1. Introduction
The tear film is a thin layer of body fluid secreted
and produced by the meibomian gland, the main and accessory
lacrimal glands, as well as the goblet cells in the conjunctiva
(1). Tear fluid serves several
functions: i) Lubricating the ocular surface; ii) providing
nutrients to the corneal epithelium; iii) providing a moist and
smooth surface for good vision; and iv) protecting the eyes against
pathogens (2). The tear film is
comprised of three layers: i) The lipid layer; ii) the aqueous
layer; and ii) the innermost mucin layer with the aqueous and mucin
layers forming a homogeneous layer (3,4).
Altogether, it consists of proteins (including enzymes),
metabolites, electrolytes, lipids and glucose, and serves a
critical function in the ocular system (5). The total tear protein concentration
ranges from 3.5 to 9.5 mg/ml in basal tears and reflex tears, but
is higher in newborns, ranging from 11 to 13 mg/ml (6), and is increased in closed eye
conditions (6 to 18 mg/ml) (7).
It has been demonstrated that the proteins in the tear fluid play a
significant role in regulating inflammatory responses (8), wound healing (9) and antibacterial protection
(10). Mass spectrometry (MS)
proteomic analysis not only provides a comprehensive
characterization of tear fluid efficiently, but the multiplex
nature of acquisition may also provide insights into the key
mediators of biological responses and the status of the ocular
surface (11). The high
concentration of proteins and easy accessibility of tear fluid,
compared with other ocular fluids, have made tears a sought-after
target for proteomic studies in ophthalmology (12). However, the presence of abundant
proteins, including lactotransferrin (LTF), secretory IgA,
lipocalin-1 (LCN1) and lysozyme C (LYZ) detected using
electrophoresis techniques (13,14) and the small volume of tears has
hampered comprehensive protein analysis of low abundant proteins.
The advancement in nano-scale liquid chromatography coupled MS
(nanoLC-MS) that offers extended dynamic range and sensitivity to
identify >1,000 proteins, has opened up the possibility of tear
biomarker research (15). With
continued advances in techniques from sample preparation to MS
acquisition, it is anticipated that the tear fluid will serve as an
important matrix to develop molecular assays for ocular diseases
and ophthalmology overall using the MS approach. Quantitative
profiling and targeted MS methods have allowed multiplexed,
reproducible screening of hundreds to thousands of proteins in a
single, microliter volume (16)
of tear fluid samples in early discovery, clinical trials and
clinical proteomics application for the discovery of multifactorial
ocular diseases.
2. Collection of tear fluid for clinical
proteomics
Tear fluid can be obtained using several established
collection methods, yet different sampling methods are known to
affect the quality of tears samples and, consequently, the results
of tear proteome analysis (17).
The three most commonly adopted sampling methods for tear fluid are
cellulose sponges, Schirmer's strips and capillary tubes. These
sampling methods are non-invasive and do not require local
anesthesia.
Cellulose sponges
A cellulose sponge may be used for tear collection
by placing it into the lower conjunctival sac for ~1 min. It has
been commonly adopted due to its high effectiveness in collecting
tears, even from patients with low tear volume. This method is
non-irritating and is generally well-tolerated by patients
(18). Additionally, the sponge
sampling method enables the standardization of the tear collection
volume (19). Nevertheless, a
variety of sponges and extraction buffers have been used in
different studies, thus making it difficult to directly compare
their results (19,20). In addition, some cytokines,
including interleukins and g-interferon, bind tightly to the
sponge, making the recovery and extraction of these proteins more
difficult (21).
Schirmer's strips
Schirmer's strips are used in the Schirmer's test
for dry eye assessment (22).
The strip is placed in the inferior conjunctival sac and left in
place until it has been wetted to the control line. Later
incubation in buffer solution to rehydrate the strip allows
proteins or metabolites to be extracted for further molecular
tests. This technique yields higher recovery of interleukins
compared to samples collected with cellulose sponges (23) and improved protein identification
than from tear fluid collected with a capillary tube (24). Although Schirmer's strips have
been considered as a convenient and easy to perform method of tear
collection, their use can cause strong irritation, leading to
reflex tearing that results in unwanted dilution of tears (25). In addition, improper handling can
also affect protein content (26). In particular, estimation of the
tear protein loss during sample manipulation at the diffusion-based
protein extraction stage ranged from 2% (LYZ) to 41.2% (mucin 4)
(26).
Both the Schirmer's strip and cellulose sponge
methods make use of absorptive materials that have contact with the
conjunctiva, which can potentially damage the ocular surface. An
increase in the number of certain proteins due to mechanical trauma
of the conjunctiva has been reported (27,28). Hence, extra care should be taken
to minimize the trauma-induced stimulation of proteins during
sample collection.
Capillary tube
To overcome the aforementioned drawbacks of
absorptive materials, capillary tube or pipette sampling can be
employed. The tear fluid is drawn from the inferior temporal tear
meniscus near the external canthus of the eyes to a disposable
borosilicate glass microcapillary tube by simple capillary force
(29). Compared with the use of
absorptive materials, this method is considered to be less
invasive, to avoid reflex tearing, and to result in less protein
disruption during the sample recovery process (30). However, it is time-consuming and
requires precise handling, and may not be suitable for anxious or
uncooperative patients and children (19). Improper handling of capillary
tubes can induce reflex tears due to contact between the tube and
the conjunctiva. In general, capillary tubes sampling is not always
practicable and feasible in clinical studies that require
reproducible data from large cohorts, particularly when children
are involved (19). Furthermore,
the collectible sample volume is limited. To overcome the limited
tear volume of samples, pooling of tears from multiple subjects can
be useful in research, but is undesirable in clinical studies as
individual characteristics cannot be determined (31).
In brief, it is important to select the appropriate
collection method for each specific study. For example, when a
large sample volume is required, Schirmer's strips are preferable,
but if dry eye patients with low tear menisci are involved,
cellulose sponges are preferred (32,33). Notably, the results of proteomics
studies using different tear fluid collection methods are not
directly comparable, and it is important to consider the potential
impact of the collection method on protein concentration and
expression.
3. MS proteomics approaches
Proteins are the key functional entities in the cell
and arguably form the principle level of information required to
understand any cellular function (34). Proteome refers to the entire
protein complement expressed by the genome, while proteomics refers
to the global analysis of protein mixtures (or their polypeptide
components). Protein research and proteomics continue to develop
and have become increasingly sophisticated. Proteomics research was
initially qualitative, i.e., proteins were identified as being
present in samples, providing the foundation for future research,
but this alone was insufficient to characterize induced protein
regulations and pathological conditions. For these purposes,
proteomics analysis needed to be quantitative (35). Consequently, proteomic platforms
with quantitative measurement of protein expression and protein
post-translational modifications (PTMs) have been developed and
become an integral and indispensable part of current proteomic
studies (36). Discovery-based
proteomics is typically conducted with a comparatively small set of
samples to identify and quantify the differential expression of
proteins. These proteins can then be verified and validated with a
larger sample cohort to better account for biological variation,
specificity and clinical longitudinal changes in expression.
Data-dependent acquisition (DDA) was the first approach developed
to survey abundant peptide masses in an unknown mixture, in which
precursors were isolated and fragmented to generate a unique
fingerprint spectrum of amino acid sequences for peptide
identification in a high-resolution mass spectrometer. However, DDA
has poor quantitative performance, because of the bias towards
redundant proteins and poor reproducibility of signals and coverage
of low abundant proteins (37).
Data-independent acquisition (DIA) utilizes software-controlled
mass isolation windows across the chromatogram, providing superior
reproducibility and consistent acquisition ideal for quantitative
results (38). In particular,
the Sequential Window Acquisition of All Theoretical Mass Spectra
(SWATH-MS) extended the data analysis concept of a targeted
approach to achieve high-throughput DIA data extraction and
statistical validation. SWATH-MS is one of the first methods to
record all fragment ions of the detectable peptide precursors and
highly multiplexed fragment ion maps included with low abundant
peptides (39). DIA method,
which relies on a high-quality mass spectral library generated from
the DDA approach for peptide identification, remains the only
label-free quantification method to survey and quantify the
hundreds of thousands of proteins in complex biological samples
without the prior knowledge of fragment mass transitions and
peptide occurrences in the sample. Advances in proteomics were
required and went hand in hand with intensive progress in
computational interfaces, including databases, data processing
algorithms, decoy peptides, accurate protein identification and
data analysis of large proteome datasets (40). Isobaric tags for relative and
absolute quantitation (iTRAQ) and Tandem mass tag (TMT) are
isobaric labeling methods used in quantitative proteomics. These
methods are based on the covalent labeling of the peptide with
designated tags of reporter mass. Peptide samples are labeled and
then pooled for preparation. This labeled approach allows
multiplexed sampling and quantification of peptides that are ideal
for pilot studies, as demonstrated in the analysis of tears in dry
eye disease to quantify differential expressed proteins in a single
MS acquisition (41).
Phosphorylation and glycosylation are common PTMs of
proteins. A pilot study of phosphorylation enrichment using a
titanium dioxide (TiO2) column identified a total of 13
phosphoproteins in tear fluid, including mammaglobin-B (SCGB2A1),
clusterin and protein UNQ773. Of note, phosphoproteins LCN1,
immunoglobulin k constant (IGKC), polymeric immunoglobulin receptor
(PIGR), lacritin (LACRT), cystatin S (CST4), proline-rich protein 4
(PRR4), deleted in malignant brain tumors 1 protein (DMBT1),
immunoglobulin heavy constant a 1 (IGHA1), LYZ and immunoglobulin J
chain (IGJ) had differentially expressed protein levels in ocular
diseases, as described in a previously mentioned study (42). The use of PTMs as a biomarker in
ocular diseases is limited, despite the high abundance of
phosphoproteins reported in tear fluid (43). For example, glycosylation in the
proline-rich protein family, and LACRT can be identified without an
enrichment procedure (37).
Methylation and acylation were observed in LCN1 and LYZ, however
there was statistically significant difference of PTMs in dry eye
disease (44). A total of 50
N-linked glycans were identified in tears, five low abundance
N-glycans (m/z 864.4, 945.5, 994.9, 1039.0 and 1112.0) and one
O-glycan (m/z 665.2) were significantly different in patients with
diabetes or diabetic retinopathy (45).
4. Protein sample preparation for MS
One-dimensional and two-dimensional gel
electrophoreses (1DGE and 2DGE, respectively) were early proteomic
tools used to separate, visualize and determine the size of
proteins (46). MS was used to
identify spots of abundant proteins and relative quantification of
proteins. With this technique, proteins are separated according to
isoelectric points (pI) through isoelectric focusing (IEF). In
1974, LTF and LYZ were found to be the major protein constituents
in tear fluid (47). Using 1DGE,
scientists found serum albumin (ALB) and transferrin were
significantly elevated in the tear fluid of eyes even in mild cases
of acute catarrhal conjunctivitis (48). Using 2DGE, scientists found lower
abundance of proteins in human reflex tears, including CST4,
cystatin SN and α-2-glycoprotein, in addition to the previously
reported LTF and LYZ (49), in
particular, high expression of PRR4 in reflex tears (50). The fluorescence visualization of
proteins in GE improved sensitivity compared with traditional
Coomassie brilliant blue staining (51). However, irrespective of the
staining method used, GE has a limited resolution of complex
protein mixtures, low abundance proteins and co-appearing protein
isoforms. It is also incompatible with hydrophobic proteins, for
which it has limited access to various protein classes (52). Additionally, its limited dynamic
range has hampered proteomic analysis of biofluids, such as human
plasma, in which protein concentrations can differ up to 12 orders
of magnitude (53). Unicellular
organisms were used to benchmark 2DGE. However, detection of low
abundance proteins remained a problem in this paradigm, despite the
use of extended separation range and increased sample load, only
193 proteins were identified. This has demonstrated the limitations
of the technique in a relatively simple model, and led to the
conclusion that GE is not suitable for comprehensive global protein
detection and quantitative profiling of protein networks (54). One-dimensional-liquid
chromatography (1D-LC) offered a solution to the limitations of GE
and has become increasingly popular over the past decade. Compared
with GE-based proteomics, LC-based proteomics have improved
reproducibility, streamlined peptide separation, increased sample
throughput and dynamic range, and reduced sample consumption
(55). These advances enabled
the characterization of proteins in tissues (56), cells (57), plasma (58) and tears (59). The separation efficiency of LC is
dependent on peak capacity, i.e., the maximum number of proteins
that can be resolved in each separation time in a single sample
acquisition (60). In human
plasma, which has a particularly complex protein content, the
highest achievable peak capacity of LC was reported to be 1,500
(61). It was also reported that
the theoretical peak capacity of GE is three times lower than LC
methods, due to its confined and definite retention volume
(62). Consequentially, MS-based
targeted proteomics have been rapidly adopted for quantifying
proteins in complex clinical samples (63,64). MS-based approaches perform
particularly well with respect to assay sensitivity and
specificity, when testing biomarker panels, rather than individual
markers. Therefore, this technology has paved the way for
multiparametric diagnostics that can significantly increase
diagnostic accuracy (65).
Currently, the only Food and Drug Administration (FDA)-approved,
multi-parametric clinical test is designed to aid in the diagnosis
of ovarian cancer. This test, which uses five serum proteins
[CA125, transthyretin, apolipoprotein A-I, β2-microglobulin (B2M)
and transferrin], correctly predicted ovarian cancer in 94% of
cases, which was significantly improved compared with the 66% rate
observed with a single-parametric assay based on CA125 alone
(66,67). Therefore, MS-based proteomics is
likely to become an important tool in the identification and
application of multi-analyte biomarker panels, including the use of
tear fluid samples for the diagnosis of ophthalmic diseases and
conditions.
5. Normal tear proteome in healthy ocular
condition
Under normal healthy ocular conditions, tear
proteins are mainly released from the lacrimal gland (68), meibomian glands (69), goblet cells (70), and accessory lacrimal glands.
Early discovery studies identified only 54 proteins in tears from
subjects without eye diseases (37). The number of proteins identified
increased notably to 491 in closed-eye tear fluid using hybrid
linear ion trap-Fourier transform (LTQ-FT) and LTQ-Orbitrap mass
spectrometers (71). The
majority of the identified proteins were involved in the modulation
of the immune system. They were responsible for carrying out
immune, inflammatory responses as well as defense responses to
pathogens. This study also focused on the identification of
proteases and antioxidant enzymes. Among the 491 proteins
identified, 64 were proteases or protease inhibitors, and 18 were
antioxidant enzymes. These findings could explain the importance of
tears in protecting the healthy ocular surface from noxious
external stimulants and irritants. The results of studies of the
proteome of human tears in healthy subjects are shown in Table I.
 | Table IHuman tear proteome identification of
healthy subjects using various proteomics approaches coupled with
mass spectrometry. |
Table I
Human tear proteome identification of
healthy subjects using various proteomics approaches coupled with
mass spectrometry.
A, Capillary tube
|
|---|
| First author,
year | Sample
preparation | Mass
spectrometer(s) | Number of protein
identification | Clinical
condition(s) | (Refs.) |
|---|
| Li, 2005 | SDS-PAGE; In-gel
digestion; In-solution digestion | LXQ Deca (Thermo
Fisher Scientific, Inc.); Reflex III (Bruker Corporation);
QSTAR® Pulsar (SCIEX) | 54 | Open eye, normal
subjects | (37) |
| de Souza, 2006 | SDS-PAGE;
In-solution digestion | LTQ-FT (Thermo
Fisher Scientific, Inc.); LTQ-Orbitrap (Thermo Fisher Scientific,
Inc.) | 491 | Closed eye, normal
subjects | (71) |
| Ananthi, 2011 | SDS-PAGE;
In-solution digestion | MicrOTOF-Q (Bruker
Corporation) | 54 | Reflex tear fluid,
normal subjects (n=40; F=20, M=20) | (72) |
| Shamsi, 2011 | SDS-PAGE; In-gel
digestion | Ultraflex III
(Bruker Corporation) | 182 | Normal subjects
(age=35±5; n=25; F=10, M=15) | (79) |
| Perumal, 2015 | SDS-PAGE; In-gel
digestion | LTQ Orbitrap XL™
(Thermo Fisher Scientific, Inc.) | 78 | Based and reflex
tears (age between 20-33 years; n=20; F=10, M=10) | (50) |
|
B, Schirmer's strip
|
| First author,
year | Sample
preparation | Mass
spectrometer(s) | Number of protein
identification | Clinical
condition(s) | (Refs.) |
|
| Zhou, 2012 | SCX-RPLC;
In-solution digestion | TripleTOF 5600
System (SCIEX) | 1,543 | Normal subjects
(age=36±14; n=4; F=3, M=1) | (15) |
| Aass, 2015 | SCX-RPLC;
In-solution digestion | LTQ Orbitrap XL™
(Thermo Fisher Scientific, Inc.) | 1,526 | Normal subjects
(n=3) | (75) |
| Tong, 2015 | RPLC; In-solution
digestion | TripleTOF 5600
System (SCIEX) | 747 | Normal subjects
(age=55.5±14.5; n=1,000; F=589; M=611) | (74) |
| Dor, 2019 | RPLC; In-solution
digestion | LTQ Orbitrap Velos
Pro (Thermo Fisher Scientific, Inc.) | 1,351 | Normal subjects
(age=37.6±18.6; n=8; F=4, M=4) | (78) |
|
C, Capillary tube
and Schirmer's strip
|
| First author,
year | Sample
preparation | Mass
spectrometer(s) | Number of protein
identification | Clinical
condition(s) | (Refs.) |
|
| Green-Church,
2008 | SDS-PAGE; SCX-RPLC;
In-gel digestion | LTQ (Thermo Fisher
Scientific, Inc.) | Total, 97; Common,
30; Schirmer's strip, 54; Capillary tube, 13 | Closed eye, normal
subjects (age=35±13; n=8; F=6, M=2) | (31) |
| Nättinen, 2020 | RPLC; In-solution
digestion | TripleTOF 5600+
System (SCIEX) | Total, 992; Common,
316; Schirmer's strip, 592; Capillary tube, 88 | Normal subjects
(n=31) | (24) |
Tear proteome profiles of normal subjects have been
the basic research standard for method assessment and development
of the clinical use of tear proteomics. LTF, SCGB2A1, haptoglobin,
α-1-antitrypsin (SERPINA1), CST4, LCN1 and LACRT were found to be
significantly upregulated in the tear fluid of female patients
compared with male patients. A total of 253 proteins and 231
proteins were identified in the tears of male and female patients,
respectively, using an electrophoresis method (72). The regulation of LCN1 in tear
fluid was shown to be hormone-dependent in an experimental rabbit
model, but the function of LCN1 in the tears of female patients
remains unknown (73). Most
upregulated proteins in the tear fluid of female patients were
responsible for local immune defense responses. In-depth analysis
with the use of fractionation, nanoscale reversed phase-liquid
chromatography (nanoRP-LC), and TripleTOF 5600 MS resulted in the
report of a comprehensive human tear proteome, comprising the
discovery of 1,543 proteins in normal healthy subjects (15). This number of proteins was
significantly higher than other reports, so it should be noted that
isoforms of the same protein were counted as separate proteins and
only 714 proteins of the reported proteins were repeatable and
reproducible in the triplicate analysis. Another study reported a
total of 747 proteins in human tears (74), of which 595 were also reported by
Zhou et al (15). Using
an optimized extraction method and two-dimensional strong cation
exchange-reversed phase (SCX-RP) with greater orthogonality of
separation, Aass et al (75) reported 1,526 proteins in
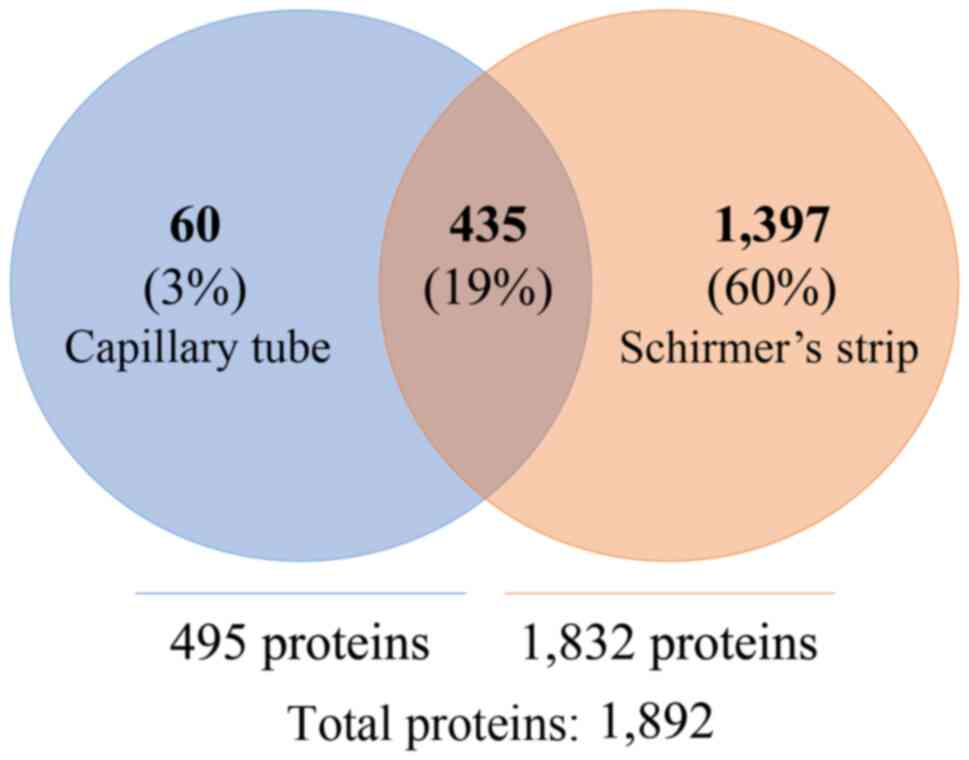
tear-fluid. We have converted the International Protein Index
(IPI), GenInfo Identifier (GI) protein identification from the
literature listed in Table I to
a matched UniProt reviewed proteome for comparison. A total of
3,724 unique proteins (1% False Discovery Rate in each study) were
identified in tear fluid, with 1,397 (60%) unique proteins only
identified in Schirmer's strip samples, and 60 (3%) unique proteins
in tear samples collected with a capillary tube (Fig. 1). These independent studies had
reported the most tear protein analyzed with LTQ-Orbitrap (Thermo
Fisher Scientific, Inc.) and TripleTOF 5600 mass spectrometers
(SCIEX). The combination of these studies is likely to increase the
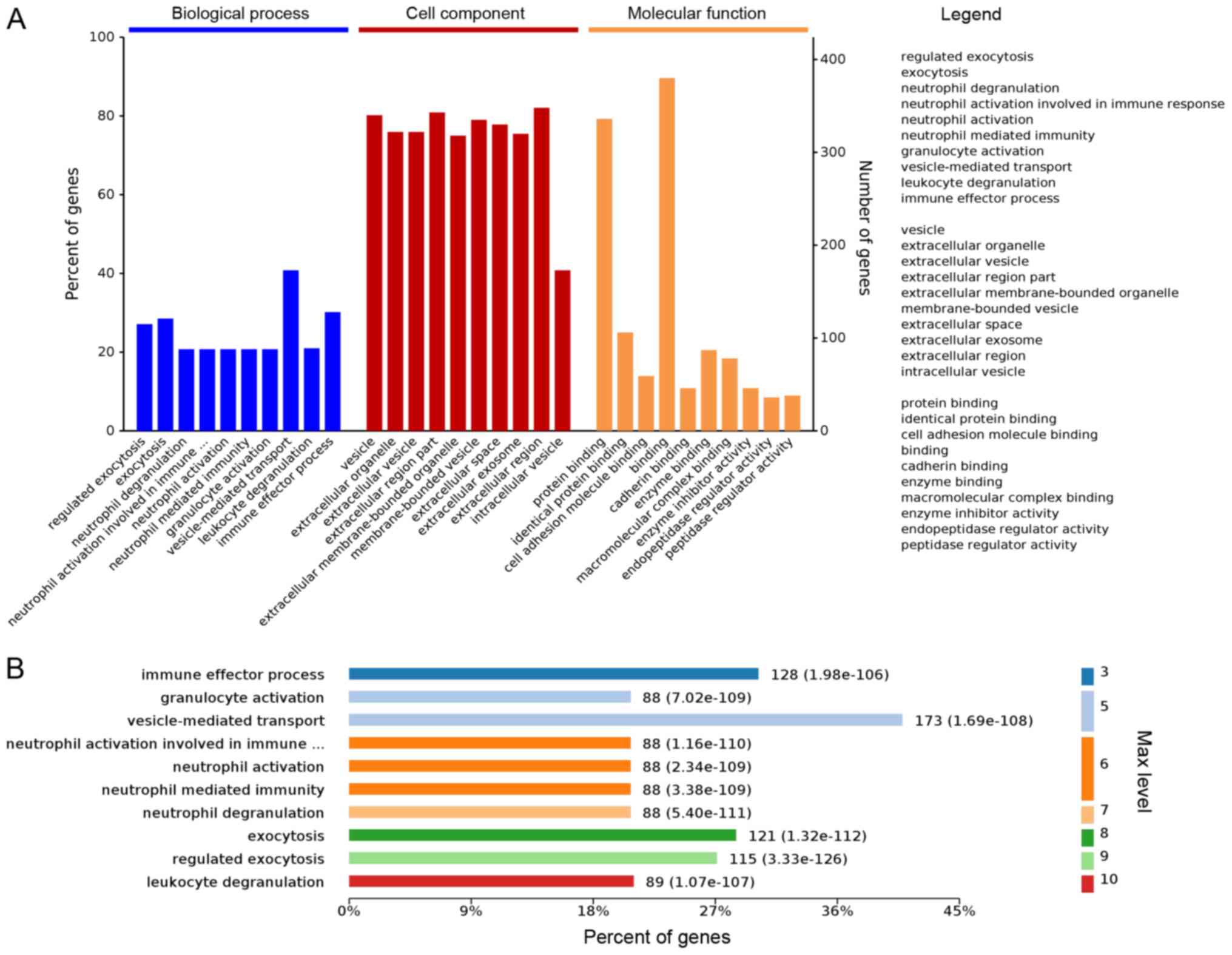
confidence of such protein identification. We propose that 435
(19%) proteins commonly reported can be identified regardless of
the tear fluid collection method and are the higher abundant, core
protein in the composition of tear fluid. Comprehensive information
of these 435 common proteins was derived from the UniProt database
(https://www.uniprot.org) and is summarized in
Table SI. Gene Ontology
information on their biological processes and protein class was
analyzed using the Omicsbean classification system (http://www.omicsbean.cn). The reported genes are
categorized into 'Biological Process', 'Cell Component' and
'Molecular Function', and it was found that the enriched genes were
involved in the top three pathways associated with
'vesicle-mediated transport', 'immune effector process' and
'exocytosis' (Fig. 2). These
data were generated from a mixture of MS and vendors. Regardless of
the MS system, common proteins are likely to be identified in tear
fluid, but this will depend on the collection method. Several
reports have stated that Orbitrap MS yields higher protein
identifications compared with the TripleTOF MS (76-79).
6. Putative protein markers in tear
fluid
Dry eye disease
Based on the definition and classification provided
by the International Dry Eye Workshop in 2017 (80), dry eye disease is a
multifactorial disease of the ocular surface characterized by a
loss of homeostasis of the tear film that leads to tear film
instability and hyperosmolarity, ocular surface inflammation, and
neurosensory abnormalities and associated ocular symptoms (81). The two common types of dry eyes
are known as the aqueous-deficient and evaporative dry eyes
(82). Clinical diagnosis of dry
eye diseases is based on questionnaires, Schirmer test, phenol red
thread test, tear breakup time, corneal staining and tear
osmolarity (83,84). However, these assessments have
shown poor reproducibility and large inter-test variability, as
well as a poor correlation between the findings and subjective
symptoms (85). Hence, an unmet
need requires a reliable prognostic method when diagnosing dry eye
diseases. Proteomic analysis of tear fluid has been increasingly
used to identify biomarkers for ocular diseases.
Ocular surface inflammation is one of the major
findings of patients with dry eye so several inflammatory proteins
can act as possible biomarkers of dry eyes (86). It is reported that several
inflammatory proteins are reported to be differentially expressed,
including upregulated proteins of α-enolase (ENO1), α-1-acid
glycoprotein 1 (ORM1), calgranulin A (S100A8), calgranulin B
(S100A9), calvasculin (S100A4) and calgizzarin, and downregulated
proteins of prolactin-inducible protein, LTF, LCN1 and LYZ
(87). ORM1 protein promotes
anti-inflammatory responses, whereas S100A8 and S100A9 proteins are
pro-inflammatory proteins and are commonly found in the area of
inflammation (88).
Downregulated proteins LTF, LYZ and LCN1 are abundant proteins that
protect against pathogens in tear fluid. The decreased expression
of these proteins may explain why patients are prone to infectious
ocular surface diseases (89).
Notably, lipocalins promote the formation and maintenance of a
compact and homogeneous outermost lipid layer of the tear film
(90). Hence, decreased levels
of lipocalins may lead to an unstable lipid layer, as well as an
increased evaporation rate of the tear fluid. The levels of S100A8
and S100A9 are associated with the severity of meibomian gland
dysfunction (MGD) and with symptoms of ocular redness and transient
blurring in patients with dry eye (91). The upregulation of S100A8 and
S100A9 occurs in response to the oxidative changes in redox
regulation and inflammatory regulation (92). Significantly upregulated levels
of ALB and downregulated lactase-phlorizin hydrolase, LCN1,
SCGB2A1, and lipophilin A were reported in the evaporative dry eye
disease (93). The increased
level of ALB is an indication of passive exudation, i.e. a leaky
blood-eye barrier in conjunctival vessels (94).
Another previous study reported the differential
expression of PRR4, zymogen granule protein 16 homolog B (ZG16B),
DMBT1, LACRT, opiorphin prepropeptide (PROL1), aldehyde
dehydrogenase dimeric NADP-preferring (ALDH3A1),
phosphatidylethanolamine-binding protein 1, serotransferrin (TF),
together with S100A8, S100A9, SCGB2A1, ENO1 and ORM1 that were
previously reported in the literature (95). The increased expression of PRR4
and ZG16B in dry eye disease may indicate an impaired neurological
process of the lacrimal gland. Downregulation of DMBT1 impairs
epithelial differentiation and cellular defense mechanisms, whereas
the reduction of LACRT may account for the reduced tears secretion
in patients with dry eye (96).
The reduction of PROL1 affects the paracrine or autocrine pathway
of the lacrimal system (97).
The ALDH3A1 protein protects against the oxidative stress of toxic
radicals on the corneal surface (98). The upregulation of TF protein was
only identified in the aqueous deficient type of dry eye (95). A previous study demonstrated the
complex molecular difference between dry eye disease and MGD.
Thioredoxin, Ig γ-1, membrane-associated phospholipase A2, SERPINA1
and antileukoproteinase (SLPI) were found to be upregulated in
patients with dry eye, yet these proteins were downregulated in
MGD. In addition, lactoperoxidase (LPO) was significantly
downregulated in dry eye disease and upregulated in MGD (99). The upregulation of these proteins
suggests enhanced immune, host-defense and proteolytic responses in
aqueous-deficient dry eye disease, whereas the contrary may be the
case in the evaporative dry eye caused by MGD. Furthermore, the
higher level of hyperosmolarity in patients with MGD may lead to an
increased expression of oxidative stress-associated LPO protein in
MGD when compared with patients with dry eye. The differential
expression of proteins between MGD and dry eye suggest different
regulatory processes. S100A8, S100A9 and ORM1 were identified as
differentially expressed in all the dry eye studies reported in the
present review (Table II).
Hence, these proteins may serve as biomarkers of dry eye disease,
in addition to the established biomarker matrix metalloproteinase-9
(MMP-9) that is already being employed in the diagnosis of dry eye
disease (100). Although
anterior ocular inflammation is a typical feature of Sjögren
syndrome, it is considered to be a systemic autoimmune disease with
some distinct clinical presentation (101). Different from physiological dry
eyes, aqueous-deficient and evaporative dry eyes, which could be
clinically difficult to differentiate using routine clinical
assessments. It was recently found that the elevated MMP-9 protein
biomarker is non-specific and difficult to distinguish Sjögren
syndrome from typical dry eye diseases (102). MS-based proteomics approaches
enabled the discovery of the upregulation of other pro-inflammatory
proteins, including LIM domain only protein 7, E3 ubiquitin-protein
ligase and Copine-1, as well as in the involvement of TNF-α
signaling (103,104), which suggested the possibility
that specific molecular biomarkers may be developed for more
specific clinical diagnosis.
| Table IIList of significantly differentiated
tear protein abundance by MS-based proteomic analysis in ocular
diseases. |
Table II
List of significantly differentiated
tear protein abundance by MS-based proteomic analysis in ocular
diseases.
A, Capillary tube
|
|---|
| First author,
year | Separation | Mass
spectrometry | Conditions | Differentially
expressed protein markers, gene name
| (Refs.) |
|---|
| Upregulated | Downregulated |
|---|
| Versura, 2010 | 2D SDS-Page |
Micromass® Q-Tof (Waters
Corporation) | Evaporative dry eye
(age=64.2±22.3; n=90; F=42, M=18) | ALB | LCN1, LTF, SCGB1D1,
SCGB1D2, SCGB2A1 | (93) |
| Csősz, 2012 | RPLC | ESI-MS/MS (QTRAP
4000, SCIEX) | General diabetic
retinopathy (average age=61; n=145) Non-proliferative diabetic
retinopathy (average age=56) Proliferative diabetic retinopathy
(average age=64) | IGLC1, LACRT, LCN1,
LFT, LYZ, SCGB1D1 CST4
APOA1, IGLC1, LACRT, LCN1, LFT, LYZ, PRB4, SCGB1D1, SCGB2A1 | | (107) |
| Soria, 2017 | RPLC | SYNAPT G2-S HDMS
System (Waters Corporation) | Aqueous deficient
dry eye and control (age=54.58±21.55; n=24; F=14, M=10) Meibomian
gland diseases and control (age=54.7±11.6; n=12; F=7, M=5) | APOD, C3, CP,
IGHG1, ORM2, PLA2G2A, S100A6, S100A8, SERPINA1, SLPI, TXN ANXA1,
CLU, LPO, ORM1 | LPO
IGHG1, PLA2G2A, TXN, SERPINA1, SLPI | (99) |
|
B, Schirmer's strip
|
| First author,
year | Separation | Mass
spectrometry | Conditions | Differentially
expressed protein markers, gene name
| (Refs.) |
| Upregulated | Downregulated |
|
| Zhou, 2009 | Online 2D
SCX-RPLC | QSTAR-XL qTOF
(SCIEX) | General dry eye and
control (average age=60; n=56; F=43, M=23) | ENO1, ORM1, S100A4,
S100A8, S100A9, S100A11 | LCN1, LTF, LYZ,
PIP | (87) |
| Wong, 2011 | Online 2D
SCX-RPLC | QSTAR-XL qTOF
(SCIEX) | Glaucoma and
control (Topical antiglaucoma medications for >1 year; age=72±7;
n=18; F=9, M=9) Glaucoma and control (Topical antiglaucoma
medications for <1 year) | S100A8, S100A9,
SCGB2A1, YWHAZ
SCGB2A1, S100A8 | PRR4
PRR4, S100A9, YWHAZ | (105) |
| Matheis, 2012 | 1D-SDS-PAGE | Ultraflex
MALDI-TOF/TOF (Bruker Corporation) | TAO and control
[median age=45 (33-74); n=45] | CST4, LYZ | B2M, PRB4 | (114) |
| Pieragostino,
2012 | 1D-SDS-PAGE | Reflex IV MALDI-TOF
(Bruker Corporation) | PXG and control
(n=5)
POAG and control (n=4)
POAG vs. PXG | TF,
S100A4
IGHG1, IGHG2, IGHG4
CST2, CST4, IGHG2, LACRT, PRR4, SCGB2A1 | AZGP1, CST1, CST2,
CST4, IGHA1, KRT1, LACRT, LCN1, LYZ, OPRPN, PIP, PRR4, SCGB2A1,
ZG16B ANXA1, AZGP1, CST1, CST2, CST4, IGHA1, IGHA2, IGKC, JCHAIN,
KRT1, LCN1, LTF, LYZ, PIGR, PIP, PRR4, SCGB2A1 JCHAIN, KRT19,
LGALS3, PIGR, PRDX1, S100A4, S100A8 | (136) |
| Pieragostino,
2013 | RPLC | LTQ Orbitrap
(Thermo Fisher Scientific, Inc.) | Primary open angle
glaucoma and control (age=55.4±14.5; n=9; F=4, M=5) | ACTB, ACTG1, ALB,
AZGP1, B2M, CST4, HSPB1, IGHA1, IGHA2, IGKC, JCHAIN, LCN1, LTF,
LYZ, OPRPN, PIGR, PIP, POTEE, POTEF, POTEI, POTEJ, PRDX1, PRR4, TF,
ZG16B | | (137) |
| Matheis, 2015 | 1D-SDS-PAGE | Ultraflex
MALDI-TOF/TOF (Bruker Corporation) | TAO and control
[median age=45.5 (17-68); n=30; F=23, M=7]
TAO with DE (TAO: DE) and control [median age=51 (31-70); n=30; F=25, M=5] DE and control
[median age=54.5 (32-80); n=30; F=23, M=7] TAO and
DE
TAO and TAO:DE TAO:DE and DE | MDN1,
POTEI
LEG3, SMCA4 ANXA1, HSPB1, LEG3, S10A8, SMCA4
LYSC | PROL1, PRP4, S10A8,
SMCA4
UGDH
ANXA1, CYTN, HSPB1, LEG3, PROL1, S10A8, SMCA4, UGDH LEG3 CYTN,
PROL1, S10A8, SMCA4, UGDH | (117) |
| Aass, 2016 | RPLC | LTQ Orbitrap
(Thermo Fisher Scientific, Inc.) | TAO and control
[median age=57 (20-77); n=21; F=15, M=6] | APOD, AZGP1,
CASP14, DCD, DMBT1, GPX3, LACRT, LYZ, MSLN, PLOD2, SLPI, ZG16B | CST5, PPL,
SCGB2A2 | (122) |
| Perumal, 2016 | IDE | LTQ Orbitrap
(Thermo Fisher Scientific, Inc.) | Evaporative dry eye
and control (F age=51.8±18.66; M age=52.9±20.45; n=20; F=10, M=10)
Aqueous deficient dry eye (F age=49.6±14.74; M age=47.6±15.32;
n=20; F=10, M=10) Aqueous deficient and evaporative dry eye (F
age=58.78±17.42; M age (57.73±19.38; n=20; F=10, M=10) | S100A8,
S100A9
ENO1, ORM1, PEBP1, S100A8, S100A9, TF
ALDH3A1, ENO1, ORM1, PEBP1, S100A8, S100A9, TF | PROL1, PRR4, ZG16B
DMBT1, PROL1, PRR4, SCGB2A1, ZG16B DMBT1, LACRT, PROL1, PRR4,
SCGB2A1, ZG16B | (95) |
| Kishazi, 2018 | 1D-SDS-PAGE | LTQ Orbitrap
(Thermo Fisher Scientific, Inc.) | TAO and control
(age=46.92±11.25; n=28; F=21, M=7) | CST3, HP, NQO1,
SERPINA3, TXNDC5 | ABHD14B, ADH5,
ALDH1A1, PLA2G2A, STAT1 | (125) |
These studies have provided preliminary data on
protein biomarkers in tear fluid using MS techniques. However,
there are several limitations of using tear proteomics to make a
diagnosis of dry eyes. The tear sampling methods and ways of sample
manipulation differ among the reported studies; hence, a direct
comparison between these studies may not be appropriate. To achieve
comparable results, standardization of sampling methods and sample
manipulation protocols are required in the future. Additionally,
S100A8 and S100A9, which were differentially expressed in all of
the studies, were also reported in patients with glaucoma (Table II), indicating that these
inflammatory proteins are not differentially expressed uniquely in
patients with dry eye (105).
In summary, several potential biomarkers have been identified in
patients with dry eyes, but whether a diagnosis of dry eyes can be
based on tear proteomics remains to be determined and defined. A
signature panel of tear fluid biomarkers is needed to address
overlap with other conditions to increase the specificity of tear
fluid protein markers for the diagnosis of dry eye diseases.
Diabetic retinopathy
Diabetic retinopathy is a common complication of
diabetes mellitus (DM). The condition is asymptomatic in the early
stages of disease development, yet it can cause irreversible
blindness in its final stages. Tear composition can be affected by
DM, although the tear film is not in direct contact with the retina
(106). Hence, tear proteins
may act as biomarkers for the screening of diabetic retinopathy.
The relative abundance of LACRT, Ig lambda chain C region (LAC),
LTF, LYZ, LCN1 and SCGB2A1 proteins were upregulated in patients
with proliferative diabetic retinopathy (PDR) compared with non-PDR
and healthy subjects (107).
The upregulated expression levels of LTF, LAC and LACRT may reflect
an increased inflammatory response, potentially caused by macular
edema, vascular abnormalities, the proliferation of the ocular
cells, and an indicator of the pro-proliferative environment that
is essential for the progression of diabetic retinopathy (108).
Thyroid eye disease
Thyroid-associated orbitopathy (TAO) is an
autoimmune disorder that affects the orbit. TAO is characterized by
enlarged extraocular muscles, orbital tissue and inflammatory
changes, including upper eyelid retraction, proptosis and erythema
of the conjunctiva (109).
There are two phases of TAO: The inflammatory phase, which requires
anti-inflammatory treatment, and a later less active stage
(110). The clinical diagnosis,
assessment and management of the disease are based on the Clinical
Activity Score (CAS) (111).
However, disease onset, prognosis and time course of TAO remain
unclear. TAO mainly affects the extraocular muscles, eyelid and
orbital tissue. These surrounding damaged tissues may release
different proteins into tears or by passive transport from blood;
therefore, tears may contain potential protein markers for the
diagnosis of TAO (112).
However, the composition of tears collected from patients with TAO
need to be analyzed carefully as it may contain certain
inflammatory proteins that are associated with exposure keratitis,
which is a common complication of TAO (113).
In one previous study, the expression of three
proteins was modulated in patients with TAO (114). LYZ was found to be upregulated,
whereas PRP4 and B2M were downregulated in patients with TAO. LYZ
is a proteolytic protein that is important in the immune response
(115) and increased LYZ is
found in patients with autoimmune diseases (116). The increase of LYZ may suggest
increased inflammatory responses of the lacrimal gland. Lacrimal
PRP4 can regulate the microflora of the eye to protect the ocular
surface (117). The
inflammatory processes of the orbit in TAO may decrease the
lacrimal expression of PRP4. It has been demonstrated that
increased levels of inflammation and higher CAS values are
associated with lower levels of PRP4, indicating the progressive
nature of the inflammatory lacrimal gland dysfunction in patients
with TAO (114). B2M belongs to
the major histocompatibility complex class I molecules and also
plays an important role in immune responses (118). The downregulation of B2M may
reflect altered immune function in this auto-immune disease.
Patients with TAO can have signs and symptoms
similar to dry eye syndrome, which can result in delayed diagnosis
of TAO (117). In comparison to
normal subjects, transcription activator BRG1 (SMCA4), PROL1, PPR4
and S100A8 proteins were downregulated, whereas midasin, POTE
ankyrin domain family member I and LYZ proteins were upregulated in
patients with TAO (117). In
comparison to patients with dry eye, UDP-glucose 6-dehydrogenase
(UGDH), annexin A1, cystatin-C (CST3), heat shock protein β1
(HSPB1), galectin-1, PROL1, S100A8 and SMCA4 proteins were
downregulated in patients with TAO (117). The apoptosis of lacrimal cells
can cause the downregulation of PROL1 and PRR4 proteins, the
protective enzymes secreted by the lacrimal acinar cells in TAO
(119). The damage to the
lacrimal cells can reduce the number of cystatin proteins, which
perform protective function in the tears (120). UGDH protein is responsible for
the indirect production of the glycosaminoglycans that are
expressed in fibroblasts in the active phase of TAO (121). The downregulation of UGDH
protein can be explained by the fact that the majority of the
patients involved in this study were in advanced and inactive
stages of TAO. A similar study reported 12 upregulated proteins in
patients with TAO, including caspase-14, SLPI, dermcidin (DCD),
procollagen-lysine 2-oxoglutarate 5-dioxygenase 2, mesothelin,
apolipoprotein D, glutathione peroxidase 3, zinc-α-2-glycoprotein
1, DMBT1, ZG16B and LACRT (122). The overexpression of CASP14,
SLPI and LYZ proteins may represent the inflammatory responses of
the ocular surface, orbital tissue or lacrimal gland. However, the
exact function of CASP14 in tear fluid remains unclear. DCD protein
has anti-microbial properties and has been detected in conjunctival
cells (123). Increased amounts
of DCD protein suggest more bulbar conjunctiva inflammation in
patients with TAO (124). In a
more recent study, retinal dehydrogenase 1, SERPINA3 and CST3
proteins were found to be upregulated in tear fluid obtained from
patients with TAO (125). CST3
protein is a cysteine protease inhibitor that is concentrated and
expressed in the retinal pigment epithelium (126). The concentration of CST3
protein in the blood is associated with thyroid functioning
(127). The downregulation of
retinol dehydrogenase 11 protein may result in reduced synthesis of
retinoic acid, hence, affecting the visual pigment and leading to
vision loss (128). Increased
expression of SERPINA3, a protein responsible for mediating
inflammatory responses, may reflect the increased level of eye
inflammation in TAO, which is an autoimmune disease with orbital
inflammatory responses. Different biomarkers for TAO have been
identified across different studies (Table II), further validation should be
carried out to confirm potential biomarkers and these biomarkers
should be analyzed according to the severity or different stages of
TAO.
Primary open-angle glaucoma (POAG)
Glaucoma is a progressive neurodegenerative disease
that causes optic nerve head damage, retinal nerve fiber layer
defects, and is associated with the loss of the visual field
(129). It is one of the main
causes of blindness worldwide (130). The underlying mechanism of
glaucoma remains unclear, and the clinical diagnosis of glaucoma
relies on several assessments, including tonometry, dilated fundus
image examination, visual field test, gonioscopy and pachymetry
(129). Visual field impairment
is a cause of irreversible damage to retinal ganglion cells
(131). Tear fluid proteomic
profiling may provide novel insights into the understanding and
diagnosis of glaucoma and may serve to monitor therapy, including
the side effects of medication. POAG is the most common subtype of
open-angle glaucoma in the European population (132). The damaged trabecular meshwork
and modification of the aqueous humor leads to an impaired drainage
system. The accumulation of fluid increases the intraocular
pressure (IOP) of the eye (133). Pseudoexfoliative glaucoma (PXG)
is another subtype of POAG and is characterized by the production
and accumulation of abnormally high concentration of fibrillar and
proteinaceous substances in the anterior segment of the eyes
(134). These substances can
block the ocular drainage system and thus increase the IOP of the
eye, one of the risk factors of glaucoma (135). A total of 23 differentially
expressed proteins have been reported in POAG and PXG. Cystatin-SA,
CST4, SCGB2A1, Ig γ-2 chain C region and PRR4 proteins were found
to be upregulated in POAG, but not PXG. Peroxiredoxin-1, IGJ,
galectin-3, PIGR, keratin type I cytoskeletal 19, S100A4, S100A8
and LACRT were found to be downregulated in POAG compared with PXG
samples. More importantly, keratin type I cytoskeletal 10 and
apolipoprotein A-II proteins are unique to POAG tear fluid
(136). B2M, HSPB1, IGHA1,
immunoglobulin heavy constant α2, IGJ, IGKC, LTF, LYZ, PIGR, TF and
ALB proteins were also upregulated in patients with POAG (136). The modulation of these proteins
between treated and untreated POAG groups indicated that PGA works
effectively via the anti-inflammatory mechanism. Proteomics was
applied to monitor patients chronically treated with topical
antiglaucoma medications, finding that SCGB2A1, S100A8, S100A9 and
14-3-3 ζ/δ proteins were upregulated, whereas PRR4 was
downregulated in patients with glaucoma treated with IOP lowering
medication (105). The results
indicated that the use of topical antiglaucoma medications for
>1 year affects the ocular surface by inducing inflammatory
responses. The tear fluid proteome of the medically treated
patients with glaucoma and patients with dry eyes compared with
normal control subjects have shown upregulation of S100A8 and
S100A9 proteins in both glaucoma and dry eye patients. Proteins
expressed in medically treated glaucoma eyes (SCGB2A1, 14-3-3 ζ/δ,
PRR4) or dry eyes (ENO1, S100A4) did not exhibit a common
expression pattern between conditions (137). These results suggested that
distinct, yet complex mechanisms lead to different inflammatory
responses in ocular diseases that can be distinguished using
MS-based proteomic techniques.
7. Conclusions
The present review provided a brief introduction to
the development of proteomics platforms for tear proteome studies.
The proteome identified in normal tear fluid and its expression in
dry eye syndrome, diabetic retinopathy, thyroid eye disease and
POAG were summarized. MS-based methods have evolved rapidly with
technological advances in high-resolution mass spectrometers and
data analysis tools for a variety of discovery-based experiments,
resulting in ever-larger proteomic datasets in tear fluid. With
respect to accurate quantitative proteomics, DIA and labeled tags
offer consistent quantification of proteins in disease conditions
for both pilot and large cohort studies. MS technology continues to
improve and has enabled in-depth protein profiling, reliable
quantification with superior flexibility for assay development, and
remains the only anti-body-free approach for protein analysis in
biological samples. The consistent results of analyzing the
microliter volumes of tear fluid or differentiated proteins has
demonstrated the potential development of assays for ocular
diseases and ophthalmology overall using a variety of MS
approaches. For future approved molecular diagnostics, a
custom-made antibody-based assay or point of care diagnostic
molecular kit could be developed to target specific proteins,
taking full advantage of established, lower-cost, and ease of use
into clinical use.
Supplementary Data
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JYWM and YHS drafted the manuscript. JFB edited and
formatted the manuscript. TCL conceived the idea, proofread the
manuscript, and provided financial support. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
The authors would like to thank Dr Maureen Boost
(Hong Kong Polytechnic University, Hong Kong, China) for her
diligent proofreading of the article.
Funding
This work was supported by a Ph.D. student scholarship (grant
no. RKTA) of The Hong Kong Polytechnic University.
References
|
1
|
Dogru M, Okada N, Asano-Kato N, Tanaka M,
Igarashi A, Takano Y, Fukagawa K, Shimazaki J, Tsubota K and
Fujishima H: Atopic ocular surface disease: Implications on tear
function and ocular surface mucins. Cornea. 24(8 Suppl): S18–S23.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gipson IK: The ocular surface: The
challenge to enable and protect vision: The Friedenwald lecture.
Invest Ophthalmol Vis Sci. 48:4390–4398. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Miano F, Mazzone M, Giannetto A, Enea V,
Mc Cauley P, Bailey A and Winlove PC: Interface properties of
simplified tear-like fluids in relation to lipid and aqueous layers
composition. Adv Exp Med Biol. 506:405–417. 2002. View Article : Google Scholar
|
|
4
|
King-Smith PE, Bailey MD and Braun RJ:
Four characteristics and a model of an effective tear film lipid
layer (TFLL). Ocul Surf. 11:236–245. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kijlstra A and Kuizenga A: Analysis and
function of the human tear proteins. Adv Exp Med Biol. 350:299–308.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Esmaeelpour M, Watts PO, Boulton ME, Cai J
and Murphy PJ: Tear film volume and protein analysis in full-term
newborn infants. Cornea. 30:400–404. 2011. View Article : Google Scholar
|
|
7
|
Sack RA, Sathe S and Beaton A: Tear
turnover and immune and inflammatory processes in the open-eye and
closed-eye environments: Relationship to extended wear contact lens
use. Eye Contact Lens. 29(Suppl 1): S80–S84. S192–S194. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Stern ME, Schaumburg CS, Dana R, Calonge
M, Niederkorn JY and Pflugfelder SC: Autoimmunity at the ocular
surface: Pathogenesis and regulation. Mucosal Immunol. 3:425–442.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schicht M, Garreis F, Hartjen N, Beileke
S, Jacobi C, Sahin A, Holland D, Schröder H, Hammer CM, Paulsen F
and Bräuer L: SFTA3-a novel surfactant protein of the ocular
surface and its role in corneal wound healing and tear film surface
tension. Sci Rep. 8:97912018. View Article : Google Scholar
|
|
10
|
Kwong MS, Evans DJ, Ni M, Cowell BA and
Fleiszig SM: Human tear fluid protects against Pseudomonas
aeruginosa keratitis in a murine experimental model. Infect Immun.
75:2325–2332. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhou L and Beuerman RW: The power of
tears: How tear proteomics research could revolutionize the clinic.
Expert Rev Proteomics. 14:189–191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hagan S, Martin E and
Enriquez-de-Salamanca A: Tear fluid biomarkers in ocular and
systemic disease: Potential use for predictive, preventive and
personalised medicine. EPMA J. 7:152016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gachon AM and Lacazette E: Tear lipocalin
and the eye's front line of defence. Br J Ophthalmol. 82:453–455.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kuizenga A, van Haeringen NJ and Kijlstra
A: Identification of lectin binding proteins in human tears. Invest
Ophthalmol Vis Sci. 32:3277–3284. 1991.PubMed/NCBI
|
|
15
|
Zhou L, Zhao SZ, Koh SK, Chen L, Vaz C,
Tanavde V, Li XR and Beuerman RW: In-depth analysis of the human
tear proteome. J Proteomics. 75:3877–3885. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mishima S, Gasset A, Klyce SD Jr and Baum
JL: Determination of tear volume and tear flow. Invest Ophthalmol.
5:264–276. 1966.PubMed/NCBI
|
|
17
|
Rentka A, Koroskenyi K, Harsfalvi J,
Szekanecz Z, Szucs G, Szodoray P and Kemeny-Beke A: Evaluation of
commonly used tear sampling methods and their relevance in
subsequent biochemical analysis. Ann Clin Biochem. 54:521–529.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Esmaeelpour M, Cai J, Watts P, Boulton M
and Murphy PJ: Tear sample collection using cellulose acetate
absorbent filters. Ophthalmic Physiol Opt. 28:577–583. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Inic-Kanada A, Nussbaumer A, Montanaro J,
Belij S, Schlacher S, Stein E, Bintner N, Merio M, Zlabinger GJ and
Barisani-Asenbauer T: Comparison of ophthalmic sponges and
extraction buffers for quantifying cytokine profiles in tears using
Luminex technology. Mol Vis. 18:2717–2725. 2012.PubMed/NCBI
|
|
20
|
López-Cisternas J, Castillo-Diaz J,
Traipe-Castro L and López-Solis RO: Use of polyurethane minisponges
to collect human tear fluid. Cornea. 25:312–318. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rohan LC, Edwards RP, Kelly LA, Colenello
KA, Bowman FP and Crowley-Nowick PA: Optimization of the weck-Cel
collection method for quantitation of cytokines in mucosal
secretions. Clin Diagn Lab Immunol. 7:45–48. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Posa A, Bräuer L, Schicht M, Garreis F,
Beileke S and Paulsen F: Schirmer strip vs capillary tube method:
Non-invasive methods of obtaining proteins from tear fluid. Ann
Anat. 195:137–142. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
VanDerMeid KR, Su SP, Krenzer KL, Ward KW
and Zhang JZ: A method to extract cytokines and matrix
metalloproteinases from Schirmer strips and analyze using Luminex.
Mol Vis. 17:1056–1063. 2011.PubMed/NCBI
|
|
24
|
Nättinen J, Aapola U, Jylhä A, Vaajanen A
and Uusitalo H: Comparison of capillary and Schirmer strip tear
fluid sampling methods using SWATH-MS proteomics approach. Transl
Vis Sci Technol. 9:162020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stuchell RN, Feldman JJ, Farris RL and
Mandel ID: The effect of collection technique on tear composition.
Invest Ophthalmol Vis Sci. 25:374–377. 1984.PubMed/NCBI
|
|
26
|
Denisin AK, Karns K and Herr AE:
Post-collection processing of Schirmer strip-collected human tear
fluid impacts protein content. Analyst. 137:5088–5096. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
van Haeringen NJ and Glasius E: The origin
of some enzymes in tear fluid, determined by comparative
investigation with two collection methods. Exp Eye Res. 22:267–272.
1976. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhou L and Beuerman RW: Tear analysis in
ocular surface diseases. Prog Retin Eye Res. 31:527–550. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Castelli S, Arasi S, Pawankar R and
Matricardi PM: Collection of nasal secretions and tears and their
use in allergology. Curr Opin Allergy Clin Immunol. 18:1–9. 2018.
View Article : Google Scholar
|
|
30
|
Leonardi A: Allergy and allergic mediators
in tears. Exp Eye Res. 117:106–117. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Green-Church KB, Nichols KK, Kleinholz NM,
Zhang L and Nichols JJ: Investigation of the human tear film
proteome using multiple proteomic approaches. Mol Vis. 14:456–470.
2008.PubMed/NCBI
|
|
32
|
Kojima T, Dogru M, Kawashima M, Nakamura S
and Tsubota K: Advances in the diagnosis and treatment of dry eye.
Prog Retin Eye Res. Jan 29–2020.Epub ahead of print. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mainstone JC, Bruce AS and Golding TR:
Tear meniscus measurement in the diagnosis of dry eye. Curr Eye
Res. 15:653–661. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Altelaar AF, Munoz J and Heck AJ:
Next-generation proteomics: Towards an integrative view of proteome
dynamics. Nat Rev Genet. 14:35–48. 2013. View Article : Google Scholar
|
|
35
|
Schubert OT, Röst HL, Collins BC,
Rosenberger G and Aebersold R: Quantitative proteomics: Challenges
and opportunities in basic and applied research. Nat Protoc.
12:1289–1294. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zhao Y and Jensen ON:
Modification-specific proteomics: Strategies for characterization
of post-translational modifications using enrichment techniques.
Proteomics. 9:4632–4641. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Li N, Wang N, Zheng J, Liu XM, Lever OW,
Erickson PM and Li L: Characterization of human tear proteome using
multiple proteomic analysis techniques. J Proteome Res.
4:2052–2061. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gillet LC, Navarro P, Tate S, Röst H,
Selevsek N, Reiter L, Bonner R and Aebersold R: Targeted data
extraction of the MS/MS spectra generated by data-independent
acquisition: A new concept for consistent and accurate proteome
analysis. Mol Cell Proteomics. 11:O111.0167172012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Collins BC, Hunter CL, Liu Y, Schilling B,
Rosenberger G, Bader SL, Chan DW, Gibson BW, Gingras AC, Held JM,
et al: Multi-laboratory assessment of reproducibility, qualitative
and quantitative performance of SWATH-mass spectrometry. Nat
Commun. 8:2912017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Molloy MP: The challenge of
industrializing proteomics. Nat Biotechnol. 21:5972003. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Srinivasan S, Thangavelu M, Zhang L, Green
KB and Nichols KK: iTRAQ quantitative proteomics in the analysis of
tears in dry eye patients. Invest Ophthalmol Vis Sci. 53:5052–5059.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Zhao Z, Liu J, Wasinger VC, Malouf T,
Nguyen-Khuong T, Walsh B and Willcox MD: Tear lipocalin is the
predominant phosphoprotein in human tear fluid. Exp Eye Res.
90:344–349. 2010. View Article : Google Scholar
|
|
43
|
You J, Fitzgerald A, Cozzi PJ, Zhao Z,
Graham P, Russell PJ, Walsh BJ, Willcox M, Zhong L, Wasinger V and
Li Y: Post-translation modification of proteins in tears.
Electrophoresis. 31:1853–1861. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Huang Z, Du CX and Pan XD: The use of
in-strip digestion for fast proteomic analysis on tear fluid from
dry eye patients. PLoS One. 13:e02007022018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Nguyen-Khuong T, Everest-Dass AV, Kautto
L, Zhao Z, Willcox MD and Packer NH: Glycomic characterization of
basal tears and changes with diabetes and diabetic retinopathy.
Glycobiology. 25:269–283. 2015. View Article : Google Scholar
|
|
46
|
Magdeldin S, Enany S, Yoshida Y, Xu B,
Zhang Y, Zureena Z, Lokamani I, Yaoita E and Yamamoto T: Basics and
recent advances of two dimensional-polyacrylamide gel
electrophoresis. Clin Proteomics. 11:162014. View Article : Google Scholar
|
|
47
|
Broekhuyse RM: Tear lactoferrin: A
bacteriostatic and complexing protein. Invest Ophthalmol.
13:550–554. 1974.PubMed/NCBI
|
|
48
|
Berta A: A polyacrylamide-gel
electrophoretic study of human tear proteins. Graefes Arch Clin Exp
Ophthalmol. 219:95–99. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Molloy MP, Bolis S, Herbert BR, Ou K,
Tyler MI, van Dyk DD, Willcox MD, Gooley AA, Williams KL, Morris CA
and Walsh BJ: Establishment of the human reflex tear
two-dimensional polyacrylamide gel electrophoresis reference map:
New proteins of potential diagnostic value. Electrophoresis.
18:2811–2815. 1997. View Article : Google Scholar
|
|
50
|
Perumal N, Funke S, Wolters D, Pfeiffer N
and Grus FH: Characterization of human reflex tear proteome reveals
high expression of lacrimal proline-rich protein 4 (PRR4).
Proteomics. 15:3370–3381. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ladner CL, Yang J, Turner RJ and Edwards
RA: Visible fluorescent detection of proteins in polyacrylamide
gels without staining. Anal Biochem. 326:13–20. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Williams JG and Gratzer WB: Limitations of
the detergent-polyacrylamide gel electrophoresis method for
molecular weight determination of proteins. J Chromatogr.
57:121–125. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Corthals GL, Wasinger VC, Hochstrasser DF
and Sanchez JC: The dynamic range of protein expression: A
challenge for proteomic research. Electrophoresis. 21:1104–1115.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Gygi SP, Corthals GL, Zhang Y, Rochon Y
and Aebersold R: Evaluation of two-dimensional gel
electrophoresis-based proteome analysis technology. Proc Natl Acad
Sci USA. 97:9390–9395. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Shi Y, Xiang R, Horvath C and Wilkins JA:
The role of liquid chromatography in proteomics. J Chromatogr A.
1053:27–36. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Uhlén M, Fagerberg L, Hallström BM,
Lindskog C, Oksvold P, Mardinoglu A, Sivertsson Å, Kampf C,
Sjöstedt E, Asplund A, et al: Proteomics. Tissue-based map of the
human proteome. Science. 347:12604192015. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Nagaraj N, Wisniewski JR, Geiger T, Cox J,
Kircher M, Kelso J, Pääbo S and Mann M: Deep proteome and
transcriptome mapping of a human cancer cell line. Mol Syst Biol.
7:5482011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Geyer PE, Kulak NA, Pichler G, Holdt LM,
Teupser D and Mann M: Plasma proteome profiling to assess human
health and disease. Cell Syst. 2:185–195. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Nättinen J, Jylhä A, Aapola U, Mäkinen P,
Beuerman R, Pietilä J, Vaajanen A and Uusitalo H: Age-associated
changes in human tear proteome. Clin Proteomics. 16:112019.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Gilar M and Neue UD: Peak capacity in
gradient reversed-phase liquid chromatography of biopolymers.
Theoretical and practical implications for the separation of
oligonucleotides. J Chromatogr A. 1169:139–150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Shen Y, Zhao R, Belov ME, Conrads TP,
Anderson GA, Tang K, Pasa-Tolić L, Veenstra TD, Lipton MS, Udseth
HR and Smith RD: Packed capillary reversed-phase liquid
chromatography with high-performance electrospray ionization
Fourier transform ion cyclotron resonance mass spectrometry for
proteomics. Anal Chem. 73:1766–1775. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Hsieh EJ, Bereman MS, Durand S, Valaskovic
GA and MacCoss MJ: Effects of column and gradient lengths on peak
capacity and peptide identification in nanoflow LC-MS/MS of complex
proteomic samples. J Am Soc Mass Spectrom. 24:148–153. 2013.
View Article : Google Scholar :
|
|
63
|
Doerr A: Mass spectrometry-based targeted
proteomics. Nat Methods. 10:232013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Carapito C and Aebersold R: Targeted
proteomics. Proteomics. 12:10732012. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Borrebaeck CA: Precision diagnostics:
Moving towards protein biomarker signatures of clinical utility in
cancer. Nat Rev Cancer. 17:199–204. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Zhang Z: An in vitro diagnostic
multivariate index assay (IVDMIA) for ovarian cancer: Harvesting
the power of multiple biomarkers. Rev Obstet Gynecol. 5:35–41.
2012.PubMed/NCBI
|
|
67
|
Ueland FR, Desimone CP, Seamon LG, Miller
RA, Goodrich S, Podzielinski I, Sokoll L, Smith A, van Nagell JR Jr
and Zhang Z: Effectiveness of a multivariate index assay in the
preoperative assessment of ovarian tumors. Obstet Gynecol.
117:1289–1297. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Janssen PT and van Bijsterveld OP: Origin
and biosynthesis of human tear fluid proteins. Invest Ophthalmol
Vis Sci. 24:623–630. 1983.PubMed/NCBI
|
|
69
|
Tsai PS, Evans JE, Green KM, Sullivan RM,
Schaumberg DA, Richards SM, Dana MR and Sullivan DA: Proteomic
analysis of human meibomian gland secretions. Br J Ophthalmol.
90:372–377. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Gipson IK: Goblet cells of the
conjunctiva: A review of recent findings. Prog Retin Eye Res.
54:49–63. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
de Souza GA, Godoy LM and Mann M:
Identification of 491 proteins in the tear fluid proteome reveals a
large number of proteases and protease inhibitors. Genome Biol.
7:R722006. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Ananthi S, Santhosh RS, Nila MV, Prajna
NV, Lalitha P and Dharmalingam K: Comparative proteomics of human
male and female tears by two-dimensional electrophoresis. Exp Eye
Res. 92:454–463. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Seamon V, Vellala K, Zylberberg C,
Ponamareva O and Azzarolo AM: Sex hormone regulation of tear
lipocalin in the rabbit lacrimal gland. Exp Eye Res. 87:184–190.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Tong L, Zhou XY, Jylha A, Aapola U, Liu
DN, Koh SK, Tian D, Quah J, Uusitalo H, Beuerman RW and Zhou L:
Quantitation of 47 human tear proteins using high resolution
multiple reaction monitoring (HR-MRM) based-mass spectrometry. J
Proteomics. 115:36–48. 2015. View Article : Google Scholar
|
|
75
|
Aass C, Norheim I, Eriksen EF, Thorsby PM
and Pepaj M: Single unit filter-aided method for fast proteomic
analysis of tear fluid. Anal Biochem. 480:1–5. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Zubarev RA and Makarov A: Orbitrap mass
spectrometry. Anal Chem. 85:5288–5296. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Perry RH, Cooks RG and Noll RJ: Orbitrap
mass spectrometry: Instrumentation, ion motion and applications.
Mass Spectrom Rev. 27:661–699. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Dor M, Eperon S, Lalive PH, Guex-Crosier
Y, Hamedani M, Salvisberg C and Turck N: Investigation of the
global protein content from healthy human tears. Exp Eye Res.
179:64–74. 2019. View Article : Google Scholar
|
|
79
|
Shamsi FA, Chen Z, Liang J, Li K, Al-Rajhi
AA, Chaudhry IA, Li M and Wu K: Analysis and comparison of
proteomic profiles of tear fluid from human, cow, sheep, and camel
eyes. Invest Ophthalmol Vis Sci. 52:9156–9165. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
The definition and classification of dry
eye disease: Report of the definition and classification
subcommittee of the international dry eye WorkShop (2007). Ocul
Surf. 5:75–92. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Craig JP, Nichols KK, Akpek EK, Caffery B,
Dua HS, Joo CK, Liu Z, Nelson JD, Nichols JJ, Tsubota K and
Stapleton F: TFOS DEWS II definition and classification report.
Ocul Surf. 15:276–283. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Shimazaki J: Definition and diagnostic
criteria of dry eye disease: Historical overview and future
directions. Invest Ophthalmol Vis Sci. 59:DES7–DES12. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Abelson MB, Ousler GW III, Nally LA, Welch
D and Krenzer K: Alternative reference values for tear film break
up time in normal and dry eye populations. Adv Exp Med Biol.
506:1121–1125. 2002. View Article : Google Scholar
|
|
84
|
Senchyna M and Wax MB: Quantitative
assessment of tear production: A review of methods and utility in
dry eye drug discovery. J Ocul Biol Dis Infor. 1:1–6. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Nichols KK, Mitchell GL and Zadnik K: The
repeatability of clinical measurements of dry eye. Cornea.
23:272–285. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Huang JF, Zhang Y, Rittenhouse KD,
Pickering EH and McDowell MT: Evaluations of tear protein markers
in dry eye disease: Repeatability of measurement and correlation
with disease. Invest Ophthalmol Vis Sci. 53:4556–4564. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Zhou L, Beuerman RW, Chan CM, Zhao SZ, Li
XR, Yang H, Tong L, Liu S, Stern ME and Tan D: Identification of
tear fluid biomarkers in dry eye syndrome using iTRAQ quantitative
proteomics. J Proteome Res. 8:4889–4905. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Ryckman C, Vandal K, Rouleau P, Talbot M
and Tessier PA: Proinflammatory activities of S100: Proteins
S100A8, S100A9, and S100A8/A9 induce neutrophil chemotaxis and
adhesion. J Immunol. 170:3233–3242. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Danjo Y, Lee M, Horimoto K and Hamano T:
Ocular surface damage and tear lactoferrin in dry eye syndrome.
Acta Ophthalmol (Copenh). 72:433–437. 1994. View Article : Google Scholar
|
|
90
|
Breustedt DA, Schönfeld DL and Skerra A:
Comparative ligand-binding analysis of ten human lipocalins.
Biochim Biophys Acta. 1764:161–173. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Tong L, Zhou L, Beuerman RW, Zhao SZ and
Li XR: Association of tear proteins with meibomian gland disease
and dry eye symptoms. Br J Ophthalmol. 95:848–852. 2011. View Article : Google Scholar
|
|
92
|
Foell D, Wittkowski H, Ren Z, Turton J,
Pang G, Daebritz J, Ehrchen J, Heidemann J, Borody T, Roth J and
Clancy R: Phagocyte-specific S100 proteins are released from
affected mucosa and promote immune responses during inflammatory
bowel disease. J Pathol. 216:183–192. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Versura P, Nanni P, Bavelloni A, Blalock
WL, Piazzi M, Roda A and Campos EC: Tear proteomics in evaporative
dry eye disease. Eye (Lond). 24:1396–1402. 2010. View Article : Google Scholar
|
|
94
|
Fukuda M, Fullard RJ, Willcox MD,
Baleriola-Lucas C, Bestawros F, Sweeney D and Holden BA:
Fibronectin in the tear film. Invest Ophthalmol Vis Sci.
37:459–467. 1996.PubMed/NCBI
|
|
95
|
Perumal N, Funke S, Pfeiffer N and Grus
FH: Proteomics analysis of human tears from aqueous-deficient and
evaporative dry eye patients. Sci Rep. 6:296292016. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Ligtenberg AJ, Veerman EC, Nieuw Amerongen
AV and Mollenhauer J: Salivary agglutinin/glycoprotein-340/DMBT1: A
single molecule with variable composition and with different
functions in infection, inflammation and cancer. Biol Chem.
388:1275–1289. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Boucher Y, Braud A, Dufour E, Agbo-Godeau
S, Baaroun V, Descroix V, Guinnepain MT, Ungeheuer MN, Ottone C and
Rougeot C: Opiorphin levels in fluids of burning mouth syndrome
patients: A case-control study. Clin Oral Investig. 21:2157–2164.
2017. View Article : Google Scholar
|
|
98
|
Pappa A, Chen C, Koutalos Y, Townsend AJ
and Vasiliou V: Aldh3a1 protects human corneal epithelial cells
from ultraviolet- and 4-hydroxy-2-nonenal-induced oxidative damage.
Free Radic Biol Med. 34:1178–1189. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Soria J, Acera A, Merayo-LLoves J, Durán
JA, González N, Rodriguez S, Bistolas N, Schumacher S, Bier FF,
Peter H, et al: Tear proteome analysis in ocular surface diseases
using label-free LC-MS/MS and multiplexed-microarray biomarker
validation. Sci Rep. 7:174782017. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Messmer EM, von Lindenfels V, Garbe A and
Kampik A: Matrix metalloproteinase 9 testing in dry eye disease
using a commercially available point-of-care immunoassay.
Ophthalmology. 123:2300–2308. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Jonsson R, Vogelsang P, Volchenkov R,
Espinosa A, Wahren-Herlenius M and Appel S: The complexity of
Sjogren's syndrome: Novel aspects on pathogenesis. Immunol Lett.
141:1–9. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Kuo MT, Fang PC, Chao TL, Chen A, Lai YH,
Huang YT and Tseng CY: Tear proteomics approach to monitoring
sjogren syndrome or dry eye disease. Int J Mol Sci. 20:19322019.
View Article : Google Scholar
|
|
103
|
Aqrawi LA, Galtung HK, Vestad B, Øvstebø
R, Thiede B, Rusthen S, Young A, Guerreiro EM, Utheim TP, Chen X,
et al: Identification of potential saliva and tear biomarkers in
primary Sjögren's syndrome, utilising the extraction of
extracellular vesicles and proteomics analysis. Arthritis Res Ther.
19:142017. View Article : Google Scholar
|
|
104
|
Aqrawi LA, Galtung HK, Guerreiro EM,
Øvstebø R, Thiede B, Utheim TP, Chen X, Utheim ØA, Palm Ø,
Skarstein K and Jensen JL: Proteomic and histopathological
characterisation of sicca subjects and primary Sjögren's syndrome
patients reveals promising tear, saliva and extracellular vesicle
disease biomarkers. Arthritis Res Ther. 21:1812019. View Article : Google Scholar
|
|
105
|
Wong TT, Zhou L, Li J, Tong L, Zhao SZ, Li
XR, Yu SJ, Koh SK and Beuerman RW: Proteomic profiling of
inflammatory signaling molecules in the tears of patients on
chronic glaucoma medication. Invest Ophthalmol Vis Sci.
52:7385–7391. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Csősz É, Deák E, Kalló G, Csutak A and
Tőzsér J: Diabetic retinopathy: Proteomic approaches to help the
differential diagnosis and to understand the underlying molecular
mechanisms. J Proteomics. 150:351–358. 2017. View Article : Google Scholar
|
|
107
|
Csősz É, Boross P, Csutak A, Berta A, Tóth
F, Póliska S, Török Z and Tőzsér J: Quantitative analysis of
proteins in the tear fluid of patients with diabetic retinopathy. J
Proteomics. 75:2196–2204. 2012. View Article : Google Scholar
|
|
108
|
Zhou X, Qu J, Xie R, Wang R, Jiang L, Zhao
H, Wen J and Lu F: Normal development of refractive state and
ocular dimensions in guinea pigs. Vision Res. 46:2815–2823. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Bartalena L and Fatourechi V:
Extrathyroidal manifestations of Graves' disease: A 2014 update. J
Endocrinol Invest. 37:691–700. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Lehmann GM, Garcia-Bates TM, Smith TJ,
Feldon SE and Phipps RP: Regulation of lymphocyte function by
PPARgamma: Relevance to thyroid eye disease-related inflammation.
PPAR Res. 2008:8959012008. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Mourits MP, Prummel MF, Wiersinga WM and
Koornneef L: Clinical activity score as a guide in the management
of patients with Graves' ophthalmopathy. Clin Endocrinol (Oxf).
47:9–14. 1997. View Article : Google Scholar
|
|
112
|
Turck N, Eperon S, De Los Angeles Gracia
M, Obéric A and Hamédani M: Thyroid-associated orbitopathy and
biomarkers: Where we are and what we can hope for the future. Dis
Markers. 2018:70101962018. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Chelala E, El Rami H, Dirani A, Fakhoury H
and Fadlallah A: Extensive superior limbic keratoconjunctivitis in
Graves' disease: Case report and mini-review of the literature.
Clin Ophthalmol. 9:467–468. 2015.PubMed/NCBI
|
|
114
|
Matheis N, Okrojek R, Grus FH and Kahaly
GJ: Proteomics of tear fluid in thyroid-associated orbitopathy.
Thyroid. 22:1039–1045. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Torsteinsdóttir I, Hâkansson L, Hällgren
R, Gudbjörnsson B, Arvidson NG and Venge P: Serum lysozyme: A
potential marker of monocyte/macrophage activity in rheumatoid
arthritis. Rheumatology (Oxford). 38:1249–1254. 1999. View Article : Google Scholar
|
|
116
|
Barrett AJ: The cystatins: Small protein
inhibitors of cysteine proteinases. Prog Clin Biol Res.
180:105–116. 1985.PubMed/NCBI
|
|
117
|
Matheis N, Grus FH, Breitenfeld M, Knych
I, Funke S, Pitz S, Ponto KA, Pfeiffer N and Kahaly GJ: Proteomics
differentiate between thyroid-associated orbitopathy and dry eye
syndrome. Invest Ophthalmol Vis Sci. 56:2649–2656. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Wiesner J and Vilcinskas A: Antimicrobial
peptides: The ancient arm of the human immune system. Virulence.
1:440–464. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Ozyildirim AM, Wistow GJ, Gao J, Wang J,
Dickinson DP, Frierson HF Jr and Laurie GW: The lacrimal gland
transcriptome is an unusually rich source of rare and poorly
characterized gene transcripts. Invest Ophthalmol Vis Sci.
46:1572–1580. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Barka T, Asbell PA, van der Noen H and
Prasad A: Cystatins in human tear fluid. Curr Eye Res. 10:25–34.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Turcu AF, Kumar S, Neumann S, Coenen M,
Iyer S, Chiriboga P, Gershengorn MC and Bahn RS: A small molecule
antagonist inhibits thyrotropin receptor antibody-induced orbital
fibroblast functions involved in the pathogenesis of Graves
ophthalmopathy. J Clin Endocrinol Metab. 98:2153–2159. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Aass C, Norheim I, Eriksen EF, Børnick EC,
Thorsby PM and Pepaj M: Comparative proteomic analysis of tear
fluid in Graves' disease with and without orbitopathy. Clin
Endocrinol (Oxf). 85:805–812. 2016. View Article : Google Scholar
|
|
123
|
McIntosh RS, Cade JE, Al-Abed M,
Shanmuganathan V, Gupta R, Bhan A, Tighe PJ and Dua HS: The
spectrum of antimicrobial peptide expression at the ocular surface.
Invest Ophthalmol Vis Sci. 46:1379–1385. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Wei YH, Chen WL, Hu FR and Liao SL: In
vivo confocal microscopy of bulbar conjunctiva in patients with
Graves' ophthalmopathy. J Formos Med Assoc. 114:965–972. 2015.
View Article : Google Scholar
|
|
125
|
Kishazi E, Dor M, Eperon S, Oberic A,
Hamedani M and Turck N: Thyroid-associated orbitopathy and tears: A
proteomics study. J Proteomics. 170:110–116. 2018. View Article : Google Scholar
|
|
126
|
Paraoan L, Grierson I and Maden BE:
Analysis of expressed sequence tags of retinal pigment epithelium:
Cystatin C is an abundant transcript. Int J Biochem Cell Biol.
32:417–426. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Yoshida A, Hsu LC and Dave V: Retinal
oxidation activity and biological role of human cytosolic aldehyde
dehydrogenase. Enzyme. 46:239–244. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Sahu B and Maeda A: Retinol dehydrogenases
regulate vitamin A metabolism for visual function. Nutrients.
8:7462016. View Article : Google Scholar :
|
|
129
|
Weinreb RN, Aung T and Medeiros FA: The
pathophysiology and treatment of glaucoma: A review. JAMA.
311:1901–1911. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Bourne RR, Taylor HR, Flaxman SR, Keeffe
J, Leasher J, Naidoo K, Pesudovs K, White RA, Wong TY, Resnikoff S,
et al: Number of people blind or visually impaired by glaucoma
worldwide and in world regions 1990-2010: A meta-analysis. PLoS
One. 11:e01622292016. View Article : Google Scholar
|
|
131
|
Harwerth RS and Quigley HA: Visual field
defects and retinal ganglion cell losses in patients with glaucoma.
Arch Ophthalmol. 124:853–859. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Rahmani B, Tielsch JM, Katz J, Gottsch J,
Quigley H, Javitt J and Sommer A: The cause-specific prevalence of
visual impairment in an urban population. The baltimore eye survey.
Ophthalmology. 103:1721–1726. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Braunger BM, Fuchshofer R and Tamm ER: The
aqueous humor outflow pathways in glaucoma: A unifying concept of
disease mechanisms and causative treatment. Eur J Pharm Biopharm.
95:173–181. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Elhawy E, Kamthan G, Dong CQ and Danias J:
Pseudoexfoliation syndrome, a systemic disorder with ocular
manifestations. Hum Genomics. 6:222012. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Weinreb RN, Leung CK, Crowston JG,
Medeiros FA, Friedman DS, Wiggs JL and Martin KR: Primary
open-angle glaucoma. Nat Rev Dis Primers. 2:160672016. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Pieragostino D, Bucci S, Agnifili L,
Fasanella V, D'Aguanno S, Mastropasqua A, Ciancaglini M,
Mastropasqua L, Di Ilio C, Sacchetta P, et al: Differential protein
expression in tears of patients with primary open angle and
pseudoexfoliative glaucoma. Mol Biosyst. 8:1017–1028. 2012.
View Article : Google Scholar
|
|
137
|
Pieragostino D, Agnifili L, Fasanella V,
D'Aguanno S, Mastropasqua R, Di Ilio C, Sacchetta P, Urbani A and
Del Boccio P: Shotgun proteomics reveals specific modulated protein
patterns in tears of patients with primary open angle glaucoma
naïve to therapy. Mol Biosyst. 9:1108–1116. 2013. View Article : Google Scholar : PubMed/NCBI
|