Introduction
For early-stage (T1-2N0M0) glottic cancer,
radiotherapy (RT) and surgery have been demonstrated to yield
significant local disease control; >90% for T1 and 80% for T2.
RT is usually the preferred treatment modality, as it has shown a
trend towards improved post-treatment functional outcomes,
including voice quality, however, a prospective randomized trial
has not been performed (1).
Such favorable outcomes of RT have been achieved
using simple RT techniques of parallel-opposed lateral beams with
wedges or tissue compensators (2).
However, advanced RT techniques, including intensity-modulated RT
(IMRT) and volumetric modulated arc therapy (VMAT), have been
adopted rapidly for various head and neck cancers. By contrast, RT
techniques used for early-stage glottic cancer have not changed
considerably, possibly since the target volume is relatively small
and involves no elective nodal irradiation, with low rates of
severe toxicity (2,3). One previous study questioned the role
of IMRT in early-stage glottic cancer (4).
The carotid artery, which is located adjacent to the
larynx, is often overlooked, but has recently received attention in
several studies that have analyzed the use of advanced RT
techniques for patients with early-stage glottic cancer (5–10). RT
has emerged as a significant risk factor for carotid artery
stenosis and ischemic stroke in head and neck cancer patients
(11,12). The thyroid gland is also located
close to the larynx, and hypothyroidism is a late complication
frequently observed following RT to the head and neck region
(13–15). The lateral beams of conventional RT
pass through a cranial portion of the thyroid gland, however, to
date, no study has investigated the benefits of advanced RT
techniques regarding this organ in early-stage glottic cancer
patients.
The aim of the present study was to investigate the
dosimetric advantages of VMAT compared with conventional RT, in
terms of sparing the thyroid gland in patients with early stage
glottic cancer.
Materials and methods
Patients
A total of 15 patients with cT1N0M0 squamous cell
carcinoma of the larynx treated with definitive RT using VMAT
between 2011 and 2012 were selected. The staging workup included
direct laryngoscopy, computed tomography (CT) and
18F-fluorodeoxyglucose positron emission tomography. The
clinical stage was determined according to the American Joint
Committee on Cancer staging system, 7th edition
(16). All patients were male, with
a median age of 66 years (range, 55–76 years).
The patients were immobilized in the supine position
with a thermoplastic head and neck mask that included the shoulders
to ensure reproducibility of treatments. The planning CT scans were
performed using a 16-slice CT scanner (Brilliance CT Big Bore;
Philips Medical Systems, Cleveland, OH, USA) with a 0.2-cm slice
thickness. Intravenous contrast was used in all patients and all RT
plans were generated using the Eclipse treatment planning system
(Varian Medical Systems, Palo Alto, CA, USA). Treatment was
conducted using a Novalis® Tx system (Varian Medical
Systems, Palo Alto, CA, USA and BrainLab, Feldkirchen, Germany) and
patient set-up was verified prior to treatment; daily by
ExacTrac® (BrainLab) and weekly by cone-beam CT.
Patients provided written informed consent.
RT planning
The clinical target volume included the false and
true vocal cords, the anterior and posterior commissure, the
arytenoids and the subglottic region, extending from the superior
thyroid notch to the bottom of the cricoid cartilage. No cervical
lymph nodes were included electively. The planning target volume
(PTV) was produced by the addition of a 0.5-cm isotropic set-up
margin surrounding the clinical target volume. The PTV was
truncated within 0.5 cm of the skin surface in the patients without
anterior commissure involvement. The surrounding organs at risk
(OARs), including the carotid artery, whole thyroid gland and
spinal cord, were delineated. The right and left common, internal
and external carotid arteries were contoured starting from the
sternoclavicular joints and extending upward to the base of the
skull.
For the purpose of comparison, a conventional RT
plan was retrospectively generated for each patient, using two
opposed-lateral wedged fields. The wedge angle was selected to
achieve the most homogeneous dose distribution in the PTV, and the
block edge margin was uniformly 0.5 cm around the PTV. The
collimator of the Novalis® Tx system was angled such
that the posterior jaw of the lateral fields was parallel to the
cervical spine, and two fields were optimally weighted to provide
adequate PTV coverage.
For VMAT, the double-arc plan, which has been
previously recommended for locally advanced head and neck cancers
due to its higher PTV homogeneity, was selected (17). The arc length or gantry span of each
arc was adjusted to avoid the OARs where possible. The collimator
was rotated to 45° or 315° to minimize the contribution of the
tongue-and-groove effect during treatment. Optimizations were
performed by interactively adapting the objectives and their
priorities to ensure lower doses to the OARs and to improve PTV
coverage and homogeneity. Following optimization, the dose
calculation was performed using the anisotropic analytical
algorithm and Eclipse dose volume optimizer (version 8.9.17; Varian
Medical Systems, Palo Alto, CA, USA). All conventional and VMAT
plans were generated using 6-MV photons and a high-definition
multileaf collimator consisting of 120 leaves, which included 64
2.5-mm central and 56 5-mm peripheral leaves. The prescription dose
was 63 Gy at 2.25 Gy per fraction and all plans were normalized so
that ≥95% of the PTV received 100% of the prescription dose.
Statistical analysis
Dose-volume histograms (DVHs) were created for all
treatment plans, and specific dose-volume parameters were compared
for the PTV, thyroid gland, carotid artery and spinal cord. For the
PTV, the minimum dose (Dmin), maximum dose
(Dmax), mean dose (Dmean) and volume
receiving ≥105% of the prescription dose (V105) were
compared to evaluate PTV coverage and dose homogeneity. For the
OARs, the following parameters were compared: Dmean,
V30 and V50 for the thyroid gland;
Dmean, V35 and V50 for the carotid
artery; and Dmax for the spinal cord. Comparisons
between the dosimetric parameters were performed using the
non-parametric Wilcoxon signed-rank test. All statistical tests
were two-sided and performed using SPSS software (version 14.0;
SPSS, Inc., Chicago, IL, USA). P<0.05 was considered to indicate
a statistically significant difference.
Results
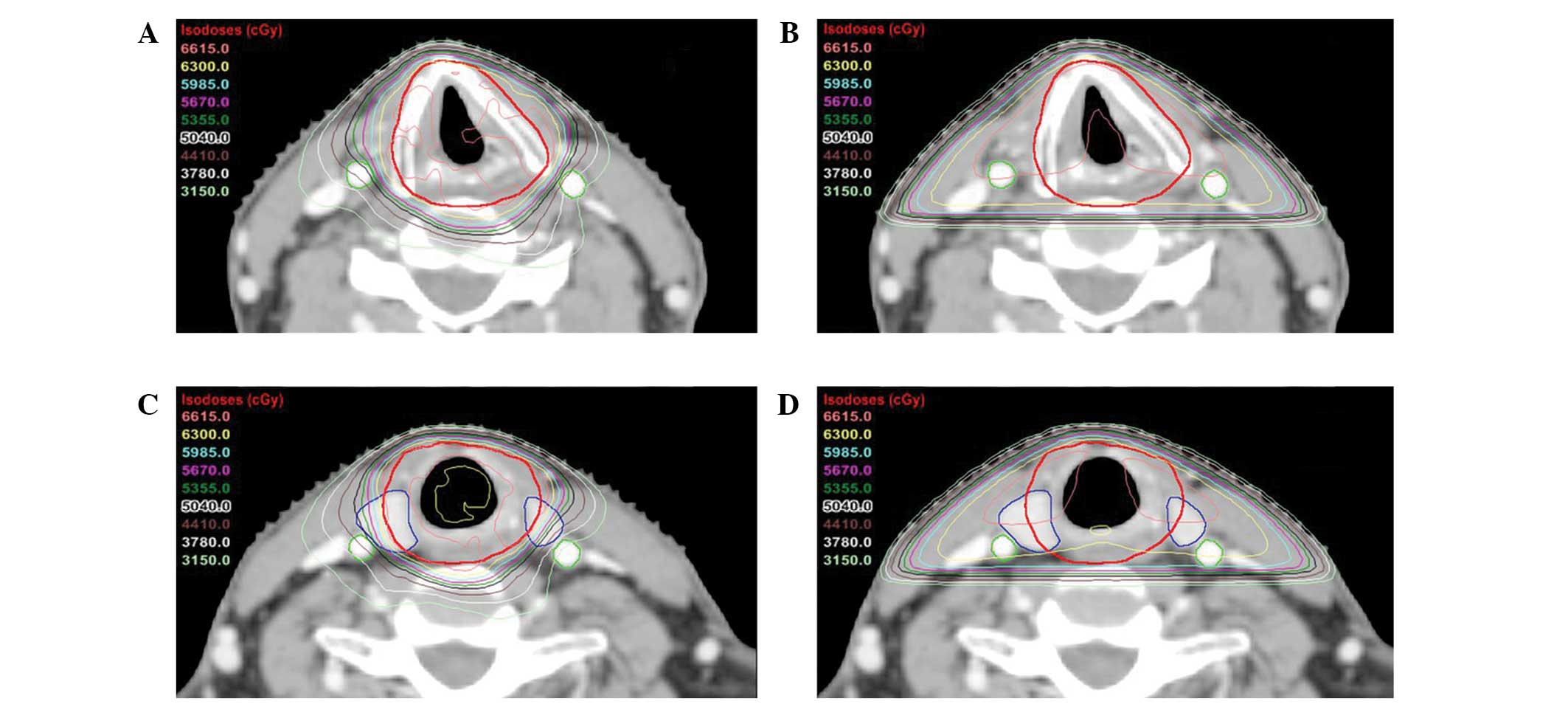
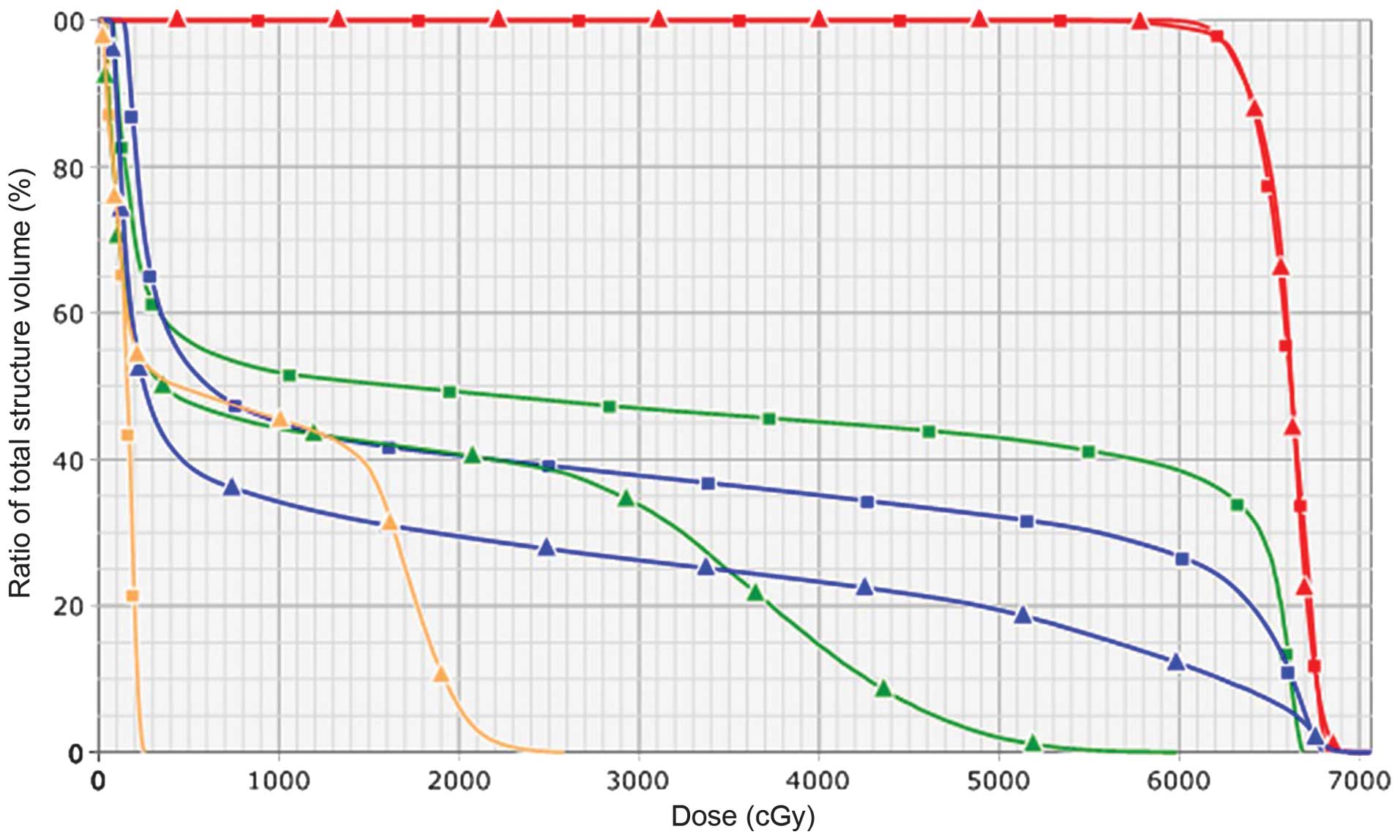
Figs. 1 and 2 show the isodose distributions and DVHs,
respectively, according to the RT plan, and Table I shows the dose-volume data for the
PTV. For the PTV, no differences were identified in the
Dmin or Dmean between VMAT and conventional
RT. The median Dmin and Dmean values were
51.0 Gy (80.9% of the prescription dose) and 62.7 Gy (99.5% of the
prescription dose) in VMAT, respectively, and 52.3 Gy (83.0%) and
62.8 Gy (99.7%) in conventional RT, respectively. The
Dmax of VMAT tended to be higher when compared with the
Dmax of the conventional RT (P=0.074), and the median
Dmax values were 66.6 Gy (105.7%) and 65.7 Gy (104.3%)
for VMAT and conventional RT, respectively. However,
V105 was not significantly different between the two
plans.
 | Table IComparison of the PTV dosimetric
parameters between VMAT and conventional RT (n=15). |
Table I
Comparison of the PTV dosimetric
parameters between VMAT and conventional RT (n=15).
| Parameters | VMAT, mean ± SD
(range) | Conventional RT, mean
± SD (range) | P-valuea |
|---|
| Dmin,
Gy | 50.0±2.6
(45.1–52.9) | 51.6±4.2
(45.2–56.8) | 0.214 |
| Dmax,
Gy | 66.8±1.3
(65.4–70.1) | 65.7±0.6
(64.9–66.5) | 0.074 |
| Dmean,
Gy | 62.8±0.6
(62.1–64.5) | 62.8±0.4
(62.0–63.3) | 0.236 |
| V105,
% | 1.7±5.4
(0.0–17.0) | 0.005±0.01
(0.0–0.05) | 0.116 |
Table II shows the
dose-volume data for the OARs. For the thyroid gland and carotid
artery, all compared parameters were significantly lower in VMAT
than in conventional RT. In the thyroid gland, the median reduction
rates of the Dmean, V30 and V50
using VMAT were 32.6% (range, 26.5–46.0%), 40.9% (range,
30.7–45.5%) and 46.0% (range, 38.4–67.2%), respectively. In the
carotid artery, the median reduction rates of the Dmean,
V35 and V50 using VMAT were 45.9% (range,
37.0–50.4%), 49.0% (range, 45.0–52.5%) and 92.5% (range,
89.1–100%), respectively.
| Table IIComparison of the OAR dosimetric
parameters between VMAT and conventional RT (n=15). |
Table II
Comparison of the OAR dosimetric
parameters between VMAT and conventional RT (n=15).
| Parameters | VMAT, mean ± SD
(range) | Conventional RT, mean
± SD (range) | P-valuea |
|---|
| Thyroid gland |
| Dmean,
Gy | 14.7±2.6
(10.2–18.0) | 22.2±3.9
(15.8–26.5) | <0.01 |
| V30,
% | 19.2±4.0
(12.0–26.2) | 31.7±6.2
(21.5–37.8) | <0.01 |
| V50,
% | 13.8±3.8
(8.0–19.4) | 26.7±5.9
(17.0–32.6) | <0.01 |
| Carotid artery |
| Dmean,
Gy | 15.7±3.1
(10.6–20.2) | 28.8±6.9
(16.8–39.9) | <0.01 |
| V35,
% | 21.1±6.4
(11.6–32.3) | 41.1±10.5
(24.1–58.7) | <0.01 |
| V50,
% | 2.8±2.0
(0.0–6.0) | 38.2±10.2
(22.0–55.2) | <0.01 |
| Spinal cord |
| Dmax,
Gy | 29.8±1.9
(25.9–33.0) | 3.3±0.8
(2.1–4.8) | <0.01 |
The measured volume of the entire thyroid gland
ranged between 7.4 and 21.9 cm3 (median, 14.9
cm3). A portion of thyroid gland volume, which was
encompassed by lateral beams of conventional RT, ranged between
2.5–7.6 cm3 (median, 4.4 cm3); on average, it
was 32.8% (range, 25.2–40.9%) of the entire thyroid gland
volume.
Discussion
The partial volume effects between the thyroid gland
and hypothyroidism were unclear in the study by Emami et al
(18), which was based on a simple
consensus of clinical experience or opinions, with little
high-quality clinical data. In addition, the Quantitative Analysis
of Normal Tissue Effects in the Clinic reports (19) did not include data concerning the
thyroid gland. Recently, a normal tissue complication probability
(NTCP) model of radiation-induced hypothyroidism has been developed
based on a prospective multivariate analysis (20). The probability of hypothyroidism
increases with a higher Dmean of the thyroid gland (odds
ratio, 1.064/Gy) and decreases with a higher thyroid gland volume
(odds ratio, 0.826/cm3), indicating that the
Dmean must be minimized (20). In the present study, VMAT exhibited
a median 32.6% reduction in the Dmean of the thyroid
gland compared with conventional RT. In addition, the absolute
reduction of the Dmean was a median of 8.0 Gy (range,
4.6–11.1 Gy). Therefore, the VMAT used for early-stage glottic
cancer patients may reduce the post-RT risk of developing
hypothyroidism, when applying this NTCP model.
Hypothyroidism is a late toxicity that frequently
occurs following curative RT to the head and neck region. The
incidence of subclinical (high serum thyrotropin) and clinical
(high serum thyrotropin and thyroxine) hypothyroidism following RT
to the head and neck region varies between 23 and 53% and 11 and
33%, respectively (15). These
values are much higher than those observed in a normal population,
in which the prevalence of subclinical hypothyroidism is ~8% in
females and ~3% in males, and where the prevalence of clinical
hypothyroidism varies between 1% and 2% (21). Observation of the thyroid gland
using ultrasonography during RT has identified vessel changes,
which have been indicated to be associated with late radiation
effects on this organ (22).
Hypothyroidism is known to develop following a median interval of
1.4–1.8 years, causing a progressively deteriorating quality of
life with various clinical symptoms, including, fatigue, weakness,
cold intolerance, weight gain, constipation and depression
(13,14).
In a study involving only early-stage glottic cancer
patients, the post-RT rates of subclinical and clinical
hypothyroidism were reported to be 24 and 6%, respectively
(23). These rates do not appear to
be low considering their relatively small target volume involving
no neck node irradiation. Conventional RT consists of
opposed-lateral beams to primarily avoid the spinal cord, however,
it exposes a certain proportion of the thyroid gland (32.8% on
average in the present study) to high radiation doses almost
identical to that of the target. To the best of our knowledge, the
present study is the first to contour and restrict the dose not
only to the carotid artery, but also to the thyroid gland, and
revealed the dosimetric benefits of the advanced RT technique in
terms of sparing the two organs. A small increase in the
Dmax of the PTV with VMAT may affect larynx function
(7), however, the V105
was not significantly different between the two techniques. The
spinal cord dose was increased, but remained within the recommended
tolerable range.
Through acceleration of the atherosclerotic process
of the carotid artery, RT may increase the risk of ischemic stroke
in head and neck cancer patients (24). The actuarial incidences of
cerebrovascular events at 10 years after definitive RT and surgery
have been reported as 34% and 26%, respectively (P<0.001)
(12). When only the early-stage
glottic cancer patients are assessed, RT is also associated with an
increased risk of fatal cerebrovascular events compared with
surgery, with a cumulative incidence at 15 years of 2.8 versus 1.5%
(P=0.024) (25). The results of the
present study indicated that VMAT significantly decreases the dose
to the carotid artery, which is consistent with previous dosimetric
studies of IMRT or VMAT in early-stage glottic cancer (5–10). A
total of 35 Gy has been indicated as the threshold for intima media
thickness and wall abnormalities of the carotid artery (26). In the present study, the
V35 was reduced by almost half (49%) with VMAT. An
additional radiation-related carotid toxicity is carotid blowout
syndrome, a rare but devastating complication following
reirradiation of the head and neck region for recurrence or a
second malignancy (27). Therefore,
it is important to minimize the unnecessary dose to the carotid
artery during initial treatment.
In conclusion, compared with conventional RT, VMAT
yields significantly improved dose-volume parameters of the thyroid
gland and carotid artery, with no differences in target coverage or
homogeneity. Considering the NTCP model for radiation-induced
hypothyroidism (20), not only the
carotid artery, but also the thyroid gland must be contoured and
protected as an avoidance structure during advanced RT planning for
early-stage glottic cancer. Considering the high rates of tumor
control and the long-term survival of patients, favorable
dosimetric features of organs associated with late-manifesting
toxicities may be valuable.
Acknowledgements
This study was supported by the Soonchunhyang
University Research Fund.
References
|
1
|
Higgins KM, Shah MD, Ogaick MJ and
Enepekides D: Treatment of early-stage glottic cancer:
meta-analysis comparison of laser excision versus radiotherapy. J
Otolaryngol Head Neck Surg. 38:603–612. 2009.PubMed/NCBI
|
|
2
|
Khan MK, Koyfman SA, Hunter GK, Reddy CA
and Saxton JP: Definitive radiotherapy for early (T1-T2) glottic
squamous cell carcinoma: a 20 year Cleveland clinic experience.
Radiat Oncol. 7:1932012.PubMed/NCBI
|
|
3
|
Mendenhall WM, Amdur RJ, Morris CG and
Hinerman RW: T1-T2N0 squamous cell carcinoma of the glottic larynx
treated with radiation therapy. J Clin Oncol. 19:4029–4036.
2001.PubMed/NCBI
|
|
4
|
Feigenberg SJ, Lango M, Nicolaou N and
Ridge JA: Intensity-modulated radiotherapy for early larynx cancer:
is there a role? Int J Radiat Oncol Biol Phys. 68:2–3. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gomez D, Cahlon O, Mechalakos J and Lee N:
An investigation of intensity-modulated radiation therapy versus
conventional two-dimensional and 3D-conformal radiation therapy for
early stage larynx cancer. Radiat Oncol. 5:742010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rosenthal DI, Fuller CD, Barker JL Jr, et
al: Simple carotid-sparing intensity-modulated radiotherapy
technique and preliminary experience for T1-2 glottic cancer. Int J
Radiat Oncol Biol Phys. 77:455–461. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chera BS, Amdur RJ, Morris CG and
Mendenhall WM: Carotid-sparing intensity-modulated radiotherapy for
early-stage squamous cell carcinoma of the true vocal cord. Int J
Radiat Oncol Biol Phys. 77:1380–1385. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Atalar B, Gungor G, Caglar H, Aydin G,
Yapici B and Ozyar E: Use of volumetric modulated arc radiotherapy
in patients with early stage glottic cancer. Tumori. 98:331–336.
2012.PubMed/NCBI
|
|
9
|
Camingue P, Christian R, Ng D, Williams P,
Amin M and Roniger DL: Comparison of external beam treatment
techniques for T1-2, N0, M0 glottic cancers. Med Dosim. 37:221–224.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Riegel AC, Antone J and Schwartz DL:
Comparative dosimetry of volumetric modulated arc therapy and
limited-angle static intensity-modulated radiation therapy for
early-stage larynx cancer. Med Dosim. 38:66–69. 2013.
|
|
11
|
Dorresteijn LD, Kappelle AC, Boogerd W, et
al: Increased risk of ischemic stroke after radiotherapy on the
neck in patients younger than 60 years. J Clin Oncol. 20:282–288.
2002.PubMed/NCBI
|
|
12
|
Smith GL, Smith BD, Buchholz TA, et al:
Cerebrovascular disease risk in older head and neck cancer patients
after radiotherapy. J Clin Oncol. 26:5119–5125. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mercado G, Adelstein DJ, Saxton JP, Secic
M, Larto MA and Lavertu P: Hypothyroidism: a frequent event after
radiotherapy and after radiotherapy with chemotherapy for patients
with head and neck carcinoma. Cancer. 92:2892–2897. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tell R, Lundell G, Nilsson B, Sjödin H,
Lewin F and Lewensohn R: Long-term incidence of hypothyroidism
after radiotherapy in patients with head-and-neck cancer. Int J
Radiat Oncol Biol Phys. 60:395–400. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Boomsma MJ, Bijl HP and Langendijk JA:
Radiation-induced hypothyroidism in head and neck cancer patients:
a systematic review. Radiother Oncol. 99:1–5. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual. 7th edition.
Springer; New York, NY: 2010
|
|
17
|
Verbakel WF, Cuijpers JP, Hoffmans D,
Bieker M, Slotman BJ and Senan S: Volumetric intensity-modulated
arc therapy vs. conventional IMRT in head-and-neck cancer: a
comparative planning and dosimetric study. Int J Radiat Oncol Biol
Phys. 74:252–259. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Emami B, Lyman J, Brown A, et al:
Tolerance of normal tissue to therapeutic irradiation. Int J Radiat
Oncol Biol Phys. 21:109–122. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Marks LB, Yorke ED, Jackson A, et al: Use
of normal tissue complication probability models in the clinic. Int
J Radiat Oncol Biol Phys. 76(Suppl 3): S10–S19. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Boomsma MJ, Bijl HP, Christianen ME, et
al: A prospective cohort study on radiation-induced hypothyroidism:
development of an NTCP model. Int J Radiat Oncol Biol Phys.
84:e351–e356. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vanderpump MP and Tunbridge WM:
Epidemiology and prevention of clinical and subclinical
hypothyroidism. Thyroid. 12:839–847. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bakhshandeh M, Hashemi B, Mahdavi SR,
Nikoofar A, Edraki HR and Kazemnejad A: Evaluation of thyroid
disorders during head-and-neck radiotherapy by using functional
analysis and ultrasonography. Int J Radiat Oncol Biol Phys.
83:198–203. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kumar S, Moorthy R, Dhanasekar G, Thompson
S and Griffiths H: The incidence of thyroid dysfunction following
radiotherapy for early stage carcinoma of the larynx. Eur Arch
Otorhinolaryngol. 268:1519–1522. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gianicolo ME, Gianicolo EA, Tramacere F,
Andreassi MG and Portaluri M: Effects of external irradiation of
the neck region on intima media thickness of the common carotid
artery. Cardiovasc Ultrasound. 8:82010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Swisher-McClure S, Mitra N, Lin A, et al:
Risk of fatal cerebrovascular accidents after external beam
radiation therapy for early stage glottic larynx cancer. Head Neck.
Apr 18–2013.(Epub ahead of print). View Article : Google Scholar
|
|
26
|
Martin JD, Buckley AR, Graeb D, Walman B,
Salvian A and Hay JH: Carotid artery stenosis in asymptomatic
patients who have received unilateral head-and-neck irradiation.
Int J Radiat Oncol Biol Phys. 63:1197–1205. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
McDonald MW, Moore MG and Johnstone PA:
Risk of carotid blowout after reirradiation of the head and neck: a
systematic review. Int J Radiat Oncol Biol Phys. 82:1083–1089.
2012. View Article : Google Scholar : PubMed/NCBI
|