Bone produces osteocalcin
Bone is a dynamic tissue in constant remodeling
(resorption and formation) and with a high capacity to regenerate.
In addition to providing support to the body, protection for
certain organs and enabling locomotion, bone produces molecules
that act in an autocrine, paracrine and endocrine manner (1). One such molecule is osteocalcin, the
endocrine function of which was discovered 10 years ago. Due to its
extensive secretion during bone mineralization, osteocalcin was
suspected to be exclusive to bone physiology. However, through
studies performed in mice, the role of osteocalcin in metabolic
modulation was elucidated (2,3).
Osteocalcin is a small protein (49 amino acids)
encoded by the BGLAP gene synthesized by osteoblasts, and is
present in two forms: Carboxylated (cOC) and undercarboxylated
(ucOC). Only ucOC can signal as a hormone while cOC cannot
(2,3).
ucOC and cOC can be measured in plasma separately or
as the total osteocalcin (tOC), which includes the two forms
independently of their degree of carboxylation, as well as
recognizable fragments released when bone resorption occurs. Only
10–30% of the secreted osteocalcin reaches systemic circulation,
while the remaining fraction is incorporated into bone matrix. In
bone, cOC represents 15% of the non-collagen proteins of the matrix
and contains three γ-carboxyglutamic acid residues. On the other
hand, ucOC represents one third of tOC. The serum concentration of
tOC has been considered a biochemical marker of osteogenesis that
reflects the number and activity of osteoblasts (4,5).
Identification of the endocrine effect of
osteocalcin and its action through GPRC6A
In 2007, Lee et al (6) demonstrated that ucOC increases the
insulin secretion and proliferation of pancreatic β-cells, as well
as adiponectin secretion from adipose tissue, thereby improving
insulin sensitivity in mice. They also demonstrated that
osteocalcin reduces fat mass and increases energy expenditure by
increasing the expression of genes involved in β-oxidation
(Pparα and Foxa2) and in the electron transport chain
(Atp5a1, Atp5b, Mt-nd2, Cox and Cyc1). This was the
first irrefutable evidence of the participation of osteocalcin in
carbohydrate, lipid and energy metabolism (6).
ucOC acts through binding to G protein-coupled
receptor family C group 6-member A (GPRC6A). In fact, ucOC and
testosterone are the only ligands of Gprc6a that have been
validated using genetics in vivo, despite other ligands
having been discovered in vitro (7–9).
Although well stablished functions of OC through GPRC6A and GPR158
are presented later, a brief description of the expression,
localization and function of GPRC6A in human cells and tissues is
displayed next.
GPRC6A is expressed in several human, chimpanzee and
small species tissues, including brain, lung, liver, heart, kidney,
pancreas, skeletal muscle, placenta, spleen, ovary, testis,
leukocytes, monocytes and adipocytes. However, the human ortholog
GPRC6A is mostly retained intracellularly, in contrast to the
cell-surface-expressed murine and goldfish ortholog (9,10).
This intracellular retention occurs in carriers of
an insertion/deletion in exon 2 (SNP rs6907580 A/G/T) that
eventually leads to a stop-codon early in the receptor sequence at
amino acid position 57 (located in the third intracellular loop of
GPRC6A), resulting in a non-functional receptor as reported by
Jørgensen et al (10).
According to this author, the functional variant is much more
prevalent in the African population than in European and Asian
populations, but further studies are required to elucidate the
clinical significance of this allele variation among different
populations (10).
As three mRNA isoforms for Gprc6a have been
identified (1365, 853 and 1165 bp), the functionality of the GPRC6A
receptor may be dependent on a tissue-specific regulation
mechanism, which is also the case for other receptors whose
function and tissue-specific expression is regulated by alternative
splicing (11). GPRC6A mRNA
isoform 1 is highly expressed in the brain, skeletal muscle, testis
and leucocytes; moderately expressed in the liver, heart, kidney
and spleen; and lowly expressed in the lung, pancreas, adipocytes,
placenta and ovary. Isoforms 2 and 3 are less abundant and are
possibly naturally occurring splice variants (12). Therefore, although the pancreas and
adipocytes express low levels of GPRC6A mRNA at the transcriptional
level, these are the main organs of ucOC action, suggesting a
different mechanism of regulation at other levels (translational
and post-translational) or the existence of an ortholog receptor
that also partially mediates the action of ucOC.
Downstream signaling pathways activated by
the osteocalcin-GPRC6A interaction
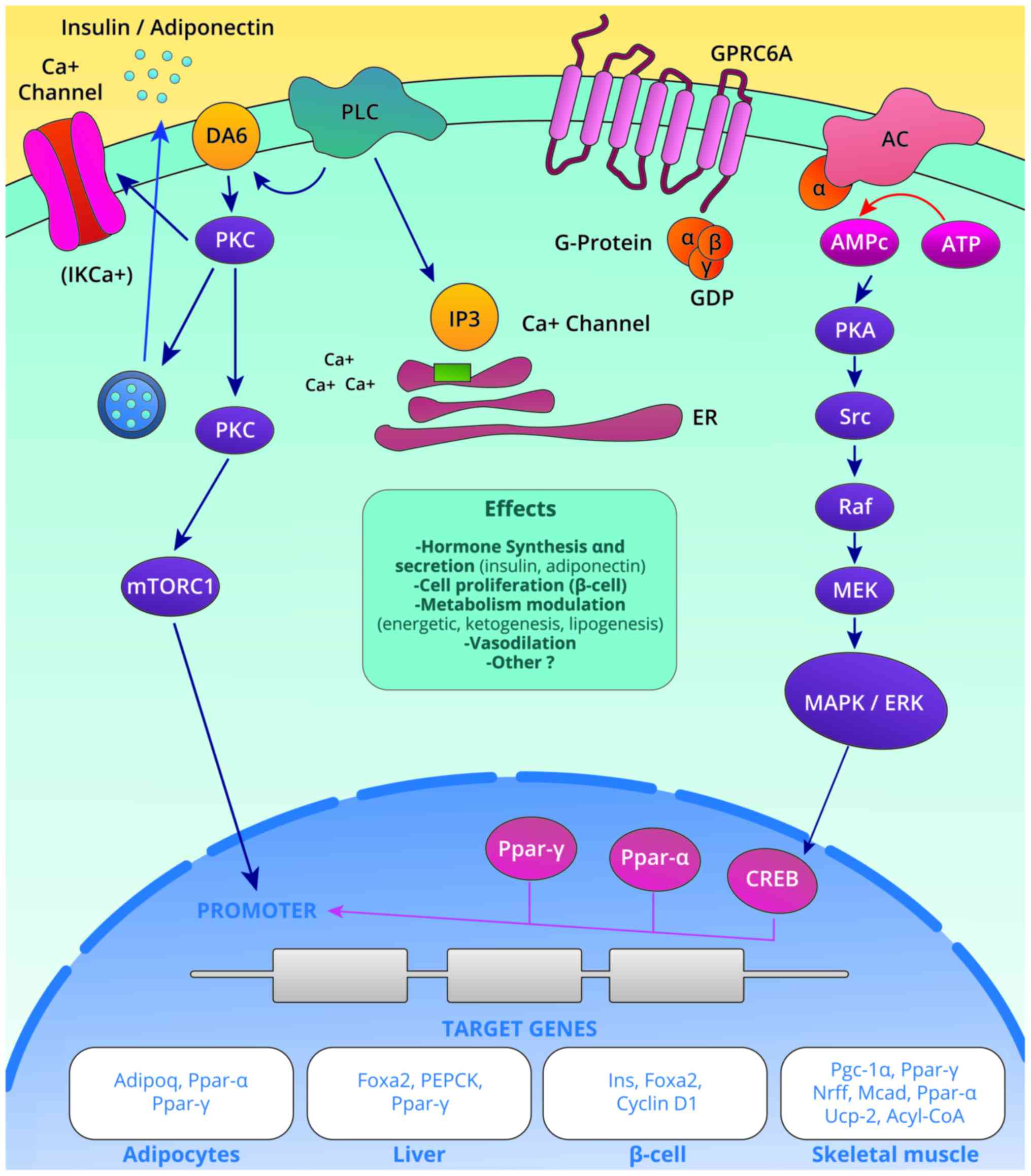
At least two signaling pathways activated by the
osteocalcin-GPRC6A interactions have been identified (Fig. 1): i) The IP3-Ca+2
pathway activated by the action of phospholipase C (PLC) that
yields the secretion of insulin, adiponectin and possibly other
hormones; and ii) the adenylyl cyclase-cAMP-PKA pathway that leads
to the activation of the Mek-Erk cascade, thereby promoting
functions in cellular proliferation, differentiation and modulation
of insulin sensitivity (13).
The extracellular signal-regulated kinases (Erk)
induce phosphorylation of CREB, which in turn binds to the cAMP
response element (CRE) in the Pparγ gene. The Pparγ
gene consequently leads to the transactivation of the adiponectin
gene (Adipoq) by linking the Pparγ-Rxr heterodimer to the
promoter region of the Adipoq gene, resulting in the
synthesis of adiponectin (14).
Signaling pathways are depicted in Fig. 1. In the pancreas, the binding of
osteocalcin to GPRC6A also induces Erk phosphorylation and
increases insulin synthesis (7).
In Leydig cells, ucOC activates the ERK1/2 signaling pathway,
increasing the intracellular calcium content and promoting the
production of 25-OH Vitamin D (8).
Furthermore, osteocalcin promotes the nuclear
translocation of activated Nrf2, while inhibiting the activation of
JNK in the liver; these are two well-described pathways in the
pathogenesis of non-alcoholic fatty liver disease (NAFLD) (15).
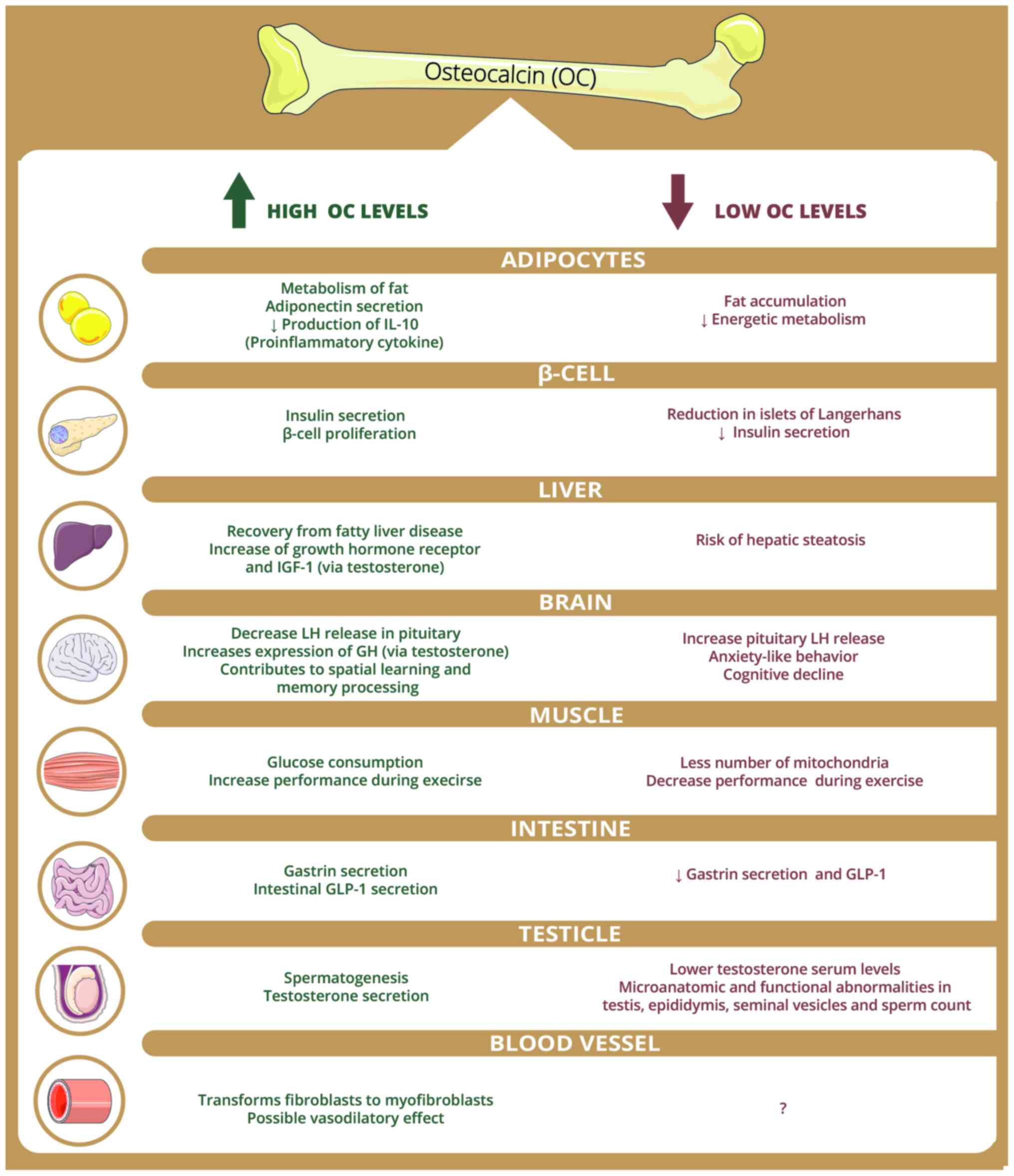
Osteocalcin target tissues
Independently of the tissues where GPRC6A is
expressed or is functionally active and, of the discoveries of
signaling pathways that it activates, there are clear effects of
ucOC in certain tissues and cells that are summarized in Fig. 2 and are described in the following
paragraphs.
Pi et al (16) reported that knockout mice for the
GPRC6A receptor (−/−) and that those that do not express the
GPRC6A gene in pancreatic islets
(GPRC6Aβ−cell-cko) have a smaller pancreatic
islet size, lower insulin content, lower pancreatic weight, lower
number of islets, lower insulin mRNA expression and lower insulin
secretion in response to osteocalcin. Furthermore, these mice
exhibit glucose intolerance with a non-altered sensitivity to
insulin. In this way, it was established that the direct activation
of GPRC6A by osteocalcin modifies β-cell proliferation and insulin
secretion (16). These findings
were confirmed by Wei et al (17), who demonstrated that osteocalcin
promotes the proliferation of pancreatic β-cells during development
and adulthood through GPRC6A in mice (14,17).
In rodent-derived cultured adipocytes, Otani et
al (18) demonstrated that
ucOC increases the expression of adiponectin by increasing cAMP
through GPRC6A activation. This occurs thanks to intracellular ERK
signaling, which leads to the expression of Pparγ and the
subsequent production of this insulin-sensitizing hormone (14,18).
In skeletal muscle, osteocalcin binds to GPRC6A,
favoring the uptake and catabolism of glucose and fatty acids
during exercise. In line with this, it stimulates the release of
interleukin-6 by the muscle, a molecule that modulates the
secretion of ucOC in the bone, increases the hepatic production of
glucose and stimulates the release of fatty acids from the
adipocyte. During aerobic exercise, circulating levels of ucOC
doubled at the time insulin reaches its lowest point. By contract,
in aged mice, osteocalcin is required and sufficient to maintain
muscle mass. Therefore, osteocalcin participates in the body's
adaptation to exercise and aids in maintaining muscle mass
(19,20).
In the liver of mice, osteocalcin has been proven to
be a deterrent of NAFLD. Following intermittent and continuous
intraperitoneal infusion, osteocalcin upregulates the expression of
antioxidant genes, including Cat, Sod and Gpx, which
encode catalase, superoxide dismutase and glutathione peroxidase.
Osteocalcin also decreases the content of triglycerides and
reverses the histological damage in the liver of mice with NAFLD
(15,20).
A potential interaction of ucOC with GPRC6A in blood
vessels is possible but requires clarification, since
identification of GPRC6A receptors in the aortic rings of rats and
its activation by their agonist ornithine leads to the modulation
of ion channels, including the intermediate-conductance
Ca2+-dependent K+ (IKCa) channel, which in
turn generates myocyte hyperpolarization, which may indicate a
potential vasodilatory effect in vivo (17). As this is only an initial
observation, vascular actions should be investigated in depth.
In the testicle, ucOC binds to GPRC6A receptors in
Leydig cells to induce testosterone biosynthesis. Furthermore,
osteocalcin acts through a pancreas-bone-testis axis that regulates
male reproductive functions by promoting testosterone production
independently of and in parallel with the
hypothalamus-pituitary-testis axis (21). Additionally, knockout mice for
osteocalcin exhibit low testosterone serum levels and secretion by
Leydig cells, in addition to microanatomical and functional
abnormalities in the testis, epididymis, seminal vesicles and sperm
count (22–24).
GPRC6A receptors have also been observed in the
basolateral membranes of intestinal endocrine cells. Here, oral,
intraperitoneal and intravenous osteocalcin exerts its action by
binding to GPRC6A, which in turn increases the secretion of
glucagon-like peptide type 1 (GLP-1) in vitro and its serum
levels in mice (25,26). In fact, the concept of a
bone-intestine axis is plausible since, in addition to the effect
of ucOC on GLP-1 release, certain animal and human studies have
demonstrated that GLP-1 stimulates bone formation (the stage where
osteocalcin release occurs at a high rate) and reduce bone
resorption (25,26). In addition, certain osteoblastic
cell lines express the GLP-1 receptor, which is regulated in
accordance to the glycemic level (27). Despite this, limitations include
the few in vivo studies on this intestine-bone communication
and the fact that osteocalcin (−/−) mice exhibit no decrease in
serum GLP-1 levels (28).
In the brain, ucOC has several direct and indirect
effects, including increasing growth hormone synthesis (29). ucOC serves an important role in
memory increasing and decreasing anxiety by binding to the newly
identified GPR158 receptor, as described by Prof. Karsenty's group
(30,31). Additionally, regions of the brain
involved in spatial learning and memory processing exhibit an
intense accumulation of osteocalcin. Notably, the brains of mice
with low levels of osteocalcin are consistently smaller than those
where normal levels of osteocalcin are observed. Additionally, mice
with defective production of osteocalcin exhibit higher rates of
anxiety-like behavior and cognitive decline, and the two symptoms
are fully corrected when osteocalcin is injected into the test
subjects (32).
Importance of biological experimental
findings regarding osteocalcin in human health and disease
There is abundant evidence of the pleiotropic
effects of osteocalcin in animal and cellular models; however,
replicating these findings in humans is paramount to embarking on
meaningful translational research that will elucidate the
therapeutic and/or prognostic value of this hormone. For this
purpose, several studies have been conducted to assess and support
the role of osteocalcin in human health and disease.
Recently, it was reported that the rs2274911
polymorphism in the GPRC6A gene is associated with insulin
resistance in healthy weight and obese subjects independently of
body mass index (BMI). Carriers of the risk allele A exhibited
higher levels of fasting insulin, fasting plasma glucose, HOMA-IR
and triglycerides, following correction for sex, age and ucOC
levels (33). Furthermore, Oury
et al (23) analyzed a
cohort of patients with primary testicular failure and identified 2
individuals harboring the same heterozygous missense variant (SNP
rs2274911; F464Y) in one of the transmembrane domains of GPRC6A,
which prevented the receptor from localizing to the cell membrane.
These patients exhibit glucose intolerance, insulin resistance and
increased BMI (23). Therefore,
the A risk allele of this variant predisposes to metabolic
abnormalities and provides evidence of the importance of GPRC6A in
human energetic metabolism, as suggested by seven studies (34–40)
published in the last 10 years, comparing serum concentrations of
osteocalcin among people with type-2 diabetes mellitus (T2DM) and
the non-diabetic population. It is clear that lower levels of
osteocalcin occur more frequently in T2DM when compared with
healthy subjects (Table I). In
fact, a recent meta-analysis also suggested that serum tOC levels
may be lower among people with T2DM (41). Furthermore, patients with metabolic
syndrome also have lower levels of serum tOC than healthy
individuals, and an increase in serum tOC levels is associated with
a significant mean increase in HOMA-B and a mean reduction of
HbA1c, fasting plasma glucose levels, HOMA-IR and BMI (42). Additionally, a significant
correlation between tOC and ucOC serum levels exists with markers
of glycemic status and other cardio-metabolic parameters (43–50).
Table II describes the
correlation between tOC and ucOC and these glycemic and
cardio-metabolic variables.
 | Table I.Comparison of total OC and ucOC
concentrations between healthy and diabetic subjects. |
Table I.
Comparison of total OC and ucOC
concentrations between healthy and diabetic subjects.
| A, Total OC
(ng/ml) |
|---|
|
|---|
| Author, year | Diabetes | HS | P-value | (Refs.) |
|---|
| Pietschmann and
Schernthaner, 1988 | 5.2 | 6.6 | 0.03 | (34) |
| Rosato et al,
1998 | 2.5 | 4.4 | 0.0006 | (35) |
| Akin et al,
2003 | 4.44 | 8.82 | 0.05 | (36) |
| Achemlal et al,
2005 | 15.3 | 18.3 | 0.012 | (37) |
|
| B, ucOC
(ng/ml) |
|
| Author,
year |
Diabetes | HS | P-value | (Refs.) |
|
| Sanchez-Enriquez et
al, 2017 | 1.5±1.4 | 2.3±1.8 | <0.05 | (38) |
| Díaz-López et al,
2013 | 3.57 | 4.45 | 0.009 | (39) |
| Razny et al,
2016 | 3.04±0.28 | 4.48±0.57 | 0.025 | (40) |
| Table II.Correlation coefficients of total OC
and ucOC serum levels with glycemia, HbA1c, insulin and HOMA-IR,
blood pressure, lipids and cIMT. |
Table II.
Correlation coefficients of total OC
and ucOC serum levels with glycemia, HbA1c, insulin and HOMA-IR,
blood pressure, lipids and cIMT.
|
| Total OC |
| Undercarboxylated
OC |
|
|---|
|
|
|
|
|
|
|---|
| Variable | r | P-value | (Refs.) | r | P-value | (Refs.) |
|---|
| Glucose | −0.213 | 0.009 | (45) | −0.283 | 0.006 | (38) |
|
| −0.085 | 0.025 | (44) | −0.220 | NS | (59) |
| HbA1c | −0.140 | 0.208 | (46) | −0.228 |
| (60) |
|
| −0.023 | 0.573 | (44) | <0.001 |
|
|
| Insulin | −0.243 | 0.003 | (45) | −0.108 | <0.001 | (60) |
| HOMA-IR | −0.005 | NS | (47) | −0.349 | <0.05 | (61) |
|
|
|
|
| −0.144 | <0.001 | (60) |
| SBP | −0.068 | 0.001 | (48) | 0.277 | 0.049 | (38) |
| DBP | −0.077 | <0.001 | (48) | 0.450 | 0.003 | (38) |
| % body fat | −0.240 | <0.05 | (49) | −0.311 | 0.048 | (38) |
| BMI | −0.258 | <0.001 | (48) | −0.310 | 0.046 | (38) |
| c-HDL | 0.097 | <0.001 | (48) | 0.150 | 0.030 | (50) |
| Apo-B/Apo A-1 | −0.01 | 0.850 | (50) | −0.160 | 0.020 | (50) |
| cIMT | −0.145 | 0.041 | (43) | −0.33 | <0.01 | (59) |
Other studies have evaluated the association between
osteocalcin serum levels and parameters of atherosclerosis. The
majority of studies have reported a significant association between
osteocalcin serum levels and determinations of carotid intima-media
thickness (cIMT), brachial-ankle wave pulse velocity and carotid
plaques in patients with diabetes and healthy subjects (43,44,51–55).
A recent observational study evaluated the
association between osteocalcin serum levels and cognitive
performance in healthy adults, demonstrating that they were
positively correlated with measures of executive functioning and
global cognition in older women. The authors reported that lower
serum osteocalcin concentrations were associated with brain
microstructural changes in the putamen, thalamus and caudate, as
well as with poorer cognitive performance (56). These findings have therefore
broadened the functions undertaken by osteocalcin to include the
brain and neural processing.
Finally, two previous studies evaluated the
association between osteocalcin and NAFLD in children and
adolescents with and without obesity. Patients with NAFLD exhibited
lower serum osteocalcin levels than those in the control group and
the osteocalcin concentration were inversely correlated with liver
enzymes and the severity of NAFLD. In addition, a serum osteocalcin
level below 44.5 ng/ml was revealed to be a good predictor of
hepatic steatosis severity with a sensitivity and specificity of
80% (57,58). Furthermore, normoglycemic
postmenopausal women with NAFLD exhibited significantly lower serum
osteocalcin levels than controls and the serum osteocalcin levels
exhibited a negative correlation with the fatty liver index values,
even following adjusting for confounding factors (51). In males, NAFLD is negatively
associated with serum osteocalcin (53). These observations highlighted the
role of osteocalcin as a potential protector against NAFLD
development and deterioration, as well as a marker of its
progression.
In conclusion, the increasing volume of evidence
regarding the multi-organ effect of ucOC, supported by in
vivo and in vitro findings, indicates the requirement
for deeper approaches to clarify its participation in human health
and disease, as well as to test its therapeutic potential. On the
other hand, the validation of ucOC as a prognostic or pathogenic
marker for metabolic-endocrine disorders remains to be fully
elucidated since no universal standardized method for its
measurements, nor any reference values, have been established.
Therefore, the medical-scientific community must continue to
advance efforts to clarify the participation of ucOC in human
health and disease and the clinical implications of this.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used during this review are available
from the corresponding author on reasonable request.
Authors' contributions
MCD-F and RF-DL performed the literature search,
interpreted the results and wrote the manuscript. JRV-B conceived
the review, performed the literature search, interpreted the
results, wrote the manuscript and gave final approval of the
version to be published.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BGLAP
|
gene for osteocalcin
|
|
GPRC6A
|
G protein-coupled receptor family C
group 6-member A
|
|
ucOC
|
undercarboxylated osteocalcin
|
References
|
1
|
Moore KL and Dalley AF: Clinically
oriented anatomy. Lipp Williams Wilkins. 2013.
|
|
2
|
Ferron M, Hinoi E, Karsenty G and Ducy P:
Osteocalcin differentially regulates beta cell and adipocyte gene
expression and affects the development of metabolic diseases in
wild-type mice. Proc Natl Acad Sci USA. 105:5266–5270. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Villafán-Bernal JR, Sánchez-Enríquez S and
Muñoz-Valle JF: Molecular modulation of osteocalcin and its
relevance in diabetes (Review). Int J Mol Med. 28:283–293.
2011.PubMed/NCBI
|
|
4
|
Hauschka PV, Lian JB, Cole DE and Gundberg
CM: Osteocalcin and matrix Gla protein: Vitamin K-dependent
proteins in bone. Physiol Rev. 69:990–1047. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hernández-Gil IFT, Gracia MAA, Pingarrón
MDC and Jerez LB: Bases fisiológicas de la regeneración ósea I.
Histología y fisiología del tejido óseo. Med Oral Patol Oral Cir
Bucal. 11:47–51. 2006.
|
|
6
|
Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD,
Confavreux C, Dacquin R, Mee PJ, McKee MD, Jung DY, et al:
Endocrine regulation of energy metabolism by the skeleton. Cell.
130:456–469. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pi M, Wu Y and Quarles LD: GPRC6A mediates
responses to osteocalcin in β-cells in vitro and pancreas in vivo.
J Bone Miner Res. 26:1680–1683. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
De Toni L, De Filippis V, Tescari S,
Ferigo M, Ferlin A, Scattolini V, Avogaro A, Vettor R and Foresta
C: Uncarboxylated osteocalcin stimulates 25-hydroxy vitamin D
production in Leydig cell line through a GPRC6a-dependent pathway.
Endocrinology. 155:4266–4274. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Clemmensen C, Smajilovic S, Wellendorph P
and Bräuner-Osborne H: The GPCR class C, group 6, subtype A
(GPRC6A) receptor: Fom cloning to physiological function. Br J
Pharmacol. 171:1129–1141. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jørgensen S, Have CT, Underwood CR,
Johansen LD, Wellendorph P, Gjesing AP, Jørgensen CV, Quan S, Rui
G, Inoue A, et al: Genetic variations in the human G
protein-coupled receptor class C, group 6, member A (GPRC6A)
control cell surface expression and function. J Biol Chem.
292:1524–1534. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Arnold KA, Eichelbaum M and Burk O:
Alternative splicing affects the function and tissue-specific
expression of the human constitutive androstane receptor. Nucl
Recept. 2:12004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wellendorph P and Bräuner-Osborne H:
Molecular cloning, expression, and sequence analysis of GPRC6A, a
novel family C G-protein-coupled receptor. Gene. 335:37–46. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ozaki KI, Awazu M, Tamiya M, Iwasaki Y,
Harada A, Kugisaki S, Tanimura S and Kohno M: Targeting the ERK
signaling pathway as a potential treatment for insulin resistance
and type 2 diabetes. Am J Physiol Endocrinol Metab. 310:E643–E651.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mera P, Laue K, Wei J, Berger JM and
Karsenty G: Osteocalcin is necessary and sufficient to maintain
muscle mass in older mice. Mol Metab. 5:1042–1047. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Du J, Zhang M, Lu J, Zhang X, Xiong Q, Xu
Y, Bao Y and Jia W: Osteocalcin improves nonalcoholic fatty liver
disease in mice through activation of Nrf2 and inhibition of JNK.
Endocrine. 53:701–709. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pi M, Kapoor K, Ye R, Nishimoto SK, Smith
JC, Baudry J and Quarles LD: Evidence for osteocalcin binding and
activation of GPRC6A in β-cells. Endocrinology. 157:1866–1880.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wei J, Hanna T, Suda N, Karsenty G and
Ducy P: Osteocalcin promotes β-cell proliferation during
development and adulthood through Gprc6a. Diabetes. 63:1021–1031.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Otani T, Mizokami A, Hayashi Y, Gao J,
Mori Y, Nakamura S, Takeuchi H and Hirata M: Signaling pathway for
adiponectin expression in adipocytes by osteocalcin. Cell Signal.
27:532–544. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mera P, Laue K, Ferron M, Confavreux C,
Wei J, Galán-Díez M, Lacampagne A, Mitchell SJ, Mattison JA, Chen
Y, et al: Osteocalcin signaling in myofibers is necessary and
sufficient for optimum adaptation to exercise. Cell Metab.
23:1078–1092. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ferron M, McKee MD, Levine RL, Ducy P and
Karsenty G: Intermittent injections of osteocalcin improve glucose
metabolism and prevent type 2 diabetes in mice. Bone. 50:568–575.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Karsenty G and Oury F: Regulation of male
fertility by the bone-derived hormone osteocalcin. Mol Cell
Endocrinol. 382:521–526. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Le B, Chen H, Zirkin B and Burnett A: New
targets for increasing endogenous testosterone production: Clinical
implications and review of the literature. Andrology. 2:484–490.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Oury F, Ferron M, Huizhen W, Confavreux C,
Wei J, Galán-Díez M, Lacampagne A, Mitchell SJ, Mattison JA, Chen
Y, et al: Osteocalcin regulates murine and human fertility through
a pancreas-bone-testis axis. J Clin Invest. 123:2421–2433. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Smith LB and Saunders PT: The skeleton:
The new controller of male fertility? Cell. 144:642–643. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Mizokami A, Yasutake Y, Higashi S,
Kawakubo-Yasukochi T, Chishaki S, Takahashi I, Takeuchi H and
Hirata M: Oral administration of osteocalcin improves glucose
utilization by stimulating glucagon-like peptide-1 secretion. Bone.
69:68–79. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mizokami A, Yasutake Y, Gao J, Matsuda M,
Takahashi I, Takeuchi H and Hirata M: Osteocalcin induces release
of glucagon-like peptide-1 and thereby stimulates insulin secretion
in mice. PLoS One. 8:e573752013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhao C, Liang J, Yang Y, Yu M and Qu X:
The impact of glucagon-like peptide-1 on bone metabolism and its
possible mechanisms. Front Endocrinol (Lausanne). 8:982017.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ducy P, Desbois C, Boyce B, Pinero G,
Story B, Dunstan C, Smith E, Bonadio J, Goldstein S, Gundberg C, et
al: Increased bone formation in osteocalcin-deficient mice. Nature.
382:448–452. 1996. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li Y and Li K: Osteocalcin induces growth
hormone/insulin-like growth factor-1 system by promoting
testosterone synthesis in male mice. Horm Metab Res. 46:768–773.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Khrimian L, Obri A and Karsenty G:
Modulation of cognition and anxiety-like behavior by bone
remodeling. Mol Metab. 6:1610–1615. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Khrimian L, Obri A, Ramos-Brossier M,
Rousseaud A, Moriceau S, Nicot AS, Mera P, Kosmidis S, Karnavas T,
Saudou F, et al: Gpr158 mediates osteocalcin's regulation of
cognition. J Exp Med. 214:2859–2873. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Obri A, Khrimian L, Karsenty G and Oury F:
Osteocalcin in the brain: From embryonic development to age-related
decline in cognition. Nat Rev Endocrinol. 14:174–182. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Di Nisio A, Rocca MS, Fadini GP, De Toni
L, Marcuzzo G, Marescotti MC, Sanna M, Plebani M, Vettor R, Avogaro
A and Foresta C: The rs2274911 polymorphism in GPRC6A gene is
associated with insulin resistance in normal weight and obese
subjects. Clin Endocrinol (Oxf). 86:185–191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pietschmann P and Schernthaner G: The
effect of pirenzepine on growth hormone and blood glucose levels in
type I diabetes mellitus. A controlled study in patients on basal
bolus insulin treatment. Acta Endocrinol (Copenh). 117:315–319.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rosato MT, Schneider SH and Shapses SA:
Bone turnover and insulin-like growth factor I levels increase
after improved glycemic control in noninsulin-dependent diabetes
mellitus. Calcif Tissue Int. 63:107–111. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Akin O, Göl K, Aktürk M and Erkaya S:
Evaluation of bone turnover in postmenopausal patients with type 2
diabetes mellitus using biochemical markers and bone mineral
density measurements. Gynecol Endocrinol. 17:19–29. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Achemlal L, Tellal S, Rkiouak F, Nouijai
A, Bezza A, Derouiche el M, Ghafir D and El Maghraoui A: Bone
metabolism in male patients with type 2 diabetes. Clin Rheumatol.
24:493–496. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sanchez-Enriquez S, Ballesteros-Gonzalez
IT, Villafán-Bernal JR, Pascoe-Gonzalez S, Rivera-Leon EA,
Bastidas-Ramirez BE, Rivas-Carrillo JD, Alcala-Zermeno JL,
Armendariz-Borunda J, Llamas-Covarrubias IM and Zepeda-Moreno A:
Serum levels of undercarboxylated osteocalcin are related to
cardiovascular risk factors in patients with type 2 diabetes
mellitus and healthy subjects. World J Diabetes. 8:11–17. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Díaz-López A, Bulló M, Juanola-Falgarona
M, Martínez-González MA, Estruch R, Covas MI, Arós F and
Salas-Salvadó J: Reduced serum concentrations of carboxylated and
undercarboxylated osteocalcin are associated with risk of
developing type 2 diabetes mellitus in a high cardiovascular risk
population: A nested case-control study. J Clin Endocrinol Metab.
98:4524–4531. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Razny U, Fedak D, Kiec-Wilk B, Goralska J,
Gruca A, Zdzienicka A, Kiec-Klimczak M, Solnica B,
Hubalewska-Dydejczyk A and Malczewska-Malec M: Carboxylated and
undercarboxylated osteocalcin in metabolic complications of human
obesity and prediabetes. Diabetes Metab Res Rev. 33:2017.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Liu C, Wo J, Zhao Q, Wang Y, Wang B and
Zhao W: Association between serum total osteocalcin level and type
2 diabetes mellitus: A systematic review and meta-analysis. Horm
Metab Res. 47:813–819. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kunutsor SK, Apekey TA and Laukkanen JA:
Association of serum total osteocalcin with type 2 diabetes and
intermediate metabolic phenotypes: Systematic review and
meta-analysis of observational evidence. Eur J Epidemiol.
30:599–614. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Luo Y, Ma X, Hao Y, Xiong Q, Xu Y, Pan X,
Bao Y and Jia W: Relationship between serum osteocalcin level and
carotid intima-media thickness in a metabolically healthy Chinese
population. Cardiovasc Diabetol. 14:822015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Sheng L, Cao W, Cha B, Chen Z, Wang F and
Liu J: Serum osteocalcin level and its association with carotid
atherosclerosis in patients with type 2 diabetes. Cardiovasc
Diabetol. 12:222013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pirilä S, Taskinen M, Turanlahti M,
Kajosaari M, Mäkitie O, Saarinen-Pihkala UM and Viljakainen H: Bone
health and risk factors of cardiovascular disease-a cross-sectional
study in healthy young adults. PLoS One. 9:e1080402014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Maser RE, Lenhard MJ, Sneider MB and
Pohlig RT: Osteoprotegerin is a better serum biomarker of coronary
artery calcification than osteocalcin in type 2 diabetes. Endocr
Pract. 21:14–22. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Giudici KV PhD, Fisberg RM, Marchioni DML,
Peters BSE and Martini LA: Crosstalk between bone and fat tissue:
Associations between vitamin D, osteocalcin, adipokines, and
markers of glucose metabolism among adolescents. J Am Coll Nutr.
36:273–280. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Tan A, Gao Y, Yang X, Zhang H, Qin X, Mo
L, Peng T, Xia N and Mo Z: Low serum osteocalcin level is a
potential marker for metabolic syndrome: Results from a Chinese
male population survey. Metabolism. 60:1186–1192. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wang JW, Tang QY, Ruan HJ and Cai W:
Relation between serum osteocalcin levels and body composition in
obese children. J Pediatr Gastroenterol Nutr. 58:729–732.
2014.PubMed/NCBI
|
|
50
|
Alfadda AA, Masood A, Shaik SA, Dekhil H
and Goran M: Association between osteocalcin, metabolic syndrome,
and cardiovascular risk factors: Role of total and
undercarboxylated osteocalcin in patients with type 2 diabetes. Int
J Endocrinol. 2013:1975192013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Magni P, Macchi C, Sirtori CR and Corsi
Romanelli MM: Osteocalcin as a potential risk biomarker for
cardiovascular and metabolic diseases. Clin Chem Lab Med.
54:1579–1587. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ma H, Lin H, Hu Y, Li X, He W, Jin X, Gao
J, Zhao N and Gao X: Serum levels of osteocalcin in relation to
glucose metabolism and carotid atherosclerosis in Chinese
middle-aged and elderly male adults: The Shanghai Changfeng Study.
Eur J Intern Med. 25:259–264. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Yang R, Ma X, Dou J, Wang F, Luo Y, Li D,
Zhu J, Bao Y and Jia W: Relationship between serum osteocalcin
levels and carotid intima-media thickness in Chinese postmenopausal
women. Menopause. 20:1194–1199. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Reyes G, arcía R, Rozas Moreno P and
Muñoz-Torres M: Osteocalcin and atherosclerosis: A complex
relationship. Diabetes Res Clin Pract. 92:405–406. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kanazawa I, Yamaguchi T, Yamamoto M,
Yamauchi M, Kurioka S, Yano S and Sugimoto T: Serum osteocalcin
level is associated with glucose metabolism and atherosclerosis
parameters in type 2 diabetes mellitus. J Clin Endocrinol Metab.
94:45–49. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Bradburn S, McPhee JS, Bagley L, Sipila S,
Stenroth L, Narici MV, Pääsuke M, Gapeyeva H, Osborne G, Sassano L,
et al: Association between osteocalcin and cognitive performance in
healthy older adults. Age Ageing. 45:844–849. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Amin S, El Amrousy D, Elrifaey S, Gamal R
and Hodeib H: Serum osteocalcin levels in children with
nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr.
66:117–121. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Abd-Allah Ebrahim HT and El-Behery EG:
Osteocalcin: A new biomarker for non alcoholic fatty liver disease
(NAFLD) in children and adolescents. Clin Med Biochem.
3:1332017.
|
|
59
|
Zhang Q, Riddle RC and Clemens TL: Bone
and the regulation of global energy balance. J Intern Med.
277:681–689. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Iki M, Tamaki J, Fujita Y, et al: Serum
undercarboxylated osteocalcin levels are inversely associated with
glycemic status and insulin resistance in an elderly Japanese male
population: Fujiwara-kyo Osteoporosis Risk in Men (FORMEN) Study.
Osteoporos Int. 23:761–770. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Villafán-Bernal JR, Llamas-Covarrubias MA,
Muñoz-Valle JF, et al: A cut-point value of uncarboxylated to
carboxylated index is associated with glycemic status markers in
type 2 diabetes. J Investig Med. 62:33–36. 2014. View Article : Google Scholar : PubMed/NCBI
|