion. J Clin
Neurosci. 30:60–64. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Heldner MR, Zubler C, Mattle HP, Schroth
G, Weck A, Mono ML, Gralla J, Jung S, El-Koussy M, Lüdi R, et al:
National institutes of health stroke scale score and vessel
occlusion in 2152 patients with acute ischemic stroke. Stroke.
44:1153–1157. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mokin M, Masud MW, Dumont TM, Ahmad G,
Kass-Hout T, Snyder KV, Hopkins LN, Siddiqui AH and Levy EI:
Outcomes in patients with acute ischemic stroke from proximal
intracranial vessel occlusion and NIHSS score below 8. J
Neurointerv Surg. 6:413–417. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Foster RL: Reporting guidelines: Consort,
prisma, and squire. J Spec Pediatr Nurs. 17:1–2. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Wells GA, Shea B, O'Connell D, Peterson J,
Welch V, Losos M and Tugwell P: The newcastle-ottawa scale (NOS)
for assessing the quality of nonrandomised studies in
meta-analyses. Ottawa Hospital Research Institute, Ottawa, ON,
2014. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
|
|
16
|
Higgins JP, Altman DG, Gøtzsche PC, Jüni
P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et
al: The cochrane collaboration's tool for assessing risk of bias in
randomised trials. BMJ. 343(d5928)2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Cochrane Handbook for Systematic Reviews
of Interventions Version 5.1.0. The Cochrane Collaboration, 2011.
Available from www.cochrane-handbook.org. Updated March 2011.
|
|
18
|
Urra X, Román LS, Gil F, Millán M, Cánovas
D, Roquer J, Cardona P, Ribó M, Martí-Fàbregas J, Abilleira S, et
al: Medical and endovascular treatment of patients with large
vessel occlusion presenting with mild symptoms: An observational
multicenter study. Cerebrovasc Dis. 38:418–424. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Haussen DC, Bouslama M, Grossberg JA,
Anderson A, Belagage S, Frankel M, Bianchi N, Rebello LC and
Nogueira RG: Too good to intervene? Thrombectomy for large vessel
occlusion strokes with minimal symptoms: An intention-to-treat
analysis. J Neurointerv Surg. 9:917–921. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Haussen DC, Lima FO, Bouslama M, Grossberg
JA, Silva GS, Lev MH, Furie K, Koroshetz W, Frankel MR and Nogueira
RG: Thrombectomy versus medical management for large vessel
occlusion strokes with minimal symptoms: An analysis from
STOPStroke and GESTOR cohorts. J Neurointerv Surg. 10:325–329.
2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Nagel S, Bouslama M, Krause LU, Küpper C,
Messer M, Petersen M, Lowens S, Herzberg M, Ringleb PA, Möhlenbruch
MA, et al: Mechanical thrombectomy in patients with milder strokes
and large vessel occlusions. Stroke. 49:2391–2397. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Sarraj A, Hassan A, Savitz SI, Grotta JC,
Cai C, Parsha KN, Farrell CM, Imam B, Sitton CW, Reddy ST, et al:
Endovascular thrombectomy for mild strokes: How low should we go?
Stroke. 49:2398–2405. 2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kastrup A, Brunner F, Hildebrandt H, Roth
C, Winterhalter M, Giessing C and Papanagiotou P: Endovascular
therapy versus thrombolysis in patients with mild strokes and large
vessel occlusions within the anterior circulation. Interv Neurol.
7:431–438. 2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Wang GF, Zhao X, Liu SP, Xiao YL and Lu
ZN: Efficacy and safety of mechanical thrombectomy for acute mild
ischemic stroke with large vessel occlusion. Med Sci Monit.
26(e926110)2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Xue R, Zhong W, Zhou Y, He Y, Yan S, Chen
Z, Wang J, Gong X and Lou M: Endovascular treatment for minor acute
ischemic strokes with large vessel occlusion. J Am Heart Assoc.
11(e027326)2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Volny O, Zerna C, Tomek A, Bar M, Rocek M,
Padr R, Cihlar F, Nevsimalova M, Jurak L, Havlicek R, et al:
Thrombectomy vs medical management in low NIHSS acute anterior
circulation stroke. Neurology. 95:e3364–e3372. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Goyal N, Tsivgoulis G, Malhotra K, Ishfaq
MF, Pandhi A, Frohler MT, Spiotta AM, Anadani M, Psychogios M, Maus
V, et al: Medical management vs mechanical thrombectomy for mild
strokes: An international multicenter study and systematic review
and meta-analysis. JAMA Neurol. 77:16–24. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Manno C, Disanto G, Bianco G, Nannoni S,
Heldner M, Jung S, Arnold M, Kaesmacher J, Müller M, Thilemann S,
et al: Outcome of endovascular therapy in stroke with large vessel
occlusion and mild symptoms. Neurology. 93:e1618–e1626.
2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Wu X, Khunte M, Payabvash S, Zhu C,
Brackett A, Matouk C, Gandhi D, Sanelli P and Malhotra A: Outcomes
after thrombectomy for minor stroke: A meta-analysis. World
Neurosurg. 149:e1140–e1154. 2021.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tian B, Tian X, Shi Z, Peng W, Zhang X,
Yang P, Li Z, Zhang X, Lou M, Yin C, et al: Clinical and imaging
indicators of hemorrhagic transformation in acute ischemic stroke
after endovascular thrombectomy. Stroke. 53:1674–1681.
2022.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Van Kranendonk KR, Treurniet KM, Boers
AMM, Berkhemer OA, van den Berg LA, Chalos V, Lingsma HF, van Zwam
WH, van der Lugt A, van Oostenbrugge RJ, et al: Clinical and
imaging markers associated with hemorrhagic transformation in
patients with acute ischemic stroke. Stroke. 50:2037–2043.
2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Dargazanli C, Consoli A, Gory B, Blanc R,
Labreuche J, Preda C, Bourdain F, Decroix JP, Redjem H, Ciccio G,
et al: Is reperfusion useful in ischaemic stroke patients
presenting with a low national institutes of health stroke scale
and a proximal large vessel occlusion of the anterior circulation?
Cerebrovasc Dis. 43:305–312. 2017.PubMed/NCBI View Article : Google Scholar
|