Introduction
Primary salivary-type lung tumors are rare
intrathoracic malignancies and account for approximately 0.1–0.2%
of all lung cancers (1,2). These tumors used to be grouped under
the name ‘bronchial adenoma’, a term that was used to describe a
group of slow-growing neoplasms thought to arise from the bronchial
glands, and included adenoid cystic carcinomas (ACC),
mucoepidermoid carcinoma (MEC), mixed tumors and carcinoid tumors
(1,3). Intrathoracic MEC tumors are usually
considered to be mild-behavior malignancies and patients have
significantly better outcomes than typical non-small-cell lung
cancer. MECs are classified as low- or high-grade depending on the
number of mitoses present and the levels of necrosis and nuclear
pleomorphisms. Low-grade tumors tend to contain a higher proportion
of mucous cells and high-grade tumors contain more squamous cells
(1). The outcomes of patients with
low-grade MEC were more positive than those of patients with
typical lung carcinoma (1,3–6). These
types of tumor have a lower tumor grade, lower clinical stages and
patients have more complete surgical procedures compared with other
types of lung cancer, which partially explains the favorable
prognosis. However, the molecular characteristics of MEC should be
further investigated.
Basement membranes (BMs) line organs and smaller
structures, such as the epithelium, capillary walls, alveoli and
the pleura. Degradation of the BM is required for local invasion of
the tumor cells and further degradation is required in metastasis
(7). In carcinogenesis, the cancer
cells gain the ability to degrade extracellular components,
including the BM, by producing proteolytic enzymes. Matrix
metalloproteinases (MMPs) are enzymes that degrade various sections
of BMs. These enzymes are associated with the ability of cancer
cells to penetrate into connective tissues. Approximately 23
different MMPs have been identified thus far. Among them, MMP-2 and
MMP-9 are most often associated with various malignancies. In
various carcinomas, MMPs have been associated with poor prognosis,
invasiveness or poor differentiation (7–9).
Furthermore, lung cancer cells produce MMP-2 and MMP-9 in
vitro (8). MMP-2 was found to
be correlated to tumor spread in NSCLC (10). In adenocarcinoma of the lung,
patients with a positive immunoreactivity for MMP-9 or MMP-2 have
also been found to have an unfavorable prognosis when compared to
patients with a lack of immunoreaction for MMP-9 or MMP-2 (9). In early-stage NSCLC, strong MMP-2
immunoreactivity predicts an unfavorable outcome (7).
Due to the low morbidity rate of MECs, the molecular
profiles of this disease were not well addressed. Consequently, for
the first time, the expression of MMP-2, MMP-7 and MMP-9 was
compared in 34 patients with low-grade MECs to that of 76 matched
NSCLC patients.
Materials and methods
Study population
In total, 37 cases of MEC were diagnosed and treated
with complete surgery in the Shanghai Pulmonary Hospital between
2000 and 2008. MEC tumors were divided into high- or low-grade by
two experienced pathologists on the basis of mitotic activity and
cellular differentiation (6,11–12).
A total of 76 consecutive typical NSCLC patients with cancers at
the same stage were selected as a control cohort during the same
period. A preoperative staging computed tomographic (CT) scan was
performed for each patient. The histology of each specimen was
assessed according to the WHO classification and the pathological
stage of the staging system. The exact TNM classification (UICC,
2002) and the stage of the tumor were recorded by reviewing the
clinical, radiological and histopathological statements from the
patient files. Histologically, the low-grade variant has a
relatively benign course allowing for conservative pulmonary
resection as the sole therapy (13). The typical lung cancer patients and
the high-grade MEC patients received chemotherapy, while the
low-grade MEC patients received surgery. No patient received either
chemotherapy or radiotherapy prior to surgery. The experimental
protocols were approved by the appropriate institutional review
committee and met the guidelines of the responsible governmental
agency.
Immunohistochemistry
MMP-2 mouse monoclonal antibody clone 42-5D11
recognizing latent and active MMP-2, at a dilution of 1:50
(Chemicon International Ltd., Billerica, MA, USA); MMP-7 mouse
monoclonal antibody clone 141-7B2 recognizing latent and active
MMP-2, at a dilution of 1:800 (Chemicon International Ltd.); and
MMP-9 mouse monoclonal antibody clone 56-2A4 recognizing latent and
active MMP-9, at a dilution of 1:100 (Chemicon International Ltd.),
were used. Formalin-fixed paraffin-embedded sections of tissue
blocks (4-μm) obtained from the tumor periphery were mounted on
silane-coated slides. Sections were de-waxed in xylene and
rehydrated through the use of graded alcohols. Antigen retrieval
for MMP-2, MMP-7 and MMP-9 was achieved by pressure cooking slides
for 2 min in 10 mM citric acid buffer at pH 6. Endogenous
peroxidase activity was blocked by treatment with 2% hydrogen
peroxide for 30 min. Sections were rinsed in deionised water and
then in Tris-buffered saline (TBS) containing 0.1% bovine serum
albumin (BSA). To block non-specific staining, slides were
incubated in 20% normal rabbit serum for 10 min. Sections were
incubated overnight at 4°C with the primary antibody. Sections were
washed in TBS, then incubated sequentially with biotinylated rabbit
anti-mouse IgG (Dako) at a dilution of 1:400, followed by
streptavidin combined in vitro with biotinylated horseradish
peroxidase at a dilution of 1:1000 (Dako). The reaction product was
developed using diaminobenzidine tetrahydrochloride. Sections were
counterstained with hematoxylin, then dehydrated through graded
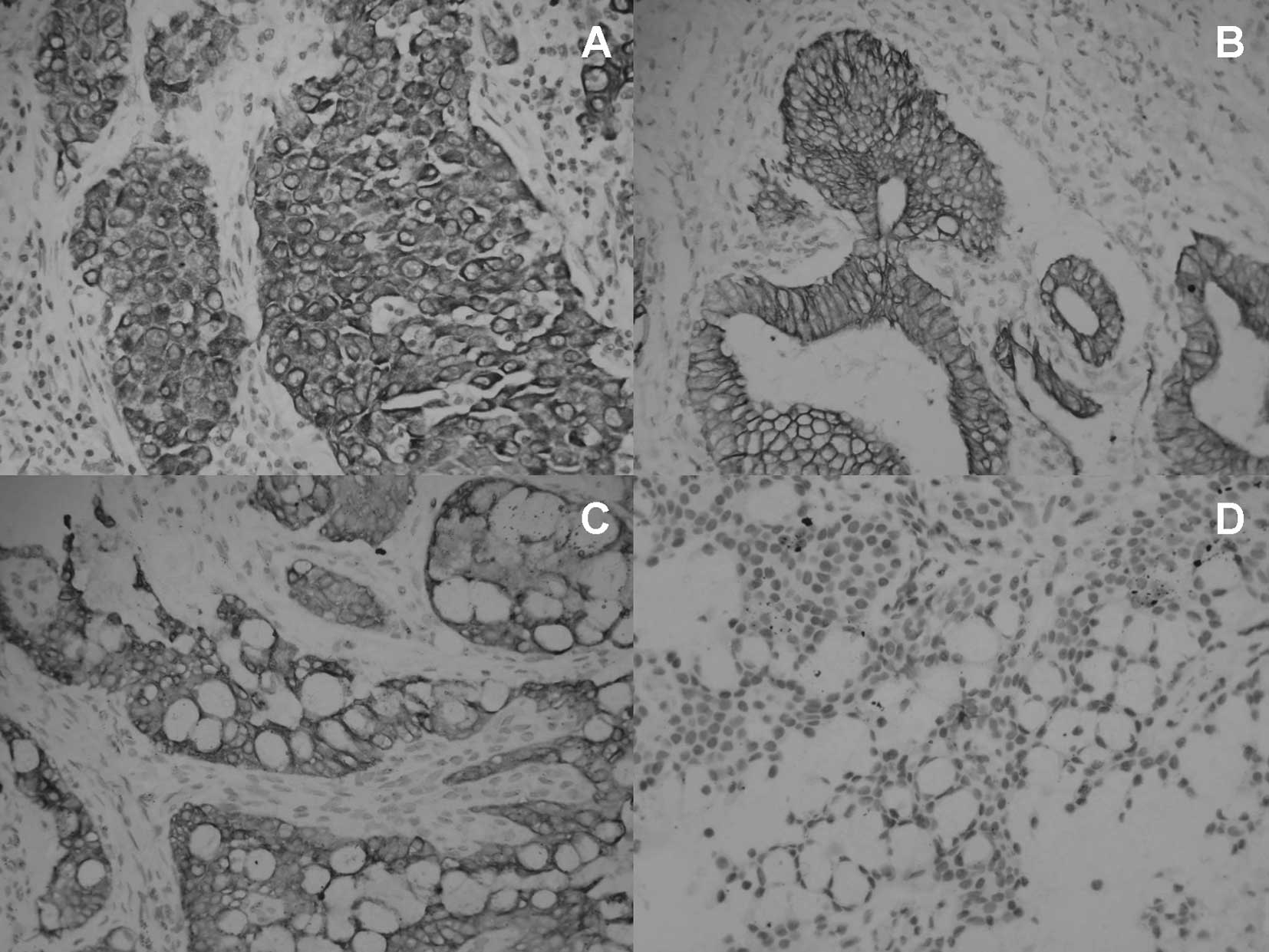
alcohols and mounted in a resinous mountant. A negative control was
included for each section where the primary antibody step was
deleted and the serum was left on. In addition, a positive control
preparation tissue that contains the specific antigen was carried
through with every batch of immunostaining to confirm that reagents
were functional and to allow assessment of staining between the
batches. For a number of antibodies the tissue also contained an
internal positive control (Fig.
1).
Evaluation of immunohistochemistry
The extent and pattern of reactivity for MMP-2,
MMP-7 and MMP-9 was recorded by two independent observers in a
blind manner, using objectives with ×10 and ×40 magnification. The
extent of expression was scored as 0 for no staining, <20%,
20–50% and 51–100%. A similar semiquantitative scale of 0, +, ++,
or +++ was used to assess the intensity of staining in comparison
with a known positive control. Cases were defined as positive if
the staining intensity was ++ or +++ in over at least 20% of the
tumors (14).
Statistical analysis
Statistical analysis was performed using the SPSS
software system (SPSS for Windows, version 11.0). The Chi-square
test was used to analyze the difference between the groups.
Results
Patient characteristics
Among the 37 MEC patients, 34 cases were diagnosed
as low-grade and only 3 cases were diagnosed as high-grade. The
characteristics of low-grade MEC patients and typical NSCLC
patients included in the study are shown in Table I. Low-grade MEC patients comprised
20 males with a mean age of 35.94 (SD 7.54) years (median 30, range
13–73) with stage Ib–IIb. For the three cases of high-grade MEC,
two cases were found with a high expression of all three types of
MMPs, and for another case, only MMP-2 was detected with a high
expression. Due to the small number of high-grade cases, the
expression of MMPs was compared only in low-grade MEC and typical
NSCLC.
 | Table IBaseline characteristics of the two
groups of patients. |
Table I
Baseline characteristics of the two
groups of patients.
| MEC (n=34) | Prevalence | Typical NSCLC
(n=76) | Prevalence | P-value |
|---|
| Gender |
| Male | 20 | 58.8% | 58 | 76.3% | |
| Female | 14 | 41.2% | 18 | 23.7% | |
| Age |
| Mean | 35.94 | - | 63 | - | |
| Median | 30 | | 65.5 | | |
| Range | - | 13–73 | - | 43–76 | |
| Stage | | | | | 0.589 |
| Ib | 16 | 47.1% | 40 | 52.6% | |
| IIb | 18 | 52.9% | 36 | 47.4% | |
Expression of MMP-2 and MMP-9 is
significantly lower in low-grade MEC than typical NSCLC
To investigate the potential relationship between
MMP expression and low-grade MEC, we compared the expression levels
of MMPs in low-grade MEC with those in typical NSCLC. The
expression of MMP-2 and MMP-9 was found to be significantly
different in the two groups; the MMP-2 positive percentage was
35.29 (12 of 34 cases) in low-grade MEC, 65.79 (50 of 76 cases) in
typical NSCLC (p=0.003), and the MMP-9 positive percentage was
35.29 (12 of 34 cases) in low-grade MEC and 57.89 (44 of 76 cases)
in normal NSCLC, respectively (p=0.028) (Table II). Thus, the results show the
expression levels of MMP-2 and MMP-9 were found to be lower in
low-grade MEC patients than in typical NSCLC patients.
| Table IIThe staining of MMPs in two groups of
patients. |
Table II
The staining of MMPs in two groups of
patients.
| Type | Negative | Positive | Prevalence | P-value |
|---|
| MMP-2 | | | | | 0.003 |
| Low-grade MEC | 22 | 12 | 35.29% | |
| Typical NSCLC | 26 | 50 | 65.79% | |
| MMP-7 | | | | | 0.172 |
| Low-grade MEC | 20 | 14 | 41.18% | |
| Typical NSCLC | 34 | 42 | 55.26% | |
| MMP-9 | | | | | 0.028 |
| Low-grade MEC | 22 | 12 | 35.29% | |
| Typical NSCLC | 32 | 44 | 57.89% | |
Expression of MMP-7 shows no difference
in low-grade MEC and typical NSCLC
No significant difference was found for MMP-7
expression between low-grade MEC and typical NSCLC tissues. The
positive MMP-7 percentage was 41.18 (14 of 34 cases) in low-grade
MEC and 55.26 (42 of 76 cases) in typical NSCLC individually
(p=0.172).
Discussion
MEC tumors are usually considered to be low-grade
malignancies and patients have significantly better outcomes than
typical non-small-cell lung cancer patients. Molina et al
(1) reported that the overall 5-
and 10-year survival rates for MEC were 88%. Patient outcomes with
MEC were found to be better than those of patients with typical
lung carcinoma (13). Several
studies have also reported high mortality in patients with MEC
(3–6). It was demonstrated that patients with
MEC, particularly those with low-grade tumors, had a better outcome
(12). Another characteristic of
MEC tumors is the rare metastasis to regional lymph nodes and the
higher stage is correlated with locally aggressive disease
(15).
Metastasis is the final stage in tumor progression
from a normal cell to a completely malignant one and involves a
number of steps. One of the initial steps in the metastatic process
involves degradation of various components of the extracellular
matrix and requires the action of proteolytic enzymes, of which
MMPs are among the most crucial. Reports have shown correlations
between degradation of the BM by MMPs and the metastatic potential
of tumor cells (16,17). Various MMPs, particularly MMP-2 and
MMP-9, appear to correlate with early cancer-related deaths in
NSCLC (7,18).
For the first time, the expression of MMP-2, MMP-7
and MMP-9 has been evaluated in MEC tumors. The current study
demonstrated that the expression of MMP-2 and MMP-9 was lower in
low-grade MEC than in typical lung carcinoma. The expression of
MMPs emphasizes the ability of the tumor to metastasize to distant
positions. The two types of MMPs investigated in this study may
explain the low metastasis rate of the low-grade MEC tumor, and the
better survival rate of the low-grade MEC. The reason for better
prognosis of low-grade MEC than that of typical lung carcinoma may
be multifactorial, and it is thought that the reason for metastasis
is significant. At the same time, no difference in MMP-7 expression
was found between low-grade MEC and typical lung carcinoma. One
reason for this observation may be the limited sample size.
MEC patients are reportedly diagnosed at a much
younger age as compared to NSCLC patients, at a mean age of
approximately 40 years (1). In the
current study, the mean age of MEC patients was found to be much
lower than that of NSCLC patients, which is consistent with
previous studies (1). This study
indicated a slight trend towards females in MEC, while gender
predilection has also been reported in numerous studies, with a
specific predilection reported for males.
Histologically, MEC tumors are divided into high-
and low-grade tumors on the basis of mitotic activity and cellular
differentiation. The low-grade variant has a relatively benign
course allowing for conservative pulmonary resection as the sole
therapy (6). By separating MEC
tumors into low-grade and high-grade tumors, Yousem and Hochholzer
(11) reported a 95% survival rate
in 41 patients with low-grade tumors who had a follow-up that
ranged between 2 months and 272 months. However, among the 13
patients with high-grade MEC, almost 25% experienced recurrences
and succumbed to the disease. This incidence was often correlated
with locally aggressive disease, with approximately 50% of patients
with high-grade tumors revealing pulmonary parenchymal invasion. In
our institute, between 2000 and 2008, only three cases of MEC were
diagnosed as high-grade and two of them were with a high expression
of three types of MMPs; one case only had a high expression of
MMP-2. Due to the small number of patients, it was not possible to
explore the difference in MMP expression between high-grade and
low-grade MEC tumors.
Due to the short follow-up time in this cohort (30%
of the MEC patients were diagnosed in 3 years), the multivariate
survival analyses for the MEC tumor were not conducted in the
current study.
In conclusion, the results show that MMP-2 and MMP-9
expression is lower in low-grade MEC than in typical NSCLC. This
reduced expression may be a reason for the non-aggressive behavior
of the low-grade MEC tumor, while the expression of MMP-7 was not
significantly different in the two groups. In addition, it appears
that high-grade MEC revealed a higher expression of MMPs than
low-grade MEC, in spite of the small numbers of high-grade MEC
cases studied. Although the present results help to clarify the
molecular profiles of MEC, further studies are required to
elucidate the molecular mechanisms of MEC, which may lead to the
appropriate treatment of MEC in the future.
Acknowledgements
The study was supported in part by a grant from the
Ph.D. Programs Foundation of the Ministry of Education of China
(No. 200802471012). This study also was supported in part by the
Natural Science Foundation of Shandong Province (2007ZRC03088). We
also gratefully acknowledge the technical assistance of two
pathologists: Dr Rong-Xuan Zhang and Dr Chao-Fu Wang.
References
|
1
|
Molina JR, Aubry MC, Lewis JE, et al:
Primary salivary gland-type lung cancer: spectrum of clinical
presentation, histopathologic and prognostic factors. Cancer.
110:2253–2259. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heitmiller RF, Mathisen DJ, Ferry JA, Mark
EJ and Grillo HC: Mucoepidermoid lung tumors. Ann Thorac Surg.
47:394–399. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chin CH, Huang CC, Lin MC, Chao TY and Liu
SF: Prognostic factors of tracheobronchial mucoepidermoid
carcinoma–15 years experience. Respirology. 13:275–280. 2008.
|
|
4
|
Yang KY, Chen YM, Huang MH and Perng RP:
Revisit of primary malignant neoplasms of the trachea: clinical
characteristics and survival analysis. Jpn J Clin Oncol.
27:305–309. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lal DR, Clark I, Shalkow J, et al: Primary
epithelial lung malignancies in the pediatric population. Pediatr
Blood Cancer. 45:683–686. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Torres AM and Ryckman FC: Childhood
tracheobronchial mucoepidermoid carcinoma: a case report and review
of the literature. J Pediatr Surg. 23:367–370. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Passlick B, Sienel W, Seen-Hibler R, et
al: Overexpression of matrix metalloproteinase 2 predicts
unfavorable outcome in early-stage non-small cell lung cancer. Clin
Cancer Res. 6:3944–3948. 2000.PubMed/NCBI
|
|
8
|
Gonzalez N, Rodriguez N, Tripari J, et al:
RT-PCR comparative study of viral load levels in the HIV positive
population in Puerto Rico before and after protease inhibitor
regimen implanted. Bol Asoc Med P R. 90:16–20. 1998.
|
|
9
|
Kodate M, Kasai T, Hashimoto H, Yasumoto
K, Iwata Y and Manabe H: Expression of matrix metalloproteinase
(gelatinase) in T1 adenocarcinoma of the lung. Pathol Int.
47:461–469. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brown PD, Bloxidge RE, Stuart NS, Gatter
KC and Carmichael J: Association between expression of activated
72-kilodalton gelatinase and tumor spread in non-small-cell lung
carcinoma. J Natl Cancer Inst. 85:574–578. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yousem SA and Hochholzer L: Mucoepidermoid
tumors of the lung. Cancer. 60:1346–1352. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Moran CA, Suster S and Koss MN: Primary
adenoid cystic carcinoma of the lung. A clinicopathologic and
immunohistochemical study of 16 cases. Cancer. 73:1390–1397. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Minna JD, Roth JA and Gazdar AF: Focus on
lung cancer. Cancer Cell. 1:49–52. 2002. View Article : Google Scholar
|
|
14
|
Hoikkala S, Paakko P, Soini Y, Makitaro R,
Kinnula V and Turpeenniemi-Hujanen T: Tissue MMP-2 and MMP-9 are
better prognostic factors than serum MMP-2/TIMP-2-complex or TIMP-1
in stage I–III lung carcinoma. Cancer Lett. 236:125–132.
2006.PubMed/NCBI
|
|
15
|
Turnbull AD, Huvos AG, Goodner JT and
Foote FW Jr: Mucoepidermoid tumors of bronchial glands. Cancer.
28:539–544. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chambers AF and Matrisian LM: Changing
views of the role of matrix metalloproteinases in metastasis. J
Natl Cancer Inst. 89:1260–1270. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Westermarck J and Kahari VM: Regulation of
matrix metalloproteinase expression in tumor invasion. FASEB J.
13:781–792. 1999.PubMed/NCBI
|
|
18
|
Sienel W, Hellers J, Morresi-Hauf A, et
al: Prognostic impact of matrix metalloproteinase-9 in operable
non-small cell lung cancer. Int J Cancer. 103:647–651. 2003.
View Article : Google Scholar : PubMed/NCBI
|