Introduction
Soft tissue sarcomas are a common type of sarcoma
and account for >3,560 mortalities each year. In 2007, the
incidence of soft tisue sarcomas in the United States was estimated
to be 9,220 (1). However, the
incidence of this heterogeneous group of mesenchymal extraskeletal
malignancies, which usually occur in the extremities, trunk,
retroperitoneum or head and neck, is relatively low (2–4). It is
believed that the dose of radiation therapy used to treat cancer
exerts a major effect on the incidence (5,6), along
with other risk factors, including exposure to certain chemicals,
herbicides, such as phenoxyacetic acids, and wood preservatives
containing chlorophenols (7,8). The
median survival rate depends on the histology subtype (3) and age at onset of the disease and is
∼1 year, with only 10% of cases surviving for up to 5 years
(2). The standard treatment
modalities are reported to have a minimal impact on the prognosis
of the patients (2,9,10).
Surgery supplemented with radiotherapy is feasible and reliable for
localized diseases (11), but
patients have a 50% chance of developing metastases (12). In these instancs, metastasectomy is
usually attempted. In cases of inoperable recurrent disease,
palliative treatment is administered, while for the metastatic form
of the disease, systemic chemotherapy is usually prescribed to
control disease progression and thus improve the survival rate of
the patients (13–15). In order to improve the current
treatment modalities, novel approaches to prevent or treat the
disease are required urgently. It has been shown that the NK cells
of sarcoma patients are as potent as the NK cells of healthy
controls in the lysing of the tumor cells (16,17).
There is an increasing amount of evidence available concerning the
involvement of the immune system and how it may be manipulated in
various ways to recognize and kill tumors. The effector activity of
NK and T cells in reacting against the cancer antigens has been
demonstrated (18), with favorable
responses being observed in various tumors (19). In concordance with previous results
showing the positive response of sarcomas to immunotherapy
(20,21), the present study reports our
experiences using in vitro cultured autologous NK and T
cells to treat a 35-year-old male diagnosed with sarcoma in
2010.
Case report
A 35-year-old Chinese male patient with a 1-year
history of left arm swelling from unknown causes was investigated
in February 2010. Written informed patient consent was obtained
from the patient. Histological investigation on multiple biopsies
revealed tumor tissue composed of nodular proliferation that was
predominantly eosinophilic, with a few spindle cells and large
areas of central necrosis and hemorrhage. The epithelial cells
exhibited abundant eosinophilic cytoplasm with large vesicular
nuclei and prominent cell nuclei. No vascular invasion was observed
and the patient had a multifocal disease that extended along the
span of the left arm in addition to the disease in the left
axillaries, left clavicular and right upper planar region.
Immunohistochemical analysis revealed positivity for cytokeratin
(CK), EMA, vimentin and CD34, but was negative for S100, desmin,
smooth muscle actin (SMA), melanin, CD68 and HMB45. The results
were consistent between the left forearm and left arm epithelioid
sarcoma. The patient sought advice from the sarcoma team at the
Peter MacCallum Cancer Institute (East Melbourne, Australia), who
advised that the patient undergo neoadjuvant chemotherapy with
ifosfamide and Adriamycin. After 6 cycles, positron emission
tomography scan images showed a partial response in the soft tissue
density of the left upper extremity and axilla. Computed tomography
scanning showed a reduction in the size of the planar base mass.
After much deliberation, the patient opted to undergo autologous
immune enhancement therapy (AIET).
As a therapeutic alternative, the patient received 7
infusions of AIET. The patient initially underwent an induction
phase, receiving 6 harvestings of peripheral blood every 2 weeks.
After a 5 month follow-up, the patient volunteered for consecutive
AIET infusions. Peripheral blood (60 ml) was collected from the
patient each time and peripheral blood mononuclear cells (PBMCs)
were isolated from the blood as per the protocol described by
Terunuma et al(22).
Isolated PBMCs were seeded onto anti-CD3 and anti-CD16-coated
flasks and incubated overnight at 39°C with 5% CO2. The
cultures were then incubated at 37°C and maintained for 14–16 days
with routine media nourishment using the patient’s own plasma
separated from the peripheral blood. Interleukin-2 was added as a
supplement during the NK and T cell seeding. After an optimal
expansion to the desired cell population, cells were harvested by
centrifugation and washed three times using phosphate-buffered
saline. The retrieved cell number was measured using the Trypan
blue dye exclusion test and the cells were then re-suspended in
100–200 ml of normal saline with human albumin for intravenous
infusion.
Discussion
Using the adopted method for the expansion of NK and
T cells, it was determined that the average expansion of the cell
population, from initial cell counts of 3.3×106 NK cells
and 19.3×106 T cells, to final cell counts of
18.8×108 and 17.6×108 cells, respectively,
was possible without using allogenic cells as a feeder layer to
ensure the safety of the cells being infused. Thus, cell number
expansions of >100-fold was achieved using the present method.
Throughout the whole process, the rate of expansion was monitored
and the cell density was manipulated according to the in
vitro culture conditions. Table
I shows the initial and final NK and T cell counts.
 | Table IInitial and final cell number of NK
and T cells. |
Table I
Initial and final cell number of NK
and T cells.
| No. of infusions | Cell number (million)
|
|---|
Initial culture
| Final culture
|
|---|
| NK cells | T cells | NK cells | T cells |
|---|
| 1 | 4.6 | 25.8 | 1,584 | 1,818.2 |
| 2 | 0.8 | 5.2 | 1,496 | 1,496 |
| 3 | 1.3 | 10.0 | 560 | 2,132 |
| 4 | 4.2 | 24.2 | 3,070 | 644 |
| 5 | 5.8 | 33.7 | 4,721 | 644 |
| 6 | 3.1 | 19.5 | 1,224 | 1,336 |
| 7 | 3.1 | 16.7 | 1,917 | 4,230 |
It was noticeable in the expanded cell number, the
large anticancer immune cell population (NK and T cells) in the
cell suspension reacted actively against the tumor cells in
vivo. The patient responded well to AIET and clear skin
improvement was observed following each infusion. The patient’s
chest radiography remained stable, therefore the tumor did not
metastisize to the lungs. Significantly, the administered in
vitro expanded cells did not exhibit any adverse reactions in
the patient, as has been shown in numerous other studies (23). The patient opted to undergo a
3-month break and during the tail-end of this period, worsening of
the skin lesion was observed. The patient decided to restart the
therapy and after one infusion, and marked improvement was noted.
Although the lesions persist, the fact that the patient has
surpassed the anticipated survival duration is encouraging.
However, certain secondary immune responses, such as wound healing,
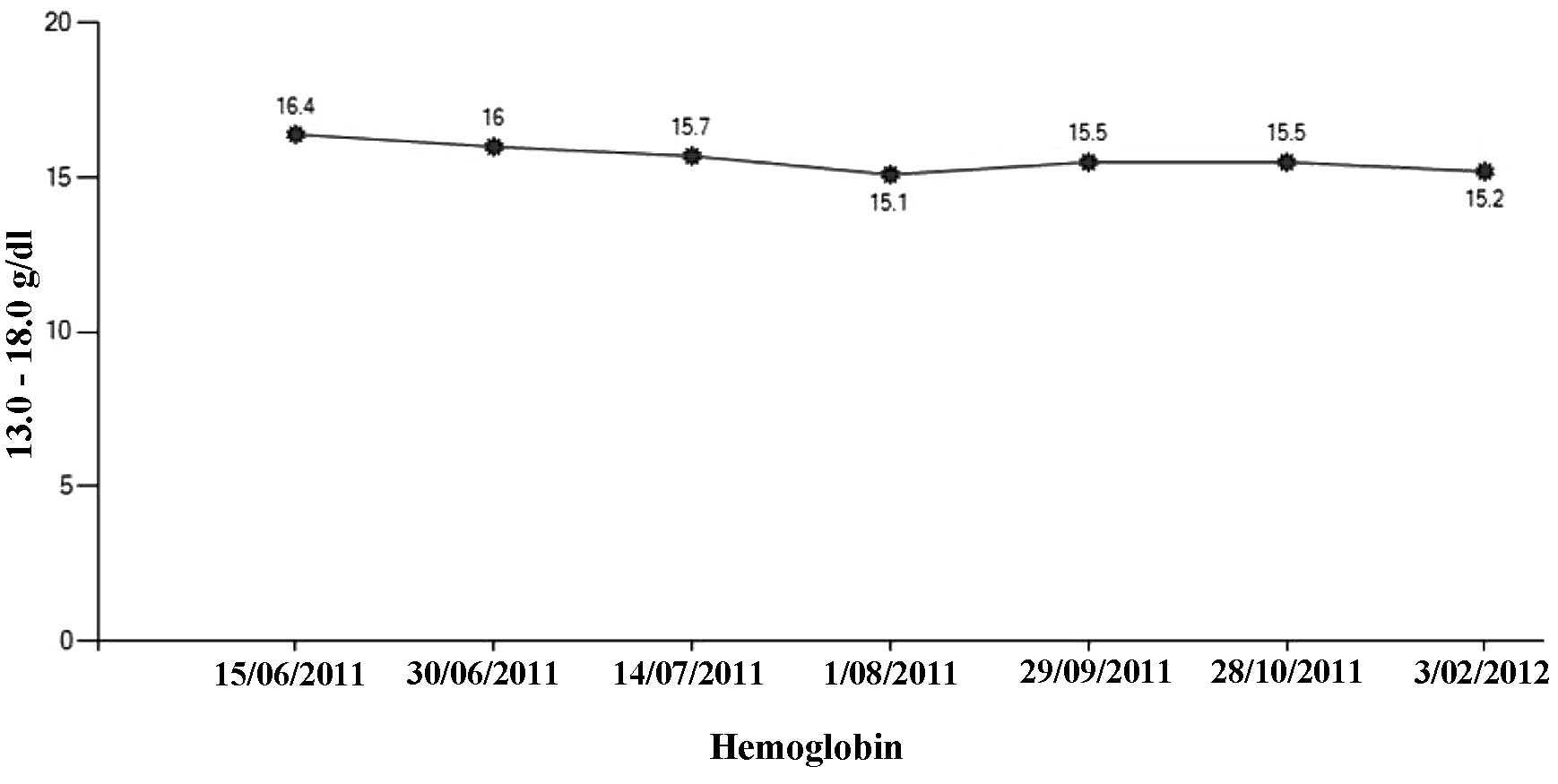
were observed. After three infusions of AIET, one of the largest
tumor areas on the forearm (4×2 cm) stopped bleeding and growth of
new tissue was visible, along with the recovery of smaller wounds,
and during the course of the AIET, the hemoglobin level, which is
believed to decrease depending on the disease severity and
progression, remained stable. Fig.
1 shows the analysis of the results concerning hemoglobin
levels between June 2011 and February 2012. The patient’s overall
survival is at present 25 months and the patient has not received
chemotherapy since August 2010. These promising results obtained
with the current therapeutic approach may be an effective
immunotherapeutic strategy for managing difficult tumors, such as
soft tissue sarcomas (24), which
were the first tumors studied for antitumor immunity (25).
In conclusion, the present case study demonstrates
the efficacy of immunotherapy for a rare type of cancer that
otherwise had no options for therapeutic approaches that may
provide a favorable outcome in the patient. In vitro
expanded NK and T cells were are able to respond via their
anticancer activity under in vivo conditions without
producing adverse reactions in the patient. With repeated
administration of AIET, the prognosis of the patient improved as
well as thei quality of life of the patient. The patient acheived
stable disease without any side-effects. Therefore, the present
study also demonstrates the safety and efficacy of AIET, although a
larger study is required for more extensive analysis.
References
|
1
|
Demetri GD, Baker LH, Benjamin RS, et al:
Soft tissue sarcoma. J Natl Compr Canc Netw. 5:364–399.
2007.PubMed/NCBI
|
|
2
|
Pedrazzoli P, Secondino S, Perfetti V,
Comoli P and Montagna D: Immunotherapeutic Intervention against
Sarcomas. J Cancer. 2:350–356. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ferrari A, Miceli R, Casanova M, et al:
The symptom interval in children and adolescents with soft tissue
sarcomas. Cancer. 116:177–183. 2010.PubMed/NCBI
|
|
4
|
Cormier JN and Pollock RE: Soft tissue
sarcomas. CA Cancer J Clin. 54:94–109. 2004. View Article : Google Scholar
|
|
5
|
Brady MS, Gaynor JJ and Brennan MF:
Radiation-associated sarcoma of bone and soft tissue. Arch Surg.
127:1379–1385. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zahm SH and Fraumeni JF Jr: The
epidemiology of soft tissue sarcoma. Semin Oncol. 24:504–514.
1997.PubMed/NCBI
|
|
7
|
Hardell L and Sandström A: Case-control
study: soft-tissue sarcomas and exposure to phenoxyacetic acids or
chlorophenols. Br J Cancer. 39:711–717. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Smith AH, Pearce NE, Fisher DO, Giles HJ,
Teague CA and Howard JK: Soft tissue sarcoma and exposure to
phenoxyherbicides and chlorophenols in New Zealand. J Natl Cancer
Inst. 73:1111–1117. 1984.PubMed/NCBI
|
|
9
|
Mori K, Rédini F, Gouin F, Cherrier B and
Heymann D: Osteosarcoma: current status of immunotherapy and future
trends (Review). Oncol Rep. 15:693–700. 2006.PubMed/NCBI
|
|
10
|
Wolf PS, Flum DR, Tanas MR, Rubin BP and
Mann GN: Epithelioid sarcoma: the University of Washington
experience. Am J Surg. 196:407–412. 2008. View Article : Google Scholar
|
|
11
|
Gough NJ, Smith C, Ross JR, Riley J and
Judson I: Symptom burden, survival and palliative care in advanced
soft tissue sarcoma. Sarcoma. 2011:3251892011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Coindre JM, Terrier P, Guillou L, et al:
Predictive value of grade for metastasis development in the main
histologic types of adult soft tissue sarcomas: a study of 1240
patients from the French Federation of Cancer Centers Sarcoma
Group. Cancer. 91:1914–1926. 2001. View Article : Google Scholar
|
|
13
|
Sinha S and Peach AH: Diagnosis and
management of soft tissue sarcoma. BMJ. 341:c71702010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Grimer R, Judson I, Peake D and Seddon B:
Guidelines for the management of soft tissue sarcomas. Sarcoma.
2010:5061822010.PubMed/NCBI
|
|
15
|
Clark MA, Fisher C, Judson I and Thomas
JM: Soft-tissue sarcomas in adults. N Engl J Med. 353:701–711.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Buddingh EP, Schilham MW, Ruslan SE, et
al: Chemotherapy-resistant osteosarcoma is highly susceptible to
IL-15-activated allogeneic and autologous NK cells. Cancer Immunol
Immunother. 60:575–586. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cho D and Campana D: Expansion and
activation of natural killer cells for cancer immunotherapy. Korean
J Lab Med. 29:89–96. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matar P, Alaniz L, Rozados V, et al:
Immunotherapy for liver tumors: present status and future
prospects. J Biomed Sci. 16:302009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Manjunath SR, Ramanan G, Dedeepiya VD, et
al: Autologous immune enhancement therapy in recurrent ovarian
cancer with metastases: a case report. Case Rep Oncol. 5:114–118.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Maki RG: Soft tissue sarcoma as a model
disease to examine cancer immunotherapy. Curr Opin Oncol.
13:270–274. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Maki RG: Future directions for
immunotherapeutic intervention against sarcomas. Curr Opin Oncol.
18:363–368. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Takada M, Terunuma H, Deng X, et al:
Refractory lung metastasis from breast cancer treated with
multidisciplinary therapy including an immunological approach.
Breast Cancer. 18:64–67. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Montagna D, Turin I, Schiavo R, et al:
Feasibility and safety of adoptive immunotherapy with ex
vivo-generated autologous, cytotoxic T lymphocytes in patients with
solid tumor. Cytotherapy. 14:80–90. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Valle AA and Kraybill WG: Management of
soft tissue sarcomas of the extremity in adults. J Surg Oncol.
63:271–279. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Francescutti V and Skitzki JJ: Sarcomas
and the immune system: implications for therapeutic strategies.
Surg Oncol Clin N Am. 21:341–355. 2012. View Article : Google Scholar : PubMed/NCBI
|