Introduction
Nesidioblastosis refers to the diffuse proliferation
of insulin-secreting cells in the pancreatic duct epithelium and
was first reported by Laidlaw in 1938(1). According to the extent of pancreatic
involvement, nesidioblastosis can be divided into focal
nesidioblastosis, which is characterized by nodular hyperplasia,
and diffuse nesidioblastosis, which involves the whole pancreas
(2). Nesidioblastosis, part of the
disease spectrum of non-insulinomatous pancreatic hypoglycemia
syndrome, is the most common cause of hyperinsulinemic hypoglycemia
in infants and children, but is rare in adults, accounting for only
0.5-7% (3,4). The clinical manifestations and
biochemical examination results of nesidioblastosis and pancreatic
islet cell tumor are similar. The initial symptoms are mainly
dizziness, cold sweating, accompanied by overeating, easy hunger,
combined with repeated consciousness disorders, memory loss, and
decreased reaction ability. Both have a history of hypoglycemic
coma, typical Whipple triple syndrome, and symptoms can be
alleviated by eating multiple meals, taking oral sugar water, or
intravenous glucose, but repeated attacks (2). Specific imaging features for
pancreatic nesidioblastosis are limited in the literature, and
pancreatic nesidioblastosis is often misdiagnosed as insulinoma,
especially the nodular type (5).
Most adult patients with focal nesidioblastosis require surgery.
However, a uniform standard for surgical resection is lacking
(6). The present study reports a
case of hypoglycemia due to nesidioblastosis diagnosed using
dual-nuclide tracers, fluorine-18-fluorodeoxyglucose
(18F-FDG) and gallium-68-labeled
1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic
acid-d-Phel-Tyr3-Thr8-OC (68Ga-DOTATATE), in positron
emission tomography/computed tomography (PET/CT).
Case report
A 48-year-old man with a 5-year history of
dizziness, palpitations, sweating, limb tremors, pale complexion,
disturbance of consciousness, and even coma in the morning on an
empty stomach, presented to the Affiliated Hospital of Zunyi
Medical University (Zunyi, China) in May 2021 due to reoccurrence
and worsening of the aforementioned over the past 2 days. The
patient had been admitted to other hospitals several times, and no
imaging tests, including CT and magnetic resonance imaging (MRI),
had been performed except for abdominal ultrasound, which did not
reveal any suspicious positive lesions. Moreover, the symptoms of
hypoglycemia were relieved each time a glucose solution was
administered, so the patient did not pay much attention to the
condition. The patient had no history of hepatitis, tuberculosis,
surgery or other illnesses. The patient's family members were
healthy and had no genetic or tumor history. No positive signs were
found on a general physical examination. A laboratory examination
revealed that the serum insulin level had increased to 219.3 µIU/ml
(normal reference value, 2.6-24.9 µIU/ml) and the blood glucose
level had decreased to 1.79 mmol/l (normal reference value, 3.9-6.1
mmol/l). Moreover, the fasting C-peptide level significantly
increased to 6,440 pmol/l (normal reference value, 370-1,470
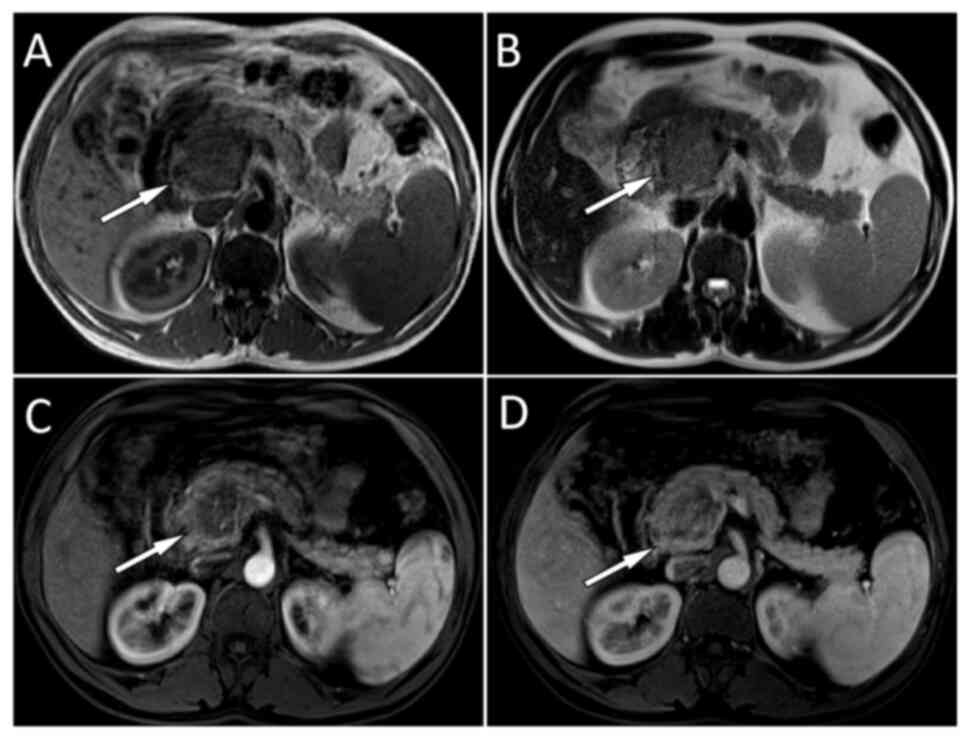
pmol/l). Abdominal MRI (Siemens Sensation 3.0T MR Scanner; Siemens
AG) was performed with the following scanning parameters: For
T1-weighted imaging (T1WI), repetition time (TR) at 100 msec and
echo time (TE) at 2.46 msec; and for T2WI, TR at 1,400 msec and TE
at 81 msec; the scanning layer thickness was 6 mm and layer spacing
was 1 mm; contrast enhanced scanning was performed by intravenous
injection of 0.1 mmol/kg gopentate meglumine. Analysis of the
results revealed an abnormal signal shadow in the pancreatic head
(Fig. 1).
When the MRI results were combined with the
patient's clinical manifestations of hypoglycemia, and increased
insulin and C-peptide levels, an insulinoma was suspected. To
confirm this hypothesis, the patient underwent PET/CT (Biograph mCT
PET/CT scanner; GE Healthcare). According to the patient's weight,
18F-FDG was injected intravenously at 0.12 mCi/kg and
68Ga-DOTATATE was injected intravenously at 0.05 mCi/kg.
18F-FDG PET/CT was performed 24 to 48 h before the
68Ga-DOTATATE PET/CT. The patient underwent imaging
45-60 min post-intravenous injection of the tracers. The scanning
range was from the top of the skull to the middle of the femur. CT
scanning was performed first using the following parameters: Tube
voltage, 120 kV; tube current, 119 mA; and layer thickness, 5 mm.
PET scanning was performed immediately after the completion of CT
scanning. The 3-dimensional acquisition mode was 2.0 min/bed, with
6 to 7 beds. The lesion of the pancreatic head had moderate
18F-FDG uptake, but no 68Ga-DOTATATE uptake
(Fig. 2). Consequently, the
initial diagnosis of an insulinoma was rejected, as insulinomas
usually express somatostatin receptor type 2 and are characterized
by strong uptake of 68Ga-DOTATATE, while
18F-FDG is usually absent or has mild uptake (7). After communicating with the patient
and obtaining consent, the patient underwent a duodeno-sparing
pancreaticocephalic focus excision and pancreaticojejunostomy
(Roux-en-Y anastomosis) with laparoscopic guidance under general
anesthesia in June 2021. The excised lesion tissues were sent for
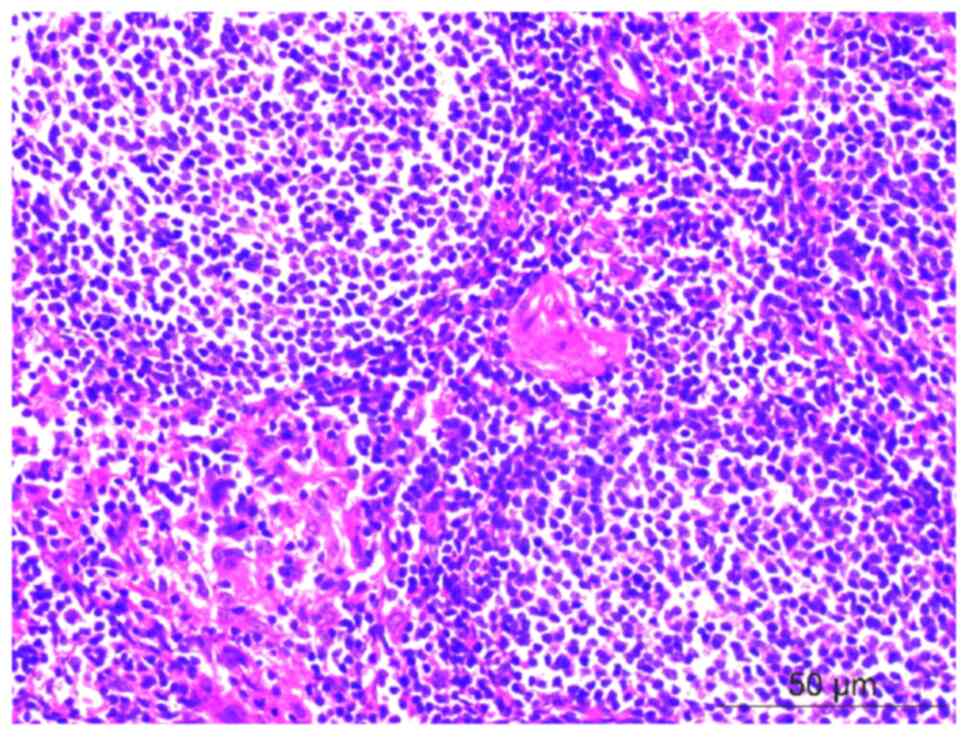
postoperative pathological examination. For hematoxylin-eosin
staining, the specimen was fixed with 10% neutral formalin,
dehydrated at room temperature for ~24 h and paraffin embedded.
Next, 3- to 4-µm thick sections were stained with hematoxylin-eosin
(Fuzhou Maixin Biotech. Co., Ltd.), and viewed at x400
magnification under an optical microscope. The staining revealed a
diffuse distribution of round or oval cells of varying sizes in the
islets with deeply stained nuclei (Fig. 3), suggesting nesidioblastosis. The
patient was treated with cefuroxime (1-2 g per dose, twice a day, 7
days in total) anti-inflammatory therapy 1 week after surgery,
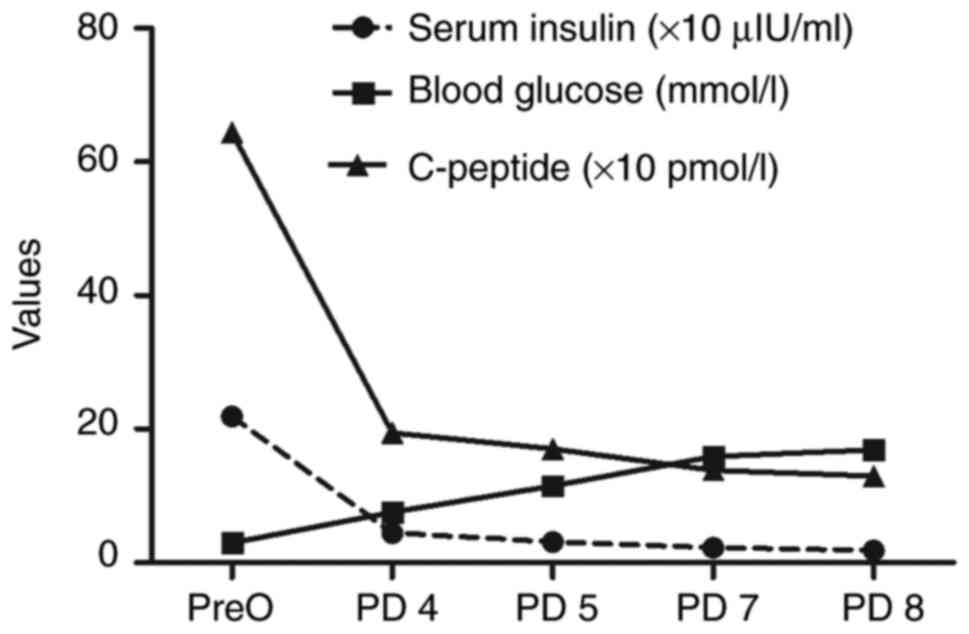
during which time hypoglycemia did not develop. The serum insulin,
blood glucose and C-peptide values returned to normal after surgery
(Fig. 4). The most recent
follow-up was conducted in November 2023 (routinely followed up
every 6 months), and the patient currently has a good prognosis
with no symptoms of hypoglycemia, such as dizziness, palpitations
or sweating.
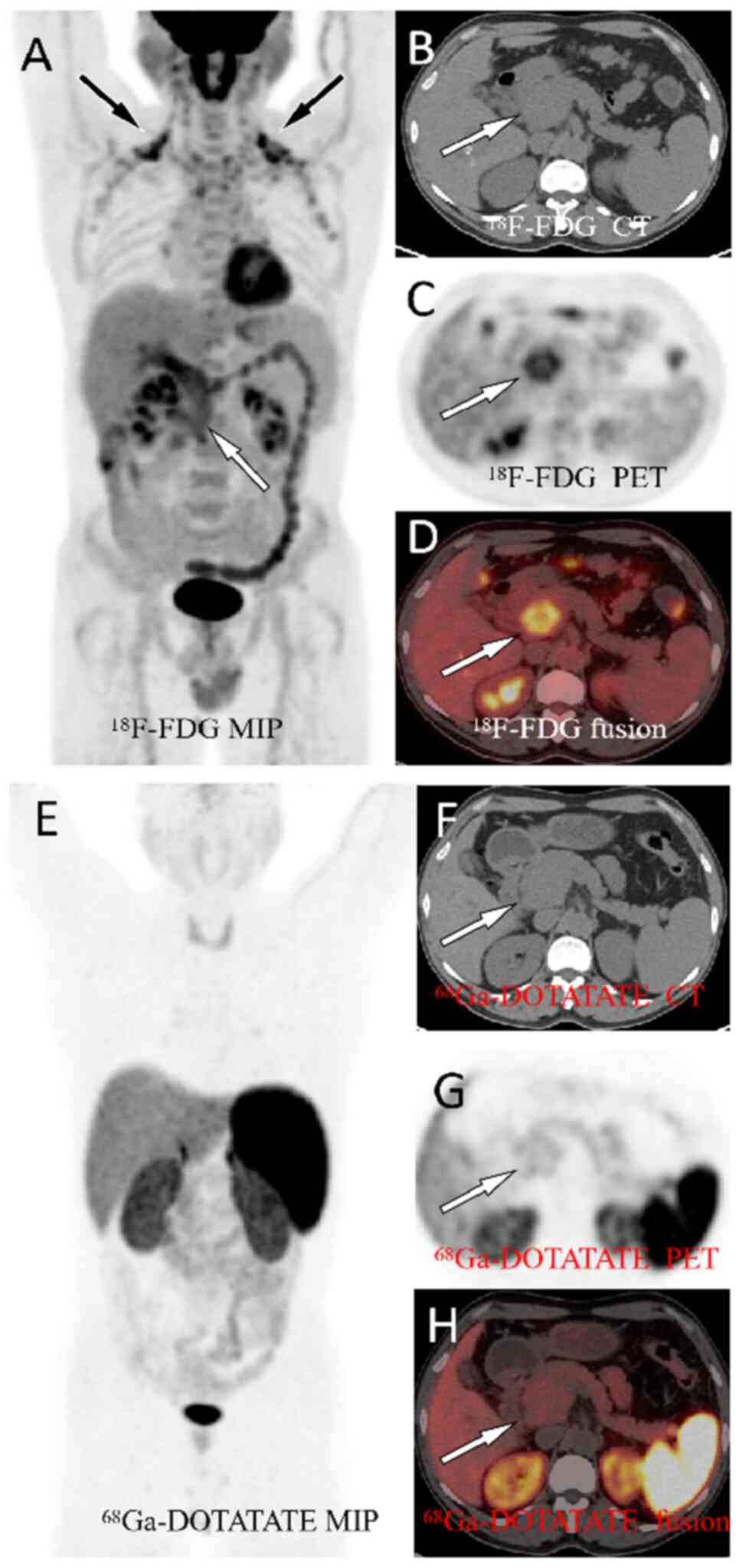 | Figure 2(A) MIP showing 18F-FDG
uptake in the lesion in the pancreatic head region (white arrow).
Moreover, symmetrical non-specific inflammatory uptake was observed
bilaterally in the neck (black arrows). An axial examination
revealed that the volume of the pancreatic head increased with
moderate focal 18F-FDG uptake (arrows), with a maximum
standardized uptake value of 4.2 [(B) CT; (C) PET; and (D) PET/CT
fusion) However, 68Ga-DOTATATE uptake was not observed
in the corresponding areas [(E) MIP; (F) CT; (G) PET and (H) PET/CT
fusion). 18F-FDG, fluorine-18-fluorodeoxyglucose; PET,
positron emission tomography; CT, computed tomography; MIP, maximum
intensity projection; 68Ga-DOTATATE, gallium-68-labeled
1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic
acid-d-Phel-Tyr3-Thr8-OC. |
Discussion
Insulinoma is the most common cause of adult
hyperinsulinemic hypoglycemia, while nesidioblastosis is a rare
cause, accounting for only 0.5-5% of cases (5). The pathogenesis of adult
nesidioblastosis is unknown, but possible causes include β-cell
dysfunction, genetic variation located on chromosome 11, and growth
factor (insulin-like growth factor receptor1 receptor-α and
transforming growth factor-β receptor 3) production and/or
increased expression of its receptors (8-10).
There is overlap between the clinical manifestations of
nesidioblastosis and insulinoma, the initial symptoms of which are
dizziness, chronic obstructive pulmonary disease, sweating,
overeating, and increased hunger; in addition to the above
symptoms, both insulinoma and neidioplastoma can be accompanied by
recurrent consciousness disorders, memory loss, and decreased
responsiveness (11). Both tumors
may present with the classic Whipple's triad of periodic coma and
psychiatric symptoms, usually with daily episodes on an empty
stomach or after exertion; episodes of a blood glucose level
<2.8 mmol/l and the rapid disappearance of symptoms after oral
or intravenous glucose administration are indicative (12). Moreover, the biochemical findings
of nesidioblastosis and insulinoma are similar in that, during the
onset of clinical symptoms, both can be detected as decreased blood
glucose values and abnormally high insulin and C-peptide levels,
making the differential diagnosis of the two relatively difficult
(5). The patient in the current
study presented with recurrent symptoms of hypoglycemia, such as
dizziness, palpitations, sweating, tremors of the limbs, pallor,
impaired consciousness and coma, which were relieved with oral
glucose. At symptom onset, the patient's insulin and C-peptide
levels were significantly elevated, consistent with report in the
literature (5).
Unexplained hypoglycemia in adult non-diabetic
patients requires thorough clinical and laboratory workups
(13). In patients with suspected
hypoglycemia, a 4- to 6-h oral glucose tolerance test and a 72-h
fasting test, and routine monitoring of blood glucose, serum
insulin and C-peptide levels are required to identify pancreatic
hyperinsulinemic hypoglycemia (11). Owing to its rarity, imaging studies
of nesidioblastosis have been poorly reported, resulting in cases
of false-negative pancreatic nesidioblastosis on both CT and MRI
due to isointense or isosignal patterns with a normal pancreatic
parenchyma (14,15). However, typical insulinomas may
show significant round or oval enhancement on contrast CT/MRI,
which lasts longer and can still be seen in the portal phase, thus
aiding the differentiation from nesidioblastosis, but smaller
insulinomas may also be undetectable (16). The current case was isointense to
the normal pancreatic parenchyma on CT; however, on
contrast-enhanced T1WI, the lesion was slightly less isointense
than the normal pancreatic parenchyma signal, which was slightly
inconsistent with the MRI findings of nesidioblastosis reported in
the literature and differed from the obvious enhancement of
insulinomas. The main advantage of nuclear medicine is that
different radiopharmaceuticals can be synthesized for targeted
imaging based on receptors expressed in the lesion.
18F-FDG PET/CT, a common functional imaging technique,
has been widely used in the localization, differential diagnosis,
staging and post-treatment response assessment of a variety of
primary tumors; however, it has shown limited value in the
diagnosis and differential diagnosis of neuroendocrine tumors,
including insulinoma (17).
New imaging techniques in nuclear medicine,
including PET/CT imaging with 68Ga-somatostatin
receptors, such as 68Ga-DOTATATE, and
68Ga-glucagon-like peptide-1 (GLP-1) receptor analogs,
such as 68Ga-DOTA-exendin-4, can facilitate the
localization and diagnosis of insulinoma to distinguish it from
other tumors such as pancreatic cancer and pancreatic cystadenoma
(7,17,18).
Due to the high expression of somatostatin receptors, insulinomas
show significant radioactivity uptake on
68Ga-somatostatin receptor and 68Ga-GLP-1
receptor analog PET/CT imaging (7,19).
Compared with the aforementioned studies, the present study
revealed that dual nuclear tracer PET/CT imaging may become a
differential diagnostic method for the cause of hypoglycemia such
as insulinoma and nesidioblastosis, as nesidoblasts do not express
somatostatin receptors, resulting in no or only slight radioactive
uptake on PET/CT imaging of 68Ga-labeled somatostatin
receptors. The patient's double-tracer PET/CT results showed
moderate 18F-FDG uptake but no 68Ga-DOTATATE
uptake, suggesting only a small possibility of insulinoma and that
nesidioblastosis should be considered. The detailed comparison of
the clinical features and imaging findings of nesidioblastosis and
insulinoma are presented in Table
I.
 | Table IComparison of the clinical features
and imaging findings of nesidioblastosis and insulinoma. |
Table I
Comparison of the clinical features
and imaging findings of nesidioblastosis and insulinoma.
| Parameters | Nesidioblastosis | Insulinoma | (Refs.) |
|---|
| Symptoms | Both conditions can
present with hypoglycemic symptoms, such as dizziness,
palpitations, sweating, trembling limbs, paleness and disturbance
of consciousness | | (11) |
| Prevalence | More common in
infants and children, while less common in adults | More common in
adults | (3,4) |
| Imaging features | | | |
|
CT | Isodense, usually
cannot be displayed | Isodense or
low-density nodules, with significant enhancement on
contrast-enhanced CT | (13,14) |
|
MRI | T1WI shows equal or
slightly low signal, and T2WI shows equal or slightly higher
signal | T1WI shows low signal
and T2WI shows high signal | (15) |
|
PET/CT | Mildly increased
18F-FDG uptake, with no 68Ga DOTATATE
uptake | No or mild increase
in 18F-FDG uptake, strong uptake of
68Ga-DOTATATE | (16-18) |
| Pathological
features | Microscopic
visualization of multiple β-cells with enlarged and deeply stained
nuclei and abundant transparent cytoplasm, the normal spatial
distribution of various cell types in the pancreatic islets and the
absence of endocrine cell proliferative activity | Tumor cells may be
arranged as flowery bands or gyrus, acinoid or Daisy clusters,
solid masses, or diffuse sheets. Different pathological grades of
insulinoma showed different cell atypia, among which G1 grade cell
atypia was low, G3 grade cell atypia was high | (3,20,24) |
The current gold standard for nesidioblastosis
diagnosis is based primarily on the histopathological diagnostic
criteria proposed by Klöppel et al (3). The main criteria include the
exclusion of insulinoma by visual, microscopic and
immunohistochemical examination, including the microscopic
visualization of multiple β-cells with enlarged and deeply stained
nuclei, and abundant transparent cytoplasm, the normal spatial
distribution of the various cell types in the pancreatic islets and
the absence of endocrine cell proliferative activity. Secondary
criteria included an increase in pancreatic islet number and size,
lobulated or irregular islet structures, and multinucleated giant β
cells. Primary criteria must be met for the pathological diagnosis
of nesidioblastosis, and secondary criteria may not be present in
all cases. The pathological examination of the patient in the
present study showed a diffuse distribution of enlarged round or
oval β cells in the pancreatic islets, with deeply stained nuclei
and abundant clear cytoplasm consistent with the diagnosis of
nesidioblastosis. Although a pathological diagnosis is the gold
standard for nesidioblastosis, the present case suggested that dual
nuclear tracer PET/CT imaging is necessary, or even crucial, for
the management of nesidioblastosis, as it can accurately locate the
lesion and guide further puncture biopsy and treatment. However,
68Ga-labeled somatostatin receptor PET/CT imaging can
also produce false-negative results and cannot differentiate
between normal pancreatic uptake, non-insulinomatous pancreatic
hypoglycemia syndrome and postoperative gastric bypass
hypoglycemia. In previous studies, patients affected by these
conditions underwent selective intra-arterial calcium stimulation
with hepatic venous sampling, which can increase the detection rate
(19,20). In addition, the greater medical
cost of dual-nuclide PET/CT imaging compared with MRI is another
disadvantage, but it should still be considered if the patient's
condition requires it.
In patients with nesidioblastosis and hypoglycemia,
a low-carbohydrate diet and medications such as diazoxides, growth
inhibitor analogs, calcium channel antagonists and α-glucosidase
inhibitors may be considered first to improve the symptoms
(21-23).
Most adult patients require surgery, with one study revealing that
total resection of the pancreatic lesion or subtotal pancreatectomy
including the lesion has a 70% probability of normalizing blood
glucose levels and an 8% risk of secondary diabetes (6). The blood glucose level of the present
patient returned to normal soon after surgical removal of the
lesion. At present, the patient has not experienced hypoglycemia
such as dizziness, palpitations, or sweating again.
In conclusion, nesidioblastosis is a rare cause of
hypoglycemia in adults and should be considered in the differential
diagnosis of insulinomas. Dual-nuclide PET/CT tracers can help
differentiate nesidioblastosis from insulinomas, both of which may
present no or mild to moderate 18F-FDG uptake.
Insulinomas present with strong 68Ga-DOTATATE uptake,
whereas nesidioblastosis does not.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed in the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
GZ, LX and XH conceived and designed the study. XH
acquired, analyzed and interpreted the data. GZ and LX confirm the
authenticity of all the raw data. GZ drafted the manuscript. XH
critically revised the manuscript for intellectual content and
approved the final version for publication. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Laidlaw GF: Nesidioblastoma, the islet
tumor of the pancreas. Am J Pathol. 14:125–134.5. 1938.PubMed/NCBI
|
|
2
|
García-Santos EP, Manzanares-Campillo Mdel
C, Padilla-Valverde D, Villarejo-Campos P, Gil-Rendo A,
Muñoz-Atienza V, Sánchez-García S, Puig-Rullán AM,
Rodríguez-Peralto JL and Martín-Fernández J: Nesidioblastosis. A
case of hyperplasia of the islets of Langerhans in the adult.
Pancreatology. 13:544–548. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Klöppel G, Anlauf M, Raffel A, Perren A
and Knoefel WT: Adult diffuse nesidioblastosis: Genetically or
environmentally induced? Hum Pathol. 39:3–8. 2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yamada Y, Kitayama K, Oyachi M, Higuchi S,
Kawakita R, Kanamori Y and Yorifuji T: Nationwide survey of
endogenous hyperinsulinemic hypoglycemia in Japan (2017-2018):
Congenital hyperinsulinism, insulinoma, non-insulinoma
pancreatogenous hypoglycemia syndrome and insulin autoimmune
syndrome (Hirata's disease). J Diabetes Investig. 11:554–563.
2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Anlauf M, Wieben D, Perren A, Sipos B,
Komminoth P, Raffel A, Kruse ML, Fottner C, Knoefel WT, Mönig H, et
al: Persistent hyperinsulinemic hypoglycemia in 15 adults with
diffuse nesidioblastosis: Diagnostic criteria, incidence, and
characterization of beta-cell changes. Am J Surg Pathol.
29:524–533. 2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Witteles RM, Straus II FH, Sugg SL, Koka
MR, Costa EA and Kaplan EL: Adult-onset nesidioblastosis causing
hypoglycemia: An important clinical entity and continuing treatment
dilemma. Arch Surg. 136:656–663. 2001.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Prasad V, Sainz-Esteban A, Arsenic R,
Plöckinger U, Denecke T, Pape UF, Pascher A, Kühnen P, Pavel M and
Blankenstein O: Role of (68)Ga somatostatin receptor PET/CT in the
detection of endogenous hyperinsulinaemic focus: An explorative
study. Eur J Nucl Med Mol Imaging. 43:1593–1600. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Dravecka I and Lazurova I:
Nesidioblastosis in adults. Neoplasma. 61:252–256. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Glaser B, Chiu KC, Anker R, Nestorowicz A,
Landau H, Ben-Bassat H, Shlomai Z, Kaiser N, Thornton PS, Stanley
CA, et al: Familial hyperinsulinism maps to chromosome 11p14-15.1,
30 cM centromeric to the insulin gene. Nat Genet. 7:185–188.
1994.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Rumilla KM, Erickson LA, Service FJ, Vella
A, Thompson GB, Grant CS and Lloyd RV: Hyperinsulinemic
hypoglycemia with nesidioblastosis: Histologic features and growth
factor expression. Mod Pathol. 22:239–245. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Dieterle MP, Husari A, Prozmann SN,
Wiethoff H, Stenzinger A, Röhrich M, Pfeiffer U, Kießling WR, Engel
H, Sourij H, et al: Diffuse, adult-onset
nesidioblastosis/non-insulinoma pancreatogenous hypoglycemia
syndrome (NIPHS): Review of the literature of a rare cause of
hyperinsulinemic hypoglycemia. Biomedicines.
11(1732)2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ahmed FW, Majeed MS and Kirresh O:
Non-Diabetic Hypoglycemia. In: StatPearls [Internet]. Treasure
Island (FL): StatPearls Publishing; 2023.
|
|
13
|
Geraghty M, Draman M, Moran D, Muldoon C,
Reynolds JV and Cullen MJ: Hypoglycaemia in an adult male: A
surprising finding in pursuit of insulinoma. Surgeon. 6:57–60.
2008.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Starke A, Saddig C, Kirch B, Tschahargane
C and Goretzki P: Islet hyperplasia in adults: Challenge to
preoperatively diagnose non-insulinoma pancreatogenic hypoglycemia
syndrome. World J Surg. 30:670–679. 2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Doi S, Yamada T, Kito Y, Obara S, Fujii Y,
Nishimura T, Kato T, Nakayama H, Tsutsumi M and Okamura R:
Adult-Onset Focal Nesidioblastosis With Nodular Formation Mimicking
Insulinoma. J Endocr Soc. 6(bvab185)2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Mehrabi A, Fischer L, Hafezi M,
Dirlewanger A, Grenacher L, Diener MK, Fonouni H, Golriz M,
Garoussi C, Fard N, et al: A systematic review of localization,
surgical treatment options, and outcome of insulinoma. Pancreas.
43:675–686. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Hu X, Li D, Wang R, Wang P and Cai J:
Comparison of the application of 18F-FDG and 68Ga-DOTATATE PET/CT
in neuroendocrine tumors: A retrospective study. Medicine
(Baltimore). 102(e33726)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Deroose CM, Hindié E, Kebebew E, Goichot
B, Pacak K, Taïeb D and Imperiale A: Molecular imaging of
gastroenteropancreatic neuroendocrine tumors: Current status and
future directions. J Nucl Med. 57:1949–1956. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kalff V, Iravani A, Akhurst T, Pattison
DA, Eu P, Hofman MS and Hicks RJ: Utility of
68Ga-DOTA-Exendin-4 positron emission
tomography-computed tomography imaging in distinguishing between
insulinoma and nesidioblastosis in patients with confirmed
endogenous hyperinsulinaemic hypoglycaemia. Intern Med J.
51:1657–1664. 2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Antwi K, Hepprich M, Müller NA, Reubi JC,
Fani M, Rottenburger C, Nicolas G, Kaul F, Christ ER and Wild D:
Pitfalls in the detection of insulinomas with glucagon-like
peptide-1 receptor imaging. Clin Nucl Med. 45:e386–e392.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Dauriz M, Maneschi C, Castelli C,
Tomezzoli A, Fuini A, Landoni L, Malleo G, Ferdeghini M, Bonora E
and Moghetti P: A case report of insulinoma relapse on background
nesidioblastosis: A rare cause of adult hypoglycemia. J Clin
Endocrinol Metab. 104:773–778. 2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Arao T, Okada Y, Hirose A and Tanaka Y: A
rare case of adult-onset nesidioblastosis treated successfully with
diazoxide. Endocr J. 53:95–100. 2006.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Demartin S, Goffette P, Christ E, Freitag
MT, Maiter D and Maria Furnica R: Adult-onset nesidioblastosis: A
challenging diagnosis revealed by glucagon-like-peptide-1 receptor
imaging. Endocrinol Diabetes Metab Case Rep. 2022:22–0325.
2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Nagtegaal ID, Odze RD, Klimstra D, Paradis
V, Rugge M, Schirmacher P, Washington KM, Carneiro F and Cree IA:
WHO Classification of Tumours Editorial Board. The 2019 WHO
classification of tumours of the digestive system. Histopathology.
76:182–188. 2020.PubMed/NCBI View Article : Google Scholar
|