Introduction
Sarcomatoid carcinoma is a rare and extremely
aggressive malignant tumor, with a mixture of carcinomatous and
sarcomatous elements (1).
Sarcomatoid carcinoma occurs in diverse locations throughout the
body (2), including the upper
respiratory tract, genitourinary tract and upper and lower
digestive tracts. Pancreatic carcinosarcoma is also extremely rare
and only a few cases have been reported in the literature (3–11).
Therefore, this disease remains a diagnostic and therapeutic
challenge for surgeons. The current case study presents the first
successful use of laparoscopic distal pancreatectomy for a case of
pancreatic sarcomatoid carcinoma and discusses the associated
literature. Written informed consent was obtained from the
patient.
Case report
Patient presentation
A 48-year-old male presented with a five-month
history of epigastralgia, with weight loss of ∼3 kg in one month.
One month prior to hospitalization, a gastroscopy revealed an ulcer
in the duodenal bulb and chronic superficial gastritis. The patient
did not respond to anti-ulcer therapy. There was no remarkable past
medical history with no alcohol consumption or history of smoking.
In addition, the patient’s family medical history was unremarkable.
A physical examination revealed epigastric tenderness upon
palpation, however, no palpable abdominal masses were identified.
Laboratory examinations reported the following results: Red blood
cell (RBC) count, 4.75×1012 cells/l; hemoglobin (HB),
144 g/l; white blood cell (WBC) count, 7.3×109 cells/l;
albumin (ALB), 43.9 g/l; total bilirubin (TBIL), 19.9
μmol/l; direct bilirubin (DBIL), 2.8 μmol/l;
aspartate aminotransferase (AST), 30 U/l; and alanine
aminotransferase (ALT), 13 U/l. The carbohydrate antigen (CA)19-9,
CA50, α-fetoprotein (AFP) and carcinoembryonic antigen (CEA) levels
were 134 U/ml, 50 U/ml, 49 ng/ml and 12 ng/ml, respectively.
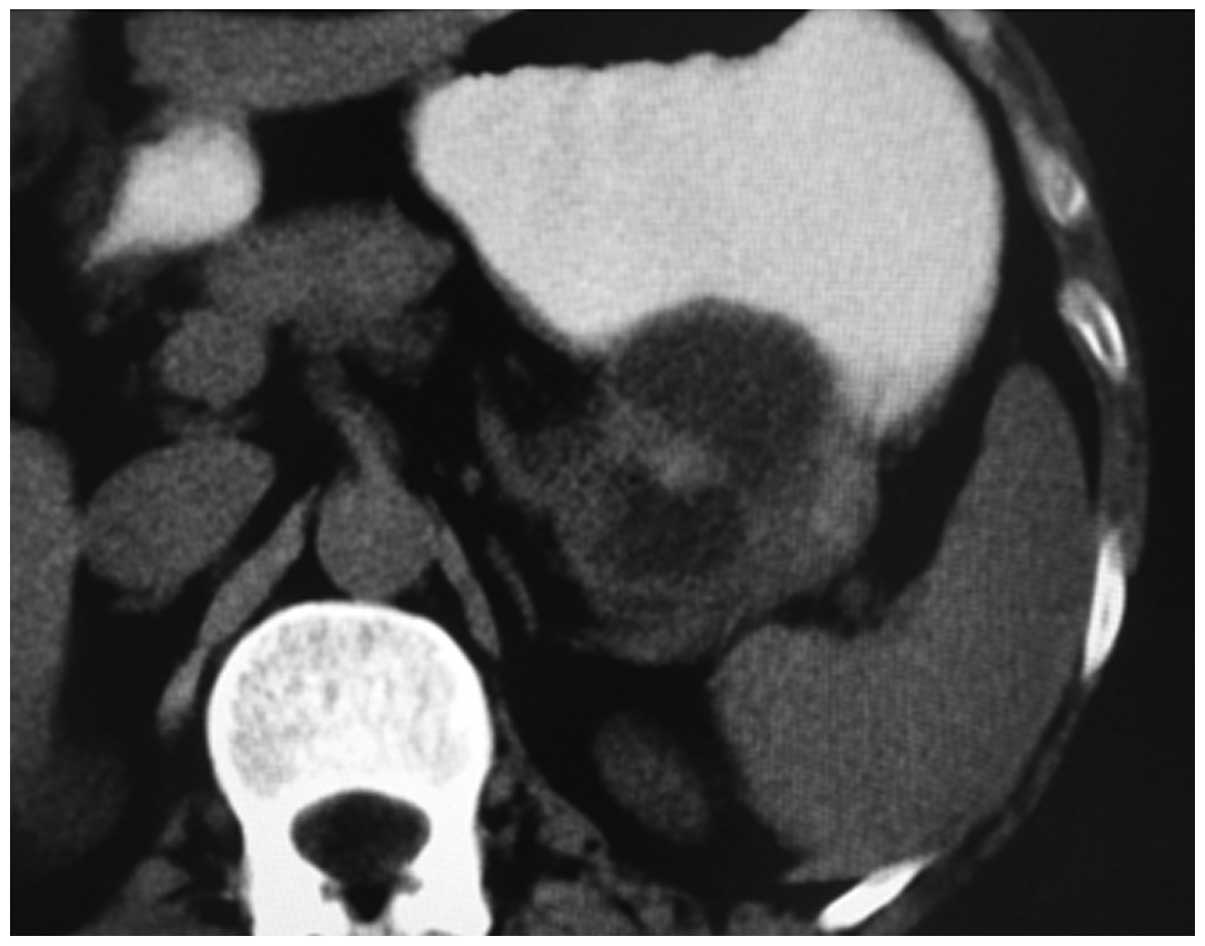
Abdominal ultrasonography revealed an ∼8×5 cm cystic mass in the
tail of the pancreas. Computed tomography revealed a large complex
cystic and solid mass in the tail of pancreas (Fig. 1).
Surgical procedures
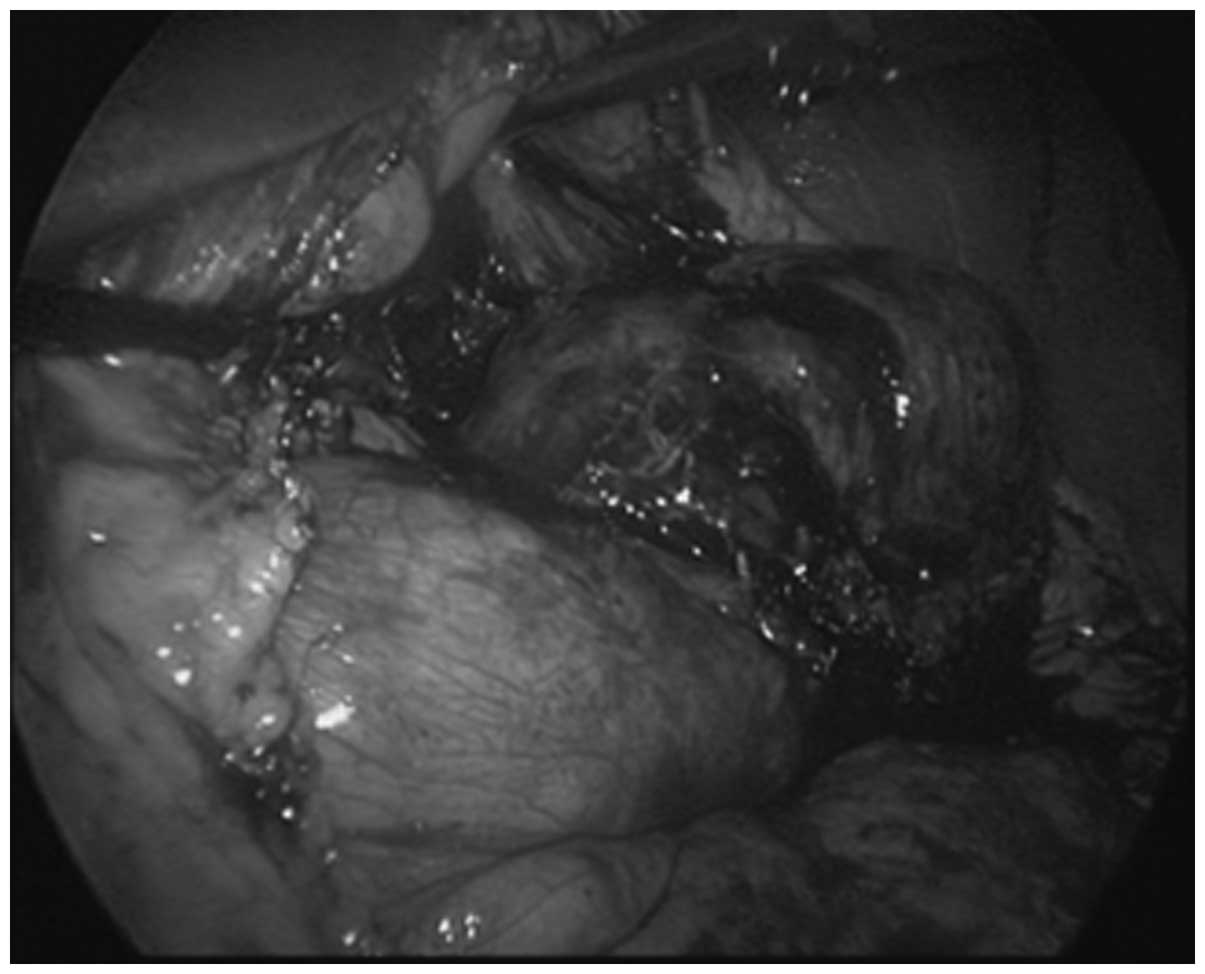
Exploratory laparoscopy was performed due to a
suspected pancreatic cystadenoma. A cystic tumor with intact peplos
was detected in the pancreatic tail (Fig. 2). As a consequence, the patient
underwent a laparoscopic spleen-preserving left pancreatectomy.
There were no post-operative complications, including
intra-abdominal bleeding or pancreatic fistula.
Histopathology
A histopathological analysis revealed that the
specimen consisted of a distal portion of the pancreas and the
mass, measuring 10×8×5 cm. The surface of the specimen was smooth
and sectioning of the pancreatic mass revealed a well-circumscribed
tumor with solid and multicystic components. The cut surface of the
solid area was grey/white and medium-hard.
HE staining
A large number of diffuse, abnormal cells were
identified by HE staining. Mitotic cells were common and duct-like
structures and small cystic formations were identified in specific
portions of the tumor. In addition, certain areas of the tumor
contained spindle cells with large, pleomorphic nuclei.
Multinucleated giant cells were also observed.
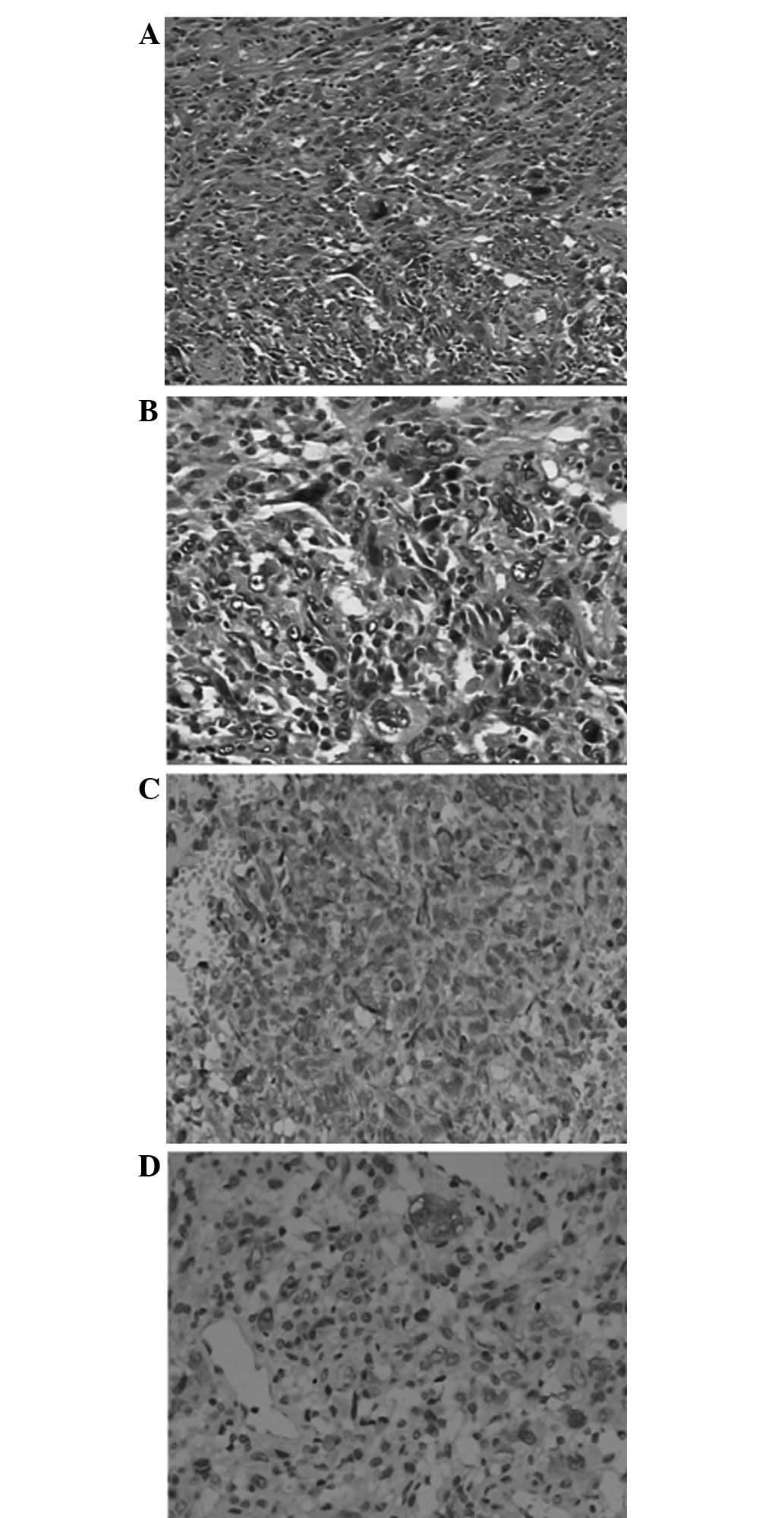
Immunohistochemistry
The adenocarcinoma component was markedly reactive
for antibodies against CK18 (++). The sarcomatous component was
negative for CK18 antibodies, but markedly reactive to vimentin
antibody (++; Fig. 3). Following
surgery, the patient received one cycle of chemotherapy with
gemcitabine, but succumbed to sarcomatoid carcinoma within three
months.
Discussion
Sarcomatoid carcinoma of the pancreas is a rare
neoplasm that contains carcinomatous and sarcomatous components, as
demonstrated by immunohistochemical reactivity to cytokeratin and
vimentin, respectively. In the present case, the tumor arose in the
body of the pancreas. A histological examination revealed a tumor
containing solid and multi-cystic components with a large number of
abnormal cells, including spindle-shaped and multinucleated giant
cells. Immunohistochemistry confirmed mixed adenocarcinoma and
sarcomatous components in the tumor. This type of tumor is
classified as a sarcomatoid carcinoma, according to the
classification by the World Health Organization (1).
The origin of truly mixed malignant carcinosarcoma
is unknown. Several theories have been hypothesized to explain the
characteristic biphasic appearance of this form of carcinosarcoma,
with histogenetic mechanisms involved in the coexistence of
carcinomatous and sarcomatous components in the same tumor. These
theories are known as the theories of ‘transformation,’
‘combination’ and ‘collision.’ ‘Transformation’ indicates that a
section of the carcinoma transforms into a sarcomatous element,
‘combination’ describes the development of a tumor from a single
stem cell that differentiates into epithelial and mesenchymal
tissues and ‘collision’ refers to the invasion of carcinomatous and
sarcomatous elements into each other. van den Berg et al
studied pancreatic mucinous cystic neoplasms with sarcomatous
stroma and identified that the two components of the
carcinosarcomas share a common clonal origin. These observations
indicated that the two components of the carcinosarcomas are
monoclonal neoplasms derived from a single stem cell (5).
The sarcomatous component of the tumor may vary.
Millis et al previously reported a case of carcinosarcoma
with leiomyosarcoma (4), which was
confirmed by immunoreactivity of the spindle cells for antibodies
against smooth muscle, vimentin and desmin. Sarcomatous components
have also been reported as malignant fibrous histiocytoma (3,6),
osteoclastic giant cell tumors (7,12,13)
and mucinous cystic neoplasms (14). Yamazaki et al (8) reported a primitive fibroblastic or
mesenchymal character without a specific differentiation
component.
Previous studies have reported an extremely poor
prognosis for pancreatic carcinosarcoma. Shen et al
(9) reported a carcinosarcoma of
the pancreas with liver metastasis combined with a gastrointestinal
stromal tumor of the stomach in a 72-year-old female. A radical
resection, including a pancreaticoduodenectomy, left hepatic lobe
resection and local resection, of the gastric mass was performed,
however, the patient succumbed to multiple organ failure at 2
months post-surgery. By contrast, in other cases, survival periods
of ≤20 months have been reported (10,11).
However, 6 months appears to be the most common period for survival
(4–7,14).
For pancreatic adenocarcinoma, a laparoscopic
pancreatectomy provides similar short- and long-term oncological
outcomes to open surgery (15). No
difference in surgical duration, margin positivity, incidence of
post-operative pancreatic fistula and mortality (16). Due to the small number of cases of
carcinosarcoma of the pancreas, a randomized control trial to
determine the efficacy of surgery for this condition has yet to be
performed. In addition, a standard chemotherapy protocol has not
been developed. The diagnosis of pancreatic carcinosarcoma remains
controversial. In the present case, prior to surgery, the patient
was diagnosed with suspected pancreatic cystadenoma as pancreatic
carcinosarcomas exhibit no characteristic symptoms or CT scan
results. It is extremely difficult to generate a correct
pre-operative diagnosis and therefore, in this case, a laparoscopic
exploration and resection was performed. Although, a negative
surgical margin was obtained, the tumor reoccurred and the patient
succumbed to sarcomatoid carcinoma within 3 months.
In summary, the current case study presents a case
of pancreatic carcinosarcoma confirmed by pathological and
immunohistochemical analysis. To the best of our knowledge, this is
the first report of a laparoscopic left pancreatectomy for
pancreatic carcinosarcoma. Although pancreatic carcinosarcoma is
rare, it must be considered in the differential diagnosis of a
pancreatic tumor. Despite the development of modern diagnostic
techniques, the formation of a pre-operative diagnosis remains
challenging and if in doubt, an analysis of intraoperative frozen
sections may be necessary to select the correct surgical
approach.
References
|
1.
|
Kloppel G, Solcia E, Longnecker DS,
Capella C and Sobin LH; World Health Organization: International
Histological Classification of Tumours. Histological Typing of the
Exocrine Pancreas. 2nd Edition. Springer-Verlag; Berlin: pp. 12–19.
1996
|
|
2.
|
Freeman AJ, Bullpitt P and Keogh GW:
Primary hepatic carcinosarcoma. ANZ J Surg. 74:1021–1023. 2004.
View Article : Google Scholar
|
|
3.
|
Tsujimura T, Kawano K, Taniguchi M,
Yoshikawa K and Tsukaguchi I: Malignant fibrous histiocytoma
coexistent with mucinous cystadenoma of the pancreas. Cancer.
70:2792–2796. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Millis JM, Chang B, Zinner MJ and Barsky
SH: Malignant mixed tumor (carcinosarcoma) of the pancreas: a case
report supporting organ-induced differentiation of malignancy.
Surgery. 115:132–137. 1994.PubMed/NCBI
|
|
5.
|
van den Berg W, Tascilar M, Offerhaus GJ,
et al: Pancreatic mucinous cystic neoplasms with sarcomatous
stroma: molecular evidence for monoclonal origin with subsequent
divergence of the epithelial and sarcomatous components. Mod
Pathol. 13:86–91. 2000.
|
|
6.
|
Darvishian F, Sullivan J, Teichberg S and
Basham K: Carcinosarcoma of the pancreas: a case report and review
of the literature. Arch Pathol Lab Med. 126:1114–1117.
2002.PubMed/NCBI
|
|
7.
|
Watanabe M, Miura H, Inoue H, et al: Mixed
osteoclastic/pleomorphic-type giant cell tumor of the pancreas with
ductal adenocarcinoma: histochemical and immunohistochemical study
with review of the literature. Pancreas. 15:201–208. 1997.
View Article : Google Scholar
|
|
8.
|
Yamazaki K: A unique pancreatic ductal
adenocarcinoma with carcinosarcomatous histology,
immunohistochemical distribution of hCG-beta, and the elevation of
serum alpha-feto-protein. J Submicrosc Cytol Pathol. 35:343–349.
2003.
|
|
9.
|
Shen ZL, Wang S, Ye YJ, et al:
Carcinosarcoma of pancreas with liver metastasis combined with
gastrointestinal stromal tumour of the stomach: is there a good
prognosis with the complete resection? Eur J Cancer Care (Engl).
19:118–123. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Gelos M, Behringer D, Philippou S and Mann
B: Pancreatic carcinosarcoma. Case report of multimodal therapy and
review of the literature. JOP. 9:50–55. 2008.PubMed/NCBI
|
|
11.
|
Zhu WY, Liu TG and Zhu H: Long-term
recurrence-free survival in a patient with pancreatic
carcinosarcoma: A case report with a literature review. Med Oncol.
29:140–143. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Fischer HP, Altmannsberger M and Kracht J:
Osteoclast-type giant cell tumour of the pancreas. Virchows Arch A
Pathol Anat Histopathol. 412:247–253. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Trepeta RW, Mathur B, Lagin S and LiVolsi
VA: Giant cell tumor (“osteoclastoma”) of the pancreas: a tumor of
epithelial origin. Cancer. 48:2022–2028. 1981.
|
|
14.
|
Bloomston M, Chanona-Vilchis J, Ellison
EC, Ramirez NC and Frankel WL: Carcinosarcoma of the pancreas
arising in a mucinous cystic neoplasm. Am Surg. 72:351–355.
2006.PubMed/NCBI
|
|
15.
|
Kooby DA, Hawkins WG, Schmidt CM, et al: A
multicenter analysis of distal pancreatectomy for adenocarcinoma:
is laparoscopic resection appropriate? J Am Coll Surg. 210:779–785.
786–787. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Venkat R, Edil BH, Schulick RD, Lidor AO,
Makary MA and Wolfgang CL: Laparoscopic distal pancreatectomy is
associated with significantly less overall morbidity compared to
the open technique: a systematic review and meta-analysis. Ann
Surg. 255:1048–1059. 2012. View Article : Google Scholar : PubMed/NCBI
|