Introduction
Traumatic Brain Injury (TBI) is an acute
neurological event that may lead to complications such as ischemia,
edema and inflammatory responses and is associated with significant
morbidity and mortality (1). TBI
is considered a major cause of mortality and disability worldwide,
with an estimated 10 million individuals affected annually and a
significant socioeconomic burden (2).
Managing a patient with TBI is complex and this
complexity is further accentuated in patients with concurrent
anticoagulant therapy, routinely prescribed for atrial
fibrillation, deep vein thrombosis, pulmonary embolism and certain
cardiac diseases (3). With an
aging population and the growing prevalence of cardiovascular
diseases, the intersection of anticoagulation therapy and TBI is
becoming increasingly commonplace in clinical practice (4).
Anticoagulant medications primarily work by
interrupting the coagulation cascade, thereby preventing clot
formation. However, in the event of trauma, especially TBI, this
anticoagulated state can exacerbate intracranial hemorrhage (ICH)
and potentially amplify the severity of injury (5). Expanding hematomas post-TBI are of
particular concern, as they can lead to increased intracranial
pressure and may affect cerebral perfusion. Therefore, outcomes of
TBI in patients who receive anticoagulation therapy are potentially
complicated by the need for the reversal of anticoagulation, timely
surgical interventions and potential complications from hemorrhagic
progression (6).
Several studies have explored the effect of prior
anticoagulation on TBI outcomes with inconclusive results. While
some studies report an amplified risk of adverse outcomes,
including increased ICH, extended hospital stays and elevated
mortality rates (5,7), others suggest that with meticulous
management, outcomes in anticoagulated patients with TBI can be
comparable to those of non-anticoagulated patients (6,8).
Nursing care plays a pivotal role in managing
patients with TBI, especially those on anticoagulant therapy. The
meticulous monitoring, timely interventions and patient education
provided by nurses can influence patient outcomes, potentially
reducing complications and promoting recovery. Recognizing and
understanding the interplay between anticoagulation and TBI is,
therefore, paramount for optimizing nursing care of these
patients.
The current study aimed to critically evaluate the
effect of prior anticoagulation therapy on outcomes post-TBI to
provide clinicians and nurses with evidence-based guidance in
managing this group of patients. It distinguished itself from prior
analyses by incorporating a comprehensive, up-to-date dataset that
included recent studies not previously evaluated.
Materials and methods
Study protocol registration
The study protocol is registered at PROSPERO, the
number is CRD42023470867.
Eligibility criteria. Population
The analysis centered on studies that included
individuals diagnosed with TBI, without restrictions based on age,
gender, ethnicity, or geographical location.
Intervention group. Patients who had been on
anticoagulation therapy prior to TBI (i.e., occurrence of TBI in
patients who are actively taking anticoagulants at the time of
injury).
Comparison group. This group consisted of
patients with TBI who were not on anticoagulation therapy.
Outcomes. The primary objective was to
compare the outcomes between patients with TBI with prior
anticoagulation and those without, particularly focusing on overall
mortality, in-hospital mortality, length of hospital stay, length
of intensive care unit (ICU) stay, need for neurosurgical
intervention and discharge rate.
Study design. The present study incorporated
cohort and case-control studies written in English, from the
commencement of database records up to September 2023.
Peer-reviewed articles and grey literature were both evaluated to
minimize publication bias.
Information sources
A comprehensive search was performed in PubMed
(https://pubmed.ncbi.nlm.nih.gov), Embase
(https://www.embase.com/search/),
Cochrane Central Register of Controlled Trials (CENTRAL)
(https://www.cochranelibrary.com/advanced-search),
Scopus (https://www.scopus.com/search/) and CINAHL (https://www.ebsco.com/products/research-databases/cinahl-database)
databases. Reference lists of relevant papers and reviews were also
manually inspected. Authors were contacted as needed for additional
data or to seek clarifications. Key words such as ‘traumatic brain
injury’, ‘anticoagulation’, ‘warfarin’, ‘direct oral
anticoagulants’ and ‘outcomes’ were integrated, leveraging both
Medical Subject Headings (MeSH) and related keywords. Filters were
applied for English language publications and to only include
articles up to September 2023.
Study records. Data management
EndNote X9 was utilized for managing and
categorizing the identified articles. After the elimination of
duplicate entries, the remaining studies were systematically
evaluated for relevance.
Selection process. Two separate reviewers
preliminary reviewed titles and abstracts of identified studies and
full texts of potentially eligible articles were examined. Any
disparities in selection were resolved through discussion between
the two reviewers. The present study was planned and executed based
on the Preferred Reporting Items for Systematic Reviews and
Meta-Analyses (PRISMA) 2020 protocol (9).
Data collection process. The two reviewers
independently extracted critical data using pre-established format.
The extracted data included study details, participant
demographics, details of anticoagulation therapy and outcome
measures. Information pertaining to the funding source and possible
conflicts of interest were also recorded.
Risk of bias assessment
The Newcastle Ottawa Scale (NOS) was used for the
evaluation of the risk of bias within the incorporated studies
(10). The NOS assesses potential
biases across three major domains: selection, comparability and
outcome. Studies are scored (0-9) based on the risk of bias, with
higher scores indicating lower risk of bias. Each study was
individually evaluated using the NOS and any discrepancies between
the reviewers in scoring were reconciled through discussion between
the two reviewers. The aggregate scores provided an overview of the
overall quality and potential biases inherent in the included
studies.
Data synthesis
STATA version 14.2 (StataCorp LP). was used for
statistical analysis. Meta-analysis was performed when studies
exhibited adequate homogeneity. Using a random-effects model,
pooled effect sizes i.e., odds ratio (OR) with 95% confidence
interval (CI) were determined. I2 statistic was used to
assess heterogeneity among the included studies (11). In cases of high heterogeneity,
subgroup analyses were executed based on variables such as severity
of TBI and patient age. Publication bias assessment was conducted
by funnel plots and Egger's regression test for outcomes having at
least 10 studies (11). The
consolidated findings were visualized using forest plots.
Results
Search results
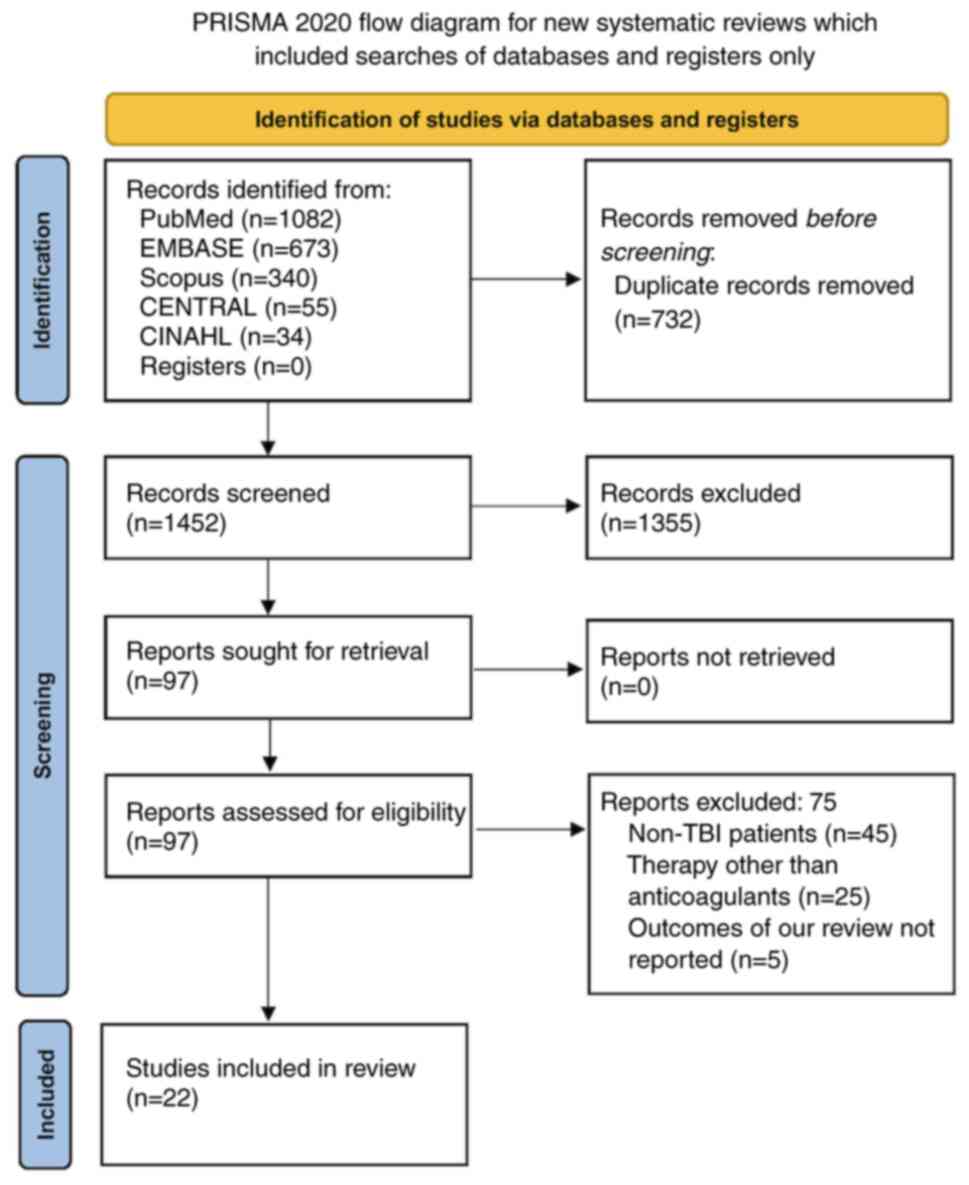
Initial literature search of databases identified
2,184 records. Of them, 732 duplicates were removed. Of the
remaining 1,452 records, 1,355 were excluded (reasons included
details on how differences in participant characteristics, outcome
measures and exposure types influenced the exclusion of records
from our analysis) and 97 full-text articles were assessed for
eligibility. Finally, 22 studies met the inclusion criteria (i.e.,
studies on patients with TBI, covering all ages, ethnicities,
locations and both sexes, comparing those on anticoagulation
therapy at injury time to those who were not, focusing on mortality
rates, hospital and ICU stay lengths, neurosurgical intervention
need and discharge rates, using cohort and case-control studies in
English up to September 2023, including peer-reviewed and grey
literature; Fig. 1) (5,12-32).
Characteristics of the included
studies
General characteristics of included studies are
summarized in Table I. Most
studies were from the USA, spanning from 2001-2023 and evaluated
the impact of various anticoagulants, [warfarin, direct oral
anticoagulants (DOAC) and vitamin K antagonists] on patients with
TBI. Multiple study designs were present, with retrospective cohort
studies being most prevalent. The sample sizes varied
significantly, ranging from a 48 to 57,056. Age groups mainly
included older adults (18 to ≥65 years). While several studies
reported data of TBI with various severities, some had specific
focus groups such as mild or moderate to severe TBI. The mean age
of participants varied across studies. DOAC users were typically
older (average age of 70-84 years). Sex distributions exhibited
diversity, with some studies showing a slight male predominance. Of
22 included studies, 11 had a high risk of bias, constituting ~42%
of the total studies assessed (Table
I).
 | Table ICharacteristics of included
studies. |
Table I
Characteristics of included
studies.
| First author(s),
year | Country | Type of
anticoagulant | Study design | Sample size | Age group of the
study participants | Inclusion of
participants based on Severity of TBI | Follow up
duration | Mean age (in
years) | Sex distribution
Male/Female | Risk of bias | (Refs.) |
|---|
| Ahmed et al,
2009 | USA |
Warfarin/heparin | Retrospective
cohort | 68 | ≥18 years | All TBI | NR | OAC=74.6 | OAC=2/3 | Low | (32) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=77.9 | OAC=33/30 | | |
| Batey et al,
2018 | USA | Warfarin, DOAC | Retrospective
cohort | 700 | ≥65 years | All TBI | In-hospital
outcomes | OAC=81 | OAC=83/94 | High | (15) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=81 | OAC=235/288 | | |
| Bazzi et al,
2023 | USA | Warfarin, DOAC | Retrospective | 1,591 | ≥18 years | All TBI | In-hospital
outcomes | OAC=76.13 | OAC= 92/47 | Low | (16) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=50.12 | OAC=836/346 | | |
| Beynon et
al, 2015 | Germany | Phenprocourmon,
rivaroxaban | Retrospective
cohort | 48 | ≥65 years | Mild TBI | In-hospital
outcomes | OAC=72.4 | OAC=6/5 | High | (25) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=60 | OAC=15/22 | | |
| Della Pepa et
al, 2022 | Italy | DOAC | Retrospective | 301 | >18 years | Mild TBI | In-hospital
outcomes | OAC=84 | OAC=9/14 | Low | (13) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=80 | OAC=137/116 | | |
| Fakhry et
al, 2021 | USA | Warfarin,
rivaroxaban | Retrospective | 33,710 | ≥65 years | All TBI | In-hospital
outcomes | OAC=NR | OAC= NR | High | (12) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=NR | OAC=NR | | |
| Fortuna et
al, 2008 | USA | Warfarin | Retrospective
cohort | 279 | ≥50 years | All TBI | In-hospital
outcomes | OAC=78.3 | OAC=NR | High | (27) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=66.4 | OAC=NR | | |
| Gavrila Laic et
al, 2023 | Belgium | DOAC | Retrospective
cohort | 1,371 | ≥65 years | All TBI | 1 month | OAC=NR | OAC= NR | High | (19) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=NR | OAC=NR | | |
| Grandhi et
al, 2015 | USA | Warfarin | Retrospective
cohort | 719 | ≥65 years | All TBI | In-hospital
outcomes | OAC=80.2 | OAC=NR | Low | (24) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=79.8 | OAC=NR | | |
| Hon 2016 et
al, 2016 | USA | Warfarin | Case control
study | 1,400 | ≥22 years | All TBI | In-hospital
outcomes | OAC=77.1 | OAC=346/354 | High | (30) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=76.7 | OAC=372/328 | | |
| Karni et al,
2001 | USA | Warfarin | Retrospective
cohort | 273 | ≥65 years | All TBI | NR | OAC=70 | OAC=8/8 | Low | (31) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=70.3 | OAC =102/155 | | |
| Krueger et
al, 2020 | USA | Warfarin,
rivaroxaban | Retrospective | 111 | >18 years | All TBI | In-hospital
outcomes | OAC=NR | OAC=NR | Low | (21) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC =NR | OAC =NR | | |
| Nederpelt et
al, 2022 | Netherlands | DOAC | Prospective | 1,724 | ≥65 years | All TBI | In-hospital
outcomes | OAC=83 | OAC=33/23 | Low | (29) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=81 | OAC=602/635 | | |
| O'Donohoe et
al, 2022 | Australia | Warfarin, DOAC,
apixaban, dabigatran, rivaroxaban | Retrospective | 81 | ≥65 years | Moderate and severe
TBI | 1 month | OAC=82.4 | OAC=13/12 | Low | (28) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC =75.34 | OAC=31/25 | | |
| Peck et al,
2014 | USA | Warfarin | Retrospective
cohort | 312 | ≥55 years | All TBI | In-hospital
outcomes | OAC=78.7 | OAC= 20/19 | High | (5) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=74.9 | OAC=140/133 | | |
| Pieracci et
al, 2007 | USA | Warfarin | Retrospective
cohort | 225 | ≥65 years | All TBI | NR | OAC=80.6 | OAC= 17/23 | Low | (14) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=79.2 | OAC=77/108 | | |
| Posti et al,
2022 | Finland | DOAC, vitamin K
antagonist | Retrospective | 57,056 | ≥18 years | All TBI | 1 month | OAC=78.9 | OAC=2067/1986 | High | (17) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=61.4 |
OAC=29439/23037 | | |
| Prexl et al,
2018 | Austria |
Pheonprocoumon/DOAC | Retrospective
cohort | 145 | ≥60 years | All TBI | NR | OAC=80.3 | OAC= 29/36 | Low | (26) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=73.2 | OAC=48/32 | | |
| Rønning et
al, 2021 | Norway | DOAC, vitamin K
antagonist | Retrospective | 830 | ≥65 years | All TBI | 1 month | OAC=81 | OAC= 106/66 | High | (18) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=73 | OAC=195/165 | | |
| Senft et al,
2009 | Germany | Phenprocoumon | Retrospective
cohort | 107 | ≥21 years | All TBI | 6 months | OAC=72.4 | OAC= 6/5 | High | (20) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=59.9 | OAC =NR | | |
| Tollefsen et
al, 2018 | Norway | Warfarin | Retrospective
cohort | 141 | ≥50 years | Moderate and Severe
TBI | 6 months | OAC=73.2 | OAC=14/6 | High | (22) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC=63.7 | OAC=80/41 | | |
| Wettervik et
al, 2021 | Sweden | Vitamin K
antagonist | Retrospective | 844 | ≥15 years | All TBI | 6 months | OAC=NR | OAC=NR | Low | (23) |
| | | | | | | | | No | No | | |
| | | | | | | | | OAC =NR | OAC =NR | | |
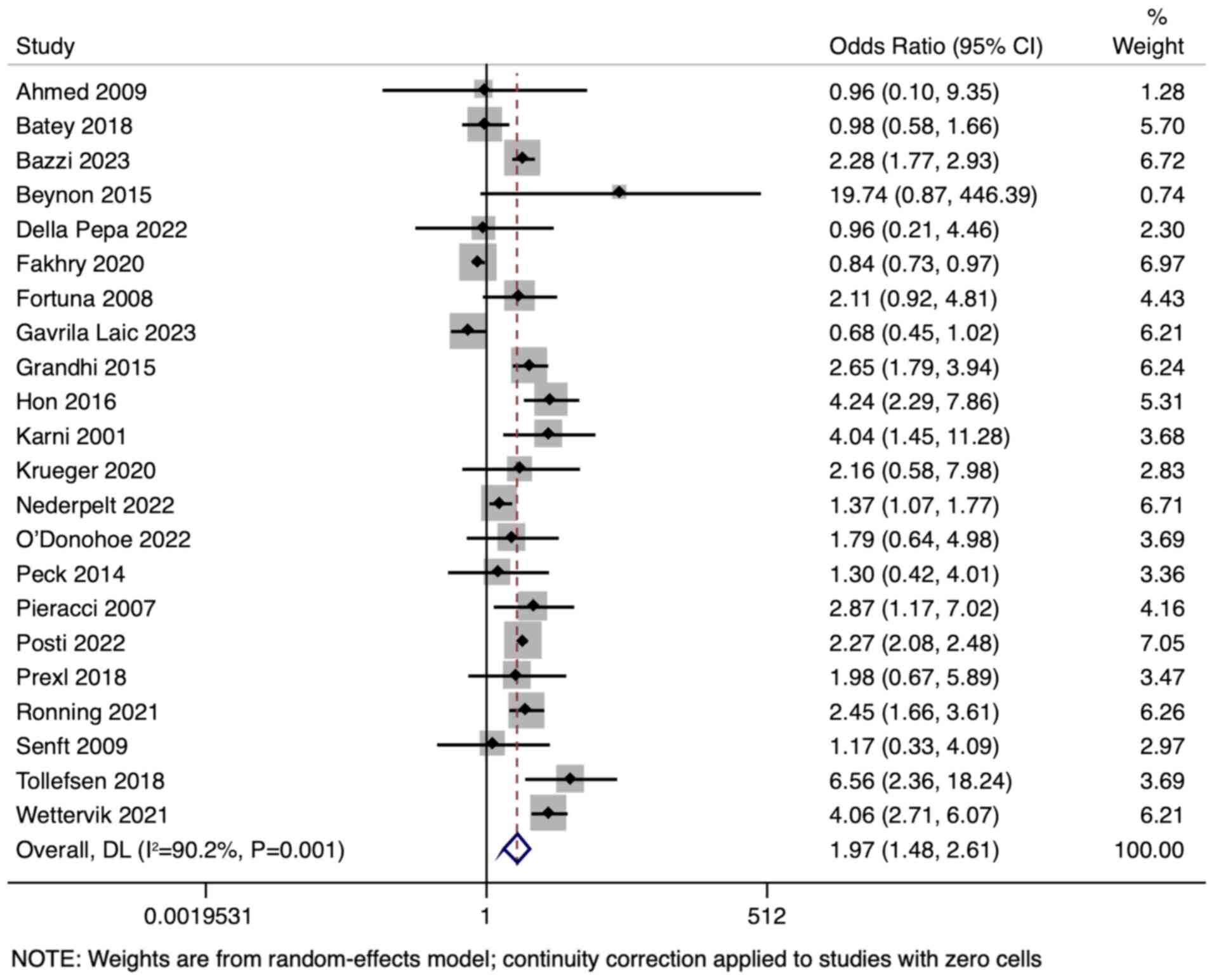
Overall mortality
Risk of overall mortality in patients with TBI with
and without prior anticoagulant therapy was reported in all 22
included studies. The pooled OR was 1.967 (95% CI 1.481-2.613),
with a significant test for the overall effect (z=4.673,
P<0.001), indicating a statistically higher risk of overall
mortality in patients with TBI with prior anticoagulant therapy
(Fig. 2). The heterogeneity among
the included studies was notably high with a Cochran's Q value of
214.57 (df=21; P<0.001) and an I² statistic of 90.2%, suggesting
that 90.2% of the total variation in study estimates was due to
heterogeneity rather than chance. Funnel plot indicated no
significant publication bias (Fig.
S1).
The subgroup analysis based on the age included 14
studies involving 40,558 participants aged ≥50 years. The OR for
mortality in anticoagulated patients with TBI of this age group was
1.776 (95% CI 1.249-2.525), a statistically significant finding
compared with patients with no prior anticoagulation treatment
(z=3.199; P=0.001).
A subgroup analysis based on the severity of TBI was
then performed. The subgroup analysis of patients with mild TBI
included three studies with a total of 32,795 participants. The
pooled OR for mortality in patients with TBI with prior
anticoagulant therapy compared with those without was 1.498 (95% CI
0.633-3.541). This result was not statistically significant
(z=0.920; P=0.358). This suggested that in patients with mild TBI,
prior anticoagulant therapy does not significantly influence the
risk of overall mortality.
The analysis focusing on patients with moderate TBI
included two studies, with the pooled OR of 2.660 (95% CI
0.150-47.111). This result was not statistically significant
(z=0.667, P=0.505).
The subset analysis for patients with severe TBI
included pooled data from two studies. The combined OR for
mortality in this subgroup of patients with TBI who received prior
anticoagulant therapy was 0.667 (95% CI 0.470-0.948). This result
was statistically significant (z=-2.255, P=0.024), indicating that
among patients with severe TBI, prior anticoagulant therapy is
associated with a decreased risk of overall mortality.
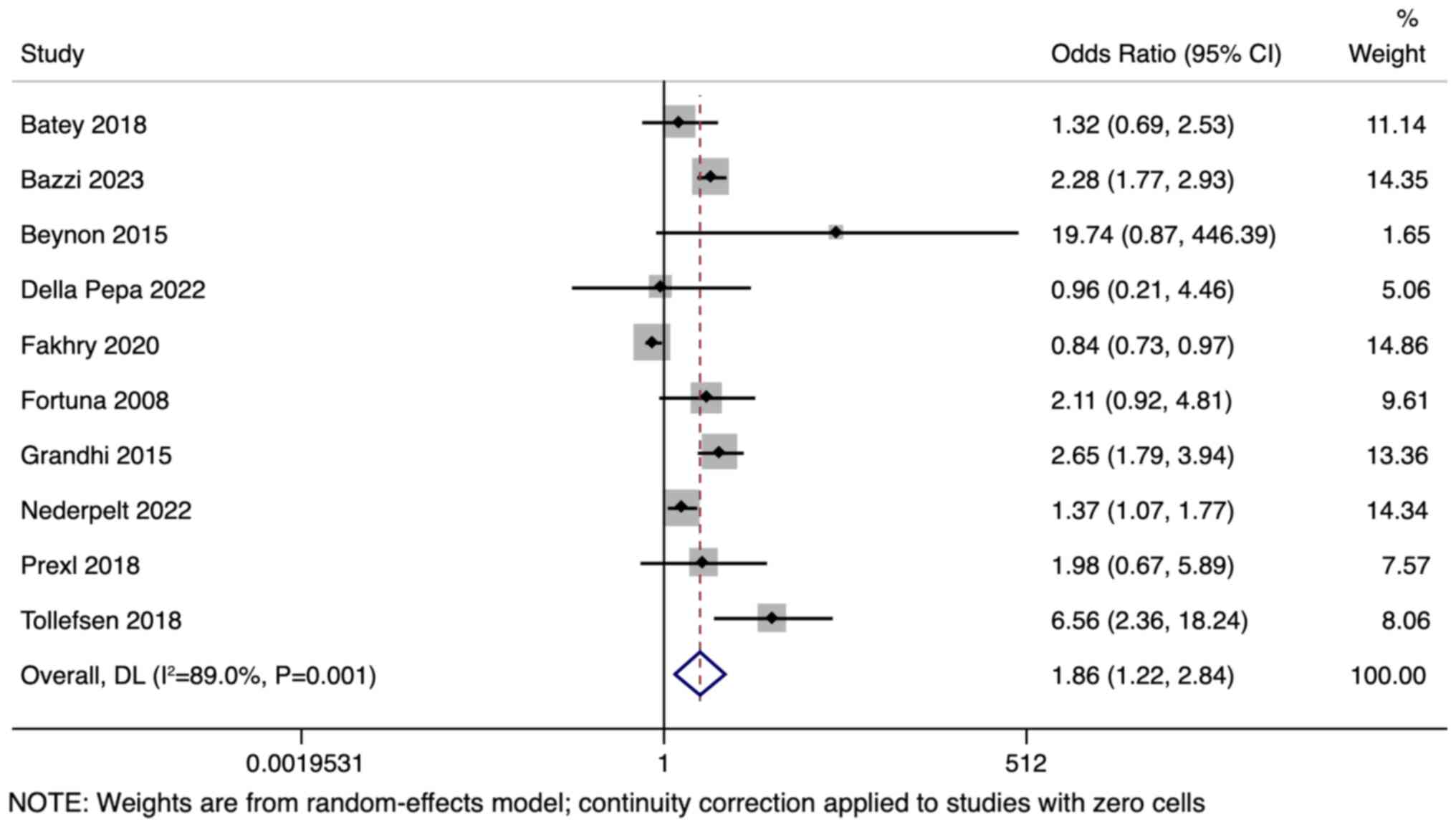
In-hospital mortality
A total of 10 studies with 39,358 participants
reported data on in-hospital mortality. The pooled OR of 1.860 (95%
CI: 1.216-2.843) indicated that the risk of in-hospital mortality
was significantly higher in anticoagulated patients with TBI
compared with the control group (z=2.864; P=0.004; Fig. 3). Significant heterogeneity was
observed among the included studies, with an I² value of 89.0% and
Cochran's Q of 81.65 (P<0.0001). Funnel plot indicated potential
publication bias with Egger's significance level of P=0.080
(Fig. S2).
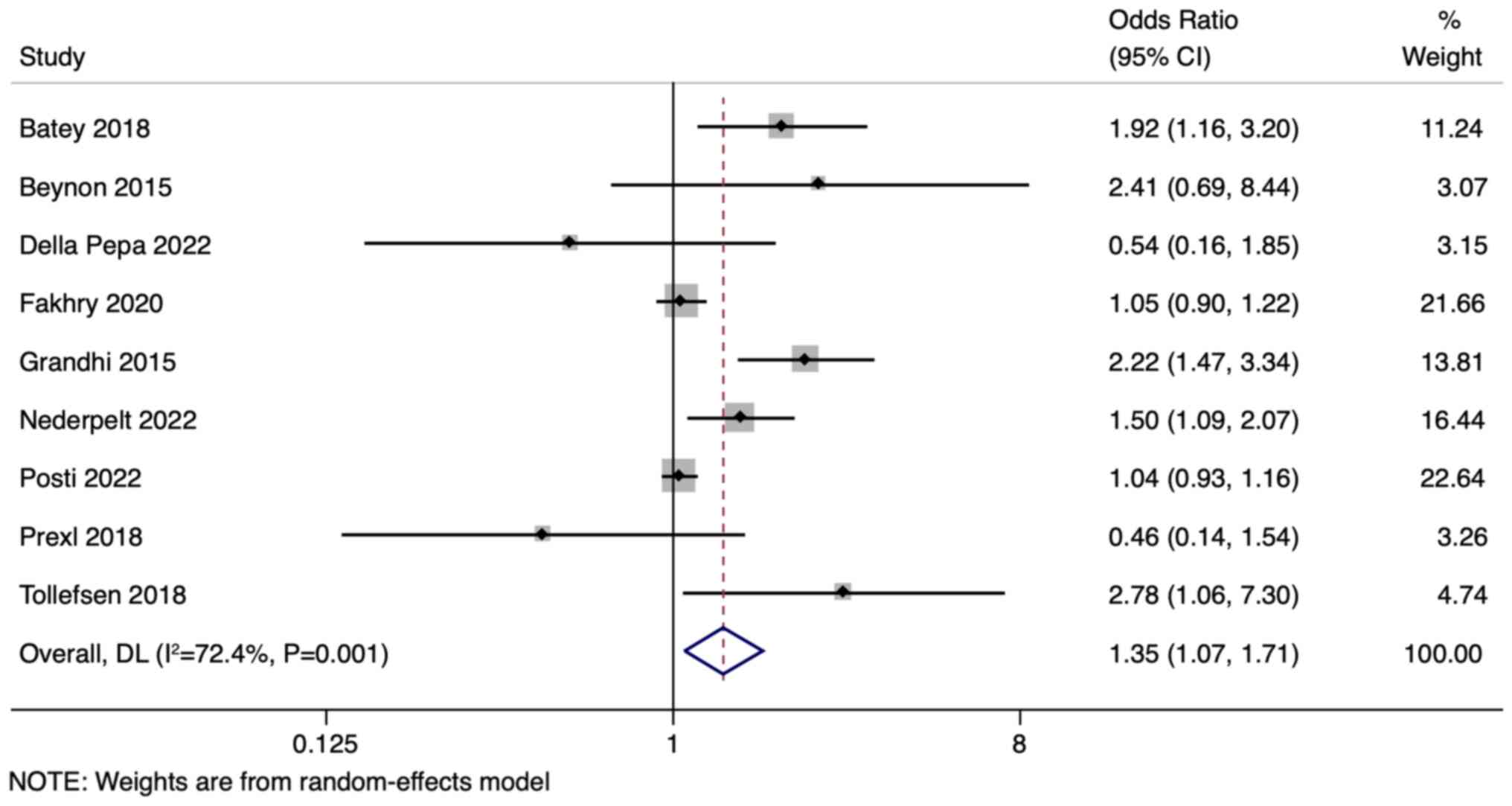
Need for neurosurgical
intervention
A total of nine studies, encompassing 94,517
participants, evaluated the need for neurosurgical intervention.
The pooled OR was 1.351 (95% CI: 1.068-1.708; P=0.012), suggesting
a statistically significant increased likelihood of requiring
neurosurgical intervention in patients with TBI with prior
anticoagulant therapy (Fig. 4).
Notably, significant heterogeneity was observed across the studies
(I²=72.4%; P<0.001).
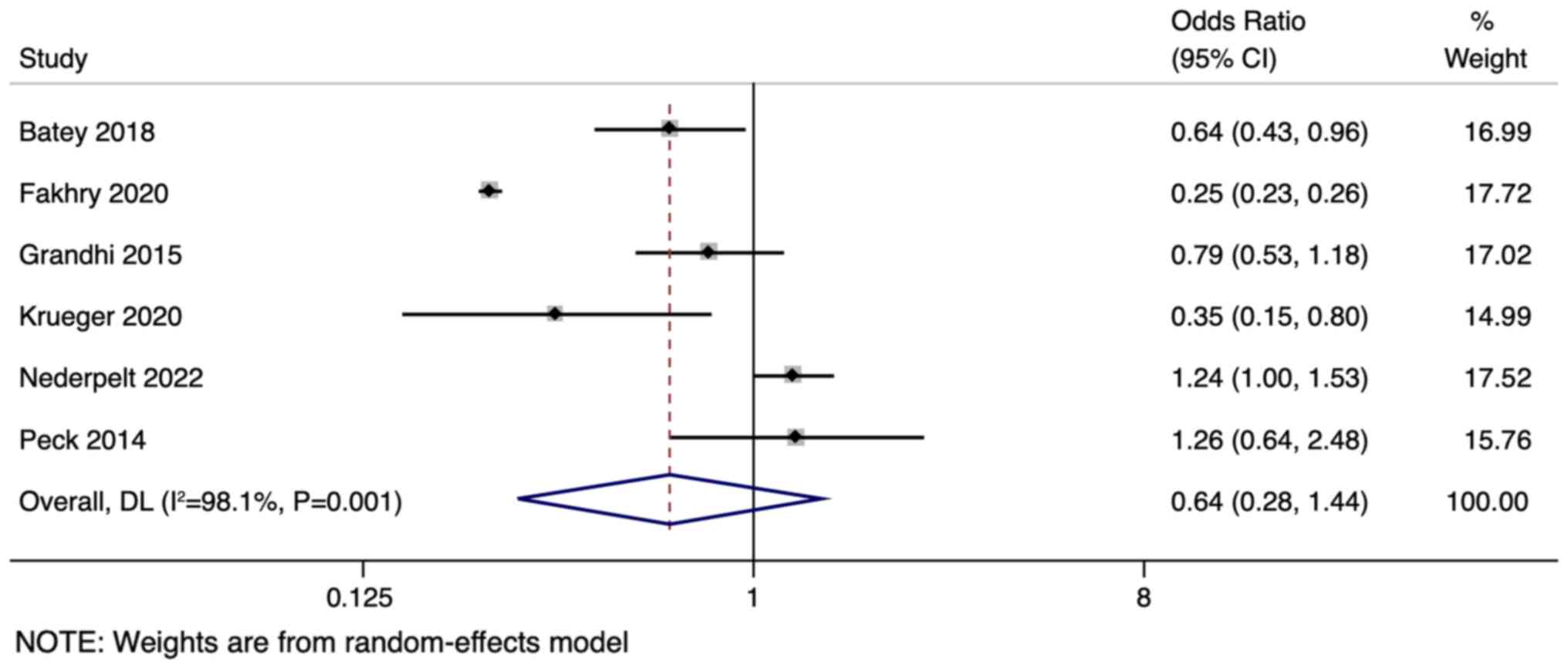
Discharge rate
In six studies involving 37,158 participants that
reported data on the discharge rates, the combined OR was 0.639
(95% CI: 0.285-1.437; P=0.279), indicating no significant
difference in the discharge rates (Fig. 5). There was substantial
heterogeneity among the studies with an I² value of 98.1%
(P<0.001).
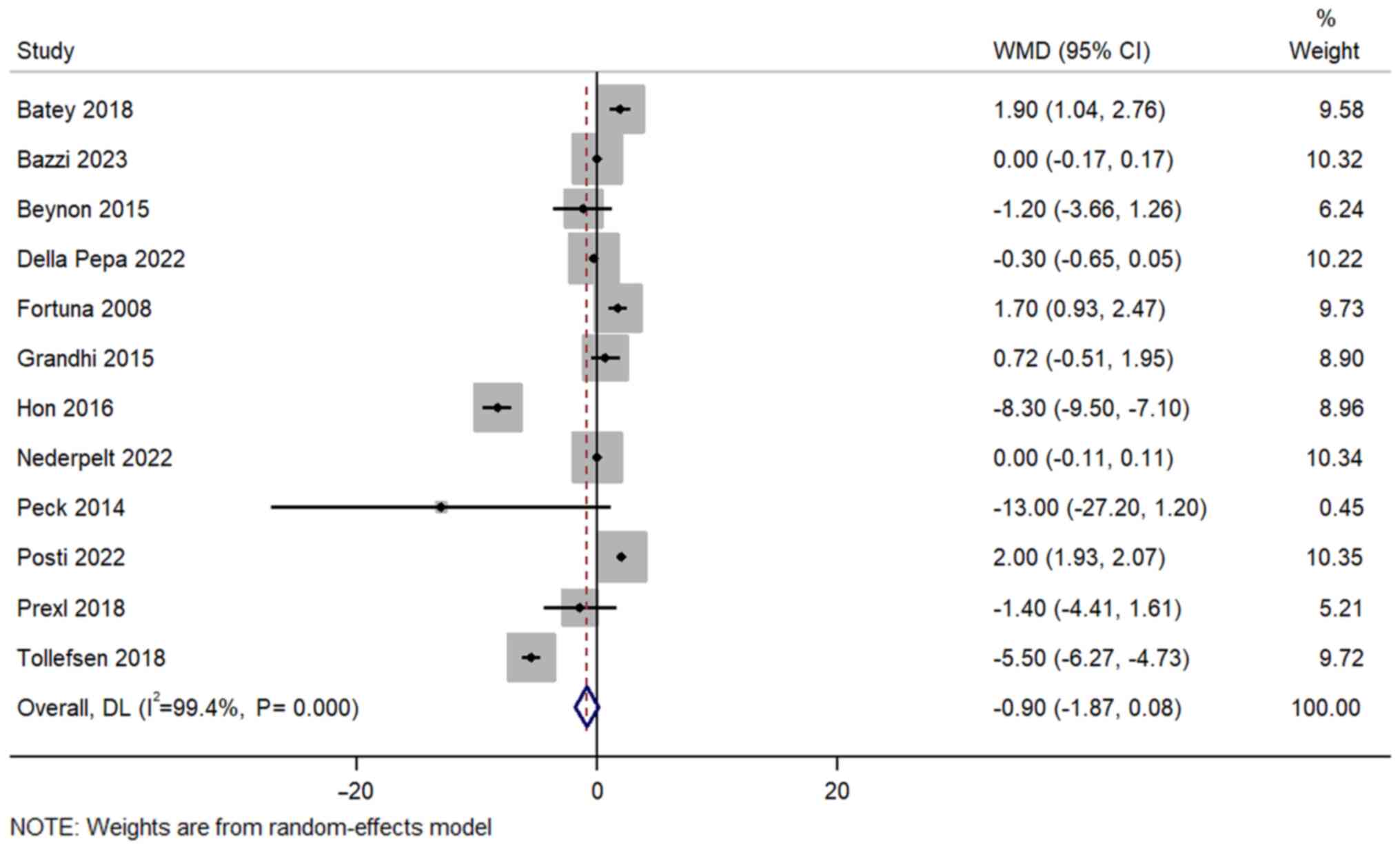
Length of hospital stay
A total of 12 studies with 63,405 participants
assessed the length of hospital stay in patients with TBI with and
without prior anticoagulant therapy. The pooled weighted mean
difference was -0.897 days (95% CI: -1.873-0.079, P=0.072),
indicating a non-significant decrease in hospital stay for patients
with TBI with prior anticoagulant therapy (Fig. 6). Significant heterogeneity was
present among the studies (I²=99.4%; P<0.001). Funnel plot
showed no publication bias (Fig.
S3).
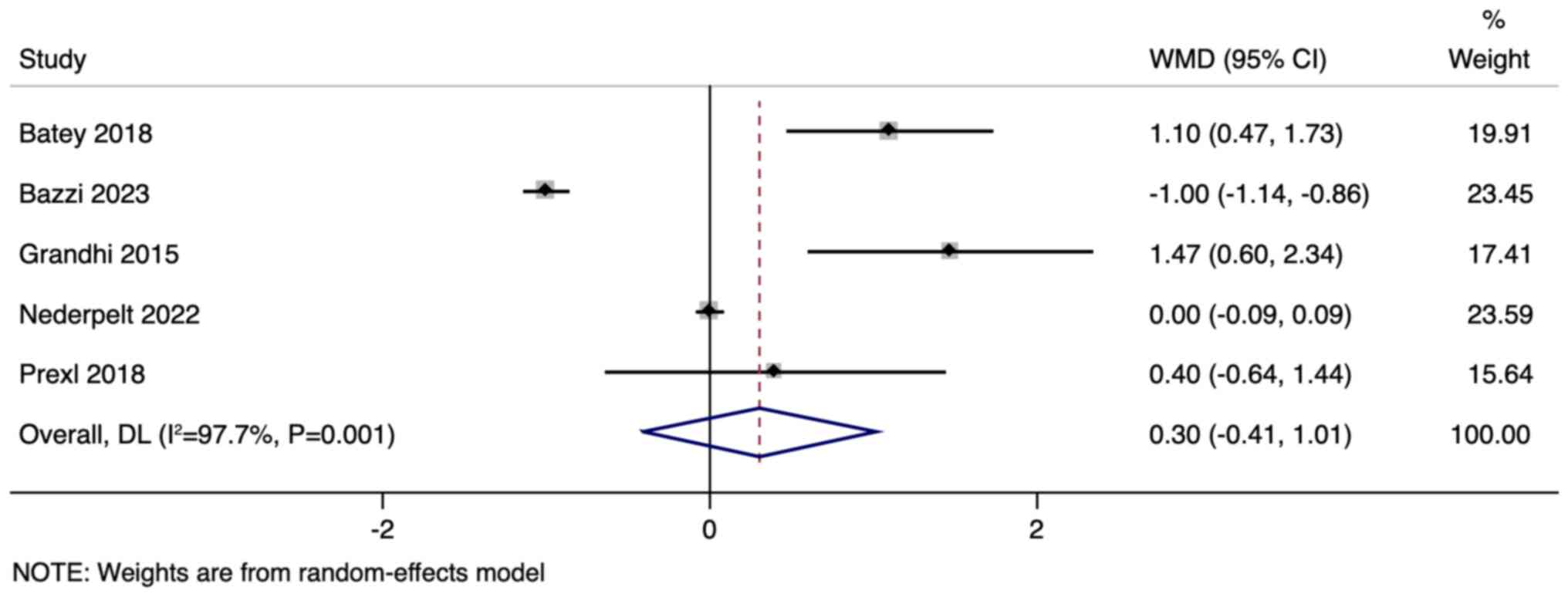
Length of ICU stay
A total of five studies, with a total of 4,823
participants, assessed the length of the ICU stay. The pooled
weighted mean difference was 0.303 days (95% CI: -0.405-1.011,
P=0.402), indicating no significant difference in the length of the
ICU stay (Fig. 7). Notably, there
was substantial heterogeneity across the studies (I²=97.7%;
P<0.001), suggesting variations in study outcomes or
methodologies.
Discussion
The present comprehensive meta-analysis encompassing
102,036 participants provided vital insights into the clinical
implications of prior anticoagulant therapy on traumatic brain
injury (TBI) outcomes. The central finding indicated that patients
with TBI with a history of anticoagulant therapy experience a
higher risk of overall and in-hospital mortality and have higher
likelihood of requiring neurosurgical intervention, compared with
patients without a history of anticoagulation therapy. However, the
present review demonstrated that this increased mortality risk does
not translate into longer hospital or ICU stays. It is suggested
that this could be attributed to the timely and efficient
interventions that are currently in place in trauma centers.
The results of the present review are consistent
with previous reports on the subject. Lim et al (33) undertook a similar meta-analysis and
found that anticoagulant therapy had detrimental outcomes in
patients who sustained a TBI. A previous review has also indicated
that, while anticoagulant therapy posed a risk, the prognosis was
largely dictated by other factors such as age, injury severity and
comorbidities (33). The present
results further confirm these finding, underlining the complexity
and multifaceted nature of TBI outcomes. While Lim et al
(33) and other previous studies
have laid the groundwork, the present research contributed novel
insights by examining the latest data and incorporating a broader
range of variables. This comprehensive approach underscored the
multifactorial nature of TBI prognosis and offered a more granular
perspective on the role of anticoagulation in TBI outcomes. The
present findings serve as a pivotal resource for clinicians and
nurses, providing an updated, evidence-based framework to guide
decision-making and optimize patient care in this challenging
clinical scenario.
It might be hypothesized that the pathogenesis of
the increased mortality rates in patients with TBI with prior
anticoagulant therapy is multifaceted. Anticoagulants diminish the
coagulation capability of blood, potentially leading to exacerbated
post-injury bleeding (34). It is
conceivable that such therapy may worsen cerebral microbleeds,
making the brain more susceptible to neuronal damage post-TBI.
These microbleeds can activate a cascade of inflammatory processes
detrimental to brain tissue (35).
The presence of anticoagulants may also further disrupt the
delicate balance between pro-coagulant and anticoagulant factors
that is affected by TBI. Additionally, increased bleeding can lead
to reduced cerebral perfusion, aggravating secondary brain injury
complications such as ischemia, elevated intracranial pressure,
herniation, or even diffuse axonal injury (36). Moreover, there is a potential risk
of drug-drug interactions that might arise when patients with TBI
on anticoagulants are administered other medications during their
hospital stay (37).
The observed increase in mortality rates among
patients with TBI with prior anticoagulant therapy demands a
comparative analysis with other clinical conditions. In a recent
observational study, patients with acute cardiovascular events on
anticoagulants had slightly higher mortality rates (38). Therefore, it is plausible that this
phenomenon is not restricted to TBI and there are more universal
risks associated with anticoagulant therapy. One aspect that
demands further investigation is the timely withdrawal or reversal
of anticoagulation post-TBI. Some anticoagulants have reversal
agents or antidotes which, when administered promptly, might
mitigate the hemorrhagic risks. However, the exact timing, dosage
and potential side effects of these antidotes remain to be
elucidated (39).
Notably, the present study revealed that patients
with severe TBI showed improved survival rates when on prior
anticoagulants. This counterintuitive finding may be attributed to
several factors. One possible explanation is the ‘anticoagulant
paradox,’ where certain anticoagulants may offer neuroprotective
effects due to their influence on cerebral blood flow and
inflammation (40). Additionally,
patients on long-term anticoagulant therapy often receive more
rigorous medical monitoring, which could lead to quicker TBI
diagnosis and treatment. It is also possible that the profile of
patients on anticoagulants differs significantly from those not on
such therapy, including factors such as improved overall health
management and quicker access to medical care. Further research is
needed to explore these hypotheses and understand the underlying
mechanisms.
Early mobilization and rehabilitation are paramount
for TBI recovery. Delays due to complications associated with
anticoagulant therapy might compromise functional recovery and
long-term quality of life. The nursing perspective in TBI care is
multifaceted, addressing not just immediate medical needs but also
holistic well-being. Nurses play a critical role in patient
education, ensuring that patients with TBI and their families are
well-informed about the implications of anticoagulant therapy. They
are often the first to notice subtle changes in a patient's
condition, making their role in monitoring patients with TBI on
anticoagulants crucial.
The present meta-analysis had several strengths. The
inclusion of a large number of participants across multiple studies
ensures a diverse and representative sample, thus enhancing the
external validity of our findings. Additionally, the rigorous
methodology and subgroup analyses ensured robust and consistent
results.
Nevertheless, the present study had several
limitations. The significant heterogeneity among studies might be
reflective of varying definitions of TBI severity, different
anticoagulant classes, or differing healthcare standards across
regions. There is the absence of detailed information on long-term
neurological outcomes and the specific use of reversal agents in
the present study. This is indeed a limitation as it would have
provided deeper insights into the recovery trajectory and
management strategies post-TBI for patients on anticoagulants.
Future studies should aim to include comprehensive data on
neurological impairments over the long term and the effects of
using reversal agents in the treatment protocol. Another notable
limitation of the analysis is the inability to conduct a detailed
comparison between patients on DOACs compared with Warfarin, as
well as an separate analysis of various DOACs. This limitation
stems from the composition of the dataset, which predominantly
included studies focusing on a combination of DOAC and Warfarin
therapies, or Warfarin alone. The prevalence of Warfarin use, often
in isolation or combined with other drugs, in the existing
literature limits the capacity for a more nuanced subgroup
analysis.
The findings of the present meta-analysis suggest
that trauma centers might need to revisit their protocols for
managing patients with TBI with a history of anticoagulant use.
Implementing a universal algorithm that encompasses rapid
diagnostics, timely drug reversal and vigilant monitoring might
improve outcomes. Furthermore, interdisciplinary collaborations
involving neurologists, hematologists and trauma surgeons could
foster comprehensive patient-centered care.
Future studies could focus on the specific classes
of anticoagulants as different anticoagulants may carry varying
risks. Future prospective studies are needed to establish more
definitive causality. Additionally, focusing on specific TBI
severity subgroups could provide more granular insights into which
patients are most at risk.
The present meta-analysis underscores the heightened
risk of adverse outcomes, such as in-hospital and overall mortality
and higher need for neurosurgical interventions in patients with
TBI with prior anticoagulant therapy. The results provided insights
for informed clinical decisions and identify areas warranting
further research.
Supplementary Material
Funnel plot for overall
mortality.
Funnel plot for in-hospital
mortality.
Funnel plot for length of hospital
stay.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
LP conceived and designed the study. LP and JH
collected the data and performed the literature search. LP was
involved in the writing of the manuscript. LP and JH confirm the
authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Werner C and Engelhard K: Pathophysiology
of traumatic brain injury. Br J Anaesth. 99:4–9. 2007.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Maas AIR, Menon DK, Adelson PD, Andelic N,
Bell MJ, Belli A, Bragge P, Brazinova A, Büki A, Chesnut RM, et al:
Traumatic brain injury: Integrated approaches to improve
prevention, clinical care, and research. Lancet Neurol.
16:987–1048. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kearon C, Akl EA, Ornelas J, Blaivas A,
Jimenez D, Bounameaux H, Huisman M, King CS, Morris TA, Sood N, et
al: Antithrombotic therapy for VTE disease: CHEST guideline and
expert panel report. Chest. 149:315–352. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Pisters R, Lane DA, Nieuwlaat R, de Vos
CB, Crijns HJGM and Lip GYH: A novel user-friendly score (HAS-BLED)
to assess 1-year risk of major bleeding in patients with atrial
fibrillation: The Euro heart survey. Chest. 138:1093–1100.
2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Peck KA, Calvo RY, Schechter MS, Sise CB,
Kahl JE, Shackford MC, Shackford SR, Sise MJ and Blaskiewicz DJ:
The impact of preinjury anticoagulants and prescription
antiplatelet agents on outcomes in older patients with traumatic
brain injury. J Trauma Acute Care Surg. 76:431–436. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Narum S, Westergren T and Klemp M:
Corticosteroids and risk of gastrointestinal bleeding: A systematic
review and meta-analysis. BMJ Open. 4(e004587)2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Batchelor JS and Grayson A: A
meta-analysis to determine the effect of anticoagulation on
mortality in patients with blunt head trauma. Br J Neurosurg.
26:525–530. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Uccella L, Zoia C, Perlasca F, Bongetta D,
Codecà R and Gaetani P: Mild traumatic brain injury in patients on
long-term anticoagulation therapy: Do they really need repeated
head CT scan? World Neurosurg. 93:100–103. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372(n71)2021.PubMed/NCBI View
Article : Google Scholar
|
|
10
|
Lo CKL, Mertz D and Loeb M:
Newcastle-Ottawa Scale: Comparing reviewers' to authors'
assessments. BMC Med Res Methodol. 14(45)2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Higgins JPT, Thomas J, Chandler J,
Cumpston M, Li T, Page MJ and Welch VA (eds): Cochrane Handbook for
Systematic Reviews of Interventions. 2nd edition. Chichester (UK):
John Wiley & Sons, 2019.
|
|
12
|
Fakhry SM, Morse JL, Garland JM, Wilson
NY, Shen Y, Wyse RJ and Watts DD: Antiplatelet and anticoagulant
agents have minimal impact on traumatic brain injury incidence,
surgery, and mortality in geriatric ground level falls: A
multi-institutional analysis of 33,710 patients. J Trauma Acute
Care Surg. 90:215–223. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Della Pepa GM, Covino M, Menna G,
Auricchio AM, Polli FM, Manno A, Simeoni B, Olivi A and Franceschi
F: Are oral anticoagulants a risk factor for mild traumatic brain
injury progression? A single-center experience focused on of direct
oral anticoagulants and vitamin K antagonists. Acta Neurochir
(Wien). 164:97–105. 2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Pieracci FM, Eachempati SR, Shou J, Hydo
LJ and Barie PS: Degree of anticoagulation, but not warfarin use
itself, predicts adverse outcomes after traumatic brain injury in
elderly trauma patients. J Trauma. 63:525–530. 2007.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Batey M, Hecht J, Callahan C and Wahl W:
Direct oral anticoagulants do not worsen traumatic brain injury
after low-level falls in the elderly. Surgery. 164:814–819.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Bazzi R, Sharp V and Hecht J: Effect of
antiplatelet and anticoagulant agents on outcomes following
emergent surgery for traumatic brain injuries. Am Surg.
89:5397–5406. 2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Posti JP, Ruuskanen JO, Sipilä JOT, Luoto
TM, Rautava P and Kytö V: Impact of oral anticoagulation and
adenosine diphosphate inhibitor therapies on short-term outcome of
traumatic brain injury. Neurology. 99:e1122–e1130. 2022.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Rønning P, Helseth E, Skaansar O, Tverdal
C, Andelic N, Bhatnagar R, Melberg M, Skaga NO, Aarhus M, Halvorsen
S and Helseth R: Impact of preinjury antithrombotic therapy on
30-day mortality in older patients hospitalized with traumatic
brain injury (TBI). Front Neurol. 12(650695)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Laic RAG, Verhamme P, Vander Sloten J and
Depreitere B: Long-term outcomes after traumatic brain injury in
elderly patients on antithrombotic therapy. Acta Neurochir (Wien).
165:1297–1307. 2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Senft C, Schuster T, Forster MT, Seifert V
and Gerlach R: Management and outcome of patients with acute
traumatic subdural hematomas and pre-injury oral anticoagulation
therapy. Neurol Res. 31:1012–1018. 2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Krueger EM, Finneran MM and Smith M:
Management strategies and outcomes of hemorrhagic traumatic brain
injury on oral anticoagulants. Cureus. 12(e10508)2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Tollefsen MH, Vik A, Skandsen T, Sandrød
O, Deane SF, Rao V and Moen KG: Patients with moderate and severe
traumatic brain injury: Impact of preinjury platelet inhibitor or
warfarin treatment. World Neurosurg. 114:e209–e217. 2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Svedung Wettervik T, Lenell S, Enblad P
and Lewén A: Pre-injury antithrombotic agents predict intracranial
hemorrhagic progression, but not worse clinical outcome in severe
traumatic brain injury. Acta Neurochir (Wien). 163:1403–1413.
2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Grandhi R, Harrison G, Voronovich Z, Bauer
J, Chen SH, Nicholas D, Alarcon LH and Okonkwo DO: Preinjury
warfarin, but not antiplatelet medications, increases mortality in
elderly traumatic brain injury patients. J Trauma Acute Care Surg.
78:614–621. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Beynon C, Potzy A, Sakowitz OW and
Unterberg AW: Rivaroxaban and intracranial haemorrhage after mild
traumatic brain injury: A dangerous combination? Clin Neurol
Neurosurg. 136:73–78. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Prexl O, Bruckbauer M, Voelckel W, Grottke
O, Ponschab M, Maegele M and Schöchl H: The impact of direct oral
anticoagulants in traumatic brain injury patients greater than
60-years-old. Scand J Trauma Resusc Emerg Med.
26(20)2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Fortuna GR, Mueller EW, James LE, Shutter
LA and Butler KL: The impact of preinjury antiplatelet and
anticoagulant pharmacotherapy on outcomes in elderly patients with
hemorrhagic brain injury. Surgery. 144:598–605. 2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
O'Donohoe RB, Lee HQ, Tan T, Hendel S,
Hunn M, Mathews J, Fitzgerald M, Rosenfeld JV and Tee J: The impact
of preinjury antiplatelet and anticoagulant use on elderly patients
with moderate or severe traumatic brain injury following traumatic
acute subdural hematoma. World Neurosurg. 166:e521–e527.
2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Nederpelt CJ, Naar L, Meier K, van Wijck
SFM, Krijnen P, Velmahos GC, Kaafarani HMA, Rosenthal MG and
Schipper IB: Treatment and outcomes of anticoagulated geriatric
trauma patients with traumatic intracranial hemorrhage after falls.
Eur J Trauma Emerg Surg. 48:4297–4304. 2022.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Hon HH, Elmously A, Stehly CD, Stoltzfus
JC, Granson MA, Stawicki SP and Hoey BA: Inappropriate preinjury
warfarin use in trauma patients: A call for a safety initiative. J
Postgrad Med. 62:73–79. 2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Karni A, Holtzman R, Bass T, Zorman G,
Carter L, Rodriguez L, Bennett-Shipman VJ and Lottenberg L:
Traumatic head injury in the anticoagulated elderly patient: A
lethal combination. Am Surg. 67:1098–1100. 2001.PubMed/NCBI
|
|
32
|
Ahmed N, Bialowas C, Kuo YH and Zawodniak
L: Impact of preinjury anticoagulation in patients with traumatic
brain injury. South Med J. 102:476–480. 2009.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lim XT, Ang E, Lee ZX and Hajibandeh S and
Hajibandeh S: Prognostic significance of preinjury anticoagulation
in patients with traumatic brain injury: A systematic review and
meta-analysis. J Trauma Acute Care Surg. 90:191–201.
2021.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Spahn DR, Bouillon B, Cerny V, Coats TJ,
Duranteau J, Fernández-Mondéjar E, Filipescu D, Hunt BJ, Komadina
R, Nardi G, et al: Management of bleeding and coagulopathy
following major trauma: An updated European guideline. Crit Care.
17(R76)2013.PubMed/NCBI View
Article : Google Scholar
|
|
35
|
Toth L, Czigler A, Horvath P, Kornyei B,
Szarka N, Schwarcz A, Ungvari Z, Buki A and Toth P: Traumatic brain
injury-induced cerebral microbleeds in the elderly. Geroscience.
43:125–136. 2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Mckee AC and Daneshvar DH: The
neuropathology of traumatic brain injury. Handb Clin Neurol.
127:45–66. 2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Amaraneni A, Chippa V and Rettew AC:
Anticoagulation Safety. In: StatPearls. Treasure Island (FL):
StatPearls Publishing, 2023.
|
|
38
|
Albrecht JS, Liu X, Baumgarten M,
Langenberg P, Rattinger GB, Smith GS, Gambert SR, Gottlieb SS and
Zuckerman IH: Benefits and risks of anticoagulation resumption
following traumatic brain injury. JAMA Intern Med. 174:1244–1251.
2014.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Thomas S and Makris M: The reversal of
anticoagulation in clinical practice. Clin Med (Lond). 18:314–319.
2018.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Bouwens EA, Stavenuiter F and Mosnier LO:
Mechanisms of anticoagulant and cytoprotective actions of the
protein C pathway. J Thromb Haemost. 11 (Suppl 1):S242–S253.
2013.PubMed/NCBI View Article : Google Scholar
|