1. Introduction
Bone-related diseases, such as fractures,
osteoporosis and osteoarthritis (OA), severely affect the quality
of life of patients due to their high incidence, slow recovery,
associated pain and negative effects on patient behavior. Due to
the aging of the population in several countries, the prevalence of
bone-related diseases is projected to further increase in the
following few decades. Data from 2013 indicated that ~57 million
Americans aged >50 years suffered from bone diseases, among
which 48 million had osteopenia and 9 million had osteoporosis. The
diseases were accompanied by a risk of fracture in these
individuals. Without intervention, the prevalence of osteopenia is
projected to increase to 64.3 million American individuals and that
of osteoporosis to 11.9 million by the year 2030 (1). Bone disease is the focus of a large
number of clinical studies, due to the accompanying high combined
lifetime risk of forearm, hip and vertebral fractures (40%), which
is comparable to the rate of cardiovascular diseases (2). In addition to the high morbidity
and mortality rates, fractures related to osteoporosis have also
created a significant financial burden to societies worldwide. For
instance, osteoporosis-related costs in the European Union amounted
to ~€37 billion in 2010; the majority of that amount was spent on
fracture therapy and long-term fracture care, accounting for 66 and
29%, respectively, of the budget (3).
Melatonin, a common molecule with a simple structure
known as N-acetyl-5-methoxytryptamine, exists in almost all
living organisms (4). Melatonin
is secreted by pinealocytes in the pineal gland, while certain
tissues can also produce a small amount of melatonin locally
(5). There is a synchronization
between melatonin production and the light/dark (L/D) cycle.
Melatonin is synthesized and secreted in dark environments. When
retinal photoreceptive ganglion cells are stimulated by light
(mainly in the blue range), the synthesis and secretion of
melatonin reduces until no more is secreted (6,7).
Generally, levels of melatonin begin to increase early in the
evening and peak at 12-2 a.m., followed by a progressive decrease
thereafter (8). As the organism
ages, melatonin production gradually declines. Melatonin levels
continuously decrease from the age of 40-45 years (6).
Currently, melatonin is considered a potent
cytoprotective agent, rather than a hormone in the classical sense
(9). Melatonin has excellent
lipophilic properties and can easily enter the cell membrane and
subcellular compartment (10).
Melatonin can synchronize the circadian clock in peripheral
tissues, maintain the synchronization of bone metabolism with L/D
cycles and participate in numerous important physiological
processes, such as anti-inflammatory, antitumor and antioxidation
processes, as well as regulating circadian and endocrine rhythms,
regulating immunity, and promoting wound healing and tissue
regeneration (7,11). Melatonin plays a positive role in
bone-related diseases by exerting multiple effects. Although there
are several physical and drug treatments for bone-related diseases,
melatonin has the advantage over other drugs of being inexpensive,
and having a wide safety margin, a wide impact on tissues and
almost no side effect, suggesting its potential as a main or
complementary treatment strategy for a large range of bone
diseases.
2. Bone injury
Basic study of bone injury
Bone injury is very common in clinical practice. A
variety of pathologies, such as tumors, trauma and surgery, as well
as other factors, are likely to cause varying degrees of bone
injury. This is a major issue for clinical treatment at present,
and an important challenge that will threaten human health in the
ensuing 50 years. The bone defect size largely determines the
amount of bone repair. The larger the defect, the more difficult to
obtain a satisfactory repair (12). Bone repair is often affected by a
variety of negative effects, such as possible infection and
ischemia of the bone injury site or adjacent tissues, and systemic
diseases. Therefore, clinical intervention is required for bone
repair.
Possible effects of melatonin on bone
injury repair
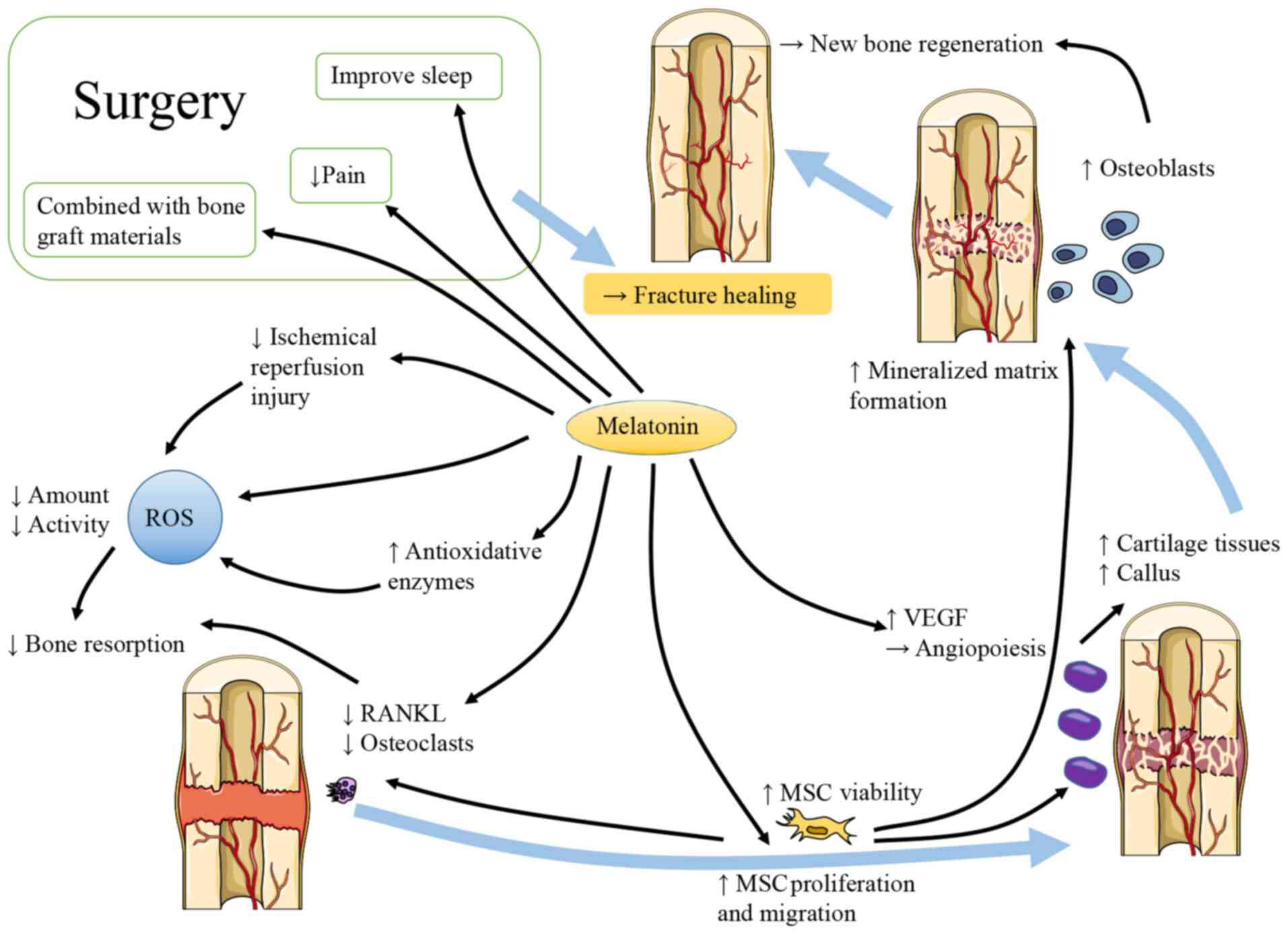
As shown in Fig.
1, considerable evidence has demonstrated that melatonin
contributes to bone repair. There are different claims about the
effects of melatonin on osteogenic and osteoclastic activities.
Melatonin has been shown to enhance the vertical bone augmentation
of rat calvaria by increasing new bone regeneration,
neovascularization and the number of osteoblast-like cells
(13). It has also been shown to
increase the cartilage and callus at the fracture site (14). At pharmacological doses,
melatonin has been shown to stimulate osteoblast proliferation and
alkaline phosphatase (ALP) activity in a dose-dependent manner.
In vitro, melatonin increases the expression of collagen
type I (Col1), bone sialoprotein, osteopontin and osteocalcin
(OCN), and promotes the production of mineralized extracellular
matrix (ECM). At the same time, femoral neocortical bone is
enhanced in mice administered an intraperitoneal (i.p.) injection
of melatonin (15). However,
Histing et al (14)
reported that melatonin delayed bone healing in a mouse model of
femoral fracture. They explained that melatonin exerted a positive
effect on bone repair by inhibiting bone resorption instead of
promoting bone regeneration. The levels of receptor activator of
NF-κB ligand (RANKL) were reduced in the mice with fractures that
received a daily dose of 50 mg/kg melatonin, which may inhibit bone
resorption by damaging the balance between osteoprotegerin (OPG)
and RANKL.
In addition to exhibiting osteogenic and osteoclast
activity, the role of osteoblast and osteoclast differentiation
during the process of bone repair is also of interest. Sethi et
al (16) noted that
osteoblast differentiation requires chronic and uninterrupted
melatonin exposure. Melatonin may promote mesenchymal stem cell
(MSC) proliferation and migration, at least partly by upregulating
neuropeptide Y (NPY) and NPY receptor Y1 (NPY1R), accelerating
osteogenic differentiation and promoting fracture healing in the
rat femur. Concurrently, NPY/NPY1R expression has been shown to be
increased in the fracture zone and serum (17). Osteogenic and chondrogenic
differentiation can be promoted, and adipogenesis can be inhibited
through the enhancement of runt-related transcription factor 2
expression and the Wnt/β-catenin signaling pathway, as well as the
inhibition of peroxisome proliferator-activated receptor (PPAR)-γ
(18). The upregulation of the
platelet-derived growth factor/protein kinase B pathway partly
contributes to the enhanced osteogenic potential and weakened
osteoclastic differentiation of MC3T3-E1 cells, and promotes
fracture healing in mice with femoral fracture following melatonin
treatment (19). In addition,
the BMP, extracellular regulated kinase (ERK) and Wnt signaling
pathways also participate in the process, while melatonin can
improve wound healing and trigger osteogenesis markers in a
dose-dependent manner (20). In
addition, endochondral bone formation is an important form of
osteogenesis. Melatonin increases the expression of chondrogenic
differentiation genes in MSCs, which could be partly blocked by
luzindole (21).
Inflammation and oxidative stress are inevitable
during bone injury. Melatonin is known for its potent antioxidant
and anti-inflammatory properties. Oxidative stress produces
reactive oxygen species (ROS) and is usually promoted by aging
(22), which can lead to
excessive bone resorption (23,24). Melatonin is considered a potent
natural antioxidant, not only due to the direct inhibition of ROS,
but also due to the mobilization of the intracellular antioxidative
enzyme system. Melatonin can protect MSCs against oxidation-induced
apoptosis by reducing ROS production, enhancing cell viability and
promoting continued differentiation (25). Melatonin can increase solute
carrier family 39 member 1 expression, activate the
mitogen-activated protein kinase (MAPK)/ERK pathway, increase
phosphorylated-ERK1/2/5 levels and significantly inhibit the
production of ROS; moreover, zinc uptake in cells is increased
(26). All the above-mentioned
processes can inhibit cell apoptosis (27). In addition, melatonin is
beneficial for the inhibition of oxygen free radical activity
during fracture healing and the regulation of antioxidant enzyme
activity, which promotes fracture healing. In a previous study, it
was observed that in contrast to the fracture group, more bone
binding was observed in the melatonin treatment fracture group at
the same healing time (28 days after the fracture) (28).
Vascular injury often exists simultaneously in bone
injuries, such as fractures, which inevitably leads to ischemia
and/or hypoxia at the injury site and is extremely unfavorable for
the repair of defects. Ischemia/reperfusion can cause excessive ROS
production in tissues and lead to cell damage (29,30). Melatonin can eliminate these
adverse effects and can be used in fractures with vascular injury
and compartment syndrome (31).
In hypoxic environments, MC3T3-E1 cells stimulated by melatonin
prefer to differentiate towards osteoblasts and promote
mineralization through the p38 mitogen-activated protein kinase and
protein kinase D1 pathways (32). The effect of melatonin on
angiogenesis mediators also plays an important role in bone
regeneration (33). Growth
factors are considered potential modulators of angiogenesis. For
instance, vascular endothelial growth factor (VEGF) contributes to
angiogenesis (34). Melatonin
treatment has been found to elevate the level of VEGF during
granulation tissue formation and accelerate the angiogenic process
(35), indicating that melatonin
can provide beneficial effects to bone defect repair with vascular
injury.
Moreover, diabetes mellitus (DM) induces high levels
of ROS production. In DM model rats with fractures, the process of
fiber formation and trabecular mineralization was more rapid in the
melatonin treatment group compared with the control group (36).
As previously demonstrated, the use of melatonin
pre-operatively helped improve the quality sleep of patients and
reduced the use of opioid drugs during surgery. The normal
circadian rhythm of melatonin secretion can be altered by
anesthesia (37). The
pre-operative use of melatonin may also have the potential to
reduce the incidence of delirium; however, certain existing studies
have reached varying conclusions. Al-Aama et al (38) thought exogenous melatonin
administered nightly may decrease delirium occurrence in elderly
medical in-patients. Sultan (39) pointed out that melatonin was
successful in decreasing post-operative delirium. However, the
study by de Jonghe et al (40) came to the conclusion that
treatment with melatonin did not reduce the incidence of delirium
in older-aged patients with hip fracture surgery. Melatonin can be
used in combination with various bone graft materials to stimulate
bone regeneration in large or comminuted bone injuries (41). In addition, melatonin can
significantly protect bones from radiation injury and prevent
epiphyseal growth plate damage (42).
The time and dose of melatonin treatment is worthy
of consideration, since high doses, such as 50 mg/kg, can cause
decreased bone remodeling in mice, thus delaying fracture healing
(14). Melatonin supplementation
should also be carried out at night as far as possible, to adhere
to its natural secretion law, to avoid breaking the normal
secretory circadian rhythm, which can have adverse consequences.
Evidence from the relevant animal studies is presented in Table I.
 | Table IEvidence of the effects of melatonin
on bone injury in animal studies. |
Table I
Evidence of the effects of melatonin
on bone injury in animal studies.
| Refs. | Objectives | Model | Route of
administration | Time of
administration | Frequency | Doses | Duration | Outcomes |
|---|
| 13 | Fischer rats | Calvarium
holes | Powder local
implantation | - | Only once | 10 mg | - | After 12 weeks:
Increased new bone regeneration, neovascularization and
osteoblast-like cells |
| 14 | CD-1 mice | Femur fracture | i.p. | - | Daily | 50 mg/kg | 2 and 5 weeks | 2 weeks: Delayed
healing 5 weeks: Increased cartilage and callus at the fracture
site |
| 15 | Mice | - | i.p. | - | Daily | 100 mg/kg | 21 days | More new femoral
neocortical bone formation |
| 17 | Sprague-Dawley
rats | Femoral
fracture | i.p. | Morning | Daily | 30 mg/kg | 8 weeks | Promotive fracture
healing and ALP activity, inhibited osteoclasts
differentiation |
| 19 | C57BL/6J mice | Femoral
fracture | i.p. | - | Daily | 50 mg/kg | 5 weeks | Promotive fracture
healing and ALP activity, inhibited osteoclasts differentiation and
obviously bridging callus formation |
| 28 | Sprague-Dawley
rats | Femoral
fracture | i.p. | - | Daily | 30 mg/kg | 28 days | More bony
union |
| 31 | Wistar-albino
rats | Tibia fracture | i.p. | - | Daily | 25 mg/kg | 14 days | Melatonin
eradicated adverse effects of ischemia on fracture healing |
| 33 | Albino New Zealand
rabbits | Tibial defect | Powder local
implantation | - | Only once | 1.2 mg | - | After 1 week and 2
weeks: Longer cortical bone and more blood vessels formation |
| 36 | Sprague-Dawley
rats | Tibial defect and
DM | i.p. | 19:00-20:00 | Daily | 250 µg | 10 and 30 days | 10 days: Higher
number of osteoblasts and blood vessels as well as larger new
mineralized surface 30 days: Lower level of advanced oxidation
protein products and malondialdehyde |
| 42 | Sprague-Dawley
rats | Radiation | i.p. | 30 min prior to
radiation | Daily | 15 mg/kg | 3 days | 6 weeks later: A
superior radioprotective function of melatonin over amifostine in
preventing radiation-induced epiphyseal growth plate injury |
3. Osteoporosis
Study basics of osteoporosis
Osteoporosis is considered one of the most common
diseases, and is becoming increasingly prevalent with the aging of
the global population. Millions of individuals worldwide suffer
from osteoporosis, particularly postmenopausal women (43-45) and the elderly (46,47). The reduced bone density and
damaged bone architecture caused by osteoporosis can increase the
risk of fragility fractures, and lead to a higher morbidity and
mortality. A variety of drugs with varying degrees of efficacy and
side-effects have been used for the treatment of osteoporosis
(48). Even with the existing
osteoporosis treatments, the prevalence of osteoporosis is steadily
increasing (49), which has
created a huge economic burden to societies worldwide (50-52). Thus, novel strategies need to be
developed to prevent or combat bone loss for the treatment of
osteoporosis and its complications.
Potential effects of melatonin on
osteoporosis
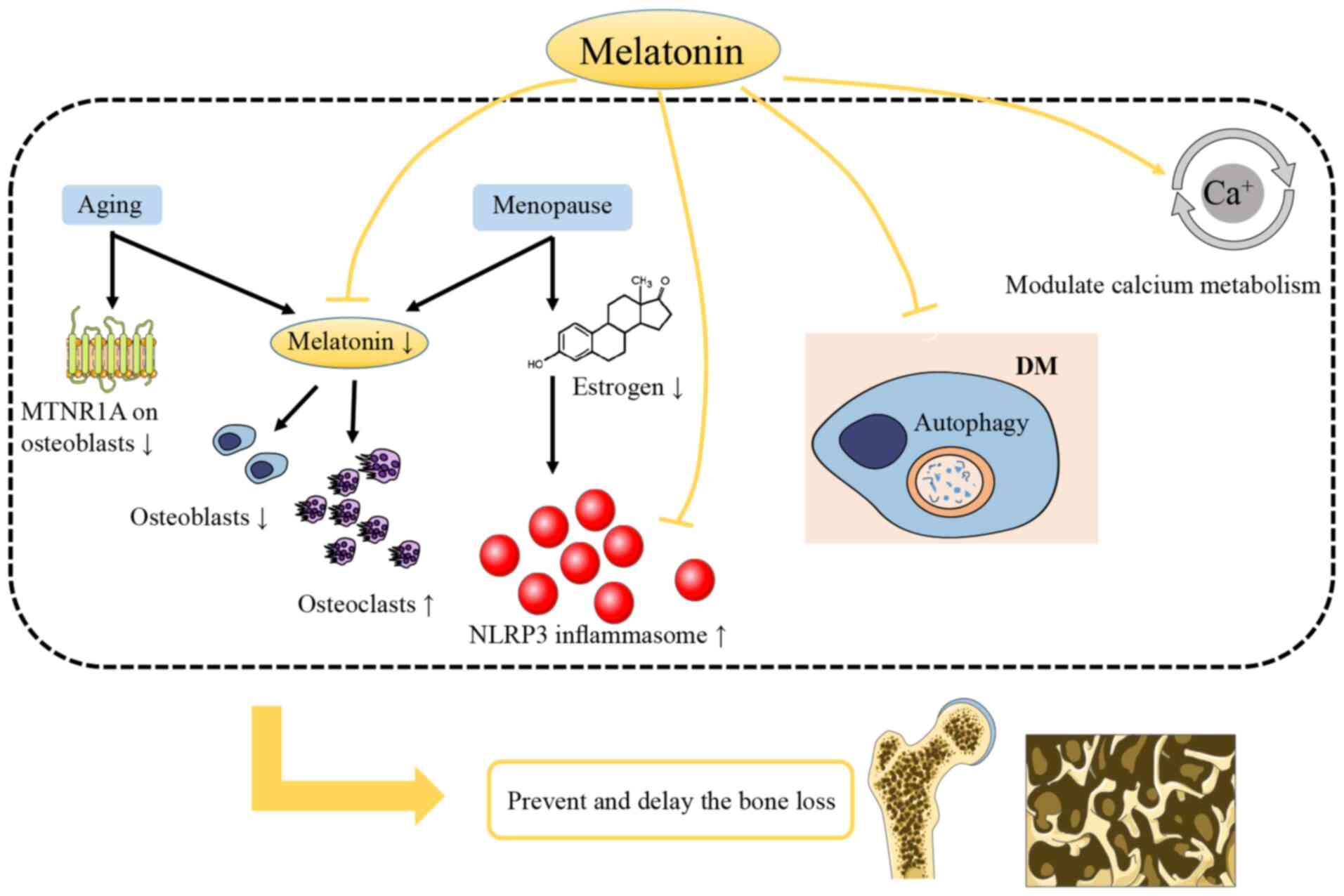
Melatonin is involved in the regulation of bone mass
accumulation and loss (Fig. 2).
Egermann et al (53)
confirmed that the bone mass significantly decreases following
pinealectomy. The decrease of melatonin secretion is associated
with menopause and is one of the most important causes of
osteoporosis (54). The
production of melatonin decreases with age (55), which may lead to a higher bone
loss among the elderly. In addition, the expression of melatonin
receptor 1A (MTNR1A) on the surface of human osteoblasts decreases
with age, which is more pronounced in women (15).
It has been demonstrated that melatonin
supplementation can improve perimenopausal- and age-related
osteoporosis. Melatonin supplementation is well-tolerated and can
attenuate perimenopausal symptoms, as well as restore the balance
of bone remodeling to avoid bone loss and osteoporosis (56). The daily oral melatonin
administration (100 mg/kg body weight) has been reported to
increase bone formation to prevent ovariectomy-induced bone
degeneration in mice (57).
Although its efficacy requires further confirmation, melatonin is
considered a safe nutritional supplement for peri- and
postmenopausal women to improve bone density (58). Moreover, a dietary melatonin
supplement has been shown to improve the microstructure and
biomechanical properties of the bones of aged rats (59).
Estrogen deficiency, the major characteristic of
menopause, contributes to osteoporosis. Increased levels of
nucleotide-binding domain and the leucine-rich repeat pyrin 3
domain (NLRP3) inflammasome have been observed in the hippocampus
of female mice with estrogen deficiency (60). Melatonin can attenuate
osteoporosis induced by estrogen deficiency and can improve the
osteoblastic differentiation potential by inhibiting NOD-, LRR- and
pyrin domain-containing protein 3 inflammasome activation. The
modulation of the Wnt/β-catenin pathway is involved in this process
(61).
Type 2 DM and osteoporosis are both negatively
affected by aging and lifestyle changes and quite often coexist. A
high risk of fracture has been identified in patients with type 2
DM, particularly those with long periods of DM, poor glycemic
control and diabetic complications (62,63). Reduced bone remodeling is one of
the characteristics of DM, and autophagy is considered to be a
potential target for the management of diabetic osteoporosis
(64,65). The level of autophagy in
osteoblasts may be reduced, and the process of DM-induced
osteoporosis may be delayed by melatonin by inhibiting the ERK
signaling pathway (66).
Patients with multiple sclerosis (MS) have decreased serum
melatonin levels and are also at risk of osteoporosis, while
melatonin therapy can reduce the risk and normalize bone
metabolites in MS (67). In
addition to the modulation of bone formation and resorption, there
are other effects of melatonin on bone metabolism, such as
modulating calcium metabolism to prevent osteoporosis and
hypocalcemia (68). Related
evidence from relevant human and animal studies is presented in
Table II.
| Table IIEvidence of the effects of melatonin
on osteoporosis in animal and clinical studies. |
Table II
Evidence of the effects of melatonin
on osteoporosis in animal and clinical studies.
|
Refs. | Objectives | Model | Route of
administration | Time of
administration | Frequency | Doses | Duration | Outcomes |
|---|
| 56 | Perimenopausal
women | - | Oral | Night | Daily | 3 mg | 6 months | The ratio of type-I
collagen cross-linked N-telopeptide (NTX): OCN trended
downward to 1:1. Improved physical domain scores |
| 57 | C57BL/6 mice
(female) | Ovariectomy | Oral gavage | 6 weeks after
surgery | Daily | 100 mg/kg | 6 weeks | Increased bone
formation |
| 59 | Wistar rats | - | Diluted in drinking
water | - | - | 10 mg/kg/day | 10 weeks | Higher bone volume,
bone trabecular number, trabecular thickness, cortical thickness,
bone stiffness, flexural modulus and ultimate load |
| 61 | C57BL/6J mice
(female) | Ovariectomy | i.p. | - | Daily | 10, 50 mg/kg | 8 weeks | Melatonin
alleviated bone loss in a dose- dependent manner |
| 66 | Sprague-Dawley
rats | Type 2 DM | i.p. | - | Daily | 50, 100 mg/kg | 4, 8, 12 weeks | Melatonin improved
the bone microstructure and reduced the level of autophagy (50
mg/kg was better than 100 mg/kg) |
| 67 | C57BL/6 mice
(female) | Experimental
autoimmune encephalomyelitis | i.p. | - | Daily | 10 mg/kg | 13 days | Increased
25-hydroxyvitamin D, calcium and OCN |
4. Osteoarthritis
Basic study of OA
OA accompanied by chronic joint degeneration is one
of the most common joint diseases, affecting ~3.8% of the world
population (69). Aging,
obesity, sex, genetics, diet-related factors, specific bone/joint
shapes and numerous other factors may cause the degenerative injury
of articular cartilage, and reactive hyperplasia of the articular
margin and subchondral bone, which may lead to the occurrence of OA
(70-72).
The functions of articular cartilage depend on
cartilage ECM, which primarily comprises proteoglycan and Col2α1
(73). OA is characterized by
the imbalance between cartilage ECM anabolism and catabolism
(74). The development of OA
occurs due to the presence of oxidative stress and inflammation
(75). For instance, interleukin
(IL)-1β is considered a primary inflammatory mediator in joints
with local OA, and is involved in the early inflammatory process of
OA, inducing chondrocyte metabolic disorders and cartilage
dysfunction, ultimately resulting in joint dysfunction (76,77).
The current therapies for OA mainly focus on
reducing joint load and large motion, with the aim of relieving
symptoms, delaying the pathological process and improving the
quality of life of patients with OA (78). Appropriate physical therapy,
proper exercise, drug therapy and joint replacement surgery, among
others, can be considered as treatment methods. Anti-inflammatory
and analgesic drugs can be used to alleviate the symptoms of
patients. However, drugs currently used in the treatment of OA,
such as glucocorticoids and analgesics, have certain side-effects
(79). Therefore, it is
necessary to evaluate the risks of drugs and to identify novel
types of low-risk drugs.
Potential effects of melatonin on OA
Inflammation plays a crucial role in the
pathogenesis of OA, since mild and chronic inflammation have been
shown to contribute to the symptoms and progression of OA (80,81). The self-repair ability of
cartilage is limited, with the cell-based articular cartilage
repair ability in inflamed joints being even lower. Melatonin
intervention can partly restore the chondrogenic differentiation
ability of MSCs affected by IL-1β-induced inflammation (21,77). In addition, the accumulation of
ECM increases due the enhancement of ECM synthesis and the
reduction of the degeneration enzyme expression induced by IL-1β
(82). The effect of long-term
intervention (21 days) is significant. Melatonin can also reduce
the phosphorylation of p65 and IκBα, thereby inhibiting downstream
NF-κB signaling pathway activation, which plays a key role in
metabolism, inflammation and apoptosis (83).
ROS can be detected in the joints of OA model rats,
which can cause hyaluronic acid depolymerization and molecular
configuration changes, resulting in a decrease in the viscosity of
synovial fluid (84). The
age-related imbalance in ROS production is responsible for
cartilage degradation and chondrocyte death (85). Pro-inflammatory cytokines mediate
intracellular ROS production during inflammation, impairing the
viability of cells and leading to apoptosis and senescence in
various cell types (86). As
part of the anti-inflammatory properties of melatonin, the dynamic
action of the sirtuin 1 (SIRT1) pathway is notable. Oxidative
stress upregulates SIRT1 in chondrocytes, while melatonin can
reduce the production of nitric oxide, cyclooxygenase-2, inducible
nitric oxide synthase and prostaglandin E2 by decreasing
the expression and activity of SIRT1 (87). The expression of SIRT1-dependent
nuclear factor of activated T cells 5 and nicotinamide
phosphoribosyltransferase in IL-1β-stimulated chondrocytes can be
suppressed by melatonin to alleviate OA (88). At the same time, melatonin also
functions by activating antioxidant enzymes. Excessive ROS
production reduces antioxidant enzyme expression in the progression
of OA (89), while melatonin can
induce the production of antioxidant enzymes, such as superoxide
dismutase (90), while
inhibiting ROS production (25),
further suppressing oxidative stress.
The improper production of circadian clock-regulated
hormones may also be involved in the occurrence of OA (91). The expression of circadian clock
genes in chondrocytes is altered during the inflammatory process of
OA (92), as the expression peak
of brain and muscle ARNT-like 1 (Bmal1) is decreased, while
that of period circadian regulator 2 (Per2) is increased
(93). Per2 knockdown can
reduce the expression of major cartilage degenerative enzymes,
suggesting that the high expression of Per2 is one of the
reasons for the progression of OA. The decline in Bmal1
expression is also associated with the mechanisms of OA (94), and can be restored by melatonin
(95). Another study
demonstrated that clock-related gene expression decreased in
abnormal cartilage samples, and a nano-molar dose of melatonin
restored clock-related gene expression and corrected the abnormal
chondrocyte phenotype (95).
Multiple microRNAs (miRNAs/miRs) are involved in OA
(96); among these, miR-140-5p
has been shown to be expressed in cartilage and plays an important
role in the differentiation of chondrocytes and the degeneration of
cartilage (97). OA-associated
cartilage changes occur in mice that lack miR-140 (98), while the overexpression of
miR-140 has been shown to inhibit the synthesis of matrix catabolic
enzyme (99). Elevated levels of
pro-inflammatory cytokines in cartilage may reduce miR-140
expression (100). The
protective roles of melatonin in OA-induced cartilage degradation
are partly associated with the upregulation of miR-140 and the
activation of the SMAD signaling pathways (82), which can inhibit NF-κB pathways
in articular cartilage (101).
In addition, other miRNAs participating in the protection of the
cartilage, such as miR-526b-3p and miR-590-5p, can be upregulated
by melatonin, improving the chondrogenic differentiation of MSCs
(102).
An intra-articular glucocorticoid (GC) injection is
a method used to alleviate inflammation and chronic pain in
patients with OA. However, evidence has suggested that treatment
with GCs may only be effective in the short-term, while the
long-term use of GCs may not be effective, or may even aggravate
cartilage degradation (103,104). It has been reported that
dexamethasone-induced ECM degradation in chondrocytes in a
dose-dependent manner and reduced the intracellular proportion of
nicotinamide adenine dinucleotide (NAD)+/NAD + hydrogen
(NADH) and the supernatant concentration of NADP/NADPH. Melatonin
pre-treatment can reverse these negative effects, possibly via the
NAD+-dependent activation of SIRT1 (105), which can promote chondrocyte
survival and ECM synthesis to prevent dexamethasone-induced damage
to chondrocytes. On the other hand, NADPH oxidase has been shown to
mediate the proliferation of multiple cell types, including stem
cells; however, it is a major source of ROS (106). Melatonin can effectively
regulate the ROS production levels of NADPH oxidase. In general,
NADPH oxidase produces ROS at non-cytotoxic levels; when ROS
production increases to a harmful level, excess ROS are removed by
melatonin (25).
Transforming growth factor (TGF)-β is considered to
be one of the synthetic factors engaged in cartilage maintenance
(107). A large amount of TGF-β
is present in healthy cartilage; however, the level of TGF-β is
decreased in OA-affected cartilage (108). Although TGF-β exerts protective
effects on cartilage, it has been proven that it can also be a
destructive factor (109).
Following the exogenous melatonin (1-10 ng/ml) treatment of porcine
articular chondrocytes, the level of intracellular TGF-β1 has been
shown to increase. This suggests that melatonin can promote porcine
chondrocyte ECM synthesis, possibly through the TGF-β signaling
pathway, and the use of melatonin instead of TGF-β in the treatment
of OA may provide a suitable amount of TGF-β and reduce adverse
reactions (110).
Melatonin can be detected in synovial fluid
(111), indicating that
melatonin secreted in its natural state can reach the articular
cavity. The nutrition of chondrocytes in articular cartilage mainly
originates from the synovial fluid, and therefore an
intra-articular melatonin injection may be a potentially effective
method of melatonin therapy for OA. However, melatonin treatment
may only be effective in the short-term and at low concentrations.
When melatonin stimulation persists, the proteolytic cleavage of
RANKL proteins in the synovium is promoted, causing severe
subchondral bone erosion (95).
Low concentrations of melatonin, such as 1 nM, can restore Col2α1
expression by inhibiting matrix metalloproteinase (MMP)-13; on the
contrary, high concentrations, such as 1 mM, cannot rescue the
reduced expression of Col2α1 caused by tumor necrosis factor
(TNF)-α exposure (112). ROS
generation is promoted if the concentration of melatonin is too
high or the incubation time is too long (113). It has been reported that
pharmacological concentrations (µm-mM) of melatonin promote
the production of ROS and pro-inflammatory cytokines (114). The results of the study by Liu
et al (25) demonstrated
that short-term melatonin treatment (5 days) promoted MSC
proliferation, while long-term culture had no significant effect.
These results suggested extra attention should be paid to the dose
and duration of melatonin therapy, in order to avoid severe
side-effects. Mild to moderate exercise can inhibit the
inflammatory processes through joint compression-mediated
biomechanical stimulation, helping to reduce the negative effects
of high-dose and/or long-term melatonin use. There may be a
synergistic effect on cartilage protection between melatonin
therapy and treadmill exercise, which appears to be more effective
in the early stage of the disease (112). Moreover, melatonin-combined
exercise can not only restore disordered molecular clocks and
correct cartilage abnormalities, but also reduce periarticular bone
defects and maintain articular bone homeostasis in late-stage OA
(95). However, only mild to
moderate exercise is beneficial, as strenuous daily exercise
aggravates OA (Fig. 3) (115). Evidence on this matter from
relevant animal studies is presented in Table III.
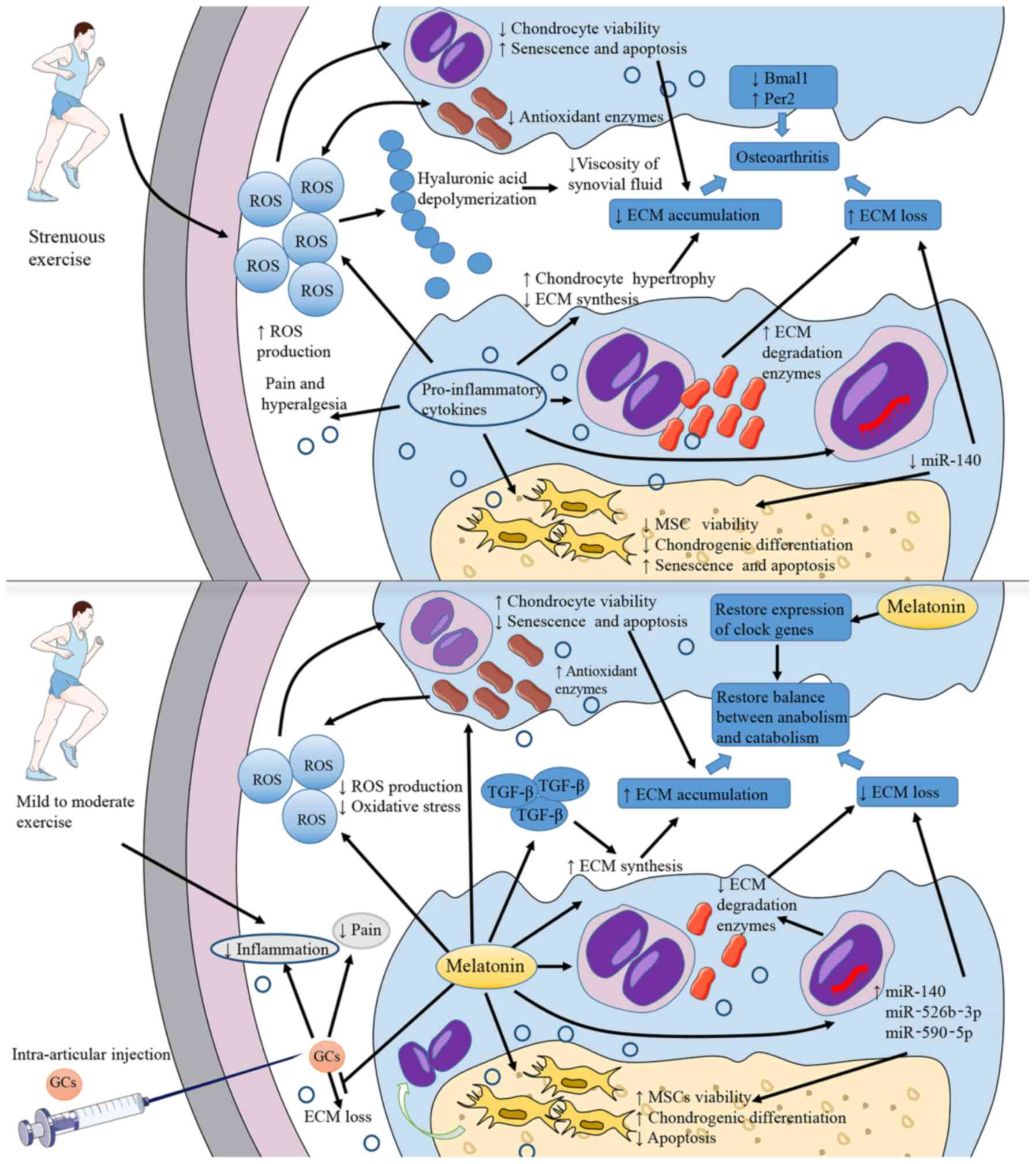 | Figure 3Pathogenesis of OA and potential
roles of melatonin. The direct cause of OA is the decrease of
cartilage ECM. Inflammation and strenuous exercise lead to an
increased ROS production, activating oxidative stress, inhibiting
chondrocytes viability, and decreasing the production of ECM
components. Pro-inflammatory cytokines promote chondrocytes
hypertrophy and then reduce ECM synthesis. Additionally,
pro-inflammatory cytokines decrease miR-140 production in
chondrocytes, inhibit the viability and chondrogenic
differentiation of MSCs and increase the production of ECM
degradation enzymes. All these mechanisms promote the loss of ECM.
Oxidative stress also leads to decreased viscosity of synovial
fluid. Pro-inflammatory cytokines are also associated with pain and
hyperalgesia. The abnormal expression of clock-related genes, such
as the decrease in Bmal1 expression and the increase in
Per2 expression, is also considered to be related to the
occurrence of OA. Melatonin application can effectively antagonize
the above-mentioned processes, reducing the level of oxidative
stress and inflammation and restoring the normal expression of
clock genes. Moreover, melatonin can upregulate TGF-β expression to
increase ECM synthesis. Intra-articular injections of
glucocorticoids can relieve inflammation and pain, but may also be
associated with the risk of aggravating ECM loss. Melatonin can
alleviate this adverse reaction. In addition, melatonin treatment
combined with mild to moderate exercise may do better in OA
therapeutic process. OA, osteoarthritis; ECM, extracellular matrix;
ROS, reactive oxygen species; Bmal1, brain and muscle
ARNT-like 1; Per2, period circadian regulator 2; TGF-β,
transforming growth factor β. |
| Table IIIEvidence of the effects of melatonin
on osteoarthritis in animal studies. |
Table III
Evidence of the effects of melatonin
on osteoarthritis in animal studies.
| Refs. | Objectives | Model | Route of
administration | Time of
administration | Frequency | Doses | Duration | Outcomes |
|---|
| 82 | C57BL/6J mice | Surgically-induced
osteoarthritis | Intra-articular
injection | After surgery | Twice a week | 10 mg/ml (10
µl) | 4 weeks | Attenuated OA
progression |
| 87 | New Zealand white
rabbits (female) | Surgically-induced
osteoarthritis | Intra-articular
injection | Beginning on the
day of surgery | Weekly | 20 mg/kg | 4 weeks | Reduced cartilage
degradation |
| 88 | Lewis rats | Surgically-induced
osteoarthritis | Intra-articular
injection | On day 3 following
the surgery | Once | 10 mg/ml (20
µl) | - | Repressed
expression of relevant genes in rat OA pathogenesis after 3
weeks |
| 95 | Sprague-Dawley
rats | Intra-articular
collagenase injection- induced osteoarthritis | Subcutaneous
injection | - | Twice daily | 10 mg/kg | 4 weeks | Melatonin prevented
periarticular muscle damage and cartilage degeneration. But
prolonged melatonin administration leaded to subchondral bone
erosion |
| 112 | Sprague Dawley
rats | Intra-articular
collagenase injection- induced osteoarthritis | Subcutaneous
injection | 07:00 and
19:00 | Twice daily | 10 mg/kg | 1, 4 weeks | Melatonin with
treadmill exercise may have both preventive and synergistic effects
on rescue from cartilage degeneration and is more effective in the
initial phase (1 week) |
5. Periodontitis
Basic study of periodontitis
Periodontitis, an inflammatory and destructive
disease of the periodontal tissues, is characterized by the loss of
periodontal attachment. Periodontitis is also considered as
inflammation of the alveolar bone, since marginal alveolar bone
loss is a key secondary feature of periodontitis, with teeth
loosening and complete loss occurring at the terminal stage. The
common characteristics of periodontitis usually include redness in
the periodontal tissue, pain, pus overflow, halitosis and dental
stone formation, which progresses to alveolar bone resorption.
Dental plaque is the primary initiating factor of periodontitis,
creating and maintaining an inflammatory environment in the
periodontal area. Gingival inflammation (gingivitis) induced by
dental plaque is the most common and mildest type of periodontal
disease, with the potential to develop into periodontitis in the
case of no intervention. ROS generation is another important
feature of periodontitis. Oral bacteria, as well as the
inflammatory and immune reaction, lead to the generation of ROS,
contributing to the progression of the disease (116,117).
Scaling and root planning (SRP) is considered an
extremely effective basic treatment method for periodontitis.
Generally, adherence to basic periodontal therapy can improve
periodontal status in most patients with chronic periodontitis.
However, in certain patients, progressive attachment loss cannot be
terminated by SRP alone (118).
For this reason, adjuvant treatment with SRP should be
considered.
Potential effects of melatonin on
periodontitis
Saliva and plasma melatonin levels are significantly
lower in individuals with periodontal disease compared to
clinically healthy subjects (119); however, the ratio of saliva and
plasma melatonin levels is similar to that in healthy subjects
(120). In a previous study,
serum melatonin was introduced into the oral cavity through the
salivary glands at a stable proportion (~33%, the ratio of salivary
and serum melatonin) (121).
Moreover, the gingiva is one of the external sites of melatonin
synthesis, and melatonin receptor 1 has been found in human
gingiva, indicating that melatonin may play a receptor-mediating
role in the oral cavity (122).
Certain studies have suggested that melatonin may serve as a
potential supplementary therapy and a biomarker detecting the
dynamics of periodontal disease (123,124).
Melatonin levels in saliva and gingival crevicular
fluid vary inversely with the severity of periodontitis (125,126), suggesting that melatonin may
provide protective effects against the destruction of periodontal
tissues. Srinath et al (119) suggested that melatonin had
antibacterial properties, since Prevotella intermedia,
Streptococcus mutans and Porphyromonas gingivalis, the
primary bacteria in the occurrence and progression of
periodontitis, were sensitive to melatonin.
In a previous study, patients with severe
periodontitis received nonsurgical periodontal therapy (NSPT)
following the oral administration of melatonin at 1 mg/day (a
dietary supplement dosage advised by the Italian Ministry of
Health) for 1 month (127). All
patients were able to tolerate melatonin well, demonstrating a
significant reduction in probing depth (PD) within 6 months,
suggesting that melatonin supplementation is likely to promote the
healing process of periodontal pockets following long-term
treatment (127). A small
number of mild adverse reactions were observed at the initial stage
of oral administration, which disappeared within a few days without
affecting the compliance of the patients (127). Another study reported that,
when combined with NSPT, the oral administration of 2 mg melatonin
daily for 30 days improved the clinical attachment level (CAL) and
PD significantly following long-term treatment (3 and 6 months)
(128). Bazyar et al
(129) obtained similar results
with 6 mg melatonin daily administration daily with NPST. In a rat
model of periapical periodontitis, following an i.p. injection of
melatonin (10 mg/kg) for 21 days, radiological periapical bone loss
and osteoclasts were decreased, the OPG level was increased, and
the IL-1β, RANK and RANKL levels were decreased, as compared with
the positive control. In addition, the bacteria localization score
has been shown to be significantly lower following melatonin
treatment (130). Renn et
al (131) reported that
preventive melatonin supplementation suppressed the Toll-like
receptor 4/myeloid differentiation factor 88 pathway to inhibit the
activation of pro-inflammatory cytokines and normalize the balance
between RANKL and OPG, thus suppressing the progression of
periodontitis.
There may be a bidirectional association between DM
and periodontitis, both of which are common chronic diseases.
According to previous studies, DM is considered to be a risk factor
of periodontitis development, increasing the prevalence and
severity and promoting the progression of periodontitis (132,133). On the other hand, periodontitis
may also increase the complications of DM (134). Patients with DM or periodontal
disease have reduced melatonin levels in serum and saliva, and when
the two diseases coexist, these levels are further reduced
(135). In a previous study, in
patients with mild to moderate periodontitis with DM, melatonin
supplementation at 6 mg once a day for 8 weeks clearly increased
the serum melatonin levels; moreover, PD, CAL loss and the high
sensitivity-C reactive protein and IL-6 levels were reduced during
NSPT (129). Balci Yuce et
al (136) reported that
melatonin decreased osteoclasts and inhibited alveolar bone
resorption in rats suffering from both DM and periodontitis;
however, no decrease in bone loss was observed in rats with
periodontitis alone. Oral local melatonin application was found to
delay bone loss during periodontitis in patients with DM by
downregulating pro-inflammatory factors (137,138).
There is a clear association between periodontitis
and obesity. The prevalence of periodontitis and degree of
inflammation in obese or overweight patients seem to be higher
compared to individuals with normal weight (139,140). An experimental study reported
that, when the two diseases coexisted, a significant elevation was
observed in periodontal destruction, lipid dysbolism, glucose
levels and hepatic damage parameters, thus revealing comorbidity
effects (141). These
comorbidity effects may be associated with the circadian clock
(142). Considered as an
important modulator of the circadian clock, melatonin may be a key
mechanism in this comorbidity effect (11,143).
Reduced levels of melatonin have been found to be
associated with obesity (144).
On the other hand, patients with periodontitis, and aggressive
periodontitis in particular, are likely to have significantly lower
levels of melatonin in saliva and gingival crevicular fluid
(120,123). Melatonin supplementation helps
restore lipid and glucose metabolism, reduce pro-inflammatory
factor expression, improve body weight control and avoid
obesity-related complications in obese patients (144-146). Rats with obesity or
periodontitis have been shown to exhibited significantly lower
circulating melatonin levels, although these levels are further
reduced in rats with both obesity and periodontitis (147). In addition, a markedly
increased destruction of periodontal tissue was observed in rats
suffering from both obesity and periodontitis, with evident
inflammatory infiltration and osteoclastic activity (147). There were almost significant
negative associations between circulating melatonin levels and
periodontal pocket depth, dental plaque index and modified gingival
index (147). Combined therapy
with SRP and melatonin supplementation significantly reduced
alveolar bone destruction and pro-inflammatory cytokines in rats
with comorbidities of obesity and periodontitis, providing a
protective effect (148). When
periodontitis, pinealectomy, or a combination of both are present,
the TNF and insulin concentration, as well as the homeostasis model
assessment of insulin resistance index, are increased, indicating
insulin resistance (149).
Pineal excision can also lead to lipid profile dysregulation, which
may be improved to a similar degree to the control group by
melatonin alternative therapy, indicating that alternative
melatonin therapy provides a therapeutic effect against
dyslipidemia (149).
Periodontal ligament cells can secrete various
cytokines to modulate and maintain the homeostasis of periodontal
tissues, thereby playing an arrestive role in alveolar bone
metabolism (150). Periodontal
tissue regeneration can be enhanced by conditioned medium from
periodontal ligament stem cells in a concentration-dependent manner
by suppressing TNF-α production (151). There is an important balance
between cementum formation and bone loss during the maintenance of
periodontal health. Melatonin inhibited ethanol-induced ROS
production and senescence-like phenotypes in human periodontal
ligament stem cells and cementoblasts. In addition, it restored the
decreased osteoblastic/cementoblastic differentiation, and
increased osteoclastic differentiation through the protein never in
mitosis gene A interacting-1 pathway. Furthermore, the
downregulation of certain pathways, such as the MAPK, AMP-activated
protein kinase, mammalian target of rapamycin (mTOR) and nuclear
factor of activated T-cells c-1 pathways, has been suggested to
exert protective effects against ethanol-induced senescence
(152).
El-Sharkawy et al (153) reported that a daily dietary
supplement of 10 mg melatonin may be an effective complementary
treatment for patients with insomnia with generalized chronic
periodontitis, resulting in an improved CAL and sleep quality, as
well as lower PD and salivary TNF-α levels. During the entire study
period, the improvement in insomnia was maintained for up to 6
months without any rebound, even though the daily dietary melatonin
supplement was administered for only 2 months. As shown by previous
data, the level of systemic inflammatory markers in sleep disorders
increased significantly (154).
There may be a certain degree of bidirectional association between
sleep disorders and periodontal disease. Therefore, improving sleep
quality may itself improve the response to periodontal therapy
(Fig. 4). Evidence from relevant
human and animal studies on this matter are presented in Table IV.
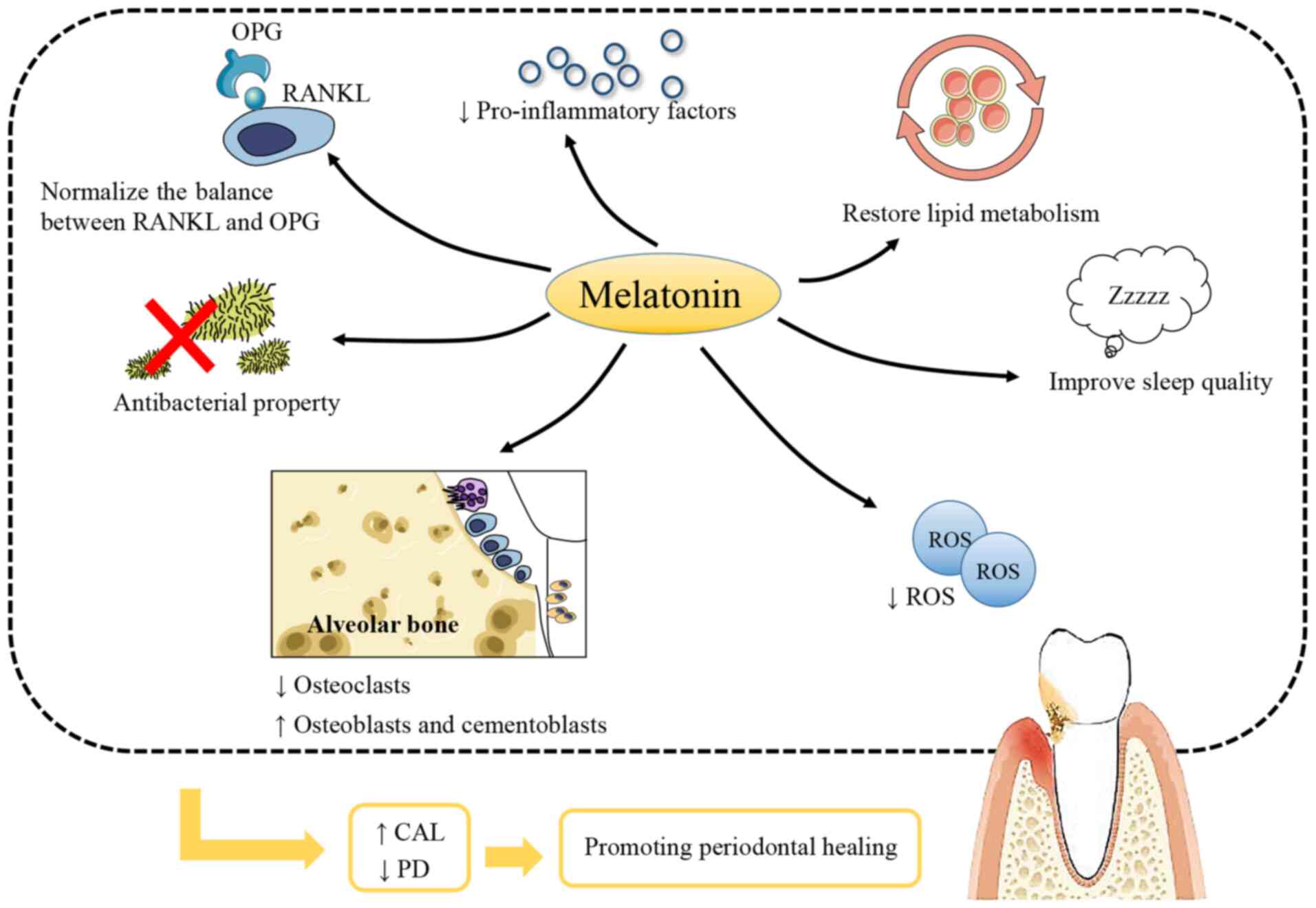 | Figure 4Melatonin promotes periodontal
healing. Melatonin is considered to have the properties of
antibiosis, regulating of the balance of RANKL and OPG, and
reducing pro-inflammatory factors and ROS production in periodontal
tissues. Melatonin cannot only reduce the number of osteoclasts and
increase that of osteoblasts in alveolar bone, but can also
increase that of cementoblasts. The ability of melatonin to restore
lipid metabolism is also beneficial to periodontal healing because
of the mutual promotion of obesity and periodontitis. In addition,
the improvement of sleep quality is helpful. On the whole,
melatonin application can effectively improve CAL and reduce PD,
further promote periodontal healing. RANKL, receptor activator of
NF-κB ligand; OPG, osteoprotegerin; ROS, reactive oxygen species;
CAL, clinical attachment level; PD, probing depth. |
| Table IVEvidence of the effects of melatonin
on periodontitis in animal and clinical studies. |
Table IV
Evidence of the effects of melatonin
on periodontitis in animal and clinical studies.
| Refs. | Objectives | Model | Route of
administration | Time of
administration | Frequency | Doses | Duration | Outcomes |
|---|
| 127 | Patients with
untreated severe periodontitis | With NSPT | Oral | After NSPT | Daily | 1 mg | 1 month | PD reduced even at
6 months |
| 128 | Patients with
chronic periodontitis | With NSPT | Oral | After NSPT | Daily | 2 mg | 4 weeks | Improved CAL and
lower PD in a long time as 3 and even 6 months |
| 129 | Patients with
chronic periodontitis and type 2 DM | With NSPT | Oral | 1 h before bed
time | Daily | 6 mg | 8 weeks | Improved CAL and
lower PD |
| 130 | Sprague-Dawley
rats | Periapical
lesions | i.p. | - | Daily | 10 mg/kg | 21 days | Reduced
radiological periapical bone loss |
| 131 | Wistar rats | Experimental
periodontitis | i.p. | 10:00-10:30 | Daily | 10, 50, 100
mg/kg | 14 and 28 days | Reduced
pro-inflammatory cytokine level and suppressed progression of
periodontitis |
| 136 | Wistar rats | Experimental DM and
periodontitis | i.p. | - | Daily | 10 mg/kg | 4 weeks | Inhibited
resorption of alveolar bone |
| 137 | Patients with
periodontal disease and DM | - | Topical
application | - | Daily | 1% orabase
cream | 20 days | Significant
decrease of the gingival index, PD and salivary levels of RANKL,
and significant rise of salivary OPG |
| 138 | Patients with
periodontal disease and DM | - | Topical
application | - | Daily | 1% orabase
cream | 21 days | Statistically
significant decrease of the gingival index, PD, and IL-1β, IL-6 and
prostaglandin E2 in gingival crevicular fluid |
| 148 | Wistar rats | Obesity and
periodontitis | Dissolved in
drinking water | - | Daily | 25
µg/ml | 4 weeks | Combined therapy of
SRP and melatonin supplement significantly reduced alveolar bone
destruction and proinflammatory cytokines |
| 149 | Wistar albino
rats | Pinealectomy and
periodontitis | Dissolved in
drinking water | 7:00 p.m. - 7:00
a.m. | Daily | 5 mg/kg | 28 days | Melatonin
efficiently prevented insulinresistance, improved lipid profile,
and increased plasma levels of insulin and TNF |
| 153 | Patients with
generalized chronic periodontitis and primary insomnia | With SRP | Oral | 1 h before bed
time | Daily | 10 mg | 2 months | Greater CAL and
sleep quality, lower PD and salivary TNF-α levels |
6. Differential effects of melatonin
administered at various concentrations and times
In the majority of previous studies, melatonin has
been found to play a positive role in bone tissue and bone-related
diseases. Melatonin supplementation in humans has a generally
favorable safety profile. Clinical studies have demonstrated that
the use of melatonin in the short-(days) and medium-term (weeks to
months) is safe, with only minor, transient adverse reactions
reported (155). In addition to
the most commonly reported adverse reactions, which are related to
fatigue, mood and psychomotor or neurocognitive performance, a few
studies have reported adverse events associated with endocrine and
cardiovascular function, as summarized in a critical systematic
review of clinical evidence (156). The safety of melatonin
application in pregnant and lactating women is unknown, due to the
lack of relevant research.
Although there is considerable evidence to suggest
that melatonin exerts a positive effect on bone health, certain
studies have reached different conclusions. Frisher et al
(157) reported an association
between melatonin and a significantly increased risk of fracture.
In addition, in that study, it was shown that the concentration and
administration time may impact the effects of melatonin treatment.
As shown in Tables I-IV, the usual strategy for animal
experiments is i.p. injection at doses between 10-50 mg/kg. A small
number of studies have used higher doses, such as 100 mg/kg
(15,66,131). The intra-articular injection is
a method commonly used in studies on OA, where the doses are lower
(0.1-0.2 µg) (82,88).
In addition, the normal dose used for subcutaneous injection is 10
mg/kg (95,112). A few studies have used other
methods, such as oral gavage (57), the addition of melatonin to
drinking water (59,148,149) and melatonin powder implantation
(13,33). Apart from one-off administration
(13,33), the shortest duration of melatonin
treatment was 3 days (42), and
the longest being up to 12 weeks (66). The majority of experiments used
melatonin for 2-4 weeks. For clinical research, the most common
route is by oral administration, with doses fluctuating between
1-10 mg/day (56,127-129,153). In addition, melatonin can be
used locally in the form of 1% orabase cream for the treatment of
periodontitis (137,138). The drug treatment durations
were ~1-2 months, and 6 months in one study (56).
To date, there is no consensus on the optimal
route, dosage and time of melatonin administration. Further
research is therefore required to explore the optimal route, dosage
and administration time of melatonin, and determine whether
long-term melatonin supplementation has any adverse effects, as
well as whether melatonin can be used as a daily adjuvant in
elderly, perimenopausal and postmenopausal women, and in patients
with periodontitis.
7. Conclusion and future prospects
Melatonin is a common molecule mainly produced by
the pineal gland. As an important regulatory factor of circadian
rhythm, melatonin has the ability to synchronize and maintain the
circadian clock in peripheral tissues with L/D cycles. In addition,
melatonin is also considered cytoprotective, due to its
anti-inflammatory, antitumor and antioxidant effects, and its
ability to regulate hormones, the immune system and tissue
regeneration.
Bone-related diseases have a high incidence, and
are associated with severe and persistent symptoms, a slow recovery
and a high impact on the lives of patients, as well as a heavy
economic burden. The most common treatment usually exerts a
curative effect and some side-effects. Since melatonin is
inexpensive, with a wide safety margin, has a wide impact on
tissues and almost no side-effects, the use of melatonin as a
supplementary treatment may be a potential therapeutic option for
bone disease (Fig. 5). As a
widely available and versatile molecule in vivo, melatonin
has potent antioxidant and anti-inflammatory properties in a
variety of bone diseases. In addition, melatonin also plays a vital
role in promoting osteogenesis and inhibiting osteoclastogenesis
(13,14). The promotion of vascularization
will also provide a good boost for bone repair (31). A close association has been
identified between cartilage and bone. Subchondral osteogenesis is
an important type of osteogenesis (21), and cartilage and bone metabolic
disorder is a common challenge in OA (72). Melatonin also protects and
promotes the differentiation of cartilage (77), which is important for bone
regeneration and bone development. Melatonin always drives MSCs to
differentiate toward osteoblasts (17-19) and chondroblasts (18,21,77) and protects MSCs from
disease-induced apoptosis (25,27,83). Patients with bone disease may
also have other chronic metabolic diseases, such as diabetes
(62,63,132-134), which have adverse effects on
bone health and lead to comorbidity effects. Despite these
comorbidity effects, melatonin can still have beneficial effects
(66,129,136), which provides a novel insight
for future multi-disease combination therapy.
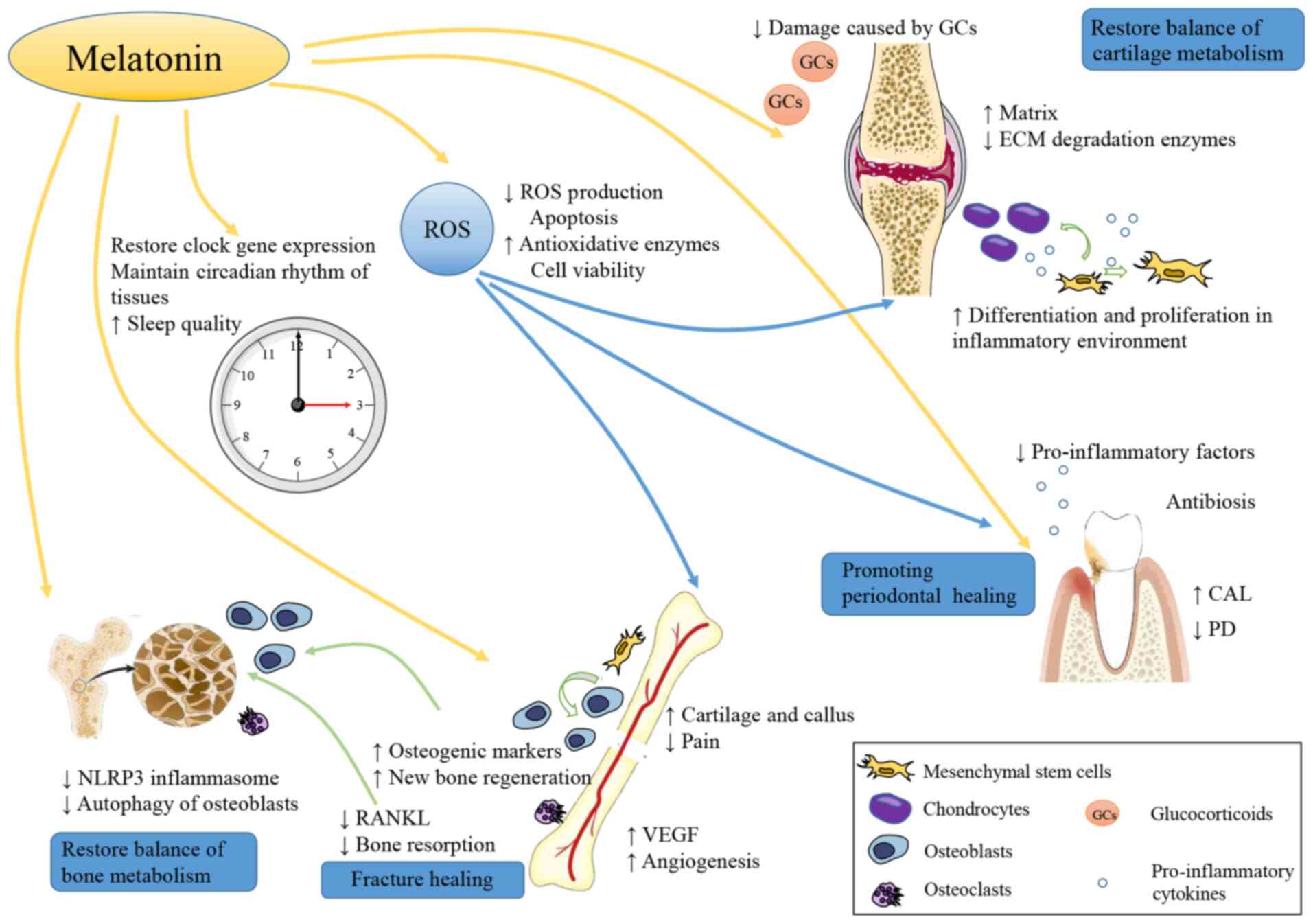 | Figure 5Roles of melatonin in bone tissue and
bone-related diseases. Melatonin plays an important role in bone
health. Melatonin promotes the proliferation, osteogenic and
chondrogenic differentiation of MSCs, accelerating cartilage and
bone formation. Moreover, melatonin inhibits osteoclasts production
and prevents bone loss. The level of ROS is significantly inhibited
by melatonin, which is associated with a decreased level of
oxidative stress. In particular, melatonin can increase VEGF and
promote angiopoiesis at the sites of bone injury, avoiding ischemic
injury. The melatonin properties of reducing the level of NLRP3
inflammasome helps restore bone metabolic balance. In patients with
DM, autophagy of osteoblasts is inhibited by melatonin and this
effect is participated in the protection of bone health in DM
patients. When used in OA, melatonin can reduce the adverse effects
of intra-articular GC injection. In addition, melatonin also has an
antibacterial effect on periodontitis bacteria. Metabolism of bone
and cartilage is closely associated with circadian rhythm. As an
important hormone regulating circadian rhythm, melatonin helps
restore the circadian rhythm and this also exerts a positive effect
on bone tissue and bone disease. MSCs, mesenchymal stem cells; ROS,
reactive oxygen species; NLRP3, nucleotide-binding domain and the
leucine-rich repeat pyrin 3 domain; VEGF, vascular endothelial
growth factor; DM, diabetes mellitus; OA, osteoarthritis; GC,
glucocorticoid. |
Stomatologists pay great attention to the
protection of periodontal tissue. The protective effects of
melatonin on periodontal tissue are significant, helping patients
with periodontitis retain more alveolar bone, providing more
possibilities for natural tooth retention and subsequent tooth
defect repair. In addition, the protective effects of melatonin on
alveolar bone can also accelerate the process of osteointegration
during implant restoration, to obtain a better implantation effect
(158). Melatonin can be used
to inhibit the enhancement of oxidative stress in oral tissues in
the period immediately following tooth extraction to avoid
excessive alveolar bone loss (159).
Human tissues are regulated by a circadian rhythm.
In particular, bone metabolism is closely associated with the
circadian rhythm, including the development, repair and remodeling
of bone tissue; cartilage metabolism is also regulated in a similar
manner (160-162). The disruption of the circadian
rhythm leads to a series of adverse effects. As an important
hormone regulating the circadian rhythm, melatonin helps restore
the circadian rhythm (143).
Sleep disorders and depression are also common symptoms among the
elderly (163) and
perimenopausal women (164).
Melatonin can improve the sleep quality and mental health of
patients, thus improving patient compliance; thus, the efficacy of
melatonin treatment can be further consolidated.
In conclusion, melatonin functions as a protector
in bone injury, osteoporosis, OA and periodontitis by exerting
multiple effects. Melatonin supplementation in humans has a
generally favorable safety profile. Due to the protective effects
of melatonin, as well as its low price and high safety, exploring
melatonin as a supplement to bone tissue and bone-related disease
therapy is worthwhile. However, since a few studies have reported
adverse effects, and there is no consensus on the optimal program
of melatonin administration, further research is required to
explore the optimal administration conditions and safety of
long-term melatonin supplementation.
Availability of data and materials
Not applicable.
Authors' contributions
XL was involved in data curation, investigation and
visualization, and in the writing of the original draft. SY was
involved in the conceptualization of the study, as well as in the
preparation of the figures, writing of the original draft, and in
the writing, reviewing and editing of the manuscript. GC, WZ, JP
and XH were involved in in the writing, reviewing and editing of
the present review article. LC was involved in the
conceptualization of the study, as well as in funding acquisition,
project administration, study supervision, and in the writing,
reviewing and editing of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
Not applicable.
Funding
The present study was supported by the National Natural Science
Foundation of China for Distinguished Young Scholars (grant no.
31725011 to LC).
Abbreviations:
|
ALP
|
alkaline phosphatase
|
|
CAL
|
clinical attachment level
|
|
DM
|
diabetes mellitus
|
|
ECM
|
extracellular matrix
|
|
GC
|
glucocorticoid
|
|
i.p. injection
|
intraperitoneal injection
|
|
L/D
|
light/dark
|
|
MSCs
|
mesenchymal stem cells
|
|
MTNR1A
|
melatonin receptor 1A
|
|
NSPT
|
nonsurgical periodontal therapy
|
|
OA
|
osteoarthritis
|
|
OCN
|
osteocalcin
|
|
OPG
|
osteoprotegerin
|
|
PD
|
probing depth
|
|
RANKL
|
receptor activator of NF-κB
ligand
|
|
ROS
|
reactive oxygen species, SRP, scaling
and root planning
|
|
TGF
|
transforming growth factor
|
|
TNF
|
tumor necrosis factor
|
|
VEGF
|
vascular endothelial growth
factor
|
References
|
1
|
Maria S and Witt-Enderby PA: Melatonin
effects on bone: Potential use for the prevention and treatment for
osteopenia, osteoporosis, and periodontal disease and for use in
bone-grafting procedures. J Pineal Res. 56:115–125. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Johnell O and Kanis JA: An estimate of the
worldwide prevalence and disability associated with osteoporotic
fractures. Osteoporos Int. 17:1726–1733. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kanis JA: Diagnosis of osteoporosis and
assessment of fracture risk. Lancet. 359:1929–1936. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Meng X, Li Y, Li S, Zhou Y, Gan RY, Xu DP
and Li HB: Dietary sources and bioactivities of melatonin.
Nutrients. 9:3672017. View Article : Google Scholar :
|
|
5
|
Cipolla-Neto J and Amaral FGD: Melatonin
as a hormone: New physiological and clinical insights. Endocr Rev.
39:990–1028. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Reiter RJ: Pineal melatonin: Cell biology
of its synthesis and of its physiological interactions. Endocr Rev.
12:151–180. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Amaral FGD and Cipolla-Neto J: A brief
review about melatonin, a pineal hormone. Arch Endocrinol Metab.
62:472–479. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Simonneaux V and Ribelayga C: Generation
of the melatonin endocrine message in mammals: A review of the
complex regulation of melatonin synthesis by norepinephrine,
peptides, and other pineal transmitters. Pharmacol Rev. 55:325–395.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tan DX, Manchester LC, Hardeland R,
Lopez-Burillo S, Mayo JC, Sainz RM and Reiter RJ: Melatonin: A
hormone, a tissue factor, an autocoid, a paracoid, and an
antioxidant vitamin. J Pineal Res. 34:75–78. 2003. View Article : Google Scholar
|
|
10
|
Permuy M, López-Peña M,
González-Cantalapiedra A and Muñoz F: Melatonin: A review of its
potential functions and effects on dental diseases. Int J Mol Sci.
18:8652017. View Article : Google Scholar :
|
|
11
|
Tordjman S, Chokron S, Delorme R, Charrier
A, Bellissant E, Jaafari N and Fougerou C: Melatonin: Pharmacology,
functions and therapeutic benefits. Curr Neuropharmacol.
15:434–443. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nauth A, Schemitsch E, Norris B, Nollin Z
and Watson JT: Critical-size bone defects: Is there a consensus for
diagnosis and treatment? J Orthop Trauma. 32(Suppl 1): S7–S11.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shino H, Hasuike A, Arai Y, Honda M,
Isokawa K and Sato S: Melatonin enhances vertical bone augmentation
in rat calvaria secluded spaces. Med Oral Patol Oral Cir Bucal.
21:e122–e126. 2016. View Article : Google Scholar :
|
|
14
|
Histing T, Anton C, Scheuer C, Garcia P,
Holstein JH, Klein M, Matthys R, Pohlemann T and Menger MD:
Melatonin impairs fracture healing by suppressing RANKL-mediated
bone remodeling. J Surg Res. 173:83–90. 2012. View Article : Google Scholar
|
|
15
|
Satomura K, Tobiume S, Tokuyama R,
Yamasaki Y, Kudoh K, Maeda E and Nagayama M: Melatonin at
pharmacological doses enhances human osteoblastic differentiation
in vitro and promotes mouse cortical bone formation in vivo. J
Pineal Res. 42:231–239. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sethi S, Radio NM, Kotlarczyk MP, Chen CT,
Wei YH, Jockers R and Witt-Enderby PA: Determination of the minimal
melatonin exposure required to induce osteoblast differentiation
from human mesenchymal stem cells and these effects on downstream
signaling pathways. J Pineal Res. 49:222–238. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dong P, Gu X, Zhu G, Li M, Ma B and Zi Y:
Melatonin induces osteoblastic differentiation of mesenchymal stem
cells and promotes fracture healing in a rat model of femoral
fracture via neuropeptide Y/neuropeptide Y receptor Y1 signaling.
Pharmacology. 102:272–280. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Luchetti F, Canonico B, Bartolini D,
Arcangeletti M, Ciffolilli S, Murdolo G, Piroddi M, Papa S, Reiter
RJ and Galli F: Melatonin regulates mesenchymal stem cell
differentiation: A review. J Pineal Res. 56:382–397. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhu G, Ma B, Dong P, Shang J, Gu X and Zi
Y: Melatonin promotes osteoblastic differentiation and regulates
PDGF/AKT signaling pathway. Cell Biol Int. 44:402–411. 2020.
View Article : Google Scholar
|
|
20
|
Park KH, Kang JW, Lee EM, Kim JS, Rhee YH,
Kim M, Jeong SJ, Park YG and Kim SH: Melatonin promotes
osteoblastic differentiation through the BMP/ERK/Wnt signaling
pathways. J Pineal Res. 51:187–194. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gao W, Lin M, Liang A, Zhang L, Chen C,
Liang G, Xu C, Peng Y, Chen C, Huang D and Su P: Melatonin enhances
chondrogenic differentiation of human mesenchymal stem cells. J
Pineal Res. 56:62–70. 2014. View Article : Google Scholar
|
|
22
|
Zhang B, Bailey WM, McVicar AL and Gensel
JC: Age increases reactive oxygen species production in macrophages
and potentiates oxidative damage after spinal cord injury.
Neurobiol Aging. 47:157–167. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fraser JH, Helfrich MH, Wallace HM and
Ralston SH: Hydrogen peroxide, but not superoxide, stimulates bone
resorption in mouse calvariae. Bone. 19:223–226. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee NK, Choi YG, Baik JY, Han SY, Jeong
DW, Bae YS, Kim N and Lee SY: A crucial role for reactive oxygen
species in RANKL-induced osteoclast differentiation. Blood.
106:852–859. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu X, Gong Y, Xiong K, Ye Y, Xiong Y,
Zhuang Z, Luo Y, Jiang Q and He F: Melatonin mediates protective
effects on inflammatory response induced by interleukin-1 beta in
human mesenchymal stem cells. J Pineal Res. 55:14–25. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu XW, Zi Y, Liu YE, Zhang YB, Xiang LB
and Hou MX: Melatonin exerts protective effect on N2a cells under
hypoxia conditions through Zip1/ERK pathway. Neurosci Lett.
595:74–80. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Xu S, Yang Y, Han S and Wu Z: ZIP1 and
zinc inhibits fluoride-induced apoptosis in MC3T3-E1 cells. Biol
Trace Elem Res. 159:399–409. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Halıcı M, Öner M, Güney A, Canöz Ö, Narin
F and Halıcı C: Melatonin promotes fracture healing in the rat
model. Eklem Hastalik Cerrahisi. 21:172–177. 2010.
|
|
29
|
Quesnelle KM, Bystrom PV and
Toledo-Pereyra LH: Molecular responses to ischemia and reperfusion
in the liver. Arch Toxicol. 89:651–657. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bagheri F, Khori V, Alizadeh AM,
Khalighfard S, Khodayari S and Khodayari H: Reactive oxygen
species-mediated cardiac-reperfusion injury: Mechanisms and
therapies. Life Sci. 165:43–55. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Erdem M, Gulabi D, Asci M, Bostan B, Gunes
T and Koseoglu RD: The effects of melatonin and caffeic acid
phenethyl ester (CAPE) on fracture healing under ischemic
conditions. Acta Orthop Traumatol Turc. 48:339–345. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Son JH, Cho YC, Sung IY, Kim IR, Park BS
and Kim YD: Melatonin promotes osteoblast differentiation and
mineralization of MC3T3-E1 cells under hypoxic conditions through
activation of PKD/p38 pathways. J Pineal Res. 57:385–392. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ramírez-Fernández MP, Calvo-Guirado JL,
de-Val JE, Delgado-Ruiz RA, Negri B, Pardo-Zamora G, Peñarrocha D,
Barona C, Granero JM and Alcaraz-Baños M: Melatonin promotes
angiogenesis during repair of bone defects: A radiological and
histomorphometric study in rabbit tibiae. Clin Oral Investig.
17:147–158. 2013. View Article : Google Scholar
|
|
34
|
Melincovici CS, Boşca AB, Şuşman S,
Mărginean M, Mihu C, Istrate M, Moldovan IM, Roman AL and Mihu CM:
Vascular endothelial growth factor (VEGF)-key factor in normal and
pathological angiogenesis. Rom J Morphol Embryol. 59:455–467.
2018.
|
|
35
|
Pugazhenthi K, Kapoor M, Clarkson AN, Hall
I and Appleton I: Melatonin accelerates the process of wound repair
in full-thickness incisional wounds. J Pineal Res. 44:387–396.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yildirimturk S, Batu S, Alatli C, Olgac V,
Firat D and Sirin Y: The effects of supplemental melatonin
administration on the healing of bone defects in
streptozotocin-induced diabetic rats. J Appl Oral Sci. 24:239–249.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
de Carvalho Nogueira EF, de Oliveira
Vasconcelos R, Teixeira Correia SS, Souza Catunda I, Amorim JA and
do Egito Cavalcanti Vasconcelos B: Is there a benefit to the use of
melatonin in preoperative zygomatic fractures? J Oral Maxillofac
Surg. 77:2017.e1–2017.e7. 2019. View Article : Google Scholar
|
|
38
|
Al-Aama T, Brymer C, Gutmanis I,
Woolmore-Goodwin SM, Esbaugh J and Dasgupta M: Melatonin decreases
delirium in elderly patients: A randomized, placebo-controlled
trial. Int J Geriatr Psychiatry. 26:687–694. 2011. View Article : Google Scholar
|
|
39
|
Sultan SS: Assessment of role of
perioperative melatonin in prevention and treatment of
postoperative delirium after hip arthroplasty under spinal
anesthesia in the elderly. Saudi J Anaesth. 4:169–173. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
de Jonghe A, van Munster BC, Goslings JC,
Kloen P, van Rees C, Wolvius R, van Velde R, Levi M, de Haan RJ and
de Rooij SE; Amsterdam Delirium Study Group: Effect of melatonin on
incidence of delirium among patients with hip fracture: A
multicentre, double-blind randomized controlled trial. CMAJ.
186:E547–E556. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Majidinia M, Reiter RJ, Shakouri SK,
Mohebbi I, Rastegar M, Kaviani M, Darband SG, Jahanban-Esfahlan R,
Nabavi SM and Yousefi B: The multiple functions of melatonin in
regenerative medicine. Ageing Res Rev. 45:33–52. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Topkan E, Tufan H, Yavuz AA, Bacanli D,
Onal C, Kosdak S and Yavuz MN: Comparison of the protective effects
of melatonin and amifostine on radiation-induced epiphyseal injury.
Int J Radiat Biol. 84:796–802. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Rachner TD, Khosla S and Hofbauer LC:
Osteoporosis: Now and the future. Lancet. 377:1276–1287. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Cipriani C, Pepe J, Bertoldo F, Bianchi G,
Cantatore FP, Corrado A, Di Stefano M, Frediani B, Gatti D,
Giustina A, et al: The epidemiology of osteoporosis in Italian
postmenopausal women according to the National Bone Health Alliance
(NBHA) diagnostic criteria: A multicenter cohort study. J
Endocrinol Invest. 41:431–438. 2018. View Article : Google Scholar
|
|
45
|
Parizad N, Baghi V, Karimi EB and Ghanei
Gheshlagh R: The prevalence of osteoporosis among Iranian
postmenopausal women with type 2 diabetes: A systematic review and
meta-analysis. Diabetes Metab Syndr. 13:2607–2612. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Melton LJ III: The prevalence of
osteoporosis: Gender and racial comparison. Calcif Tissue Int.
69:179–181. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Coughlan T and Dockery F: Osteoporosis and
fracture risk in older people. Clin Med (Lond). 14:187–191. 2014.
View Article : Google Scholar
|
|
48
|
Liu GF, Wang ZQ, Liu L, Zhang BT, Miao YY
and Yu SN: A network meta-analysis on the short-term efficacy and
adverse events of different anti-osteoporosis drugs for the
treatment of postmenopausal osteoporosis. J Cell Biochem.
119:4469–4481. 2018. View Article : Google Scholar
|
|
49
|
Cui Z, Meng X, Feng H, Zhuang S, Liu Z,
Zhu T, Ye K, Xing Y, Sun C, Zhou F and Tian Y: Estimation and
projection about the standardized prevalence of osteoporosis in
mainland China. Arch Osteoporos. 15:22019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Lane NE: Epidemiology, etiology, and
diagnosis of osteoporosis. Am J Obstet Gynecol. 194(2 Suppl):
S3–S11. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Mohd-Tahir NA and Li SC: Economic burden
of osteoporosis-related hip fracture in Asia: A systematic review.
Osteoporos Int. 28:2035–2044. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Hopkins RB, Burke N, Von Keyserlingk C,
Leslie WD, Morin SN, Adachi JD, Papaioannou A, Bessette L, Brown
JP, Pericleous L and Tarride J: The current economic burden of
illness of osteoporosis in Canada. Osteoporos Int. 27:3023–3032.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Egermann M, Gerhardt C, Barth A, Maestroni
GJ, Schneider E and Alini M: Pinealectomy affects bone mineral
density and structure-an experimental study in sheep. BMC
Musculoskelet Disord. 12:2712011. View Article : Google Scholar
|
|
54
|
Pines A: Circadian rhythm and menopause.
Climacteric. 19:551–552. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Sack RL, Lewy AJ, Erb DL, Vollmer WM and
Singer CM: Human melatonin production decreases with age. J Pineal
Res. 3:379–388. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kotlarczyk MP, Lassila HC, O'Neil CK,
D'Amico F, Enderby LT, Witt-Enderby PA and Balk JL: Melatonin
osteoporosis prevention study (MOPS): A randomized, double-blind,
placebo-controlled study examining the effects of melatonin on bone
health and quality of life in perimenopausal women. J Pineal Res.
52:414–426. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Sharan K, Lewis K, Furukawa T and Yadav
VK: Regulation of bone mass through pineal-derived melatonin-MT2
receptor pathway. J Pineal Res. 63. pp. e124232017, View Article : Google Scholar
|
|
58
|
Bao T, Zeng L, Yang K, Li Y, Ren F, Zhang
Y and Gao Z: Can melatonin improve the osteopenia of perimenopausal
and postmenopausal women? A meta-analysis. Int J Endocrinol.
2019:51516782019. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Tresguerres IF, Tamimi F, Eimar H,
Barralet JE, Prieto S, Torres J, Calvo-Guirado JL and Tresguerres
JA: Melatonin dietary supplement as an anti-aging therapy for
age-related bone loss. Rejuvenation Res. 17:341–346. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Xu Y, Sheng H, Bao Q, Wang Y, Lu J and Ni
X: NLRP3 inflammasome activation mediates estrogen
deficiency-induced depression- and anxiety-like behavior and
hippocampal inflammation in mice. Brain Behav Immun. 56:175–186.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Xu L, Zhang L, Wang Z, Li C, Li S, Li L,
Fan Q and Zheng L: Melatonin suppresses estrogen deficiency-induced
osteoporosis and promotes osteoblastogenesis by inactivating the
NLRP3 inflammasome. Calcif Tissue Int. 103:400–410. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Si Y, Wang C, Guo Y, Xu G and Ma Y:
Prevalence of osteoporosis in patients with type 2 diabetes
mellitus in the Chinese mainland: A systematic review and
meta-analysis. Iran J Public Health. 48:1203–1214. 2019.PubMed/NCBI
|
|
63
|
Paschou SA, Dede AD, Anagnostis PG,
Vryonidou A, Morganstein D and Goulis DG: Type 2 diabetes and
osteoporosis: A guide to optimal management. J Clin Endocrinol
Metab. 102:3621–3634. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Lecka-Czernik B: Diabetes, bone and
glucose-lowering agents: Basic biology. Diabetologia. 60:1163–1169.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Meng HZ, Zhang WL, Liu F and Yang MW:
Advanced glycation end products affect osteoblast proliferation and
function by modulating autophagy via the receptor of advanced
glycation end products/raf protein/mitogen-activated protein
kinase/extracellular signal-regulated kinase kinase/extracellular
signal-regulated kinase (RAGE/Raf/MEK/ERK) pathway. J Biol Chem.
290:28189–28199. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Zhang WL, Meng HZ, Yang RF, Yang MW, Sun
GH, Liu JH, Shi PX, Liu F and Yang B: Melatonin suppresses
autophagy in type 2 diabetic osteoporosis. Oncotarget.
7:52179–52194. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Ghareghani M, Scavo L, Arnoult D, Zibara K
and Farhadi N: Melatonin therapy reduces the risk of osteoporosis
and normalizes bone formation in multiple sclerosis. Fundam Clin
Pharmacol. 32:181–187. 2018. View Article : Google Scholar
|
|
68
|
Witt-Enderby PA, Radio NM, Doctor JS and
Davis VL: Therapeutic treatments potentially mediated by melatonin
receptors: Potential clinical uses in the prevention of
osteoporosis, cancer and as an adjuvant therapy. J Pineal Res.
41:297–305. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
March L, Smith EU, Hoy DG, Cross MJ,
Sanchez-Riera L, Blyth F, Buchbinder R, Vos T and Woolf AD: Burden
of disability due to musculoskeletal (MSK) disorders. Best Pract
Res Clin Rheumatol. 28:353–366. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Neogi T and Zhang Y: Epidemiology of
osteoarthritis. Rheum Dis Clin North Am. 39:1–19. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Thomas AC, Hubbard-Turner T, Wikstrom EA
and Palmieri-Smith RM: Epidemiology of Posttraumatic
Osteoarthritis. J Athl Train. 52:491–496. 2017. View Article : Google Scholar :
|
|
72
|
Vina ER and Kwoh CK: Epidemiology of
osteoarthritis: Literature update. Curr Opin Rheumatol. 30:160–167.
2018. View Article : Google Scholar :
|
|
73
|
Gentili C and Cancedda R: Cartilage and
bone extracellular matrix. Curr Pharm Des. 15:1334–1348. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Mobasheri A, Rayman MP, Gualillo O, Sellam
J, van der Kraan P and Fearon U: The role of metabolism in the
pathogenesis of osteoarthritis. Nat Rev Rheumatol. 13:302–311.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Buckwalter JA, Anderson DD, Brown TD,
Tochigi Y and Martin JA: The roles of mechanical stresses in the
pathogenesis of osteoarthritis: Implications for treatment of joint
injuries. Cartilage. 4:286–294. 2013. View Article : Google Scholar
|
|
76
|
Kapoor M, Martel-Pelletier J, Lajeunesse
D, Pelletier JP and Fahmi H: Role of proinflammatory cytokines in
the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 7:33–42.
2011. View Article : Google Scholar
|
|
77
|
Gao B, Gao W, Wu Z, Zhou T, Qiu X, Wang X,
Lian C, Peng Y, Liang A, Qiu J, et al: Melatonin rescued
interleukin 1β-impaired chondrogenesis of human mesenchymal stem
cells. Stem Cell Res Ther. 9:1622018. View Article : Google Scholar
|
|
78
|
Taruc-Uy RL and Lynch SA: Diagnosis and
treatment of osteoarthritis. Prim Care. 40:821–836. vii2013.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Hainque B, Dominice J, Jaffray P, Ronot X
and Adolphe M: Effects of dexamethasone on the growth of cultured
rabbit articular chondrocytes: Relation with the nuclear
glucocorticoid-receptor complex. Ann Rheum Dis. 46:146–152. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Robinson WH, Lepus CM, Wang Q, Raghu H,
Mao R, Lindstrom TM and Sokolove J: Low-grade inflammation as a key
mediator of the pathogenesis of osteoarthritis. Nat Rev Rheumatol.
12:580–592. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Liu-Bryan R and Terkeltaub R: Emerging
regulators of the inflammatory process in osteoarthritis. Nat Rev
Rheumatol. 11:35–44. 2015. View Article : Google Scholar :
|
|
82
|
Zhang Y, Lin J, Zhou X, Chen X, Chen AC,
Pi B, Pan G, Pei M, Yang H, Liu T and He F: Melatonin prevents
osteoarthritis-induced cartilage degradation via targeting
MicroRNA-140. Oxid Med Cell Longev. 2019:97059292019. View Article : Google Scholar
|
|
83
|
Hosseinzadeh A, Kamrava SK, Joghataei MT,
Darabi R, Shakeri-Zadeh A, Shahriari M, Reiter RJ, Ghaznavi H and
Mehrzadi S: Apoptosis signaling pathways in osteoarthritis and
possible protective role of melatonin. J Pineal Res. 61:411–425.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Milam SB, Zardeneta G and Schmitz JP:
Oxidative stress and degenerative temporomandibular joint disease:
A proposed hypothesis. J Oral Maxillofac Surg. 56:214–223. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Bolduc JA, Collins JA and Loeser RF:
Reactive oxygen species, aging and articular cartilage homeostasis.
Free Radic Biol Med. 132:73–82. 2019. View Article : Google Scholar :
|
|
86
|
Bakker AD, Silva VC, Krishnan R, Bacabac
RG, Blaauboer ME, Lin YC, Marcantonio RA, Cirelli JA and
Klein-Nulend J: Tumor necrosis factor alpha and interleukin-1beta
modulate calcium and nitric oxide signaling in mechanically
stimulated osteocytes. Arthritis Rheum. 60:3336–3345. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Lim HD, Kim YS, Ko SH, Yoon IJ, Cho SG,
Chun YH, Choi BJ and Kim EC: Cytoprotective and anti-inflammatory
effects of melatonin in hydrogen peroxide-stimulated CHON-001 human
chondrocyte cell line and rabbit model of osteoarthritis via the
SIRT1 pathway. J Pineal Res. 53:225–237. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Guo JY, Li F, Wen YB, Cui HX, Guo ML,
Zhang L, Zhang YF, Guo YJ and Guo YX: Melatonin inhibits
Sirt1-dependent NAMPT and NFAT5 signaling in chondrocytes to
attenuate osteoarthritis. Oncotarget. 8:55967–55983. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Cuzzocrea S, Zingarelli B, Gilad E, Hake
P, Salzman AL and Szabó C: Protective effect of melatonin in
carrageenan-induced models of local inflammation: Relationship to
its inhibitory effect on nitric oxide production and its
peroxynitrite scavenging activity. J Pineal Res. 23:106–116. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Ozturk G, Coşkun S, Erbaş D and Hasanoglu
E: The effect of melatonin on liver superoxide dismutase activity,
serum nitrate and thyroid hormone levels. Jpn J Physiol.
50:149–153. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Hossain FM and Hong Y, Jin Y, Choi J and
Hong Y: Physiological and pathological role of circadian hormones
in osteoarthritis: Dose-dependent or time-dependent? J Clin Med.
8:14152019. View Article : Google Scholar :
|
|
92
|
Jahanban-Esfahlan R, Mehrzadi S, Reiter
RJ, Seidi K, Majidinia M, Baghi HB, Khatami N, Yousefi B and
Sadeghpour A: Melatonin in regulation of inflammatory pathways in
rheumatoid arthritis and osteoarthritis: Involvement of circadian
clock genes. Br J Pharmacol. 175:3230–3238. 2018. View Article : Google Scholar :
|
|
93
|
Rong J, Zhu M, Munro J, Cornish J,
McCarthy GM, Dalbeth N and Poulsen RC: Altered expression of the
core circadian clock component PERIOD2 contributes to
osteoarthritis-like changes in chondrocyte activity. Chronobiol
Int. 36:319–331. 2019. View Article : Google Scholar
|
|
94
|
Yang W, Kang X, Liu J, Li H, Ma Z, Jin X,
Qian Z, Xie T, Qin N, Feng D, et al: Clock gene Bmal1 modulates
human cartilage gene expression by crosstalk with Sirt1.
Endocrinology. 157:3096–3107. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Hong Y, Kim H, Lee S, Jin Y, Choi J, Lee
SR, Chang KT and Hong Y: Role of melatonin combined with exercise
as a switch-like regulator for circadian behavior in advanced
osteoarthritic knee. Oncotarget. 8:97633–97647. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Nugent M: MicroRNAs: Exploring new
horizons in osteoarthritis. Osteoarthritis Cartilage. 24:573–580.
2016. View Article : Google Scholar
|
|
97
|
Miyaki S and Asahara H: Macro view of
microRNA function in osteoarthritis. Nat Rev Rheumatol. 8:543–552.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Miyaki S, Sato T, Inoue A, Otsuki S, Ito
Y, Yokoyama S, Kato Y, Takemoto F, Nakasa T, Yamashita S, et al:
MicroRNA-140 plays dual roles in both cartilage development and
homeostasis. Genes Dev. 24:1173–1185. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Si HB, Zeng Y, Liu SY, Zhou ZK, Chen YN,
Cheng JQ, Lu YR and Shen B: Intra-articular injection of
microRNA-140 (miRNA-140) alleviates osteoarthritis (OA) progression
by modulating extracellular matrix (ECM) homeostasis in rats.
Osteoarthritis Cartilage. 25:1698–1707. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Miyaki S, Nakasa T, Otsuki S, Grogan SP,
Higashiyama R, Inoue A, Kato Y, Sato T, Lotz MK and Asahara H:
MicroRNA-140 is expressed in differentiated human articular
chondrocytes and modulates interleukin-1 responses. Arthritis
Rheum. 60:2723–2730. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Karlsen TA, de Souza GA, Ødegaard B,
Engebretsen L and Brinchmann JE: microRNA-140 inhibits inflammation
and stimulates chondrogenesis in a model of interleukin 1β-induced
osteoarthritis. Mol Ther Nucleic Acids. 5:e3732016. View Article : Google Scholar
|
|
102
|
Wu Z, Qiu X, Gao B, Lian C, Peng Y, Liang
A, Xu C, Gao W, Zhang L, Su P, et al: Melatonin-mediated
miR-526b-3p and miR-590-5p upregulation promotes chondrogenic
differentiation of human mesenchymal stem cells. J Pineal Res.
65:e124832018. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Jüni P, Hari R, Rutjes AW, Fischer R,
Silletta MG, Reichenbach S and da Costa BR: Intra-articular
corticosteroid for knee osteoarthritis. Cochrane Database Syst Rev.
pp. CD0053282015
|
|
104
|
McAlindon TE, LaValley MP, Harvey WF,
Price LL, Driban JB, Zhang M and Ward RJ: Effect of intra-articular
triamcinolone vs saline on knee cartilage volume and pain in
patients with knee osteoarthritis: A randomized clinical trial.
JAMA. 317:1967–1975. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Yang W, Kang X, Qin N, Li F, Jin X, Ma Z,
Qian Z and Wu S: Melatonin protects chondrocytes from impairment
induced by glucocorticoids via NAD+-dependent SIRT1.
Steroids. 126:24–29. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Garrido-Urbani S, Jaquet V and Imhof BA:
ROS and NADPH oxidase: Key regulators of tumor vascularisation. Med
Sci (Paris). 30:415–421. 2014.In French. View Article : Google Scholar
|
|
107
|
Ahn J, Kim SA, Kim KW, Oh JH and Kim SJ:
Optimization of TGF-β1-transduced chondrocytes for cartilage
regeneration in a 3D printed knee joint model. PLoS One.
14:e02176012019. View Article : Google Scholar
|
|
108
|
Verdier MP, Seité S, Guntzer K, Pujol JP
and Boumédiène K: Immunohistochemical analysis of transforming
growth factor beta isoforms and their receptors in human cartilage
from normal and osteoarthritic femoral heads. Rheumatol Int.
25:118–124. 2005. View Article : Google Scholar
|
|
109
|
Fang J, Xu L, Li Y and Zhao Z: Roles of
TGF-beta 1 signaling in the development of osteoarthritis. Histol
Histopathol. 31:1161–1167. 2016.PubMed/NCBI
|
|
110
|
Pei M, He F, Wei L and Rawson A: Melatonin
enhances cartilage matrix synthesis by porcine articular
chondrocytes. J Pineal Res. 46:181–187. 2009. View Article : Google Scholar
|
|
111
|
Maestroni GJ, Sulli A, Pizzorni C,
Villaggio B and Cutolo M: Melatonin in rheumatoid arthritis:
Synovial macrophages show melatonin receptors. Ann N Y Acad Sci.
966:271–275. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Hong Y, Kim H, Lee Y, Lee S, Kim K, Jin Y,
Lee SR, Chang KT and Hong Y: Salutary effects of melatonin combined
with treadmill exercise on cartilage damage. J Pineal Res.
57:53–66. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Osseni RA, Rat P, Bogdan A, Warnet JM and
Touitou Y: Evidence of prooxidant and antioxidant action of
melatonin on human liver cell line HepG2. Life Sci. 68:387–399.
2000. View Article : Google Scholar
|
|
114
|
Zhang HM and Zhang Y: Melatonin: A
well-documented anti-oxidant with conditional pro-oxidant actions.
J Pineal Res. 57:131–146. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Saito R, Muneta T, Ozeki N, Nakagawa Y,
Udo M, Yanagisawa K, Tsuji K, Tomita M, Koga H and Sekiya I:
Strenuous running exacerbates knee cartilage erosion induced by low
amount of mono-iodoacetate in rats. BMC Musculoskelet Disord.
18:362017. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Gustafsson A and Asman B: Increased
release of free oxygen radicals from peripheral neutrophils in
adult periodontitis after Fc delta-receptor stimulation. J Clin
Periodontol. 23:38–44. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Battino M, Bullon P, Wilson M and Newman
H: Oxidative injury and inflammatory periodontal diseases: The
challenge of anti-oxidants to free radicals and reactive oxygen
species. Crit Rev Oral Biol Med. 10:458–476. 1999. View Article : Google Scholar
|
|
118
|
Walters J and Lai PC: Should antibiotics
be prescribed to treat chronic periodontitis? Dent Clin North Am.
59:919–933. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Srinath R, Acharya AB and Thakur SL:
Salivary and gingival crevicular fluid melatonin in periodontal
health and disease. J Periodontol. 81:277–283. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Gómez-Moreno G, Cutando-Soriano A, Arana
C, Galindo P, Bolaños J, Acuña-Castroviejo D and Wang HL: Melatonin
expression in periodontal disease. J Periodontal Res. 42:536–540.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Laakso ML, Porkka-Heiskanen T, Alila A,
Stenberg D and Johansson G: Correlation between salivary and serum
melatonin: Dependence on serum melatonin levels. J Pineal Res.
9:39–50. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Madapusi BT and Rao SR: Preliminary
evaluation of human gingiva as an extrapineal site of melatonin
biosynthesis in states of periodontal health and disease. J Clin
Diagnostic Res. 12:ZF1–ZF7. 2018.
|
|
123
|
Ghallab NA, Hamdy E and Shaker OG:
Malondialdehyde, superoxide dismutase and melatonin levels in
gingival crevicular fluid of aggressive and chronic periodontitis
patients. Aust Dent J. 61:53–61. 2016. View Article : Google Scholar
|
|
124
|
Lodhi K, Saimbi CS, Khan MA, Nath C and
Shukla R: Evaluation of melatonin levels in saliva in gingivitis
and periodontitis cases: A pilot study. Contemp Clin Dent.
7:519–523. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Cutando A, Galindo P, Gómez-Moreno G,
Arana C, Bolaños J, Acuña-Castroviejo D and Wang HL: Relationship
between salivary melatonin and severity of periodontal disease. J
Periodontol. 77:1533–1538. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Almughrabi OM, Marzouk KM, Hasanato RM and
Shafik SS: Melatonin levels in periodontal health and disease. J
Periodont Res. 48:315–321. 2013. View Article : Google Scholar
|
|
127
|
Tinto M, Sartori M, Pizzi I, Verga A and
Longoni S: Melatonin as host modulating agent supporting
nonsurgical periodontal therapy in patients affected by untreated
severe periodontitis: A preliminary randomized, triple-blind,
placebo-controlled study. J Periodont Res. 55:61–67. 2020.
View Article : Google Scholar
|
|
128
|
Chitsazi M, Faramarzie M, Sadighi M,
Shirmohammadi A and Hashemzadeh A: Effects of adjective use of
melatonin and vitamin C in the treatment of chronic periodontitis:
A randomized clinical trial. J Dent Res Dent Clin Dent Prospects.
11:236–240. 2017.
|
|
129
|
Bazyar H, Gholinezhad H, Moradi L, Salehi
P, Abadi F, Ravanbakhsh M and Zare Javid A: The effects of
melatonin supplementation in adjunct with non-surgical periodontal
therapy on periodontal status, serum melatonin and inflammatory
markers in type 2 diabetes mellitus patients with chronic
periodontitis: A double-blind, placebo-controlled trial.
Inflammopharmacology. 27:67–76. 2019. View Article : Google Scholar
|
|
130
|
Sarıtekin E, Üreyen Kaya B, Aşcı H and
Özmen Ö: Anti-inflammatory and antiresorptive functions of
melatonin on experimentally induced periapical lesions. Int Endod
J. 52:1466–1478. 2019. View Article : Google Scholar
|
|
131
|
Renn TY, Huang YK, Feng SW, Wang HW, Lee
WF, Lin CT, Burnouf T, Chen LY, Kao PF and Chang HM: Prophylactic
supplement with melatonin successfully suppresses the pathogenesis
of periodontitis through normalizing RANKL/OPG ratio and depressing
the TLR4/MyD88 signaling pathway. J Pineal Res. 64:2018. View Article : Google Scholar
|
|
132
|
Botero JE, Yepes FL, Roldán N, Castrillón
CA, Hincapie JP, Ochoa SP, Ospina CA, Becerra MA, Jaramillo A,
Gutierrez SJ and Contreras A: Tooth and periodontal clinical
attachment loss are associated with hyperglycemia in patients with
diabetes. J Periodontol. 83:1245–1250. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Daniel R, Gokulanathan S, Shanmugasundaram
N, Lakshmigandhan M and Kavin T: Diabetes and periodontal disease.
J Pharm Bioallied Sci. 4(Suppl 2): S280–S282. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Grover HS and Luthra S: Molecular
mechanisms involved in the bidirectional relationship between
diabetes mellitus and periodontal disease. J Indian Soc
Periodontol. 17:292–301. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Abdolsamadi H, Goodarzi MT, Ahmadi
Motemayel F, Jazaeri M, Feradmal J, Zarabadi M, Hoseyni M and
Torkzaban P: Reduction of melatonin level in patients with type II
diabetes and periodontal diseases. J Dent Res Dent Clin Dent
Prospects. 8:160–165. 2014.PubMed/NCBI
|
|
136
|
Balci Yuce H, Karatas O, Aydemir Turkal H,
Pirim Gorgun E, Ocakli S, Benli I and Cayli S: The effect of
melatonin on bone loss, diabetic control, and apoptosis in rats
with diabetes with ligature-induced periodontitis. J Periodontol.
87:e35–e43. 2016. View Article : Google Scholar
|
|
137
|
Cutando A, López-Valverde A, de Diego RG,
de Vicente J, Reiter R, Fernández MH and Ferrera MJ: Effect of
topical application of melatonin to the gingiva on salivary
osteoprotegerin, RANKL and melatonin levels in patients with
diabetes and periodontal disease. Odontology. 102:290–296.
2014.
|
|
138
|
Montero J, López-Valverde N, Ferrera MJ
and López-Valverde A: Changes in crevicular cytokines after
application of melatonin in patients with periodontal disease. J
Clin Exp Dent. 9:e1081–e1087. 2017.PubMed/NCBI
|
|
139
|
Martens L, De Smet S, Yusof MY and
Rajasekharan S: Association between overweight/obesity and
periodontal disease in children and adolescents: A systematic
review and meta-analysis. Eur Arch Paediatr Dent. 18:69–82. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Keller A, Rohde JF, Raymond K and Heitmann
BL: Association between periodontal disease and overweight and
obesity: A systematic review. J Periodontol. 86:766–776. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Virto L, Cano P, Jiménez-Ortega V,
Fernández-Mateos P, González J, Esquifino AI and Sanz M: Obesity
and periodontitis: An experimental study to evaluate periodontal
and systemic effects of comorbidity. J Periodontol. 89:176–185.
2018.
|
|
142
|
Shimizu I, Yoshida Y and Minamino T: A
role for circadian clock in metabolic disease. Hypertens Res.
39:483–491. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Zisapel N: New perspectives on the role of
melatonin in human sleep, circadian rhythms and their regulation.
Br J Pharmacol. 175:3190–3199. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Szewczyk-Golec K, Woźniak A and Reiter RJ:
Inter-relationships of the chronobiotic, melatonin, with leptin and
adiponectin: Implications for obesity. J Pineal Res. 59:277–291.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Ríos-Lugo MJ, Cano P, Jiménez-Ortega V,
Fernández-Mateos MP, Scacchi PA, Cardinali DP and Esquifino AI:
Melatonin effect on plasma adiponectin, leptin, insulin, glucose,
triglycerides and cholesterol in normal and high fat-fed rats. J
Pineal Res. 49:342–348. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Favero G, Stacchiotti A, Castrezzati S,
Bonomini F, Albanese M, Rezzani R and Rodella LF: Melatonin reduces
obesity and restores adipokine patterns and metabolism in obese
(ob/ob) mice. Nutr Res. 35:891–900. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Virto L, Haugen HJ, Fernández-Mateos P,
Cano P, González J, Jiménez-Ortega V, Esquifino AI and Sanz M:
Melatonin expression in periodontitis and obesity: An experimental
in-vivo investigation. J Periodont Res. 53:825–831. 2018.
View Article : Google Scholar
|
|
148
|
Virto L, Cano P, Jiménez-Ortega V,
Fernández-Mateos P, González J, Haugen HJ, Esquifino AI and Sanz M:
Melatonin as adjunctive therapy in the treatment of periodontitis
associated with obesity. J Clin Periodontol. 45:1336–1346. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Santos RMD, Marani F, Chiba FY, Mattera
MSLC, Tsosura TVS, Tessarin GWL, Pereira RF, Belardi BE, Pinheiro
BCES and Sumida DH: Melatonin promotes reduction in TNF levels and
improves the lipid profile and insulin sensitivity in
pinealectomized rats with periodontal disease. Life Sci. 213:32–39.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Diomede F, Zingariello M, Cavalcanti MFXB,
Merciaro I, Pizzicannella J, De Isla N, Caputi S, Ballerini P and
Trubiani O: MyD88/ERK/NFkB pathways and pro-inflammatory cytokines
release in periodontal ligament stem cells stimulated by
Porphyromonas gingivalis. Eur J Histochem. 61:27912017.
|
|
151
|
Nagata M, Iwasaki K, Akazawa K, Komaki M,
Yokoyama N, Izumi Y and Morita I: Conditioned medium from
periodontal ligament stem cells enhances periodontal regeneration.
Tissue Eng Part A. 23:367–377. 2017. View Article : Google Scholar :
|
|
152
|
Bae WJ, Park JS, Kang SK, Kwon IK and Kim
EC: Effects of melatonin and its underlying mechanism on
ethanol-stimulated senescence and osteoclastic differentiation in
human periodontal ligament cells and cementoblasts. Int J Mol Sci.
19:17422018. View Article : Google Scholar :
|
|
153
|
El-Sharkawy H, Elmeadawy S, Elshinnawi U
and Anees M: Is dietary melatonin supplementation a viable
adjunctive therapy for chronic periodontitis?-A randomized
controlled clinical trial. J Periodont Res. 54:190–197. 2019.
View Article : Google Scholar
|
|
154
|
Irwin MR, Olmstead R and Carroll JE: Sleep
disturbance, sleep duration, and inflammation: A Systematic review
and meta-analysis of cohort studies and experimental sleep
deprivation. Biol Psychiatry. 80:40–52. 2016. View Article : Google Scholar
|
|
155
|
Andersen LP, Gögenur I, Rosenberg J and
Reiter RJ: The safety of melatonin in humans. Clin Drug Investig.
36:169–175. 2016. View Article : Google Scholar
|
|
156
|
Foley HM and Steel AE: Adverse events
associated with oral administration of melatonin: A critical
systematic review of clinical evidence. Complement Ther Med.
42:65–81. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
Frisher M, Gibbons N, Bashford J, Chapman
S and Weich S: Melatonin, hypnotics and their association with
fracture: A matched cohort study. Age Ageing. 45:801–806. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Sun T, Li J, Xing HL, Tao ZS and Yang M:
Melatonin improves the osseointegration of hydroxyapatite-coated
titanium implants in senile female rats. Z Gerontol Geriatr.
53:770–777. 2020. View Article : Google Scholar
|
|
159
|
Cutando A, Arana C, Gómez-Moreno G,
Escames G, López A, Ferrera MJ, Reiter RJ and Acuña-Castroviejo D:
Local application of melatonin into alveolar sockets of beagle dogs
reduces tooth removal-induced oxidative stress. J Periodontol.
78:576–583. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Swanson CM, Kohrt WM, Buxton OM, Everson
CA, Wright KP Jr, Orwoll ES and Shea SA: The importance of the
circadian system & sleep for bone health. Metabolism. 84:28–43.
2018. View Article : Google Scholar :
|
|
161
|
Wu QY, Wang J, Tong X, Chen J, Wang B,
Miao ZN, Li X, Ye JX and Yuan FL: Emerging role of circadian rhythm
in bone remodeling. J Mol Med (Berl). 97:19–24. 2019. View Article : Google Scholar
|
|
162
|
Yang N and Meng QJ: Circadian clocks in
articular cartilage and bone: A compass in the sea of matrices. J
Biol Rhythms. 31:415–427. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
163
|
Tian Y and Li LM: Epidemiological study of
sleep disorder in the elderly. Zhonghua Liu Xing Bing Xue Za Zhi.
38:988–992. 2017.In Chinese. PubMed/NCBI
|
|
164
|
Santoro N: Perimenopause: From research to
practice. J Womens Health (Larchmt). 25:332–339. 2016. View Article : Google Scholar
|