Introduction
Intratumor heterogeneity is one of the recognized
characteristics of human tumors, and occurs on multiple levels,
such as the genetic, protein and macroscopic level in a wide range
of tumors, including breast, colorectal (CRC), non-small cell lung
(NSCLC), prostate, ovarian, pancreatic, gastric, and brain cancer
and renal clear cell carcinoma (1). In recent years, many studies have
focused on the heterogeneity found in primary tumors and related
metastases with the consideration that evaluation of metastatic
rather than primary sites could be of clinical relevance. Numerous
reports have evaluated the genetic heterogeneity in primary tumors
and corresponding metastases in a range of solid tumors such as
breast cancer (2–9), CRC (10–13)
and NSCLC (14,15). Heterogeneity in primary tumors and
related metastases may result in the failure of antitumor
therapies, particularly in targeted therapies for the treatment of
cancer (16).
However, without a suitable tumor model we cannot
elucidate whether such heterogeneity results in different responses
to anticancer therapy. In a previous study, we successfully
established the patient-derived tumor tissue (PDTT) xenograft
models of colon carcinoma with lymphatic and hepatic metastases
(17). The ideal biological
characteristics of such PDTT xenograft models, as previously
described (17), confirmed our
hypothesis that such PDTT models would help us investigate the
underlying mechanism of the differences in heterogeneity-related
anticancer therapy response in primary colon carcinoma and its
corresponding lymphatic and hepatic metastases.
In this study, PDTT xenograft models of colon
carcinoma with lymphatic and hepatic metastases were used to
evaluate the response to EGFR- and VEGF-targeted therapies. We also
investigated heterogeneity in primary colon carcinoma tissue and
its corresponding lymphatic and hepatic metastatic tissues from the
same metastatic colon carcinoma patient focusing on the cell
signaling pathway proteins.
Materials and methods
Reagents and drugs
Anti-Akt, anti-ERK, anti-MAPK and anti-mTOR
antibodies, and phosphorylation-specific antibodies against Akt
(Ser308 and Ser473), ERK
(Thr202/Tyr204), MAPK
(Thr180/Tyr182) and mTOR (Ser2448)
as well as the antibody against cleaved caspase-3 were purchased
from Cell Signaling Technology Inc. (Cell Signaling, Beverly, MA).
The antibodies against VEGF and EGFR were purchased from Epitomics
Inc. (Burlingame, CA). The antibody against GAPDH was purchased
from Santa Cruz Biotechnology, Inc. (Santa Cruz, CA). Horseradish
peroxidase-conjugated secondary antibodies were purchased from
Santa Cruz Biotechnology, Inc. (Santa Cruz, CA). Chemiluminescent
detection system was purchased from Amersham Pharmacia Biotech
(Arlington Heights, IL). Bevacizumab (Avastin®) was
purchased from Roche, Inc. (Roche, USA). Cetuximab was purchased
from Merck, Inc. (Merck, Darmstadt, Germany).
Patient and tissue samples
Tumor specimens were obtained at initial surgery
from a 40-year-old female colon carcinoma patient with lymphatic
and hepatic metastases. Prior written informed consent was obtained
from the patient and the study received approval from the Ethics
Board of the First Affiliated Hospital, College of Medicine,
Zhejiang University. The patient had not received chemotherapy or
radiation therapy before surgery. The histological type was
determined according to WHO criteria. The tumor was diagnosed as
mucinous adenocarcinoma (T3N2M1). The tumor samples of colon
carcinoma with lymphatic and hepatic metastases were put into
medium immediately after surgical resection under sterile
conditions and transported without delay to the animal
facility.
Establishment of xenografts and treatment
protocol
Four-to six-week-old female BALB/c nude mice
purchased from Slaccas (Slaccas Laboratory Animal, Shanghai, China)
were housed in a barrier facility and acclimated to 12-h light/12-h
dark cycles for at least three days before use. The use of
experimental animals adhered to the ‘Principles of Laboratory
Animal Care’ (NIH publication No. 85–23, revised in 1985). All
experiments were approved by the Institutional Animal Care and Use
Committee of Zhejiang University [approval ID: SYXK(ZHE)2005–0072].
The method to establish the PDTT xenograft models of human colon
carcinoma with lymphatic and hepatic metastases were described
previously (1,17–20).
Xenografts from this second mouse-to-mouse passage
were allowed to grow to a size of 200 mm3, at which time
mice were randomized into the following three cohorts: cohort of
primary colon carcinoma xenografts, cohort of lymphatic metastasis
xenografts, and cohort of hepatic metastasis xenografts. In each
cohort, xenografts were randomized into four groups with 10 mice in
each group: (a) control (saline 100 μl i.v. + 200 μl
i.p., twice per week); (b) bevacizumab (Avastin), 10 mg/kg in 100
μl, i.v., twice per week; (c) cetuximab, 10 mg/kg in 200
μl, i.p., twice per week; (d) cetuximab, 10 mg/kg in 200
μl, i.p., twice per week + bevacizumab, 10 mg/kg in 100
μl, i.v., twice per week. Mice were treated for 21 days,
monitored twice per week for signs of toxicity, and were weighed
once a week. Tumor size was evaluated twice a week by caliper
measurements using the following formula: tumor volume = (length ×
width2)/2. Relative tumor growth inhibition (TGI) was
calculated by relative tumor growth of treated mice divided by
relative tumor growth of control mice (T/C). Experiments were
terminated on day 30. This experiment was repeated twice with
similar results.
DNA extraction and mutation analyses
DNA was extracted from paraffin-embedded samples of
colon carcinoma with lymphatic and hepatic metastases. For every
tumor tissue, 10-μm sections were prepared, and an
additional representative 2-μm section was deparaffinized,
stained with haematoxylin and eosin, and analyzed for detailed
morphology. Regions of tumor tissue were marked, and this tissue
was extracted with 0.2 M sodium hydroxide in 1 mM edetic acid and
neutralized with 100 mM Tris-TE (pH 6.5). After extraction, DNA was
purified with Qiagen PCR purification kit (Qiagen, Hilden,
Germany). KRAS gene exon 1 was analysed at codons 12 and 13 with
pyrosequencing using a previously described assay which has been
shown to be of greater sensitivity (21).
Immunohistochemistry
Selected tumor specimens were fixed in 10%
neutral-buffered formalin and embedded in paraffin. Sections (5
μm) were cut, dewaxed, rehydrated, and subjected to antigen
retrieval. After blocking endogenous peroxidase activity, the
sections were incubated with the primary antibodies against EGFR
(1:100) and VEGF (1:100) overnight at 4°C. Immunohistochemistry was
performed using the streptavidin-biotin peroxidase complex method
(Lab Vision, Fremont, CA). The slides were examined and images were
captured using an Olympus BX60 (Olympus, Japan). Sections known to
stain positively were incubated in each batch and negative controls
were also prepared by replacing the primary antibody with preimmune
sera.
Western blotting
Protein expression profiles were analyzed by western
blotting as previously described (22–24).
Briefly, lysates for immunoblotting were prepared by adding lysis
buffer [50 mM Tris-HCl (pH 7.4), 1% Nonidet P-40, 0.5% sodium
deoxycholate, 150 mM NaCl, 0.02% sodium azide, and 0.1% SDS]
containing protease and phosphatase inhibitors (Sigma, St. Louis,
MO) to the tumor tissue homogenized in fluid nitrogen. After
centrifugation at 15,000 rpm at 4°C for 10 min, the supernatants
were collected, and the protein concentration was determined using
Bio-Rad protein assay kit (Bio-Rad, Hercules, CA). Protein extracts
of tumor lysates (30 μg) were added to a loading buffer [10
mmol/l Tris-HCl (pH 6.8), 1% SDS, 25% glycerol, 0.1 mmol/l
mercaptoethanol, and 0.03% bromophenol blue], boiled, and separated
on 8–12% (w/v) polyacrylamide gels in the presence of SDS.
Molecular weights of the immunoreactive proteins were estimated
based on the relative migration with colored molecular weight
protein markers (Amersham Pharmacia Biotech, Piscataway, NJ).
Following electrophoresis, the protein blots were
electro-transferred to PVDF membranes (Millipore, Billerica, MA).
The membranes were then blocked at room temperature with 5% nonfat
milk in TBS [10 mmol/l Tris-HCl (pH 7.5), 0.5 mol/l NaCl, and 0.05%
(v/v) Tween-20] buffer for 1 h. The primary antibodies were diluted
at 1:1,000 and the membranes were incubated with primary antibodies
overnight at 4°C. The antibodies tested were anti-Akt, anti-ERK,
anti-MAPK, anti-mTOR antibodies, anti-EGFR, anti-VEGF, anti-cleaved
caspase-3, and phosphorylation-specific antibodies against Akt
(Ser308 and Ser473), ERK
(Thr202/Tyr204), MAPK
(Thr180/Tyr182) and mTOR
(Ser2448). The following day, the membranes were washed
and incubated for 1 h at room temperature with rabbit
immunoglobulin G-horseradish peroxidase-conjugated secondary
antibodies (Santa Cruz Biotechnology), at a final dilution of
1:5,000. After washing thrice with TBS, antibody binding was
visualized using enhanced chemiluminescence detection system
(SuperSignal West Pico, Pierce) as described by the manufacturer
and autoradiography. To show equal protein loading, the blots were
stripped and reprobed for GAPDH. This experiment was repeated three
times with similar results.
Statistical analysis
Drug sensitivity data are presented as the mean ±
SEM and analyzed by SPSS 16.0 software. Difference among mean of
the groups is determined with one-way ANOVA. Comparison is
considered to be statistically significant at p<0.05.
Results
PDTT xenograft models of primary colon
carcinoma and related metastases have different response rates to
dual-inhibition of EGFR and VEGF
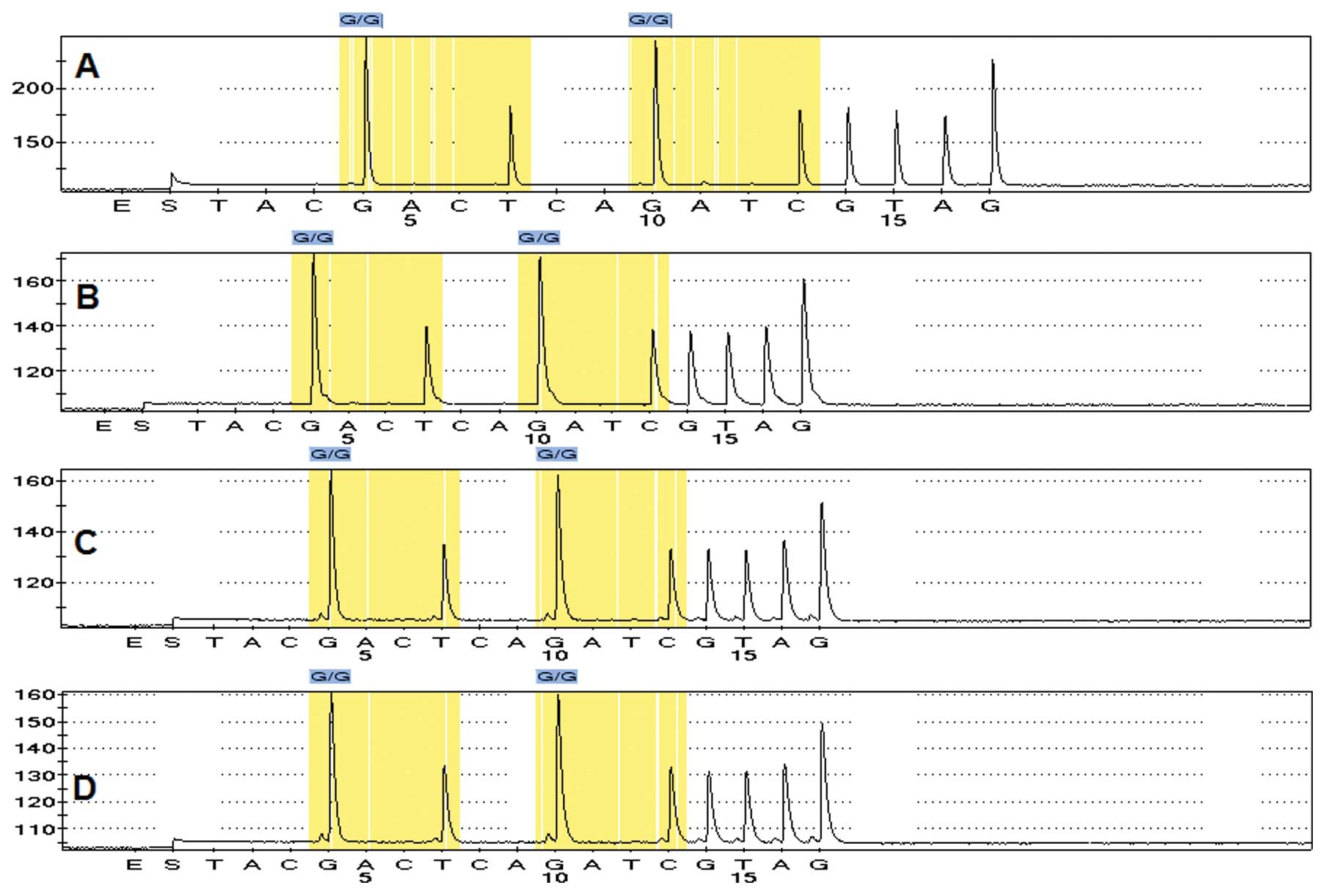
It is necessary to ascertain the molecular basis for
the response to cetuximab in metastatic colon carcinoma. For this
purpose, we assessed the mutation status of the KRAS gene exon 1 at
codons 12 and 13 in primary colon carcinoma and its lymphatic and
hepatic metastases. Our results revealed that the KRAS gene status
in the three tumor sites are all wild-type (Fig. 1).
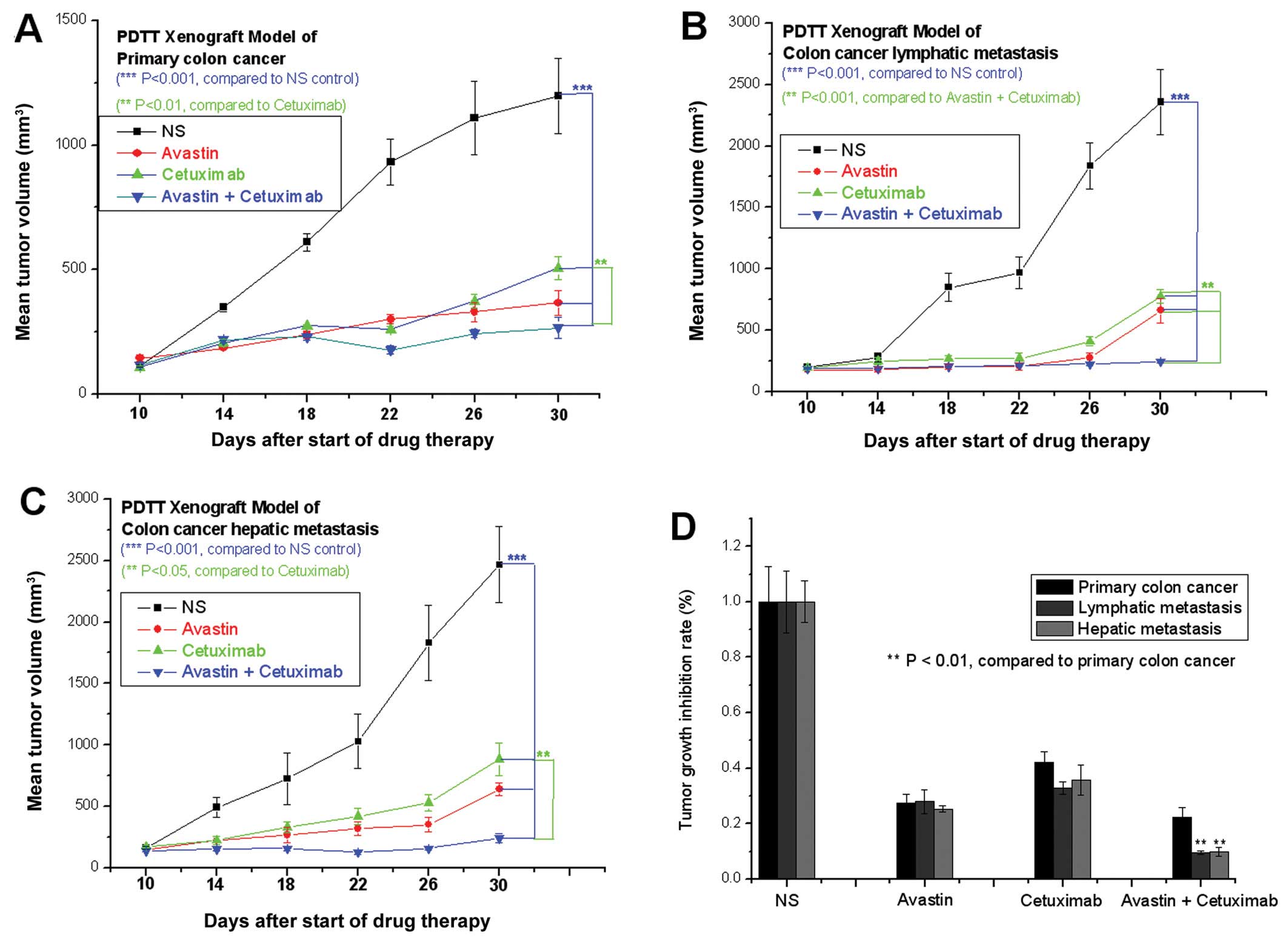
We subsequently evaluated the therapy response of
cetuximab in combination with bevacizumab in the primary colon
carcinoma and its corresponding lymphatic and hepatic metastases
using the PDTT xenograft models. Our results showed that all
xenografts of primary colon carcinoma and corresponding lymphatic
and hepatic metastases in nude mice responded to the
dual-inhibition of EGFR and VEGF (Fig.
2A–C). However, dual-inhibition of EGFR and VEGF resulted in
significantly different relative TGI in xenografts of primary colon
carcinoma (22.2%) and corresponding lymphatic (9.6%) and hepatic
metastasis (9.9%) (Fig. 2A–D). Our
results demonstrate that primary colon carcinoma and its
corresponding lymphatic and hepatic metastases have different
response rates to anti-EGFR and anti-VEGF therapies.
Heterogeneity in primary colon carcinoma
and its corresponding lymphatic and hepatic metastases
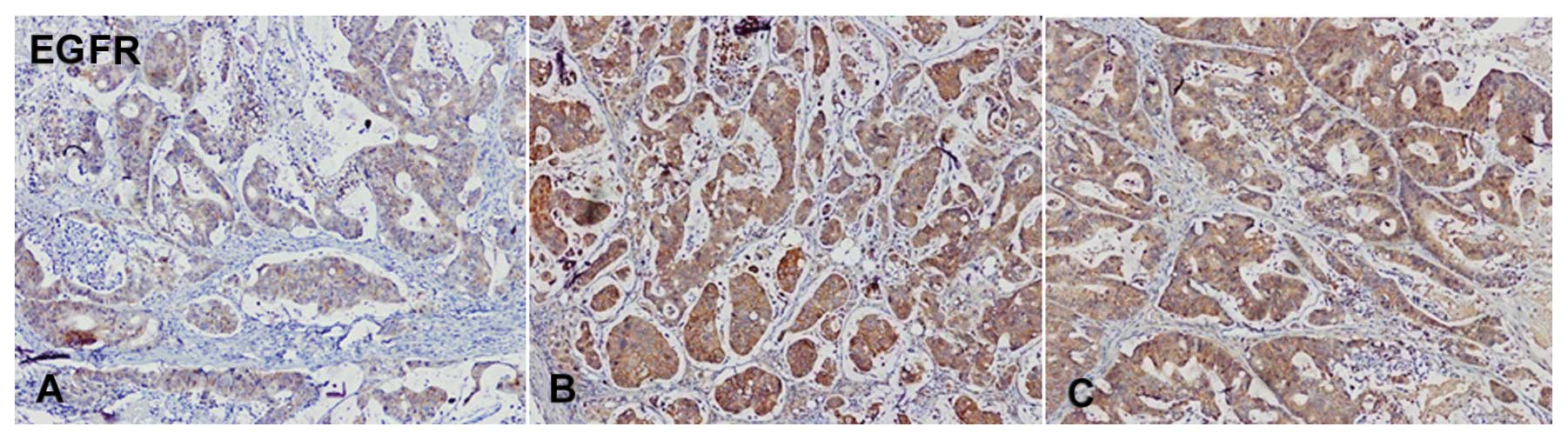
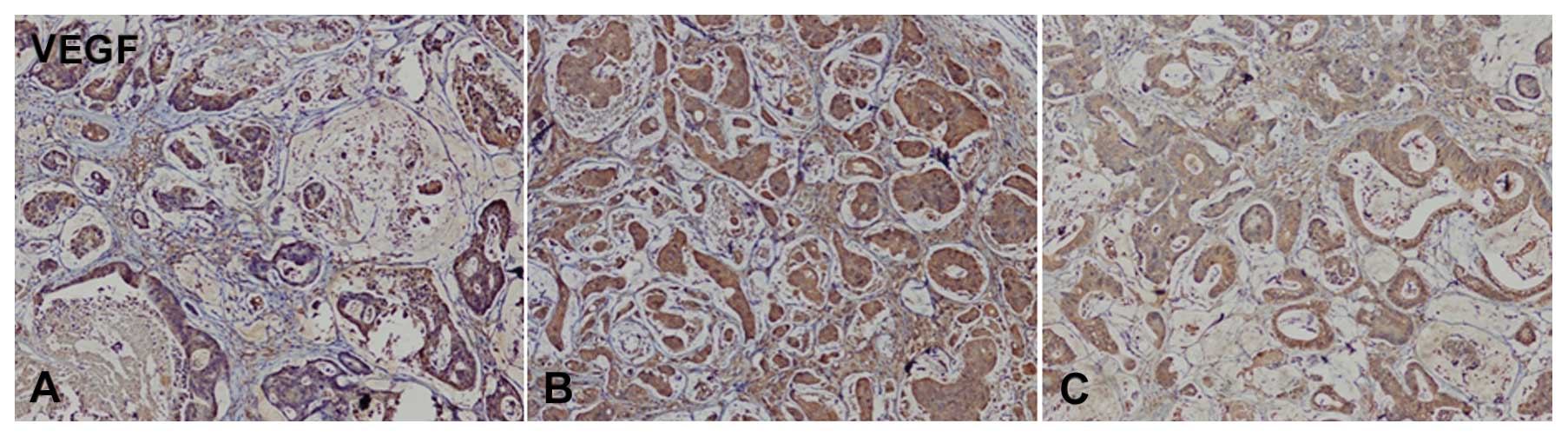
Immunohistochemical staining revealed that EGFR and
VEGF expression levels in primary colon carcinoma tissue are
different from those in its lymphatic and hepatic metastases. Our
findings reveal that the expression levels of EGFR (Fig. 3) and VEGF (Fig. 4) in metastatic tissues were higher
than those in primary colon carcinoma tissue.
In this study, the expression levels of the EGFR and
VEGF downstream signaling pathway proteins were further determined
using western blotting. The expression levels of EGFR, VEGF, pAkt,
and mTOR in metastatic tissues were found to be higher than those
in primary colon carcinoma tissue (Fig. 5), while the expression levels of
Akt, ERK, MAPK, and pmTOR in primary colon carcinoma tissue were
higher than those in metastatic tissues (Fig. 5). Hepatic metastasis had the
highest expression levels of pERK and pMAPK (Fig. 5). Our results indicate that the
heterogeneity of EGFR- and VEGF-related signaling pathway proteins
exist in primary colon carcinoma and its corresponding lymphatic
and hepatic metastases. Furthemore, our findings indicate that
heterogeneity in primary colon carcinoma and its corresponding
lymphatic and hepatic metastases may partially make contribute to
differences in response to anti-EGFR or anti-VEGF targeted
therapies.
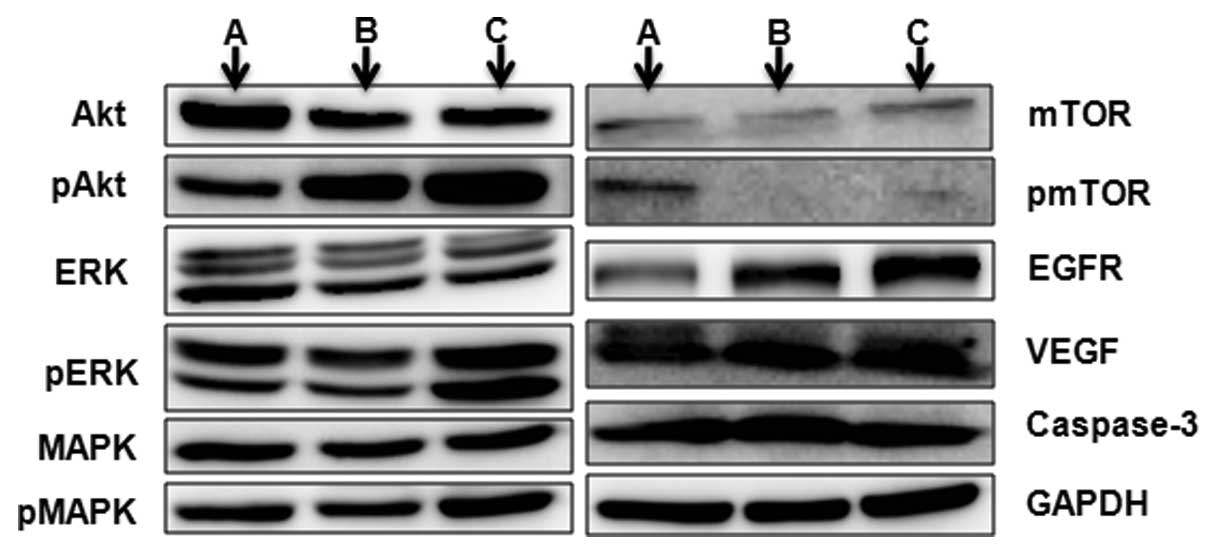 | Figure 5Immunoblotting data of the proteins
Akt, pAkt (Ser308 and Ser473), ERK, pERK
(Thr202/Tyr204), MAPK, pMAPK
(Thr180/Tyr182), mTOR, pmTOR
(Ser2448), EGFR, VEGF, cleaved caspase-3, and GAPDH (as
loading control) of (A) primary colon carcinoma and its
corresponding (B) lymphatic and (C) hepatic metastases. |
Discussion
The main purpose of investigating the heterogeneity
in primary tumors and their corresponding metastases is to evaluate
the effects of such heterogeneity on the efficacy of anticancer
therapy and cancer patients' prognosis. As we have previously
reported (1,17,19),
the PDTT xenograft model which has a sound establishing method and
a retained similarity to the corresponding original donor tumors in
histological presentation and biological behavior, such as protein
expression, tumor biomarker status, and genomic and genetic status,
has the potential to be a good strategy to achieve our purpose.
In our previous study, we established the PDTT
xenograft models of colon carcinoma with lymphatic and hepatic
metastases (17). The biological
characteristics of such PDTT xenograft models, as previously
described (17), confirmed our
belief that such PDTT models would aid in our investigation of the
underlying mechanism of heterogeneity-related anticancer therapy
response differences in primary colon carcinoma and its
corresponding lymphatic and hepatic metastases. Based on this
hypothesis and considering that the KRAS gene status in the three
tumor sites are all wild-type, the drug sensitivity of bevacizumab
(Avastin) in combination with cetuximab in the primary colon
carcinoma and its corresponding lymphatic and hepatic metastases
was evaluated in this study using the PDTT xenograft models.
In the present study we also investigated the
heterogeneity in primary colon carcinoma and its corresponding
lymphatic and hepatic metastases focusing on the cell signaling
pathway proteins using immunohistochemical staining and western
blotting. We found that the expression levels of EGFR, VEGF,
Akt/pAkt, ERK/pERK, MAPK/pMAPK, and mTOR/pmTOR were different in
primary colon carcinoma and matched lymphatic and hepatic
metastases, although the KRAS gene status in all was wild-type.
With regard to CRC, the therapeutic benefit of
EGFR-targeted monoclonal antibodies such as cetuximab and
panitumumab has been established in various studies (25–27).
Notably, no correlation was observed between the expression levels
of EGFR and therapeutic success (25–27),
and even patients with tumors apparently lacking EGFR expression
responded to antibody therapy in up to 25% of the cases (28–30).
In our study, xenografts of primary colon carcinoma and its
corresponding lymphatic and hepatic metastases all responded to
cetuximab (Fig. 2A–C). However, no
significant difference could be observed in these groups (Fig. 2D) although they have different
expression levels of EGFR (Fig. 3
and 5).
Across a wide range of human tumors and/or cell
lines, expression of VEGF has been shown to lead to the development
and maintenance of a vascular network that promotes tumor growth
and metastasis. Moreover, a large and growing body of evidence
indicates that both VEGF gene expression and production are
associated closely with poor prognosis (31–35).
However, no correlation was observed between the expression levels
of VEGF and clinical outcomes of VEGF targeted therapy (36). Our findings show that primary colon
carcinoma and its corresponding lymphatic and hepatic metastases
have different expression levels of VEGF (Fig. 4 and 5), but they all responded to bevacizumab
(Fig. 2A–C), and no significant
difference was observed in these groups (Fig. 2D).
Moreover, xenografts of primary colon carcinoma and
its corresponding lymphatic and hepatic metastases have different
response rates to treatment of bevacizumab in combination with
cetuximab (Fig. 2D) although all
xenografts responded to the dual-inhibition of EGFR and VEGF
(Fig. 2A–C). Our results
demonstrated that dual-inhibition of EGFR and VEGF could result in
significantly different response rates in primary colon carcinoma
and corresponding metastases if the EGFR and VEGF expression levels
are different in these tumors. Our results indicate that
heterogeneity in primary colon carcinoma and its corresponding
lymphatic and hepatic metastases may result in differences in
response to dual-inhibition of EGFR and VEGF.
In this study, we investigated heterogeneity in
primary colon carcinoma and its corresponding lymphatic and hepatic
metastases focusing on the cell signaling pathway proteins, and we
found that the levels of EGFR, VEGF, Akt/pAkt, ERK/pERK,
MAPK/pMAPK, and mTOR/pmTOR were different in primary colon
carcinoma and matched lymphatic and hepatic metastases.
Furthermore, with the help of PDTT xenograft models, we
demonstrated that such heterogeneity would result in different
responses to anti-EGFR and anti-VEGF targeted therapies. The PDTT
xenograft model could be a good in vivo tool to examine whether the
primary tumors and corresponding metastases have different
responses to the same anticancer drugs.
Acknowledgements
This work was supported by the State
Key Basic Research and Development Program of China (973 Program,
Grant No. 2009CB521704), National High-tech Research &
Development Program of China (863 Program, Grant No. 2006AA02A245),
National Natural Science Foundation of China (Grant No. 81000894),
Zhejiang Provincial Science and Technology Projects (Grants No.
2009C13021, 2011C23087), Zhejiang Provincial Medical and Healthy
Science and Technology Projects (Grants No. 2011KYB137), Science
Research Fund of Taizhou (Grant No. A102KY09), Science Research
Fund of Shaoxing (Grants No. 2011D10013) and Science Research Fund
of Zhuji (Grants No. 2011CC7874).
References
|
1
|
Jin KT, He KF, Teng F, Han N, Li GL, Xu ZZ
and Teng LS: Heterogeneity in primary tumors and corresponding
metastases: could it provide us with any hints to personalize
cancer therapy? Pers Med. 8:175–182. 2011. View Article : Google Scholar
|
|
2
|
Gong Y, Booser DJ and Sneige N: Comparison
of HER-2 status determined by fluorescence in situ hybridization in
primary and metastatic breast carcinoma. Cancer. 103:1763–1769.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gancberg D, Di Leo A, Cardoso F, Rouas G,
Pedrocchi M, Paesmans M, Verhest A, Bernard-Marty C, Piccart MJ and
Larsimont D: Comparison of HER-2 status between primary breast
cancer and corresponding distant metastatic sites. Ann Oncol.
13:1036–1043. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Regitnig P, Schippinger W, Lindbauer M,
Samonigg H and Lax SF: Change of HER-2/neu status in a subset of
distant metastases from breast carcinomas. J Pathol. 203:918–926.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bozzetti C, Personeni N, Nizzoli R, Guazzi
A, Flora M, Bassano C, Negri F, Martella E, Naldi N, Franciosi V
and Cascinu S: HER-2/neu amplification by fluorescence in situ
hybridization in cytologic samples from distant metastatic sites of
breast carcinoma. Cancer. 99:310–315. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tanner M, Järvinen P and Isola J:
Amplification of HER-2/neu and topoisomerase IIalpha in primary and
metastatic breast cancer. Cancer Res. 61:5345–5348. 2001.PubMed/NCBI
|
|
7
|
Tapia C, Savic S, Wagner U, et al: HER2
gene status in primary breast cancers and matched distant
metastases. Breast Cancer Res. 9:R312007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Akcakanat A, Sahin A, Shaye AN, Velasco MA
and Meric-Bernstam F: Comparison of Akt/mTOR signaling in primary
breast tumors and matched distant metastases. Cancer.
112:2352–2358. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu JM, Fackler MJ, Halushka MK, et al:
Heterogeneity of breast cancer metastases: comparison of
therapeutic target expression and promoter methylation between
primary tumors and their multifocal metastases. Clin Cancer Res.
14:1938–1946. 2008. View Article : Google Scholar
|
|
10
|
Baldus SE, Schaefer KL, Engers R, Hartleb
D, Stoecklein NH and Gabbert HE: Prevalence and heterogeneity of
KRAS, BRAF, and PIK3CA mutations in primary colorectal
adenocarcinomas and their corresponding metastases. Clin Cancer
Res. 16:790–799. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Molinari F, Martin V, Saletti P, De Dosso
S, Spitale A, Camponovo A, Bordoni A, Crippa S, Mazzucchelli L and
Frattini M: Differing deregulation of EGFR and downstream proteins
in primary colorectal cancer and related metastatic sites may be
clinically relevant. Br J Cancer. 100:1087–1094. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Scartozzi M, Bearzi I, Berardi R,
Mandolesi A, Fabris G and Cascinu S: Epidermal growth factor
receptor (EGFR) status in primary colorectal tumors does not
correlate with EGFR expression in related metastatic sites:
implications for treatment with EGFR-targeted monoclonal
antibodies. J Clin Oncol. 22:4772–4778. 2004. View Article : Google Scholar
|
|
13
|
Scartozzi M, Bearzi I, Berardi R,
Mandolesi A, Pierantoni C and Cascinu S: Epidermal growth factor
receptor (EGFR) downstream signalling pathway in primary colorectal
tumours and related metastatic sites: optimising EGFR-targeted
treatment options. Br J Cancer. 97:92–97. 2007. View Article : Google Scholar
|
|
14
|
Sasatomi E, Finkelstein SD, Woods JD,
Bakker A, Swalsky PA, Luketich JD, Fernando HC and Yousem SA:
Comparison of accumulated allele loss between primary tumor and
lymph node metastasis in stage II non-small cell lung carcinoma:
implications for the timing of lymph node metastasis and prognostic
value. Cancer Res. 62:2681–2689. 2002.PubMed/NCBI
|
|
15
|
Park S, Holmes-Tisch AJ, Cho EY, et al:
Discordance of molecular biomarkers associated with epidermal
growth factor receptor pathway between primary tumors and lymph
node metastasis in non-small cell lung cancer. J Thorac Oncol.
4:809–815. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li Z, Jin K, Lan H and Teng L:
Heterogeneity in primary colorectal cancer and its corresponding
metastases: a potential reason of EGFR-targeted therapy failure?
Hepatogastroenterology. 58:411–416. 2011.PubMed/NCBI
|
|
17
|
Jin K, Li G, Cui B, et al: Assessment of a
novel VEGF targeted agent using patient-derived tumor tissue
xenograft models of colon carcinoma with lymphatic and hepatic
metastases. PLoS One. 6:e283842011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jin K, Teng L, Shen Y, He K, Xu Z and Li
G: Patient-derived human tumour tissue xenografts in
immunodeficient mice: a systematic review. Clin Transl Oncol.
12:473–480. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jin KT, He KF, Li GL and Teng LS:
Personalized cancer therapy using a patient-derived tumor tissue
xenograft model: a translational field worthy of exploring further?
Pers Med. 7:597–606. 2010. View Article : Google Scholar
|
|
20
|
Jin K, He K, Han N, Li G, Wang H, Xu Z,
Jiang H, Zhang J and Teng L: Establishment of a PDTT xenograft
model of gastric carcinoma and its application in personalized
therapeutic regimen selection. Hepatogastroenterology.
58:1814–1822. 2011.PubMed/NCBI
|
|
21
|
Ogino S, Kawasaki T, Brahmandam M, Yan L,
Cantor M, Namgyal C, Mino-Kenudson M, Lauwers GY, Loda M and Fuchs
CS: Sensitive sequencing method for KRAS mutation detection by
Pyrosequencing. J Mol Diagn. 7:413–421. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huynh H, Chow PK, Ooi LL and Soo KC: A
possible role for insulin-like growth factor-binding protein-3
autocrine/paracrine loops in controlling hepatocellular carcinoma
cell proliferation. Cell Growth Differ. 13:115–122. 2002.
|
|
23
|
Rubio-Viqueira B, Jimeno A, Cusatis G, et
al: An in vivo platform for translational drug development in
pancreatic cancer. Clin Cancer Res. 12:4652–4661. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Perez-Soler R, Kemp B, Wu QP, Mao L, Gomez
J, Zeleniuch-Jacquotte A, Yee H, Lee JS, Jagirdar J and Ling YH:
Response and determinants of sensitivity to paclitaxel in human
non-small cell lung cancer tumors heterotransplanted in nude mice.
Clin Cancer Res. 6:4932–4938. 2000.PubMed/NCBI
|
|
25
|
Cunningham D, Humblet Y, Siena S, Khayat
D, Bleiberg H, Santoro A, Bets D, Mueser M, Harstrick A, Verslype
C, Chau I and Van Cutsem E: Cetuximab monotherapy and cetuximab
plus irinotecan in irinotecan-refractory metastatic colorectal
cancer. N Engl J Med. 351:337–345. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Saltz LB, Meropol NJ, Loehrer PJ Sr,
Needle MN, Kopit J and Mayer RJ: Phase II trial of cetuximab in
patients with refractory colorectal cancer that expresses the
epidermal growth factor receptor. J Clin Oncol. 22:1201–1208. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Amado RG, Wolf M, Peeters M, et al:
Wild-type KRAS is required for panitumumab efficacy in patients
with metastatic colorectal cancer. J Clin Oncol. 26:1626–1634.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cappuzzo F, Varella-Garcia M, Finocchiaro
G, et al: Primary resistance to cetuximab therapy in EGFR
FISH-positive colorectal cancer patients. Br J Cancer. 99:83–89.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Moroni M, Veronese S, Benvenuti S,
Marrapese G, Sartore-Bianchi A, Di Nicolantonio F, Gambacorta M,
Siena S and Bardelli A: Gene copy number for epidermal growth
factor receptor (EGFR) and clinical response to anti-EGFR treatment
in colorectal cancer: a cohort study. Lancet Oncol. 6:279–286.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Benvenuti S, Sartore-Bianchi A, Di
Nicolantonio F, Zanon C, Moroni M, Veronese S, Siena S and Bardelli
A: Oncogenic activation of the RAS/RAF signaling pathway impairs
the response of metastatic colorectal cancers to anti-epidermal
growth factor receptor antibody therapies. Cancer Res.
67:2643–2648. 2007. View Article : Google Scholar
|
|
31
|
Foekens JA, Peters HA, Grebenchtchikov N,
Look MP, Meijer-van Gelder ME, Geurts-Moespot A, van der Kwast TH,
Sweep CG and Klijn JG: High tumor levels of vascular endothelial
growth factor predict poor response to systemic therapy in advanced
breast cancer. Cancer Res. 61:5407–5414. 2001.PubMed/NCBI
|
|
32
|
Gasparini G, Toi M, Gion M, et al:
Prognostic significance of vascular endothelial growth factor
protein in node-negative breast carcinoma. J Natl Cancer Inst.
89:139–147. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Konecny GE, Meng YG, Untch M, et al:
Association between HER-2/neu and vascular endothelial growth
factor expression predicts clinical outcome in primary breast
cancer patients. Clin Cancer Res. 10:1706–1716. 2004. View Article : Google Scholar
|
|
34
|
Linderholm B, Grankvist K, Wilking N,
Johansson M, Tavelin B and Henriksson R: Correlation of vascular
endothelial growth factor content with recurrences, survival, and
first relapse site in primary node-positive breast carcinoma after
adjuvant treatment. J Clin Oncol. 18:1423–1431. 2000.
|
|
35
|
Gasparini G, Toi M, Miceli R, et al:
Clinical relevance of vascular endothelial growth factor and
thymidine phosphorylase in patients with node-positive breast
cancer treated with either adjuvant chemotherapy or hormone
therapy. Cancer J Sci Am. 5:101–111. 1999.
|
|
36
|
Verschraegen CF, Arias-Pulido H, Lee SJ,
et al: Phase IB study of the combination of docetaxel, gemcitabine,
and bevacizumab in patients with advanced or recurrent soft tissue
sarcoma: the Axtell regimen. Ann Oncol. 23:785–790. 2012.
View Article : Google Scholar : PubMed/NCBI
|