Introduction
Metastases to the supraclavicular region may
originate from the head and neck and from infraclavicular tumors.
The principal metastatic sites from the head and neck region are
the hypopharynx, oropharynx and nasopharynx. Infraclavicular
primary sites mostly originate from the lung, breast, lower
digestive tract and genitourinary tract (1). Ovarian malignancies are rare primary
sites for supraclavicular lymph node metastases. The present study
reports a case of an occult ovarian cancer patient with bilateral
supraclavicular lymph node metastases, where positive circulating
tumor cells (CTC) were detected by the CellSearch system at the
time of diagnosis. To the best of our knowledge, this is the first
study to demonstrate that CTCs may be identified in patients with
cancer of unknown primary (CUP) using the CellSearch system. In
addition, the diagnostic procedures of CUP metastatic to the
cervical lymph nodes and the clinical features of CTC are discussed
with regard to the current knowledge.
Case report
In February 2011, a female 60-year-old Chinese
patient was admitted to the Otolaryngology-Head and Neck Surgery
Department of the Beijing Tongren Hospital (Key Laboratory of
Otolaryngology-Head and Neck Surgery, Ministry of Education,
Capital Medical University, Beijing, China) complaining of a
growing mass in the right side of the neck that had been present
for six months. No other symptoms were observed. The patient’s
surgical, medical and family histories were unremarkable. In the
ear-nose-throat examination, a 2×2.5 cm solid, fixed mass was
identified in the right supraclavicular fossa and multiple 1×1.5 cm
solid masses were observed in the left supraclavicular fossa. A
fine-needle aspiration biopsy (FNAB) was performed in the right
supraclavicular mass and the pathological diagnosis was of a
metastatic poorly-differentiated squamous cell carcinoma.
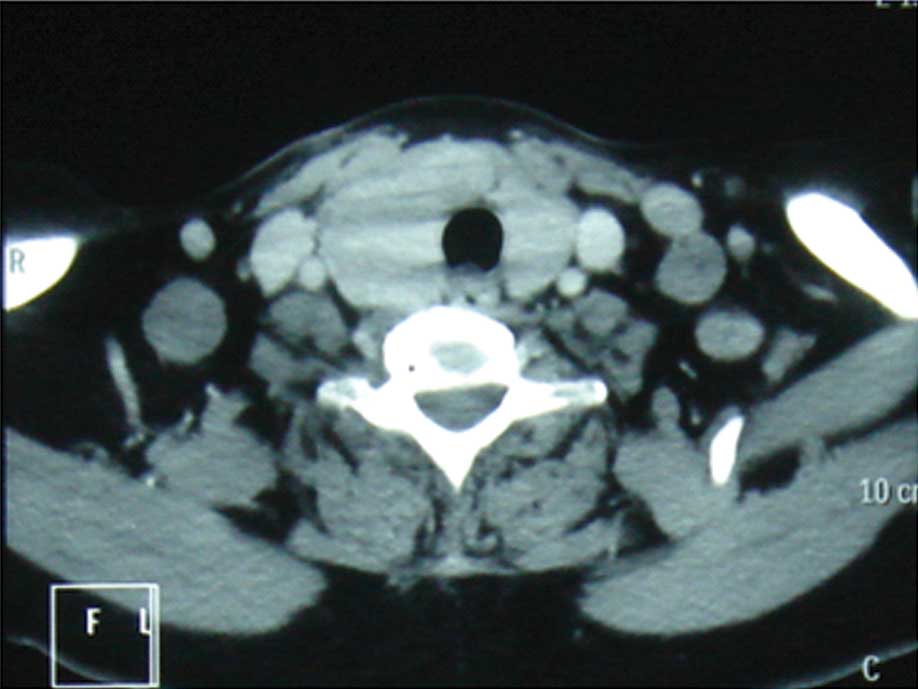
Subsequently, the patient underwent a detailed comprehensive
examination of the head, neck and upper aerodigestive tract using
nasolaryngoscopy, bronchoscopy and gastroenteroscopy and CT scans
of the neck and chest for primary malignancy, which demonstrated
only lymphadenopathy in the bilateral supraclavicular region
(Fig. 1). The patient was,
therefore, diagnosed with metastatic cervical carcinoma of unknown
primary.
Once informed consent had been obtained, a 7.5-ml
peripheral blood sample was collected from the patient and then
analyzed with the CellSearch system as described previously
(2). Three positive circulating
tumor cells (CTCs) were identified with positive expression for
epithelial cell adhesion molecule (EpCAM) and cytokeratin (CK)8, 18
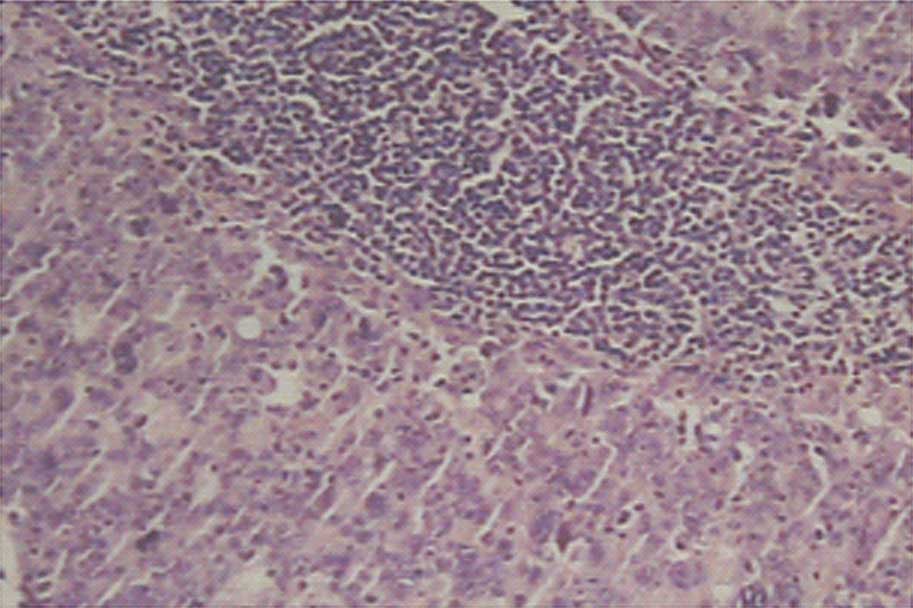
and 19. Since EpCAM is usually expressed in adenocarcinoma, an
excisional biopsy of the right supraclavicular lymph node was
performed. The findings supported the diagnosis of a
poorly-differentiated, metastatic adenocarcinoma (Fig. 2). Immunohistochemistry revealed that
the specimen tested positive for cancer antigen (CA)-125,
cytokeratin (CK)8/18, CK7, estrogen receptor (ER) and
carcinoembryonic antigen (CEA), indicating a possible gynecological
origin for the metastasis. Negative reactions were observed for
thyroid transcription factor (TTF)-1, CK20, CK5/6, Epstein-Barr
virus, vimentin, neuron specific enolase (NSE), S-100 protein,
gross cystic disease fluid protein (GCDFP)-15, thyroglobulin (TG),
calcitonin and the progesterone receptor (PR). The serum CA-125
level was elevated to 1,028 U/ml (normal <35 U/ml).
18F-fluorodeoxyglucose (FDG) positron emission
tomography combined with computed tomography (PET-CT) revealed an
intense uptake of FDG in the bilateral supraclavicular lymph nodes
and a right pelvic mass with a diameter of 3.9 cm (Fig. 3).
The patient was referred to the Gynecology
Department for further therapy. The patient underwent a bilateral
salpingo-oophorectomy and cytoreductive surgery and an ultimate
diagnosis of ovarian low-grade serous carcinoma [International
Federation of Gynecology and Obstetrics (FIGO) Stage IV] was
established by histological examination. Subsequent to surgery, the
patient was treated with 135 mg/m2 paclitaxel on day 1
and 75 mg/m2 cisplatin on day 2 intravenously,
continuing at 3-week intervals. The patient succumbed to the
disease six months later due to disease progression.
Discussion
CUP is defined as the histological diagnosis of
metastasis without the detection of a primary tumor. CUP metastatic
to the cervical lymph nodes accounts for ∼3–5% of all head and neck
cancers (3). Squamous cell
carcinoma (SCC) is the most common histology, representing 65% of
cases, followed by undifferentiated carcinoma (22%) and
adenocarcinoma (13%) (4). However,
in the case of supraclavicular node metastases, 50–76% patients
have adenocarcinoma (5). Patients
with adenocarcinoma in the metastatic lymph nodes usually have a
primary lesion located outside of the head and neck area, including
in the lung, breast, lower digestive tract or genitourinary tract
(6). The location of the lymph node
may indicate the site of origin of the primary tumor. For example,
the presence of left supraclavicular lymphadenopathy, ‘Virchow’s
node’, has been regarded as indicating the presence of cancer in
the gastrointestinal tract. By contrast, right supraclavicular
lymphadenopathy indicates the presence of cancer mainly from the
lungs, esophagus and mediastinum.
The main objectives of the diagnostic evaluation of
a patient with CUP are to determine the histology of the metastatic
tumor and identify the primary tumor. Following a routine detailed
physical examination of the head and neck and of the upper
aerodigestive tract using panendoscopy, the initial tissue
diagnostic procedure is a FNAB (7).
A FNAB results in a representative cellular sample in the majority
of CUP patients. A diagnosis is usually established with routine
histological staining, supplemented with immunochemistry, achieving
a diagnostic sensitivity of 83–97% and a specificity of 91–100% for
metastatic lesions (1)
In the majority of cases, the biological material
obtained by FNAB is sufficient for diagnosis. However, in certain
cases, insufficient immunophenotypic characterization of the
available biological material may lead to misdiagnosis (8). For example, poorly-differentiated
adenocarcinoma and carcinoma may be observed with descriptions of
the same spectrum of histological appearance, with carcinoma cells
showing a lesser degree of glandular differentiation. However, a
subset of patients with poorly-differentiated adenocarcinoma may be
distinctive in their tumor biology and responsiveness to
radiotherapy and chemotherapy. For the last few years, CTCs have
received significant attention as alternative markers (9). It has long been hypothesized that the
levels of CTCs in the peripheral blood correlates with the
aggressiveness of the tumor (10).
The detection and characterization of these cells is likely to
significantly improve the early detection of tumor spreading. The
molecular characterization and specific biological properties of
CTC may provide important diagnostic information, including the
assessment of the tumor of origin (11). Furthermore, case reports have
suggested that the morphological features of CTCs resemble the
corresponding primary and/or metastatic lesions in the breast
(12). CTCs may be used to survey
primary and metastatic lesions through minimally invasive
peripheral blood draws or ‘fluid biopsies’.
In the present study, it was shown that the analysis
of peripheral blood using the CellSearch system provided additional
information on the immunophenotype of the tumor cells. To the best
of our knowledge, the present study is the first to demonstrate
that CTCs may be identified in patients with CUP. This technology
uses positive selection with magnetically labeled anti-EpCAM and
immunocytochemical staining for CK8, 18 and 19 to isolate and
enumerate CTCs. In this regard, the expression of EpCAM has been
shown to occur in almost all adenocarcinomas, including ovarian
adenocarcinomas (13,14).
The CellSearch system has been approved by the US
Food and Drug Administration (FDA) and is the only validated and
standardized CTC detection system to be introduced into clinics.
Increasing evidence suggests that CTC numbers are an independent
predictor of progression-free survival (PFS) and overall survival
(OS) in breast, colorectal and prostate cancer according to the
CellSearch system (15). Poveda
et al reported a multicenter, randomized, exploratory study
that included 216 patients with relapsed/recurrent advanced ovarian
cancer (16). The study observed
that 45% (97/216) of the patients were CTC-positive and that the
patients with ≥2 CTCs at baseline had a significantly shorter
overall survival time and time to disease progression compared with
CTC-negative patients. However, the use of the CellSearch system to
identify CTCs in CUP has not been studied at this time.
During the last two decades, PET and PET-CT have
been increasingly used in diagnostic procedures for CUP. Several
studies have evaluated the ability of PET-CT to detect primary
tumors in patients with cervical lymph node metastases of unknown
origin. Rusthoven et al published a meta-analysis based on
16 studies that included 302 patients with cervical lymph node
metastasis from an unknown primary (17). PET detected the primary tumor in 25%
of the patients in whom panendoscopy and CT failed to identify a
primary tumor. Kwee and Kwee published a meta-analysis with 11
studies and 433 CUP patients analyzed using PET-CT (18). The global rate of tumor detection
was 37%, with a sensitivity and specificity of 84%. Al-Ibraheem
et al analyzed another set of eight studies from between
2000 and 2009, in which PET or PET-CT was used in 180 patients with
cervical lymphadenopathy of unknown origin. The study reported a
28.3% detection rate for primary tumors with 37% false-positive
scans (19). Accordingly, a recent
interdisciplinary consensus conference stated that PET-CT may be
regarded as a procedure in the diagnostic workup of CUP patients
(7). However, it is essential to be
aware of the limitations and drawbacks of PET-CT, including the
high rate of false-positive findings, the limited availability of
the procedure, the costs and the burden to the patient. Further
studies are required to assess the value of this procedure when
weighed against other diagnostic techniques.
Ovarian cancer is the second most common
gynecological cancer and the leading cause of mortality from
gynecological malignancy. The distant metastasis of ovarian cancer
mostly involves the liver, lung and bone. Lymphadenopathy in the
neck is an unusual presentation of malignant neoplasms of the ovary
and may occur prior to there being evidence of an ovarian mass;
their detection may represent a challenge for the oncologist
(20). Only a few cases of neck
metastases associated with ovarian malignancies have been reported.
Table I shows a summary of case
reports for ovarian tumors with bilateral supraclavicular
metastases from the English-language literature. In a series of 100
autopsies on female patients who succumbed to ovarian carcinoma,
the incidence of extra-abdominal lymphadenopathy in the
supraclavicular lymph nodes was shown to be only 4% (21). In a review of 35 patients with
extra-abdominal lymphadenopathy of ovarian cancer, 11 patients were
demonstrated to exhibit supraclavicular metastases (22). However, no patient exhibited
bilateral supraclavicular metastases such as that shown in Table I.
 | Table I.Cases of ovarian cancer with bilateral
supraclavicular lymph node metastases reported in the
English-language literature. |
Table I.
Cases of ovarian cancer with bilateral
supraclavicular lymph node metastases reported in the
English-language literature.
| First author, year
(ref.) | No. of cases | Pathology | FIGO stage | Treatment | Follow-up
(years) |
|---|
| Malpica et al,
2001 (29) | 1 | LGS Ca | IB | S+C | NED (6.0) |
| Verbruggen et
al, 2006 (30) | 1 | Serous borderline
ovarian tumor | IV | S+C | NED (4.5) |
| Present study | 1 | LGS Ca | IV | S+C | STD (0.5) |
Clinically, a differential diagnosis in terms of
cervical adenocarcinomas of unknown primary is that of metastases
from the lung, breast and gastrointestinal tracts.
Immunohistochemical findings are crucial in forming a differential
diagnosis. Communication between the pathologist and clinician is
extremely important for defining the tumor origin (4). There are a number of relatively
specific tumor markers that may aid in the identification of the
site of the cancer. CK7 and CK20 are the most common CK strains
used for identifying adenocarcinomas. CK7 is detected in tumors of
the lung, ovary, endometrium and breast, but not in lower
gastrointestinal tract tumors. CK20 is normally expressed in the
gastrointestinal epithelium, urothelium and Merkel cells (23). The CK phenotype
CK20+/CK7− markedly favors colonic primary
tumors. Certain studies have reported that 75–95% of colon tumors
are CK20+/CK7−, while ∼85% of lung carcinomas
are CK20−/CK7+(24). TTF-1 is another lung cancer marker
and one that ∼68% of adenocarcinomas and 25% of squamous cell lung
carcinomas have been shown to stain positively for (25). GCDFP-15 is an apocrine
differentiation marker and is specifically expressed in patients
with breast carcinomas. Among the patients with breast carcinomas,
62–72% have been identified as GCDFP-15-positive (26).
The main positive markers for ovarian
adenocarcinomas are ER, PR, CA-125 and Wilm’s tumor 1 (WT1). ER
and/or PR are positive in 50–83% of ovarian serous carcinomas.
Carcinomas arising in the breast and other sites in the female
genital tract are also ER- and PR-positive, whereas carcinomas from
other locations are ER- and PR-negative (27). WT1 and CA-125 are expressed in the
majority of ovarian serous carcinomas, but the majority of ovarian
clear cell and mucinous carcinomas are negative for the markers
(28). CA-125 is also expressed in
a minority of carcinomas, including those of the breast,
endometrium, cervix and lung. The expression of WT1 is usually
negative in breast, gastrointestinal and pancreatobiliary
primaries.
In conclusion, to the best of our knowledge, the
present study is the first to demonstrate that CTC may be detected
in the peripheral blood of patients with CUP when using the
CellSearch system. The molecular characterization and specific
biological properties of CTC may provide important information for
the diagnosis of CUP. Further studies on a larger patient
population are required to evaluate the significance of CTCs as
diagnostic decision markers in CUP. Although ovarian cancer rarely
metastasizes to the cervical lymph node, it should be considered in
the differential diagnosis of lymphadenopathy in the
supraclavicular area of postmenopausal individuals.
Acknowledgements
The present study was supported by the
Beijing Municipal Natural Science Grant (7122039) and the Beijing
Municipal Health Bureau Grant (2009208).
References
|
1.
|
Strojan P, Ferlito A, Medina JE, et al:
Contemporary management of lymph node metastases from an unknown
primary to the neck: I. A review of diagnostic approaches. Head
Neck. 35:123–132. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Gervasoni A, Sandri MT, Nascimbeni R, et
al: Comparison of three distinct methods for the detection of
circulating tumor cells in colorectal cancer patients. Oncol Rep.
25:1669–1703. 2011.PubMed/NCBI
|
|
3.
|
Strojan P, Ferlito A, Langendijk JA, et
al: Contemporary management of lymph node metastases from an
unknown primary to the neck: II. a review of therapeutic options.
Head Neck. 35:286–293. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Haas I, Hoffmann TK, Engers R and Ganzer
U: Diagnostic strategies in cervical carcinoma of an unknown
primary (CUP). Eur Arch Otorhinolaryngol. 259:325–333.
2002.PubMed/NCBI
|
|
5.
|
Giridharan W, Hughes J, Fenton JE and
Jones AS: Lymph node metastases in the lower neck. Clin Otolaryngol
Allied Sci. 28:221–226. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Chepeha D, Koch W and Pitman K: Management
of unknown primary tumor. Head Neck. 25:499–504. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Cerezo L, Raboso E and Ballesteros AI:
Unknown primary cancer of the head and neck: a multidisciplinary
approach. Clin Transl Oncol. 13:88–97. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Oien KA: Pathologic evaluation of unknown
primary cancer. Semin Oncol. 36:8–37. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
van de Stolpe A, Pantel K, Sleijfer S,
Terstappen LW and den Toonder JM: Circulating tumor cell isolation
and diagnostics: toward routine clinical use. Cancer Res.
71:5955–5960. 2011.PubMed/NCBI
|
|
10.
|
Pantel K, Brakenhoff RH and Brandt B:
Detection, clinical relevance and specific biological properties of
disseminating tumour cells. Nat Rev Cancer. 8:329–340. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Smirnov DA, Foulk BW, Doyle GV, Connelly
MC, Terstappen LW and O’Hara SM: Global gene expression profiling
of circulating endothelial cells in patients with metastatic
carcinomas. Cancer Research. 66:2918–2922. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Marrinucci D, Bethel K, Bruce RH, et al:
Case study of the morphologic variation of circulating tumor cells.
Human Pathol. 38:514–519. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Bellone S, Siegel ER, Cocco E, et al:
Overexpression of epithelial cell adhesion molecule in primary,
metastatic, and recurrent/chemotherapy-resistant epithelial ovarian
cancer: implications for epithelial cell adhesion molecule-specific
immunotherapy. Int J Gynecol Cancer. 19:860–866. 2009. View Article : Google Scholar
|
|
14.
|
Shim HS, Yoon BS and Cho NH: Prognostic
significance of paired epithelial cell adhesion molecule and
E-cadherin in ovarian serous carcinoma. Human Pathol. 40:693–698.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Miller MC, Doyle GV and Terstappen LW:
Significance of circulating tumor cells detected by the CellSearch
system in patients with metastatic breast colorectal and prostate
cancer. J Oncol. 2010:6174212010. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Poveda A, Kaye SB, McCormack R, et al:
Circulating tumor cells predict progression free survival and
overall survival in patients with relapsed/recurrent advanced
ovarian cancer. Gynecol Oncol. 122:567–572. 2011. View Article : Google Scholar
|
|
17.
|
Rusthoven KE, Koshy M and Paulino AC: The
role of fluorodeoxyglucose positron emission tomography in cervical
lymph node metastases from an unknown primary tumor. Cancer.
101:2641–2649. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Kwee TC and Kwee RM: Combined FDG-PET/CT
for the detection of unknown primary tumors: systematic review and
meta-analysis. Eur Radiol. 19:731–744. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Al-Ibraheem A, Buck A, Krause BJ,
Scheidhauer K and Schwaiger M: Clinical applications of FDG PET and
PET/CT in head and neck cancer. J Oncol. 2009:2087252009.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Fanti S, Nanni C, Castellucci P, et al:
Supra-clavicular lymph node metastatic spread in patients with
ovarian cancer disclosed at 18F-FDG-PET/CT: an unusual finding.
Cancer Imaging. 6:20–23. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Dvoretsky PM, Richards KA, Angel C, et al:
Distribution of disease at autopsy in 100 women with ovarian
cancer. Hum Pathol. 19:57–63. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Euscher ED, Silva EG, Deavers MT, Elishaev
E, Gershenson DM and Malpica A: Serous carcinoma of the ovary,
fallopian tube, or peritoneum presenting as lymphadenopathy. Am J
Surg Pathol. 28:1217–1223. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Moll R, Löwe A, Laufer J and Franke WW:
Cytokeratin 20 in human carcinomas. A new histodiagnostic marker
detected by monoclonal antibodies. Am J Pathol. 140:427–447.
1992.PubMed/NCBI
|
|
24.
|
Rubin BP, Skarin AT, Pisick E, Rizk M and
Salgia R: Use of cytokeratins 7 and 20 in determining the origin of
metastatic carcinoma of unknown primary, with special emphasis on
lung cancer. Eur J Cancer Prev. 10:77–82. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Roh MS and Hong SH: Utility of thyroid
transcription factor-1 and cytokeratin 20 in identifying the origin
of metastatic carcinomas of cervical lymph nodes. J Korean Med Sci.
17:512–517. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Kaufmann O, Deidesheimer T, Muehlenberg M,
Deicke P and Dietel M: Immunohistochemical differentiation of
metastatic breast carcinomas from metastatic adenocarcinomas of
other common primary sites. Histopathology. 29:233–240. 1996.
View Article : Google Scholar
|
|
27.
|
Mittal K, Soslow R and McCluggage WG:
Application of immunohistochemistry to gynecologic pathology. Arch
Pathol Lab Med. 132:402–423. 2008.PubMed/NCBI
|
|
28.
|
Acs G, Pasha T and Zhang PJ: WT1 is
differentially expressed in serous, endometrioid, clear cell, and
mucinous carcinomas of the peritoneum, fallopian tube, ovary, and
endometrium. Int J Gynecol Pathol. 23:110–118. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Malpica A, Deavers MT, Gershenson D,
Tortolero-Luna G and Silva EG: Serous tumors involving
extra-abdominal/extra-pelvic sites after the diagnosis of an
ovarian serous neoplasm of low malignant potential. Am J Surg
Pathol. 25:988–996. 2001. View Article : Google Scholar
|
|
30.
|
Verbruggen MB, Verheijen RH, van de Goot
FR, van Beurden M, Dorsman JC and van Diest PJ: Serous borderline
tumor of the ovary presenting with cervical lymph node involvement:
a report of 3 cases. Am J Surg Pathol. 30:739–743. 2006. View Article : Google Scholar : PubMed/NCBI
|