Introduction
Sinonasal small cell carcinoma (SmCC) is a subtype
of sinonasal neuroendocrine carcinoma (SNEC). Until 2013, only 76
cases of SmCC had been reported in the literature (1). In 2016, a study by Van der Laan et
al (2) published the cases of
115 patients with SmCC. An analysis of the National Cancer Database
performed by Pointer et al (3) described 162 cases of SmCC. Smoking is
known to be associated with aggressive SmCC and the median survival
for SmCC is 22 months (2,3).
The histological subtypes of SNEC depend on the
differentiation grade and include poorly differentiated small cell
SmCC, poorly differentiated or undifferentiated large cell SNEC and
well to moderately differentiated SNEC (2). Diagnosis of the SmCC subtype requires
positivity for certain immunohistochemical markers, such as CD55
and thyroid transcription factor-1 (TTF-1). Positive synaptophysin
or chromogranin A expression may also be present, but these markers
are not required for diagnosis. Positive Ki-67 protein expression
is also used as a cell proliferation marker for SmCC (4,5).
The treatment response of patients with SmCC depends
on the stage, differentiation grade and proliferation rate
(6). It is known that stage IV
disease, poor differentiation and high cell proliferation rate
predict a worse treatment response (6,7). It
has been suggested that radiotherapy (RT) may be the most effective
treatment option for these patients (2,4).
However, other studies and the guidelines issued by the French
Cervico-facial Carcinological Society have indicated that etoposide
plus cisplatin may be the best treatment option (1,3,6,7).
Currently, no consensus has been reached regarding the optimal
treatment approach to SmCC (8).
Irinotecan plus gemcitabine can be used as second-line therapy for
relapsed or refractory small cell carcinoma (9,10).
SmCC has a poor prognosis; according to Pointer
et al (3), the median
survival time of patients with SmCC is 36.4 months. Another
systematic review of 80 patients with SmCC revealed a survival rate
of 46.3% after a mean follow-up of 30.8 months, whereby 43.1% of
the patients succumbed to the disease due to metastasis and 5.6%
due to other causes (8).
Case report
The current case report presents the case of a
30-year-old male patient with diabetes, who was a smoker (20
cigarettes/day) and a fisherman by profession; the patient
presented with daily headaches and mild recurrent episodes of
unilateral epistaxis from the left nostril that had persisted for
40 days. The patient attended Los Arcos del Mar Menor University
Hospital (Murcia, Spain). Fibroscopy examination performed in
September 2019 showed an exophytic pink mass in the left nasal
cavity. Cervical and paranasal sinus computed tomography (CT)
performed 5 days later revealed a mass in the left maxillary sinus
extending to the nasal cavity, ethmoidal sinus, sphenoid sinus,
cribriform plate, lamina papyracea, posterior intraconal orbital
space and left jugular foramen. A sinonasal biopsy was taken under
topical anesthesia. Immunohistochemistry was subsequently
performed. Paranasal tissues were fixed in 10% formalin at room
temperature (26˚C) for 24 h. The tissues were then
paraffin-embedded (60˚C), cut into 2.5-µm sections and introduced
in an integrated staining and mounting system (Tissue Tek
Prisma® Plus-Tissue Tek Film®; Sakura Finetek
USA) for 45 min at 26˚C, followed by deparaffinization with xylene,
rehydration in various grades of alcohol (100% up to distilled
water), staining with Harris hematoxylin (9 min at 26˚C, followed
by rinsing in distilled water), staining with eosin yellow (8 min
at 26˚C), dehydration in various grades of alcohol (70% up to
100%), and mounting in xylene-based medium (DPX-Tissue
Tek® Coverslipping film; Sakura Finetek USA). The
sections were subsequently incubated with primary antibodies
against CD56, TTF-1, chromogranin A, synaptophysin and Ki67. The
duration of the incubation of these antibody incubations ranged
between 12 and 16 min at 36-37˚C. Sections were visualized under a
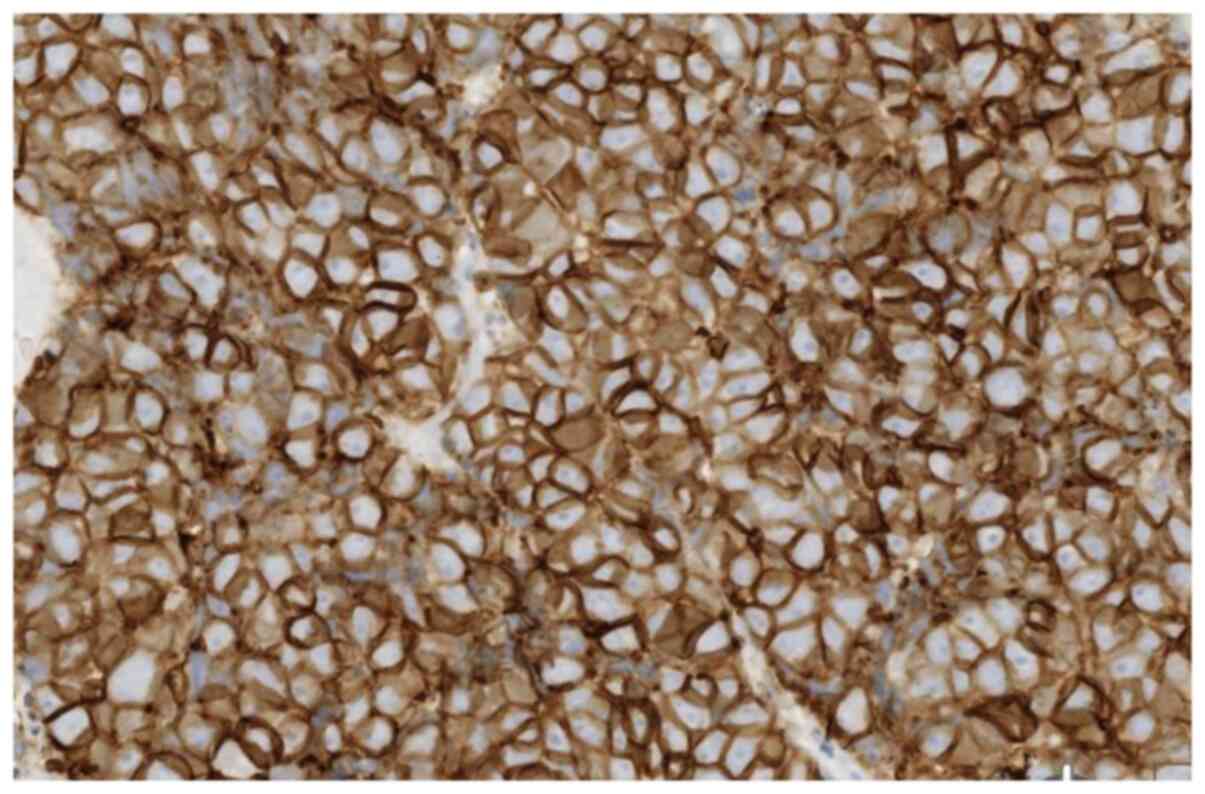
light microscope (magnification, x40). Anti-CD56 (1:125; cat. no.
123C3, Roche Diagnostics) exhibited intense membrane positivity in
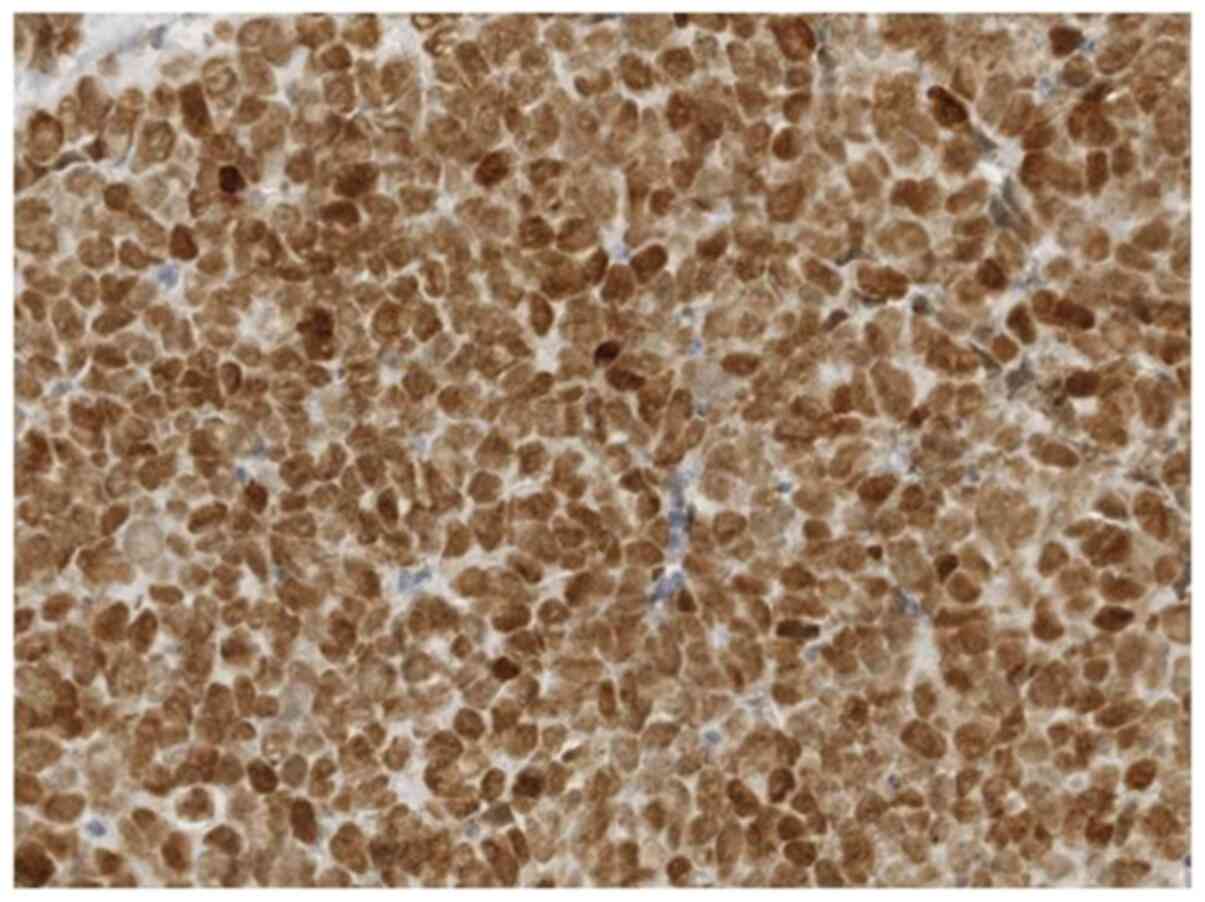
100% of the tumor cells. Anti-TTF-1 (1:175; cat. no. SP141, Roche
Diagnostics) exhibited intense nuclear positivity in 100% of the
tumor cells. Anti-chromogranin A (1:1,000; cat. no. LH2H10, Roche
Diagnostics) staining was negative. Anti-synaptophysin (1:200; cat.
no. SP11, Roche Diagnostics) staining was negative. Anti-Ki-67
(1:500; cat. no. 30-9, Roche Diagnostics) was positive in 90% of
the tumor cells. Immunohistochemistry examination demonstrated
neuroendocrine marker CD56 (Fig.
1) and TTF-1 (Fig. 2)
positivity. Sinonasal biopsy revealed an SmCC.
Metastasis was ruled out by positron emission
tomography (PET)/CT (cT4N0M0). In October 2019, RT plus
etoposide-cisplatin was administered as the first-line treatment. A
total of 50 Gy was delivered in 25 daily fractions of RT. The
patient received four cycles (every 21 days) of cisplatin (100
mg/m2; IV) and etoposide (100 mg/m2; IV) on
day 1, followed by etoposide (200 mg/m2) on days 2-3.
PET/CT and fibroscopy confirmed complete remission in March 2020.
The patient was evaluated every 2 months according to the National
Comprehensive Cancer Network (11). Subsequently, 5 months later, the
patient underwent lumbar MRI due to lumbar back pain that had
persisted for >3 weeks, which revealed leptomeningeal metastasis
(LM) in the medullary cone. In September 2020, the patient received
palliative RT (20 Gy in 5 fractions) plus six cycles (every 21
days) of irinotecan (100 mg/m2; IV) on days 1-8 and
gemcitabine (1,000 mg/m2; IV). During the sixth cycle of
irinotecan-gemcitabine (October 2020), the patient was admitted to
intensive care due to severe acute respiratory syndrome-related
coronavirus 2 (SARS-Cov-2)-associated pneumonia. A total of 3
months after the clearance of the pneumonia, LM was assessed using
PET/CT, and a complete response to irinotecan-gemcitabine was
confirmed. However, in May 2021, the patient succumbed to the
disease following LM recurrence.
Discussion
The present case study reports an extremely rare and
aggressive carcinoma of the paranasal sinuses with an unusual site
of metastasis. Literature searches reveal few reported cases of
SmCC. In the present study, three Anatomical Pathology Units at
different public hospitals in Murcia were required to confirm the
histological diagnosis of SmCC. In the present case report,
immunohistochemical staining for chromogranin A and synaptophysin
was negative, while staining for CD56, TTF-1 and Ki-67 (90%) was
positive (5,7). The three Anatomical Pathology Units
reached the same histological diagnosis.
The Head and Neck Tumors Committee of Los Arcos del
Mar Menor University Hospital considered RT plus chemotherapy to be
the most appropriate treatment instead of nasal surgery based on
the result of an analysis of the National Cancer Database published
in 2017, in which it was stated that nasal surgery did not improve
the survival rate of patients with stage IV SmCC (3). At present, there are no clear
guidelines regarding SmCC treatment. Only 30 articles were found in
the PubMed database using the keywords ‘sinonasal’ AND ‘small cell
carcinoma’ AND ‘treatment’ (https://pubmed.ncbi.nlm.nih.gov/?term=%22sinonasal%22+AND+%22Small+Cell+Carcinoma%22+AND+%22+Treatment%22).
The limited number of reports on SmCC in the literature could be
one of the reasons for the lack of treatment guidelines. Three
articles were found in the PubMed database using the keywords
‘leptomeningeal metastasis’ AND ‘neuroendocrine carcinoma’, but no
articles were found using the keywords ‘leptomeningeal metastasis’
AND ‘small cell carcinoma’ (https://pubmed.ncbi.nlm.nih.gov/?term=%22leptomeningeal+metastasis%22+AND+%22neuroendocrine+carcinoma%22).
In the present study, irinotecan-gemcitabine was
used as the treatment for the LM based on data reported in some
publications which found that the irinotecan-gemcitabine
combination was effective and well-tolerated as second-line therapy
for small-cell lung cancer (9,10).
Only one article was found in the PubMed database
using the keywords ‘irinotecan’ AND ‘gemcitabine’ AND ‘SARS CoV-2’,
and no patient infected with SARS-CoV-2 was described in that
article (12). The sample size of
the study by Vidra et al (12) was too small as it only included 11
patients; thus, the result is not conclusive. More clinical trials
are required to determine the true relationship between SARS-CoV-2
infection and irinotecan-gemcitabine combination treatment
(12).
In May 2021, the patient required intensive care
admission due to impaired consciousness and abdominal pain.
Analysis of lumbar puncture fluid revealed LC recurrence despite a
PET/CT scan ruling out metastasis 1 month prior. The patient
succumbed to the disease 5 days later.
In conclusion, there are no clear guidelines
regarding SmCC treatment at present. Thus, other authors should be
encouraged to publish their treatment outcomes regarding SmCC. More
clinical trials should be performed to optimize treatment and
improve patient outcome.
Acknowledgements
Not applicable.
Funding
Funding: The publication of this study was supported by AMPLIFON
IBERICA SAU.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AR designed the study; MJMO acquired the data; CB
interpreted the data; EG and AB drafted the manuscript and acquired
the data; and FGP analyzed and interpreted the data. All authors
have read and approved the final manuscript. EG and AB confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent
regarding the publication of all case details and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Krishnamurthy A, Ravi P, Vijayalakshmi R
and Majhi U: Small cell neuroendocrine carcinoma of the paranasal
sinus. Natl J Maxillofac Surg. 4:111–113. 2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
van der Laan TP, Iepsma R, Witjes MJ, van
der Laan BF, Plaat BE and Halmos GB: Meta-analysis of 701 published
cases of sinonasal neuroendocrine carcinoma: The importance of
differentiation grade in determining treatment strategy. Oral
Oncol. 63:1–9. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Pointer KB, Ko HC, Brower JV, Witek ME,
Kimple RJ, Lloyd RV, Harari PM and Baschnagel AM: Small cell
carcinoma of the head and neck: An analysis of the National Cancer
Database. Oral Oncol. 69:92–98. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rosenthal DI, Barker JL Jr, El-Naggar AK,
Glisson BS, Kies MS, Diaz EM Jr, Clayman GL, Demonte F, Selek U,
Morrison WH, et al: Sinonasal malignancies with neuroendocrine
differentiation: patterns of failure according to histologic
phenotype. Cancer. 101:2567–2573. 2004.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Agoff SN, Lamps LW, Philip AT, Amin MB,
Schmidt RA, True LD and Folpe AL: Thyroid transcription factor-1 is
expressed in extrapulmonary small cell carcinomas but not in other
extrapulmonary neuroendocrine tumors. Mod Pathol. 13:238–242.
2000.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wani SQ, Dar IA, Khan T and Lone MM:
Primary Sino-nasal Neuroendocrine Carcinoma: A Rare Tumor. Cureus.
11(e4144)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Iacovou E, Chrysovergis A, Eleftheriadou
A, Yiotakis I and Kandiloros D: Neuroendocrine carcinoma arising
from the septum. A very rare nasal tumour. Acta Otorhinolaryngol
Ital. 31:50–53. 2011.PubMed/NCBI
|
|
8
|
Rivero A and Liang J: Sinonasal small cell
neuroendocrine carcinoma: A systematic review of 80 patients. Int
Forum Allergy Rhinol. 6:744–751. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Rocha-Lima CM, Herndon JE II, Lee ME,
Atkins JN, Mauer A, Vokes E and Green MR: Cancer and Leukemia Group
B. Phase II trial of irinotecan/gemcitabine as second-line therapy
for relapsed and refractory small-cell lung cancer: Cancer and
Leukemia Group B Study 39902. Ann Oncol. 18:331–337.
2007.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Schuette W, Nagel S, Juergens S, Bork I,
Wollschlaeger B, Schaedlich S and Blankenburg T: Phase II trial of
gemcitabine/irinotecan in refractory or relapsed small-cell lung
cancer. Clin Lung Cancer. 7:133–137. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
National Comprehensive Cancer Network
(NCCN): NCCN Guidelines for Head and Neck Cancers V.1.2021. NCCN,
Plymouth Meeting, PA, 2021. https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManager?fileManagerId=11180.
Accessed October 18, 2021.
|
|
12
|
Vidra R, Bodea R, Mercea V and Nemes A:
Challenges of pancreatic cancer chemotherapy in the COVID-19 era. J
Gastrointestin Liver Dis. 29:273–275. 2020.PubMed/NCBI View Article : Google Scholar
|