Introduction
Gestational trophoblastic disease (GTD) covers a
spectrum of disorders, which includes hydatidiform molar
pregnancies, and neoplastic and neoplastic tumor-like lesions
arising from trophoblasts (1).
Gestational trophoblastic neoplasia (GTN) includes invasive moles,
choriocarcinoma, placental site trophoblastic tumor (PSTT) and
epithelioid placental site nodules (ETTs) (1). Exaggerated placental sites (EPSs) are
rare neoplastic tumor-like trophoblastic lesions that occur in
~1.6% of terminations of pregnancy, as well as following normal
pregnancy, ectopic pregnancy or molar pregnancy (2). Despite being associated with uterine
bleeding and massive hemorrhage (2), EPS is generally described as an
exaggerated physiological process that differs from GTN in that it
involves villi and shows no confluent growth or mitosis (1). However, the clinical manifestations
are similar, and it is, at times, difficult to distinguish EPS from
GTN, particularly PSTT and choriocarcinoma. The importance of
identifying EPS lies in the fact that GTN warrants surgical
intervention and/or chemotherapy. Although a differential diagnosis
algorithm between EPS and GTN for histological and
immunohistochemical workup has been established (3), it remains ambiguous for certain cases
due to the subjectivity of the assessment, and a definite
diagnostic criterion has not been officially reported by the World
Health Organization (1).
Cesarean scar pregnancy (CSP), occurring in 1.5% of
women with previous cesarean scars, has shown an increasing
prevalence in recent years (4).
CSP refers to an early pregnancy in which a CSP is implanted on a
prior cesarean scar defect, in which trophoblasts pathologically
invade the myometrium (5). EPSs or
GTNs secondary to cesarean scar are rare; however, both have been
rarely reported (2,6). The current study presents a case of
EPS occurring in a cesarean scar in a patient who underwent
hysteroscopic resection and was misdiagnosed with GTN by
postoperative imaging, including magnetic resonance imaging (MRI)
and ultrasound, because of a heterogeneous mass and
hypervascularity.
Case report
A 38-year-old G2P4 Cantonese woman was referred to
Jinan University First Affiliated Hospital, Guangzhou, Guangdong,
China, because of suspected GTD in October 2022. Review of the
patient's obstetric history revealed 1 prior miscarriage and 2
uncomplicated cesarean deliveries in 2012 and 2017. The patient had
no remarkable past medical history, no additional past surgical
history and no family history of malignancy.
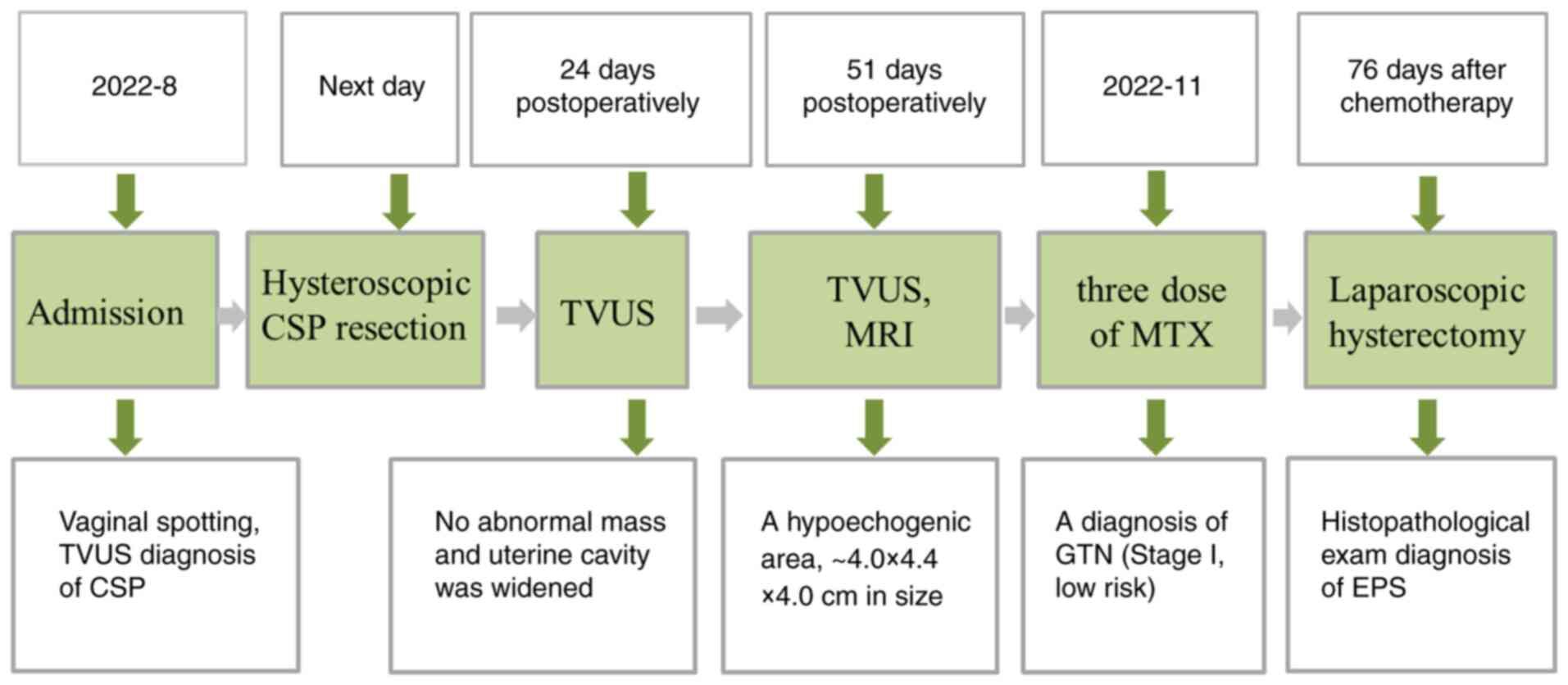
The patient first visited Jinan University First
Affiliated Hospital in August 2022, presenting with vaginal
spotting and abdominal discomfort after amenorrhea for 37 days.
Laboratory tests revealed elevated serum β-human chorionic
gonadotropin (β-hCG) levels (22,200 mIU/ml) (normal, 217-71,380
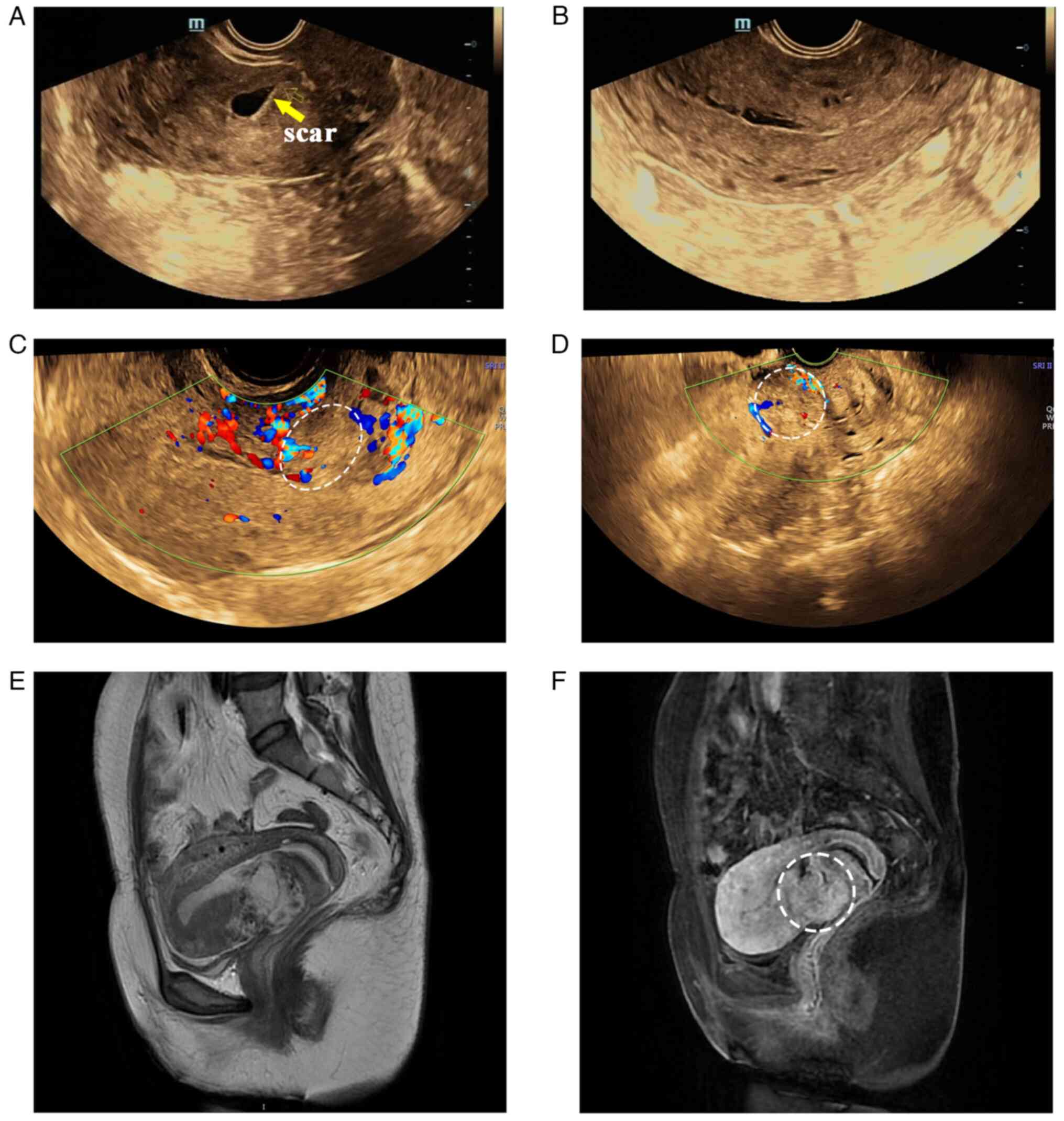
mIU/ml) (UniCel DXI 800; Beckman Coulter, Inc.). Ultrasound
examination revealed a gestational sac located at the anterior part
of the uterine isthmus within the previous hysterotomy site, which
was diagnosed as CSP (Fig. 1A).
The next day, a hysteroscopic resection was performed and the
postoperative course was uncomplicated, with a decreased β-hCG
level (17,965 mIU/ml) on the second postoperative day. At the
24-day postoperative follow-up visit, the patient's physical
examination revealed no abnormalities except for elevated β-hCG
levels (76,196 mIU/ml). During transvaginal ultrasonography (TVUS)
examination, the uterine cavity in the lower segment was widened by
6 mm compared to normal uterine cavity, No mass was detected in the
wall of the uterus (Fig. 1B). The
patient was encouraged to maintain close follow-up.
At 51 days postoperatively, the patient experienced
vaginal bleeding for three days and was readmitted. β-hCG levels
were 2,799 mIU/ml. TVUS showed a hypoechogenic tumor-like area,
5.8x2.7 cm in size, with unclear borders within the myometrium of
the lower uterine segment, at the site of the previous cesarean
section (Fig. 1C). The color
Doppler image revealed an abundant blood flow signal (Fig. 1D). T1 and T2-weighted magnetic
resonance imaging (MRI) (Discovery MR750 3.0T; GE Healthcare)
further confirmed a heterogeneous mass in the previous cesarean
scar, ~4.0x4.4x4.0 cm in size, surrounded by an enlarged and
thickened vascular shadow (Fig. 1E
and F). Based on these findings, a
gestational trophoblastic tumor was suspected. Finally, a diagnosis
of GTN (stage I, low risk) was made. The patient then received
adjuvant single-agent chemotherapy with methotrexate (MTX, 20 mg/d)
for 5 days (3 cycles). The serum β-hCG level decreased sharply to
8.5 mIU/ml 60 days after MTX treatment, and TVUS examination
revealed that there was no change in the size of the hypoechogenic
area. The patient requested hysterectomy due to the serious side
effects of chemotherapy and no desire to preserve her fertility,
and she ultimately underwent total laparoscopic hysterectomy and
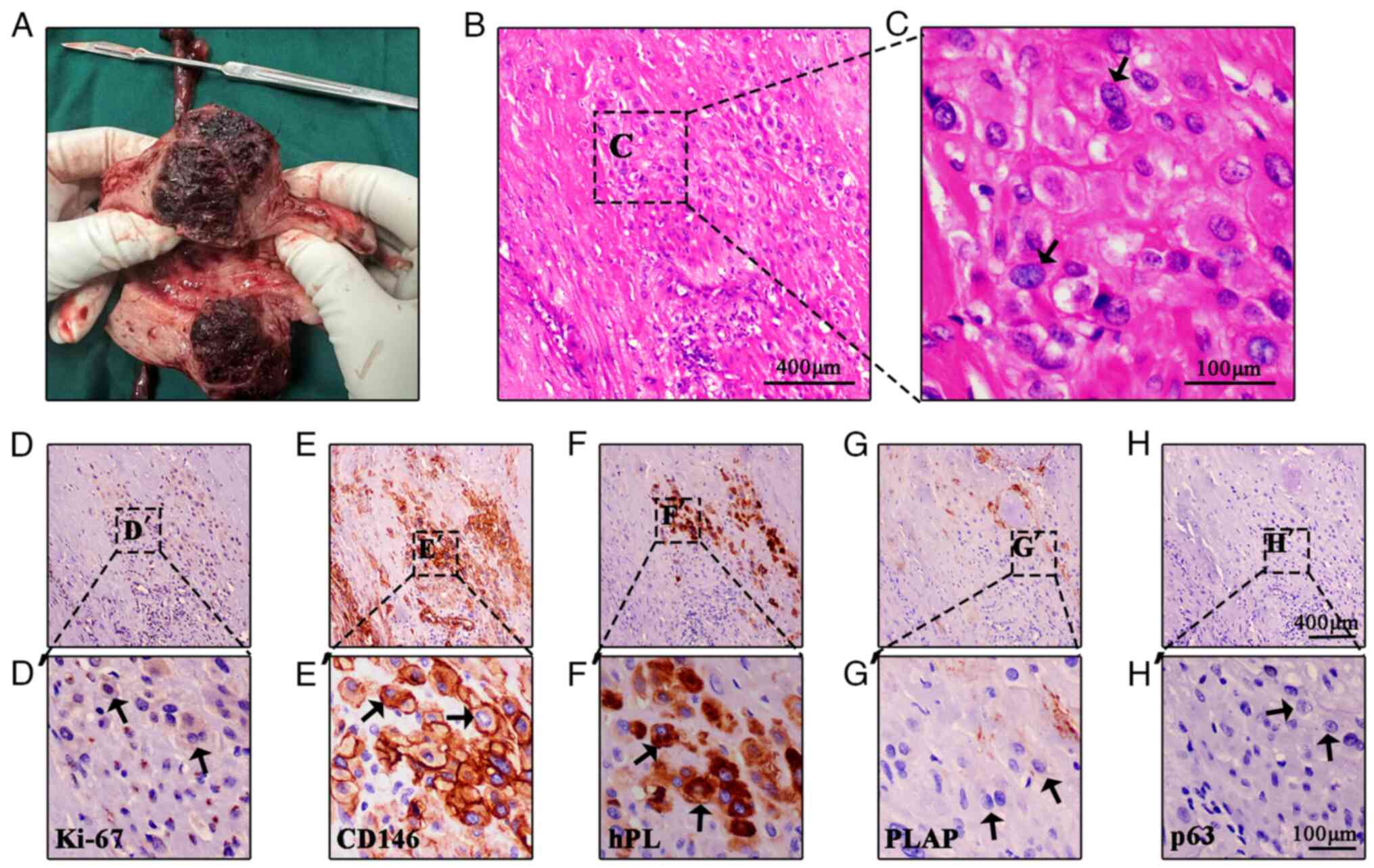
bilateral salpingectomy 76 days after MTX treatment. Intraoperative
exploration revealed that the uterus was enlarged and distorted,
and there was a purple bulge in the anterior and inferior segments
of the uterus. The dissected whole uterus including the lesion is
presented in Fig. 2A. A 5x4x3 cm
mass was observed in the lower uterine segment near the endocervix,
which appeared to infiltrate almost the full thickness of the
myometrium on both the anterior and posterior walls with a thin rim
of intact myometrium. The mass appeared tough in texture with
hemorrhage and necrosis indicated by a dark red color (Fig. 2A). The tissues were fixed in 10%
(v/v) neutral buffered formalin for 24 h at room temperature,
dehydrated in ethanol, cleared in xylene and embedded in wax,
sectioned and stained with hematoxylin and eosin (H&E) at room
temperature for 10 min. Serial sections (5 µm) were also prepared
for immunohistochemistry staining. The histopathological
examination and immunohistochemistry staining was performed as
previously described (5). However,
histopathological examination revealed a few intact hydropic
chorionic villi and intermediate trophoblast cell aggregation in
the superficial myometrium (Fig.
2B and C). Intermediate
trophoblasts had large eosinophilic cytoplasm and hyperchromatic
nuclei of variable shapes and sizes, and were surrounded by
calcification areas and a hyaline matrix with low Ki-67 (1:2,000
dilution; cat. no. 27309-1-AP; Proteintech Group, Inc.).
Intermediate trophoblast cells were diffusely positive for CD146
[ready-to-use; cat. no. GT234602; GeneTech (Shanghai) Co., Ltd.]
and human placental lactogen [hPL; ready-to-use, cat. no. GT220502;
GeneTech (Shanghai) Co., Ltd.], but were negative for placental
alkaline phosphatase (PLAP; ready-to-use; cat. no. GM719102; DaKo;
Agilent Technologies, Inc.) and p63 (ready-to-use; cat. no.
790-4509; Ventana; Roche Diagnostics GmbH) (Fig. 2D-H). Based on the histological and
immunohistochemical findings, the patient was diagnosed with EPS.
The postoperative course was uneventful. The patient was discharged
without any adjuvant treatment because she had a β-hCG level of 0.9
mIU/ml (normal, <5 mIU/ml) on postoperative day 7. There were no
observable abnormalities. The β-hCG levels of the patient was
checked every month and remained normal during the 12 consecutive
month follow-up. The timeline of events is provided in Fig. 3.
Discussion
Although CSP is generally considered rare, its
incidence has risen due to the high rate of cesarean section in
recent years (5). CSP carries a
risk for morbidly adherent placenta and further substantial
postpartum hemorrhage, with a substantial risk of mortality and a
risk of recurrence. Furthermore, the incidence of retained products
of conception (RPOC), indicating the persistence of placental
tissue, is greater in women with CSP than in those with
intrauterine miscarriages (7).
Thus, although hysteroscopic removal is used as an effective
treatment, CSPs may occasionally be associated with complications
due to continuous growth of the retained tissue (8). It was reported that 3.3% of GTNs are
located in cesarean scars (9),
with rare case reports on choriocarcinomas, PSTTs and ETTs and a
high rate of misdiagnosis (10).
Indeed, it is crucial but challenging to make an acute diagnosis of
GTN and tumor-like lesions by histology (10). For CSP choriocarcinoma,
misdiagnosis can result in delayed treatment or even tumor
metastasis (2). Early diagnosis
and effective treatment remain key for the successful management of
cesarean scar complications.
By contrast, there is no specific treatment for EPS,
although follow-up of β-hCG levels is necessary. EPS may also be
present in women with CSP and there are very few reports describing
the clinical course of EPS (10,11).
The pathogenesis of EPS has not been clearly determined. It has
been speculated that EPS is an exuberant infiltration of the
endometrium and myometrium through the implantation site
intermediate trophoblasts (ISITs), mainly due to decidual
deficiency. In normal pregnancy, the decidua serves to not only
limit the depth of trophoblast invasion by the secretion of a range
of factors, but also facilitates the differentiation of
trophoblasts to noninvasive giant cells. In addition, uterine
myometrial destruction in cesarean scars is an important factor in
the deep invasion of ISITs (12).
Histologically, EPSs have infiltrative borders and
are composed of ISITs that are arranged on cords, nests and
diffusers. Although reliable quantitative histological criteria are
lacking, the course of GTN may be invasive and involve metastasis.
The differential diagnosis of these lesions is made using
immunohistochemical staining for p63, hPL and Ki-67 in addition to
histological findings (1). PSTTs
are positive for hPL while having a lower serum β-hCG level, often
variable mitotic activity, the absence of villi and an elevated
Ki-67 index (1). In the present
case, a lower percentage of positive Ki-67 staining supported a
diagnosis of EPS rather than of PSTT. Furthermore, a concurrent
pregnancy and no mass in the myometrium are helpful for the
diagnosis of EPS. However, under rare circumstances, EPS may
exhibit unusual imaging features of heterogeneous masses and can
cause diagnostic confusion. In the present case, the patient
presented with irregular bleeding and increased β-hCG levels, and
the possibility of EPS, PSTT or choriocarcinoma was considered.
Although hysteroscopic resection was used to terminate the CSP,
ultrasonography and MRI showed that the mass did not change in size
and was still hypervascular; this was easily mistaken for GTN in
cesarean scar. The treatment option was the administration of MTX
with prolonged follow-up of β-hCG levels, since chemotherapy is a
standard treatment option for GTN (13).
However, with the histological findings, including
the proliferation of trophoblasts in the placental site with no
mitotic activity, and a low Ki-67 labeling index, the diagnosis of
EPS was suitable (3). In fact, a
correct diagnosis of EPS can be made and identified by routine
histological and immunohistochemical examination (1). However, EPS has not received much
attention in our department. In addition, hysteroscopic resection
is not needed for the management of GTN (13). Since preservation of fertility was
not desired, GTN was suspected, chemotherapy had serious side
effects and total hysterectomy was performed, this may have been
the reason for the misdiagnosis of GTN, leading to inappropriate
surgical management.
In conclusion, the current study presented a rare
case of EPS in a cesarean scar that was misdiagnosed as GTN by
ultrasonography and MRI, resulting in unnecessary surgical
treatment. EPS differs from GTN both clinically and pathologically
and should be considered a possible diagnosis in any woman who has
irregular bleeding following CSP resection. The Ki67 labeling index
and the ISITs (hPL and CD146) are particularly useful in the
differential diagnosis of an EPS from a GTN. The present case is
unique because of the rare intrauterine mass and possibility of
subsequent RPOC causing trophoblastic changes. EPS is difficult to
diagnose without histopathological examination of hysterectomy
specimens. Awareness of EPS and recognition of various types of
trophoblastic diseases in women with cesarean scars are important
for preventing misdiagnosis and guiding patient management,
particularly in reproductive-age women who desire further
pregnancies.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by the Guangdong Basic and
Applied Basic Research Foundation (grant nos. 2024A1515011821 and
2023A1515140168); and the University and Hospital Joint Fund of The
Chinese University of Hong Kong Second Affiliated Hospital,
Shenzhen (grant no. YXLH2219).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article
Authors' contributions
ZC recruited the patient, obtained specimens and
collected the images. HS and PL conceived the study, provided
financial support and wrote the manuscript. MW analyzed the data
and prepared the figures. BY and PY performed the histological
analyses. HS and PL confirm the authenticity of all the raw data.
All of the authors have read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Clinical Trial Ethics
Committee of the Jinan University First Affiliated Hospital
(Guangzhou, China; approval no. KY-2023-143).
Patient consent for publication
Written informed consent for publication of the case
report and images was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kaur B: Pathology of gestational
trophoblastic disease (GTD). Best Pract Res Clin Obstet Gynaecol.
74:3–28. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Takebayashi A, Kimura F, Yamanaka A,
Takahashi A, Tsuji S, Ono T, Kaku S, Kita N, Takahashi K, Okabe H
and Murakami T: Exaggerated placental site, consisting of
implantation site intermediate trophoblasts, causes massive
postpartum uterine hemorrhage: Case report and literature review.
Tohoku J Exp Med. 234:77–82. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ozdemir O, Sari ME, Selimova V, Ilgin BU
and Atalay CR: A case report of complete mole with co-existent
exaggerated placental site reaction and review of the literature.
Niger Med J. 55:180–182. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zhou X, Li H and Fu X: Identifying
possible risk factors for cesarean scar pregnancy based on a
retrospective study of 291 cases. J Obstet Gynaecol Res.
46:272–278. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Gao L, Chen H, Liu J, Wang M, Lin F, Yang
G, Lash GE and Li P: Extravillous trophoblast invasion and
decidualization in cesarean scar pregnancies. Acta Obstet Gynecol
Scand. 101:1120–1128. 2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Yang C, Li J, Zhang Y, Xiong H and Sheng
X: Epithelioid trophoblastic tumor coexisting with choriocarcinoma
around an abdominal wall cesarean scar: A case report and review of
the literature. J Med Case Rep. 14(178)2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lin F, Chen Z, Tao H, Ren X, Ma P, Lash
GE, Shuai H and Li P: Sonographic findings of vascular signals for
retained products of conception in women following first trimester
termination of pregnancy. J Obstet Gynecol Can.
46(102266)2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Qian ZD, Weng Y, Du YJ, Wang CF and Huang
LL: Management of persistent caesarean scar pregnancy after
curettage treatment failure. BMC Pregnancy Childbirth.
17(208)2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Wang X, Li Y, Yang J, He Y, Wang M, Wan X
and Xiang Y: Identification and treatment of gestational
trophoblastic neoplasia located in the cesarean scar. Int J
Gynaecol Obstet. 141:222–227. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Jashnani KD, Sangoi NN, Pophalkar MP and
Patil LY: Caesarean scar ectopic pregnancy masquerading as
gestational trophoblastic disease. J Postgrad Med. 68:35–37.
2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Akbayir O, Alkis I, Corbacioglu A, Ekiz A,
Akca A and Cekic S: Exaggerated placental site reaction detected
during caesarean delivery: A case report. Clin Exp Obstet Gynecol.
39:234–235. 2012.PubMed/NCBI
|
|
12
|
Cramer SF and Heller DS: Placenta increta
presenting as exaggerated placental site reaction. Pediatr Dev
Pathol. 20:152–157. 2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Hoeijmakers YM, Eysbouts YK, Massuger
LFAG, Dandis R, Inthout J, van Trommel NE, Ottevanger PB, Thomas
CMG and Sweep FCGJ: Early prediction of post-molar gestational
trophoblastic neoplasia and resistance to methotrexate, based on a
single serum human chorionic gonadotropin measurement. Gynecol
Oncol. 163:531–537. 2021.PubMed/NCBI View Article : Google Scholar
|