Introduction
Complication of coronary heart disease (CAD) is a
type of coronary artery atherosclerosis disease caused by
myocardial ischemia (1,2). CAD is also associated with
inflammation and thrombosis, which leads to luminal stenosis or
occlusion (3). Myocardial
infarction is one type of CAD, caused by obstruction of the
coronary artery lumen, which is induced by rupture of coronary
artery atheromatous plaque and formation of thrombus (4,5).
Morbidity and the mortality rate of myocardial infarction are
increasing worldwide (2,6). A review of the current clinical
evidence suggests that cardiovascular interventions can help
myocardial infarction patients and reduce the high mortality rate
(7). The body protects the heart
against myocardial ischemia and reperfusion injury by modulating
myocardial apoptosis and levels of inflammation (8,9).
Previous studies have also demonstrated that early apoptotic
myocardial vascular aggravates the progression of myocardial
infarction (10,11).
Statins are hydroxymethyl glutaric acyl coenzyme A
(HMG CoA) reductase inhibitors that can competitively inhibit the
endogenous HMG CoA and block cell hydroxy valeric acid metabolic
pathways, which further reduce cholesterol synthesis in the cell
(12). A previous study found that
statins cause secondary prevention in elderly patients following
acute myocardial infarction (13).
Chronic pre-treatment of statins is associated with the reduction
of the no-reflow phenomenon in the patients with reperfused acute
myocardial infarction (14).
Statins demonstrate an early antiplatelet effect in patients with
acute myocardial infarction, which results in a reduction in
collagen-induced platelet aggregation (15). The effect of statins on long-term
survival in patients hospitalized with acute myocardial infarction
was investigated in 1,706 heart failure patients (16). These studies suggested that statins
may be beneficial for the treatment of myocardial infarction.
Statins protect against arrhythmogenic calcium
alternans in the post-myocardial infarction diabetic heart
(17). Statins induce sirtuin 1
protein and have a cardioprotective role following premature
myocardial infarction by impairment of endothelial nitric oxide
synthase expression (18). In
addition, rosuvastatin treatment was found to improve the efficacy
of stem cell transplantation in infarcted hearts by activation of
the Janus kinase (JAK) 2-signal transducer and activator of
transcription (STAT)3 signaling pathway (19). Simvastatin treatment was found to
ameliorate apoptosis of cardiomyocytes by reducing the expression
of Bax and non-cleaved caspase-3 and increasing STAT3 (20). In addition, atorvastatin was found
to confer anti-inflammatory and anti-apoptotic effects under acute
myocardial infarction settings which is hypothesized to ultimately
contribute to cardiac function improvement (21). Therefore, concerns have been raised
concerning statins due to their potential adverse impacts on
myocardial infarction.
A previous study showed that CoCl2
induces hypoxic injury and mimics the hypoxia condition-induced
injury in cardiomyocytes (22). In
addition, apoptosis of coronary artery endothelial cells is a
pro-atherogenic adhesion molecule central to initiation of
atherosclerosis and progression towards plaque instability
(23). Thus, the present study
analyzed the anti-apoptotic effect of the statin rosuvastatin on
human coronary artery endothelial cells (HCAECs). The present study
used CoCl2 to mimic hypoxia condition-induced
cardiomyocyte injury. The therapeutic effects of the statin
rosuvastatin in myocardial infarction were examined and it was
found that statin treatment significantly inhibited apoptosis of
the HCAECs induced by CoCl2. It was also noted that
rosuvastatin can protect the myocardium against myocardial
infarction by regulation of the JAK2/STAT3 pathway.
Materials and methods
HCAEC culture
HCAECs were obtained from PromoCell GmbH and
cultured in MEM medium (Sigma-Aldrich; Merck KGaA) containing 10%
fetal bovine serum (Sigma-Aldrich; Merck KGaA). CoCl2
(20 mM, Sigma-Aldrich; Merck KGaA) was used to induce hypoxic
stimulation. The cells were grown in a humidified atmosphere
containing 5% CO2 at 37°C. HCAECs were treated with the
statin rosuvastatin (0, 1, 2 and 3 mg/ml, Sigma-Aldrich; Merck
KGaA) and/or JAK2 inhibitor AG490 (2 mg/ml, Sigma-Aldrich; Merck
KGaA) for further analysis.
Reverse transcription-quantitative
(RT-q) PCR
Total RNA was extracted from human coronary artery
endothelial cells (1×107) using RNAeasy Mini kit (Qiagen
Sciences, Inc.). RNA was purified using the PureLink™ Pro 96 total
RNA Purification Kit (Thermo Fisher Scientific, Inc.) and
quantified using a Nanodrop 2000c UV–Vis Spectrophotometer (Thermo
Fisher Scientific, Inc.) according to the manufacturer's
instructions. Expression levels of Bcl-xl, Bcl-2, Bax and Bad in
HCAEC were measured by RT-qPCR with β-actin as an endogenous
control (24) (Invitrogen, Thermo
Fisher Scientific, Inc.). The following thermocycling conditions
were used for qPCR: Initial denaturation at 95°C for 300 sec; 45
cycles of 95°C for 30 sec, 57°C for 30 sec and 72°C for 30 sec. All
the forward and reverse primers were synthesized by Invitrogen
(Thermo Fisher Scientific, Inc.) (Table I). Relative mRNA expression changes
were calculated by the 2−ΔΔCq method (25). The results are expressed as n-fold
change compared with β-actin.
 | Table I.Primers for reverse
transcription-quantitative PCR. |
Table I.
Primers for reverse
transcription-quantitative PCR.
|
| Sequence |
|---|
|
|
|
|---|
| Gene name | Reverse | Forward |
|---|
| Bax |
5′-CTTCTCACTGTCGACTACCGC-3′ |
5′-GCGTCTCCTGTGCATTCG-3′ |
| Bad |
5′-GCAAGGACAAGATTCGATACT-3′ |
5′-GCCAGACTACATGGAAATCTA-3′ |
| Bcl-2 |
5′-CATGCTGGGGCCGTACAG-3′ |
5′-TTGTCCGACCTTTGGCAACT-3′ |
| Bcl-xl |
5′-ATTTGCGTGTGGAGTATTTGG-3′ |
5′-GCTGTTCCGTCCCAGTAGATTA-3′ |
|
Caspase-3 |
5′-AGCAATAAATGAATGGGCTGAG-3′ |
5′-GTATGGAGAAATGGGCTGTAGG-3′ |
|
Caspase-9 |
5′-CATTTCATGGTGGAGGTGAAG-3′ |
5′-GGGAACTGCAGGTGGCTG-3′ |
| β-actin |
5′-CGGAGTCAACGGATTTGGTC-3′ |
5′-AGCCTTCTCCATGGTCGTGA-3′ |
Cell viability assay
Viability of endothelial cells was analyzed using
the Cell Counting Kit-8 (CCK-8; Sigma-Aldrich; Merck KGaA).
Briefly, HCAEC at 1×105 cells/ml density were seeded
into 6-well plates, 0.2% H2O2 was added with
or without rosuvastatin (0, 1.0, 2.0 and 3.0 mg/ml) and then
cultured for 24, 48 and 72 h at 37°C. A total of 10 µl CCK-8
solution was added to the cells and then the cells were cultured
for 30 min at 37°C. Cell viability was measured at 450 nm
absorbance using a Microplate Reader (Bio-Rad Laboratories,
Inc.).
Western blot analysis
HCAEC were homogenized in lysate buffer containing
protease-inhibitor and were centrifuged at 6,000 × g at 4°C for 10
min. The supernatant was used for analysis of the purpose protein.
Total protein was quantified using a bicinchoninic acid assay kit
(Thermo Fisher Scientific, Inc.). A total of 40 µg protein/lane was
separated via 15% SDS-PAGE and transferred onto nitrocellulose
membranes, which were blocked with 5% BSA (Sigma-Aldrich; Merck
KGaA) at 4°C overnight. The primary antibodies used in the
immunoblotting assays were: Bad (1:1,200, cat. no. ab32445, Abcam),
Bax (1:1,200, cat. no. ab32503, Abcam), matrix metalloproteinase
(MMP) 9 (1:1,200, cat. no. ab388981, Abcam), tumor necrosis factor
(TNF) α (1:1,200, cat. no. ab6671, Abcam), NF-κB (1:1,200, cat. no.
ab220803, Abcam), interleukin (IL) 1β (1:1,200, cat. no. ab9722,
Abcam), IL-10 (1:1,200, cat. no. ab9969, Abcam), peroxisome
proliferator-activated receptor γ coactivator (PGC) 1α (1:1,200,
cat. no. ab54481, Abcam), brain natriuretic peptide (BNP; 1:1,200,
cat. no. ab19645, Abcam), α myosin heavy chain (MHC; 1:1,200, cat.
no. ab134189, Abcam), Bcl-xl (1:1,200, cat. no. ab32370, Abcam),
Bcl-2 (1:1,200, cat. no. ab32124, Abcam), JAK2 (1:1,200, cat. no.
ab108596, Abcam), phosphorylated (p-)JAK2 (1:1,200, cat. no.
ab32101, Abcam), STAT3 (1:1,200, cat. no. ab68153, Abcam), p-STAT3
(1:1,200, cat. no. ab126459, Abcam) and β-actin (1:2,000, cat. no.
ab8226, Abcam) for 12 h at 4°C. The blots were then incubated with
HRP-conjugated secondary antibody (1:5,000, cat. no. ab205718,
Abcam) for 2 h at 37°C The bands of proteins were observed with an
enhanced chemiluminescence substrate kit (cat. no. P0018F, Beyotime
Institute of Biotechnology). Quantitative expression of proteins
was quantified by ImageJ software (v4.6.2, National Institutes of
Health).
TUNEL assay
To analyze the apoptosis of HCAECs in experimental
rats following statin treatment (10 mg/kg/day, Sigma-Aldrich; Merck
KGaA) or the same dose of PBS, a TUNEL assay (Biotool Service GmbH)
was used to detect TUNEL-positive cells. The procedures were
performed as in a previous study (26). Finally, hippocampal neuron cell
images were captured with a ZEISS LSM 510 confocal microscope at
488 nm.
Animals studies
Male SD rats (6-8-week, body weight, 200–220 g,
n=40) were purchased from the Chinese Academy of Sciences Institute
of Biophysics. All rats were housed at 23–25°C with 50–60%
humidity, 12-h light/dark cycles, and food and water ad
libitum. Animal breeding and experiments were carried out under
IACUC approved protocols at Provincial Hospital Affiliated to
Shandong University. A myocardial infarction rat model was
established by ligating the left anterior descending (LAD) coronary
artery for 30 min followed by reperfusion for 4 h (27). Briefly, rats were anesthetized
using pentobarbitone sodium (50 mg/kg). After disinfecting the
surgical area, the left chest was opened to expose the heart. Rats
were subjected to permanent LAD ligation using 6.0 prolene,
approximately 2 mm in width and depth, in order to induce
myocardial ischemia. Successful occlusion of the LAD was confirmed
by observing the appearance of a paler color below the ligation
area and ST-segment elevation on ECG (PowerLab System, AD
Instruments Ltd.) were used to confirm a successful occlusion of
the LAD coronary artery. Myocardial infarction rats were divided
into two groups (n=20 in each group) and received rosuvastatin (1
mg/kg, Sigma-Aldrich; Merck KGaA) or the same PBS dose in a total
of 60-day treatment once a day. At the end of experimental period,
rats were euthanized by cervical dislocation under pentobarbital
(50 mg/kg i.p.) anesthesia.
Blood biochemical parameters
Blood samples (0.5 ml) in vena caudalis were
collected from experimental rats at the end of experiments and
immediately transferred to the Central Laboratory. Serum was
obtained using centrifugation (12,000 × g, 10 min, 4°C) and used to
determine concentrations of serum low-density lipoprotein
cholesterol (LDL-c), hypersensitive C-reactive protein (hsCRP;
reference value: 0–5 mg/l), leucocytes (WBC), neutrophil counts (%)
and mean platelet volume (MPV). Left ventricular ejection fraction
(LVEF) and left ventricular fractional shortening (LVFS) were
measured as described previously (28).
Measurement of the myocardial infarct
size
At the end of treatment, the hearts from the two
groups were immediately placed in a −80°C freezer for 10 min and
cut into 2–3 mm thick slices along the sagittal plane of the heart.
Myocardial tissues were stained in 2,3,5-triphenyl-2H-tetrazolium
chloride (TTC) solution (37°C, 1% TTC, pH 7.4) for 30 min.
Subsequently, myocardial tissues were incubated with 10%
formaldehyde solution for fixation for 24 h at 4°C. The infarct
area in the myocardial tissues was analyzed with ImageJ (v4.6.2,
National Institutes of Health) and images were captured with a
digital camera.
Determination of mitochondrial
reactive oxygen species (ROS) generation
Mitochondrial ROS production rate was detected using
fluorometric methods (29). In
brief, 2.9 ml of mitochondrial ROS assay medium and 3 ml of 5
mmol/l 2′,7′-dichlorofluorescin diacetate were incubated at 37°C
for 15 min and the fluorescence intensity of the reaction system
with mitochondria was measured using the fluorescence intensity of
the reaction system without mitochondria. The ROS generation rate
was calculated by subtracting the basal fluorescence intensity from
the sample florescence intensity.
Immunological staining
The effects of rosuvastatin treatment on neuronal
loss were evaluated using immunohistochemical staining of
myocardial tissue from experimental rats. Staining was performed on
myocardial tissues in animals following treatment by statin or PBS
only. Immunohistochemical procedures were previously reported in
detail (30). Free-floating
sections were rinsed and placed in the solution with the rabbit
anti-rat primary antibody of Bad (1:1,200, cat. no. ab32445,
Abcam), Bax (1:1,200, cat. no. ab32503, Abcam), JAK2 (1:1,200, cat.
no. ab108596, Abcam) and STAT3 (1:1,200, cat. no. ab68153, Abcam).
After rinsing, sections were incubated in the presence of
horseradish peroxidase-conjugated anti-rabbit IgG antibodies
(1:5,000; cat. no. ab6721; Abcam) for 24 h at 4°C. The results were
visualized by using a chemiluminescence detection system
(Cytiva).
Statistical analysis
All data are expressed as mean ± standard deviation
of triplicate dependent experiments and analyzed by using Student's
t-tests or one-way ANOVA followed by Tukey's HSD test. All data
were analyzed using SPSS Statistics 19.0 (IBM Corp.) and GraphPad
Prism version 5.0 (GraphPad Software, Inc.) with Microsoft Excel
(version 2010; Microsoft Corporation). P<0.05 was considered to
indicate a statistically significant difference.
Results
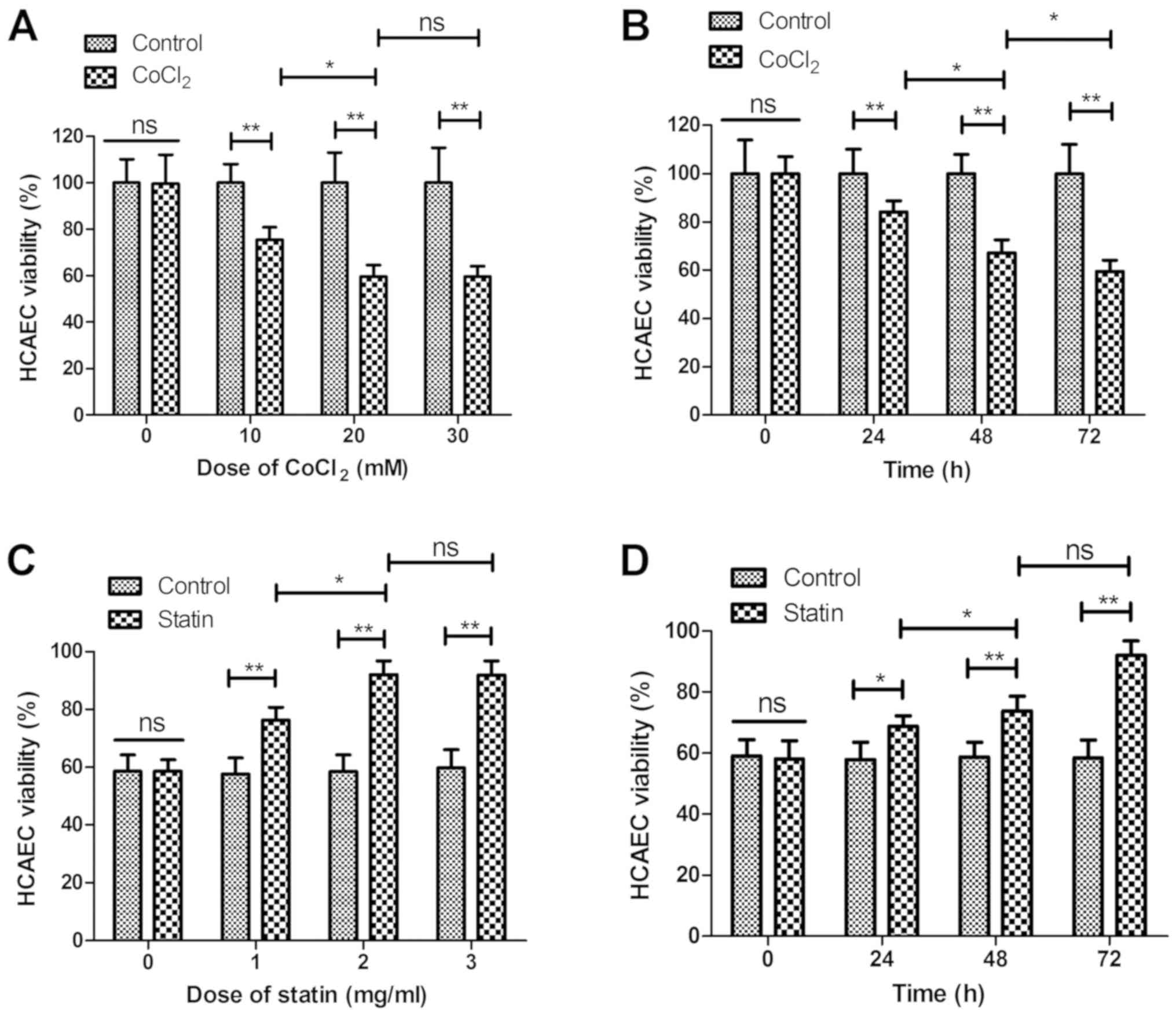
Statin rosuvastatin increases survival
of HCAECs treated by CoCl2
The effect of rosuvastatin on the survival of HCAEC
apoptosis induced by CoCl2 was analyzed in the present
study. As shown in Fig. 1A and B,
CoCl2 decreased the viability of the sHCAEC in a dose-
and time-dependent manner. Viability of the HCAECs was increased in
the statin-treated (CoCl2 + statin) group compared with
CoCl2-treated group (Fig.
1C). Data demonstrated that 2 mg/ml of statin presented the
optimal efficacy in increasing the viability of the HCAECs. As
depicted in Fig. 1D, 2 mg/ml of
statin increased viability of the HCAECs in a time-dependent
manner. These results indicate that statin is beneficial for
myocardial infarction by reversing the CoCl2-reduced
viability of HCAECs.
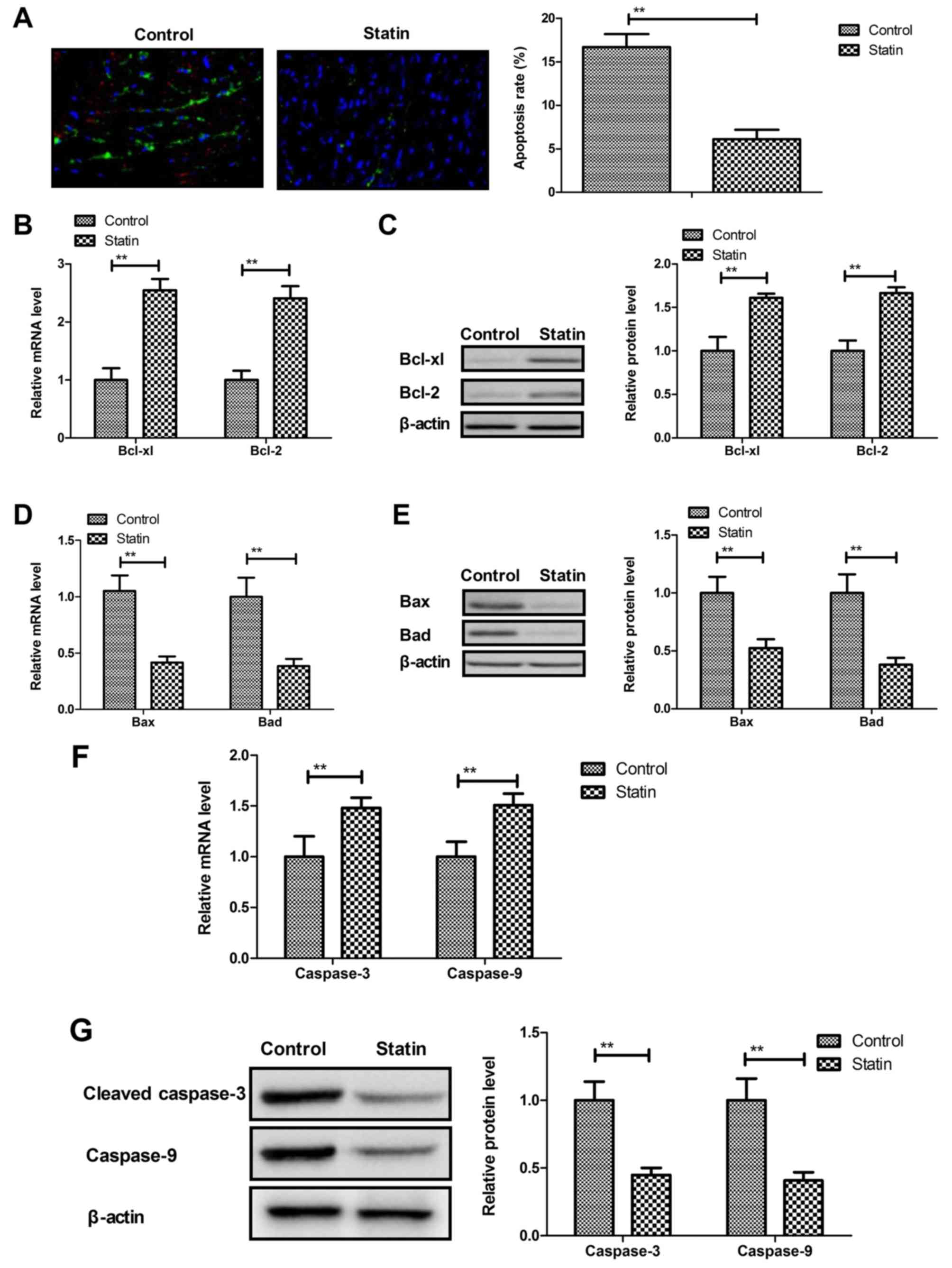
Statin rosuvastatin inhibits apoptosis
of HCAECs induced by CoCl2
Apoptosis of HCAECs plays an important role in the
progression of myocardial infarction. The present study showed that
rosuvastatin inhibited apoptosis of HCAECs induced by
CoCl2 (Fig. 2A).
Results demonstrated that rosuvastatin treatment increased
anti-apoptosis Bcl-xl and Bcl-2 protein and mRNA expression
(Fig. 2B and C), while
pro-apoptosis Bax and Bad mRNA and protein expression was decreased
by statin treatment (Fig. 2D and
E). Statin treatment also decreased the apoptotic markers
caspase-3 and caspase-9 mRNA and protein in HCAECs compared with
the control (Fig. 2F and G). These
results indicated that statin treatment inhibits the apoptosis of
HCAECs induced by CoCl2.
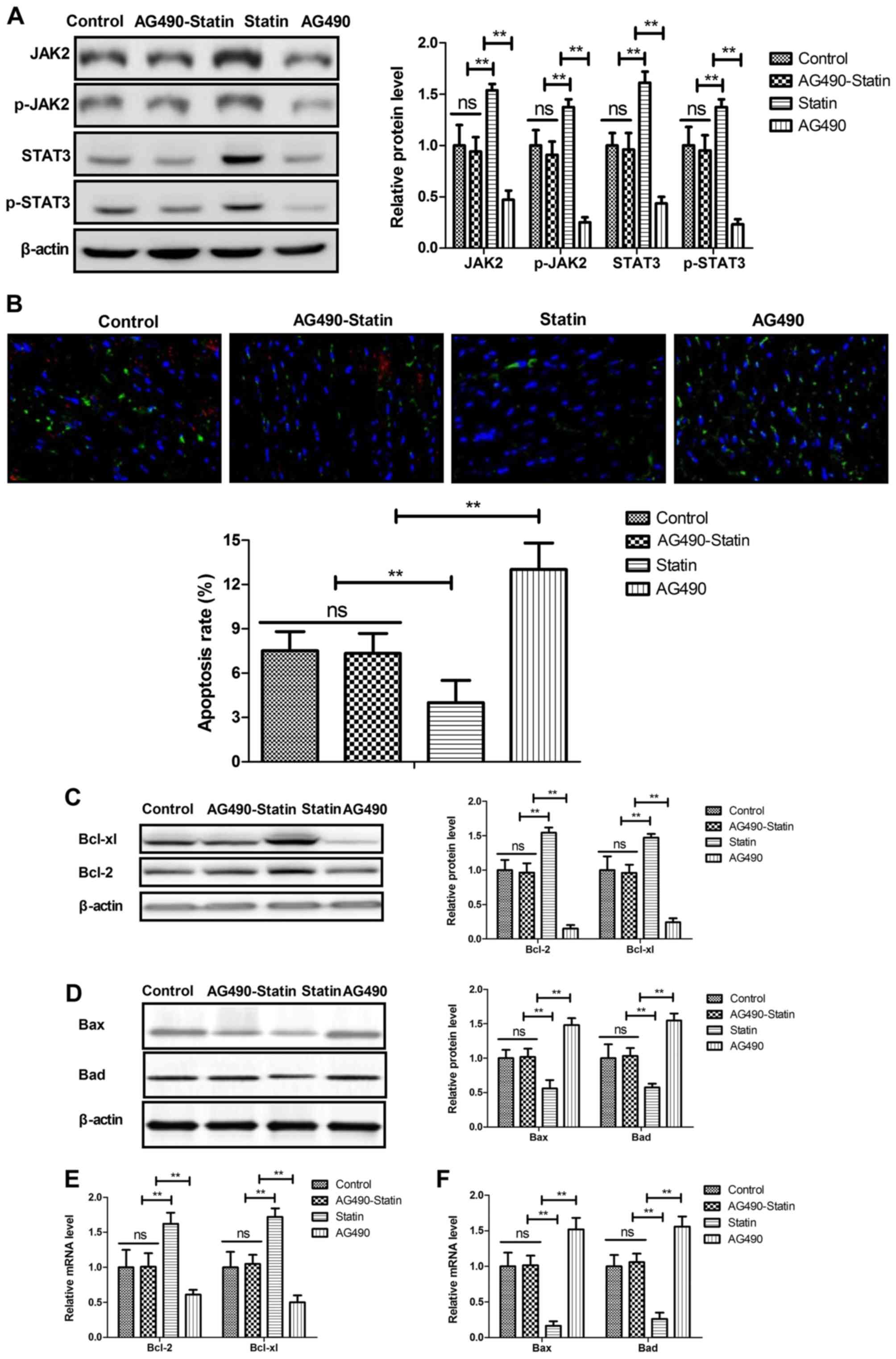
Statin rosuvastatin suppresses
apoptosis of HCAECs through regulation of the JAK2/STAT3
pathway
The potential mechanism mediated by rosuvastatin was
investigated in HCAECs induced by CoCl2. Statin
treatment significantly increased JAK2, p-JAK2, STAT3 and p-STAT3
expression in the HCAECs (Fig.
3A). Results showed that the JAK2 selective inhibitor AG490
decreased and abolished statin-promoted JAK2 and STAT3 expression
in the HCAECs. In addition, statin-inhibited apoptosis of HCAECs
was abolished by JAK2 inhibitor AG490 (Fig. 3B). Apoptosis-regulated protein
expression levels were also reversed by JAK2 inhibitor AG490 in
statin-regulated HCAECs (Fig. 3C and
D). Results also showed that JAK2 inhibitor AG490 abolished
statin-regulated Bcl-2, Bcl-xl, Bad and Bax levels in the HCAECs
induced by CoCl2 (Fig.
3E). These results indicate that statin can significantly
suppress apoptosis of HCAECs through regulation of the JAK2/STAT3
pathway.
Impact of statin treatment on
inflammatory markers and cellular parameters in myocardial
infarction rats
The effects of rosuvastatin treatment on
inflammatory markers and cellular parameters were further analyzed
in myocardial infarction rats. Results showed that statin treatment
reduced hsCRP, white blood cell (WBC) and LDL-c levels, but
increased neutrophils, MPV, LVEF and LVFS compared with the control
(Fig. 4A-E). These results
indicated that statin could decrease inflammatory markers in
myocardial infarction rats.
 | Figure 4.Effects of statin rosuvastatin on
inflammatory markers and cellular parameters in a myocardial
infarction rat model. Effects of statin on (A) blood hsCRP
concentration, (B) number of WBCs, (C) LDL-c, (D) neutrophils, (E)
MPV, (F) LVEF and (G) LVFS in myocardial infarction rat model.
*P<0.05, **P<0.01. hsCRP, hypersensitive C-reactive protein;
WBC, leucocytes; LDL-c, low-density lipoprotein cholesterol; MPV,
mean platelet volume; LVEF, left ventricular ejection fraction;
LVFS, left ventricular fractional shortening. |
Expression of inflammatory,
mitochondrial damaged and cardiac hypertrophic failure in
myocardial infarction rats
As shown in Fig.
5A, protein levels of MMP-9, TNF-α, NF-κB and IL-1β were
decreased by rosuvastatin compared with the control.
Anti-inflammatory cytokine IL-10 was increased by treatment with
rosuvastatin (Fig. 5B). An
indicator of mitochondrial damage and mitochondrial integrity,
cytosolic cytochrome c, was decreased by statin (Fig. 5C). A major upstream regulator of
lipid catabolism PGC-1α, indicator of heart failure BNP and α-MHC
were increased by statin in the myocardial infarction rats
(Fig. 5D). These data indicated
that statin treatment presented benefits in improvement of
inflammation, mitochondrial damage and cardiac hypertrophic
failure.
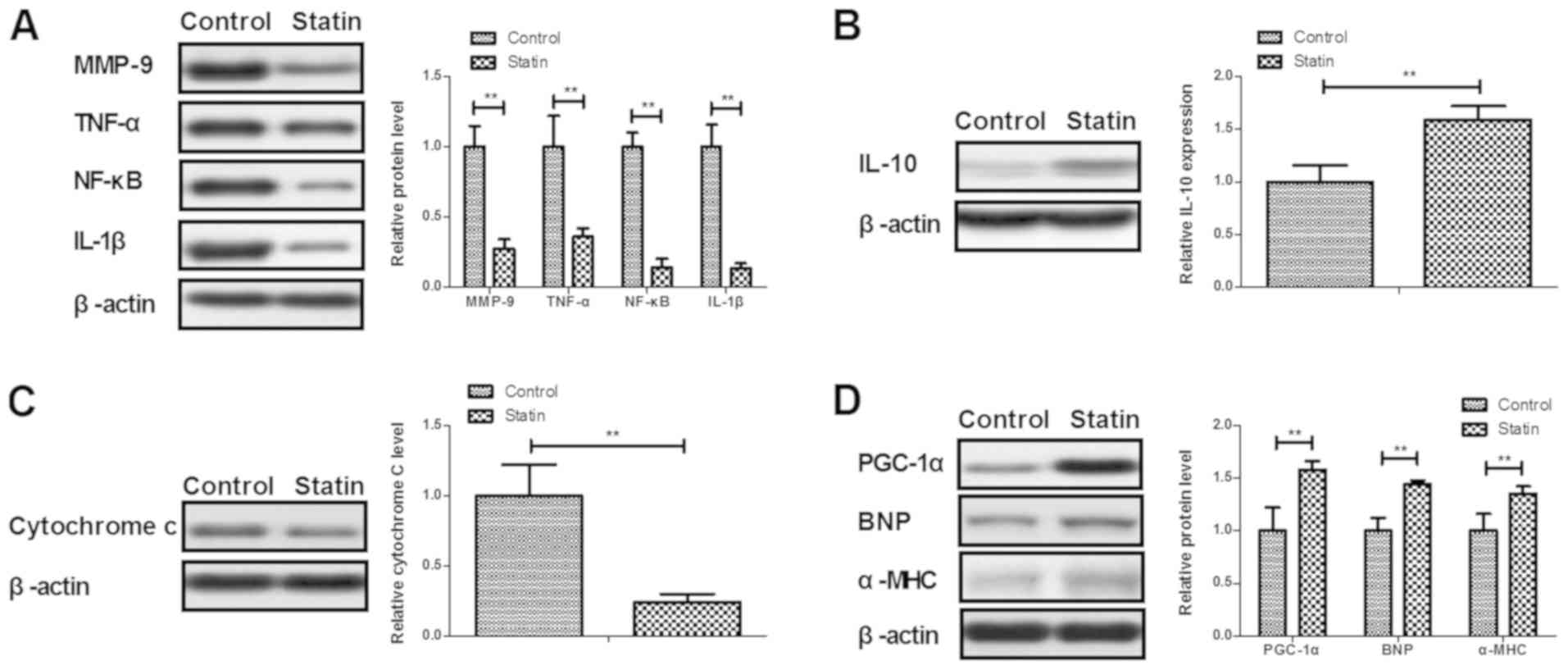 | Figure 5.Expression levels of inflammatory
factors, mitochondrial damage and cardiac hypertrophic failure in a
myocardial infarction rat model. (A) Effects of statin rosuvastatin
on the protein levels of MMP-9, TNF-α, NF-κB and IL-1β in heart
tissue. (B) Effects of statin on anti-inflammatory cytokine IL-10
in heart tissue. (C) Effects of statin on cytosolic Cytochrome c
expression in heart tissue. (D) Effects of statin on PGC-1α, BNP
and α-MHC expression in heart tissue. **P<0.01. MMP, matrix
metalloproteinase; TNF, tumor necrosis factor; NF-κΒ, nuclear
factor κΒ; IL, interleukin; PGC, peroxisome proliferator-activated
receptor γ coactivator; BNP, brain natriuretic peptide; α-MHC, α
myosin heavy chain. |
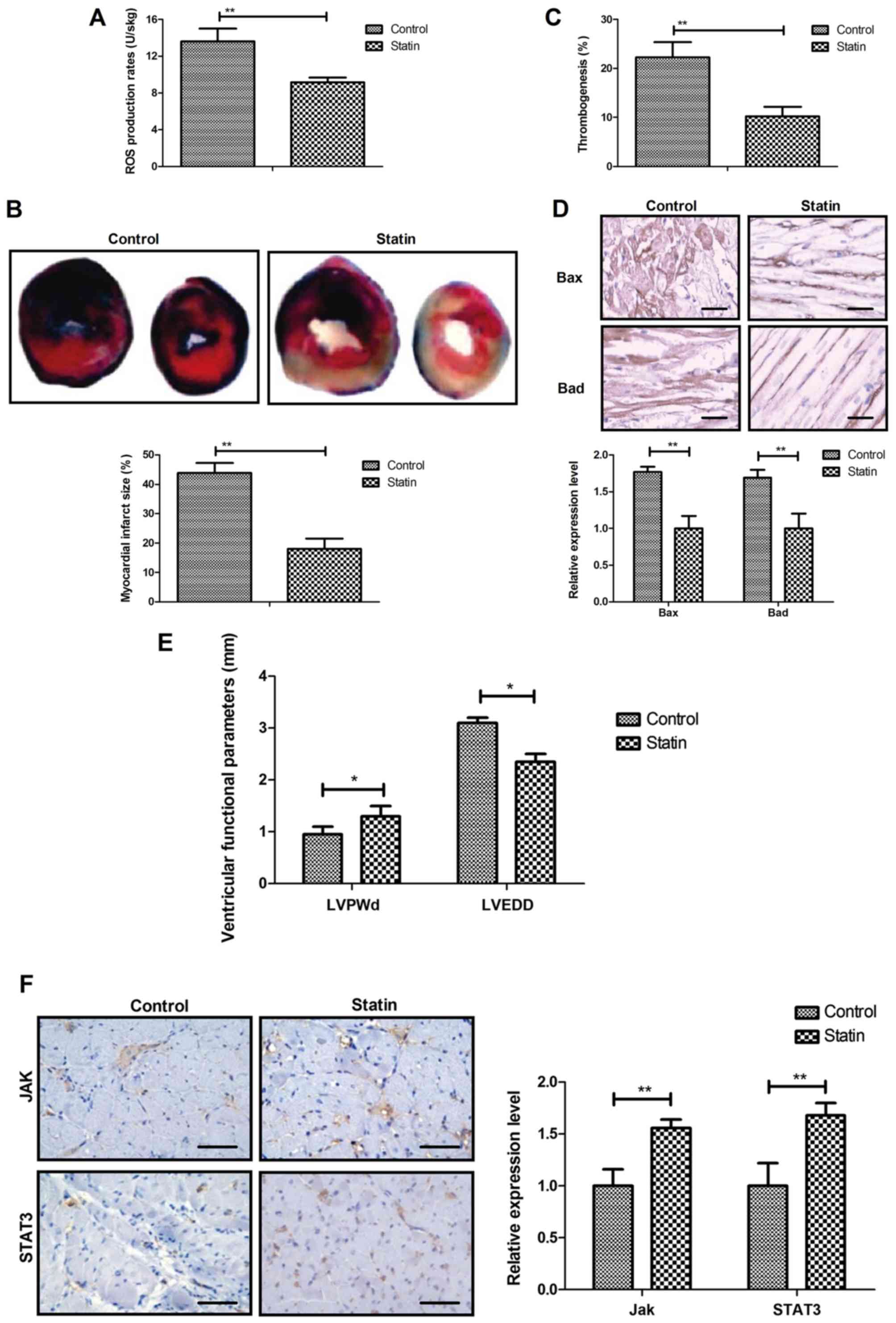
In vivo efficacy of statin for
myocardial infarction
In vivo efficacy of the statin rosuvastatin
was investigated in a myocardial infarction rat model. It was
observed that statin treatment markedly decreased the mitochondrial
ROS and the myocardial infarction areas (Fig. 6A and B). Results also indicated
that rosuvastatin treatment significantly decreased thrombogenesis
in the experiment rats after the 60-day treatment (Fig. 6C). The results revealed that Bax
and Bad production was also decreased by statin treatment compared
with the control (Fig. 6D).
Treatment with the statin significantly improved the cardiac
function indicators left ventricular end-diastolic posterior wall
thickness and left ventricular end-diastolic diameter (Fig. 6E) and significantly increased
expression levels of JAK and STAT3 in myocardial tissue (Fig. 6F). These results indicate that
statin treatment was beneficial for the treatment of myocardial
infarction.
Discussion
Prospective review and randomized clinical trials
have investigated factors associated with increased coronary heart
disease risk (31). Expression of
apoptosis factors following coronary heart disease are increased in
patients in the clinic (32). Data
in a systematic review and meta-analysis indicate the therapeutic
effects of perioperative statins on death, myocardial infarction,
atrial fibrillation and length of stay (33). The present study first investigated
the beneficial effects of statin rosuvastatin for coronary artery
endothelial cells induced by CoCl2 both in vitro
and in vivo. Statin treatment decreased serum level of
hsCRP, WBCs, LDL-c, but increased serum level of neutrophils, MPV,
LVEF and LVFS compared with control treatment in a myocardial
infarction rat model. Statin significantly improved viability of
HCAECs induced by CoCl2 and improved inflammation,
mitochondrial damage and cardiac hypertrophic failure. Statin
suppressed apoptosis of HCAECs by increasing JAK2/STAT3 signaling
pathway-related proteins.
A previous study evaluated the kinetics of
cardiomyocyte apoptosis in patients undergoing primary percutaneous
coronary intervention and thrombolytic therapy (34). Statin administration was found to
mitigate cellular inflammatory response following ST-elevation
myocardial infarction in a total of 404 patients (35). The present study reported that
statin treatment presented anti-apoptotic effects on HCAECs induced
by CoCl2. In addition, Bax deficiency was previously
found to reduce infarct size and improve long-term function
following myocardial infarction (36). Activation of the Bad apoptotic
pathway and the PI3K/Akt survival pathway has been observed
following myocardial infarction (37). The present study showed that
rosuvastatin administration significantly decreased Bax and Bad
expression levels in HCAECs. Furthermore, Bcl-2 upregulation
contributed to anti-apoptosis of cardiomyocytes in rats with
myocardial infarction injury (38). Effects of statin on the
anti-apoptosis of HCAECs and the increasing expression of Bcl-2
were identified in rats with myocardial infarction injury.
A previous study indicated that the role of JAK2
plays an important role in premature myocardial infarction, in
support of the revised World Health Organization diagnostic
criteria for essential thrombocythemia (39). The cardiac-specific ablation of the
STAT3 gene in the subacute phase of myocardial infarction
exacerbates cardiac remodeling (40). Notably, activation of the
JAK2/STAT3 pathway protects myocardium against ischemia/reperfusion
injury (41). The present study
reported that rosuvastatin significantly suppressed apoptosis of
HCAECs through regulation of the JAK2/STAT3 pathway. A previous
study noted that myocardial caspase-3 activation promotes
calpain-induced septic apoptosis (42). Another study indicated that
decreasing cleaved-caspase-9 expression inhibits myocardial cell
apoptosis during myocardial ischemia-reperfusion injury in rats
(43). In the present study, it
was observed that statin treatment decreased caspase-3 and
caspase-9 expression in HCAECs induced by CoCl2.
However, HCAECs should be isolated from the myocardial infarction
rat model for detection in future studies. The present study also
suggested that statin treatment contributes to improvements in
myocardial infarction via decreasing mitochondrial ROS and the
myocardial infarction areas. Statin treatment significantly
decreased thrombogenesis in the experimental rats following the
60-day treatment, decreased Bax and Bad production and increased
the expression levels of JAK and STAT3 in myocardial tissue.
The novelty of the present study was that its data
demonstrated that the statin rosuvastatin inhibited the apoptosis
of HCAECs through regulation of JAK2/STAT3. However, there were
several limitations in the present study. First, the data of cells
without CoCl2 treatment were not collected in the in
vitro experiments. Second, data in a sham group was not
investigated in in vivo experiments. Third, the present
study only analyzed the associations between statin and the
JAK2/STAT3 signaling pathway in HCAECs. Fourth, HCAECs were not
isolated from the myocardial infarction rats. Therefore, more
experiments should investigate the effect of statins on HCAECs
isolated from myocardial infarction rats in future studies. In
addition, the effect of statins on cardiac tissue cannot directly
demonstrate the anti-apoptotic effect of statins on HCAECs.
In conclusion, the present study indicated that the
cardioprotective effects of statin are associated with the
upregulation of JAK2/STAT3, which further decreased the apoptosis
of HCAECs. It was found that rosuvastatin significantly improved
mitochondrial ROS and the myocardial infarction areas in experiment
rats following the 60-day treatment. However, further studies of
the JAK2/STAT3 signaling pathway should be further investigated in
the progression of myocardial infarction.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KW and BL performed the experiments. YX, NX and ML
acquired, analyzed and interpreted the data. GG designed the study
and drafted the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of AnZhen Hospital of Beijing (Beijing, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fan FF, Xu Q, Sun Q, Zhao SJ, Wang P and
Guo XR: Assessment of the reporting quality of randomized
controlled trials on treatment of coronary heart disease with
traditional Chinese medicine from the Chinese journal of integrated
traditional and Western medicine: A systematic review. PLoS One.
9:e863602014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Doyle F, Rohde D, Rutkowska A, Morgan K,
Cousins G and McGee H: Systematic review and meta-analysis of the
impact of depression on subsequent smoking cessation in patients
with coronary heart disease: 1990 to 2013. Psychosom Med. 76:44–57.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tully PJ and Baumeister H: Collaborative
care for the treatment of comorbid depression and coronary heart
disease: A systematic review and meta-analysis protocol. Syst Rev.
3:1272014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schwingshackl L and Hoffmann G: Dietary
fatty acids in the secondary prevention of coronary heart disease:
A systematic review, meta-analysis and meta-regression. BMJ Open.
4:e0044872014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tully PJ, Cosh SM and Baumeister H: The
anxious heart in whose mind? A systematic review and
meta-regression of factors associated with anxiety disorder
diagnosis, treatment and morbidity risk in coronary heart disease.
J Psychosom Res. 77:439–448. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li SM, Xu H and Chen KJ: Integrative
medicine on coronary heart disease: Annual academic review 2013.
Zhongguo Zhong Xi Yi Jie He Za Zhi. 34:1029–1034. 2014.(In
Chinese). PubMed/NCBI
|
|
7
|
Ray IB, Menezes AR, Malur P, Hiltbold AE,
Reilly JP and Lavie CJ: Meditation and coronary heart disease: A
review of the current clinical evidence. Ochsner J. 14:696–703.
2014.PubMed/NCBI
|
|
8
|
Niermann C, Gorressen S, Klier M, Gowert
NS, Billuart P, Kelm M, Merx MW and Elvers M: Oligophrenin1
protects mice against myocardial ischemia and reperfusion injury by
modulating inflammation and myocardial apoptosis. Cell Signal.
28:967–978. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Guo CX, Jiang X, Zeng XJ, Wang HX, Li HH,
Du FH and Chen BX: Soluble receptor for advanced glycation
end-products protects against ischemia/reperfusion-induced
myocardial apoptosis via regulating the ubiquitin proteasome
system. Free Radic Biol Med. 94:17–26. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shi ZY, Liu Y, Dong L, Zhang B, Zhao M,
Liu WX, Zhang X and Yin XH: Cortistatin improves cardiac function
after acute myocardial infarction in rats by suppressing myocardial
apoptosis and endoplasmic reticulum stress. J Cardiovasc Pharmacol
Ther. 22:83–93. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nishikido T, Oyama J, Shiraki A, Komoda H
and Node K: Deletion of Apoptosis Inhibitor of Macrophage
(AIM)/CD5L attenuates the inflammatory response and infarct size in
acute myocardial infarction. J Am Heart Assoc. 5:e0028632016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kvan E, Pettersen KI, Landmark K and
Reikvam A: Treatment with statins after acute myocardial infarction
in patients >or=80 years: Underuse despite general acceptance of
drug therapy for secondary prevention. Pharmacoepidemiol Drug Saf.
15:261–267. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou Z, Rahme E, Abrahamowicz M, Tu JV,
Eisenberg MJ, Humphries K, Austin PC and Pilote L: Effectiveness of
statins for secondary prevention in elderly patients after acute
myocardial infarction: An evaluation of class effect. CMAJ.
172:1187–1194. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Iwakura K, Ito H, Kawano S, Okamura A,
Kurotobi T, Date M, Inoue K and Fujii K: Chronic pre-treatment of
statins is associated with the reduction of the no-reflow
phenomenon in the patients with reperfused acute myocardial
infarction. Eur Heart J. 27:534–539. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Matetzky S, Fefer P, Shenkman B, Shechter
M, Novikov I, Savion N, Varon D and Hod H: Statins have an early
antiplatelet effect in patients with acute myocardial infarction.
Platelets. 22:103–110. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lewinter C, Bland JM, Crouch S, Cleland
JG, Doherty P, LeWinter MM, Køber L, Hall AS and Gale CP: Impact of
aspirin and statins on long-term survival in patients hospitalized
with acute myocardial infarction complicated by heart failure: An
analysis of 1706 patients. Eur J Heart Fail. 16:95–102. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Verrier RL: Statins protect against
arrhythmogenic calcium alternans in the post-myocardial infarction
diabetic heart: Pleiotropy on steroids. Heart Rhythm. 14:1417–1418.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yamac AH and Kilic U: Effect of statins on
sirtuin 1 and endothelial nitric oxide synthase expression in young
patients with a history of premature myocardial infarction. Turk
Kardiyol Dern Ars. 46:205–215. 2018.PubMed/NCBI
|
|
19
|
Xu H, Yang YJ, Qian HY, Tang YD, Wang H
and Zhang Q: Rosuvastatin treatment activates JAK-STAT pathway and
increases efficacy of allogeneic mesenchymal stem cell
transplantation in infarcted hearts. Circ J. 75:1476–1485. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rajtik T, Carnicka S, Szobi A, Mesárošová
L, Máťuš M, Švec P, Ravingerová T and Adameová A: Pleiotropic
effects of simvastatin are associated with mitigation of apoptotic
component of cell death upon lethal myocardial reperfusion-induced
injury. Physiol Res. 61 (Suppl 2):S33–S41. 2012.PubMed/NCBI
|
|
21
|
Qiu R, Cai A, Dong Y, Zhou Y, Yu D, Huang
Y, Zheng D, Rao S, Feng Y and Mai W: SDF-1α upregulation by
atorvastatin in rats with acute myocardial infarction via nitric
oxide production confers anti-inflammatory and anti-apoptotic
effects. J Biomed Sci. 19:992012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Han L, Zhang X and Qian Y: Propofol
protects human cardiac AC16 cells from CoCl2-induced hypoxic
injury. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 44:307–314. 2019.(In
Chinese). PubMed/NCBI
|
|
23
|
Radecke CE, Warrick AE, Singh GD, Rogers
JH, Simon SI and Armstrong EJ: Coronary artery endothelial cells
and microparticles increase expression of VCAM-1 in myocardial
infarction. Thromb Haemost. 113:605–616. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xiao S, Wang J and Xiao N: MicroRNAs as
noninvasive biomarkers in bladder cancer detection: A diagnostic
meta-analysis based on qRT-PCR data. Int J Biol Markers.
31:e276–e285. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Naganuma Y, Ichii O, Otsuka S, Hashimoto Y
and Kon Y: Analysis of TdT-mediated dUTP nick end labeling
(TUNEL)-positive cells associated with cardiac myogenesis in mouse
embryo. J Vet Med Sci. 75:283–290. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhang R, Kang X, Wang Y, Wang F, Yu P,
Shen J and Fu L: Effects of carvedilol on ventricular remodeling
and the expression of β3-adrenergic receptor in a diabetic rat
model subjected myocardial infarction. Int J Cardiol. 222:178–184.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bagno LL, Carvalho D, Mesquita F, Louzada
RA, Andrade B, Kasai-Brunswick TH, Lago VM, Suhet G, Cipitelli D,
Werneck-de-Castro JP and Campos-de-Carvalho AC: Sustained IGF-1
secretion by adipose-derived stem cells improves infarcted heart
function. Cell Transplant. 25:1609–1622. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Paradiso A, Caretto S, Leone A, Bove A,
Nisi R and De Gara L: ROS production and scavenging under anoxia
and re-oxygenation in arabidopsis cells: A balance between redox
signaling and impairment. Front Plant Sci. 7:18032016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dirani M, Nasreddine W, Abdulla F and
Beydoun A: Seizure control and improvement of neurological
dysfunction in Lafora disease with perampanel. Epilepsy Behav Case
Rep. 2:164–166. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hashemian M, Poustchi H,
Mohammadi-Nasrabadi F and Hekmatdoost A: Systematic review of zinc
biochemical indicators and risk of coronary heart disease. ARYA
Atheroscler. 11:357–365. 2015.PubMed/NCBI
|
|
32
|
Liu LL, Lin LR, Lu CX, Fu JG, Chao PL, Jin
HW, Zhang ZY and Yang TC: Expression of inflammatory and apoptosis
factors following coronary stent implantation in coronary heart
disease patients. Int Immunopharmacol. 11:1850–1854. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chopra V, Wesorick DH, Sussman JB, Greene
T, Rogers M, Froehlich JB, Eagle KA and Saint S: Effect of
perioperative statins on death, myocardial infarction, atrial
fibrillation, and length of stay: A systematic review and
meta-analysis. Arch Surg. 147:181–189. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Gultekin N, Bulut G, Kucukates E, Yildiz
A, Kocas C and Bulut L: Apoptosis kinetics at reperfusion period in
patients with acute ST-Segment Elevation Myocardial Infarction
undergoing primary percutaneous coronary intervention and treated
with thrombolytic therapy. J Pak Med Assoc. 66:808–814.
2016.PubMed/NCBI
|
|
35
|
Pourafkari L, Visnjevac O, Ghaffari S and
Nader ND: Statin drugs mitigate cellular inflammatory response
after ST elevation myocardial infarction, but do not affect
in-hospital mortality. J Cardiovasc Thorac Res. 8:34–39. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hochhauser E, Cheporko Y, Yasovich N,
Pinchas L, Offen D, Barhum Y, Pannet H, Tobar A, Vidne BA and Birk
E: Bax deficiency reduces infarct size and improves long-term
function after myocardial infarction. Cell Biochem Biophys.
47:11–20. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Li T, Kilic A, Wei X, Wu C, Schwartzbauer
G, Yankey GK, DeFilippi C, Bond M, Wu ZJ and Griffith BP: Regional
imbalanced activation of the calcineurin/BAD apoptotic pathway and
the PI3K/Akt survival pathway after myocardial infarction. Int J
Cardiol. 166:158–165. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lv FH, Yin HL, He YQ, Wu HM, Kong J, Chai
XY and Zhang SR: Effects of curcumin on the apoptosis of
cardiomyocytes and the expression of NF-κB, PPAR-γ and Bcl-2 in
rats with myocardial infarction injury. Exp Ther Med. 12:3877–3884.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mercier E, Cochery-Nouvellon E, Lavigne G,
Bertinchant JP and Gris JC: In support of the revised World Health
Organization diagnostic criteria for essential thrombocythemia:
JAK2 V617F and premature myocardial infarction. J Thromb Haemost.
6:206–207. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Enomoto D, Obana M, Miyawaki A, Maeda M,
Nakayama H and Fujio Y: Cardiac-specific ablation of the STAT3 gene
in the subacute phase of myocardial infarction exacerbated cardiac
remodeling. Am J Physiol Heart Circ Physiol. 309:H471–H480. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wu J, Yu J, Xie P, Maimaitili Y, Wang J,
Yang L, Ma H, Zhang X, Yang Y and Zheng H: Sevoflurane
postconditioning protects the myocardium against
ischemia/reperfusion injury via activation of the JAK2-STAT3
pathway. PeerJ. 5:e31962017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Luo R, Chen X, Ma H, Yao C, Liu M, Tao J
and Li X: Myocardial caspase-3 and NF-κB activation promotes
calpain-induced septic apoptosis: The role of Akt/eNOS/NO pathway.
Life Sci. 222:195–202. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhao Q, Cui Z, Zheng Y, Li Q, Xu C, Sheng
X, Tao M and Xu H: Fenofibrate protects against acute myocardial
I/R injury in rat by suppressing mitochondrial apoptosis as
decreasing cleaved caspase-9 activation. Cancer Biomark.
19:455–463. 2017. View Article : Google Scholar : PubMed/NCBI
|