Introduction
Strabismus is a common condition of binocular
misalignment, with a prevalence rate ranging from 3-5%, which
differs between ethnic groups (1-4).
In East-Asian populations, concomitant exotropia is the most
prevalent type of strabismus (5,6),
which presents as a constant angle of deviation. This condition can
lead to visual acuity problems, such as amblyopia and suppression,
and further result in deficits in binocular visual function and
impact stereopsis.
The pathogenesis of strabismus is mainly associated
with the dysplasia of extraocular muscles and surrounding
structures, particularly in incomitant strabismus (7,8).
However, the association of concomitant strabismus with changes in
the central nervous system remains inconclusive. Ocular movement is
related to the activity of neurons in specific brain regions, such
as the frontal eye field, which is associated with conjugate ocular
movement (9,10). It is therefore important to explore
the origin of neurons in brain regions.
To evaluate the morphological changes in the entire
brain objectively and assess the differences in brain structures,
MRI technology may be used. Voxel-based morphometry (VBM) is a
technique that allows for the objective evaluation of changes in
brain structures (11). The
present study utilized the VBM method to analyze the changes in
functional brain areas in patients with concomitant exotropia and
further expand the knowledge on the pathogenesis of exotropia in
the central nervous system.
Subjects and methods
Patients
For the present prospective study, a total of 11
adult patients with concomitant exotropia (5 males and 6 females)
who visited the Department of Pediatric Ophthalmology and
Strabismus at Tianjin Eye Hospital (Tianjin, China) from October
2021 to March 2022 were recruited. In addition, 11 healthy adult
individuals (5 males and 6 females), who were age- and sex-matched,
were recruited into the normal control group. All participants
underwent complete eye examinations and their corrected visual
acuities were 20/20. The dominant eyes were the left eyes and any
subjects with organic eye lesions, anisometropia, ocular trauma,
surgeries, mental or psychological diseases, systemic diseases and
neurological disorders were excluded. All participants were
right-handed and ethnic Han individuals, whereas their body height
and weight were recorded. The near and distant strabismus angle of
patients with concomitant exotropia was also measured. Written
informed consent was obtained from all selected subjects and the
study was approved by the ethics review committee of Tianjin Eye
Hospital (approval no. 2021046; Tianjin, China), according to the
Declaration of Helsinki.
MRI data processing. MRI technology
parameters
A 3.0 Tesla MRI (Prisma; Siemens Healthineers) was
used to acquire the structural and functional images from the
subjects. Foam cushions were used to cover the heads of all
subjects to minimize movement during imaging. The
3D-magnetization-prepared rapid gradient echo (MPRAGE) sequence was
utilized to reconstruct T1-weighted structural images with high
resolution. The 3D-MPRAGE sequence parameters were as follows:
Repetition time (TR)/echo time (TE), 2,000/2.26 msec; flip angle
(FA), 8˚; field of view (FOV), 256x256 mm2; slice
thickness, 1 mm; with 192 slices. Echo-planar imaging (EPI) was
used for the resting-state MRI scan. The EPI scan parameters were
as follows: TR/TE, 750/30 msec; FA, 54˚; FOV, 222x222
mm2; slice thickness, 3 mm; interval, 0; and 640
time-points were acquired each time.
Structural MRI data processing. The
high-resolution T1-weighted structural images were preprocessed
using the statistical parametric mapping software package (SPM12;
https://www.fil.ion.ucl.ac.uk/spm/software/spm12)
on the MATLAB R2016b platform (The MathWorks, Inc.) and the
voxel-based morphometry tool (CAT12; Salford Systems; Computational
Anatomy Toolbox; http://www.neuro.uni-jena.de). First, the original
images were registered to the standard space of the Montreal
Neurological Institute (MNI; https://www.mcgill.ca/bic/software/tools-data-analysis/anatomical-mri/atlases).
Next, the standard images were segmented into gray matter, white
matter and cerebrospinal fluid (CSF) using tissue segmentation in
SPM12. Finally, the gray matter volume (GMV) images were spatially
smoothed by a 6-mm Gaussian kernel with full width at half maximum
(FWHM). The smoothed images were then used for statistical
analysis.
Functional MRI (fMRI) data processing. The
resting-state fMRI data were preprocessed using the statistical
parametric mapping software package (SPM12) on the MATLAB R2016b
platform and the DPARSF_V5.3 software (http://rfmri.org/DPARSF). The 640 volumes were
acquired for functional scanning, where the first 10 time-points
were excluded in order to remove the instable data caused by the
signal equilibrium and participants' adaption to scanning noise.
Slice-timing correction was not applied due to the significantly
shortened TR. To remove head movement, head motion correction was
performed. The functional images were coregistered with the
structural images and spatially normalized using the MNI template.
Resampling of each voxel was performed to 3x3x3 mm3. The
spatial smoothing process was then performed using a Gaussian
kernel of 6 mm FWHM. The liner drift, band filter, Friston-24
parameters, the mean global signal, the white matter signal and CSF
signal were then extracted as covariates and regressed out to
minimize non-neural signals.
The amplitude of low-frequency fluctuation (ALFF),
regional homogeneity (Reho) and functional connectivity (FC)
analyses were perfomed using the DPARSF_V5.3 software. In the ALFF
analysis, the time series was converted to the frequency domain
using fast Fourier transform. The square root of the power spectrum
was also calculated and averaged over 0.01-0.08 Hz. A
standardization procedure was applied by dividing the individual
ALFF map by its own mean ALFF. The Reho analysis was conducted by
calculating the Kendall consistency coefficient of neighboring
vertices' blood-oxygen-level dependent time series before the
spatial smoothing procedure. For standardization purposes, each
individual Reho map was divided by its own mean Reho. Subsequently,
all Reho maps were smoothed using 6 mm FWHM. For the FC analysis,
the spherical region (3 mm radius) with the spatial coordinates of
the significant GMV differences between the groups was used as the
regions of interest (ROI). FC analysis was conducted by calculating
the correlation coefficient between the average time series of ROIs
and residual brain voxels. The ALFF, Reho and FC values of each
voxel were transformed by Fisher-Z transformation to obtain the
Z-score maps of FC for each subject.
Statistical analysis. Statistical
analysis of clinical data and MRI data
The clinical data were analyzed using the SPSS 25.0
software (IBM Corp). The quantitative data of each group were
examined for normality of distribution (Shapiro-Wilk test) with a
threshold of α=0.05 and expressed as the mean ± standard deviation.
An unpaired two-samples t-test was used to compare age, body mass
index and deviation angle. The χ2 test was employed for
sex analysis between the groups. P<0.05 was considered to
indicate a statistically significant difference or association.
Statistical analysis of structural MRI data.
An unpaired two-samples t-test was conducted in GMV between the
concomitant exotropia group and the normal control group, with sex,
age and whole brain volume serving as the covariates. The
statistical threshold was P<0.05 [false discovery rate (FDR)
correction].
Statistical analysis of functional MRI data.
The regions with significant GMV differences were used as masks and
the ALFF and Reho values of the masks were extracted. The general
linear model in the SPSS 25.0 software was used to compare the ALFF
and Reho values between the two groups, with sex and age as
covariates. The statistical significance level was set at
P<0.05. The t-statistics maps for each group were obtained using
an unpaired one-sample t-test (significance threshold set at
P<0.05, familywise error correction at the voxel level). The
explicit masks for two-samples t-tests were defined as the union of
the binarized corrected t-maps of the two groups. Subsequently,
two-samples t-tests between groups were performed within the
explicit masks, with age, sex and head movement parameters as
covariates. The significance threshold was set at P<0.001
corrected for Gaussian random-field (GRF) at the cluster level,
corresponding to a corrected P<0.05 at the cluster level. The
correlation between GMV, ALFF, Reho and FC values, and strabismus
angle were analyzed by Pearson's correlation analysis.
Results
Comparison of baseline data and
clinical characteristics between groups
Table I shows the
comparison of sex, age, BMI and exotropia angle (near and distance)
between the concomitant exotropia group and the normal control
group (Table I). There were no
significant differences in sex, age or BMI between the two groups.
However, the near and distant exotropia angles were significantly
higer in the concomitant exotropia group compared with those in the
normal control group (P<0.001).
 | Table IComparison of baseline data and
clinical characteristics between the concomitant exotropia group
and the normal control group. |
Table I
Comparison of baseline data and
clinical characteristics between the concomitant exotropia group
and the normal control group.
| Variable | Concomitant
exotropia | Normal control | Statistical
parameter | P-value |
|---|
| Sex
(male/female) | 5/6 | 5/6 | χ2=0 | >0.999 |
| Age, years | 29.91±6.75 | 30.36±6.64 | t=-0.159 | 0.875 |
| BMI,
kg/m2 | 23.28±1.94 | 23.52±1.50 | t=-0.322 | 0.751 |
| Near exotropia angle
(PD, 33 cm) | -33.18±6.81 | -4.45±2.16 | t=-13.337 | <0.001 |
| Distance exotropia
angle (PD, 5 m) | -30.45±5.68 | -2.91±1.92 | t=-15.234 | <0.001 |
Comparison of GMV between groups
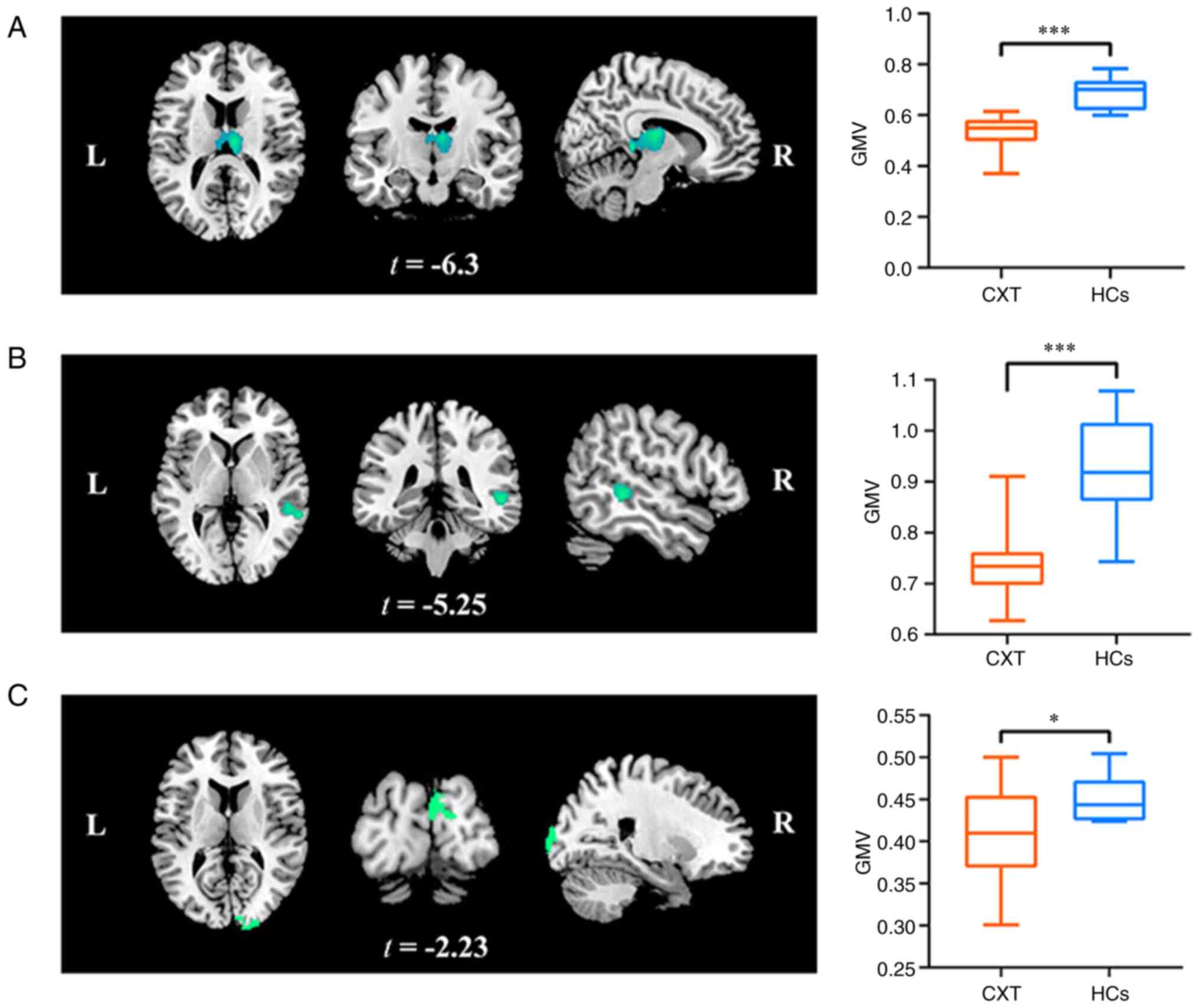
The analysis of GMV differences between the
concomitant exotropia group and the normal control group indicated
that the bilateral thalamus (t=-6.3, FDR corrected, P<0.05), the
right MTG (t=-5.25, FDR corrected, P<0.05 and the right cuneus
(t=-2.23, FDR corrected, P<0.05) of the concomitant exotropia
group had significantly reduced GMV compared with those in the
normal control group (Fig. 1;
Tables II and III).
| Table IIDecreased gray matter volume in the
brain regions of the concomitant exotropia group and the normal
control group. |
Table II
Decreased gray matter volume in the
brain regions of the concomitant exotropia group and the normal
control group.
| | MNI coordinates | |
|---|
| Brain region | Location (L/R/B) | x | y | z | Voxel size | t-value |
|---|
| Thalamus | B | 9 | -36 | 3 | 2,912 | -6.30 |
| MTG | R | 55.5 | -36 | -1.5 | 359 | -5.25 |
| Cuneus | R | 5 | -90 | 14 | 820 | -2.23 |
| Table IIIComparison of gray matter volume
between the concomitant exotropia group and the normal control
group. |
Table III
Comparison of gray matter volume
between the concomitant exotropia group and the normal control
group.
| Brain region | Location
(L/R/B) | Concomitant
exotropia group | Normal control
group | P-value |
|---|
| Thalamus | B | 0.53±0.07 | 0.69±0.06 | <0.001 |
| MTG | R | 0.73±0.07 | 0.93±0.10 | <0.001 |
| Cuneus | R | 0.40±0.06 | 0.45±0.03 | 0.03 |
Comparison of ALFF and Reho values
between the two groups
After conducting ALFF and Reho analyses, there were
no significant differences between the concomitant exotropia and
normal control groups (P>0.05). Specifically, in the ALFF
analysis, the bilateral thalamus (t=0.10, P=0.74), right MTG
(t=-0.07, P=0.95) and right cuneus (t=0.02, P=0.99) exhibited no
significant differences between the two groups. Similarly, in the
Reho analysis, the bilateral thalamus (t=-1.58, P=0.13), right MTG
(t=-1.31, P=0.21) and right cuneus (t=-0.75, P=0.46) did not
exhibit any significant differences (Table IV).
| Table IVComparison of ALFF and Reho values
between the concomitant exotropia group and the normal control
group. |
Table IV
Comparison of ALFF and Reho values
between the concomitant exotropia group and the normal control
group.
| A, ALFF |
|---|
| Brain region | Location
(L/R/B) | Concomitant
exotropia | Normal control | P-value |
|---|
| Thalamus | B | 0.0034±0.0021 | 0.0029±0.0042 | 0.74 |
| MTG | R | 0.0163±0.0161 | 0.0172±0.0349 | 0.95 |
| Cuneus | R | 0.38±0.47 | 0.38±0.36 | 0.99 |
| B, Reho |
| Brain region | Location
(L/R/B) | Concomitant
exotropia | Normal control | P-value |
| Thalamus | B | -0.006±0.004 | -0.004±0.003 | 0.13 |
| MTG | R | -0.06±0.02 | -0.04±0.03 | 0.21 |
| Cuneus | R | 0.82±0.56 | 1.02±0.69 | 0.46 |
Resting-state FC results compared
within and between groups
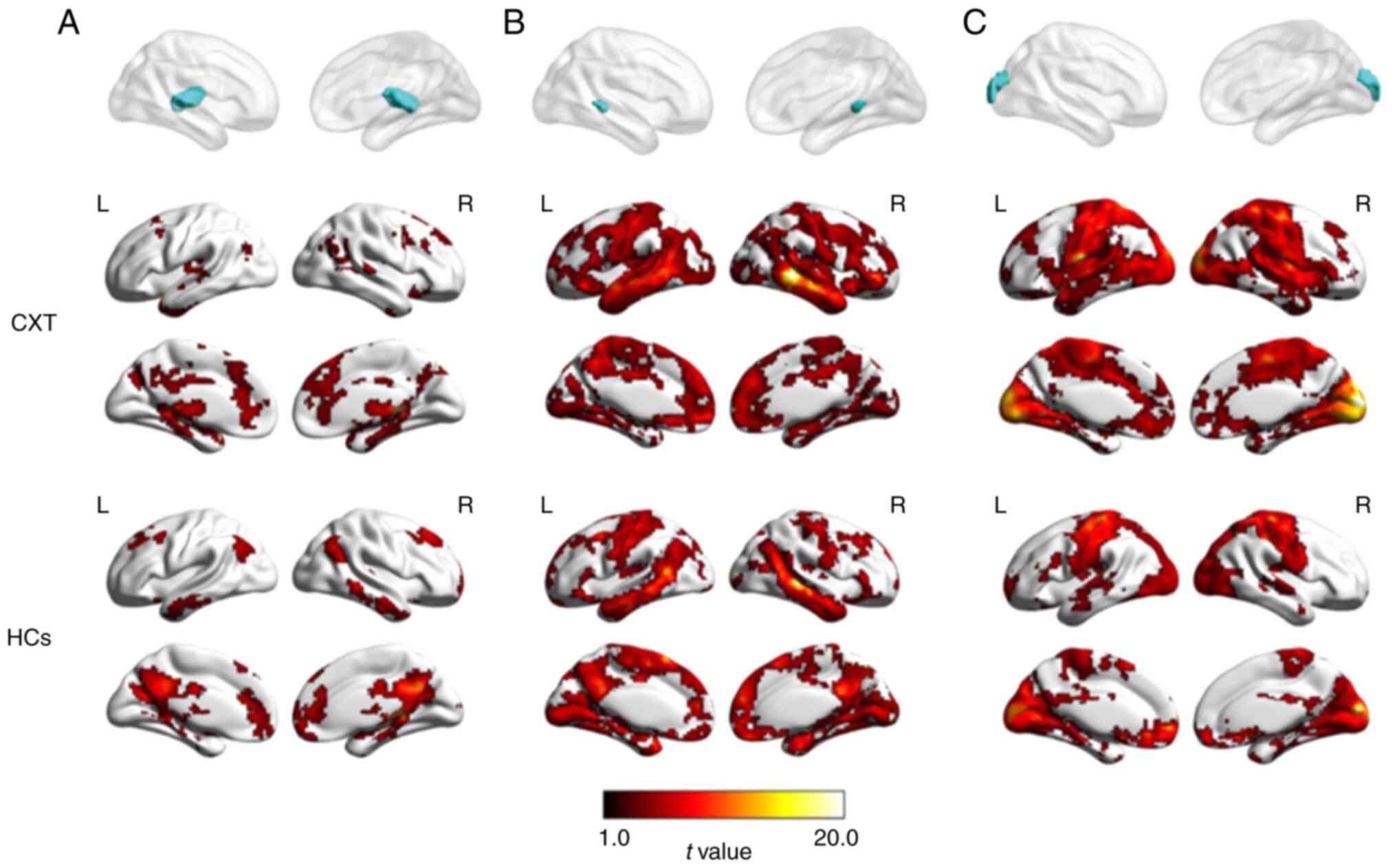
The intra-group one-sample t-test revealed similar
FC patterns in the concomitant exotropia group and the normal
control group. Strong FC was observed between the bilateral
thalamus and the bilateral cerebellum, frontal lobe, left parietal
lobe, anterior cingulate and posterior cingulate gyrus in both
groups, while the normal control group also showed strong
connectivity with the temporal lobe and parietal lobe. The right
MTG and right cuneus showed strong FC with several brain regions in
both groups, including the bilateral cerebellum, frontal lobe,
temporal lobe, parietal lobe, primary sensorimotor cortex, anterior
cingulate cortex and posterior cingulate cortex (FEW corrected,
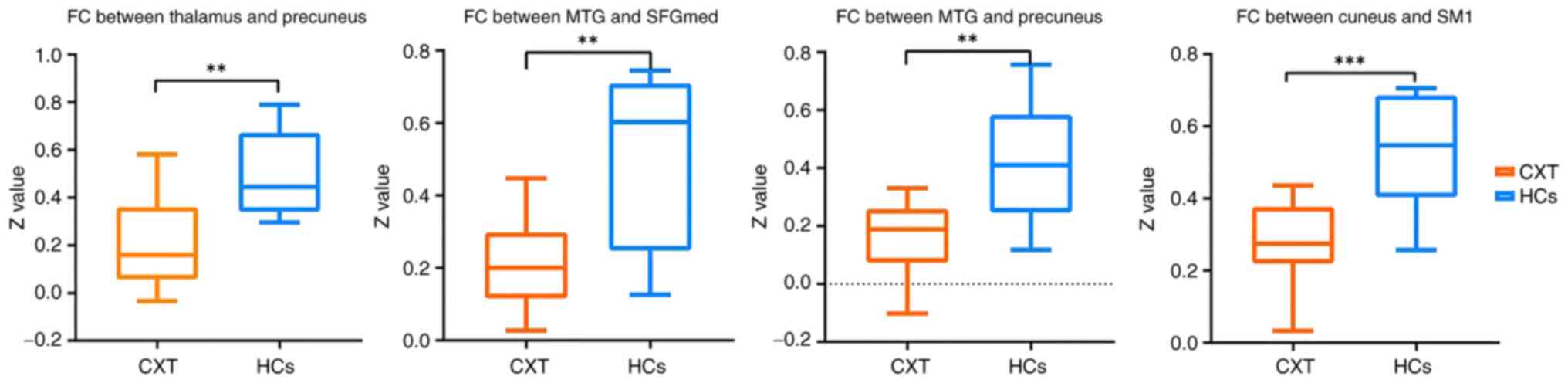
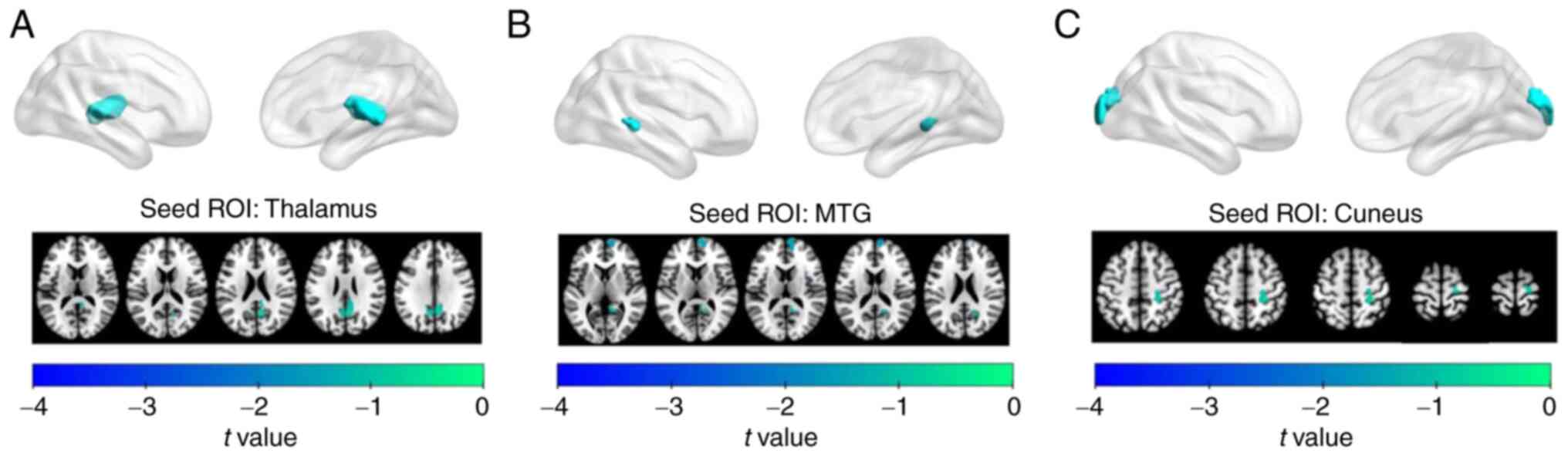
P<0.05; Fig. 2). However, a
two-sample t-test indicated reduced FC between the bilateral
thalamus and bilateral precuneus in the concomitant exotropia group
compared with that in the normal control group (GRF corrected,
P<0.05). The concomitant exotropia group also had decreased FC
between the right MTG and the right medial superior frontal gyrus
and the right precuneus (GRF-corrected, P<0.05), as well as
reduced FC between the right cuneus and the right primary
sensorimotor cortex (GRF-corrected, P<0.05) (Figs. 3 and 4; Tables
V and VI).
| Table VBrain regions with statistically
significant differences in functional connectivity values between
the concomitant exotropia group and the normal control group. |
Table V
Brain regions with statistically
significant differences in functional connectivity values between
the concomitant exotropia group and the normal control group.
| | MNI
coordinates | |
|---|
| Brain regions | x | y | z | Voxel size | t-value |
|---|
| Bilateral thalamus
and bilateral precuneus | 9 | -63 | 21 | 203 | -3.827 |
| Right MTG and right
medial superior frontal gyrus | 3 | 69 | 9 | 103 | -4.777 |
| Right MTG and right
precuneus | 21 | -57 | 21 | 63 | -3.968 |
| Right cuneus and
right primary sensorimotor cortex | 24 | -24 | 51 | 98 | -4.214 |
| Table VIComparison of functional connectivity
values between the concomitant exotropia group and the normal
control group. |
Table VI
Comparison of functional connectivity
values between the concomitant exotropia group and the normal
control group.
| Brain regions | Concomitant
exotropia | Normal control | P-value |
|---|
| Bilateral thalamus
and bilateral precuneus | 0.21±0.19 | 0.49±0.17 | 0.002 |
| Right MTG and right
medial superior frontal gyrus | 0.21±0.12 | 0.50±0.24 | 0.001 |
| Right MTG and right
precuneus | 0.15±0.13 | 0.42±0.20 | 0.001 |
| Right cuneus and
right primary sensorimotor cortex | 0.28±0.12 | 0.54±0.16 | <0.001 |
Correlation analysis between clinical
variables and GMV, ALFF values, Reho values and abnormal FC in the
concomitant exotropia group
Pearson correlation analysis indicated that the
atrophy value of GMV in the bilateral thalamus was positively
correlated with the deviation angle (PD) in the concomitant
exotropia group (r=0.673, P=0.023). However, no statistically
significant correlation was found between the PD and other brain
regions of GMV atrophy values, ALFF values, Reho values or FC in
the concomitant exotropia group (Tables VII and VIII).
| Table VIIUnivariate correlation between
deviation angle and ALFF as well as Reho values. |
Table VII
Univariate correlation between
deviation angle and ALFF as well as Reho values.
| A, ALFF |
|---|
| Brain region | R | P-value |
|---|
| Right MTG | -0.390 | 0.235 |
| Thalamus | 0.078 | 0.819 |
| Right cuneus | 0.257 | 0.445 |
| B, Reho |
| Brain region | R | P-value |
| Right MTG | -0.149 | 0.662 |
| Thalamus | -0.079 | 0.818 |
| Right cuneus | -0.148 | 0.665 |
| Table VIIIUnivariate correlation between
deviation angle and GMV as well as FC. |
Table VIII
Univariate correlation between
deviation angle and GMV as well as FC.
| A, GMV |
|---|
| Brain region | R | P-value |
|---|
| Thalamus | 0.673 | 0.023 |
| Right MTG | -0.210 | 0.534 |
| Right cuneus | -0.024 | 0.943 |
| B, FC |
| Brain region | R | P-value |
| Bilateral thalamus
and bilateral precuneus | 0.008 | 0.981 |
| Right cuneus and
right primary sensorimotor cortex | -0.019 | 0.956 |
| Right MTG and right
medial superior frontal gyrus | 0.289 | 0.388 |
| Right MTG and right
precuneus | 0.374 | 0.257 |
Discussion
Although strabismus is typically characterized by
the misalignment of both eyes, with or without abnormal extraocular
muscle function, it is currently considered to be a developmental
anomaly of the central visual pathway, associated with ocular
movement (12). In addition,
changes in eye position may lead to developmental changes in
binocular vision and stereopsis (13). However, the pathogenesis of
concomitant exotropia remains to be fully elucidated. It was
previously reported that patients with concomitant exotropia
exhibit relatively reduced volumes of the medial rectus muscle on
MRI, resulting in a relatively weaker function of contraction. This
change may be the peripheral mechanism underlying concomitant
exotropia (14). However, in
addition to this peripheral mechanism, several studies have
previously demonstrated that strabismus is associated with abnormal
development of the central visual pathway that mediates ocular
movement (12,15). A previous study has indicated that
early correction of strabismus prevented maldevelopment of ocular
movements driven by cerebral motor pathways in a strabismus rhesus
monkey model and may be beneficial for brain development in human
infants (16).
The dorsal pathway of the visual afferent system
exhibits some activation which is not associated with the
visuomotor region and it is located more posteriorly, or caudally,
to the parietal lobe (17).
Previous studies have indicated that MT is related to visual depth
perception and may participate in the coding calculation of visual
information (18,19). In addition, MT is involved in the
processing of parallax signals (20), which is crucial in the coding of
three-dimensional information from different sources (21). The present study found a reduction
in GMV in the right MTG in patients with concomitant exotropia,
suggesting that this change may be associated with a decline of
binocular visual function and impairment of stereoscopic function
in these patients. A previous study also proposed that the dorsal
pathway of the visual afferent system is involved in ocular
movement and spatial position information (22), suggesting that abnormal changes in
this dorsal pathway may contribute to the development of
strabismus.
After the onset of strabismus, alterations in the
nervous system are not limited to the visual cortex but can also
involve the thalamus (23,24). The thalamus acts as the brain's
relay station, with abundant nerve fibers connecting to numerous
brain regions (25). A previous
study by Chan et al (10)
revealed that the GMV of the right thalamus was increased in
patients with exotropia, which is contrary to the present findings.
In the present study, a reduction in the volume of gray matter was
observed in the bilateral thalamic region in patients with
concomitant exotropia. This disparity may be due to differences in
the inclusion criteria of patients. However, changes in thalamic
function in patients with exotropia have been established and
further research is required to unravel the specific changes and
underlying mechanisms.
The cuneate lobe, located above the medial surface
of the posterior occipital lobe, has been indicated to have a
decreased GMV in patients with common strabismus (26). Yan et al (27) also previously found changes in the
function of the cuneate lobe after analyzing brain FC in
resting-state MRI images of 10 patients with concomitant exotropia.
The present study on patients with concomitant exotropia also
revealed decreased GMV of the cuneate lobe compared with that in
the normal control group. The ventral pathway of the human visual
afferent system, mainly distributed along the occipitotemporal
lobe, is relevant to object recognition (17). In the present study, the cuneate
lobe, adjacent to the occipital lobe, atrophied to a certain extent
and changed its function. The precuneus, located in front of the
cuneate lobe, is an inward part of the parietal lobe located in the
cerebral hemisphere, separated from the cuneate lobe by the
parietooccipital sulcus. It is related to advanced functions, such
as eye movement and visual-spatial processing (28). The FC between the bilateral
thalamus and bilateral precuneus was decreased in patients with
concomitant exotropia, as did the FC between the right MTG and the
right medial superior frontal gyrus, and that with the right
precuneus was reduced. The FC between the right cuneus and the
right primary sensorimotor cortex also decreased, suggesting that a
series of changes may have occurred in the precuneus region as the
GMV decreases. However, further studies are required to understand
these changes more fully.
Abnormal visual input, such as amblyopia, and
changes in ocular position, may lead to changes in the development
of the visual center, resulting in alterations in GMV (29). However, the present study excluded
patients with amblyopia and anisometropia in the inclusion
criteria, thereby minimizing the effects of abnormal visual
experience on the changes in central GMV observed in patients with
concomitant exotropia without visual acuity abnormalities. The
present study provides a foundation for further investigation into
the changes in relevant central brain areas associated with the
occurrence of concomitant exotropia. However, due to the small
sample size and different disease courses, it remains uncertain
whether other changes and compensatory mechanisms occur in
different brain areas, warranting further research and accumulation
of data.
In the present study, FC patterns of the brain were
investigated in patients with concomitant exotropia and normal
controls. The results of the intra-group analysis indicated that
the FC patterns were similar in both groups, with the bilateral
thalamus showing strong FC with several brain regions. However, the
inter-group analysis revealed decreased FC between the bilateral
thalamus and bilateral precuneus in patients with concomitant
exotropia compared to normal controls. The study also included a
correlation analysis between the clinical variables and brain
imaging measures in the concomitant exotropia group, revealing a
positive correlation between the GMV atrophy value of the bilateral
thalamus and deviation angle.
The present study adds to the growing body of
literature on the neural mechanisms underlying strabismus. Except
for changes in the volume of extraocular muscles (14), the findings suggested that the
pathogenesis of concomitant exotropia may involve central
mechanisms, as well as abnormal development of the central visual
pathway, contributing to the disorder. The results also clarify
another idea that the early correction of ocular position deviation
may help stabilize eye position and prevent abnormal development of
the central visual pathway. However, the limitation of this study
is that the sample size is small and the subjects did not undergo
surgical treatment. Therefore, the corresponding neural changes
pre- and post-operation and at different follow-up times after
surgery cannot be compared. Future studies may build on these
findings by investigating the causal relationships between FC
patterns and clinical variables in patients with concomitant
exotropia, as well as exploring potential interventions aimed at
improving FC and clinical outcomes in this population.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the National Natural
Science Foundation of China (grant no. 81800861), the General
Project of Tianjin Health Science and Technology Fund (grant no.
TJWJ2021MS041), the Natural Science Foundation of Tianjin Grant
(grant no. 22JCZDJC00160), the Scientific Research Foundation of
Tianjin Education Commission (grant no. 2021KJ222) and the Tianjin
Key Medical Discipline (Specialty) Construction Project (grant no.
TJYXZDXK-016A).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RH and YW wrote the manuscript. YW performed the MRI
imaging. RH, YW, KW and AW performed the data analyses. WZ
contributed to the conception of the study and revised the
manuscript. All authors contributed to the article and have read
and approved the final manuscript. RH and YW confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and was approved by the Tianjin Eye
Hospital Committee on Human Research (approval no. 2021046;
Tianjin, China). Written informed consent to participate in this
study was obtained from the participants.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Caoli A, Sabatini SP, Gibaldi A, Maiello
G, Kosovicheva A and Bex P: A dichoptic feedback-based oculomotor
training method to manipulate interocular alignment. Sci Rep.
10(15634)2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
McKean-Cowdin R, Cotter SA, Tarczy-Hornoch
K, Wen G, Kim J, Borchert M and Varma R: Multi-Ethnic Pediatric Eye
Disease Study Group. Prevalence of amblyopia or strabismus in asian
and non-Hispanic white preschool children: Multi-ethnic pediatric
eye disease study. Ophthalmology. 120:2117–2124. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Pathai S, Cumberland PM and Rahi JS:
Prevalence of and early-life influences on childhood strabismus:
Findings from the Millennium Cohort Study. Arch Pediatr Adolesc
Med. 164:250–257. 2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bruce A and Santorelli G: Prevalence and
risk factors of strabismus in a UK Multi-ethnic Birth Cohort.
Strabismus. 24:153–160. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jie Y, Xu Z, He Y, Wang N, Wang J, Lu W,
Wu X and Jiao Y: A 4 year retrospective survey of strabismus
surgery in Tongren Eye Centre Beijing. Ophthalmic Physiol Opt.
30:310–314. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Li JH, Xie WF, Tian JN, Zhang LJ, Cao MM
and Wang L: Changing strabismus surgery distribution at shanxi
province eye hospital in Central China. J Pediatr Ophthalmol
Strabismus. 54:112–116. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Oh SY, Clark RA, Velez F, Rosenbaum AL and
Demer JL: Incomitant strabismus associated with instability of
rectus pulleys. Invest Ophthalmol Vis Sci. 43:2169–2178.
2002.PubMed/NCBI
|
|
8
|
Lueder GT, Dunbar JA, Soltau JB, Lee BC
and McDermott M: Vertical strabismus resulting from an anomalous
extraocular muscle. J AAPOS. 2:126–128. 1998.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ferraina S, Paré M and Wurtz RH: Disparity
sensitivity of frontal eye field neurons. J Neurophysiol.
83:625–629. 2000.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Chan ST, Tang KW, Lam KC, Chan LK, Mendola
JD and Kwong KK: Neuroanatomy of adult strabismus: A voxel-based
morphometric analysis of magnetic resonance structural scans.
Neuroimage. 22:986–994. 2004.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ashburner J and Friston KJ: Voxel-based
morphometry-the methods. Neuroimage. 11:805–821. 2000.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Brodsky MC, Fray KJ and Glasier CM:
Perinatal cortical and subcortical visual loss: Mechanisms of
injury and associated ophthalmologic signs. Ophthalmology.
109:85–94. 2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gunton KB, Wasserman BN and DeBenedictis
C: Strabismus. Prim Care. 42:393–407. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hao R, Suh SY, Le A and Demer JL: Rectus
extraocular muscle size and pulley location in concomitant and
pattern exotropia. Ophthalmology. 123:2004–2012. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Battaglini PP, Battaglia Parodi M, Tiacci
I, Ravalico G and Muzur A: Visual representation of space in
congenital and acquired strabismus. Behav Brain Res. 101:29–36.
1999.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wong AMF, Foeller P, Bradley D, Burkhalter
A and Tychsen L: Early versus delayed repair of infantile
strabismus in macaque monkeys: I. Ocular motor effects. J AAPOS.
7:200–209. 2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Freud E, Plaut DC and Behrmann M: ‘What’
is happening in the dorsal visual pathway. Trends Cogn Sci.
20:773–784. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Maunsell JH and Van Essen DC: Topographic
organization of the middle temporal visual area in the macaque
monkey: Representational biases and the relationship to callosal
connections and myeloarchitectonic boundaries. J Comp Neurol.
266:535–555. 1987.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Albright TD and Desimone R: Local
precision of visuotopic organization in the middle temporal area
(MT) of the macaque. Exp Brain Res. 65:582–592. 1987.PubMed/NCBI View Article : Google Scholar
|
|
20
|
DeAngelis GC and Uka T: Coding of
horizontal disparity and velocity by MT neurons in the alert
macaque. J Neurophysiol. 89:1094–1111. 2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Nguyenkim JD and DeAngelis GC:
Disparity-based coding of three-dimensional surface orientation by
macaque middle temporal neurons. J Neurosci. 23:7117–7128.
2003.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Tootell RB, Hadjikhani NK, Mendola JD,
Marrett S and Dale AM: From retinotopy to recognition: fMRI in
human visual cortex. Trends Cogn Sci. 2:174–183. 1998.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Chino YM, Cheng H, Smith EL III, Garraghty
PE, Roe AW and Sur M: Early discordant binocular vision disrupts
signal transfer in the lateral geniculate nucleus. Proc Natl Acad
Sci USA. 91:6938–6942. 1994.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cheng H, Chino YM, Smith EL III, Hamamoto
J and Yoshida K: Transfer characteristics of X LGN neurons in cats
reared with early discordant binocular vision. J Neurophysiol.
74:2558–2572. 1995.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Moustafa AA, McMullan RD, Rostron B,
Hewedi DH and Haladjian HH: The thalamus as a relay station and
gatekeeper: Relevance to brain disorders. Rev Neurosci. 28:203–218.
2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ouyang J, Yang L, Huang X, Zhong YL, Hu
PH, Zhang Y, Pei CG and Shao Y: The atrophy of white and gray
matter volume in patients with comitant strabismus: Evidence from a
voxel-based morphometry study. Mol Med Rep. 16:3276–3282.
2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yan X, Wang Y, Xu L, Liu Y, Song S, Ding
K, Zhou Y, Jiang T and Lin X: Altered functional connectivity of
the primary visual cortex in adult comitant strabismus: A
resting-state functional MRI study. Curr Eye Res. 44:316–323.
2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Min YL, Su T, Shu YQ, Liu WF, Chen LL, Shi
WQ, Jiang N, Zhu PW, Yuan Q, Xu XW, et al: Altered spontaneous
brain activity patterns in strabismus with amblyopia patients using
amplitude of low-frequency fluctuation: A resting-state fMRI study.
Neuropsychiatr Dis Treat. 14:2351–2359. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Su T, Zhu PW, Li B, Shi WQ, Lin Q, Yuan Q,
Jiang N, Pei CG and Shao Y: Gray matter volume alterations in
patients with strabismus and amblyopia: Voxel-based morphometry
study. Sci Rep. 12(458)2022.PubMed/NCBI View Article : Google Scholar
|