In 2020, there were an estimated 19.3 million new
cancer cases worldwide (18.1 million excluding non-melanoma skin
cancer) and nearly 10 million cancer deaths (9.9 million excluding
non-melanoma skin cancer). It is estimated that by 2040, the global
cancer burden will reach 28.4 million cases, an increase of 47%
over 2020 (1). There is no doubt
that cancer is one of the most important risk factors affecting
human health in the world today. Surgery remains the most important
and effective treatment approach for the majority of tumor types.
However, a large number of tumor patients present with treatment
difficulties, such as late diagnosis, inability to tolerate
surgery, or a cancer which spreads with ease or has recurred
(2). Therefore, more effective
treatment methods are required.
In recent years, immunotherapy has gradually entered
the arena. Immune targeted drugs, such as programmed cell death
protein 1/programmed cell death protein ligand 1 (PD-1/PD-L1) have
achieved unprecedented results in the field of tumor therapy.
Immunotherapy has become a mainstream direction of development of
novel tumor therapeutics and the development of immunotherapeutic
drugs has also exhibited explosive growth (3-5).
The 2019 anti-cancer progress report released by the American
Association for Cancer Research (6) listed cancer immunotherapy with
surgery, chemotherapy, radiotherapy and targeted therapies as the
five pillars of cancer treatment. Compared with 2017, the total
number of global immunotherapeutics in 2019 expanded from 2,030 to
3,876, an increase of 91%, the discovery of potential
immunotherapeutic targets has increased by 78% and the number of
R&D companies focused on immunotherapy have increased by 60%
(7). At present, clinical tumor
immunotherapy is primarily divided into four categories: Regulatory
T lymphocyte immune checkpoints, chimeric antigen receptor T cell
immunotherapy, in vitro activation methods and
tumor-specific antigen therapy. Among these, the use of antibodies
to block cytotoxic T lymphocyte-related antigen 4, PD-1 and its
ligand PD-L1 pathways belong to T lymphocyte cellular immune
checkpoints (8). The present
review primarily focuses on PD1/PD-L1 immune checkpoint
inhibitors.
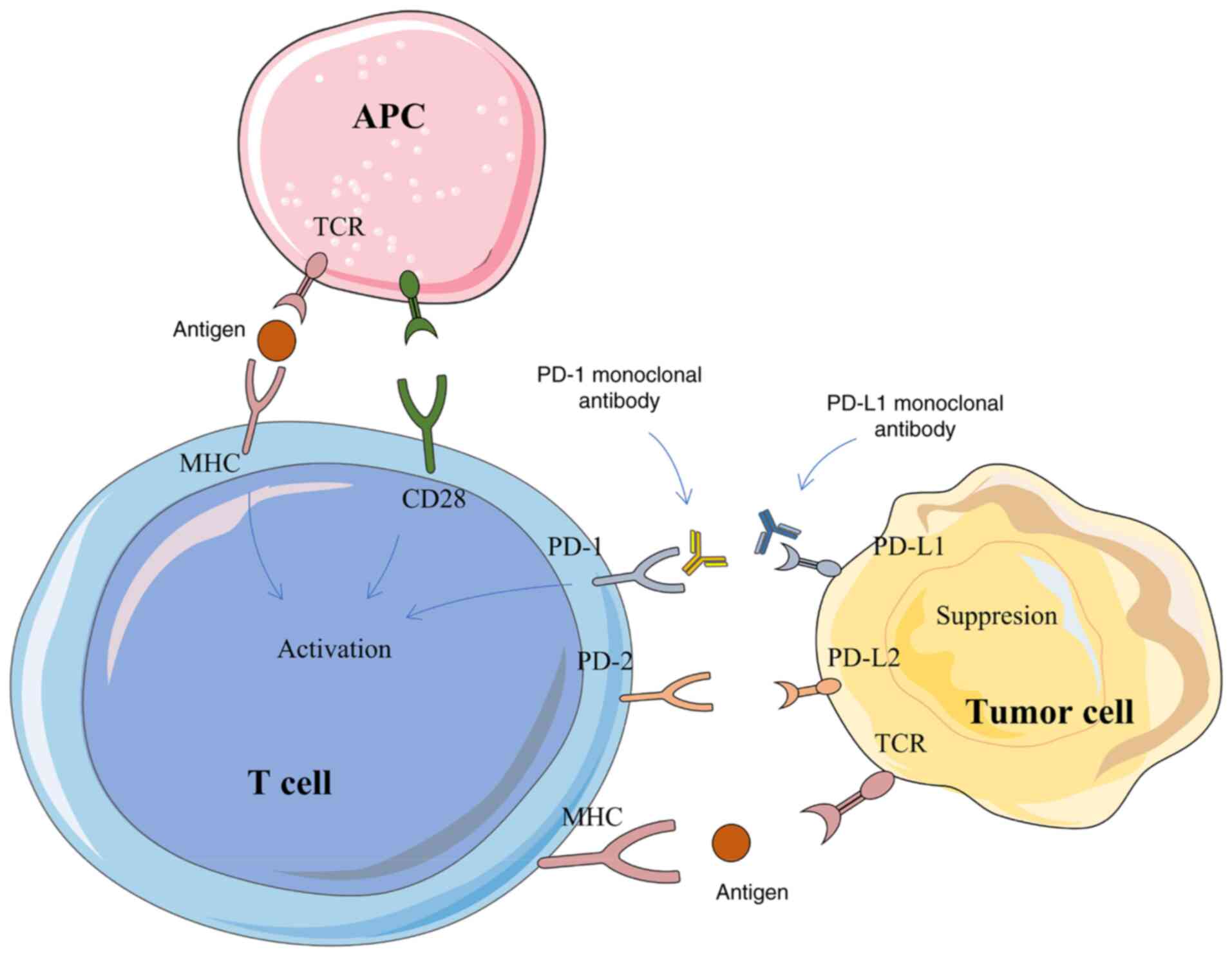
The PD-1 protein is primarily expressed in activated
T/B cells, monocytes, dendritic cells, regulatory T cells and
natural killer T cells (9), while
the PD-L1 protein is widely expressed in antigen presenting cells,
activated T/B cells, macrophages and some non-immune cells, such as
placental trophoblasts, myocardial endothelium cells and thymic
cortical epithelial cells (10).
The expression of PD-L1 protein is detectable in several human
tumor tissues (11). In a healthy
individual, PD-1 binds to the PD-L1 receptor on the surface of T
cells, thereby inhibiting the proliferation and activation of T
cells, blocking their immune functions and preventing the body from
autoimmune diseases (12).
However, the tumor tissue also cunningly evades the immune system's
attack through the characteristic action of PD-1/PD-L1 (13). Due to the lack of an effective
immune response in tumor patients, tumor cells proliferate in large
quantities and the PD-L1 receptor protein on the surface can bind
to the PD-1 protein on the surface of T cells, leading to the
recruitment of tyrosine phosphatase-2 in the src homologous region
and then lead to phosphorylation of downstream protein spleen
tyrosine kinase and phosphoinositide-3 kinase, inhibit downstream
signal transduction, T cell proliferation, cytokine secretion and
cytotoxicity (14). Ultimately,
this leads to substantial depletion of T cells. PD-1/PD-L1
monoclonal antibody (mAb)-based therapeutics can block the binding
between the receptor and its ligand, reactivate T cells and
re-initiate the killing of tumorigenic cells (14). At present, there are >10
approved PD-1/PD-L1 mAbs worldwide. In addition, dozens of drugs
have been or are about to enter the clinical trial stage. The
exploration of their regulatory mechanisms are still the key for
improving the development of novel targets, such as FBXO38, a key
enzyme for PD-1 ubiquitination and degradation and CMTM6, a key
molecule for PD-L1 expression regulation (15-17). In addition, small molecule
peptides, treatment-related biomarkers and treatment of drug
resistance remain the focus of research (18,19). The mechanism of PD-1/PD-L1 based
therapeutics is briefly described in Fig. 1.
According to a study in 2020, the PD-L1 mAb
atezizumab combined with bevacizumab in the treatment of advanced
liver cancer was significantly improved on traditional sorafenib
treatment in terms of overall survival and progression-free
survival (20). A clinical study
in 2018 reported that the preoperative use of neoadjuvant PD-1
related immunotherapy achieved favorable surgical results in
patients with lung cancer (21).
The combination of immunization and targeted neoadjuvant
therapy-PD-1 mAb combined with TKI also achieved curative effects
in liver cancer in preliminary studies (22-24). However, as with almost all
therapeutics, PD-1/PD-L1 immunotherapy may inevitably cause
patients to exhibit varying degrees of immune-related damage. A
phase II clinical trial calculated that the probability of
treatment-related adverse events in the treatment of advanced
hepatocellular carcinoma with carrelizumab combined with apatinib
was 77%; 29% of patients experienced more serious adverse effects
including liver damage and two patients died due to treatment
(25). According to the
statistics of reported adverse reactions, skin injuries including
pruritus, psoriasis and nodular dermatitis accounted for 46-62% of
adverse events, autoimmune colitis accounted for 22-48% of adverse
events and autoimmune hepatitis accounted for 7-33% of adverse
events. Endocrine diseases such as thyroiditis, hypophysitis,
adrenalitis and diabetes accounted for 12-34% of adverse events. In
addition, there are other rare adverse effects including pneumonia
(3-8%), nephritis (1-7%), cardiac adverse effects including
myocarditis (5%) and nervous system adverse effects (1-5%)
(26,27). As these adverse effects result
from the immune response to endogenous tissues, they are defined as
immune-related adverse events (irAEs) (28).
The present review appraises the typical adverse
reactions caused by the use of PD-1/PD-L1 related inhibitors and
the management strategies developed in recent years, with the aim
of providing an up-to-date reference for clinical response to these
adverse reactions in the future.
The manifestations of neuromuscular system-related
adverse events primarily include symptoms such as tremor, visual
disturbances, dysarthria, ataxia, paresthesia and seizures;
however, symptoms may also be unspecific, such as headaches,
dizziness, fatigue and drowsiness. The most common neuromuscular
system-related side effect is myasthenia gravis (29). In addition to cancer, immune
checkpoint inhibitors are often used to treat neurological
diseases, such as ipilimumab for aseptic meningitis (30,31), Guillain-Barre syndrome (32), transversal Myelitis (33) and enteric neuropathy (34), it is therefore of interest to
discuss the nervous system-related side effects of these drugs. A
case in China reported a patient with melanoma who developed
exertional dyspnea and diplopia after 20 days of nivolumab
treatment. Laboratory tests revealed myositis with myocarditis and
rhabdomyolysis. Following diagnosis, patients should be
administered a course of intravenous immunoglobulin (IVIG). During
IVIG, weekly subcutaneous methotrexate and methylprednisolone were
administered and discontinued slowly. This coping strategy was
clearly beneficial to the patient, who gradually exhibited clinical
improvements (35). A case report
described an 85-year-old woman with metastatic melanoma who
developed diplopia after a second cycle of pembrolizumab
monotherapy, followed by asymmetric bilateral ptosis; Myasthenia
gravis was highly suspected clinically. After a diagnosis was made,
the primary treatment options were intravenous immunoglobulin,
prednisone and pyridamide. This protocol elicited a rapid clinical
response and completely resolved the problems of bilateral ptosis
and diplopia. Subsequent treatment included monthly IVIG and daily
oral pyridostigmine without any further recurrence of symptoms
(36). In addition to the
aforementioned reports, there are also reports documenting the
adverse effects of myasthenia gravis after the use of pembrolizumab
in undifferentiated cholangiopancreatic carcinoma (37-40). The management strategy is
administration of pyridostigmine and cessation of pembrolizumab
(41). Another article reported
on a patient with melanoma who received dacarbazine and ipilimumab.
On the fifth treatment cycle, he developed progressive ataxia and
dizziness, with intermittent numbness in his left arm. On the
seventh cycle, his left arm began to twitch. The final diagnosis
was persistent seizures. He was treated with oxcarbazepine plus
oxcarbazepine and levetiracetam. After being discharged from the
hospital, his seizures continued for three weeks. The management
strategy was addition of phenobarbital to oxcarbazepine and
levetiracetam. The motor seizures gradually improved after
treatment (42). Additional
neuromuscular related adverse events and their management
strategies are described in Table
SI.
Respiratory adverse events are relatively common
irAEs. Several life-threatening respiratory events have been
reported following the use of anti-CTLA-4 blockers, including
tissue inflammatory pneumonitis, sarcoidosis and pulmonary
granulomatosis (43-46). The incidence of
respiratory-related adverse events in patients receiving
anti-PD-1/PD-L1 therapy cannot be ignored. In total, 18-38% of
patients most frequently develop a cough and dyspnea. In this
subset of patients, 2-9% had a severe grade 3-4 cough and 1-2% had
life-threatening grade 3-4 dyspnea (47-49). Below, some of the more serious
clinical adverse effects and their management strategies are
described.
There is a case report of a patient with poorly
differentiated squamous cell lung cancer who was diagnosed with
grade 3 immune checkpoint inhibitor-associated pneumonitis
(Pneumonia Severity Index classification) after receiving
second-line single-agent nivolumab (50). After diagnosis, the management
strategy was high-dose glucocorticoid pulse therapy, following
which the patient's clinical symptoms gradually eased. Subsequent
treatment included oral pirfenidone for 11 months. During
pirfenidone treatment, the CT images and clinical symptoms of the
patients showed significant improvements (50). Donato and Krol (51) report a case of allergic
bronchopulmonary aspergillosis after four months of treatment with
the PD-1 inhibitor pembrolizumab. The final diagnosis was
pembrolizumab-induced allergic bronchopulmonary aspergillosis. The
management strategy for the patient was administration of
corticosteroids and voriconazole. The patient responded to
treatment, showing improvement and was able to resume pembrolizumab
with a good clinical response. Fragkou et al (52) report a lower respiratory tract
infection affecting all lobes of a patient with metastatic melanoma
following second-line pembrolizumab immunotherapy. Following
confirmation of the diagnosis, the management strategy for this
side effect was administration of the corticosteroid prednisolone
(50 mg/day intravenously). The patient was sensitive to this
treatment and his clinical symptoms and radiological results
improved rapidly. Unfortunately, three months later, the patient
died of advanced metastatic disease in the brain. Additional
respiratory related adverse events and their management strategies
are described in Table SI.
To date, there have been numerous reports of
circulatory system-related adverse events in patients with cancer
receiving anti-PD-1/PD-L1 treatment. A case of third-degree
atrioventricular block was reported in a patient with metastatic
non-small cell lung cancer receiving ipilimumab-nivolumab
combination therapy. The patient first developed symptoms of lower
extremity swelling after 15 days of ipilimumab and nivolumab
treatment and was subsequently diagnosed with left bundle branch
block, progressive PR interval prolongation, neutropenia and
normocytic anemia. Due to metastatic disease and comorbidities, the
patient and medical team chose not to undergo emergency pacemaker
placement and the patient was instead scheduled for outpatient
event monitoring. Unfortunately, during the hospital stay, the
patient was found to have suffered cardiac arrest and eventually
succumbed (53). Läubli et
al (54) report a case of a
melanoma patient who developed myocarditis following pembrolizumab
treatment. Echocardiography of the patient revealed severely
impaired left ventricular function with dyssynchrony and
histological analysis of myocardial biopsy showed lymphocytic
infiltration, predominance of CD8+ cells and a decrease
in FOXP3+ regulatory T cells. The management strategy
employed resulted in rapid improvement of symptoms and recovery of
left ventricular function and included initiation of
corticosteroids and heart failure treatment according to relevant
guidelines. Bukamur et al (55) document the case of a patient on
statins with a history of hypertension and hyperlipidemia who
developed muscle mass pain after completing two cycles of nivolumab
(240 mg every two weeks). The management strategy for her condition
after admission was cessation of statin use and administration of
high-dose pulsed steroids. Sinus bradycardia developed and
progressed to complete atrioventricular block. After consultation
with an electrophysiologist, the patient was implanted with a
temporary transvenous pacemaker and then a permanent pacemaker. The
overall condition of the patient with this management strategy
improved.
The probability of digestive system-related AEs in
patients with cancer treated with immune checkpoint inhibitors
varies with the specific medications administered. The incidence of
gastrointestinal reactions in patients treated with
anti-CTLA-4/anti-PD-1 combination therapy is 44%, 23-33% in
patients treated with CTLA-4 alone and <20% in patients treated
with anti-PD-1/PD-L1 alone (56).
Gastrointestinal-related irAEs in patients treated with
anti-PD-1/PD-L1 primarily include diarrhea, abdominal pain and
occasionally fever and some of these will be severe enough to cause
substantial damage to the gastrointestinal system (57). Immune-related liver injury is a
relatively common irAE. Immune-related hepatitis is the most common
liver-related adverse event, affecting ~5% of patients receiving
anti-PD-1 therapy, 5-15% of patients receiving ipilimumab
monotherapy and one-third of patients receiving combination therapy
(57). The following are a few
typical digestive system-related adverse events and the associated
clinical response strategies adopted. A case report by Tso et
al (58) documents a patient
with metastatic non-small cell lung cancer who presented with acute
abdominal pain following long-term treatment with nivolumab and a
CT scan showed small dilatation of the proximal ileum, thickening
of the vessel wall and perforation near the transition point. The
management strategy was a laparotomy and the patient eventually
recovered. There is also a report of hepatitis in a woman treated
for recurrent renal cell carcinoma. The physicians eventually
attributed the hepatitis to the use of nivolumab. The management
strategy for this side effect was administration of steroids and
the patient began to exhibit improvements in liver function.
However, she later developed substantial upper gastrointestinal
bleeding secondary to a gastroduodenal ulcer and then developed
acute tubular necrosis, ultimately succumbing to the complications
(59). Lankes et al
(60) reported severe diarrhea
with ≤18 watery bowel movements per day in a patient with
metastatic melanoma treated with ipilimumab. The management
strategy was immunosuppression (high-dose steroids and infliximab)
combined with parenteral therapy. After nutritional therapy, his
condition initially improved, but subsequently worsened. The
patient's symptoms improved by changing the treatment strategy to
antiviral drugs whilst reducing the application of glucocorticoids.
In addition to the aforementioned more common and severe digestive
system-related adverse events, additional digestive related adverse
events and their management strategies are described in Table SI.
Endocrine-related AEs caused by the use of immune
checkpoint inhibitors are more common when treated with anti-CTLA-4
antibodies, whereas a relatively lower incidence of events is
recorded in patients treated with anti-PD-1/PD-L1 treatment. Major
AEs include hypophysitis, abnormal thyroid function and other less
common endocrine diseases such as diabetes and hypercalcemia. In
total, ~1% of patients treated with anti-PD-1/PD-L1 develop
hypophysitis and 4% of patients develop abnormal thyroid function.
Most of these adverse effects are irreversible and require lifelong
hormone replacement therapy (56). The next is a case of a more
typical anti-PD-1/PD-L1 treatment-related immune adverse event and
the clinical management strategy employed. A 77-year-old woman with
stage IV left sigmoid colon cancer developed somnolence and fatigue
after receiving second-line pembrolizumab monotherapy and
progressively developed polydipsia, nausea and vomiting every day,
with progressively more severe symptoms. Diabetic ketoacidosis was
diagnosed based on laboratory tests and the management strategy for
the patient included fluid replacement, insulin therapy, dose
adjustment and electrolyte management. Eventually, the patient
recovered and was discharged home for basal and dietary insulin
therapy (61).
Immunotherapy-related skin damage is the most common
irAE and is very common in patients with cancer treated with
anti-CTLA-4 and anti-PD-1/PD-L1. In total, ~50% of patients treated
with anti-CTLA-4 exhibit some form of skin damage. The incidence of
patients treated with anti-PD-1/PD-L1 who exhibit skin damage is
slightly lower at <40% (62).
The most common skin-related irAE is skin rashes; most patients
report itchy skin. Skin biopsies show large quantities of
infiltrated T cells (63,64). The primary treatment measures
include topical steroids. Next, a few examples of typical clinical
cases reported in recent years are described. Mullangi et al
(65) reported a patient with
renal cell carcinoma who developed psoriasis with nivolumab and
showed involvement of the palms and soles. After a diagnosis of
palmoplantar psoriasis, he was started on a regimen of topical
steroids with triamcinolone acetonide. This did not help his
symptoms. Thus, he was instead administered apremilast and retinoic
acid and continued nivolumab. After three months, he developed
severe diarrhea requiring systemic steroids and infliximab, which
improved his condition. No recurrence of symptoms in the last two
years of follow-up after discontinuing nivolumab were reported.
Acar et al (66) also
reported localized plaques and hard plaques, but no systemic
involvement in a melanoma patient treated with nivolumab. The
patient was treated with topical corticosteroids and calcipotriol.
Following treatment, the patient's lesions responded well and the
patient's condition was ultimately relieved. Mobini et al
(67) report a patient with renal
cell carcinoma who received nivolumab and ipilimumab after
developing lung metastases. A total of one month following the
first round of treatment, the patient developed large, nontender,
firm subcutaneous nodules and plaques on the left forearm and
elbow. These nodules and plaques were visible to the naked eye.
Skin biopsy showed granulomatous inflammation of the dermis and
subcutaneous tissue. Dermatitis nodosa and panniculitis are thought
to be secondary to combination therapy with nivolumab and
ipilimumab (67). Following
consultation with the oncologist, the attending physician decided
to discontinue checkpoint inhibitor therapy after the third round.
Over the next three weeks of follow-up, the patient reported that
the size and stiffness of the lesions were decreasing. There is
also a case report of a melanoma patient with a history of
psoriasis that worsened during treatment with nivolumab
(anti-PD-1). The patient was treated with topical steroids with
good results (68). More skin
lesion-related irAEs are described in the Table SI.
Urinary system-related irAEs rarely occur. In total,
~2% of patients using anti-CTLA-4 will develop urinary
system-related irAEs, such as renal injury nephritis and only
sporadic adverse effects have been reported in patients treated
with anti-PD-1/PD-L1 (69). One
of the most serious reports describes a patient treated with
anti-PD-1 who exhibited immune rejection following kidney
transplantation (70). Next, some
of the more common urinary system-related irAEs after the use of
anti-PD-1/PD-L1 are described. Schneider et al (71) report a patient with melanoma who
developed aseptic cystitis during combination therapy with
nivolumab and ipilimumab, with diarrhea, frequent urination, severe
bladder pain and urgency. The final diagnosis was aseptic cystitis.
Treatment with oral steroids was the most effective treatment
option. Thummalapalli et al (72) report on a patient with BRAF-mutant
melanoma who received anti-PD-1 therapy while taking a RAF/MEK
inhibitor and experienced severe acute kidney injury at the start
of therapy. This process was quickly reversed after symptomatic
treatment with corticosteroids. Uchida et al (73) report on a patient with lung
adenocarcinoma who gradually developed complications of acute
tubulointerstitial nephritis following nivolumab treatment. Kidney
biopsy showed massive proliferation of CD38+ and
IgG+ plasma cells and massive infiltration of
FoxP3+ regulatory T cells. Following the onset of
symptoms, the management strategy was discontinuation of nivolumab
and initiation of oral prednisolone, which was tapered off
gradually. The patient eventually recovered from nivolumab-induced
tubulointerstitial nephritis without any treatment for lung cancer.
More urinary system-related irAEs are described in the Table SI.
Compared with conventional tumor chemotherapy
methods that often cause adverse effects of the blood system, tumor
patients treated with immune checkpoint inhibitors rarely exhibit
related adverse effects, especially for patients treated with
anti-PD-1/PD-L1 based therapy. Of those reported, adverse effects
primarily included aplastic anemia (bone marrow) and autoimmune
hemolytic anemia, which often occurred in the twelfth week of
treatment (74-76). Jotatsu et al (77) report on a patient with non-small
cell lung cancer who developed nivolumab-induced immune
thrombocytopenia after nivolumab treatment. The day after the first
nivolumab infusion, the patient presented with fever and elevated
C-reactive protein levels. Computed tomography of the chest showed
no interstitial lung disease or pneumonia. The fever subsided on
day 9 and has not recurred since. On day 15 after the first
infusion of nivolumab, severe thrombocytopenia developed suddenly
and was diagnosed as nivolumab-induced immune thrombocytopenia.
This was managed with 60 mg prednisolone per day, which restored
the patient's platelet counts and platelet-associated IgG levels,
with the patient eventually achieving remission. Another lung
cancer patient developed immune-mediated thrombocytopenia and
hypothyroidism after receiving nivolumab treatment. The specific
manifestation was detection of IgG in the red blood cells of the
patient, consistent with the warm autoimmune hemolytic anemia. The
patient recovered after receiving steroid treatment (77). Additional hematological AEs and
their management strategies are described in Table SI.
The eyes are not typically regulated by the
immune-system and the probability of irAEs there is very low, ~1%.
A few sporadic cases report vision-related adverse reactions in
patients with cancer receiving anti-PD-1/PD-L1 therapy (62,78). Next, several typical adverse
effects of tumor patients treated with anti-PD-1/PD-L1 are
described. Obata et al (79) report bilateral vision loss in a
63-year-old woman with metastatic cutaneous malignant melanoma 10
days after the second nivolumab injection. Following the onset of
symptoms, the patient was started on topical glucocorticoid
therapy. This management strategy proved effective and after 3
weeks, the patient's ante-rior chamber inflammation disappeared.
Theillac et al (80)
report on a man treated with nivolumab for a melanoma of the leg
with duodenal and lymph node metastases who suddenly developed
bilateral visual impairment and bilateral painless-ness after the
third infusion of the drug. The patient was eventually treated with
oral corticosteroids and his symptoms improved. Additional
ocular-related adverse events and their management strategies are
described in Table SI.
Joint-related irAEs occur in ~15% of tumor patients
treated with anti-PD-1/PD-L1 and is considerably higher compared
with that in tumor patients treated with anti-CTLA-4 (~1%). These
adverse effects often manifest as joint swelling, stiffness,
tenderness and erythema, which can last for several years and
persist after immunotherapy is discontinued, and joint-related
irAEs often occur in patients who have had at least one organ irAE
(81-84). There have been case reports of
arthralgias in some patients when pembrolizumab or nivolumab have
been administered in combination with ipilimumab for treatment of
metastatic cutaneous malignancies (85-87). Most patients with this
complication receive nonsteroidal anti-inflammatory drugs (NSAIDs),
23.1% require additional low-dose corticosteroids and only 7.6%
receive further immunosuppressive therapy. Arthralgia patients
recovered following these treatments and exhibited improved PFS and
OS (88).
There are also some published case reports
documenting granulomatous lesions in patients following use of
PD-1/PD-L1. Al-Dliw et al (89) report on a 65-year-old Caucasian
woman with superficial melanoma of the left hip who, 1 year after
pembrolizumab treatment, had a biopsy showing chronic granulomatous
inflammation in histiocytes. The patient was started on a high-dose
of intravenous steroids and showed significant clinical
improvement. Noguchi et al (90) report on a case of a patient with
cT1aN2M1b stage IV left upper lobe pleomorphic carcinoma who
received nivolumab as a second treatment and had reduced swelling
of the left supraclavicular lymph nodes and left adrenal gland but
increased tumor shad-owing in the right upper lobe. Bronchoscopy
biopsy revealed a granuloma that resembled a sarcomatoid reaction.
The patient was not administered a specific targeted therapy and
following the withdrawal of nivolumab, the granuloma disappeared.
Additional granulomatous-related adverse events and their
management strategies are described in Table SI.
In addition to the irAEs of the various systems
aforementioned, patients using anti-PD-1/PD-L1 have also been
recorded to have lymphatic system, oral cavity and other idiopathic
irAEs, but the probability of these is very small. In the lymphatic
system, a patient with malignant melanoma received pembrolizumab
for 3 months. Although there was a partial response to skin
metastasis and tumor progression was abated, the patient developed
mediastinal lymphadenopathy. The patient under-went selective lymph
node resection. The histopathological results were consistent with
the nodule response. The patient's pembrolizumab treatment was
interrupted and systemic steroid pulse therapy was used, which
significantly relieved the lymphadenopathy (91). Lederhandler et al (92) report an oral-related irAE in a
patient with grade 3 ulcerative oral mucositis in a 78-year-old
woman with lung adenocarcinoma 13 months after starting treatment
with the PD-1 inhibitor pembrolizumab. The condition was
successfully relieved after treatment with prednisone.
Additionally, it was reported that patients with metastatic
melanoma developed delayed autoimmunity 8 months after stopping the
anti-PD-1 antibody nivolumab treatment (93). Therefore, even after the treatment
is discontinued, patients receiving immune checkpoint inhibitor
therapy need continuous monitoring, especially as the propor-tion
of individuals who have ended treatment after achieving a lasting
response increases. Other AEs and the management strategies are
listed in Table SI.
As the number of PD-1/PD-L1-related inhibitors
developed increases, an growing number of patients with cancer will
benefit from them. However, unfortunately this also means there
will be an increase in the number of irAEs and this danger should
be taken into consideration when administering these drugs and
patients should be carefully monitored throughout the treatment
course and even after treatment is discontinued.
A phase II clinical trial calculated a 77%
probability of treatment-related adverse events for camrelizumab in
combination with apatinib in advanced hepatocellular carcinoma. It
was shown that 29% of patients experienced more serious adverse
reactions, including liver damage and two patients died as a result
of the treatment (25). According
to the reported statistics on adverse reactions, skin lesions
including pruritus, psoriasis and nodular dermatitis account for
46-62% of reports, autoimmune colitis accounted for 22-48% of
reports, autoimmune hepatitis accounted for 7-33% of reports and
endocrine diseases such as thyroiditis, hypophysitis, adrenalitis
and diabetes account for 12-34% of reports. In addition, there were
other rarer adverse reactions including pneumonia (3-8%), nephritis
(1-7%), cardiac adverse reactions including myocarditis (5%) and
neurological adverse reactions (1-5%). The types and severity of
irAEs differ for patients with different constitutions. In severe
cases, it will cause irreversible damage to the patient and
potentially even life-threatening complications. As with all
treatments, the risks from immunotherapy should be minimized
through a careful combination of monitoring, management of side
effects and improvements in the therapeutic regimens including the
choice of drugs available. Additionally, methods for detecting and
diagnosing irAEs at an early stage are of paramount importance.
However, at present, there is no perfect system for
detecting and diagnosing these side effects in a timely manner and
most physicians just follow a simple 'discovery-symptom treatment'
model. This will undoubtedly increase the risk of missed diagnoses
and misdiagnoses. Therefore, further exploration of relevant
markers and how to deal with these treatment-related immune side
effects are increasing becoming an important part of broadening the
efficacy of immunotherapy.
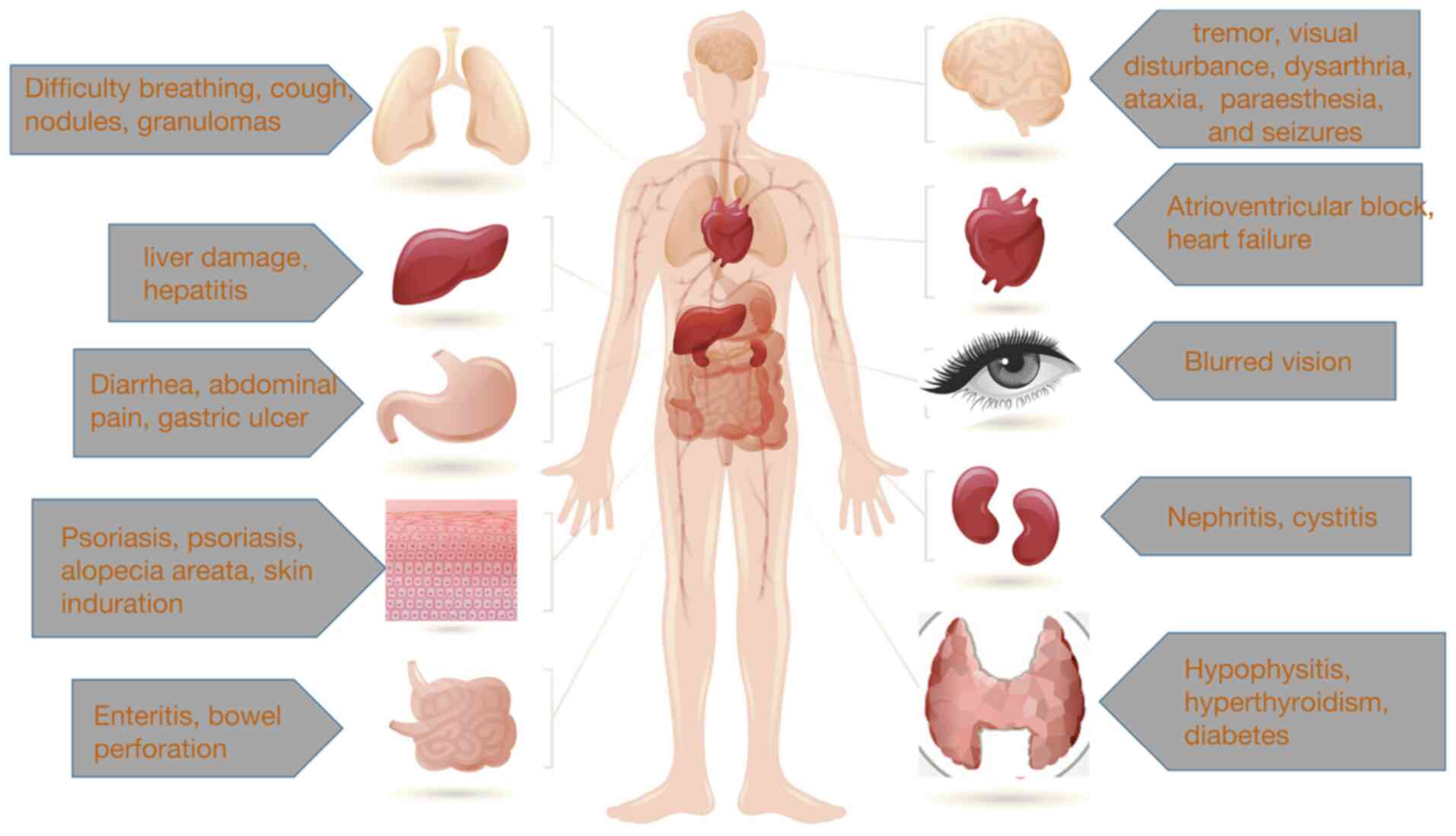
The present review summarized the different adverse
reactions reported by patients with various types of cancer after
treatment with PD-1/PD-L1-related inhibitors and summarized the
management options adopted by the attending physician as well as
the outcomes of the patients. These adverse reactions include
damage to the hematological system, circulatory system, digestive
system, urinary system, lymphatic system, neuromuscular system,
vision and oral cavity, among others. The purpose of the present
review was to highlight the need for improvement of the knowledge
of the physicians to these side effects, to improve early
detection, early diagnosis and early treatment. In Fig. 2 some of the adverse effects on the
various systems listed in this review are summarized for a more
intuitive understanding.
In conclusion, immune checkpoint inhibitor therapy
has exhibited significant potential. However, such drugs will
inevitably cause adverse reactions in clinical applications and the
existing case reports and the management strategies used can aid
clinicians awareness and guide their response in dealing with these
adverse reactions, ultimately improving the health and quality of
care for the patients.
Data sharing is not applicable to this article, as
no data sets were generated or analyzed during the current
study.
GS, XC, HL and GS were responsible for gathering the
related research and designing the review. WY, XK and ZZ were
responsible for creating the figures. HC, XS, GS and WT contributed
to study design, interpretation of the research articles, editing
of the manuscript and critical revision of the manuscript. PT and
GS contributed to respond to reviewer comments and make revisions.
PT contributed to the language editing. All authors read and
approved the final manuscript. Data authentication is not
applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
Not applicable.
No funding was received.
|
1
|
Ferlay J, Colombet M, Soerjomataram I,
Parkin DM, Pineros M, Znaor A and Bray F: Cancer statistics for the
year 2020: An overview. Int J Cancer. Apr 5–2021.Epub ahead of
print. View Article : Google Scholar
|
|
2
|
Xia YX, Zhang F, Li XC, Kong LB, Zhang H,
Li DH, Cheng F, Pu LY, Zhang CY, Qian XF, et al: Surgical treatment
of primary liver cancer:A report of 10 966 cases. Zhonghua Wai Ke
Za Zhi. 59:6–17. 2021.In Chinese.
|
|
3
|
Cordova-Bahena L and Velasco-Velazquez MA:
Anti-PD-1 And Anti-PD-L1 antibodies as immunotherapy against
cancer: A structural perspective. Rev Invest Clin. 73:008–016.
2020.
|
|
4
|
Kuol N, Stojanovska L, Nurgali K and
Apostolopoulos V: PD-1/PD-L1 in disease. Immunotherapy. 10:149–160.
2018. View Article : Google Scholar
|
|
5
|
Emens LA: Breast cancer immunotherapy:
Facts and hopes. Clin Cancer Res. 24:511–520. 2018. View Article : Google Scholar
|
|
6
|
Sengupta R and Honey K: AACR cancer
progress report 2019: Transforming lives through innovative cancer
science. Clin Cancer Res. 25:54312019. View Article : Google Scholar
|
|
7
|
Xin Yu J, Hubbard-Lucey VM and Tang J:
Immuno-oncology drug development goes global. Nat Rev Drug Discov.
18:899–900. 2019. View Article : Google Scholar
|
|
8
|
Ho YJ, Li JP, Fan CH, Liu HL and Yeh CK:
Ultrasound in tumor immunotherapy: Current status and future
developments. J Control Release. 323:12–23. 2020. View Article : Google Scholar
|
|
9
|
Keir ME, Butte MJ, Freeman GJ and Sharpe
AH: PD-1 and its ligands in tolerance and immunity. Annu Rev
Immunol. 26:677–704. 2008. View Article : Google Scholar
|
|
10
|
Patel SP and Kurzrock R: PD-L1 expression
as a predictive biomarker in cancer immunotherapy. Mol Cancer Ther.
14:847–856. 2015. View Article : Google Scholar
|
|
11
|
Kythreotou A, Siddique A, Mauri FA, Bower
M and Pinato DJ: Pd-L1. J Clin Pathol. 71:189–194. 2018. View Article : Google Scholar
|
|
12
|
Ghosh C, Luong G and Sun Y: A snapshot of
the PD-1/PD-L1 pathway. J Cancer. 12:2735–2746. 2021. View Article : Google Scholar
|
|
13
|
Ai L, Xu A and Xu J: Roles of PD-1/PD-L1
pathway: Signaling, cancer, and beyond. Adv Exp Med Biol.
1248:33–59. 2020. View Article : Google Scholar
|
|
14
|
Jiang Y, Chen M, Nie H and Yuan Y: PD-1
and PD-L1 in cancer immunotherapy: Clinical implications and future
considerations. Hum Vaccin Immunother. 15:1111–1122. 2019.
View Article : Google Scholar
|
|
15
|
Meng X, Liu X, Guo X, Jiang S, Chen T, Hu
Z, Liu H, Bai Y, Xue M, Hu R, et al: FBXO38 mediates PD-1
ubiquitination and regulates anti-tumour immunity of T cells.
Nature. 564:130–135. 2018. View Article : Google Scholar
|
|
16
|
Burr ML, Sparbier CE, Chan YC, Williamson
JC, Woods K, Beavis PA, Lam EYN, Henderson MA, Bell CC, Stolzenburg
S, et al: CMTM6 maintains the expression of PD-L1 and regulates
anti-tumour immunity. Nature. 549:101–105. 2017. View Article : Google Scholar
|
|
17
|
Mezzadra R, Sun C, Jae LT, Gomez-Eerland
R, de Vries E, Wu W, Logtenberg MEW, Slagter M, Rozeman EA, Hofland
I, et al: Identification of CMTM6 and CMTM4 as PD-L1 protein
regula-tors. Nature. 549:106–110. 2017. View Article : Google Scholar
|
|
18
|
Baumeister SH, Freeman GJ, Dranoff G and
Sharpe AH: Coinhibitory Pathways in Immunotherapy for Cancer. Annu
Rev Immunol. 34:539–573. 2016. View Article : Google Scholar
|
|
19
|
Burugu S, Dancsok AR and Nielsen TO:
Emerging targets in cancer immunotherapy. Semin Cancer Biol.
52:39–52. 2018. View Article : Google Scholar
|
|
20
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar
|
|
21
|
Forde PM, Chaft JE and Pardoll DM:
Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med.
379:e142018. View Article : Google Scholar
|
|
22
|
Zhu XD, Huang C, Shen YH, Ji Y, Ge NL, Qu
XD, Chen L, Shi WK, Li ML, Zhu JJ, et al: Downstaging and resection
of initially unresectable hepatocellular carcinoma with tyrosine
kinase inhibitor and anti-PD-1 antibody combinations. Liver Cancer.
10:320–329. 2021. View Article : Google Scholar
|
|
23
|
Xu ZN, Huang JJ, Zhou J, Huang WS, Guo YJ,
Cai MY, Zhou JW, Lin LT, Liang LC and Zhu KS: Efficacy and safety
of anti-PD-1 monoclonal antibody in advanced hepatocellular
carcinoma after TACE combined with TKI therapy. Zhonghua Nei Ke Za
Zhi. 60:630–636. 2021.In Chinese.
|
|
24
|
Xie D, Sun Q, Wang X, Zhou J, Fan J, Ren Z
and Gao Q: Immune checkpoint inhibitor plus tyrosine kinase
inhibitor for unresectable hepatocellular carcinoma in the real
world. Ann Transl Med. 9:6522021. View Article : Google Scholar
|
|
25
|
Xu J, Shen J, Gu S, Zhang Y, Wu L, Wu J,
Shao G, Zhang Y, Xu L, Yin T, et al: Camrelizumab in combination
with apatinib in patients with advanced hepatocellular carcinoma
(RESCUE): A nonrandomized, open-label, phase II trial. Clin Cancer
Res. 27:1003–1011. 2021. View Article : Google Scholar
|
|
26
|
Hussaini S, Chehade R, Boldt RG, Raphael
J, Blanchette P, Maleki Vareki S and Fernandes R: Association
between immune-related side effects and efficacy and benefit of
immune checkpoint inhibitors-A systematic review and meta-analysis.
Cancer Treat Rev. 92:1021342021. View Article : Google Scholar
|
|
27
|
Heinzerling L, de Toni EN, Schett G,
Hundorfean G and Zimmer L: Checkpoint Inhibitors. Dtsch Arztebl
Int. 116:119–126. 2019.
|
|
28
|
Martins F, Sofiya L, Sykiotis GP, Lamine
F, Maillard M, Fraga M, Shabafrouz K, Ribi C, Cairoli A,
Guex-Crosier Y, et al: Adverse effects of immune-checkpoint
inhibitors: Epidemiology, management and surveillance. Nat Rev Clin
Oncol. 16:563–580. 2019. View Article : Google Scholar
|
|
29
|
Zimmer L, Goldinger SM, Hofmann L, Loquai
C, Ugurel S, Thomas I, Schmidgen MI, Gutzmer R, Utikal JS, Goppner
D, et al: Neurological, respiratory, musculoskeletal, cardiac and
ocular side-effects of anti-PD-1 therapy. Eur J Cancer. 60:210–225.
2016. View Article : Google Scholar
|
|
30
|
Liao B, Shroff S, Kamiya-Matsuoka C and
Tummala S: Atypical neurological complications of ipilimumab
therapy in patients with metastatic melanoma. Neuro Oncol.
16:589–593. 2014. View Article : Google Scholar
|
|
31
|
Voskens CJ, Goldinger SM, Loquai C, Robert
C, Kaehler KC, Berking C, Bergmann T, Bockmeyer CL, Eigentler T,
Fluck M, et al: The price of tumor control: An analysis of rare
side effects of anti-CTLA-4 therapy in metastatic melanoma from the
ipilimumab network. PLoS One. 8:e537452013. View Article : Google Scholar
|
|
32
|
Wilgenhof S and Neyns B: Anti-CTLA-4
antibody-induced Guillain-Barre syndrome in a melanoma patient. Ann
Oncol. 22:991–993. 2011. View Article : Google Scholar
|
|
33
|
Bot I, Blank CU, Boogerd W and Brandsma D:
Neurological immune-related adverse events of ipilimumab. Pract
Neurol. 13:278–280. 2013. View Article : Google Scholar
|
|
34
|
De Giorgio R, Guerrini S, Barbara G,
Stanghellini V, De Ponti F, Corinaldesi R, Moses PL, Sharkey KA and
Mawe GM: Inflammatory neuropathies of the enteric nervous system.
Gastroenterology. 126:1872–1883. 2004. View Article : Google Scholar
|
|
35
|
Liu WK, Naban N, Kaul A, Patel N and Fusi
A: Life-threatening polymyositis with spontaneous hematoma induced
by nivolumab in a patient with previously resected melanoma.
Melanoma Res. 31:85–87. 2021. View Article : Google Scholar
|
|
36
|
Makarious D, Horwood K and Coward JIG:
Myasthenia gravis: An emerging toxicity of immune checkpoint
inhibitors. Eur J Cancer. 82:128–136. 2017. View Article : Google Scholar
|
|
37
|
Hayakawa N, Kikuchi E, Suzuki S and Oya M:
Myasthenia gravis with myositis induced by pembrolizumab therapy in
a patient with metastatic urothelial carcinoma. Int Cancer Conf J.
9:123–126. 2020. View Article : Google Scholar
|
|
38
|
Safa H, Johnson DH, Trinh VA, Rodgers TE,
Lin H, Suarez-Almazor ME, Fa'ak F, Saberian C, Yee C, Davies MA, et
al: Immune checkpoint inhibitor related myasthenia gravis: Single
center experience and systematic review of the literature. J
Immunother Cancer. 7:3192019. View Article : Google Scholar
|
|
39
|
Pottier C, El Habnouni C, Kervarrec T,
Beltran S and Samimi M: Myasthenia gravis induced by pembrolizumab
in a patient with metastatic Merkel cell carcinoma. Ann Dermatol
Venereol. Feb 18–2022.Epub ahead of print. View Article : Google Scholar
|
|
40
|
Tian CY, Ou YH, Chang SL and Lin CM:
Pembrolizumab-induced myasthenia gravis-like disorder, ocular
myositis, and hepatitis: A case report. J Med Case Rep. 15:2442021.
View Article : Google Scholar
|
|
41
|
Heleno CT, Mustafa A, Gotera NA and Tesar
A: Myasthenia gravis as an immune-mediated side effect of
checkpoint inhibitors. Cureus. 13:e163162021.
|
|
42
|
Vogel WV, Guislain A, Kvistborg P,
Schumacher TN, Haanen JB and Blank CU: Ipilimumab-induced
sarcoidosis in a patient with metastatic melanoma undergoing
complete remission. J Clin Oncol. 30:e7–e10. 2012. View Article : Google Scholar
|
|
43
|
Eckert A, Schoeffler A, Dalle S, Phan A,
Kiakouama L and Thomas L: Anti-CTLA4 monoclonal antibody induced
sarcoidosis in a metastatic melanoma patient. Dermatology.
218:69–70. 2009. View Article : Google Scholar
|
|
44
|
Wilgenhof S, Morlion V, Seghers AC, Du
Four S, Vanderlinden E, Hanon S, Vandenbroucke F, Everaert H and
Neyns B: Sarcoidosis in a patient with metastatic melanoma
sequentially treated with anti-CTLA-4 monoclonal antibody and
selective BRAF inhibitor. Anticancer Res. 32:1355–1359. 2012.
|
|
45
|
Mandel JJ, Olar A, Aldape KD and
Tremont-Lukats IW: Lambrolizumab induced central nervous system
(CNS) toxicity. J Neurol Sci. 344:229–231. 2014. View Article : Google Scholar
|
|
46
|
Barjaktarevic IZ, Qadir N, Suri A,
Santamauro JT and Stover D: Organizing pneumonia as a side effect
of ipilimumab treatment of melanoma. Chest. 143:858–861. 2013.
View Article : Google Scholar
|
|
47
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity, and immune
correlates of anti-PD-1 antibody in cancer. N Engl J Med.
366:2443–2454. 2012. View Article : Google Scholar
|
|
48
|
Rizvi NA, Mazieres J, Planchard D,
Stinchcombe TE, Dy GK, Antonia SJ, Horn L, Lena H, Minenza E,
Mennecier B, et al: Activity and safety of nivolumab, an anti-PD-1
immune check-point inhibitor, for patients with advanced,
refractory squamous non-small-cell lung cancer (CheckMate 063): A
phase 2, single-arm trial. Lancet Oncol. 16:257–265. 2015.
View Article : Google Scholar
|
|
49
|
Topalian SL, Sznol M, McDermott DF, Kluger
HM, Carvajal RD, Sharfman WH, Brahmer JR, Lawrence DP, Atkins MB,
Powderly JD, et al: Survival, durable tumor remission, and
long-term safety in patients with advanced melanoma receiving
nivolumab. J Clin Oncol. 32:1020–1030. 2014. View Article : Google Scholar
|
|
50
|
Yu H, Li J, Yu L, Cheng X, Han X and Zhang
X: A case report of checkpoint inhibitor pneumonitis caused by
PD-1Antibody-safety and effectiveness of pirfenidone. Zhongguo Fei
Ai Za Zhi. 24:519–525. 2021.In Chinese.
|
|
51
|
Donato AA and Krol R: Allergic
bronchopulmonary aspergillosis presumably unmasked by PD-1
inhibition. BMJ Case Rep. 12:e2278142019. View Article : Google Scholar
|
|
52
|
Fragkou P, Souli M, Theochari M,
Kontopoulou C, Loukides S and Koumarianou A: A case of organizing
pneumonia (OP) associated with pembrolizumab. Drug Target Insights.
10:9–12. 2016. View Article : Google Scholar
|
|
53
|
Vartanov A, Kalotra A, Varughese J, Gautam
S, Kandel S and Hosmer W: Immunotherapy-associated complete heart
block in a patient with NSCLC: A case report and literature review.
Respir Med Case Rep. 33:1013902021.
|
|
54
|
Läubli H, Balmelli C, Bossard M, Pfister
O, Glatz K and Zippelius A: Acute heart failure due to autoimmune
myocarditis under pembrolizumab treatment for metastatic melanoma.
J Immunother Cancer. 3:112015. View Article : Google Scholar
|
|
55
|
Bukamur HS, Mezughi H, Karem E, Shahoub I
and Shweihat Y: Nivolumab-induced third degree atrioventricular
block in a patient with stage IV squamous cell lung carcinoma.
Cureus. 11:e48692019.
|
|
56
|
Cousin S, Seneschal J and Italiano A:
Toxicity profiles of immunotherapy. Pharmacol Ther. 181:91–100.
2018. View Article : Google Scholar
|
|
57
|
Puzanov I, Diab A, Abdallah K, Bingham CO
III, Brogdon C, Dadu R, Hamad L, Kim S, Lacouture ME, LeBoeuf NR,
et al: Managing toxicities associated with immune checkpoint
inhibitors: Consensus recommendations from the Society for
Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J
Immunother Cancer. 5:952017. View Article : Google Scholar
|
|
58
|
Tso DK, Avery LL, Lev MH and Kamalian S:
Nivolumab-induced small bowel obstruction and perforation: A rare
but life-threatening side effect of immunotherapy. Emerg Radiol.
27:107–110. 2020. View Article : Google Scholar
|
|
59
|
Mathew Thomas V, Bindal P, Ann Alexander S
and McDonald K: Nivolumab-induced hepatitis: A rare side effect of
an immune check point inhibitor. J Oncol Pharm Pract. 26:459–461.
2020. View Article : Google Scholar
|
|
60
|
Lankes K, Hundorfean G, Harrer T, Pommer
AJ, Agaimy A, Angelovska I, Tajmir-Riahi A, Gohl J, Schuler G,
Neurath MF, et al: Anti-TNF-refractory colitis after checkpoint
inhibitor therapy: Possible role of CMV-mediated
immunopathogenesis. Oncoimmunology. 5:e11286112016. View Article : Google Scholar
|
|
61
|
Kichloo A, Albosta MS, McMahon S,
Movsesian K, Wani F, Jamal SM, Aljadah M and Singh J:
Pembrolizumab-induced diabetes mellitus presenting as diabetic
ketoacidosis in a patient with metastatic colonic adenocarcinoma. J
Investig Med High Impact Case Rep. 8:23247096209513392020.
|
|
62
|
Villadolid J and Amin A: Immune checkpoint
inhibitors in clinical practice: Update on management of
immune-related toxicities. Transl Lung Cancer Res. 4:560–575.
2015.
|
|
63
|
Belum VR, Benhuri B, Postow MA, Hellmann
MD, Lesokhin AM, Segal NH, Motzer RJ, Wu S, Busam KJ, Wolchok JD
and Lacouture ME: Characterisation and management of dermatologic
adverse events to agents targeting the PD-1 receptor. Eur J Cancer.
60:12–25. 2016. View Article : Google Scholar
|
|
64
|
Naidoo J, Page DB, Li BT, Connell LC,
Schindler K, Lacouture ME, Postow MA and Wolchok JD: Toxicities of
the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann
Oncol. 27:13622016. View Article : Google Scholar
|
|
65
|
Mullangi S, Ponnam S, Lekkala MR and Koya
S: A case of de novo psoriasis secondary to nivolumab in a patient
with meta-static renal cell carcinoma. Cureus. 13:e157032021.
|
|
66
|
Acar A, Oraloglu G, Yaman B and Karaarslan
I: Nivolumab-induced plaque morphea in a malign melanoma patient. J
Cosmet Dermatol. 20:2645–2647. 2021. View Article : Google Scholar
|
|
67
|
Mobini N, Dhillon R, Dickey J, Spoon J and
Sadrolashrafi K: Exclusive cutaneous and subcutaneous sarcoidal
granulomatous inflammation due to immune checkpoint inhibitors:
Report of two cases with unusual manifestations and review of the
literature. Case Rep Dermatol Med. 2019:67028702019.
|
|
68
|
De Bock M, Hulstaert E, Kruse V and
Brochez L: Psoriasis vulgaris exacerbation during treatment with a
PD-1 check-point inhibitor: Case report and literature review. Case
Rep Dermatol. 10:190–197. 2018. View Article : Google Scholar
|
|
69
|
Izzedine H, Gueutin V, Gharbi C, Mateus C,
Robert C, Routier E, Thomas M, Baumelou A and Rouvier P: Kidney
injuries related to ipilimumab. Invest New Drugs. 32:769–773. 2014.
View Article : Google Scholar
|
|
70
|
Lefebvre J and Glezerman IG: Kidney
toxicities associated with novel cancer therapies. Adv Chronic
Kidney Dis. 24:233–240. 2017. View Article : Google Scholar
|
|
71
|
Schneider S, Alezra E, Yacoub M, Ducharme
O, Gerard E, Dutriaux C and Prey S: Aseptic cystitis induced by
nivolumab and ipilimumab combination for metastatic melanoma.
Melanoma Res. 31:487–489. 2021. View Article : Google Scholar
|
|
72
|
Thummalapalli R, Melms JC, Mier J and Izar
B: Rapid evolution of acute kidney injury after initial infusion of
pembrolizumab in a melanoma patient concurrently treated with
RAF/MEK inhibitors. Melanoma Res. 30:219–222. 2020. View Article : Google Scholar
|
|
73
|
Uchida A, Watanabe M, Nawata A, Ikari Y,
Sasaki M, Shigemoto K, Hisano S and Nakashima H: Tubulointerstitial
nephritis as adverse effect of programmed cell death 1 inhibitor,
nivolumab, showed distinct histological findings. CEN Case Rep.
6:169–174. 2017. View Article : Google Scholar
|
|
74
|
Atwal D, Joshi KP, Ravilla R and Mahmoud
F: Pembrolizumab-induced pancytopenia: A case report. Perm J.
21:17–004. 2017.
|
|
75
|
Michot JM, Vargaftig J, Leduc C, Quere G,
Burroni B, Lazarovici J, Champiat S, Ribrag V and Lambotte O:
Immune-related bone marrow failure following anti-PD1 therapy. Eur
J Cancer. 80:1–4. 2017. View Article : Google Scholar
|
|
76
|
Comito RR, Badu LA and Forcello N:
Nivolumab-induced aplastic anemia: A case report and literature
review. J Oncol Pharm Pract. 25:221–225. 2019. View Article : Google Scholar
|
|
77
|
Jotatsu T, Oda K, Yamaguchi Y, Noguchi S,
Kawanami T, Kido T, Satoh M and Yatera K: Immune-mediated
thrombocytopenia and hypothyroidism in a lung cancer patient
treated with nivolumab. Immunotherapy. 10:85–91. 2018. View Article : Google Scholar
|
|
78
|
Kumar V, Chaudhary N, Garg M, Floudas CS,
Soni P and Chandra AB: Corrigendum: Current diagnosis and
management of immune related adverse events (irAEs) induced by
immune checkpoint inhibitor therapy. Front Pharmacol.
8:3112017.
|
|
79
|
Obata S, Saishin Y, Teramura K and Ohji M:
Vogt-koyanagiharada disease-like uveitis during nivolumab
(Anti-PD-1 Antibody) treatment for metastatic cutaneous malignant
melanoma. Case Rep Ophthalmol. 10:67–74. 2019. View Article : Google Scholar
|
|
80
|
Theillac C, Straub M, Breton AL, Thomas L
and Dalle S: Bilateral uveitis and macular edema induced by
Nivolumab: A case report. BMC Ophthalmol. 17:2272017. View Article : Google Scholar
|
|
81
|
Lidar M, Giat E, Garelick D, Horowitz Y,
Amital H, Steinberg-Silman Y, Schachter J, Shapira-Frommer R and
Markel G: Rheumatic manifestations among cancer patients treated
with immune checkpoint inhibitors. Autoimmun Rev. 17:284–289. 2018.
View Article : Google Scholar
|
|
82
|
Spain L, Diem S and Larkin J: Management
of toxicities of immune checkpoint inhibitors. Cancer Treat Rev.
44:51–60. 2016. View Article : Google Scholar
|
|
83
|
Cappelli LC, Gutierrez AK, Baer AN,
Albayda J, Manno RL, Haque U, Lipson EJ, Bleich KB, Shah AA, Naidoo
J, et al: Inflammatory arthritis and sicca syndrome induced by
nivolumab and ipilimumab. Ann Rheum Dis. 76:43–50. 2017. View Article : Google Scholar
|
|
84
|
Belkhir R, Burel SL, Dunogeant L,
Marabelle A, Hollebecque A, Besse B, Leary A, Voisin AL, Pontoizeau
C, Coutte L, et al: Rheumatoid arthritis and polymyalgia rheumatica
occurring after immune checkpoint inhibitor treatment. Ann Rheum
Dis. 76:1747–1750. 2017. View Article : Google Scholar
|
|
85
|
Almutairi AR, McBride A, Slack M, Erstad
BL and Abraham I: Potential immune-related adverse events
associated with mono-therapy and combination therapy of ipilimumab,
nivolumab, and pembrolizumab for advanced melanoma: A systematic
review and meta-analysis. Front Oncol. 10:912020. View Article : Google Scholar
|
|
86
|
Xu C, Chen YP, Du XJ, Liu JQ, Huang CL,
Chen L, Zhou GQ, Li WF, Mao YP, Hsu C, et al: Comparative safety of
immune checkpoint inhibitors in cancer: Systematic review and
network meta-analysis. BMJ. 363:k42262018. View Article : Google Scholar
|
|
87
|
Lee J, Graham A and Sion A: Evaluation of
arthralgias in adult oncology patients receiving immune checkpoint
inhibitors. J Oncol Pharm Pract. 25:1867–1872. 2019. View Article : Google Scholar
|
|
88
|
Buder-Bakhaya K, Benesova K, Schulz C,
Anwar H, Dimitrakopoulou-Strauss A, Weber TF, Enk A, Lorenz HM and
Hassel JC: Characterization of arthralgia induced by PD-1 antibody
treatment in patients with metastasized cutaneous malignancies.
Cancer Immunol Immunother. 67:175–182. 2018. View Article : Google Scholar
|
|
89
|
Al-Dliw M, Megri M, Shahoub I, Sahay G,
Limjoco TI and Shweihat Y: Pembrolizumab reactivates pulmonary
granulomatosis. Respir Med Case Rep. 22:126–129. 2017.
|
|
90
|
Noguchi S, Kawachi H, Yoshida H, Fukao A,
Terashita S, Ikeue T, Horikawa S and Sugita T: Sarcoid-Like
granulomatosis induced by nivolumab treatment in a lung cancer
patient. Case Rep Oncol. 11:562–566. 2018. View Article : Google Scholar
|
|
91
|
Nikolakis G, Brunner M, Boye H, Arndt N,
Altenburg A, Vaiopoulos A and Zouboulis CC: Enlarged mediastinal
lymph nodes of a patient with malignant melanoma stage IV under
pembrolizumab treatment. Hautarzt. 70:443–446. 2019.In German.
View Article : Google Scholar
|
|
92
|
Lederhandler MH, Ho A, Brinster N, Ho RS,
Liebman TN and Lo Sicco K: Severe oral mucositis: A rare adverse
event of pembrolizumab. J Drugs Dermatol. 17:807–809. 2018.
|
|
93
|
Parakh S, Cebon J and Klein O: Delayed
autoimmune toxicity occurring several months after cessation of
anti-PD-1 therapy. Oncologist. 23:849–851. 2018. View Article : Google Scholar
|
|
94
|
Moreira A, Loquai C, Pfohler C, Kahler KC,
Knauss S, Heppt MV, Gutzmer R, Dimitriou F, Meier F, Mitzel-Rink H,
et al: Myositis and neuromuscular side-effects induced by immune
checkpoint inhibitors. Eur J Cancer. 106:12–23. 2019. View Article : Google Scholar
|
|
95
|
Neilan TG, Rothenberg ML, Amiri-Kordestani
L, Sullivan RJ, Steingart RM, Gregory W, Hariharan S, Hammad TA,
Lindenfeld J, Murphy MJ, et al: Myocarditis associated with immune
checkpoint inhibitors: An expert consensus on data Gaps and a call
to action. Oncologist. 23:874–878. 2018. View Article : Google Scholar
|
|
96
|
Alnabulsi R, Hussain A and DeAngelis D:
Complete ophthal-moplegia in Ipilmumab and Nivolumab combination
treatment for metastatic melanoma. Orbit. 37:381–384. 2018.
View Article : Google Scholar
|
|
97
|
Kurokawa M, Kurokawa R, Hagiwara A, Gonoi
W, Harayama S, Koizumi K, Yoshino K, Hishima T, Baba A, Ota Y, et
al: CT imaging findings of anti-PD-1 inhibitor-related
enterocolitis. Abdom Radiol (NY). 46:3033–3043. 2021. View Article : Google Scholar
|
|
98
|
Luoma AM, Suo S, Williams HL, Sharova T,
Sullivan K, Manos M, Bowling P, Hodi FS, Rahma O, Sullivan RJ, et
al: Molecular pathways of colon inflammation induced by cancer
immunotherapy. Cell. 182:655–671.e22. 2020. View Article : Google Scholar
|
|
99
|
Zhao L, Yu J, Wang J, Li H, Che J and Cao
B: Risk of immune-related diarrhea with PD-1/PD-L1 inhibitors in
different cancer types and treatment regimens. J Cancer. 11:41–50.
2020. View Article : Google Scholar
|
|
100
|
Shivaji UN, Jeffery L, Gui X, Smith SCL,
Ahmad OF, Akbar A, Ghosh S and Iacucci M: Immune checkpoint
inhibitor-associated gastrointestinal and hepatic adverse events
and their manage-ment. Therap Adv Gastroenterol. Nov 5–2019.Epub
ahead of print. View Article : Google Scholar
|
|
101
|
Alvarez M, Otano I, Minute L, Ochoa MC,
Perez-Ruiz E, Melero I and Berraondo P: Impact of prophylactic TNF
blockade in the dual PD-1 and CTLA-4 immunotherapy efficacy and
toxicity. Cell Stress. 3:236–239. 2019. View Article : Google Scholar
|
|
102
|
Nadeau BA, Fecher LA, Owens SR and
Razumilava N: Liver toxicity with cancer checkpoint inhibitor
therapy. Semin Liver Dis. 38:366–378. 2018. View Article : Google Scholar
|
|
103
|
Straub BK, Ridder DA, Schad A, Loquai C
and Schattenberg JM: Liver injury induced by immune checkpoint
inhibitor-therapy: Example of an immune-mediated drug side effect.
Pathologe. 39:556–562. 2018.In German. View Article : Google Scholar
|
|
104
|
Rahman W, Conley A and Silver KD:
Atezolizumab-induced type 1 diabetes mellitus in a patient with
metastatic renal cell carcinoma. BMJ Case Rep. 13:e2338422020.
View Article : Google Scholar
|
|
105
|
Quandt Z, Young A and Anderson M: Immune
checkpoint inhibitor diabetes mellitus: A novel form of autoimmune
diabetes. Clin Exp Immunol. 200:131–140. 2020. View Article : Google Scholar
|
|
106
|
Agrawal L, Bacal A, Jain S, Singh V,
Emanuele N, Emanuele M and Meah F: Immune checkpoint inhibitors and
endocrine side effects, a narrative review. Postgrad Med.
132:206–214. 2020. View Article : Google Scholar
|
|
107
|
Bailly C: Potential use of edaravone to
reduce specific side effects of chemo-, radio-and immuno-therapy of
cancers. Int Immunopharmacol. 77:1059672019. View Article : Google Scholar
|
|
108
|
Zhu Y, Wu HH and Wang W: A case of
small-cell lung cancer with adrenocorticotropic hormone deficiency
induced by nivolumab. Onco Targets Ther. 12:2181–2186. 2019.
View Article : Google Scholar
|
|
109
|
Li S, Zhang Y, Sun Z, Hu J and Fang C:
Anti-PD-1 pembrolizumab induced autoimmune diabetes in Chinese
patient: A case report. Medicine (Baltimore). 97:e129072018.
View Article : Google Scholar
|
|
110
|
Solinas C, Porcu M, De Silva P, Musi M,
Aspeslagh S, Scartozzi M, Willard-Gallo K, Mariotti S and Saba L:
Cancer immunotherapy-associated hypophysitis. Semin Oncol.
45:181–186. 2018. View Article : Google Scholar
|
|
111
|
Briet C, Albarel F, Kuhn E, Merlen E,
Chanson P and Cortet C: Expert opinion on pituitary complications
in immunotherapy. Ann Endocrinol (Paris). 79:562–568. 2018.
View Article : Google Scholar
|
|
112
|
Clotman K, Janssens K, Specenier P, Weets
I and De Block CEM: Programmed cell death-1 inhibitor-induced type
1 diabetes mellitus. J Clin Endocrinol Metab. 103:3144–3154. 2018.
View Article : Google Scholar
|
|
113
|
Sagiv O, Kandl TJ, Thakar SD, Thuro BA,
Busaidy NL, Cabanillas M, Jimenez C, Dadu R, Graham PH, Debnam JM
and Esmaeli B: Extraocular muscle enlargement and thyroid eye
disease-like orbital inflammation associated with immune checkpoint
inhibitor therapy in cancer patients. Ophthalmic Plast Reconstr
Surg. 35:50–52. 2019. View Article : Google Scholar
|
|
114
|
Gauci ML, Laly P, Vidal-Trecan T,
Baroudjian B, Gottlieb J, Madjlessi-Ezra N, Da Meda L,
Madelaine-Chambrin I, Bagot M, Basset-Seguin N, et al: Autoimmune
diabetes induced by PD-1 inhibitor-retrospective analysis and
pathogenesis: A case report and literature review. Cancer Immunol
Immunother. 66:1399–1410. 2017. View Article : Google Scholar
|
|
115
|
Okamoto M, Okamoto M, Gotoh K, Masaki T,
Ozeki Y, Ando H, Anai M, Sato A, Yoshida Y, Ueda S, et al:
Fulminant type 1 diabetes mellitus with anti-programmed cell
death-1 therapy. J Diabetes Investig. 7:915–918. 2016. View Article : Google Scholar
|
|
116
|
Rossi E, Sgambato A, De Chiara G, Casaluce
F, Losanno T, Sacco PC, Santabarbara G and Gridelli C:
Endocrinopathies induced by immune-checkpoint inhibitors in
advanced non-small cell lung cancer. Expert Rev Clin Pharmacol.
9:419–428. 2016. View Article : Google Scholar
|
|
117
|
Kim KH, Sim WY and Lew BL:
Nivolumab-induced alopecia areata: A case report and literature
review. Ann Dermatol. 33:284–288. 2021. View Article : Google Scholar
|
|
118
|
Navarro-Fernandez I, Gonzalez-Vela C,
Gomez-Fernandez C, Duran-Vian C, Reguero L and Gonzalez-Lopez M:
Vitiligo-like depigmentation in a patient undergoing treatment with
nivolumab for advanced renal-cell carcinoma. Acta Dermatovenerol
Croat. 291:54–55. 2021.
|
|
119
|
Gracia-Cazana T, Padgett E,
Hernandez-Garcia A and Sanchez-Salas MP: Vitiligo-like lesions
located over In-transit metastases of malignant melanoma as a
clinical marker of complete response to pembrolizumab. Dermatol
Online J. 25:13030/qt8d3818j52019. View Article : Google Scholar
|
|
120
|
Cardis MA, Jiang H, Strauss J, Gulley JL
and Brownell I: Diffuse lichen planus-like keratoses and clinical
pseudo-progression associated with avelumab treatment for Merkel
cell carcinoma, a case report. BMC Cancer. 19:5392019. View Article : Google Scholar
|
|
121
|
Rambhia PH, Honda K and Arbesman J:
Nivolumab induced inflammation of seborrheic keratoses: A novel
cutaneous manifestation in a metastatic melanoma patient. Melanoma
Res. 28:475–477. 2018. View Article : Google Scholar
|
|
122
|
Lopez AT, Khanna T, Antonov N,
Audrey-Bayan C and Geskin L: A review of bullous pemphigoid
associated with PD-1 and PD-L1 inhibitors. Int J Dermatol.
57:664–669. 2018. View Article : Google Scholar
|
|
123
|
Obara K, Masuzawa M and Amoh Y: Oral
lichenoid reaction showing multiple ulcers associated with
anti-programmed death cell receptor-1 treatment: A report of two
cases and published work review. J Dermatol. 45:587–591. 2018.
View Article : Google Scholar
|
|
124
|
Seethapathy H, Zhao S, Strohbehn IA, Lee
M, Chute DF, Bates H, Molina GE, Zubiri L, Gupta S, Motwani S, et
al: Incidence and clinical features of immune-related acute kidney
injury in patients receiving programmed cell death ligand-1
inhibitors. Kidney Int Rep. 5:1700–1705. 2020. View Article : Google Scholar
|
|
125
|
Bickel A, Koneth I, Enzler-Tschudy A,
Neuweiler J, Flatz L and Fruh M: Pembrolizumab-associated minimal
change disease in a patient with malignant pleural mesothelioma.
BMC Cancer. 16:6562016. View Article : Google Scholar
|
|
126
|
Boegeholz J, Brueggen CS, Pauli C,
Dimitriou F, Haralambieva E, Dummer R, Manz MG and Widmer CC:
Challenges in diagnosis and management of neutropenia upon exposure
to immune-checkpoint inhibitors: Meta-analysis of a rare
immune-related adverse side effect. BMC Cancer. 20:3002020.
View Article : Google Scholar
|
|
127
|
Wang W, Lam WC and Chen L: Recurrent grade
4 panuveitis with serous retinal detachment related to nivolumab
treatment in a patient with metastatic renal cell carcinoma. Cancer
Immunol Immunother. 68:85–95. 2019. View Article : Google Scholar
|
|
128
|
Yatim N, Mateus C and Charles P:
Sarcoidosis post-anti-PD-1 therapy, mimicking relapse of metastatic
melanoma in a patient undergoing complete remission. Rev Med
Interne. 39:130–133. 2018. View Article : Google Scholar
|
|
129
|
Zheng Y, Meng X, Zweigenbaum P, Chen L and
Xia J: Hybrid phenotype mining method for investigating off-target
protein and underlying side effects of anti-tumor immunotherapy.
BMC Med Inform Decis Mak. 20(Suppl 3): S1332020. View Article : Google Scholar
|
|
130
|
Gauci ML, Baroudjian B, Laly P, Madelaine
I, Da Meda L, Vercellino L, Bagot M, Liote F, Pages C and Lebbe C:
Remitting seronegative symmetrical synovitis with pitting edema
(RS3PE) syndrome induced by nivolumab. Semin Arthritis Rheum.
47:281–287. 2017. View Article : Google Scholar
|
|
131
|
Uemura M, Fa'ak F, Haymaker C, McQuail N,
Sirmans E, Hudgens CW, Barbara L, Bernatchez C, Curry JL, Hwu P, et
al: Erratum to: A case report of Grover's disease from
immunotherapy-a skin toxicity induced by inhibition of CTLA-4 but
not PD-1. J Immunother Cancer. 5:72017. View Article : Google Scholar
|