The coronavirus disease 2019 (COVID-19) outbreak has
spread worldwide with overwhelming speed, infecting >48.3
million individuals and causing >1.23 million deaths across ~200
countries as of 2nd of November, 2020 (1). COVID-19, caused by SARS-CoV-2 virus,
hit China, the US and European countries considerably hard, with
the aforementioned countries becoming the epicentres of the
SARS-CoV-2 virus pandemic (2).
Early prevention of transmission of SARS-CoV-2 via imposed
lockdowns and social distancing have been the primary means of
preventing the spread of COVID-19 (2,3).
Strategies aimed at interrupting interactions
between the virus and host have been primarily utilised from the
viewpoint of public epidemiology (4,5).
To control the spread of the virus, several countries have limited
or outright banned accesses to international flights, locked down
the entire country or several cities, have instructed the public to
follow social distancing measures, and made the wearing of masks
either mandatory or recommended. Moreover, body temperatures are
being measured wherever individuals congregate and social
activities have been diminished in hopes of curbing peak prevalence
and death (5-7). Remdesivir has received emergency use
authorization by the US Food and Drug Administration (FDA) for the
treatment of COVID-19 (8) for
SARS-CoV-2 virus infections (1).
However, the development of novel agents and vaccines against
SARS-CoV-2 is now one of the most intensively researched subjects
worldwide.
The current review summarises the clinical
manifestations, SARS-CoV-2 viral genome structure and sequence,
SARS-CoV-2 viral life cycle, diagnosis, preventative methods, and
management measures of COVID-19. Finally, an over-view is provided
of the possible molecular pharmacological mechanisms of
anti-SARS-CoV-2 agents and the effectiveness of remdesivir
(GS-5734), chloroquine, hydroxychloroquine, steroids and
anti-coagulant agents as well as traditional Chinese medicines
(TCM) for management of COVID-19.
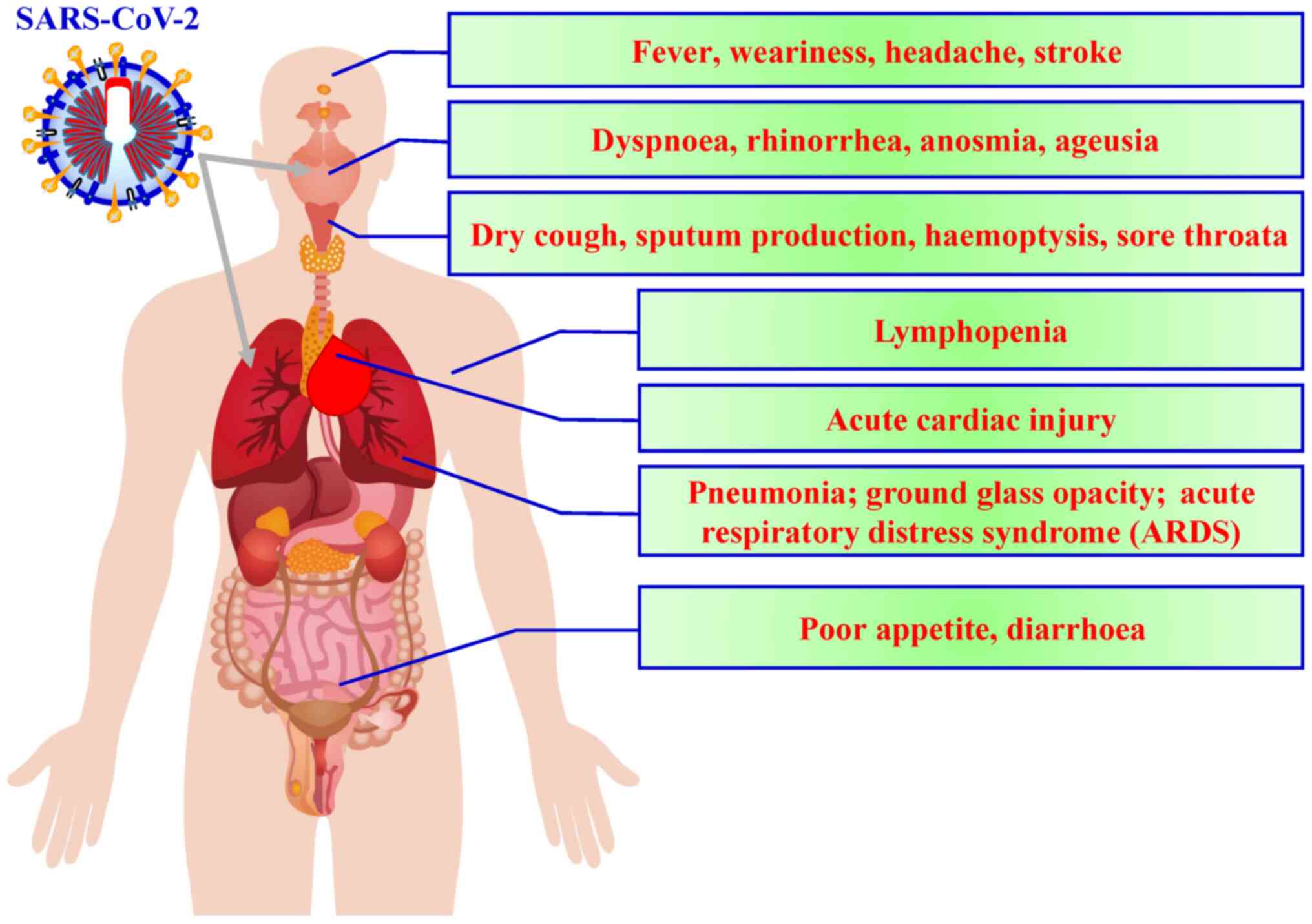
According to the current literature, fever, dry
cough and fatigue are the most common symptoms observed at the
onset of COVID-19, with other symptoms including muscle pain,
productive cough, headache, diarrhoea, dyspnoea and haemoptysis
developing later (Fig. 1)
(9). Symptoms gener-ally appear
~5.2 days after COVID-19 (10).
Although 50-75% of patients with COVID-19 remain asymptomatic, ~14%
of infected individuals present with serious symptoms requiring
hospitalisation and oxygen therapy, while 5% require intensive
care. The median duration from symptom onset to intensive care unit
admission is ~10 days, while the duration between symptom onset and
death ranges from 2-8 weeks (10-13).
Coronaviruses primarily cause respiratory and
gastrointestinal tract infections and are genetically classified
into four major genera: α-coronavirus, β-coronavirus, γ-coronavirus
and δ-coronavirus (27). Six
types of human coronaviruses have been previously identified, which
include HCoV-NL63 and HCoV-229E belonging to the α-coronavirus
genus and HCoV-OC43, HCoV-HKU1, SARS-CoV and MERS-CoV belonging to
the β-coronavirus genus (27).
Coronaviruses had not attracted worldwide attention until the 2003
SARS pandemic, followed by the 2012 MERS and, most recently, the
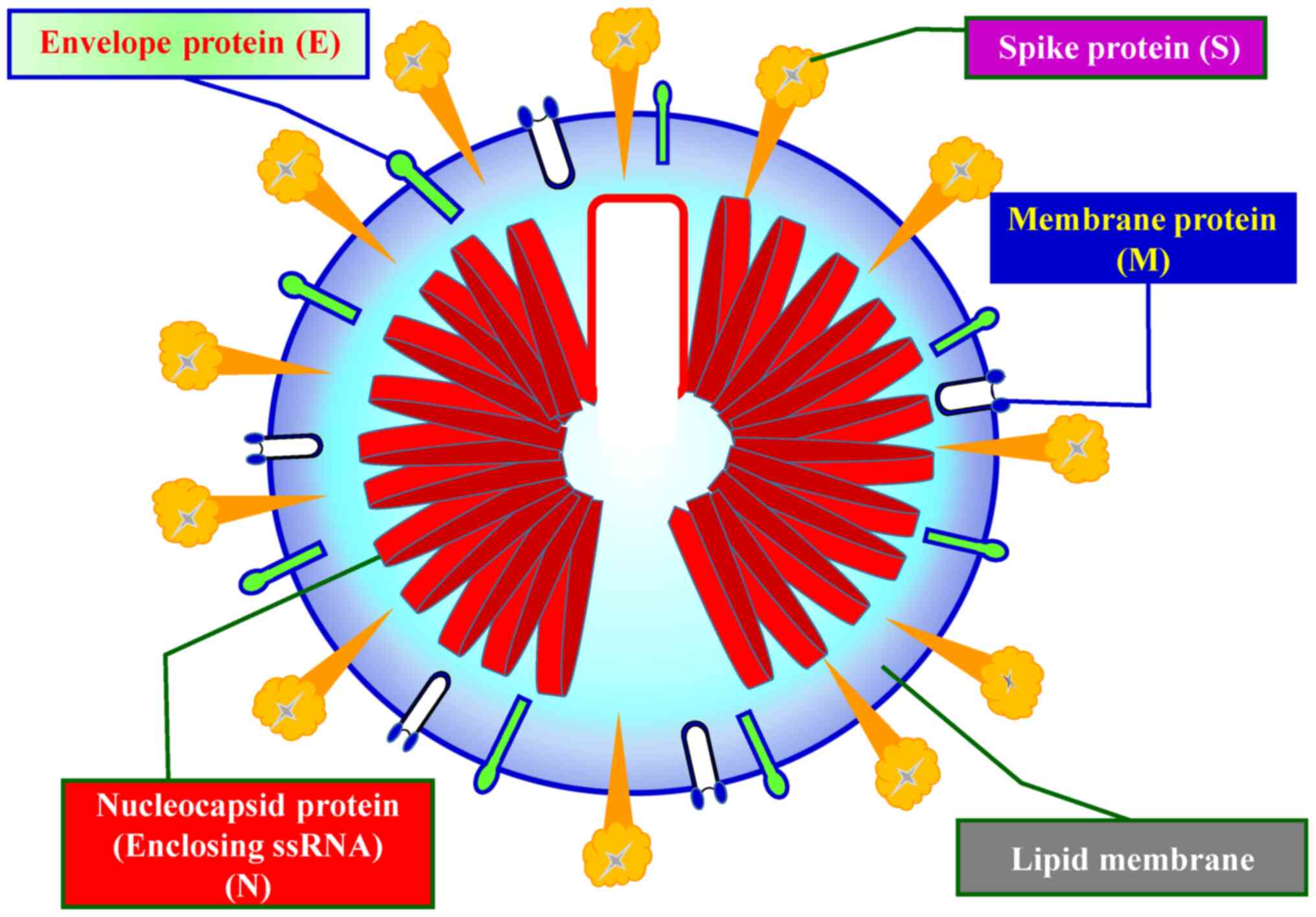
COVID-19 outbreaks (27). Both
SARS-CoV-2 and MERS-CoV have been considered highly pathogenic
(28). Fig. 2 shows the schematic structure of
SARS-CoV-2 (29,30).
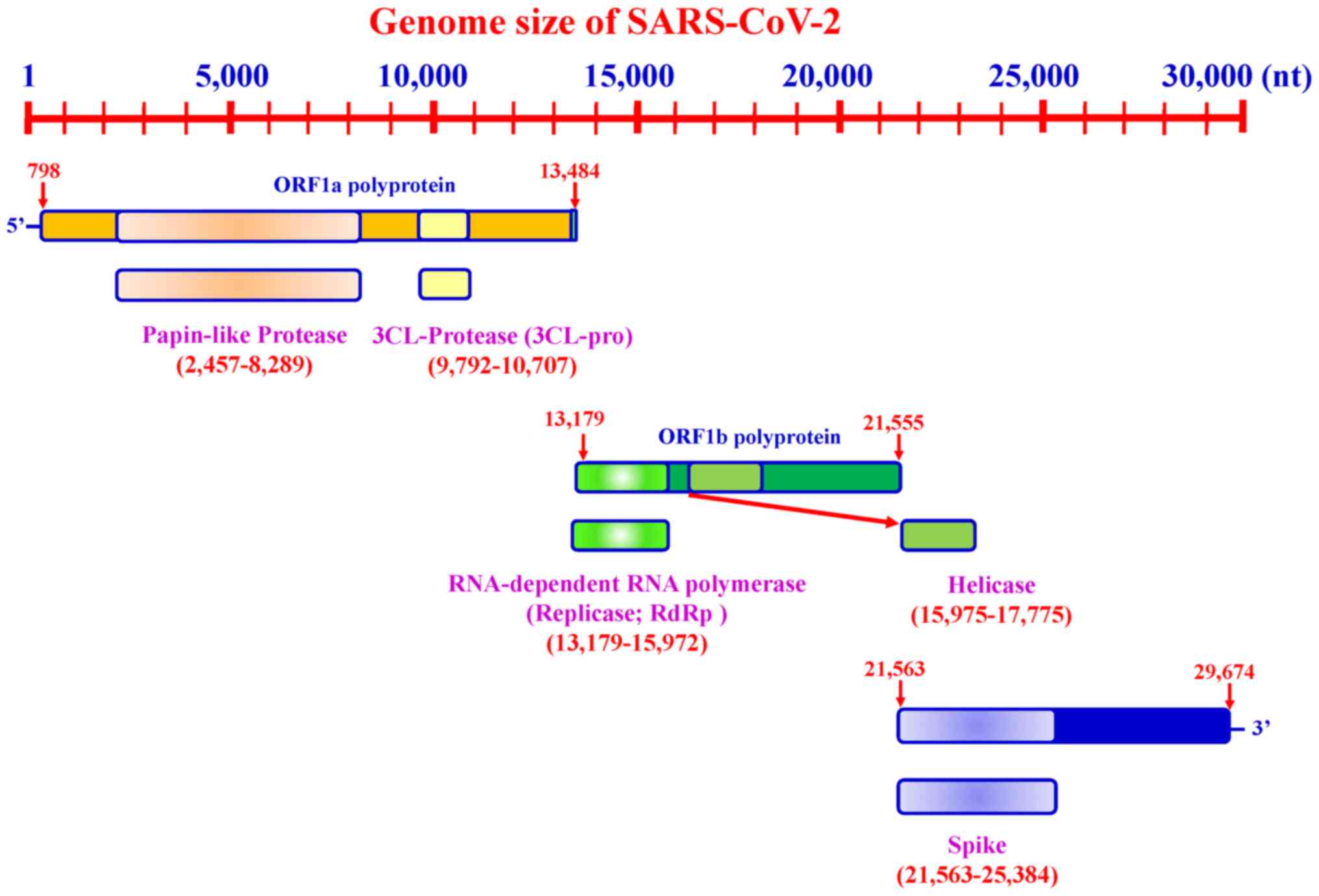
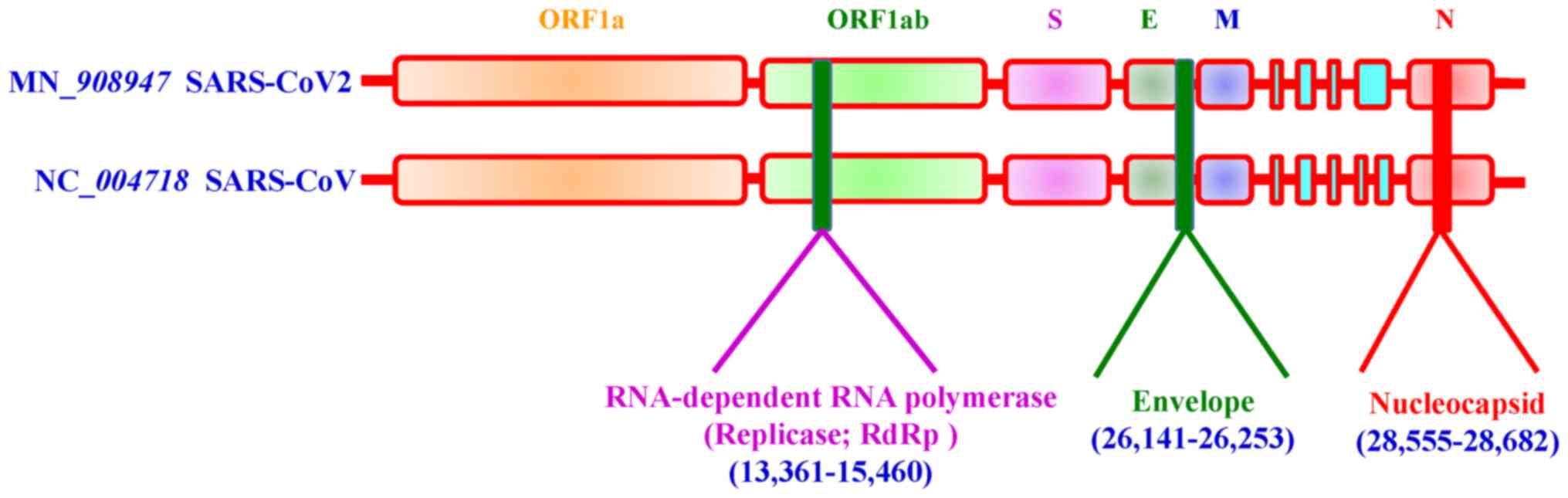
SARS-CoV-2 possesses a genome length of ~30 kb.
Accordingly, SARS-CoV-2 genome sequences from NCBI (30), covering between ~798 and 29,674
bases, include a variable number of open reading frames (ORFs)
(Fig. 3). The first ORF,
representing ~67% of the entire genome, encodes two large
polyproteins, PP1a and PP1ab, which are proteolytically cleaved
into 16 non-structural proteins (NSPs), including papain-like
protease, 3-chymotrypsin-like cysteine protease (3CLpro),
RNA-dependent RNA poly-merase (RdRp), helicase and exonuclease
(ExoN). The remaining ORFs encode accessory and structural
proteins. The four major structural proteins include the spike
surface glycoprotein (S) (31),
envelope protein (E) (32),
membrane (M) (33) and
nucleocapsid protein (N) (34).
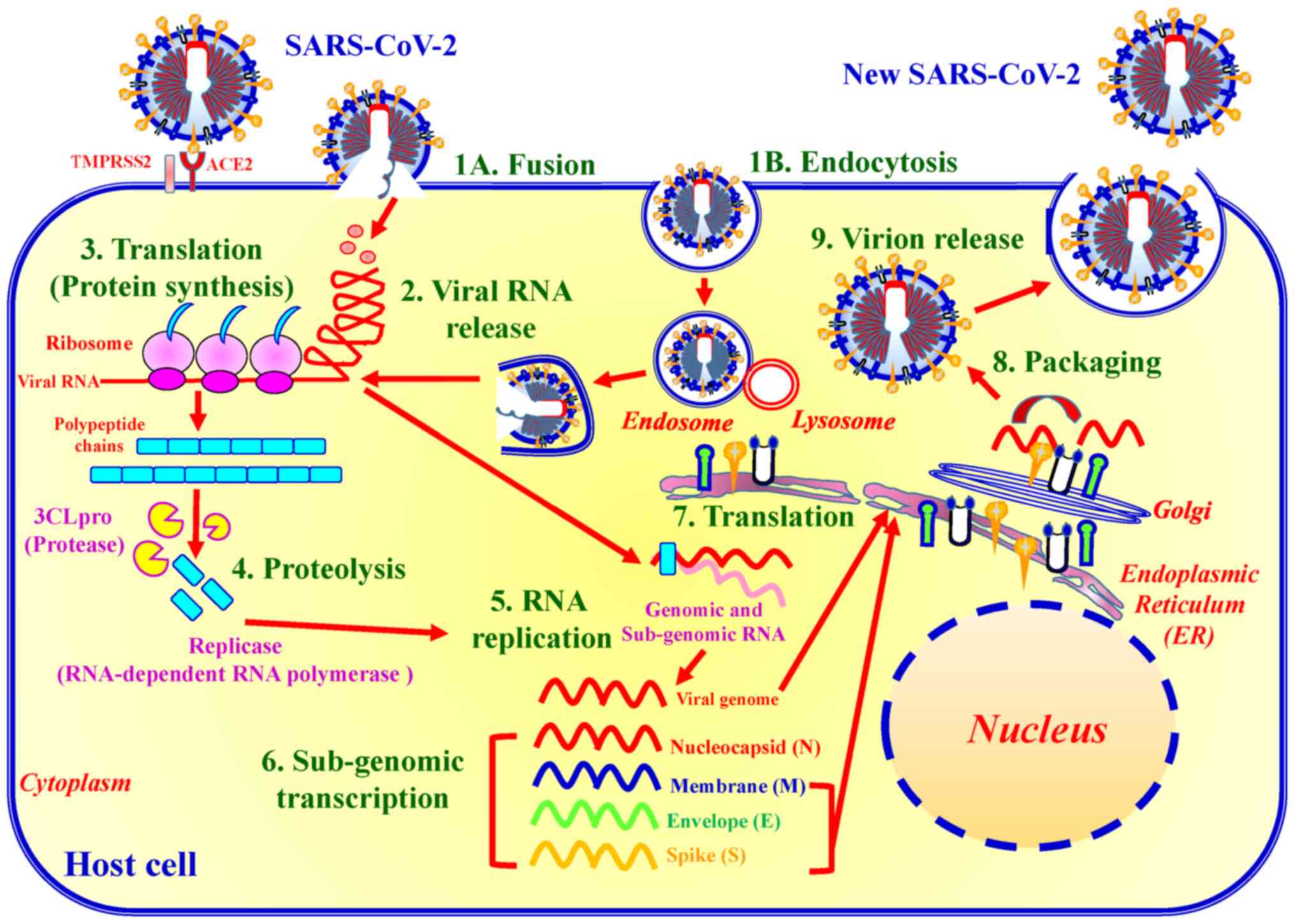
Recent studies have revealed six major NSP subtypes, including nsp3
(35), nsp4 (36), nsp6 (37), nsp12 (38), nsp13 (39) and nsp14 (38) for SARS-CoV-2. Spike proteins of
viruses bind to host cell receptors for entry. Accordingly, the
spike proteins of SARS-CoV-2 and MERS-CoV bind to different host
receptors through different receptor-binding domains. SARS-CoV-2
uses angiotensin-converting enzyme 2 (ACE2) as one of the main
receptors with CD209L as an alternative receptor, whereas MERS-CoV
uses dipeptidyl peptidase 4 (DPP4, also known as CD26) as its
primary receptor (40-44). The cleavage of trimer S protein is
initiated by the cell surface-associated transmembrane protease
serine 2 (TMPRSS2) and cathepsin (45,46).
Two approaches have generally been utilised for the
diagnostic screening of SARS-CoV-2: i) Reverse
transcription-quantitative PCR (RT-qPCR) and, ii) rapid screening
(48,49). Detection time and duration until
COVID-19 diagnosis are detailed in Table II.
RT-qPCR assay utilises viral RNA extracted from
patient samples (for example, material collected through
nasopharyngeal and oropharyngeal swabs), synthesises of
complementary DNA (cDNA) through the action of a reverse
transcriptase enzyme, and amplifies the target sequences of the
viral genome from the cDNA template. RT-qPCR can be interpreted
semi-quantitatively, with the target amplification speed dependent
on the concentration and quality of the viral RNA in the initial
sample, thereby allowing the amplification rate to be used as a
proxy for the sample viral load (49). The three target screening assays
include E gene, RdRp gene and N assaying (Fig. 5) (50). For a routine workflow, the Taiwan
Centers for Disease Control recommends the E gene assay as the
first-line screening tool, followed by confirmatory testing with
the RdRp gene assay. Utilising the RdRp gene assay with dual colour
technology can discriminate between SARS-CoV-2 (both probes
positive) and SARS-CoV RNA provided that the latter is used as a
positive control. Alternatively, laboratories may choose to run the
RdRp assay with only the SARS-CoV-2-specific probe. Despite also
performing well, the N gene assay has not been subjected to further
intensive validation given its slightly inferior sensitivity
(51).
To date, five antibody-based tests have been used
for detecting the presence of IgG and IgM in body fluids, such as
whole blood, serum or plasma. The BioMedomics rapid test and
Surescreen rapid test cassette utilise lateral flow immunoassays,
which are diagnostic devices used to examine antibodies (12,52-55). Moreover, Goldsite diagnostics has
developed a time-resolved fluorescence immunoassay kit, while the
Assay Genie rapid POC kit and VivaDiag COVID-19 IgG-IgM tests are
colloidal gold-based immunoassays for detecting viral infection
(56). To perform the assay, a
few drops of blood obtained from the individual using a
finger-stick or vein are applied onto the immunoassay. A few drops
of buffer solution are then added onto the assay, after which the
results are obtained within 10-15 min at room temperature. RT-qPCR
testing is used as the reference standard to which immunoassays are
compared. Amongst the five rapid screening tests, the BioMedomics
IgM-IgG rapid test has been widely used for detecting antibody
production in the human body (57).
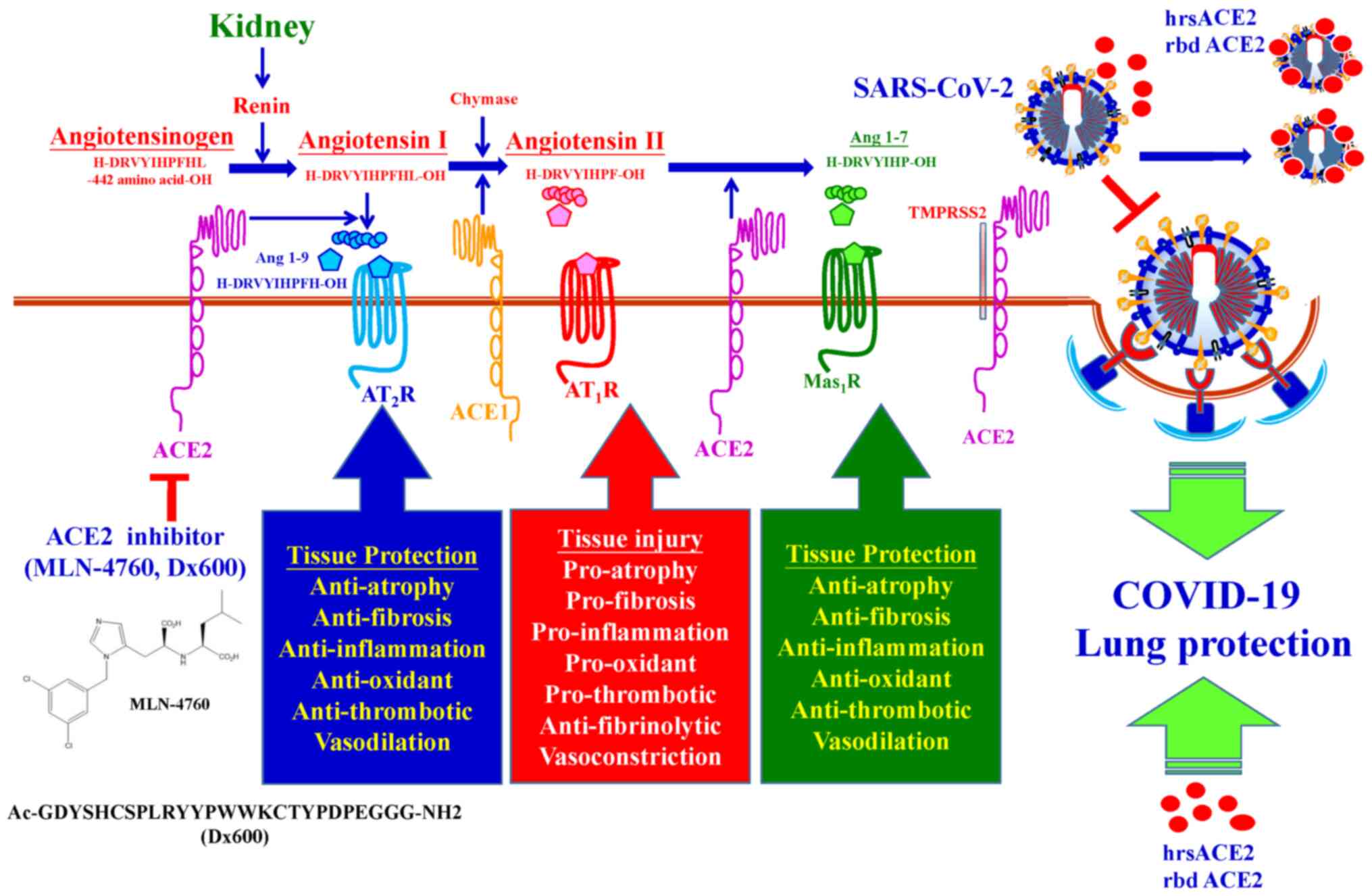
SARS-CoV-2 possesses several problematic properties,
such as transmission from asymptomatic individuals and nonspecific
features of COVID-19, and utilises the ACE2 and TMPRSS2 receptors
for attachment and transmission (31,59). Both ACE2 and TMPRSS2 proteins are
expressed in <10% of human respiratory and gastrointestinal
tract cells, including nasal goblet secretory cells, lung type II
pneumocytes and ileal absorptive enterocytes (60,61). At present, prevention of viral
entry into the human body has been the best option for controlling
viral spread. The TCDC has established technical guidelines for
COVID-19 (1). The following are
crucial steps for preventing viral spread: i) Stay at home, unless
essential, the general public should avoid travelling to affected
countries and regions, as well as avoiding contact with animals,
dead or alive. The general public should make a habit of applying
alcohol-based hand sanitisers after entering any public spaces. ii)
Maintain decontamination: Rooms should be regularly decontaminated,
preferably with 5 to 10% sodium hypo-chlorite. iii) Keep a safe
social distance, the general public must avoid public gatherings.
Individuals should preferably maintain a distance of at least 1.5 m
(5 ft) between themselves and anyone who is coughing or sneezing
indoors. Individuals should maintain a distance of at least 1 m (3
ft) distance between themselves and anyone else outdoors. iv)
Regularly sanitize hands, individuals are advised to practice
appropriate hygiene, such as frequently washing their hands with
soap after sneezing or coughing. Avoid touching any secretions,
such as stool or urine. In addition, individuals should refrain
from touching their eyes, nose and mouth with unclean hands. v)
Wear face masks, healthcare personnel must use personal protective
equipment, such as medical masks (including surgical face masks and
N95s), eye protection, gloves, gowns and protective gear. The
general public must wear a face mask to help prevent viral
transmission, particularly in public spaces. Given the supply
shortages, each country has their own recommendations regarding
wearing of face masks.
Given the lack of clinical evidence supporting the
efficacy of any existing anti-viral agents or the existence of
vaccines which have completed Phase II clinical trials and have
been approved by a regulatory body for COVID-19, supportive
treatments for clinical conditions in the early stages is
imperative. In addition, conservative fluid management should be
employed among patients with COVID-19 when no evidence of shock is
present. Details and targets of supportive treatments for clinical
conditions are presented in Table
III (26).
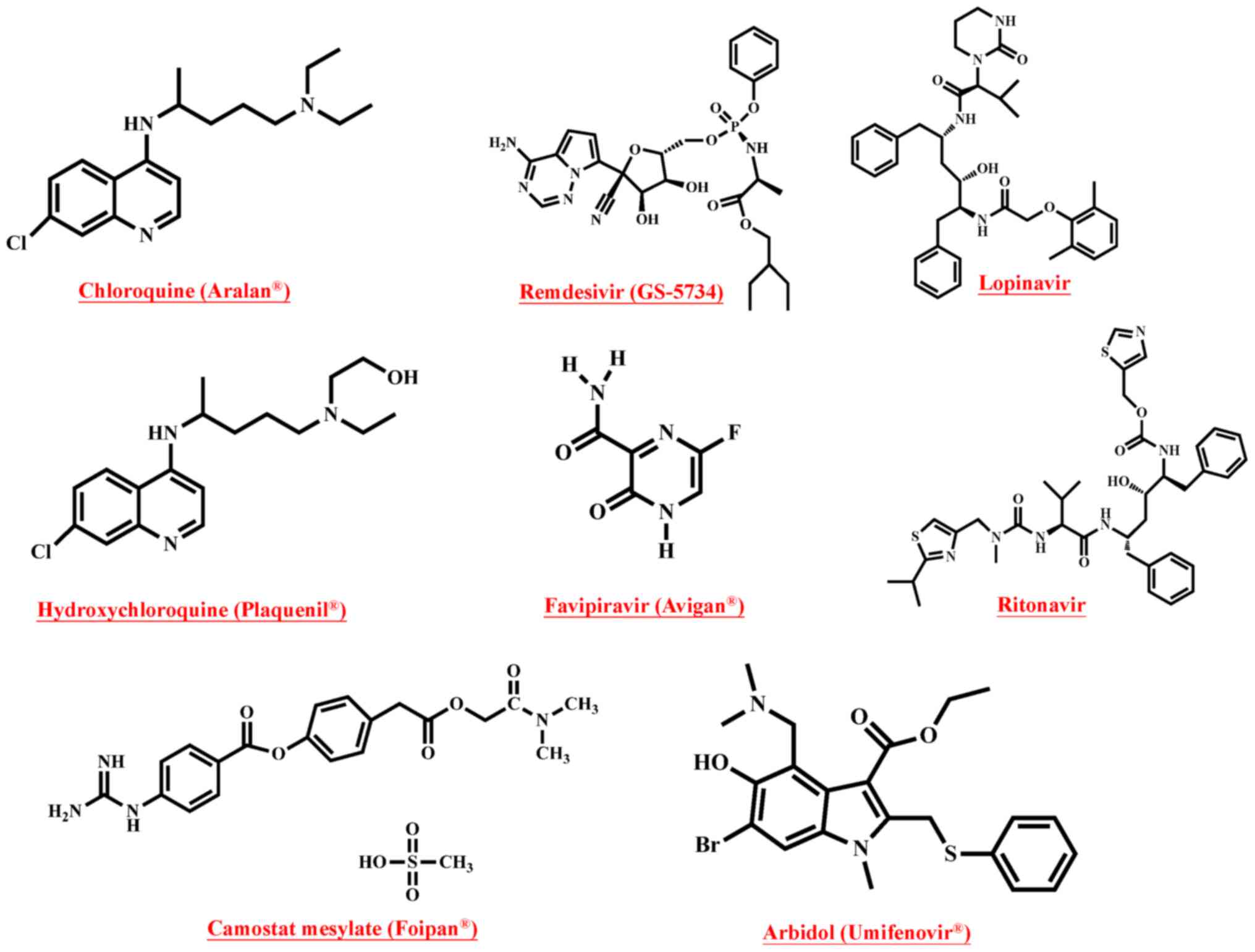
Several ongoing clinical trials have evaluated the
following direct treatments for SARS-CoV-2: Chloroquine
(Aralan®), hydroxychloroquine (Plaquenil®),
arbidol (Umifenovir®), camostat mesylate
(Foipan®), remdesivir (GS-5734), favipiravir
(Avigan®), ribavirin (Rebetol®),
lopinavir/ritonavir (Kaletra®) and interferon-α and
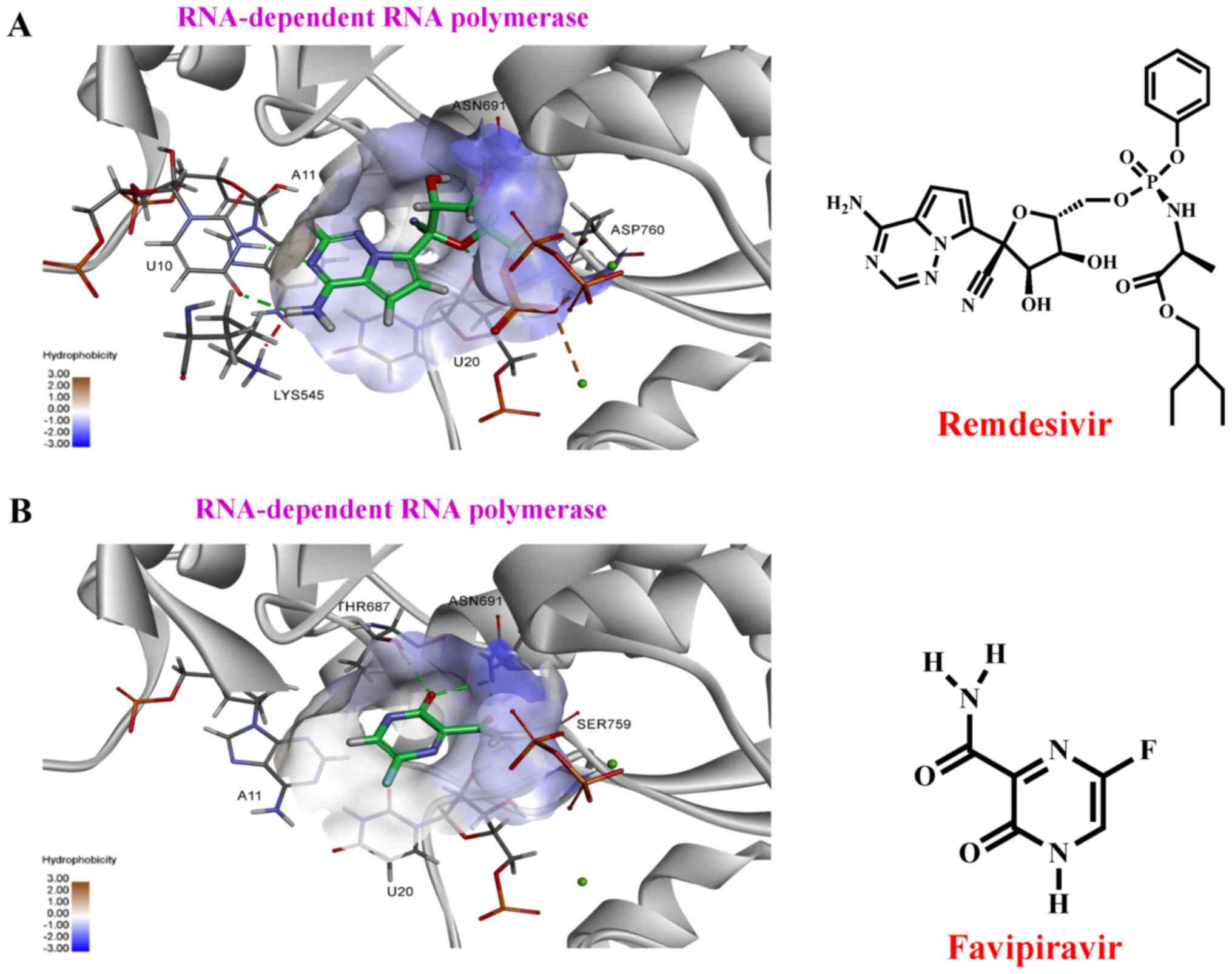
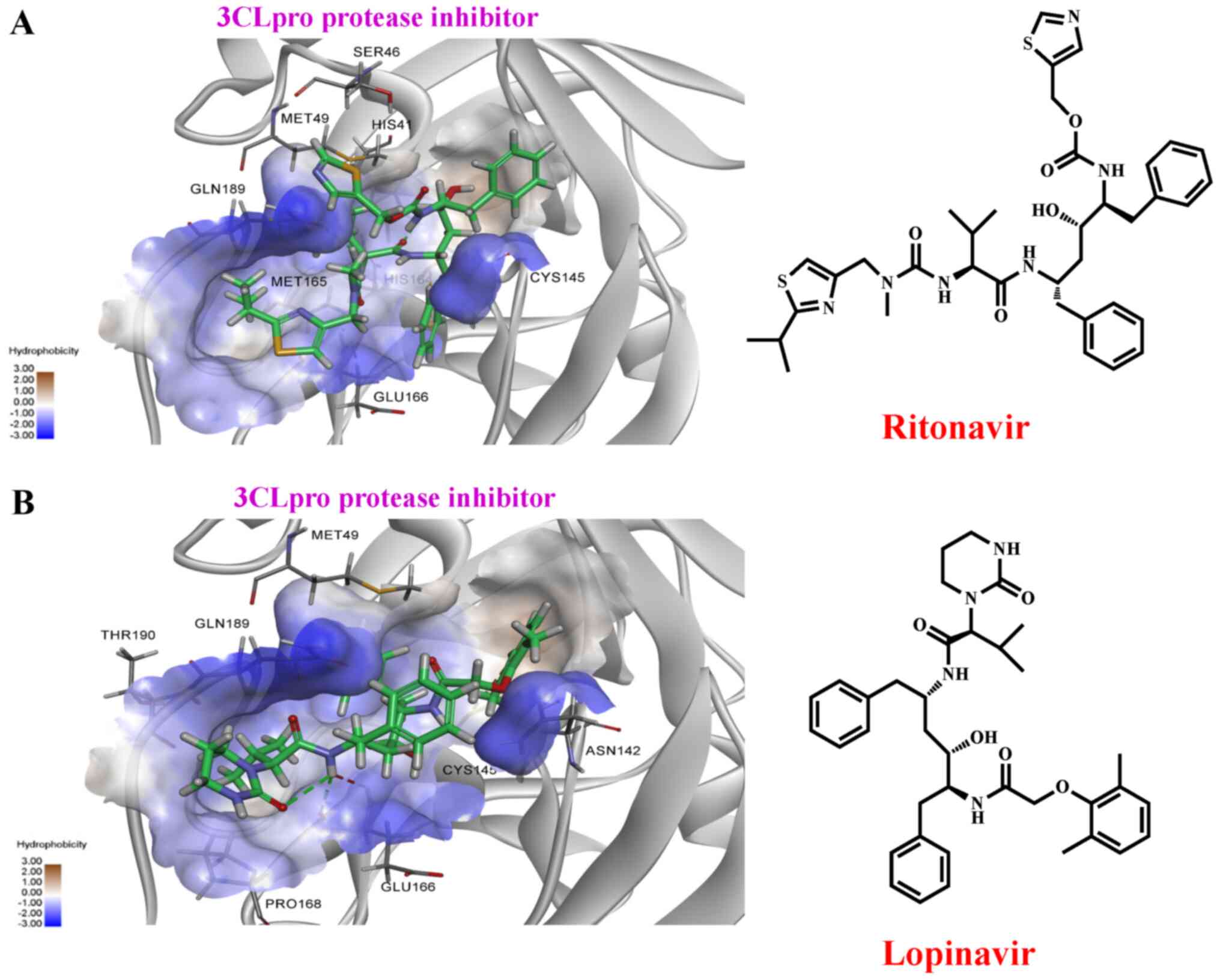
interferon-β (47). The chemical
structures of hydroxychloroquine (Plaquenil®),
chloroquine (Aralan®), remdesivir (GS-5734), favipiravir
(Avigan®), ribavirin (Rebetol®),
lopinavir/ritonavir (Kaletra®), and camostat mesylate
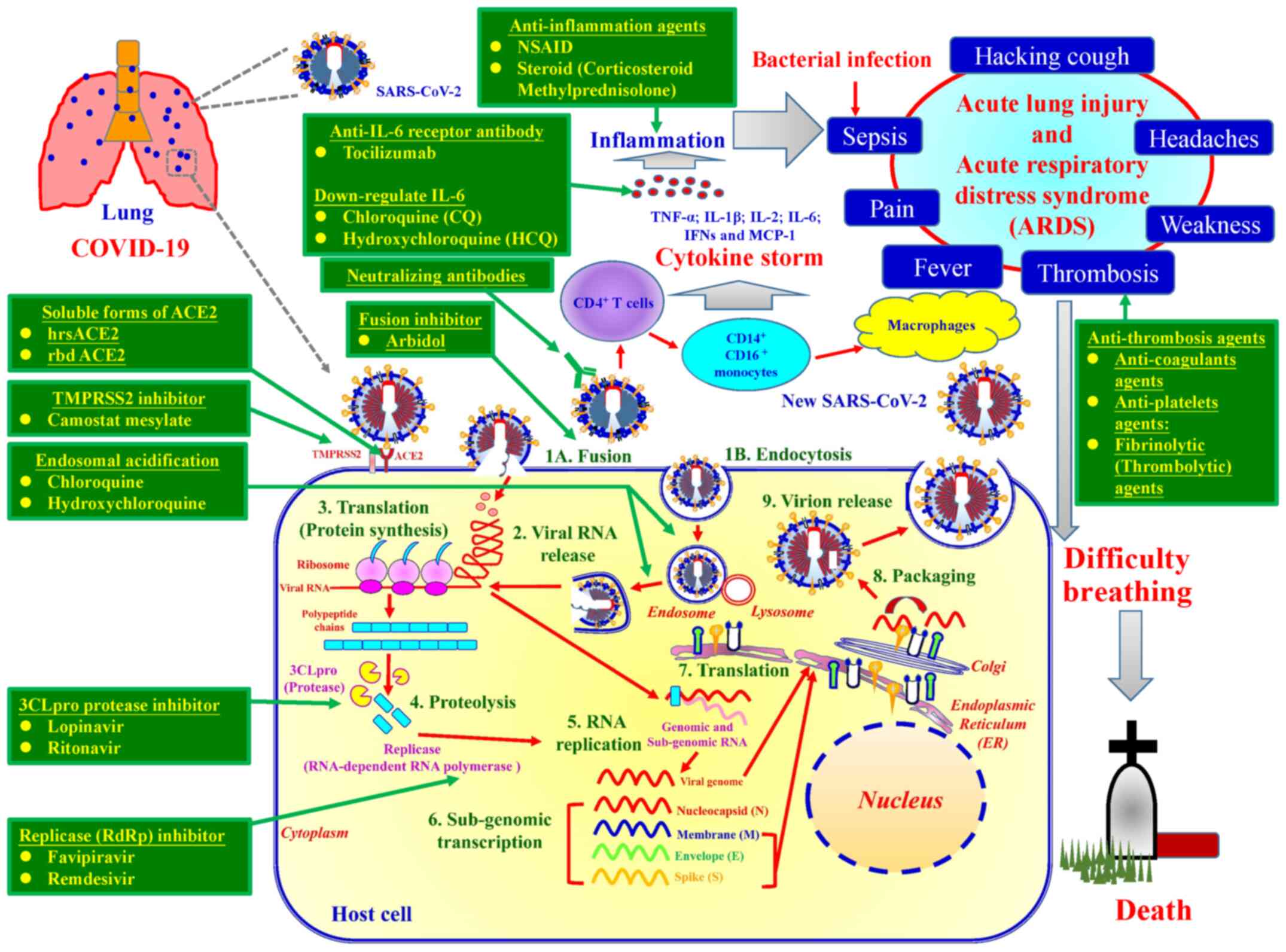
(Foipan®) are presented in Fig. 6. Table III and Fig. 7 summarise ongoing therapeutic
agents being evaluated for management of COVID-19 and their
molecular pharmacologic mechanisms. The mechanisms by which
suitable therapeutic agents against SARS-CoV2 exhibit their effects
are discussed below.
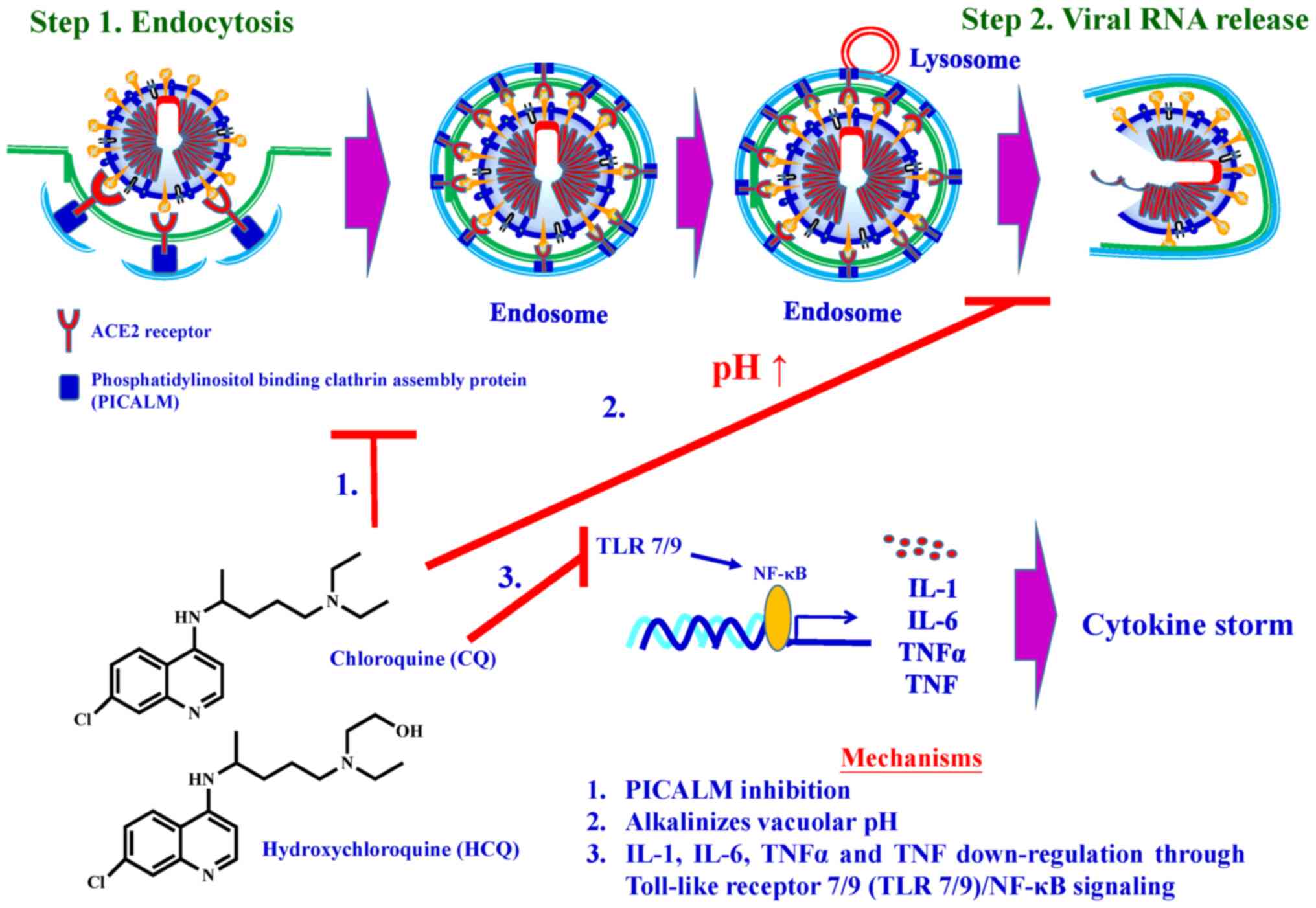
Reports have shown that chloroquine and
hydroxychlo-roquine increase endosomal and lysosomal pH
(alkalinises vacuolar pH) and then disrupt intracellular
trafficking (90-94). Recent studies have demonstrated
that chloroquine reduces the expression of phosphatidylinositol
binding clathrin assembly protein (PICALM), a cargo-selecting
clathrin adaptor that senses and drives membrane curvature, which
regulates endocytosis (95).
In vitro studies have demonstrated that chloroquine
significantly inhibits SARS-CoV-2 from infecting Vero E6 cells. One
of the mechanisms for the chloroquine-mediated effects against
SARS-CoV-2 is the decrease in the ability of cells to perform
clathrin-mediated endocytosis of nanosized structures due to PICALM
suppression (95).
Clinical investigations have shown that patients
with COVID-19 had high concentrations of cytokines, such as IL-1β,
IL-1β, IL-2, IL-6, IFNs and MCP-1 (96-98), in their plasma, subsequently
causing a cytokine storm. In addition, hydroxychloroquine has been
demonstrated to exhibit anti-inflammatory activity and can
significantly decrease the IL-1, IL-6, TNF-α and TNF production
through Toll-like receptor/NF-κB signalling (99,100).
The molecular pharmacological mechanisms of
chloro-quine and hydroxychloroquine are summarised in Fig. 9. A total of 52 clinical trials on
chloroquine and 150 clinical trials on hydroxychloroquine for the
treatment of COVID-19 are ongoing (64). Given that chloroquine and
hydroxychloroquine are longstanding therapeutic agents widely used
for disease treatment in hospitals, several ongoing clinical trials
on COVID-19 have focused on both. However, it has more recently
been reported that hydroxychloroquine does exhibit beneficial
effects in the management of infection with COVID-19, and may in
fact result in increased deaths due to its side-effects, resulting
in the early halting an Oxford-based study (101).
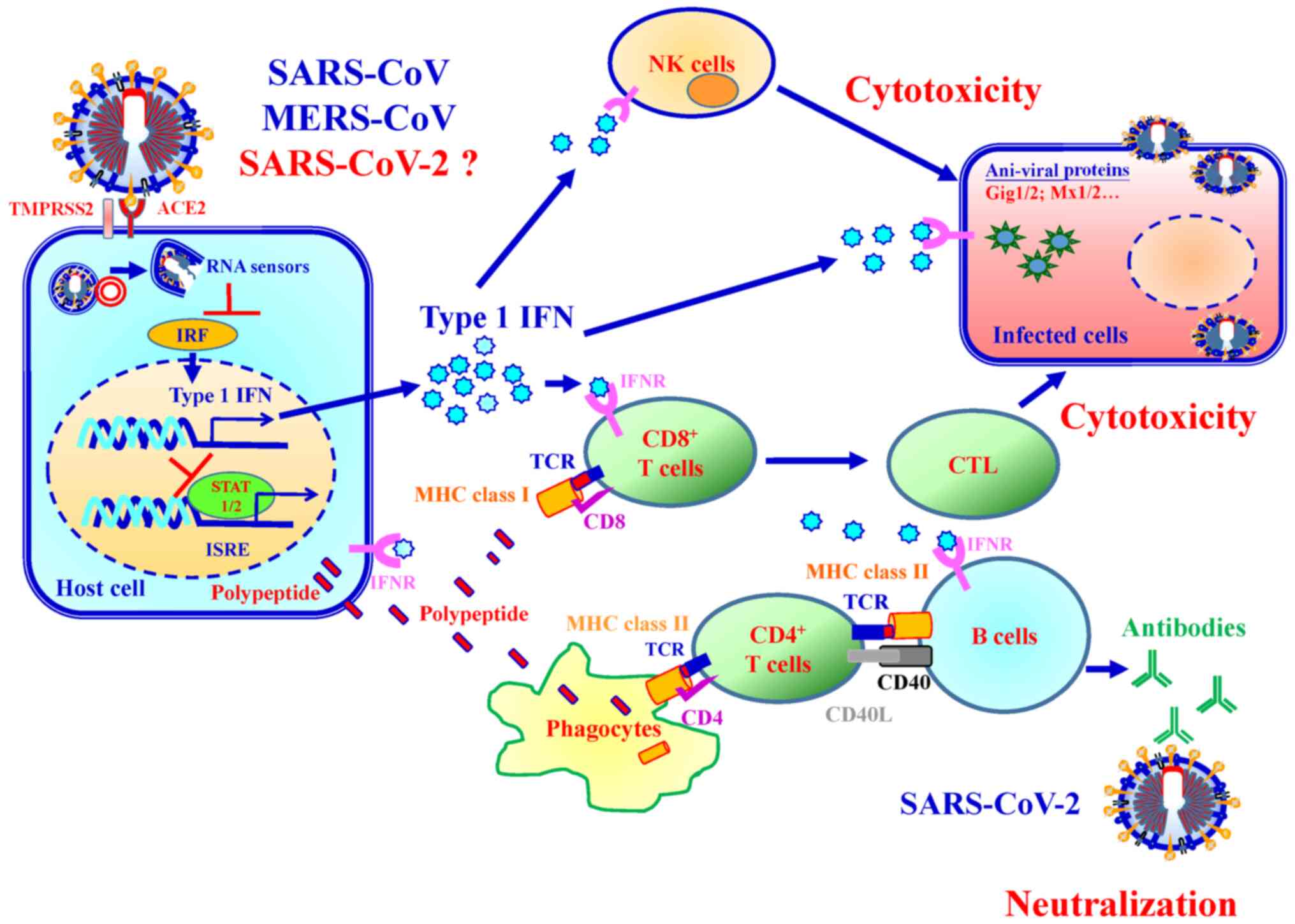
Cells infected with SARS-CoV and MERS-CoV exhibit
reduced type I IFN. As such, it is hypothesized that SARS-CoV-2 may
utilise a similar manner for type I IFN reduction. It has
previously been shown that type I IFN treatments improve
anti-SARS-CoV and anti-MERS-CoV activity amongst infected mice and
exhibits synergistic effects with ribavirin against SARS-CoV in
vitro (132).
Immunocompromised patients are at higher risk for severe COVID-19
than the general public. Type I IFN treatments can thus be a safe
and efficient approach to manage SARS-CoV-2 infection (121,133). A total of 37 clinical trials on
IFN for COVID-19 are ongoing worldwide (64). Fig.
12 presents a schematic overview of the type I IFN-mediated
immune response mechanism following SARS-CoV, MERS-CoV and
SARS-CoV-2 infection.
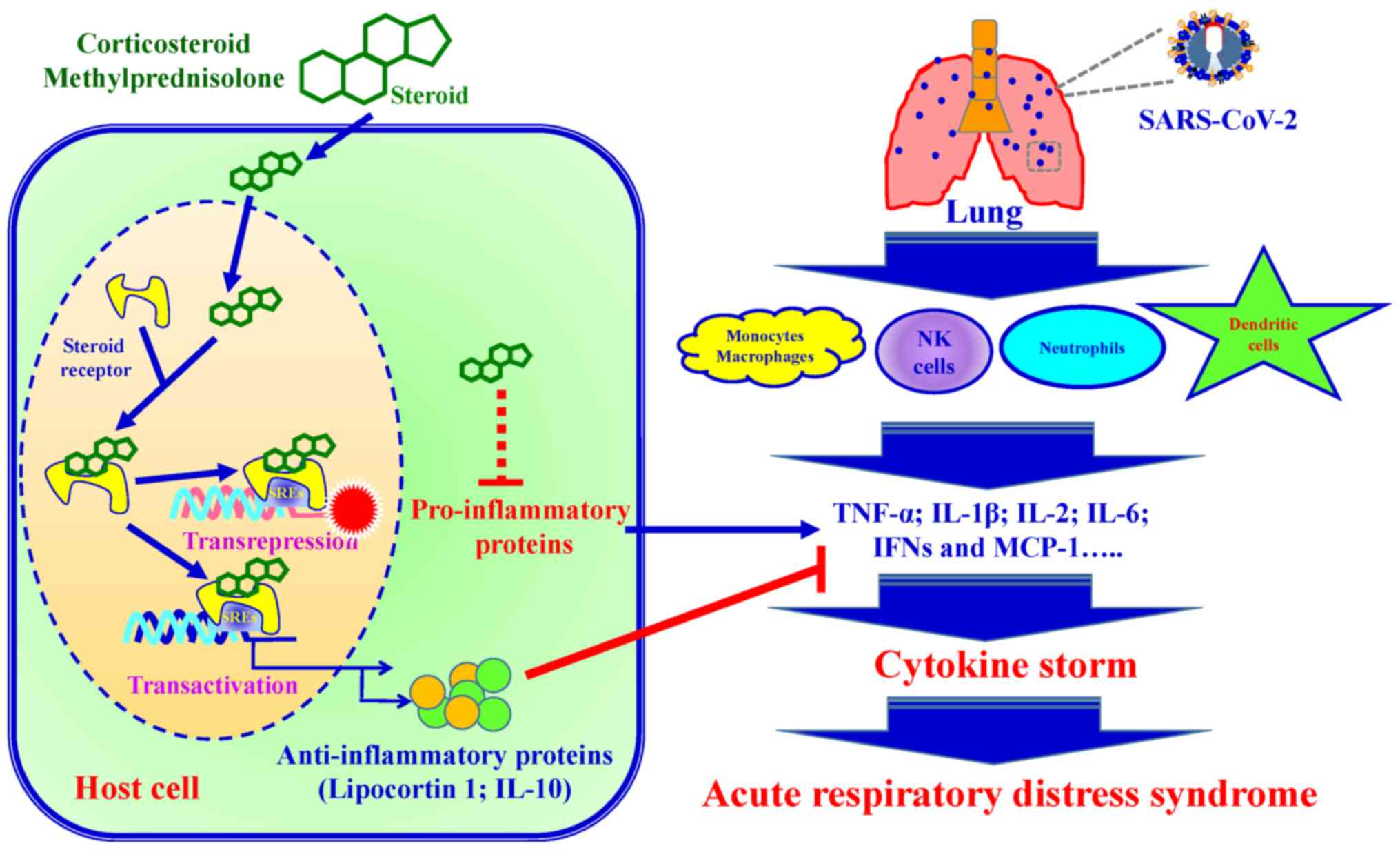
Combining anti-viral and anti-inflammatory agents
is another attractive therapeutic option for the prevention and
treatment of COVID-19. Upon infection, innate
immune cells including macrophages, natural killer cells,
neutrophils and dendritic cells produce large amounts of
pro-inflammatory cytokines (TNF, Type 1 IFN, IL-6 and IL-12).
Previous clinical studies have demonstrated that steroids
(corticosteroid and methylprednisolone) modulate inflammatory
responses, reducing the incidence of treatment failure and reducing
cytokine storms (123,134). The anti-inflammatory mechanisms
of steroids is involved in the presence of steroid receptors and
regulates down-stream gene transcription processes (135). Steroid receptor signaling
mechanisms regulate down-stream gene expression via transactivation
and trans-repression. i) In the process of transactivation, steroid
receptors bind steroid hormones and form dimers. The ligand bound
steroid receptor dimer complex binds to specific DNA sequences
(steroid response elements; SREs), increasing anti-inflammatory
gene transcription (such as Lipocortin 1 and IL-10). ii) In the
process of trans-repression, the ligand bound steroid receptor
tethers to SREs and inters pro-inflammatory transcription factors,
which leads to a reduction of pro-inflammatory cytokines (136). SARS-CoV-2 infection induces
pro-inflammatory cytokine production, resulting in local tissue
inflammation and a systemic inflammatory response, termed a
cytokine storm (137). Cytokine
storm injures host cells and causes an increased risk of
respiratory failure such as acute respiratory distress syndrome
(ARDS) and eventually death. Fig.
13 presents a schematic diagram of the steroid-mediated immune
response following SARS-CoV-2 infection.
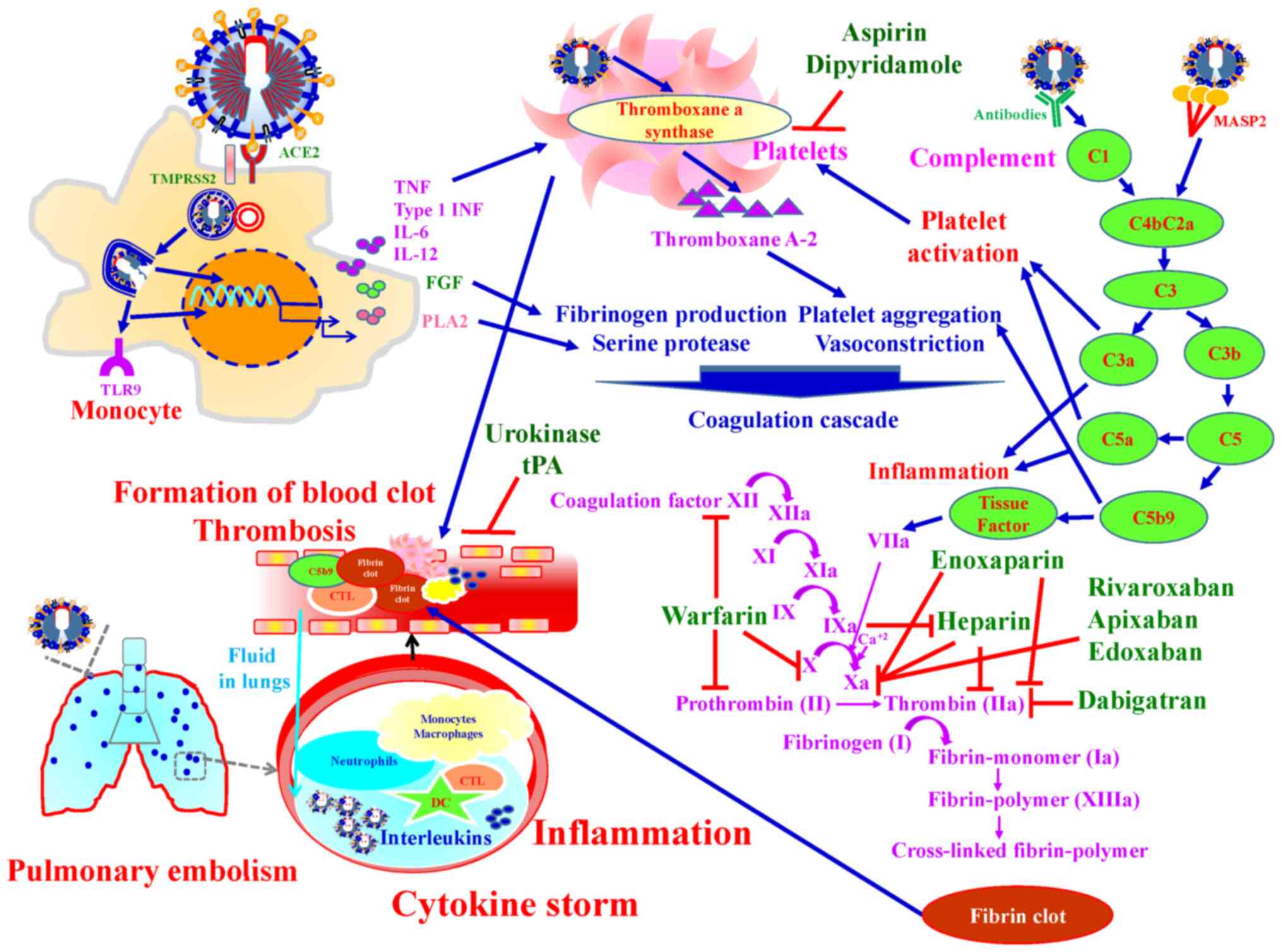
It was reported that SARS-CoV-2 infection increased
the risk of thrombosis and up to 50% of severe COVID-19 patients
developed coagulopathy (138).
Coagulation and thrombosis are associated with pathogenesis of
COVID-19 (139). SARS-CoV-2
results in direct injuries to the vascular endothelium cells or
induces a cytokine storm, leading to systemic thrombus formation,
thrombosis on pulmonary artery, and potentially lower limb arterial
and cerebral infarction (138).
Upon SARS-CoV-2 infection, the complement system, a bridge between
innate and adaptive immune response, is activated and triggers
inflammation. In addition, the complement system links the immune
system with the coagulation system. C5a in the complement system
induces tissue factor expression, and C5b-9 activates platelet
(140) Tissue factor/factor VIIa
complex converts prothrombin into thrombin. Thrombin catalyzes
fibrinogen to fibrin and promotes fibrin formation by coagulation
cascade activation and by activating platelets (140-144).
Pharmacological agents targeting thrombosis in
COVID-19 are divided into three groups: i) Anti-coagulant agents;
Unfractionated heparin, low-molecular-weight heparins (Enoxaparin),
Danaparoid (a mixture of heparan sulfate, dermatan sulfate, and
chondroitin sulfate) and Vitamin-K antagonists (warfarin). Heparin
and Enoxaparin have strong anti-thrombotic activity, and
anti-inflammatory properties via selectin blockade, bradykinin
downregulation and thrombin generation. In addition, Heparins
attenuate interactions between SARS-CoV-2 spike protein and ACE-2
(145). Enoxaparin is a first
choice drug to prevent thromboembolic phenomena in COVID-19
patients (138). ii)
Anti-platelets agents; Aspirin and Dipyridamole. Aspirin has been
demonstrated with ARDS prevention and higher survival rates from
acute lung injury in clinical studies (146,147). Dipyridamole is a
phosphodiesterase inhibitor that inhibits platelet aggregation by
increasing cyclic adenosine monophosphate concentrations. In
vitro studies demonstrated that dipyridamole has
anti-SARS-CoV-2 activity through binding with 3CLpro of SARS-CoV-2
(148). iii) Fibrinolytic
(thrombolytic) agents; Urokinase, Streptokinase and Tissue-type
plasminogen activator (tPA). The blood clots are broken down by
plasmin call fibrinolysis. Fibrinolysis intermediate tPA and
urokinase plasminogen activator convert plasminogen to plasmin.
When tPA, a thrombolytic agent, is intravenously injected into the
vasculature, increased fibrinolytic ability in the plasma and lyses
of the thrombosis was observed in COVID-19 patients (149). Fig. 14 presents an over-view of the
mechanisms by which anti-thrombotic agents exert their effects in
the treatment of SARS-CoV-2 infection.
Two promising countermeasures for controlling the
current COVID-19 pandemic are recombinant neutralizing anti-bodies
(150) and vaccines (151) directed against SARS-CoV-2.
Recombinant human or humanized monoclonal antibodies are proving to
be safe, effective, and highly specific in their ability to target
an invading pathogen. More than 70 recombinant monoclonal
antibodies have now been approved by the FDA for use in the
treatment of infectious, autoimmune and inflammatory, malignant, or
cardiovascular diseases (152).
Thus, recombinant neutralizing antibodies isolated from those
infected with SARS-CoV-2 are the most rapid and readily
manufacturable immune intervention for passive administration that
may be developed to either prevent or treat COVID-19 disease. Of
note, US President Donald Trump, who recently suffered from
infection with COVID-19 was treated with monoclonal antibodies
generated by Regeneron.
Vaccines are a time-honored method for establishing
long-lived immune memory for controlling infectious diseases, and
technologies have been developed such that vaccines can now be
developed faster than previously (151). Over 100 companies or academic
institutions are working on COVID-19 vaccines with strategies that
include recombinant vectors, mRNA in lipid nanoparticles, DNA,
inactivated virus, live attenuated virus, virus-like particles and
protein subunits (153). Three
vaccine candidates have already advanced to Phase II testing that
include an mRNA vaccine encoding the viral spike protein from
Moderna, an Adenotype 5 vector vaccine expressing the S protein
from CanSino Biologicals, and a chimpanzee adenovirus encoding the
spike protein from the Jenner Institute in Oxford, UK. There are
several mRNA/LNP (for example, from Moderna/NIAID, BioNTech/Fosum,
Pharma/Pfizer) or DNA (Inovio) vaccines as well as attenuated
viruses, proteins, nanoparticles and viral vectors containing
SARS-CoV-2 viral genes as vaccine candidates moving through safety
and immunogenicity trials, and a smaller subset of vaccine
candidates will be tested in Phase III or efficacy trials to better
determine if they are safe, as well to determine their efficacy. In
parallel now with Phase I and II trials, it is important to develop
capacity for large-scale vaccine production, in the event of a
successful efficacy trial (154). It is possible that genetic
immunization strategies such as DNA or mRNA in LNPs can be
manufactured more rapidly than proteins or viral vectors and can be
more cost effective.
Based on >3,500 years of Chinese medical
practice, TCM has spread to numerous countries worldwide, has
profoundly influenced lives and has gradually merged with and
complemented modern Western medicine and therapy (155). In recent decades, mounting
evidence has suggested that TCM may be helpful in the prevention
and treatment of human virus-related disorders, including
influenza, liver diseases and acquired immune deficiency syndrome
(114,156-158). Following the COVID-19 outbreak,
TCM schemes have been included into the guidelines for the
diagnosis and therapy of COVID-19 in China (114,159,160). Recently, in silico data
showed that binding of curcuminoid derivatives to COVID-19 3CLpro
is stronger than that of Lopinavir and curcumin (126). It is hypothesized that more
convenient methods for the early detection of COVID-19 via
genotyping will emerge in the near future. Even amongst
severe/critical cases, TCMs can still serve as a complementary and
integrative therapy to modern Western medicine to shorten the
recovery period and relieve symptoms among patients with
COVID-19.
This review describes several clinical
manifestations of COVID-19, analyses the SARS-CoV-2 genome and
outlines the life cycle of SARS-CoV-2. Several methods have been
used to examine SARS-CoV-2 infections. For example, RT-qPCR has
been widely applied for RNA detection, whereas rapid screening has
been used for antibody or virus detection. Despite the lack of
medications for COVID-19, several clinical trials have been
proposed for its treatment. In addition, several TCMs have been
discussed for the readers' reference.
Global interaction and cooperation amongst several
countries is expected to underlie the development of rapid and
accurate screening assays, produce vaccines, design novel agents
against SARS-CoV-2 and reduce the side effects of therapeutic TCMs,
with the ultimate, long-term goal of eradication of COVID-19.
This work was supported by the China Medical
University Hospital (grant nos. DMR-109-147, CMU-103-S-16 and MOST
106-2314-B-039-046), and also by the Chinese Medicine Research
Center, China Medical University from The Featured Areas Research
Center Program within the framework of the Higher Education Sprout
Project by the Ministry of Education in Taiwan.
Not applicable.
SCT, FJT and JSY were involved in the conception of
the study. CCL, DTB, YJC, YTY, YMH, CWF, SCK, YSL, HYC and YNJ were
involved in the literature search and critical reviewing of the
manuscript. SCT, CCL, DTB, YJC, YTY, YMH, SCK and JSY were involved
in the preparation of the draft of the manuscript. SCT, FJT and JSY
were involved in the revising and editing of the manuscript. All
authors have read and approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
We thank Kuan-Wen Chen and Tzu-Mao Hung in GGA
Corporation, Molecular Science Center (Taiwan) for performing the
molecular docking to RdRp and 3CLpro. We wish to acknowledge the
work of Nian-Gu Chen, Pei-Jen Chung, Chien-Jung Huang, Yi-Chia Li
and Chia-Wen Tsai for their assistance on this work. We also would
also like thank Merck Ltd. Taiwan company for providing Synthia
Organic Retrosynthesis Software.
|
1
|
World Health Organization (WHO):
Coronavirus disease (COVID-19) pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019urisimplehttps://www.who.int/emergencies/diseases/novel-coronavirus-2019.
Accessed November 2, 2020.
|
|
2
|
Liu YC, Kuo RL and Shih SR: COVID-19: The
first documented coronavirus pandemic in history. Biomed J.
43:328–333. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tsay SF, Kao CC, Wang HH and Lin CC:
Nursing's response to COVID-19: Lessons learned from SARS in
Taiwan. Int J Nurs Stud. 108:1035872020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chang CL and McAleer M: Alternative global
health security indexes for risk analysis of COVID-19. Int J
Environ Res Public Health. 17:31612020. View Article : Google Scholar :
|
|
5
|
Hsu YC, Liu YA, Lin MH, Lee HW, Chen TJ,
Chou LF and Hwang SJ: Visiting policies of hospice wards during the
COVID-19 pandemic: An environmental scan in Taiwan. Int J Environ
Res Public Health. 17:28572020. View Article : Google Scholar :
|
|
6
|
Schwartz J, King CC and Yen MY: Protecting
healthcare workers during the coronavirus disease 2019 (COVID-19)
outbreak: lessons from Taiwan's severe acute respiratory syndrome
response. Clin Infect Dis. 71:858–860. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wu YC, Chen CS and Chan YJ: The outbreak
of COVID-19: An overview. J Chin Med Assoc. 83:217–220. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
U.S. Food & Drug Administration (FDA):
Coronavirus Disease 2019 (COVID-19). https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-broadens-emergency-use-authorization-veklury-remdesivir-include-all-hospitalizedurisimplehttps://www.fda.gov/news-events/press-announcements/covid-19-update-fda-broadens-emergency-use-authorization-veklury-remdesivir-include-all-hospitalized.
Accessed August 28, 2020.
|
|
9
|
Park SE: Epidemiology, virology, and
clinical features of severe acute respiratory syndrome
-coronavirus-2 (SARS-CoV-2; Coronavirus Disease-19). Clin Exp
Pediatr. 63:119–124. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong
Y, Ren R, Leung KSM, Lau EHY, Wong JY, et al: Early transmission
dynamics in Wuhan, China, of novel coronavirus-infected pneumonia.
N Engl J Med. 382:1199–1207. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Day M: Covid-19: Identifying and isolating
asymptomatic people helped eliminate virus in Italian village. BMJ.
3:m11652020. View Article : Google Scholar
|
|
12
|
Chang TH, Wu JL and Chang LY: Clinical
characteristics and diagnostic challenges of pediatric COVID-19: A
systematic review and meta-analysis. J Formos Med Assoc.
119:982–989. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z,
Xiang J, Wang Y, Song B, Gu X, et al: Clinical course and risk
factors for mortality of adult inpatients with COVID-19 in Wuhan,
China: A retrospective cohort study. Lancet. 395:1054–1062. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lin CT, Bookman K, Sieja A, Markley K,
Altman RL, Sippel J, Perica K, Reece L, Davis C, Horowitz E, et al:
Clinical informatics accelerates health system adaptation to the
COVID-19 pandemic: Examples from Colorado. J Am Med Inform Assoc.
Jul 20–2020.Epub ahead of print. View Article : Google Scholar
|
|
15
|
Liu X, Zhang R and He G: Hematological
findings in corona-virus disease 2019: Indications of progression
of disease. Ann Hematol. 99:1421–1428. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ippolito D, Maino C, Pecorelli A,
Allegranza P, Cangiotti C, Capodaglio C, Mariani I, Giandola T,
Gandola D, Bianco I, et al: Chest X-ray features of SARS-CoV-2 in
the emergency department: A multicenter experience from northern
Italian hospitals. Respir Med. 170:1060362020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J,
Wang B, Xiang H, Cheng Z, Xiong Y, et al: Clinical characteristics
of 138 hospitalized patients with 2019 novel coronavirus-infected
pneumonia in Wuhan, China. JAMA. 323:1061–1069. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tu YF, Chien CS, Yarmishyn AA, Lin YY, Luo
YH, Lin YT, Lai WY, Yang DM, Chou SJ, Yang YP, et al: A review of
SARS-CoV-2 and the Ongoing Clinical Trials. Int J Mol Sci.
21:26572020. View Article : Google Scholar :
|
|
19
|
Davis B, Rothrock AN, Swetland S, Andris
H, Davis P and Rothrock SG: Viral and atypical respiratory
co-infections in COVID-19: A systematic review and meta-analysis. J
Am Coll Emerg Physicians Open. 1:533–548. 2020. View Article : Google Scholar
|
|
20
|
Oliva A, Siccardi G, Migliarini A,
Cancelli F, Carnevalini M, D'Andria M, Attilia I, Danese VC,
Cecchetti V, Romiti R, et al: Co-infection of SARS-CoV-2 with
Chlamydia or Mycoplasma pneumoniae: A case series and review of the
literature. Infection. Jul 28–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Assiri A, Al-Tawfiq JA, Al-Rabeeah AA,
Al-Rabiah FA, Al-Hajjar S, Al-Barrak A, Flemban H, Al-Nassir WN,
Balkhy HH, Al-Hakeem RF, et al: Epidemiological, demographic, and
clinical characteristics of 47 cases of Middle East respiratory
syndrome coronavirus disease from Saudi Arabia: A descriptive
study. Lancet Infect Dis. 13:752–761. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Phan LT, Nguyen TV, Luong QC, Nguyen TV,
Nguyen HT, Le HQ, Nguyen TT, Cao TM and Pham QD: Importation and
human-to-human transmission of a novel coronavirus in Vietnam. N
Engl J Med. 382:872–874. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rothan HA and Byrareddy SN: The
epidemiology and pathogenesis of coronavirus disease (COVID-19)
outbreak. J Autoimmun. 109:1024332020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tan L, Wang Q, Zhang D, Ding J, Huang Q,
Tang YQ, Wang Q and Miao H: Lymphopenia predicts disease severity
of COVID-19: A descriptive and predictive study. Signal Transduct
Target Ther. 5:332020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Su YJ and Lai YC: Comparison of clinical
characteristics of coronavirus disease (COVID-19) and severe acute
respiratory syndrome (SARS) as experienced in Taiwan. Travel Med
Infect Dis. 36:1016252020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sung YY, Wu YC, Li CY, Hsu CY, Hsu CY,
Liang ST, Huang WC, Pan KY, Tsai JH and Yen YH: Interim Guidelines
for Clinical Management of SARS-CoV-2 Infection (5th edition)
Ministry of Health and Welfare. Taiwan: Centers for Disease
Control; 2020, https://www.cdc.gov.tw/File/Get/-ewtg9-RCAetCPKR4_rnCwurisimplehttps://www.cdc.gov.tw/File/Get/-ewtg9-RCAetCPKR4_rnCw.
Accessed March 26, 2020.
|
|
27
|
Wu A, Peng Y, Huang B, Ding X, Wang X, Niu
P, Meng J, Zhu Z, Zhang Z, Wang J, et al: Genome composition and
divergence of the novel coronavirus (2019-nCoV) originating in
China. Cell Host Microbe. 27:325–328. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Singhal T: A Review of coronavirus
disease-2019 (COVID-19). Indian J Pediatr. 87:281–286. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li G and De Clercq E: Therapeutic options
for the 2019 novel coronavirus (2019-nCoV). Nat Rev Drug Discov.
19:149–150. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
National Institutes of Health (NIH),
National Center for Biotechnology Information (NCBI): NCBI
SARS-CoV-2 Resources. https://www.ncbi.nlm.nih.gov/Structure/SARS-CoV-2.htmlurisimplehttps://www.ncbi.nlm.nih.gov/Structure/SARS-CoV-2.html.
Accessed October 27, 2020.
|
|
31
|
Hoffmann M, Kleine-Weber H and Pöhlmann S:
A multibasic cleavage site in the spike protein of SARS-CoV-2 is
essential for infection of human lung cells. Mol Cell.
78:779–784.e5. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Schoeman D and Fielding BC: Is there a
link between the pathogenic human coronavirus envelope protein and
immunopathology? A review of the literature. Front Microbiol.
11:20862020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Malik YA: Properties of coronavirus and
SARS-CoV-2. Malays J Pathol. 42:3–11. 2020.PubMed/NCBI
|
|
34
|
Mu J, Xu J, Zhang L, Shu T, Wu D, Huang M,
Ren Y, Li X, Geng Q, Xu Y, et al: SARS-CoV-2-encoded nucleocapsid
protein acts as a viral suppressor of RNA interference in cells.
Sci China Life Sci. 63:1–4. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Baez-Santos YM, Mielech AM, Deng X, Baker
S and Mesecar AD: Catalytic function and substrate specificity of
the papain-like protease domain of nsp3 from the Middle East
respiratory syndrome coronavirus. J Virol. 88:12511–12527. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sakai Y, Kawachi K, Terada Y, Omori H,
Matsuura Y and Kamitani W: Two-amino acids change in the nsp4 of
SARS coronavirus abolishes viral replication. Virology.
510:165–174. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Angelini MM, Akhlaghpour M, Neuman BW and
Buchmeier MJ: Severe acute respiratory syndrome coronavirus
nonstructural proteins 3, 4, and 6 induce double-membrane vesicles.
mBio. 4:e00524–13. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Snijder EJ, Decroly E and Ziebuhr J: The
nonstructural proteins directing coronavirus RNA synthesis and
processing. Adv Virus Res. 96:59–126. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Rathnasinghe R, Karlicek RF, Schotsaert M,
Koffas MA, Arduini B, Jangra S, Wang B, Davis JL, Alnaggar M, Costa
A, et al: Scalable, effective, and rapid decontamination of
SARS-CoV-2 contaminated N95 respirators using germicidal
ultra-violet C (UVC) irradiation device. medRxiv. View Article : Google Scholar
|
|
40
|
Boopathi S, Poma AB and Kolandaivel P:
Novel 2019 corona-virus structure, mechanism of action, antiviral
drug promises and rule out against its treatment. J Biomol Struct
Dyn. Apr 30–2020.Epub ahead of print. View Article : Google Scholar
|
|
41
|
Verdecchia P, Cavallini C, Spanevello A
and Angeli F: The pivotal link between ACE2 deficiency and
SARS-CoV-2 infection. Eur J Intern Med. 76:14–20. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chen WH, Strych U, Hotez PJ and Bottazzi
ME: The SARS-CoV-2 vaccine pipeline: An overview. Curr Trop Med
Rep. Mar 3–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Chan VS, Chan KY, Chen Y, Poon LL, Cheung
AN, Zheng B, Chan KH, Mak W, Ngan HY, Xu X, et al: Homozygous
L-SIGN (CLEC4M) plays a protective role in SARS coronavirus
infection. Nat Genet. 38:38–46. 2006. View
Article : Google Scholar
|
|
44
|
Jeffers SA, Tusell SM, Gillim-Ross L,
Hemmila EM, Achenbach JE, Babcock GJ, Thomas WD Jr, Thackray LB,
Young MD, Mason RJ, et al: CD209L (L-SIGN) is a receptor for severe
acute respiratory syndrome coronavirus. Proc Natl Acad Sci USA.
101:15748–15753. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
McKee DL, Sternberg A, Stange U, Laufer S
and Naujokat C: Candidate drugs against SARS-CoV-2 and COVID-19.
Pharmacol Res. 157:1048592020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Stahlmann R and Lode H: Medication for
COVID-19-an over-view of approaches currently under study. Dtsch
Arztebl Int. 117:213–219. 2020.PubMed/NCBI
|
|
47
|
Kupferschmidt K and Cohen J: Race to find
COVID-19 treatments accelerates. Science. 367:1412–1413. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Yip CC, Ho CC, Chan JF, To KK, Chan HS,
Wong SC, Leung KH, Fung AY, Ng AC, Zou Z, et al: Development of a
novel, genome subtraction-derived, SARS-CoV-2-specific
COVID-19-nsp2 real-time RT-PCR assay and its evaluation using
clinical specimens. Int J Mol Sci. 21:25742020. View Article : Google Scholar :
|
|
49
|
Yan C, Cui J, Huang L, Du B, Chen L, Xue
G, Li S, Zhang W, Zhao L, Sun Y, et al: Rapid and visual detection
of 2019 novel coronavirus (SARS-CoV-2) by a reverse transcription
loop-mediated isothermal amplification assay. Clin Microbiol
Infect. 26:773–779. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rahman H, Carter I, Basile K, Donovan L,
Kumar S, Tran T, Ko D, Alderson S, Sivaruban T, Eden JS, et al:
Interpret with caution: An evaluation of the commercial
AusDiagnostics versus in-house developed assays for the detection
of SARS-CoV-2 virus. J Clin Virol. 127:1043742020. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Pujadas E, Ibeh N, Hernandez MM, Waluszko
A, Sidorenko T, Flores V, Shiffrin B, Chiu N, Young-Francois A,
Nowak MD, et al: Comparison of SARS-CoV-2 detection from
nasopharyngeal swab samples by the Roche cobas(R) 6800 SARS-CoV-2
test and a laboratory-developed real-time RT-PCR test. J Med Virol.
May 8–2020.Epub ahead of print. View Article : Google Scholar
|
|
52
|
Montesinos I, Gruson D, Kabamba B, Dahma
H, Van den Wijngaert S, Reza S, Carbone V, Vandenberg O, Gulbis B,
Wolff F and Rodriguez-Villalobos H: Evaluation of two automated and
three rapid lateral flow immunoassays for the detection of
anti-SARS-CoV-2 antibodies. J Clin Virol. 128:1044132020.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Thabet L, Mhalla S, Naija H, Jaoua MA,
Hannachi N, Fki-Berrajah L, Toumi A and Karray-Hakim H: SARS-CoV-2
infection virological diagnosis. Tunis Med. 98:304–308.
2020.PubMed/NCBI
|
|
54
|
Vásárhelyi B, Kristóf K, Ostorházi E,
Szabó D, Prohászka Z and Merkely B: The diagnostic value of rapid
anti IgM and IgG detecting tests in the identification of patients
with SARS CoV-2 virus infection. Orv Hetil. 161:807–812. 2020.In
Hungarian. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Green K, Graziadio S, Turner P, Fanshawe T
and Allen J: Molecular and antibody point-of-care tests to support
the screening, diagnosis and monitoring of COVID-19. Centre for
Evidence- Based Medicine (CEBM); Oxford; 2020, https://www.cebm.net/covid-19/molecular-and-antibody-point-of-care-tests-to-support-the-screening-diagnosis-and-monitoring-of-covid-19/urisimplehttps://www.cebm.net/covid-19/molecular-and-antibody-point-of-care-tests-to-support-the-screening-diagnosis-and-monitoring-of-covid-19/.
Accessed April 7, 2020.
|
|
56
|
Xue X, Zhu C, Huang S, Pan L, Xu J and Li
W: Effect of heat inactivation of blood samples on the efficacy of
three detection methods of SARS-CoV-2 antibodies. Nan Fang Yi Ke Da
Xue Xue Bao. 40:316–320. 2020.In Chinese. PubMed/NCBI
|
|
57
|
Huang P, Liu T, Huang L, Liu H, Lei M, Xu
W, Hu X, Chen J and Liu B: Use of chest CT in combination with
negative RT-PCR assay for the 2019 novel coronavirus but high
clinical suspicion. Radiology. 295:22–23. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Wang P: Combination of serological total
antibody and RT-PCR test for detection of SARS-COV-2 infections. J
Virol Methods. 283:1139192020. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Lange C, Wolf J, Auw-Haedrich C, Schlecht
A, Boneva S, Lapp T, Horres R, Agostini H, Martin G, Reinhard T and
Schlunck G: Expression of the COVID-19 receptor ACE2 in the human
conjunctiva. J Med Virol. May 6–2020.Epub ahead of print.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Zhou J, Li C, Liu X, Chiu MC, Zhao X, Wang
D, Wei Y, Lee A, Zhang AJ, Chu H, et al: Infection of bat and human
intestinal organoids by SARS-CoV-2. Nat Med. 26:1077–1083. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Ziegler CGK, Allon SJ, Nyquist SK, Mbano
IM, Miao VN, Tzouanas CN, Cao Y, Yousif AS, Bals J, Hauser BM, et
al: SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in
human airway epithelial cells and is detected in specific cell
subsets across tissues. Cell. 181:1016–1035.e19. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Rahman N, Basharat Z, Yousuf M, Castaldo
G, Rastrelli L and Khan H: Virtual screening of natural products
against type II transmembrane serine protease (TMPRSS2), the
priming agent of coronavirus 2 (SARS-CoV-2). Molecules.
25:22712020. View Article : Google Scholar :
|
|
63
|
Huang J, Song W, Huang H and Sun Q:
Pharmacological therapeutics targeting RNA-dependent RNA
polymerase, proteinase and spike protein: From mechanistic studies
to clinical trials for COVID-19. J Clin Med. 9:11312020. View Article : Google Scholar :
|
|
64
|
ClinicalTrials.gov: NUnlom: COVID-19.
https://clinicaltrials.gov/ct2/results?cond=covid-19urisimplehttps://clinicaltrials.gov/ct2/results?cond=covid-19.
Accessed August 17, 2020.
|
|
65
|
Amawi H, Abu Deiab GI, A Aljabali AA, Dua
K and Tambuwala MM: COVID-19 pandemic: An overview of epidemiology,
pathogenesis, diagnostics and potential vaccines and therapeutics.
Ther Deliv. 11:245–268. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Vankadari N: Arbidol: A potential
antiviral drug for the treatment of SARS-CoV-2 by blocking
trimerization of the spike glycoprotein. Int J Antimicrob Agents.
56:1059982020. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zhu Z, Lu Z, Xu T, Chen C, Yang G, Zha T,
Lu J and Xue Y: Arbidol monotherapy is superior to
lopinavir/ritonavir in treating COVID-19. J Infect. 81:e21–e23.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Deng L, Li C, Zeng Q, Liu X, Li X, Zhang
H, Hong Z and Xia J: Arbidol combined with LPV/r versus LPV/r alone
against Corona Virus Disease 2019: A retrospective cohort study. J
Infect. 81:e1–e5. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Wang X, Cao R, Zhang H, Liu J, Xu M, Hu H,
Li Y, Zhao L, Li W, Sun X, et al: The anti-influenza virus drug,
arbidol is an efficient inhibitor of SARS-CoV-2 in vitro. Cell
Discov. 6:282020. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Dong L, Hu S and Gao J: Discovering drugs
to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther.
14:58–60. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Hulseberg CE, Fénéant L, Szymańska-de Wijs
KM, Kessler NP, Nelson EA, Shoemaker CJ, Schmaljohn CS, Polyak SJ
and White JM: Arbidol and other low-molecular-weight drugs that
inhibit lassa and Ebola viruses. J Virol. 93:e02185–18. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Kadam RU and Wilson IA: Structural basis
of influenza virus fusion inhibition by the antiviral drug Arbidol.
Proc Natl Acad Sci USA. 114:206–214. 2017. View Article : Google Scholar
|
|
73
|
Zeng LY, Yang J and Liu S: Investigational
hemagglutinin-targeted influenza virus inhibitors. Expert Opin
Investig Drugs. 26:63–73. 2017. View Article : Google Scholar
|
|
74
|
Roshanravan N, Ghaffari S and Hedayati M:
Angiotensin converting enzyme-2 as therapeutic target in COVID-19.
Diabetes Metab Syndr. 14:637–639. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Hamming I, Timens W, Bulthuis ML, Lely AT,
Navis G and van Goor H: Tissue distribution of ACE2 protein, the
functional receptor for SARS coronavirus. A first step in
understanding SARS pathogenesis. J Pathol. 203:631–637. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Xu J and Lazartigues E: Expression of ACE2
in human neurons supports the neuro-invasive potential of COVID-19
virus. Cell Mol Neurobiol. Jul 4–2020.Epub ahead of print.
View Article : Google Scholar :
|
|
77
|
Wedell J, Banzhaf G, Meier zu Eissen P and
Schlageter M: Experiences with a subcutaneous, fully resorbable
bridge in construction a double loop ileo- and colostomy. Chirurg.
61:36–38. 1990.In German. PubMed/NCBI
|
|
78
|
Li MY, Li L, Zhang Y and Wang XS:
Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide
variety of human tissues. Infect Dis Poverty. 9:452020. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Zhang X, Zheng J, Yan Y, Ruan Z, Su Y,
Wang J, Huang H, Zhang Y, Wang W, Gao J, et al:
Angiotensin-converting enzyme 2 regulates autophagy in acute lung
injury through AMPK/mTOR signaling. Arch Biochem Biophys.
672:1080612019. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
de Moraes PL, Kangussu LM, Castro CH,
Almeida AP, Santos RAS and Ferreira AJ: Vasodilator effect of
angiotensin-(17) on vascular coronary bed of rats: Role of Mas, ACE
and ACE2. Protein Pept Lett. 24:869–875. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Basu R, Poglitsch M, Yogasundaram H,
Thomas J, Rowe BH and Oudit GY: Roles of angiotensin peptides and
recombinant human ACE2 in heart failure. J Am Coll Cardiol.
69:805–819. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Qiao B and Olvera de la Cruz M: Enhanced
binding of SARS-CoV-2 spike protein to receptor by distal polybasic
cleavage sites. ACS Nano. 14:10616–10623. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Kruse RL: Therapeutic strategies in an
outbreak scenario to treat the novel coronavirus originating in
Wuhan, China. F1000Res. 9:722020. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Zhang H, Penninger JM, Li Y, Zhong N and
Slutsky AS: Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2
receptor: Molecular mechanisms and potential therapeutic target.
Intensive Care Med. 46:586–590. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Mejia Torres RE, Banegas EI, Mendoza M,
Diaz C, Bucheli ST, Fontecha GA, Alam MT, Goldman I, Udhayakumar V
and Zambrano JO: Efficacy of chloroquine for the treatment of
uncomplicated Plasmodium falciparum malaria in Honduras. Am J Trop
Med Hyg. 88:850–854. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Taherian E, Rao A, Malemud CJ and Askari
AD: The biological and clinical activity of anti-malarial drugs in
autoimmune disorders. Curr Rheumatol Rev. 9:45–62. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Pastick KA, Okafor EC, Wang F, Lofgren SM,
Skipper CP, Nicol MR, Pullen MF, Rajasingham R, McDonald EG, Lee
TC, et al: Review: Hydroxychloroquine and chloroquine for treatment
of SARS-CoV-2 (COVID-19). Open Forum Infect Dis. 7:ofaa1302020.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Piszczatoski CR and Powell J: Emergency
approval of chloroquine and hydroxychloroquine for treatment of
COVID-19. Ann Pharmacother. 54:827–831. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Shukla AM, Archibald LK, Shukla AW, Mehta
HJ and Cherabuddi K: Chloroquine and hydroxychloroquine in the
context of COVID-19. Drugs Context. 9(2020)–4. –5. 2020. View Article : Google Scholar
|
|
90
|
Sturrock BR and Chevassut TJ: Chloroquine
and COVID-19-a potential game changer? Clin Med (Lond). 20:278–281.
2020. View Article : Google Scholar
|
|
91
|
Colson P, Rolain JM, Lagier JC, Brouqui P
and Raoult D: Chloroquine and hydroxychloroquine as available
weapons to fight COVID-19. Int J Antimicrob Agents. 55:1059322020.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Annangi S: Chloroquine and
hydroxychloroquine for COVID-19: A word of caution. Respirology.
25:683–684. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Ferner RE and Aronson JK: Chloroquine and
hydroxychloroquine in covid-19. BMJ. 369:m14322020. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Badyal DK and Mahajan R: Chloroquine: Can
it be a novel drug for COVID-19. Int J Appl Basic Med Res.
10:128–130. 2020.PubMed/NCBI
|
|
95
|
Hu TY, Frieman M and Wolfram J: Insights
from nano-medicine into chloroquine efficacy against COVID-19. Nat
Nanotechnol. 15:247–249. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Ren Y, Yao MC, Huo XQ, Gu Y, Zhu WX, Qiao
YJ and Zhang YL: Study on treatment of 'cytokine storm' by
anti-2019-nCoV prescriptions based on arachidonic acid metabolic
pathway. Zhongguo Zhong Yao Za Zhi. 45:1225–1231. 2020.In Chinese.
PubMed/NCBI
|
|
97
|
McGonagle D, Sharif K, O'Regan A and
Bridgewood C: The role of cytokines including interleukin-6 in
COVID-19 induced pneumonia and macrophage activation syndrome-like
disease. Autoimmun Rev. 19:1025372020. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Lagunas-Rangel FA and Chávez-Valencia V:
High IL-6/IFN-γ ratio could be associated with severe disease in
COVID-19 patients. J Med Virol. Apr 16–2020.Epub ahead of print.
View Article : Google Scholar
|
|
99
|
Aizawa T, Imaizumi T, Hirono K, Watanabe
S, Tsugawa K and Tanaka H: Chloroquine attenuates TLR3-mediated
plasminogen activator inhibitor-1 expression in cultured human
glomerular endothelial cells. Clin Exp Nephrol. 23:448–454. 2019.
View Article : Google Scholar
|
|
100
|
Clancy RM, Markham AJ, Reed JH, Blumenberg
M, Halushka MK and Buyon JP: Targeting downstream transcription
factors and epigenetic modifications following Toll-like receptor
7/8 ligation to forestall tissue injury in anti-Ro60 associated
heart block. J Autoimmun. 67:36–45. 2016. View Article : Google Scholar :
|
|
101
|
Mahase E: Hydroxychloroquine for covid-19:
The end of the line? BMJ. 369:m23782020. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Wu R, Wang L, Kuo HD, Shannar A, Peter R,
Chou PJ, Li S, Hudlikar R, Liu X, Liu Z, et al: An update on
current therapeutic drugs treating COVID-19. Curr Pharmacol Rep.
May 11–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Ahsan W, Javed S, Bratty MA, Alhazmi HA
and Najmi A: Treatment of SARS-CoV-2: How far have we reached? Drug
Discov Ther. 14:67–72. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Du YX and Chen XP: Favipiravir:
Pharmacokinetics and concerns about clinical trials for 2019-nCoV
infection. Clin Pharmacol Ther. 108:242–247. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Reina J: Remdesivir, the antiviral hope
against SARS-CoV-2. Rev Esp Quimioter. 33:176–179. 2020.In Spanish.
View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Cao YC, Deng QX and Dai SX: Remdesivir for
severe acute respiratory syndrome coronavirus 2 causing COVID-19:
An evaluation of the evidence. Travel Med Infect Dis.
35:1016472020. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Augustin M, Hallek M and Nitschmann S:
Remdesivir for patients with severe COVID-19. Internist (Berl).
61:644–645. 2020.In German. View Article : Google Scholar
|
|
108
|
Li Z, Wang X, Cao D, Sun R, Li C and Li G:
Rapid review for the anti-coronavirus effect of remdesivir. Drug
Discov Ther. 14:73–76. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Jean SS, Lee PI and Hsueh PR: Treatment
options for COVID-19: The reality and challenges. J Microbiol
Immunol Infect. 53:436–443. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Lu CC, Chen MY, Lee WS and Chang YL:
Potential therapeutic agents against COVID-19: What we know so far.
J Chin Med Assoc. 83:534–536. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Simsek Yavuz S and Ünal S: Antiviral
treatment of COVID-19. Turk J Med Sci. 50:611–619. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Choy KT, Wong AY, Kaewpreedee P, Sia SF,
Chen D, Hui KPY, Chu DKW, Chan MCW, Cheung PP, Huang X, et al:
Remdesivir, lopinavir, emetine, and homoharringtonine inhibit
SARS-CoV-2 replication in vitro. Antiviral Res. 178:1047862020.
View Article : Google Scholar : PubMed/NCBI
|
|
113
|
U.S. Food & Drug Administration (FDA):
Coronavirus (COVID-19) Update: FDA issues emergency use
authorization for potential COVID-19 treatment. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatmenturisimplehttps://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatment.
Accessed May 1, 2020.
|
|
114
|
Chan KW, Wong VT and Tang SCW: COVID-19:
An update on the epidemiological, clinical, preventive and
therapeutic evidence and Guidelines of integrative Chinese-Western
medicine for the management of 2019 novel coronavirus disease. Am J
Chin Med. 48:737–762. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Martinez MA: Compounds with therapeutic
potential against novel respiratory 2019 coronavirus. Antimicrob
Agents Chemother. 64:e0039920–2020. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Guzik TJ, Mohiddin SA, Dimarco A, Patel V,
Savvatis K, Marelli-Berg FM, Madhur MS, Tomaszewski M, Maffia P,
D'Acquisto F, et al: COVID-19 and the cardiovascular system:
Implications for risk assessment, diagnosis, and treatment options.
Cardiovasc Res. 116:1666–1687. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Elfiky AA: Ribavirin, remdesivir,
sofosbuvir, galidesivir, and tenofovir against SARS-CoV-2 RNA
dependent RNA polymerase (RdRp): A molecular docking study. Life
Sci. 253:1175922020. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Elfiky AA: Anti-HCV, nucleotide
inhibitors, repurposing against COVID-19. Life Sci. 248:1174772020.
View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Costanzo M, De Giglio MAR and Roviello GN:
SARS-CoV-2: Recent reports on antiviral therapies based on
lopinavir/rito-navir, darunavir/umifenovir, hydroxychloroquine,
remdesivir, favipiravir and other drugs for the treatment of the
new coronavirus. Curr Med Chem. 27:4536–4541. 2020. View Article : Google Scholar
|
|
120
|
Ye XT, Luo YL, Xia SC, Sun QF, Ding JG,
Zhou Y, Chen W, Wang XF, Zhang WW, Du WJ, et al: Clinical efficacy
of lopinavir/ritonavir in the treatment of Coronavirus disease
2019. Eur Rev Med Pharmacol Sci. 24:3390–3396. 2020.PubMed/NCBI
|
|
121
|
Sallard E, Lescure FX, Yazdanpanah Y,
Mentre F and Peiffer-Smadja N: Type 1 interferons as a potential
treatment against COVID-19. Antiviral Res. 178:1047912020.
View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Sauñe PM, Bryce-Alberti M,
Portmann-Baracco AS and Accinelli RA: Methylprednisolone pulse
therapy: An alternative management of severe COVID-19. Respir Med
Case Rep. 31:1012212020.PubMed/NCBI
|
|
123
|
Yang JW, Yang L, Luo RG and Xu JF:
Corticosteroid administration for viral pneumonia: COVID-19 and
beyond. Clin Microbiol Infect. 26:1171–1177. 2020. View Article : Google Scholar :
|
|
124
|
Li SF, Gong MJ, Zhao FR, Shao JJ, Xie YL,
Zhang YG and Chang HY: Type I interferons: Distinct biological
activities and current applications for viral infection. Cell
Physiol Biochem. 51:2377–2396. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Andreakos E and Tsiodras S: COVID-19:
Lambda interferon against viral load and hyperinflammation. EMBO
Mol Med. 12:e124652020. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Du B, Qiu HB, Zhan X, Wang YS, Kang HYJ,
Li XY, Wang F, Sun B and Tong ZH: Pharmacotherapeutics for the New
Coronavirus Pneumonia. Zhonghua Jie He He Hu Xi Za Zhi.
43:E0122020.In Chinese.
|
|
127
|
Vidal P: Interferon α in cancer
immunoediting: From elimination to escape. Scand J Immunol.
91:e128632020. View Article : Google Scholar
|
|
128
|
Nelemans T and Kikkert M: Viral innate
immune evasion and the pathogenesis of emerging RNA virus
infections. Viruses. 11:9612019. View Article : Google Scholar :
|
|
129
|
Abdul-Sater AA, Majoros A, Plumlee CR,
Perry S, Gu AD, Lee C, Shresta S, Decker T and Schindler C:
Different STAT transcription complexes drive early and delayed
responses to type I IFNs. J Immunol. 195:210–216. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Langevin C, Aleksejeva E, Passoni G, Palha
N, Levraud JP and Boudinot P: The antiviral innate immune response
in fish: Evolution and conservation of the IFN system. J Mol Biol.
425:4904–4920. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Zhou Q, Wei XS, Xiang X, Wang X, Wang ZH,
Chen V, Shannon CP, Tebbutt SJ, Kollmann TR and Fish EN:
Interferon-a2b treatment for COVID-19. medRxiv. https://www.101101/2020040620042580urisimplehttps://101101/2020040620042580.
|
|
132
|
Morgenstern B, Michaelis M, Baer PC, Doerr
HW and Cinatl J Jr: Ribavirin and interferon-beta synergistically
inhibit SARS-associated coronavirus replication in animal and human
cell lines. Biochem Biophys Res Commun. 326:905–908. 2005.
View Article : Google Scholar
|
|
133
|
Mantlo E, Bukreyeva N, Maruyama J,
Paessler S and Huang C: Antiviral activities of type I interferons
to SARS-CoV-2 infection. Antiviral Res. 179:1048112020. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Young MJ, Clyne CD and Chapman KE:
Endocrine aspects of ACE2 regulation: RAAS, steroid hormones and
SARS-CoV-2. J Endocrinol. 247:R45–R62. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Xavier AM, Anunciato AK, Rosenstock TR and
Glezer I: Gene expression control by glucocorticoid receptors
during innate immune responses. Front Endocrinol (Lausanne).
7:312016. View Article : Google Scholar
|
|
136
|
Hardy RS, Raza K and Cooper MS:
Therapeutic glucocorticoids: Mechanisms of actions in rheumatic
diseases. Nat Rev Rheumatol. 16:133–144. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Song P, Li W, Xie J, Hou Y and You C:
Cytokine storm induced by SARS-CoV-2. Clin Chim Acta. 509:280–287.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Komiyama M and Hasegawa K: Anticoagulant
therapy for patients with coronavirus disease 2019: Urgent need for
enhanced awareness. Eur Cardiol. 15:e582020. View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Merrill JT, Erkan D, Winakur J and James
JA: Emerging evidence of a COVID-19 thrombotic syndrome has
treatment implications. Nat Rev Rheumatol. 16:581–589. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Fletcher-Sandersjöö A and Bellander BM: Is
COVID-19 associated thrombosis caused by overactivation of the
complement cascade? A literature review. Thromb Res. 194:36–41.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Conway EM and Pryzdial ELG: Is the
COVID-19 thrombotic catastrophe complement-connected? J Thromb
Haemost. Aug 6–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Furie B and Furie BC: Mechanisms of
thrombus formation. N Engl J Med. 359:938–949. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Giannis D, Ziogas IA and Gianni P:
Coagulation disorders in coronavirus infected patients: COVID-19,
SARS-CoV-1, MERS-CoV and lessons from the past. J Clin Virol.
127:1043622020. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Bikdeli B, Madhavan MV, Jimenez D, Chuich
T, Dreyfus I, Driggin E, Nigoghossian C, Ageno W, Madjid M, Guo Y,
et al: COVID-19 and thrombotic or thromboembolic disease:
Implications for prevention, antithrombotic therapy, and follow-up:
JACC State-of-the-Art review. J Am Coll Cardiol. 75:2950–2973.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Liu J, Li J, Arnold K, Pawlinski R and Key
NS: Using heparin molecules to manage COVID-2019. Res Pract Thromb
Haemost. 4:518–523. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Panka BA, de Grooth HJ, Spoelstra-de Man
AM, Looney MR and Tuinman PR: Prevention or treatment of ards with
aspirin: A review of preclinical models and meta-analysis of
clinical studies. Shock. 47:13–21. 2017. View Article : Google Scholar
|
|
147
|
Chen W, Janz DR, Bastarache JA, May AK,
O'Neal HR Jr, Bernard GR and Ware LB: Prehospital aspirin use is
associated with reduced risk of acute respiratory distress syndrome
in critically ill patients: A propensity-adjusted analysis. Crit
Care Med. 43:801–807. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Li Z, Li X, Huang YY, Wu Y, Liu R, Zhou L,
Lin Y, Wu D, Zhang L, Liu H, et al: Identify potent SARS-CoV-2 main
protease inhibitors via accelerated free energy perturbation-based
virtual screening of existing drugs. Proc Natl Acad Sci USA.
117:27381–27387. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Whyte CS, Morrow GB, Mitchell JL, Chowdary
P and Mutch NJ: Fibrinolytic abnormalities in acute respiratory
distress syndrome (ARDS) and versatility of thrombolytic drugs to
treat COVID-19. J Thromb Haemost. 18:1548–1555. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Ju B, Zhang Q, Ge J, Wang R, Sun J, Ge X,
Yu J, Shan S, Zhou B, Song S, et al: Human neutralizing antibodies
elicited by SARS-CoV-2 infection. Nature. 584:115–119. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Graham BS: Rapid COVID-19 vaccine
development. Science. 368:945–946. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Shepard HM, Phillips GL, D Thanos C and
Feldmann M: Developments in therapy with monoclonal antibodies and
related proteins. Clin Med (Lond). 17:220–232. 2017. View Article : Google Scholar
|
|
153
|
Thanh Le T, Andreadakis Z, Kumar A, Gómez
Román R, Tollefsen S, Saville M and Mayhew S: The COVID-19 vaccine
development landscape. Nat Rev Drug Discov. 19:305–306. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Corey L, Mascola JR, Fauci AS and Collins
FS: A strategic approach to COVID-19 vaccine R&D. Science.
368:948–950. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Zhao Z, Li Y, Zhou L, Zhou X, Xie B, Zhang
W and Sun J: Prevention and treatment of COVID-19 using Traditional
Chinese Medicine: A review. Phytomedicine. 153308:2020.
|
|
156
|
Zhang YS, Cong WH, Zhang JJ, Guo FF and Li
HM: Research progress of intervention of Chinese herbal medicine
and its active components on human coronavirus. Zhongguo Zhong Yao
Za Zhi. 45:1263–1271. 2020.In Chinese. PubMed/NCBI
|
|
157
|
McKimm-Breschkin JL, Jiang S, Hui DS,
Beigel JH, Govorkova EA and Lee N: Prevention and treatment of
respiratory viral infections: Presentations on antivirals,
traditional therapies and host-directed interventions at the 5th
ISIRV Antiviral Group conference. Antiviral Res. 149:118–142. 2018.
View Article : Google Scholar
|
|
158
|
Teschke R, Larrey D, Melchart D and Danan
G: Traditional Chinese Medicine (TCM) and herbal hepatotoxicity:
RUCAM and the role of novel diagnostic biomarkers such as
MicroRNAs. Medicines (Basel). 3. pp. 182016, View Article : Google Scholar
|
|
159
|
Hu XY, Logue M and Robinson N:
Antimicrobial resistance is a global problem - a UK perspective.
Eur J Integr Med. 36:1011362020. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Ho LTF, Chan KKH, Chung VCH and Leung TH:
Highlights of traditional Chinese medicine frontline expert advice
in the China national guideline for COVID-19. Eur J Integr Med.
36:1011162020. View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Porte L, Legarraga P, Vollrath V, Aguilera
X, Munita JM, Araos R, Pizarro G, Vial P, Iruretagoyena M, Dittrich
S and Weitzel T: Evaluation of a novel antigen-based rapid
detection test for the diagnosis of SARS-CoV-2 in respiratory
samples. Int J Infect Dis. 99:328–333. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
162
|
Mirijello A, D'Errico MM, Lamarca A,
Piscitelli P and De Cosmo S: Comment on Matricardi PM et al: The
first, holistic immunological model of COVID-19: Implications for
prevention, diagnosis, and public health measures. Pediatr Allergy
Immunol. May 17–2020.Epub ahead of print. View Article : Google Scholar
|