Introduction
Malignant pleural mesothelioma (MPM) is a rare but
aggressive tumor that arises from mesothelial cells lining the
pleural cavities, and is linked to exposure to carcinogenic
asbestos, and its worldwide incidence continues to increase
(1). It will continue to be a
global health concern in the next few decades due to the continued
use of asbestos in developing countries (1,2).
Depending on different etiologies of the disease, MPM can be
divided into four types: epithelioid, sarcomatoid, desmoplastic and
biphasic, according to the World Health Organization (WHO)
classification of pleural tumors (3). MPM has an extremely poor prognosis,
and the median survival time for the main three types (epithelioid,
sarcomatoid and biphasic) is 18, 8 and 11 months, respectively and
current treatment strategies are limited (4–6).
Aggressive surgery, screening with proposed biomarkers, advances in
modern systemic chemotherapy, and combination of radiotherapy and
chemotherapy regimens are currently being tested, but their
benefits of these treatments are unclear at this time, and
long-term survival in patients with MPM is still rare (7,8). The
lack of major improvements in the survival rate has facilitated
research into identifying new strategies aimed at improving MPM
survival. To improve these survival rates, more specific, effective
and less toxic therapies are needed. Investigating molecular
analyses of MPM samples has led to novel targeted strategies that
inhibit specific key molecules in tumor growth and progression.
We have been attempting to isolate potential
molecular targets for diagnosis and/or treatment of advanced lung
cancer (9) and malignant
mesothelioma by analyzing gene expressions using real-time
reverse-transcriptase polymerase chain reaction (RT-PCR) based on
profiles of various types of database, NCBI-Gene®
(10), GeneCards®
(11), GenomeRNAi®
(12) and CTDatabase®
(13). Throughout these
screenings, we identified two kinesin family members: kinesin
family member 11 (KIF11; alias EG5) and kinesin family member 23
(KIF23; alias KNSL5; MKLP1), as potential candidate target genes
for the treatment of MPMs.
The aims of the present study were to examine the
frequency of transcriptional expression of these target genes in
MPM samples, to investigate its functional role in MPM cell
proliferation by using an RNA interference (RNAi) technique, to
assess clinicopathological relationships in MPM by
immunohistochemistry (IHC) using tissue microarray (TMA), and to
explore the possibilities of these target genes as a potential
molecular target for therapeutic agents.
Materials and methods
Malignant mesothelioma clinical samples
and tissue samples
Thirteen samples were obtained from patients with
MPMs, including subtypes of 6 epithelioids, 6 biphasics and 1
sarcomatoid, with written informed consent at Toronto General
Hospital (Toronto, Canada). For TMA analysis, a total of 53 MPM
were obtained from patients who underwent surgery at Hokkaido
University Hospital and its affiliated hospital between February
1990 and April 2012. Patient's clinical information was extracted
from the medical records. The protocol was approved by the
appropriate institutional review board of Hokkaido University (no.
012-0136). Detailed information about demography, clinical
characteristics and pathological stage are summarized in Table I. Postoperative pathological
staging evaluation was demonstrated only in curative operative
cases (n=21), showing stage I disease in 1 case, stage II disease
in 5 cases, and stage III disease in 15 cases. In all, 1 patient
had T1 disease, 7 patients had T2 disease and 13 patients had T3
disease. A total of 9 patients had N0 disease, 5 patients had N1
disease and 7 patients had N2 disease. Histological classification
of tumors and stage were performed according to the Union for
International Cancer Control (UICC) pathological
tumor/node/metastasis (pTNM) classification criteria (14).
 | Table IPatient and tumor
characteristics. |
Table I
Patient and tumor
characteristics.
| Variables | n (%) |
|---|
| Gender
(Male/female) | 49/4
(92.5/7.5) |
| Age (years)
(mean) | 65.5 (range,
35–80) |
| Histology |
| Epithelioid
type | 34 (64.2) |
| Biphasic type | 13 (24.5) |
| Sarcomatoid
type | 5 (9.4) |
| Desmoplastic
type | 1 (1.9) |
| Surgical
procedure |
| Extrapleural
pleuropneumonectomy (EPP) | 21 (39.6) |
| Pleural
biopsy | 28 (52.8) |
| Recurrent tumor
resection | 3 (5.7) |
| Radical
pleurectomy | 1 (1.9) |
| Total | 53 |
Malignant mesothelioma cell lines
The human malignant mesothelioma cell lines used in
the present study were as follows: NCI-H28, -H226, -H2052 and
-H2452 were purchased from the ATCC (Manassas, VA, USA). All cancer
cells were grown in monolayers in RPMI-1640 medium supplemented
with 10% fetal bovine serum (FBS). A human adult normal mesothelial
cell line (MES-F) was purchased from Zimbio Inc. (Research Triangle
Park, NC, USA) and was grown in mesothelial cell growth medium
(Zimbio). All cell lines were maintained at 37°C in atmospheres of
humidified air with 5% CO2.
cDNA sample preparation
Tumor samples from MPM patients with surgery were
excised and stored at −80°C. QIAzol lysis reagent (Qiagen,
Valencia, CA, USA) and one 5-mm stainless steel Bead (Qiagen) were
added before homogenizing with a TissueLyser Adapter Set (Qiagen)
for 2 min at 20 Hz (15,16). Total RNA was then purified using a
miRNeasy Mini kit (Qiagen). The amount and purity were measured
using a spectrophotometer (NanoDrop; Thermo Fisher Scientific,
Wilmington, DE, USA).
Quantitative RT-PCR analysis
cDNA was synthesized from 1 μg total RNA using
QuantiTect® Reverse Transcription kit (Qiagen). The
primers were designed as follows: for KIF11, forward primer,
5′-acagcctgagctgttaatgatg-3′ and reverse,
5′-gatggctcttgacttagaggttc-3′; for KIF23, forward primer,
5′-tggttcctacattcagaaatgaga-3′ and reverse,
5′-cgttctgatcaggttgaaagagta-3′; for actin, beta (ACTB), forward
primer, 5′-gaaatcgtgcgtgacattaa-3′ and reverse,
5′-aaggaaggctggaagagtg-3′; Quantitative RT-PCR analysis was
performed using the LightCycler480® SYBR-Green I Master
Ready-to-use hot start reaction mix and LightCycler480®
system (Roche, South San Francisco, CA, USA). The thermal cycler
conditions were as follows: 5 min at 95°C for denaturation, 45
cycles at 95°C for 10 sec, 56°C for 20 sec, and 72°C for 10 sec for
PCR amplification, and 1 min at 65°C for melting. The threshold
cycle value was defined as the value obtained in the PCR cycle when
the fluorescence signal increased above the background threshold.
PCR reactions were carried out in duplicates.
RNA interference and cell viability
assay
All short interference RNA (siRNA) oligonucleotide
sequences for KIF11 and KIF23 siRNAs were purchased from Qiagen for
the present study. AllStar Negative Control siRNA®
(Qiagen) were used as the negative control (NC-siRNA). The final
concentration of 10 nM of siRNAs was incubated with
HiPerFect® transfection reagent (Qiagen) according to
the manufacturer's instructions. The CellTiter96®
AQueous One Solution Cell Proliferation Assay (Promega, Madison,
WI, USA) was used for the evaluation of the number of viable cells
according to the manufacturer's instructions, using a microplate
spectrophotometer (μQuant; BioTek Instruments, Inc., Winooski, VT,
USA). Each experiment was performed in triplicates.
Tissue microarray construction and
immunohistochemistry
Archival slides for all the cases were reviewed to
select three representative areas for each sample by an experienced
pathologist (K.H.). TMA blocks were then constructed using a manual
tissue microarrayer (JF-4; Sakura Finetek Japan Co., Ltd., Tokyo,
Japan) with a 1.0-mm diameter needle. The finalized array blocks
were sliced into 4-μm-thick sections and mounted on glass slides.
To check the histopathological diagnosis and adequacy of tissue
sampling, a section from each TMA was stained with regular
hematoxylin and eosin (H&E), as well as calretinin
immunohistochemistry (IHC), and examined by the same pathologist
(K.H.). For KIF23 immunostaining, deparaffinization, antigen
retrieval and IHC were performed on paraffin-embedded TMA sections
and on whole sections using an automated IHC platform (Bond Max™;
Leica Microsystems, Newcastle, UK). Antigen retrieval was performed
in the condition of pH 6.0 for 20 min. The detection kit used was
the Bond Polymer Refine Detection (DS9800; Leica Microsystems),
incubation with post-primary for 20 min, 3 times at room
temperature (RT). Anti-KIF23 monoclonal antibody [MKLP-1 (H-110):
sc-22793; Santa Cruz Biotechnology, Santa Cruz, CA, USA; 1/100] was
diluted using mixed antibody diluent (Dako:X0909 Protein Block
Serum-Free: Dako:S0809 antibody diluent: Nichirei 10% normal goat
serum 1:1:1). A polymer-based detection system (Refine cat.
#DS9800) was used with 3′,3-diaminobenzidine (DAB) as the
chromogen. The positive controls included a sample of testis and
the negative control was performed on all cases by the rabbit
primary antibody (Dako:X0903, rabbit immunoglobulin fraction
(normal)]. KIF11 immunostaining were performed using an automated
IHC platform (Autostainer plus; Dako, Glostrup, Denmark). Antigen
retrieval was performed at pH 9.0 for 20 min. The detection kit
used was the EnVision™+ Dual Link (K4063; Dako), incubation with
post-primary for 60 min at RT. Anti-KIF11 polyclonal antibody
(GTX109054; GeneTex, Inc., Irvine, CA, USA; 1:1,500) was diluted
using mixed antibody diluent (Dako S2022 antibody diluent). A
polymer-based detection system (EnVision™+ Dual Link #K4063) was
used with 3′,3-diaminobenzidine (DAB) as the chromogen. The
positive controls included a sample of testis, and normal lung and
normal pleural samples were used as negative controls. Slides were
dehydrated and placed on coverslips.
Evaluation of immunohistochemical
staining and statistical analysis
Digital images of IHC-stained TMA slides including
53 MPM cases were obtained using a whole slide scanner (ScanScope
CS, Aperio ePathology; Leica Microsystems Inc., Toronto, ON,
Canada). Annotation of tumor regions on whole slides was performed
blinded to clinical follow-up data using Aperio's annotation
software (ImageScope Viewing software, positive pixel count ver.
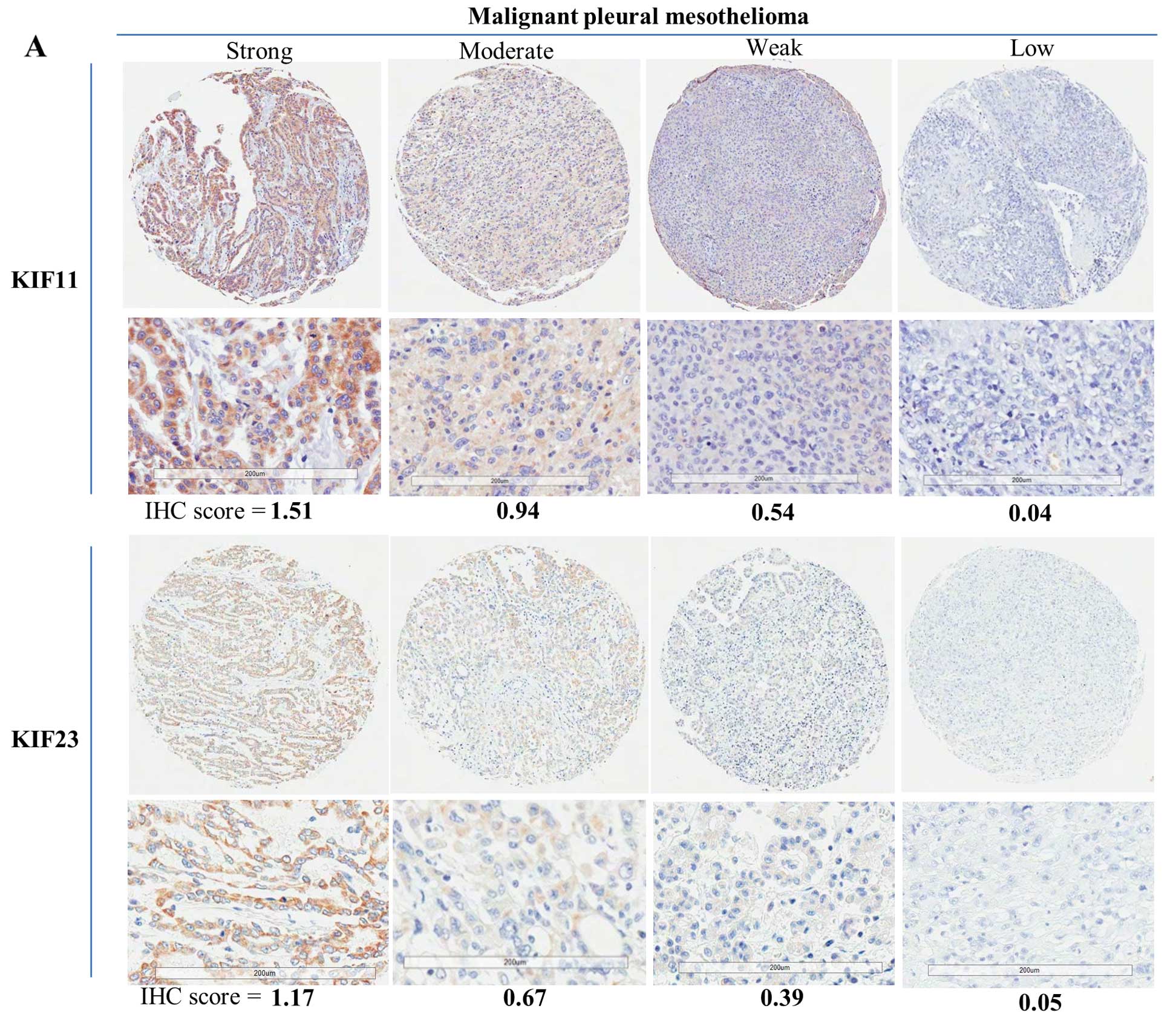
9.1). KIF11 and KIF23 were quantified by IHC scoring, which
summated the percentage of area stained at each intensity level
multiplied by the weighted intensity (0, 1, 2 or 3) reported in
other studies (17–19) (Fig.
3). Initially, the weighted intensity of staining was graded as
follows; grade 0 (negative), 1+ (weak positive), 2+ (moderate
positive), and 3+ (strong positive) according to Aperio's
annotation software). According to the total amount of IHC scores,
KIF11 and KIF23 expression were then finally divided into two
groups each (the threshold leading to the lowest P-value in
log-rank test): low-level KIF11 expression (KIF11-L, with an IHC
score <0.7) and high-level KIF11 expression (KIF11-H, with an
IHC score ≥0.7), and low-level KIF23 expression (KIF23-L, with an
IHC score <0.4) and high-level KIF23 expression (KIF23-H, with
an IHC score ≥0.4). We attempted to correlate clinicopathological
variables such as age, gender, pathological TNM stage, and
histological classification with expression levels of KIF11 and
KIF23 protein as determined by TMA analysis. Immunoreactivity was
assessed for association with clinicopathological variables using
the Fisher's exact for variables. Kaplan-Meier method was used to
generate survival curves, and survival differences were analyzed
with the log-rank test, based on the status of KIF11 and KIF23
expression. Values of P<0.05 were considered statistically
significant. All analyses were performed using StatView version 5.0
software (SAS Institute, Inc., Cary, NC, USA).
Results
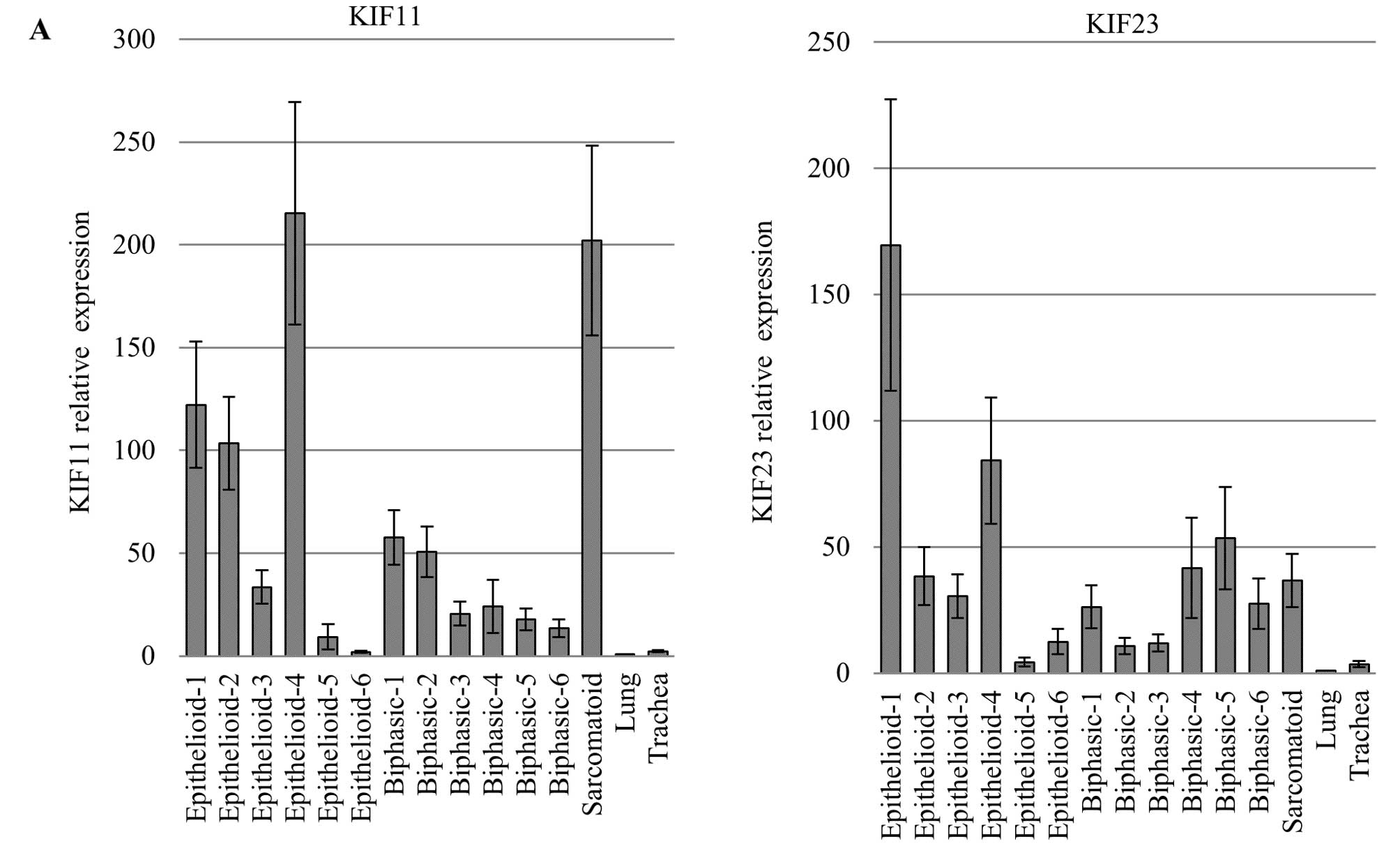
Expression of KIF11 and KIF23 transcripts
in mesotheliomas and normal human tissues
By screening for molecular targeted genes as
described above, we identified KIF11 and KIF23 overexpression with
quantitative RT-PCR experiments in a majority of MPM cases
(Fig. 1A). We also confirmed a
high expression of these genes using 4 human MPM cell lines and low
expression in a normal human mesothelial cell line (MES-F)
(Fig. 1B). Quantitative PCR
analysis using a cDNA panel containing normal human tissues also
showed that these genes expressed mainly in the testis and thymus
among different normal human organs examined (data not shown),
which provides further evidence supporting these genes as promising
molecular targets.
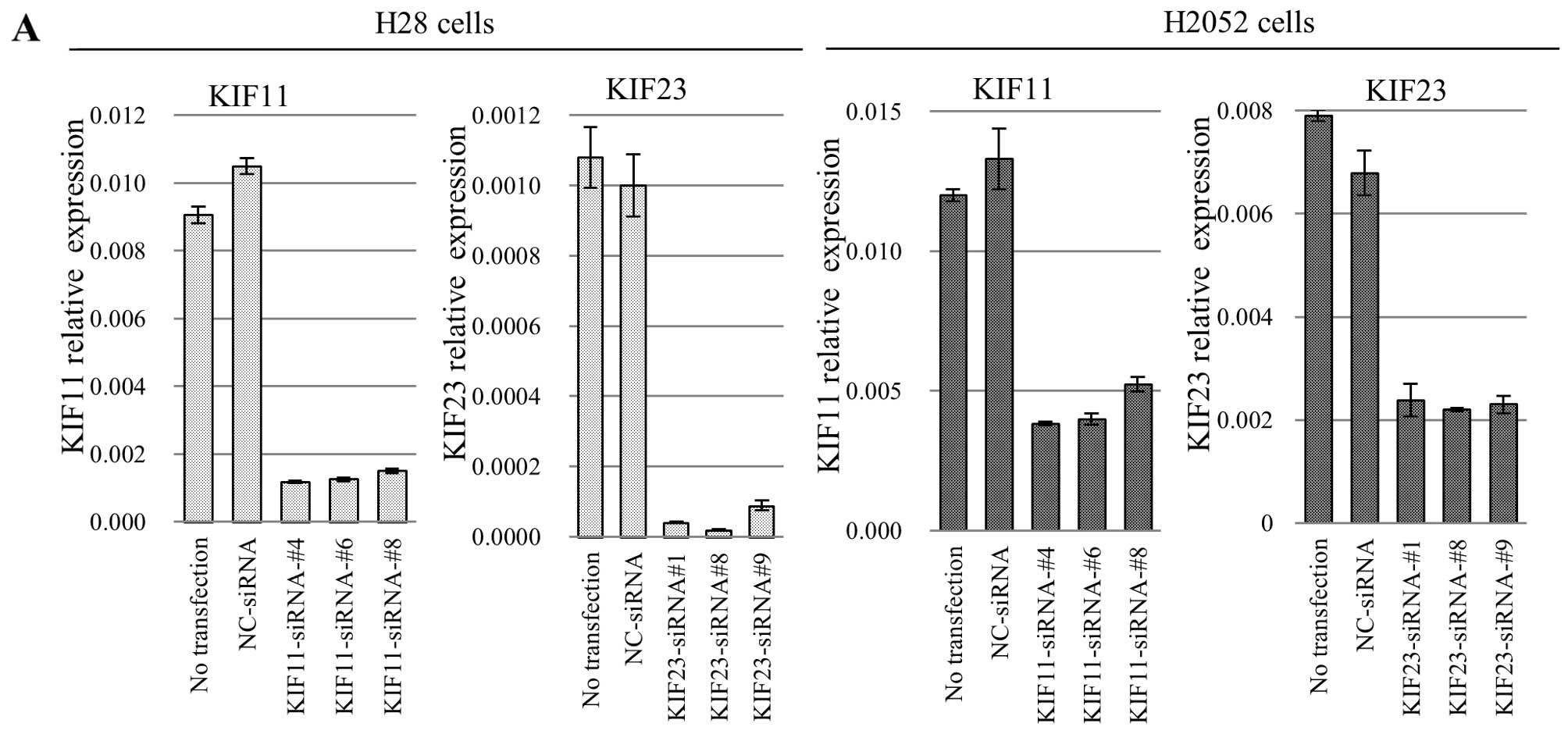
Growth inhibition of mesothelioma cells
by specific siRNA against KIF11 and KIF23
To assess whether therapeutic candidate genes are
essential for growth or survival of MPM cells, we transfected
specific siRNAs against KIF11 (si-KIF11-#4, si-KIF11-#6 and
si-KIF11-#8), KIF23 (si-KIF23-#1, si-KIF23-#8 and si-KIF23-#9) into
human MPM cell lines H28 and H2052, using AllStar siRNA®
as the negative control (NC-siRNA). The mRNA levels of transfected
cells with independent siRNAs targeting these genes were
significantly decreased in comparison to cells transfected with
control siRNAs 48 h after transfection (Fig. 2A). Next, to evaluate the
relationship between cell proliferation and gene knockdown, we
conducted a cell viability assay using the CellTiter 96®
AQueous One Solution Cell Proliferation Assay. After siRNA
treatment, proliferation of H28 and H2052 cells was significantly
suppressed compared with control groups at day 4 after transfection
(Fig. 2B), suggesting that
upregulation of these candidate genes are related to growth or
survival of MPM cells. Typical microscopic images of the cells are
shown in Fig. 2C. Compared to
control cells or control siRNA-treated cells, KIF11 siRNA-treated
mesothelioma cells more frequently induced cell cycle arrest for
mitotic cells with monopolar spindles called ‘monoastral spindle’
(20,21). KIF23 siRNA-treated mesothelioma
cells exhibited large cell bodies with two or more nuclei.
Depletion of KIF23 induces the formation of ‘multinucleate cells’,
likely because of a cytokinesis defect (22–24).
Pattern of KIF11 and KIF23 expression in
MPMs and correlation to clinicopathological parameters and
prognostic significance
We categorized KIF11 and KIF23 expression on the TMA
according to the IHC score described above. Positive staining of
tumor cells by KIF11 and KIF23 generally showed a cytoplasmic
pattern in cancer tissue, and no staining was observed in benign
chronic or fibrous pleuritis and normal lung tissues (Fig. 3B). Of the 53 malignant mesothelioma
cases examined, KIF11-H was observed in 23 cases (43.4%) and
KIF23-H was observed in 27 cases (50.9%) (details are shown in
Table II). Of those, 16
epithelioid type (47.1% of 34 cases), 6 biphasic type (46.2% of 13
cases), and 1 sarcomatoid type (20.0% of 5 cases) showed KIF11-H.
Twenty-two epithelioid type (64.7% of 34 cases), 5 biphasic type
(38.5% of 13 cases) expressed KIF23-H, but no KIF23-H case was
found in sarcomatoid and desmoplastic type. We then tried to
correlate KIF11 and KIF23 expression with various
clinicopathological parameters. However, no significant association
was noted between KIF11 and KIF23 expression and other
clinicopathological variables in curative operative cases (data not
shown). Analysis using the Kaplan-Meier method indicated
significant associations between KIF23-H and MPM patients who
received curative resection with KIF23-H had shorter overall 5-year
survival than those with KIF23-L (P=0.0194, by a log-rank test;
Fig. 3C). A similar trend was
observed in KIF11 expression even though the difference was not
statistically significant.
| Table IIImmunopositivity of KIF11 and KIF23
protein in MPMs (n=53). |
Table II
Immunopositivity of KIF11 and KIF23
protein in MPMs (n=53).
| KIF11
expression |
|---|
|
|---|
| KIF11 low
expression (n=30) | KIF11 high
expression (n=23) | | |
|---|
|
|
| | |
|---|
| Histology/IHC
score | Negative (IHC
score, -0.299) | Weak (IHC score,
0.300–0.699) | Moderate (IHC
score, 0.700–0.999) | Strong (IHC score,
1.000-) | Total (n) | % of high
expression cases |
|---|
| Epithelioid | 5 | 13 | 10 | 6 | 34 | 47.1 |
| Biphasic | 2 | 5 | 4 | 2 | 13 | 46.2 |
| Sarcomatoid | 2 | 2 | 0 | 1 | 5 | 20.0 |
| Desmoplastic | 1 | 0 | 0 | 0 | 1 | 0.0 |
| Total | 10 | 20 | 14 | 9 | 53 | 43.4 |
|
| KIF23
expression |
|
| KIF23 low
expression (n=26) | KIF23 high
expression (n=27) | | |
|
|
| | |
| Histology | Negative (IHC
score, -0.199) | Weak (IHC score,
0.200–0.399) | Moderate (IHC
score, 0.400–0.699) | Strong (IHC score,
0.700-) | Total (n) | % of high
expression cases |
|
| Epithelioid | 6 | 6 | 13 | 9 | 34 | 64.7 |
| Biphasic | 3 | 5 | 4 | 1 | 13 | 38.5 |
| Sarcomatoid | 1 | 4 | 0 | 0 | 5 | 0.0 |
| Desmoplastic | 1 | 0 | 0 | 0 | 1 | 0.0 |
| Total | 11 | 15 | 17 | 10 | 53 | 50.9 |
Discussion
Despite the availability of more advanced surgical
techniques and adjuvant chemoradiotherapy, MPM still has poor
prognosis compared to malignant tumors. Therefore, there is an
urgent need to identify novel diagnostic biomarkers for early
detection of cancer and to offer alternative or improved adjuvant
treatment modalities to individual patients, as well as for
developing new types of anticancer drugs and cancer vaccines. To
investigate appropriate diagnostic and therapeutic target genes, we
used a real-time RT-PCR and RNAi-based approach. Through the
screening, we have identified several therapeutic candidate genes:
PLK1, NDC80, KIF11 and KIF23 for MPM. An involvement in MPM cell
growth and survival has already been demonstrated for PLK1
(25,26) and NDC80 (26). Taken together, these observations
support our RNAi-based screens to identify molecular targets in
MPMs. In further characterizing candidate therapeutic targets, we
focused on kinesin family members, KIF11 and KIF23, in the present
study.
KIF11, a homotetramer motor protein belonging to the
kinesin superfamily, was initially identified in Xenopus
laevis and was shown to play an essential role in centrosome
separation by cross-linking microtubules in the mitotic spindle
(27–30). KIF11 was also identified as an
important molecule during G2-M phase transition, underlining the
importance of this cell cycle checkpoint for non-small cell lung
cancer (NSCLC) and head and neck squamous cell carcinoma (HNSCC)
cell survival (31).
Overexpression of KIF11 has been associated with poor prognosis in
various types of cancer (32,33).
A KIF11 inhibitor, monastrol, has been selected as an antimitotic
agent using a phenotype-based screening (20). Monastrol prevents centrosome
separation and generates a monoastral spindle phenotype as shown in
our RNAi experiment (Fig. 2C),
triggering mitotic arrest and eventual apoptosis (21). Recently, more potent
monastrol-based compounds and other small molecules targeting the
ATPase activity of KIF11 have been developed (34–41).
Kinesin inhibitors have been shown to exhibit strong antitumor
activity and many are currently undergoing clinical trials
(38,42,43).
However, in spite of the important role KIF11 plays during cell
proliferation, the significance of KIF11 transactivation in
carcinogenesis and its potential as a prognostic biomarker of MPM
is yet to be reported. Our findings suggest that the therapeutic
value of KIF11 extends also to MPM.
KIF23, a human homolog of mouse Kif23, is a member
of kinesin motor protein involved in the regulation of cytokinesis
(44,45). Suppression of KIF23 expression
inhibits midbody formation and thus completion of cytokinesis
(23). Previous studies have
reported that inhibiting KIF23 induces the formation of
binucleated/multinucleated cells because of a cytokinesis defect
(23,24). In the present study, we also
confirmed this phenomenon in H28 human MPM cells (Fig. 2C). KIF23 overexpression is a common
event seen in various tumors, such as glioma (22), breast (46), and paclitaxel-resistant gastric
cancer (47). In addition,
down-regulating KIF23 expression significantly suppressed glioma
cell proliferation both in vitro and in vivo
(22). Importantly, high levels of
the KIF23 mRNA are strongly associated with poor survival in
patients with glioma and ER-positive breast cancer (22,46).
Although this result needs to be further validated using another
set of TMA due to the small sample size in the present study, and
intra-tumoral homogeneity of KIF23 expression should be indicated
by whole section IHC, before correlating TMA-IHC data with
survivals of each individual case, this study suggests a
possibility that KIF23 overexpression offers a valuable prognostic
factor in MPMs.
In conclusion, the present study demonstrates that a
high level of KIF11 and KIF23 expression is observed in the
majority of MPM clinical cases as well as several human
mesothelioma cell lines. These two kinesin family member genes are
crucial for the growth and survival of MPM cells. We also found
that a high level of KIF23 is associated with poor survival. Thus,
the results strongly suggest that these genes may have an important
future role in identifying new therapeutic targets for MPMs.
Acknowledgements
The authors are especially thankful to Mr. Hiraku
Shida (Tonan Hospital, Sapporo, Japan). The authors also thank Ms.
Judy McConnell and Ms. Alexandria Grindlay (Toronto General
Hospital) for laboratory management.
References
|
1
|
Yang H, Testa JR and Carbone M:
Mesothelioma epidemiology, carcinogenesis, and pathogenesis. Curr
Treat Options Oncol. 9:147–157. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carbone M, Kratzke RA and Testa JR: The
pathogenesis of mesothelioma. Semin Oncol. 29:2–17. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Travis WD, Brambilla E, Burke AP, Marx A
and Nicholson AG: WHO Classification of Tumours of the Lung,
Pleura, Thymus and Heart. WHO Classification of Tumours. 7. 4th
edition. IARC Press; Lyon: 2015
|
|
4
|
Robinson BW and Lake RA: Advances in
malignant mesothelioma. N Engl J Med. 353:1591–1603. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Robinson BW, Musk AW and Lake RA:
Malignant mesothelioma. Lancet. 366:397–408. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Becklake MR, Bagatin E and Neder JA:
Asbestos-related diseases of the lungs and pleura: Uses, trends and
management over the last century. Int J Tuberc Lung Dis.
11:356–369. 2007.PubMed/NCBI
|
|
7
|
Vogelzang NJ, Rusthoven JJ, Symanowski J,
Denham C, Kaukel E, Ruffie P, Gatzemeier U, Boyer M, Emri S,
Manegold C, et al: Phase III study of pemetrexed in combination
with cisplatin versus cisplatin alone in patients with malignant
pleural mesothelioma. J Clin Oncol. 21:2636–2644. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zucali PA, De Vincenzo F, Simonelli M and
Santoro A: Future developments in the management of malignant
pleural mesothelioma. Expert Rev Anticancer Ther. 9:453–467. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kato T, Wada H, Patel P, Hu S, Lee D,
Hirohashi K, Nakajima T, Kaji M, Kaga K, Matsui Y, et al:
Overexpression of KIF23 predicts clinical outcome in primary lung
cancer patients. Lung Cancer. 92:53–61. 2016. View Article : Google Scholar
|
|
10
|
NCBI. Gene. http://www.ncbi.nlm.nih.gov/gene.
|
|
11
|
Science WIo. GeneCards. v4.0 Build
17http://www.genecards.org/.
|
|
12
|
Schmidt E: GenomeRNAi. 2013, http://genomernai.dkfz.de/GenomeRNAi//.
|
|
13
|
Research LIfC. CTDatabase. http://www.cta.lncc.br/.
|
|
14
|
Sobin LH, Gospodarowicz MK and Wittekind
C: Union for International Cancer Control (UICC), TNM
Classification of Malignant Tumours. 7th edition. Wiley-Blackwell;
New York: 2009
|
|
15
|
Nakajima T, Anayama T, Koike T, Waddell T,
Keshavjee S, Kimura H, Yoshino I and Yasufuku K: Simultaneous
isolation of total RNA, DNA, and protein using samples obtained by
EBUS-TBNA. J Bronchology Interv Pulmonol. 18:301–305. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nakajima T, Zamel R, Anayama T, Kimura H,
Yoshino I, Keshavjee S and Yasufuku K: Ribonucleic acid microarray
analysis from lymph node samples obtained by endobronchial
ultrasonography-guided transbronchial needle aspiration. Ann Thorac
Surg. 94:2097–2101. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rizzardi AE, Johnson AT, Vogel RI,
Pambuccian SE, Henriksen J, Skubitz AP, Metzger GJ and Schmechel
SC: Quantitative comparison of immunohistochemical staining
measured by digital image analysis versus pathologist visual
scoring. Diagn Pathol. 7:422012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nagashio R, Sato Y, Jiang SX, Ryuge S,
Kodera Y, Maeda T and Nakajima T: Detection of tumor-specific
autoantibodies in sera of patients with lung cancer. Lung Cancer.
62:364–373. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nagashio R, Sato Y, Matsumoto T, Kageyama
T, Satoh Y, Shinichiro R, Masuda N, Goshima N, Jiang SX and Okayasu
I: Expression of RACK1 is a novel biomarker in pulmonary
adenocarcinomas. Lung Cancer. 69:54–59. 2010. View Article : Google Scholar
|
|
20
|
Mayer TU, Kapoor TM, Haggarty SJ, King RW,
Schreiber SL and Mitchison TJ: Small molecule inhibitor of mitotic
spindle bipolarity identified in a phenotype-based screen. Science.
286:971–974. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kapoor TM, Mayer TU, Coughlin ML and
Mitchison TJ: Probing spindle assembly mechanisms with monastrol, a
small molecule inhibitor of the mitotic kinesin, Eg5. J Cell Biol.
150:975–988. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Takahashi S, Fusaki N, Ohta S, Iwahori Y,
Iizuka Y, Inagawa K, Kawakami Y, Yoshida K and Toda M:
Downregulation of KIF23 suppresses glioma proliferation. J
Neurooncol. 106:519–529. 2012. View Article : Google Scholar
|
|
23
|
Zhu C, Bossy-Wetzel E and Jiang W:
Recruitment of MKLP1 to the spindle midzone/midbody by INCENP is
essential for midbody formation and completion of cytokinesis in
human cells. Biochem J. 389:373–381. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu X, Zhou T, Kuriyama R and Erikson RL:
Molecular interactions of Polo-like-kinase 1 with the mitotic
kinesin-like protein CHO1/MKLP-1. J Cell Sci. 117:3233–3246. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kawata E, Ashihara E, Nakagawa Y, Kiuchi
T, Ogura M, Yao H, Sakai K, Tanaka R, Nagao R, Yokota A, et al: A
combination of a DNA-chimera siRNA against PLK-1 and zoledronic
acid suppresses the growth of malignant mesothelioma cells in
vitro. Cancer Lett. 294:245–253. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Linton A, Cheng YY, Griggs K, Kirschner
MB, Gattani S, Srikaran S, Chuan-Hao Kao S, McCaughan BC, Klebe S,
van Zandwijk N, et al: An RNAi-based screen reveals PLK1, CDK1 and
NDC80 as potential therapeutic targets in malignant pleural
mesothelioma. Br J Cancer. 110:510–519. 2014. View Article : Google Scholar
|
|
27
|
Le Guellec R, Paris J, Couturier A, Roghi
C and Philippe M: Cloning by differential screening of a Xenopus
cDNA that encodes a kinesin-related protein. Mol Cell Biol.
11:3395–3398. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sawin KE, LeGuellec K, Philippe M and
Mitchison TJ: Mitotic spindle organization by a plus-end-directed
microtubule motor. Nature. 359:540–543. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sawin KE and Mitchison TJ: Mutations in
the kinesin-like protein Eg5 disrupting localization to the mitotic
spindle. Proc Natl Acad Sci USA. 92:4289–4293. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Blangy A, Lane HA, d'Hérin P, Harper M,
Kress M and Nigg EA: Phosphorylation by p34cdc2 regulates spindle
association of human Eg5, a kinesin-related motor essential for
bipolar spindle formation in vivo. Cell. 83:1159–1169. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Martens-de Kemp SR, Nagel R, Stigter-van
Walsum M, van der Meulen IH, van Beusechem VW, Braakhuis BJ and
Brakenhoff RH: Functional genetic screens identify genes essential
for tumor cell survival in head and neck and lung cancer. Clin
Cancer Res. 19:1994–2003. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ding S, Xing N, Lu J, Zhang H, Nishizawa
K, Liu S, Yuan X, Qin Y, Liu Y, Ogawa O, et al: Overexpression of
Eg5 predicts unfavorable prognosis in non-muscle invasive bladder
urothelial carcinoma. Int J Urol. 18:432–438. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sun D, Lu J, Ding K, Bi D, Niu Z, Cao Q,
Zhang J and Ding S: The expression of Eg5 predicts a poor outcome
for patients with renal cell carcinoma. Med Oncol. 30:4762013.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vijapurkar U, Wang W and Herbst R:
Potentiation of kinesin spindle protein inhibitor-induced cell
death by modulation of mitochondrial and death receptor apoptotic
pathways. Cancer Res. 67:237–245. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Garcia-Saez I, DeBonis S, Lopez R, Trucco
F, Rousseau B, Thuéry P and Kozielski F: Structure of human Eg5 in
complex with a new monastrol-based inhibitor bound in the R
configuration. J Biol Chem. 282:9740–9747. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Luo L, Parrish CA, Nevins N, McNulty DE,
Chaudhari AM, Carson JD, Sudakin V, Shaw AN, Lehr R, Zhao H, et al:
ATP-competitive inhibitors of the mitotic kinesin KSP that function
via an allosteric mechanism. Nat Chem Biol. 3:722–726. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Brier S, Lemaire D, Debonis S, Forest E
and Kozielski F: Identification of the protein binding region of
S-trityl-L-cysteine, a new potent inhibitor of the mitotic kinesin
Eg5. Biochemistry. 43:13072–13082. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sakowicz R, Finer JT, Beraud C, Crompton
A, Lewis E, Fritsch A, Lee Y, Mak J, Moody R, Turincio R, et al:
Antitumor activity of a kinesin inhibitor. Cancer Res.
64:3276–3280. 2004. View Article : Google Scholar
|
|
39
|
Lad L, Luo L, Carson JD, Wood KW, Hartman
JJ, Copeland RA and Sakowicz R: Mechanism of inhibition of human
KSP by ispinesib. Biochemistry. 47:3576–3585. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cox CD, Coleman PJ, Breslin MJ, Whitman
DB, Garbaccio RM, Fraley ME, Buser CA, Walsh ES, Hamilton K,
Schaber MD, et al: Kinesin spindle protein (KSP) inhibitors. 9
Discovery of
(2S)-4-(2,5-difluorophenyl)-N-[(3R,4S)-3-fluoro-1-methyl-piperidin-4-yl]-2-(hydroxymethyl)-N-methyl-2-phenyl-2,5-dihydro-1H-pyrrole-1-carboxamide
(MK-0731) for the treatment of taxane-refractory cancer. J Med
Chem. 51:4239–4252. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Theoclitou ME, Aquila B, Block MH, Brassil
PJ, Castriotta L, Code E, Collins MP, Davies AM, Deegan T,
Ezhuthachan J, et al: Discovery of
(+)-N-(3-aminopropyl)-N-[1-(5-benzyl-3-methyl-4-oxo-[1,2]
thiazolo[5,4-d]pyrimidin-6-yl)-2-methylpropyl]-4-methyl-benzamide
(AZD4877), a kinesin spindle protein inhibitor and potential
anticancer agent. J Med Chem. 54:6734–6750. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Souid AK, Dubowy RL, Ingle AM, Conlan MG,
Sun J, Blaney SM and Adamson PC: A pediatric phase I trial and
pharmacokinetic study of ispinesib: A Children's Oncology Group
phase I consortium study. Pediatr Blood Cancer. 55:1323–1328. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Infante JR, Kurzrock R, Spratlin J, Burris
HA, Eckhardt SG, Li J, Wu K, Skolnik JM, Hylander-Gans L, Osmukhina
A, et al: A Phase I study to assess the safety, tolerability, and
pharmacokinetics of AZD4877, an intravenous Eg5 inhibitor in
patients with advanced solid tumors. Cancer Chemother Pharmacol.
69:165–172. 2012. View Article : Google Scholar
|
|
44
|
Glotzer M: The molecular requirements for
cytokinesis. Science. 307:1735–1739. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Neef R, Klein UR, Kopajtich R and Barr FA:
Cooperation between mitotic kinesins controls the late stages of
cytokinesis. Curr Biol. 16:301–307. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Zou JX, Duan Z, Wang J, Sokolov A, Xu J,
Chen CZ, Li JJ and Chen HW: Kinesin family deregulation coordinated
by bromo-domain protein ANCCA and histone methyltransferase MLL for
breast cancer cell growth, survival, and tamoxifen resistance. Mol
Cancer Res. 12:539–549. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Murakami H, Ito S, Tanaka H, Kondo E,
Kodera Y and Nakanishi H: Establishment of new intraperitoneal
paclitaxel-resistant gastric cancer cell lines and comprehensive
gene expression analysis. Anticancer Res. 33:4299–4307.
2013.PubMed/NCBI
|