Introduction
Lung cancer is the most common type of cancer
worldwide, ranking second in incidence and first in mortality among
malignant tumors (1). Non-small
cell lung cancer (NSCLC) accounts for ~85% of lung cancer (2). Despite advancements in the diagnosis
and treatment of lung cancer in recent years, the 5-year survival
rate of patients with lung cancer remains <20% (3). The 5-year survival rate is closely
related to tumor recurrence and metastasis following treatment
(4). Liquid biopsy, a convenient
and non-invasive method that dynamically reflects the genetic
profile of tumors, serves a crucial role in lung cancer therapy and
prognostic monitoring (5). Liquid
biopsy is a minimally invasive and easily repeatable test for the
cytological and molecular analysis of cancer markers that are
secreted from the tumor cells into the blood. The detection of
circulating tumor cells (CTCs) in blood, as the earliest liquid
biopsy technique, has been widely used in early tumor diagnosis,
prognostic assessment, disease monitoring and treatment management
(6). CTCs are rare and have a
limited survival time in the bloodstream, and thus, their
identification and isolation is challenging (7). Lung cancer is a type of epithelial
cancer, and thus, the current detection method of CTCs is mainly
through enriching and selecting EpCAM antigen positive cells in the
blood (8,9).
CTCs are a highly heterogeneous cell population, and
most CTCs entering the bloodstream undergo apoptosis due to immune
recognition, mechanical damage and tumor cell-intrinsic factors,
which prevent the formation of metastatic lesions. This phenomenon
is referred to as ‘ineffective metastasis’ (10). Only a small number of CTCs with
high metastatic potential survive in the circulatory system. These
CTCs then aggregate to form microemboli and, under certain
conditions, develop into metastatic tumors (11). It is these cells with metastatic
potential that require further study. CTC-subsets retain a
mesenchymal-like phenotype to adapt EMT, characterized by an
up-regulation of Vimentin and N-cadherin genes (12). Because of EMT-process, tumor cells
and derived-CTCs can undergo to various alterations during the
early stages of carcinogenesis, leading to cancer cell
dissemination and micrometast (13). Studies have reported that the EMT
phenotype of CTCs in the peripheral blood of patients with NSCLC is
associated with the distant metastasis of tumors (14,15).
CTCs with epithelial cell markers can undergo EMT and enter nearby
blood vessels for distant dissemination. During EMT, cancer cells
lose their epithelial characteristics due to the downregulation of
epithelial genes, including E-cadherin, EpCAM and β-catenin, and
obtain mesenchymal properties due to the upregulation of
mesenchymal genes, including N-cadherin, vimentin and fibronectin.
Different types of CTCs have been identified by combining
epithelial [EpCAM and cytokeratin (CK)8/18/19] and mesenchymal
(vimentin) markers (16).
In the past few years, immune checkpoint inhibitors
targeting programmed cell death-1 (PD-1) or programmed death ligand
1 (PD-L1) have revolutionized the treatment of advanced NSCLC
(17). The PD-L1/PD-1 system
regulates the immune response mainly through the intracellular
inhibitory signal transduction mechanism of effector T cells and
regulatory T cells (18). In the
tumor microenvironment, combination of PD-L1 and PD-1 can inhibit
the initiation and activation of T cells and promotes cancer
progression (19). Therefore,
PD-L1 serves a key role in the immune escape of cancer cells. By
blocking the interaction between PD-1 and PD-L1, these inhibitors
enable the immune system to eliminate tumors. Notably, PD-L1 is
also the only approved predictive biomarker in clinical practice
for monitoring the application of anti-PD-1 drugs in NSCLC
(20). Currently, researchers
primarily detect PD-L1 expression in tumor tissues (21), whereas the expression status of
PD-L1 on CTCs remains unclear.
Therefore, in addition to the expression of PD-L1 in
tumor tissues, the present study aimed to assess the expression of
PD-L1 and EMT markers on CTCs to evaluate the feasibility of
detecting these as indicators for clinical staging of NSCLC and
patient prognosis, and to identify suitable biomarkers for improved
assessment of NSCLC occurrence and progression, as well as patient
prognosis.
Patients and methods
Subjects
The present study included 100 patients with NSCLC
enrolled at the Department of Respiratory Medicine, The Second
Affiliated Hospital of Jiaxing University (Jiaxing, China) between
January 2021 and June 2023. The inclusion criteria were as follows:
i) Pathologically confirmed diagnosis of NSCLC; ii) availability of
suitable tissue samples for immunohistochemical testing; and iii)
collection of 7.5 ml peripheral blood from patients before
treatment. The exclusion criteria were as follows: i) Age <18 or
>85 years; ii) history of other malignant tumors; iii) severe
impairment of liver or kidney function or severe congestive heart
failure, as ascites or edema can cause peripheral blood to be
diluted; iv) active infection defined as a sharp increase in the
number of white blood cells, which leads to a decrease in the
detection rate of CTCs; v) irreversible coagulation disorders and
marked hemogram abnormalities or evident bleeding tendencies; vi) a
history of cranial or brain injury or trauma; and vii) patients
lost to follow-up during the study.
Sample collection
Tumor tissue samples were obtained from patients who
were pathologically diagnosed with lung cancer and treated with
chemotherapy. The samples were selected for immunohistochemical
testing of PD-L1 expression. Peripheral blood samples (7.5 ml) were
collected from 100 patients with NSCLC before chemotherapy and
placed in EDTA-K2 solution. The blood samples were
obtained in the middle of the venipuncture procedure after the
first 5 ml of blood was discarded, to avoid contamination by
epithelial cells from the skin. A total of 7.5 ml peripheral blood
was prepared for CTC detection.
Immunohistochemical staining
The fresh tissues of NSCLC patients were fixed with
10% neutral formalin (pH 7.0) for 24 h at room temperature.
Paraffin-embedded tissue was performed on 3-µm-thick sections and
dewaxing. The tissues were then treated with 3%
H2O2 at room temperature for 5-10 min and
washed with PBS. Sections were placed in citrate buffer (pH 6.0) at
95˚C for 15 min, cooled at room temperature and washed with PBS.
The sections were blocked with 10% normal goat serum (Balb, WK300,
China) at room temperature for 10 min, and the serum was discarded
without washing. Subsequently, the PD-L1 antibody (1:100; cat. no.
15165; Cell Signaling Technology, Inc.) was added, and the sections
were incubated overnight at 4˚C. Sections were rinsed with PBS for
5 min, after which 50 µl biotin-conjugated goat anti-rabbit IgG
(cat. no. as-7002, 1:1,000, Guangzhou Ascend Biotechnology Co.,
Ltd.) was added and the sections were incubated at 37˚C for 30 min.
After rinsing with PBS for 5 min, the sections were stained with
3,3'-diaminobenzidine for 10 min. Sections were then thoroughly
rinsed with PBS, counterstained with hematoxylin at room
temperature for 3 min and rehydration in descending alcohol series
for 5 min. Finally, the sections were cleared in xylene and
observed under a light microscope.
The IHC sections were analyzed by three independent
investigators and determined manually. PD-L1 expression in tumor
tissue was classified according to the percentage of cells with a
positive score for staining. The sum of intensity (0: negative; 1:
weak; 2: clear; 3: strong) and percentage (0: 0-1%; 1: 1-10%; 2:
10-25%; 3: 25-50%; 4: 50-75%; 5: 75-100%). The positivity rate of
PD-L1 staining was defined as 1% (22). According to IHC, patients were
divided into two groups: PD L1+ group (≧1%) and PD
L1-group (<1%).
H&E staining
Paraffin sections were deparaffinized with xylene
and rehydration in descending alcohol series for 5 min. They were
washed with distilled water once, then placed in hematoxylin for 5
min and washed with distilled water again after staining. Paraffin
sections were soaked in hydrochloric acid alcohol (1%) for 30 sec
to differentiate, and in ammonia water (1%) for 30 sec back to blue
after washed with clean water, and in eosin alcohol for 1 min to
stain after washed with clean water. Paraffin sections were
dehydrated with 75, 90 and 100% ethanol for 10 sec, respectively.
Then washed with clean water, and soaked in xylene for 1 min.
Finally, sections sealed and observed by a light microscope.
Tumor cells were identified using hematoxylin and
eosin staining. Tumor cells are generally large, more than three
times the size of normal cells. The nuclear chromatin is rough, the
nucleolus is clear, the cytoplasm is rich and mucus vacuoles can be
seen (23).
CTC detection and immunofluorescence
staining
CTC detection experiments were performed using blood
samples and the EpCAM/Vimentin/EGFR/Folic Acid magnetic bead system
(cat. no. 2001, Hangzhou Fanglue Biotechnology Co., Ltd.) according
to the product instructions. Magnetically labeled EpCAM or Vimentin
or EGFR or Folic Acid WBCs are retained within the column, while
unlabeled cells pass through the column. The isolated cell
population was fixed using 4% neutral buffered formalin at room
temperature for 15 min followed by permeabilization with 0.4%
Triton X-100 for 10 min. The cells were blocked by 5% BSA) at room
temperature for 30 min. The cells were then incubated with CK-FITC
(1:50, Cat No. FITC-66187, Proteintech Group, Inc.),
CD45-phycoerythrin (1:100, Cat No. PE-65082, Proteintech, China)
and PD-L1-Alexa Fluor 647 (1:50, Cat No. CL647-65082, Proteintech,
China) antibodies at room temperature in the dark for 2 h, followed
by washing with PBS and DAPI staining at room temperature for 10
min. Subsequently, the coverslip was added, and excess liquid was
removed. Finally, the cells were scanned using a Fluorescence
microscope (LEICA DMi8, Germany) and images were collected and
observed using Leica Application Suite X (Leica Germany).
The CTC interpretation criteria were as follows: i)
Clear cell morphology under white light; ii) CD45 staining negative
in CTCs; iii) separation of cells using EpCAM/Vimentin/EGFR/Folic
Acid magnetic beads; iv) positive cells were CK+ and
DAPI+. Cells with EpCAM+, CK+ and
DAPI+ staining were categorized as epithelial-type CTCs
(E-CTCs). Cells with Vimentin+, CK+ and
DAPI+ staining were categorized as mesenchymal-type CTCs
(M-CTCs). Cells with CK+, DAPI+ and
PD-L1+ staining were classified as PD-L1+
CTC.
Statistical analysis
Statistical analysis was performed using GraphPad
Prism 7.0 software (Dotmatics). The χ2 test or Fisher's
exact test was used to analyze the relationship between PD-L1
expression and clinical information. Data are presented as the mean
± standard deviation. Statistically significant differences between
two groups were evaluated using unpaired Student's t-test. Survival
analysis was performed using the log-rank test to compare
Kaplan-Meier curves. Univariate and multivariate Cox regression
analyses were used to identify independent prognostic factors.
P≤0.05 was considered to indicate a statistically significant
difference.
Results
Expression and clinical significance
of PD-L1 in the tumor tissues of patients with NSCLC
Blood samples from 100 patients with NSCLC were used
in the present study. The mean age of the patients was 62.8±10.3
years (range, 39-82), 43 patients were male and 57 patients were
female. The histological types included adenocarcinoma (78%),
squamous cell carcinoma (21%) and other NSCLC (1%). The longest
follow-up time of the two groups was 36 months, the median
follow-up time was 20 months and the shortest follow-up time was 4
months.
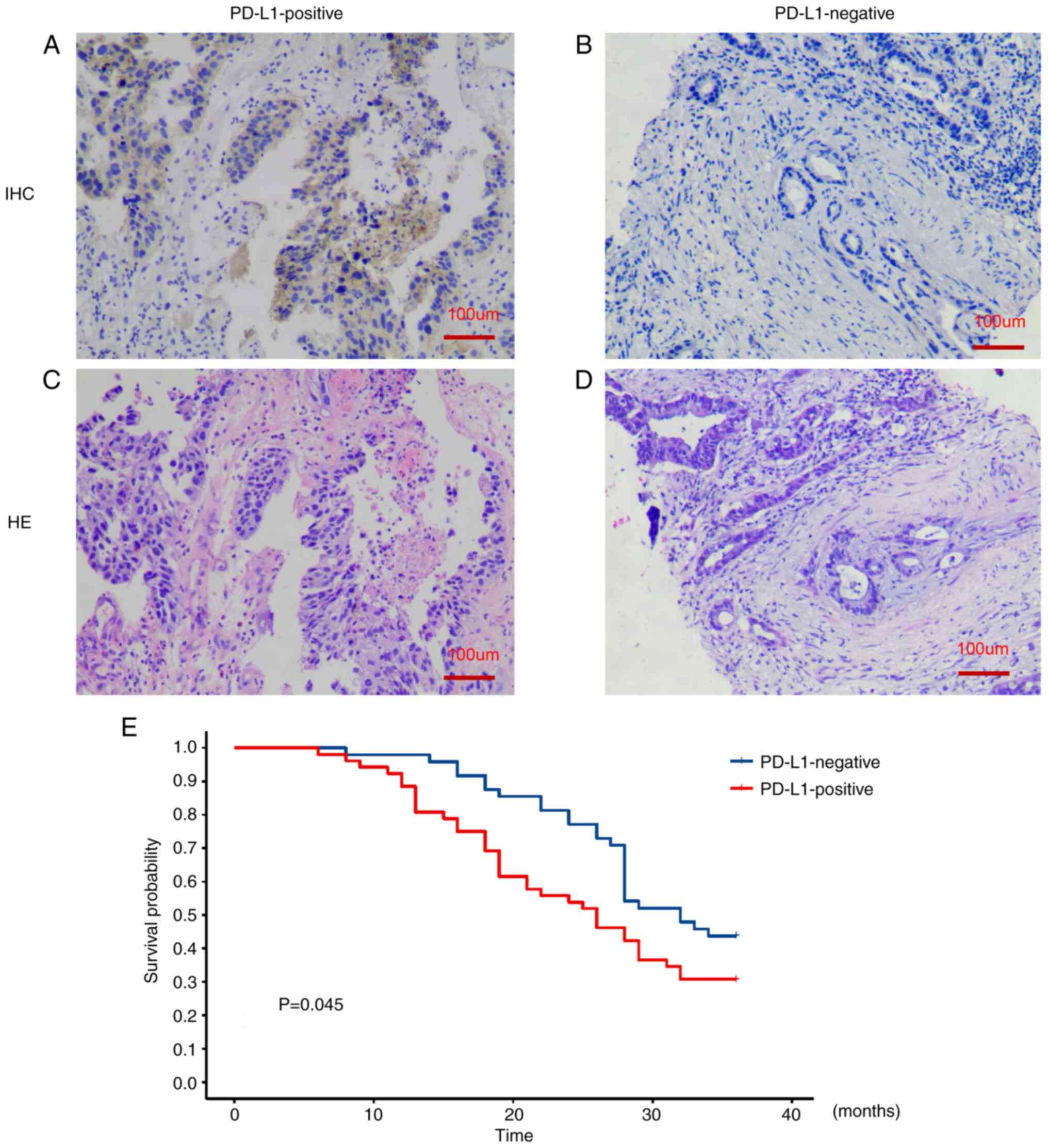
Immunohistochemical staining was performed to detect
PD-L1 protein expression in the pathological sections from 100
patients with NSCLC. PD-L1 was demonstrated to be mainly expressed
on the cell membrane of tumor cells (Fig. 1A-D). Based on the intensity of
PD-L1 protein expression, patients with NSCLC were divided into the
PD-L1-positive group and the PD-L1-negative group to assess the
difference in survival time between the patient groups. There were
60 samples in the PD-L1-positive group and 40 samples in the
PD-L1-negative group. Patients in the PD-L1-positive group had a
significantly shorter overall survival (OS) time compared with
those in the PD-L1-negative group (P≤0.05; Fig. 1E). Furthermore, in the analysis of
clinical characteristics of patients with NSCLC, there were
statistically significant differences in TNM stage, tumor
differentiation and diameter and lymph node metastasis between the
PD-L1-positive group and the PD-L1-negative group (P≤0.05).
However, there were no statistically significant differences
between the two groups in terms of sex, age, smoking history,
pathological type and tumor location (P>0.05; Table I).
 | Table IBaseline demographic and clinical
characteristics of the patients with non-small cell lung
cancer. |
Table I
Baseline demographic and clinical
characteristics of the patients with non-small cell lung
cancer.
| Characteristic | PD-L1-positive, n
(n=60) | PD-L1-negative, n
(n=40) | χ2 | P-value |
|---|
| Sex | | | 0.109 | 0.741a |
|
Male | 25 | 18 | | |
|
Female | 35 | 22 | | |
| Age, years | | | 1.127 | 0.288a |
|
≤60 | 32 | 17 | | |
|
>60 | 28 | 23 | | |
| Smoking
history | | | 1.255 | 0.262a |
|
Yes | 23 | 11 | | |
|
No | 37 | 29 | | |
| Pathological
type | | | | 0.678b |
|
Adenocarcinoma | 48 | 30 | | |
|
Squamous
cell carcinoma | 11 | 10 | | |
|
Mixed
carcinoma | 1 | 0 | | |
| TNM stage | | | 4.342 | 0.037a,c |
|
Stage
I-II | 15 | 18 | | |
|
Stage
III-IV | 45 | 22 | | |
| Tumor
differentiation | | | 5.402 | 0.020a,c |
|
High-moderate | 19 | 22 | | |
|
Poor | 41 | 18 | | |
| Tumor location | | | 0.432 | 0.511a |
|
Left | 28 | 16 | | |
|
Right | 32 | 24 | | |
| Tumor diameter,
cm | | | 3.991 | 0.045a,c |
|
≥3 | 38 | 17 | | |
|
<3 | 22 | 23 | | |
| Lymphatic
metastasis | | | 6.750 | 0.009a,c |
|
Yes | 41 | 18 | | |
|
No | 19 | 22 | | |
Number of CTCs and CTC subtypes in
patients with NSCLC and their relationship with prognosis
The EpCAM/Vimentin/EGFR/Folic Acid magnetic bead
system was used to isolate the positive cell population
(EpCAM+ cells, Vimentin+ cells,
EGFR+ cells, Folic Acid+ cells) from
peripheral blood samples. Cell morphology was observed under light
microscope, immunofluorescence staining with CK, CD45 and DAPI was
then used to detect
CK+/DAPI+/CD45- cells, which were
defined as CTCs (Fig. 2A).
Furthermore, E-CTCs and M-CTCs were identified by isolating
EpCAM+ and Vimentin+ cell populations using
the magnetic bead system, and then detecting CK, CD45 and DAPI
using immunofluorescence staining.
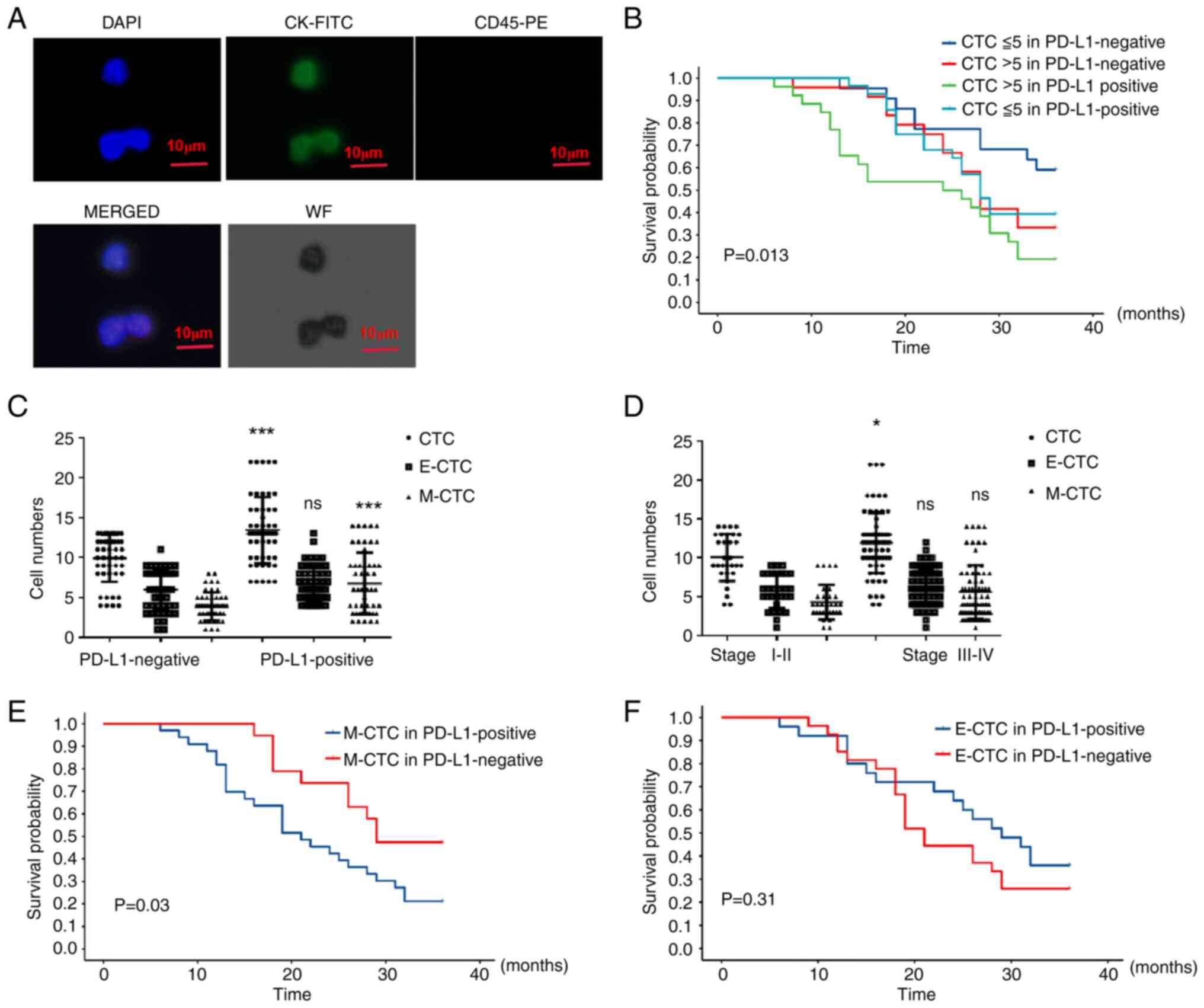 | Figure 2Quantification of CTCs in patients
with NSCLC and association with prognosis. (A) Representative
images of cells stained with DAPI, CK-FITC and CD45-PE to identify
CTCs in peripheral circulation of patients with NSCLC by
immunofluorescence staining. Scale bar, 10 µm. (B) Kaplan-Meier
analysis of OS in ≤5 CTC and >5 CTC groups of PD-L1-positive and
PD-L1-negative patients. Quantification of CTCs, E-CTCs and M-CTCs
in peripheral circulation of (C) PD-L1-positive and PD-L1-negative
groups and (D) stage I-II and stage III-IV groups. Data are
presented as the mean ± SD. Kaplan-Meier analysis of survival
probability in (E) The OS of M-CTC on the PD-L1+-group
and PD-L1--group; (F) The OS of E-CTC on the
PD-L1+-group and PD-L1--group.
*P<0.05, ***P<0.001. CK, cytokeratin;
CTC, circulating tumor cell; E-CTC, epithelial-type CTC; M-CTC,
mesenchymal-type CTC; ns, not significant; NSCLC, non-small cell
lung cancer; PD-L1, programmed death ligand 1; PE, phycoerythrin;
WF, white field. |
Peripheral blood samples from 100 patients with
NSCLC demonstrated that the presence of CTCs per 7.5 ml peripheral
blood were 9.92±0.42 in the PD-L1-negative group and 13.42±0.58 in
the PD-L1-positive group. The quantity of CTCs in the
PD-L1-positive group was significantly higher compared with the
PD-L1-negative group (P<0.0001). The quantity of E-CTCs in the
PD-L1-negative group was 6.02±0.37 and the quantity of E-CTCs in
the PD-L1-positive group was 6.64±0.31. There was no statistically
significant difference between the two groups in terms of E-CTC
counts (P=0.20). The quantity of M-CTCs in the PD-L1-negative group
was 3.90±0.25 and the quantity of M-CTCs in the PD-L1-positive
group was 6.79±0.54. The quantity of M-CTCs in the PD-L1-positive
group was significantly higher compared with that in the
PD-L1-negative group (P=0.001) (Fig.
2C).
The quantity of CTCs in the stage I-II NSCLC group
was 10.07±0.55 and the quantity of CTCs in the stage III-IV NSCLC
group was 11.91±0.46. The quantity of CTCs in the stage III-IV
NSCLC group was significantly higher compared with that in the
stage I-II NSCLC group (P=0.02). Furthermore, the quantity of
E-CTCs in the stage I-II NSCLC group was 5.77±0.40 and the quantity
of E-CTCs in the stage III-IV NSCLC group was 6.30±0.28. There was
no statistically significant difference between the two groups
(P=0.29). Furthermore, the quantity of M-CTCs in the stage I-II
NSCLC group was 4.30±0.41 and the quantity of M-CTCs in the stage
III-IV NSCLC group was 5.61±0.71. There was no statistically
significant difference between the two groups (P=0.06) (Fig. 2D).
A previous study has reported an association between
a baseline level of ≥5 CTCs/7.5 ml peripheral blood and poor OS in
patients with prostate cancer (24). By grouping patients based on the
number of CTCs (>5 or ≤5), it was demonstrated that CTCs >5,
patients in the PD-L1-positive group had a worse overall survival
compared to PD-L1-negative group, while CTCs ≤5, patients in the
PD-L1-negative group had an improved overall survival compared with
PD-L1-positive group (Fig.
2B).
Furthermore, patients with PD L1+ M-CTCs
had a worse prognosis compared with those with PD L1-M-CTCs
(P=0.03; Fig. 2E); however, there
was no significant difference in prognosis between the two groups
based on E-CTCs (P=0.31; Fig.
2F).
PD-L1 expression in patients with
different CTC numbers and subtypes and its relationship with
prognosis
Immunofluorescence staining was performed to detect
the protein expression levels of PD-L1 in CTCs from the peripheral
blood samples of 100 patients with NSCLC (Fig. 3A). The results demonstrated that
the quantity of PD-L1+ CTCs in the PD-L1-negative group
was 5.79±0.32 and the quantity of PD-L1+ CTCs in the
PD-L1-positive group was 7.89±0.51. The quantity of
PD-L1+ CTCs in the PD-L1-positive group was
significantly higher compared with that in the PD-L1-negative group
(P<0.001). The quantity of PD-L1+ M-CTCs in the
PD-L1-negative group was 2.65±0.25 and the quantity of
PD-L1+ M-CTCs in the PD-L1-positive group was 4.50±0.44.
The quantity of PD-L1+ M-CTCs in the PD-L1-positive
group was significantly higher compared with that in the
PD-L1-negative group (P<0.001). The quantity of
PD-L1+ E-CTCs in the PD-L1-negative group was 3.15±0.19
and the quantity of PD-L1+ E-CTCs in the PD-L1-positive
group was 3.39±0.23. There was no statistically significant
difference between the two groups (P=0.43) (Fig. 3C).
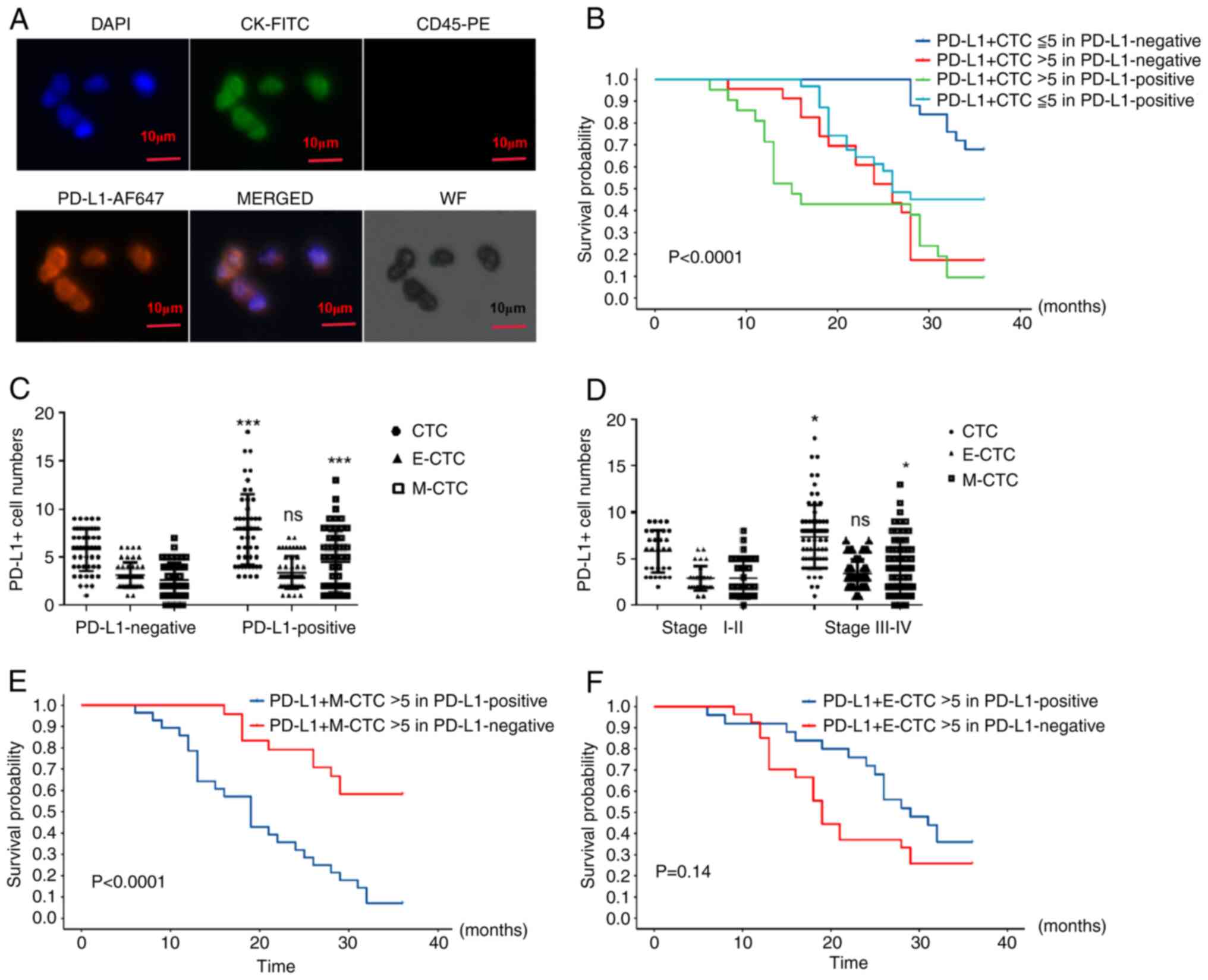 | Figure 3Quantification of PD-L1+ CTCs and CTC
subtypes in patients with NSCLC. (A) Representative images of cells
stained with DAPI, pcytokeratins (CK-FITC), CD45-PE and PD-L1
(AF647) to identify PD-L1+ CTCs in peripheral
circulation of patients with NSCLC by immunofluorescence staining.
Scale bar, 10 µm. (B) Kaplan-Meier analysis of survival probability
in ≤5 PD-L1+ CTCs and >5 PD-L1+ CTCs
groups of PD-L1-positive patients, and ≤5 CTCs and >5 CTCs
groups of PD-L1-negative patients. Quantification of
PD-L1+ CTCs, PD-L1+ E-CTCs and
PD-L1+ M-CTCs in peripheral circulation of (C)
PD-L1-positive and PD-L1-negative groups and (D) stage I-II and
stage III-IV groups. Data are presented as the mean ± SD.
Kaplan-Meier analysis of survival probability in (E)
PD-L1+ M-CTC on the PD-L1+-group and
PD-L1--group; (F) OS of PD-L1+ E-CTC on the
PD-L1+-group and PD-L1--group.
*P<0.05, ***P<0.001. CK, cytokeratin;
CTC, circulating tumor cell; E-CTC, epithelial-type CTC; M-CTC,
mesenchymal-type CTC; ns, not significant; NSCLC, non-small cell
lung cancer; PD-L1, programmed death ligand 1; PE, phycoerythrin;
WF, white field. |
Furthermore, the quantity of PD-L1+ CTCs
in the stage I-II NSCLC group was 5.80±0.41 and the quantity of
PD-L1+ CTCs in the stage III-IV NSCLC group was
7.34±3.26. The quantity of PD-L1+ CTCs in the stage
III-IV NSCLC group was significantly higher compared with that in
the stage I-II NSCLC group (P=0.02). The quantity of
PD-L1+ M-CTCs in the stage I-II NSCLC group was
2.70±0.39 and the quantity of PD-L1+ M-CTCs in the stage
III-IV NSCLC group was 3.98±0.35. The quantity of PD-L1+
M-CTCs in the stage III-IV NSCLC group was significantly higher
compared with that in the stage I-II NSCLC group (P=0.04). The
quantity of PD-L1+ E-CTCs in the stage I-II NSCLC group
was 2.90±0.24 and the quantity of PD-L1+ E-CTCs in the
stage III-IV NSCLC group was 3.43±0.19. There was no significant
difference between the two groups (P=0.11) (Fig. 3D).
By grouping patients based on the number of
PD-L1+ CTCs (>5 and ≤5), it was demonstrated that
patients in the PD-L1-positive group with >5 PD-L1+
CTCs had a worse overall survival compared to PD-L1-negative group,
while patients in the PD-L1-negative group with ≤5
PD-L1+ CTCs had the better overall survival compared to
PD-L1-positive group (P﹤0.0001, Fig.
3B). Patients with PD-L1+ M-CTCs >5 in
PD-L1-positive group had a worse prognosis compared with those in
PD-L1-negative group (P<0.0001, Fig. 3E); however, there was no
significant difference in prognosis between the two groups based on
PD-L1+ E-CTCs >5 (P=0.14, Fig. 3F).
Univariate and multivariate analysis
of clinicopathological parameters associated with OS
To further determine independent prognostic factors,
univariate and multivariate analysis was performed. Univariate Cox
regression analysis demonstrated an association between OS and TNM
stage [hazard ratio (HR), 3.943; 95% CI, 0.982-14.231; P=0.049],
the quantity of M-CTCs (HR, 3.063; 95% CI, 0.560-10.353; P=0.036)
and the quantity of PD-L1+ M-CTCs (HR, 3.677; 95% CI,
0.108-6.579; P=0.027). Multivariate Cox regression analysis
revealed an association between OS and the quantity of
PD-L1+ M-CTCs (HR, 4.112; 95% CI, 0.288-9.417; P=0.039)
and E-CTCs (HR, 4.057; 95% CI, 1.305-20.237; P=0.013). The results
demonstrated that the quantity of PD-L1+ M-CTCs in the
peripheral blood of patients with NSCLC was an independent
prognostic factor associated with OS (Table II).
| Table IIUnivariate and multivariate Cox
hazard regression analysis in patients with non-small cell lung
cancer. |
Table II
Univariate and multivariate Cox
hazard regression analysis in patients with non-small cell lung
cancer.
| | Univariate
analysis | Multivariate
analysis |
|---|
| Parameter | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| Sex (female vs.
male) | 1.527
(0.538-3.975) | 0.421 | 2.282
(0.810-7.592) | 0.649 |
| Age (<60 vs. ≥60
years) | 2.329
(0.271-17.354) | 0.612 | 4.325
(1.339-16.354) | 0.238 |
| Smoking history,
yes vs. No | 0.413
(0.065-3.543) | 0.214 | 1.267
(0.482-6.834) | 0.532 |
| Tumor
differentiation (high-moderate vs. poor) | 1.365
(0.914-5.951) | 0.679 | 4.817
(1.254-10.691) | 0.317 |
| Tumor size (<3
vs. ≥3 cm) | 1.987
(1.443-7.541) | 0.871 | 2.541
(1.637-9.572) | 0.657 |
| Lymphatic
metastasis (yes vs. no) | 1.085
(0.833-5.955) | 0.163 | 1.975
(0.612-7.833) | 0.320 |
| TNM stage (III- vs.
I-II ) | 3.943
(1.232-14.231) | 0.049a | 4.057
(1.254-8.941) | 0.175 |
| CTC (≤5 vs.
>5) | 2.561
(0.829-5.124) | 0.294 | 3.079
(0.927-6.938) | 0.598 |
| E-CTC (≤5 vs.
>5) | 3.473
(1.220-14.274) | 0.096 | 4.057
(1.305-20.237) | 0.013a |
| M-CTC (≤5 vs.
>5) | 3.063
(0.560-10.353) | 0.036a | 5.433
(0.341-12.174) | 0.066 |
| PD-L1+
CTC (≤5 vs. >5) | 3.641
(0.894-6.117) | 0.053 | 3.221
(0.904-7.892) | 0.779 |
| PD-L1+
M-CTC (≤5 vs. >5) | 3.677
(0.108-6.579) | 0.027a | 4.112
(0.288-9.417) | 0.039a |
| PD-L1+
E-CTC (≤5 vs. >5) | 1.527
(0.538-3.975) | 0.421 | 2.282
(0.810-7.592) | 0.649 |
Discussion
The present study assessed the association between
the number of CTCs, CTC subtypes and PD-L1 expression in CTCs and
the clinical characteristics or prognosis of patients with NSCLC.
The aim of the present study was to evaluate the association of
PD-L1 expression on CTCs with advanced staging and poor prognosis,
and to assess PD-L1+ M-CTCs as potential markers for
prognostic assessment and clinical staging evaluation.
CTCs are tumor cells that enter the circulatory
system, which have been confirmed as a basis for tumor metastasis
(7,25). With ongoing research, studies have
reported the use of CTCs in early diagnosis, early chemotherapy
response assessment and prognostic evaluation in various solid
tumors, such as colorectal cancer, breast cancer and genitourinary
tumors (26-29).
The present study also demonstrated that a higher number of CTCs in
the peripheral circulation of patients with NSCLC was associated
with worse clinical staging and prognosis, which is consistent with
the results of national and international research (15,30).
Previous studies (14,15) have reported the association of
total CTCs and M-CTCs with clinical characteristics, tumor
genotypes and survival rates. A baseline CTC count of >5 is a
poor prognostic factor for advanced NSCLC (27). Chen et al (31) reported that EMT was associated with
tumor resistance while M-CTCs may suggest the progression of NSCLC.
The results of the present study suggested an negative association
between peripheral circulation of M-CTCs and the clinical staging
and prognosis of patients with NSCLC. As previously reported
(31), M-CTCs may potentially
promote tumor cell dissemination and metastasis via EMT. However,
there are limitations of CTC detection. Although liquid biopsy is a
powerful method in oncology, it has disadvantages. Notably,
technical inconsistencies and a lack of standardization have
hindered its widespread and routine use in clinical practice. In
patients with NSCLC, numerous CTCs do not have sufficient
epithelial characteristics and may therefore evade detection.
Therefore, the limitation of CTC detection is the lack of
standardized and unified procedures. This highlights the need for
multifaceted efforts to optimize and standardize accessible and
efficient methods of CTC (11,13).
Due to the lack of specific clinical manifestations
of NSCLC, numerous patients are diagnosed at an advanced stage and
their survival time can only be extended through non-surgical
treatment methods. Currently, the efficacy and safety of PD-1
inhibitors in the second-line therapy of NSCLC have been
demonstrated. However, research data show that few patients with
advanced NSCLC benefit from PD-1 inhibitor treatment (20). Therefore, it is necessary to
identify suitable indicators to accurately assess and predict the
effectiveness of PD-1 inhibitor treatment in patients with NSCLC.
Currently, research on PD-L1 mainly focuses on tissue samples, with
little research conducted on the evasion of immune surveillance by
CTCs in the blood. During circulation in the bloodstream, most CTCs
undergo EMT (15,31). Some CTCs, such as those expressing
PD-L1, possess a higher degree of metastatic characteristics,
possibly because this subset of CTCs is more likely to evade immune
surveillance and promote tumor metastasis (32). The results of the present study
also demonstrated that higher counts of PD-L1+ CTCs were
associated with a worse prognosis and that PD-L1+ M-CTCs
served as an independent risk factor for OS in NSCLC. International
research on lung cancer has suggested that the proportion of
PD-L1+ CTCs increases after the start of radiotherapy
and chemotherapy in patients with lung cancer, and the increased
PD-L1 expression in CTCs is associated with poor prognosis
(33). The detection of PD-L1
expression in CTCs has potential clinical applications in
evaluating tumor prognosis and guiding personalized immunotherapies
(34). We hypothesized that CTCs
may trigger the EMT process in tumor cells via PD-L1, thereby
promoting tumor progression and affecting the prognosis of patients
with NSCLC. This should be verified in further study. The detection
of PD-L1 expression and EMT status in CTCs may assist in assessing
disease progression and prognosis in patients with NSCLC, assisting
clinicians in making decisions regarding drug treatments.
The present study had numerous limitations,
including the small number of samples and the fact that it is not
clear whether CTCs had undergone the EMT process during
immunotherapy for lung cancer. Therefore, future studies with an
increased number of samples and long-term CTC detection will
strengthen the current results on the efficacy of these markers.
Another limitation is that the number of total CTCs in peripheral
blood samples may be underestimated, since CTCs are difficult to
identify and separate. There may be some non-specific fluorescence
identified in the fluorescence immunoassay, and the method of
detecting CTCs needs to be further optimized in the future.
The present study aimed to evaluate PD-L1 expression
in the tumor tissues of patients with NSCLC, and assessed the
number of CTCs, CTC subtypes and PD-L1 expression in different
types of peripheral blood CTCs. The association between these
factors and clinical staging and prognosis of patients was also
assessed. The results of the present study suggested that M-CTCs
and PD-L1+ M-CTCs on the peripheral blood CTCs may be an
independent risk factor for poor prognosis in patients with NSCLC,
enabling an improved evaluation of tumor occurrence and
development, and potentially improving the prognosis of patients
with NSCLC.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by the Health Bureau of
Zhejiang Province (grant no. 2021PY029) and the Science and
Technology Bureau of Jiaxing (grant no 2022AD30028).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
HW and HC conceived and designed the study. JJ, WM
and XL designed the methodology and contributed to data
acquisition. JJ and DC performed the statistical analyses. JJ and
HW drafted the manuscript. JJ, HC and HW confirm the authenticity
of all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study complied with the tenets of The
Declaration of Helsinki and was approved by the Medical Ethics
Committee of The Second Affiliated Hospital of Jiaxing University
(approval no. JXEY-2021SW007; Jiaxing, China). Written informed
consent for participation was obtained from all patients in the
present study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Adjei AA: Lung cancer worldwide. J Thorac
Oncol. 14(956)2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Thai AA, Solomon BJ, Sequist LV, Gainor JF
and Heist RS: Lung cancer. Lancet. 398:535–554. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Adams SJ, Stone E, Baldwin DR,
Vliegenthart R, Lee P and Fintelmann FJ: Lung cancer screening.
Lancet. 401:390–408. 2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yu Y, Zeng D, Ou Q, Liu S, Li A, Chen Y,
Lin D, Gao Q, Zhou H, Liao W and Yao H: Association of survival and
Immune-related biomarkers with immunotherapy in patients with
non-small cell lung cancer: A Meta-analysis and individual
patient-level analysis. JAMA Netw Open. 2(e196879)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Steven A, Fisher SA and Robinson BW:
Immunotherapy for lung cancer. Respirology. 21:821–833.
2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Rupp B, Ball H, Wuchu F, Nagrath D and
Nagrath S: Circulating tumor cells in precision medicine:
Challenges and opportunities. Trends Pharmacol Sci. 43:378–391.
2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Aceto N: Bring along your friends:
Homotypic and heterotypic circulating tumor cell clustering to
accelerate metastasis. Biomed J. 43:18–23. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gires O, Pan M, Schinke H, Canis M and
Baeuerle PA: Expression and function of epithelial cell adhesion
molecule EpCAM: Where are we after 40 years? Cancer Metastasis Rev.
39:969–987. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Krebs MG, Hou JM, Sloane R, Lancashire L,
Priest L, Nonaka D, Ward TH, Backen A, Clack G, Hughes A, et al:
Analysis of circulating tumor cells in patients with non-small cell
lung cancer using epithelial marker-dependent and -independent
approaches. J Thorac Oncol. 7:306–315. 2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lin D, Shen L, Luo M, Zhang K, Li J, Yang
Q, Zhu F, Zhou D, Zheng S, Chen Y and Zhou J: Circulating tumor
cells: Biology and clinical significance. Signal Transduct Target
Ther. 6(404)2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Bae SY, Kamalanathan KJ, Galeano-Garces C,
Konety BR, Antonarakis ES, Parthasarathy J, Hong J and Drake JM:
Dissemination of circulating tumor cells in breast and prostate
cancer: Implications for early detection. Endocrinology.
165(bqae022)2024.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Mitra A, Mishra L and Li SL: EMT, CTCs and
CSCs in tumor relapse and drug-resistance. Oncotarget.
6:10697–10711. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Joosse SA, Gorges TM and Pantel K:
Biology, detection, and clinical implications of circulating tumor
cells. Embo Mol Med. 7:1–11. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zhang X, Wei L, Li J, Zheng J, Zhang S and
Zhou J: Epithelial-mesenchymal transition phenotype of circulating
tumor cells is associated with distant metastasis in patients with
NSCLC. Mol Med Rep. 19:601–608. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Zhang Y, Men Y, Wang J, Xing P, Zhao J, Li
J, Xu D, Hui Z and Cui W: Epithelial circulating tumor cells with a
heterogeneous phenotype are associated with metastasis in NSCLC. J
Cancer Res Clin Oncol. 148:1137–1146. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pantazaka E, Vardas V, Roumeliotou A,
Kakavogiannis S and Kallergi G: Clinical relevance of mesenchymal-
and stem-associated phenotypes in circulating tumor cells isolated
from lung cancer patients. Cancers (Basel). 13(2158)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bie F, Tian H, Sun N, Zang R, Zhang M,
Song P, Liu L, Peng Y, Bai G, Zhou B and Gao S: Research progress
of Anti-PD-1/PD-L1 immunotherapy related mechanisms and predictive
biomarkers in NSCLC. Front Oncol. 12(769124)2022.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hu CB, Huang C, Wang J, Hong Y, Fan DD,
Chen Y, Lin AF, Xiang LX and Shao JZ: PD-L1/BTLA checkpoint axis
exploited for bacterial immune escape by restraining CD8+ T
Cell-initiated adaptive immunity in Zebrafish. J Immunol.
211:816–835. 2023.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Juneja VR, McGuire KA, Manguso RT, LaFleur
MW, Collins N, Haining WN, Freeman GJ and Sharpe AH: PD-L1 on tumor
cells is sufficient for immune evasion in immunogenic tumors and
inhibits CD8 T cell cytotoxicity. J Exp Med. 214:895–904.
2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Brody R, Zhang Y, Ballas M, Siddiqui MK,
Gupta P, Barker C, Midha A and Walker J: PD-L1 expression in
advanced NSCLC: Insights into risk stratification and treatment
selection from a systematic literature review. Lung Cancer.
112:200–215. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Barclay J, Creswell J and León J: Cancer
immunotherapy and the PD-1/PD-L1 checkpoint pathway. Arch Esp Urol.
71:393–399. 2018.PubMed/NCBI
|
|
22
|
Ligero M, Serna G, El Nahhas OSM, Sansano
I, Mauchanski S, Viaplana C, Calderaro J, Toledo RA, Dienstmann R,
Vanguri RS, et al: Weakly supervised deep learning predicts
immunotherapy response in solid tumors based on PD-L1 expression.
Cancer Res Commun. 4:92–102. 2024.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hou F, Qi C, Lu Y, Li F and Hao Z: Cell HE
staining smears and paired cell paraffin sections in detection of
epithelial growth factor receptor gene of pleural fluid specimens.
Zhong Nan Da Xue Xue Bao Yi Xue Ban. 47:35–44. 2022.PubMed/NCBI View Article : Google Scholar : (In English,
Chinese).
|
|
24
|
Davies CR, Guo T, Burke E, Stankiewicz E,
Xu L, Mao X, Scandura G, Rajan P, Tipples K, Alifrangis C, et al:
The potential of using circulating tumour cells and their gene
expression to predict docetaxel response in metastatic prostate
cancer. Front Oncol. 12(1060864)2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Castro-Giner F and Aceto N: Tracking
cancer progression: From circulating tumor cells to metastasis.
Genome Med. 12(31)2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Zhang H, Yuan F, Qi Y, Liu B and Chen Q:
Circulating tumor cells for Glioma. Front Oncol.
11(607150)2021.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Liang DH, Hall C and Lucci A: Circulating
tumor cells in breast cancer. Recent Results Cancer Res.
215:127–145. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Pantel K: Circulating tumor cells in head
and neck carcinomas. Clin Chem. 65:1193–1195. 2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Massari F, Di Nunno V, Comito F, Cubelli
M, Ciccarese C, Iacovelli R, Fiorentino M, Montironi R and
Ardizzoni A: Circulating tumor cells in genitourinary tumors. Ther
Adv Urol. 10:65–77. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Castello A, Carbone FG, Rossi S, Monterisi
S, Federico D, Toschi L and Lopci E: Circulating tumor cells and
metabolic parameters in NSCLC patients treated with checkpoint
inhibitors. Cancers (Basel). 12(487)2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Chen M, Xu R, Wu L and Chen X:
Relationship between circulating tumor cells undergoing EMT and
short-term efficacy following interventional treatment in patients
with hepatocellular carcinoma. J Interv Med. 3:146–150.
2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Thunnissen E, de Langen AJ and Smit EF:
PD-L1 IHC in NSCLC with a global and methodological perspective.
Lung Cancer. 113:102–105. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Wang Y, Kim TH, Fouladdel S, Zhang Z, Soni
P, Qin A, Zhao L, Azizi E, Lawrence TS, Ramnath N, et al: PD-L1
expression in circulating tumor cells increases during
Radio(chemo)therapy and indicates poor prognosis in Non-small cell
lung cancer. Sci Rep. 9(566)2019.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Cheng Y, Wang T, Lv X, Li R, Yuan L, Shen
J, Li Y, Yan T, Liu B and Wang L: Detection of PD-L1 expression and
its clinical significance in circulating tumor cells from patients
with Non-small-cell lung cancer. Cancer Manag Res. 12:2069–2078.
2020.PubMed/NCBI View Article : Google Scholar
|