Introduction
Medication adherence is often defined as follows:
Subsequent to sufficient explanation of the effects and
side-effects of medication, the patient agrees to be treated with
the medication, understands the significance of the medication and
continues to take the medication voluntarily (1). By contrast, the conventionally used
definition of medication compliance refers to the patient taking
medication in the amount and at the times directed by pharmacists
and physicians. Cancer treatment through oral anticancer agents has
the advantage of ease of delivery, but since medication management
is left to the family or patient, medication adherence can be a
problem. It is important that the patient understands the effects
of the prescribed drugs, the side-effects and the methods to
assuage these, and that they also understand that medication
adherence can lead to effective treatment, safety and continuity in
cancer chemotherapy. A lack of medication adherence can decrease
treatment efficiency, change the seriousness of the side-effects
and increase the number of hospitalizations and doctor visits, all
of which can lead to higher medical costs (2,3).
Therefore, the improvement of medication adherence is an important
component in cancer treatment.
Patients who are diagnosed with cancer are generally
observed as having strong reasons for adhering to treatment, as a
lack of adherence could lead to serious side-effects, cancer
relapse or mortality. Despite the serious effects of non-adherence,
previous studies have indicated that the medication adherence rate
in cancer patients is not 100% (4–8).
Research into medication adherence in patients
taking oral anticancer agents has generally focused on a specific
disease, such as chronic myeloid leukemia (CML) or breast cancer,
and the disease-specific medicine (4–8). At
present, neither the adherence to tegafur/gimeracil/oteracil
potassium (S-1) and multiple tyrosine kinase inhibitors nor the
level of consciousness behind non-adherence or non-compliance has
been examined. Therefore, a questionnaire survey was conducted to
evaluate the factors that affect medication adherence in patients
taking oral anticancer agents. The results of the survey were
explored using a customer satisfaction (CS) analysis.
Materials and methods
Participants
The participants in the present study were
outpatients undergoing treatment with oral anticancer agents at
Ogaki Municipal Hospital (Ogaki, Gifu, Japan) in June 2013. A
self-report questionnaire survey was administered to these
patients, and those who had difficulty reading or writing were
assisted. The questionnaires were distributed to 182 individuals.
The return rate for the questionnaires was 94.5% (172 out of
182).
The present study was approved by the Institutional
Review Board of Ogaki Municipal Hospital and was explained in a
handout distributed to participants prior to obtaining their
informed consent.
Measures
Questionnaire survey items
The questionnaire items are shown in Table I. The survey items included:
Medication adherence (six items total), with one item each for the
dosing method, effect of drugs, side-effects, understanding of the
treatment method, treatment policy and compliance; personality
(three items); and factors potentially affecting adherence, namely,
the living environment (one item), awareness of medication dosage
(three items), knowledge of the drug (six items), daily schedule
(two items), understanding of the disease (one item), sense of
trust (two items), expectations and attitude (two items) and
condition (one item). The participants were instructed to include
all currently prescribed medications in one of the dosing method
questions.
 | Table IQuestionnaire. |
Table I
Questionnaire.
A questionnaire
relating to taking your medication
Please answer the following questions by indicating the answers
which apply to you (please circle the number or position which
applies to you) |
|---|
|
|---|
| Question | Yes | I think so | I cannot say either
way | I do not think
so | No |
|---|
| 1. I understand how
to take the medication | 5 | 4 | 3 | 2 | 1 |
| 2. I know the effect
(efficacy) of the medication | 5 | 4 | 3 | 2 | 1 |
| 3. I know the side
effects of the medication | 5 | 4 | 3 | 2 | 1 |
| 4. I understand the
current therapy | 5 | 4 | 3 | 2 | 1 |
| 5. I agree with the
current treatment policy | 5 | 4 | 3 | 2 | 1 |
| 6. I have forgotten
to take the medication or I have mistakenly taken the
medication | Never | Rarely | I cannot say either
way | Occasionally | Often |
| 7. Currently, what is
the composition of your household? | I live alone | Husband and wife | Other |
| 8. I take care not to
forget my medication | 5 | 4 | 3 | 2 | 1 |
| 9. I think I take a
lot of medications | 5 | 4 | 3 | 2 | 1 |
| 10. Dosing times are
complicated or awkward | 5 | 4 | 3 | 2 | 1 |
| 11. The current
treatment costs (prescription charges) are an economic burden | 5 | 4 | 3 | 2 | 1 |
| 12. I believe the
medication is necessary for me | 5 | 4 | 3 | 2 | 1 |
| 13. I believe the
medication is effective | 5 | 4 | 3 | 2 | 1 |
| 14. I have actively
researched about my medication | 5 | 4 | 3 | 2 | 1 |
| 15. I worry about
side effects | 5 | 4 | 3 | 2 | 1 |
| 16. I would like to
talk to someone further about the medication | 5 | 4 | 3 | 2 | 1 |
| 17. I have a regular
daily schedule | 5 | 4 | 3 | 2 | 1 |
| 18. I eat regular
meals | 5 | 4 | 3 | 2 | 1 |
| 19. I am
methodical | 5 | 4 | 3 | 2 | 1 |
| 20. I am a
worrier | 5 | 4 | 3 | 2 | 1 |
| 21. I tend to find
things bothersome | 5 | 4 | 3 | 2 | 1 |
| 22. I have a good
understanding of my disease | 5 | 4 | 3 | 2 | 1 |
| 23. I trust the
attending physician | 5 | 4 | 3 | 2 | 1 |
| 24. I trust the
pharmacist | 5 | 4 | 3 | 2 | 1 |
| 25. I hope that the
medication is valuable in curing the disease or that it will be
able to improve my quality of life | 5 | 4 | 3 | 2 | 1 |
| 26. I have a positive
attitude towards the disease | 5 | 4 | 3 | 2 | 1 |
| 27. What is your
general condition (health)? | Very good | Good | Average | Bad | Very bad |
|
| Thank you for your
cooperation |
The survey items were rated on a five-point Likert
scale, with 5 being ‘Yes’, 4 being ‘I think so’, 3 being ‘I cannot
say either way’, 2 being ‘I do not think so’ and 1 being ‘No’.
Items 9–11 were reverse-scored.
Using the scores on the medication adherence scale
of the questionnaire, the participants were divided into two
groups: The ‘good medication adherence’ group, consisting of those
who adhered to medication regimens, with a score ≥4 on all items;
and the ‘insufficient medication’ group, which consisted of those
who did not adhere, classified as participants who scored ≤3 on all
items. The scores across the two groups were compared for each
variable. All data, including the evaluation score value, the
number of drugs taken and the dosing time, are presented as the
median value within the range.
Evaluation of medication adherence by
CS analysis
CS object variable analysis was performed with the
lowest point for each item in medication adherence in order to
investigate adherence factors, and the questions associated with
the factors that potentially affected medication adherence were
analyzed to determine an explanatory variable. For the questions
associated with the factors that potentially affected medication
adherence, CS analysis was performed with the items that possessed
significant differences between the good and insufficient
groups.
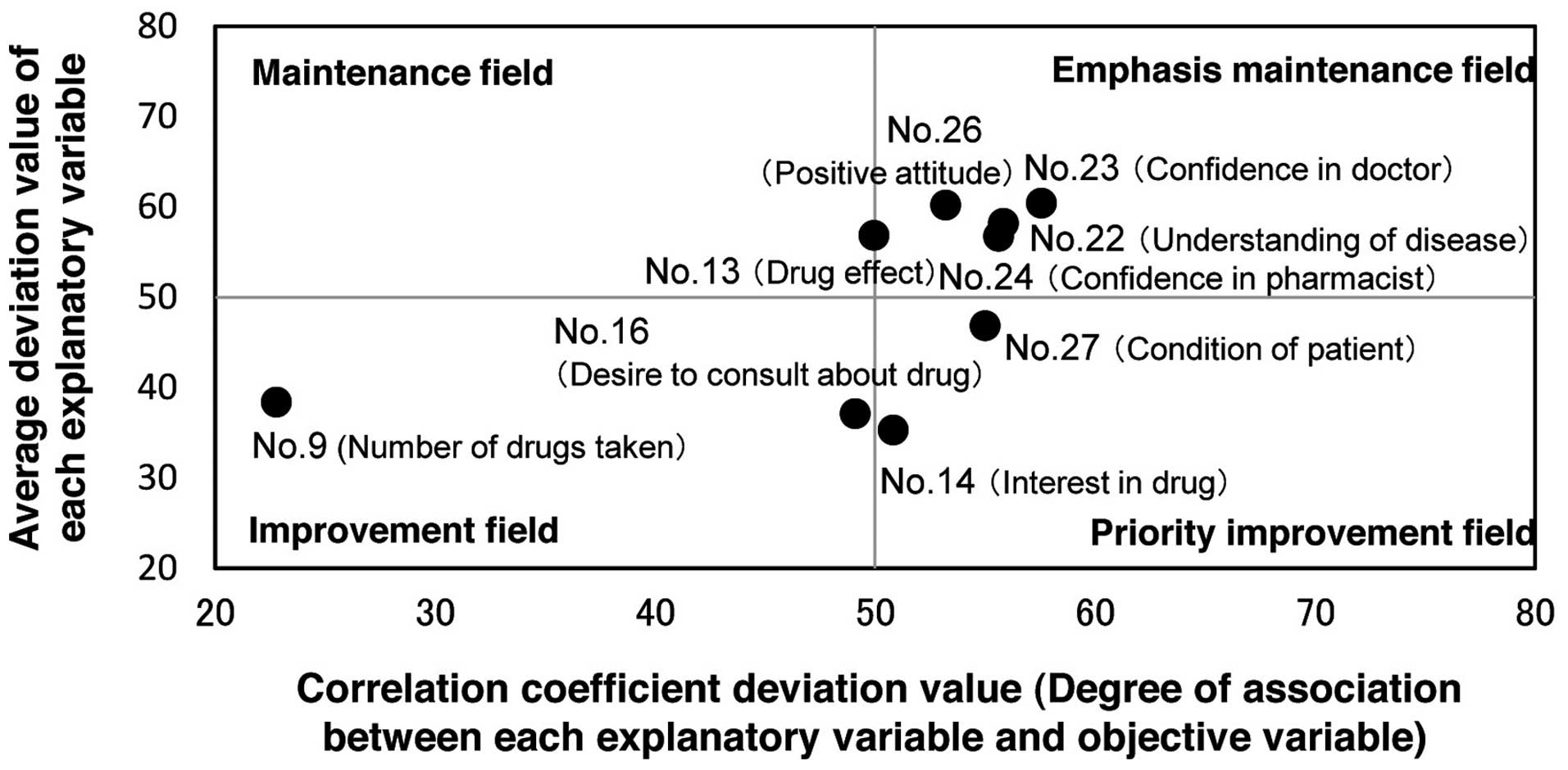
The CS analysis graph was plotted on two-dimensional
coordinates. The average deviations of the scores for each item on
the questionnaire were plotted on the vertical axis of the CS
analysis graph, while the association value (correlation
coefficient deviation value) between adherence factors and the
individual evaluation was plotted on the horizontal axis. In the CS
analysis graph, factors with a high score and a high degree of
influence on adherence are plotted in the first quadrant, termed
the emphasis maintenance field. Factors with a high score and low
degree of influence on adherence are plotted in the second
quadrant, termed the maintenance field. Factors with a low score
and low degree of influence on adherence are plotted in the third
quadrant, termed the improvement field, and factors with a low
score and high degree of influence on adherence are plotted in the
fourth quadrant, termed the priority improvement field. The CS
analysis improvement degree for each question was calculated. This
degree is an index indicating the magnitude of the effect a factor
has on adherence. If the CS analysis improvement degree is
positive, improvement is required in the items with a score of five
points or greater. Conversely, a negative CS analysis improvement
degree would indicate that improvement is not necessary.
Statistical analysis
The Mann-Whitney U test was used to compare the two
groups. In all statistical tests, P<0.05 was considered to
indicate a statistically significant difference. For the CS
analysis, the statistical software, EXCEL® Quality
Management (Esumi Co., Ltd., Tokyo, Japan), was used.
Results
Drugs
The drugs represented in the current study and the
number of patients taking those drugs were S-1 (n=83), capecitabine
(n=26), molecularly-targeted drugs, such as sorafenib (n=45),
tegafur-uracil combination (n=10) and other drugs, including
cyclophosphamide, mercaptopurine and hydroxycarbamide (n=10).
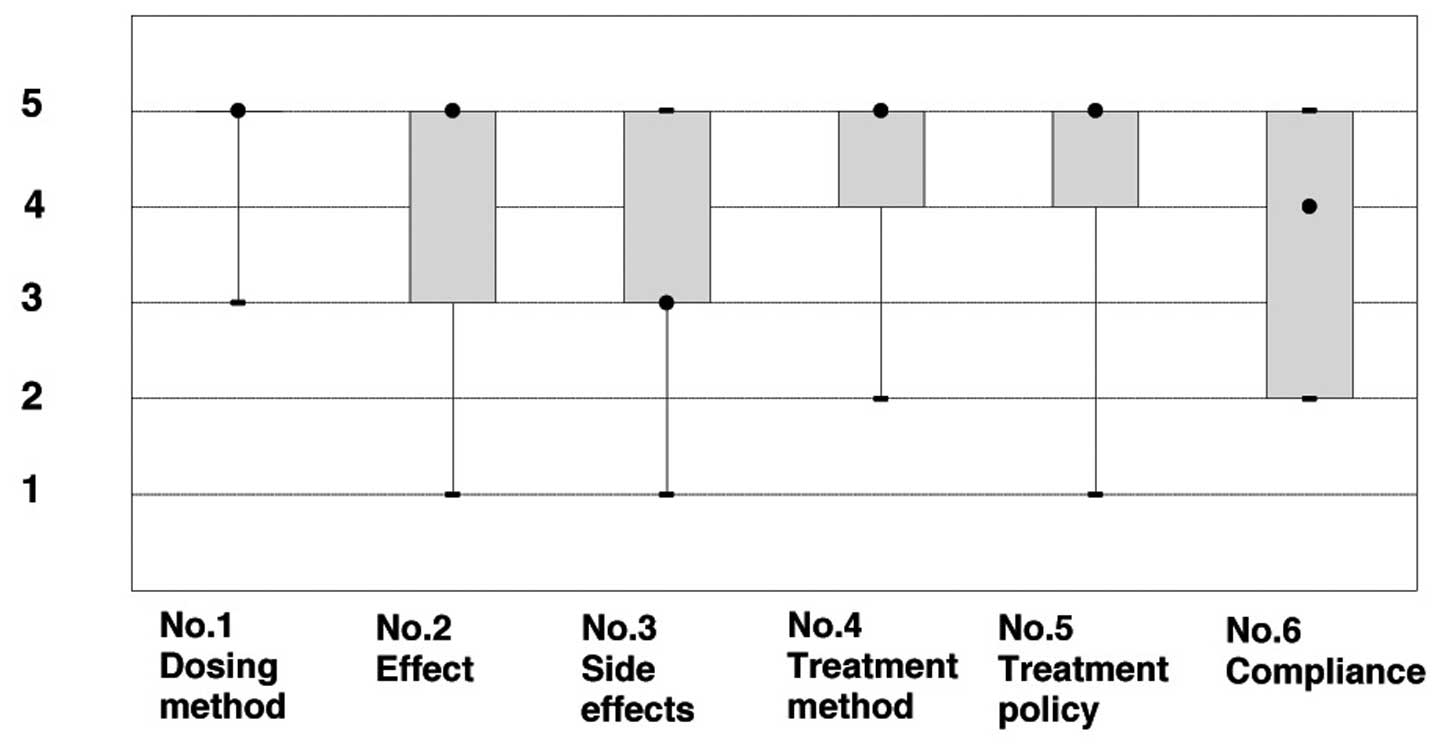
Evaluation of medication adherence
Good medication adherence was found for 64.0% of the
patients (110 out of 172). The scores of the patients with
insufficient adherence to medication are shown in Fig. 1. The scores [median (range)] were
5.0 (3.0–5.0) for the dosing method, 5.0 (1.0–5.0) for the effect
of the drug, 3.0 (1.0–5.0) for the side-effects, 5.0 (2.0–5.0) for
the understanding of the treatment method, 5.0 (1.0–5.0) for the
treatment policy and 4.0 (2.0–5.0) for compliance.
In 36.0% (62 out of 172) of the cases, there was
insufficient medication adherence. However, 64.5% of those cases
(40 out of 62) had good medication compliance, with a score of 4–5
points. It is likely that these patients did not fully understand
the effects of the drugs or side-effects, giving a score of three
points or less on these items. However, the percentage of patients
with good medication compliance was 87.2% (150 out of 172).
Evaluation of patient demographic factors
that affect medication adherence
The patient demographics that potentially affected
medication adherence are shown in Table II. Patients with good and
insufficient adherence to medication had a median age of 66 years
(range, 21–85 years) and 73 years (range, 30–90 years),
respectively (P=0.0004). The median number of drugs taken was four
for each group (good adherence range, 1–10 drugs; insufficient
adherence range, 1–14 drugs; P=0.0401) and the length of time on
the medication was 131 days (range, 3–3,585 days) in the good
adherence to medication group and 219 days (24–3,465 days)
(P=0.0447) in the insufficient adherence group.
| Table IIScore of patient attribute factors
that affect medication adherence. |
Table II
Score of patient attribute factors
that affect medication adherence.
| Medication
adherence | |
|---|
|
| |
|---|
| Factor | Good (n=109) | Insufficient
(n=62) | P-value |
|---|
| Age, yearsa | 66 (21–85) | 73 (30–90) | 0.0004 |
| Gender, n | | | 0.7249 |
| Male | 60 | 34 | |
| Female | 49 | 28 | |
| Number of drugs taken
(range)a,b | 4 (1–10) | 4 (1–14) | 0.0401 |
| Dosing time, days
(range)a | 131 (3–3585) | 219 (24–3465) | 0.0447 |
| Stage, n | | | 0.6609 |
| Adjuvant | 29 | 19 | |
| Progressive | 80 | 43 | |
| Family, n | | | 0.5692 |
| Living alone | 96 | 54 | |
| Other | 13 | 8 | |
Evaluation of factors that affect
medication adherence
The scores associated with factors that affected
medication adherence are shown in Table III. For patients with good or
insufficient adherence to medication, there were significant
differences (P<0.05) in nine items on the following subscales:
Awareness of dosing (one out of three items), awareness about the
drug (three out of six items), understanding the disease (one out
of one item), sense of trust (two out of two items), expectations
and attitudes (one out of two items) and the condition of the
patient (one out of one item).
| Table IIIScore of factors that affect
medication adherence. |
Table III
Score of factors that affect
medication adherence.
| | | Median medication
adherence score (range) | |
|---|
| | |
| |
|---|
| Topic | Question
number | Question | Good (n=109) | Insufficient
(n=62) | P-value |
|---|
| Living
environment | 7 | Currently, what is
the composition of your household? | 2 (1–3) | 3 (1–3) | 0.9915 |
| Awareness about
dosing | 8 | I take care not to
forget my medication | 5 (4–5) | 5 (3–5) | 0.4968 |
| 9 | I think I take a
lot of medications | 2 (1–5) | 3 (1–5) | 0.0116a |
| 10 | Dosing times are
complicated or awkward | 1 (1–5) | 1 (1–5) | 0.1819 |
| Awareness about
drug | 11 | The current
treatment costs (prescription charges) are an economic burden | 3 (1–5) | 3 (1–5) | 0.6207 |
| 12 | I believe the
medication is necessary for me | 5 (1–5) | 5 (1–5) | 0.1199 |
| 13 | I believe the
medication is effective | 5 (2–5) | 5 (2–5) | 0.0358a |
| 14 | I have actively
researched about my medication | 2 (1–5) | 1 (1–5) | 0.0397a |
| 15 | I worry about side
effects | 4 (1–5) | 4 (1–5) | 0.2185 |
| 16 | I would like to
talk to someone further about the medication | 3 (1–5) | 2 (1–5) | 0.0413a |
| Daily schedule | 17 | I have a regular
daily schedule | 5 (1–5) | 5 (2–5) | 0.1528 |
| 18 | I eat regular
meals | 5 (2–5) | 5 (2–5) | 0.3231 |
| Personality | 19 | I am
methodical | 4 (1–5) | 4 (1–5) | 0.1716 |
| 20 | I am a worrier | 4 (1–5) | 3 (1–5) | 0.1143 |
| 21 | I tend to find
things bothersome | 3 (1–5) | 3 (1–5) | 0.4135 |
| Understanding of
the stage of the disease | 22 | I have a good
understanding of my disease | 5 (2–5) | 5 (1–5) | 0.0262a |
| Sense of trust | 23 | I trust the
attending physician | 5 (3–5) | 5 (1–5) | 0.0262a |
| 24 | I trust the
pharmacist | 5 (2–5) | 5 (1–5) | 0.0345a |
| Expectations and
attitude | 25 | I hope that the
medication is valuable in curing the disease or that it will be
able to improve my quality of life | 5 (2–5) | 5 (2–5) | 0.3717 |
| 26 | I have a positive
attitude towards the disease | 5 (3–5) | 5 (1–5) | 0.0245a |
| Condition | 27 | What is your
general condition (health)? | 3 (2–5) | 3 (2–5) | 0.0196a |
CS analysis on the improvement of
medication adherence
The CS analysis graph is shown in Fig. 2 and the data obtained from CS
analysis are shown in Table IV.
From the CS analysis, three items, namely interest in the drug,
desire to consult about the drug and condition of the patient, were
found to be areas requiring improvement (degree of improvement;
11.00, 8.50, and 5.77, respectively).
| Table IVData obtained from CS analysis. |
Table IV
Data obtained from CS analysis.
| Question
number | Topic | Average value of
explanatory variables | Correlation
coefficient | Average value of
explanatory variables, deviation value | Correlation
coefficient, deviation value | Angle | Distance | Degree of
improvement |
|---|
| 14 | Interest in
druga | 2.29 | 0.1544 | 35.28 | 50.83 | 41.77 | 14.743 | 11.00 |
| 16 | Desire to consult
about druga | 2.47 | 0.1367 | 37.09 | 49.12 | 48.91 | 12.937 | 8.50 |
| 27 | Condition of
patienta | 3.45 | 0.1976 | 46.86 | 55.01 | 12.90 | 5.916 | 5.77 |
| 24 | Confidence in
pharmacist | 4.44 | 0.2040 | 56.74 | 55.63 | 95.09 | 8.782 | −0.78 |
| 22 | Understanding of
disease | 4.58 | 0.2062 | 58.20 | 55.85 | 99.51 | 10.068 | −1.66 |
| 23 | Confidence in
doctor | 4.81 | 0.2241 | 60.42 | 57.58 | 98.97 | 12.884 | −2.01 |
| 13 | Drug effect | 4.45 | 0.1455 | 56.85 | 49.97 | 135.29 | 6.853 | −4.87 |
| 26 | Positive
attitude | 4.78 | 0.1790 | 60.19 | 53.22 | 117.48 | 10.681 | −4.93 |
| 9 | Number of drugs
taken | 2.60 | −0.1349 | 38.38 | 22.80 | 111.86 | 29.576 | −11.01 |
Discussion
Numerous studies have examined medication adherence
in patients taking oral anticancer agents for CML and breast cancer
(5,7–13).
These studies have reported considerably different medication
adherence rates; for example, the adherence rate of patients with
CML was 14.2% in a study by Noens et al (7), but 98% in a study by Marin et
al (5). Thus, it may be that
differences in medication adherence rates depend largely on the
survey method. In the present study, the percentage of patients
with good medication adherence was not high (64.0%), however, the
percentage of patients with good medication compliance was 87.2%.
As numerous patients took the medication as directed, it can be
concluded that the medication compliance of patients taking oral
anticancer agents was good, but that the medication adherence,
according to the definition of the present study, was
insufficient.
Medication non-adherence in cancer chemotherapy can
lead to an increase in the seriousness of side-effects, a
deterioration in general health and a worse prognosis. Therefore,
it is important to learn the causes of non-adherence to improve
overall adherence.
The present study found that medication adherence
decreased with age. Hasegawa et al (14) and Tsuboi et al (15) reported that medication adherence is
higher in elderly patients compared with young patients. These
differences may be accounted for by differences in the
participants, but since this is not the only possibility,
differences in participants should be a topic for future
investigations. In addition, the patients with a longer course of
medication were more likely to be in the insufficient medication
adherence category. Ziller et al (16) reported that when patients received
supplementary information, medication adherence was good after 12
months. Therefore, in cases with a long course of medication,
patient guidance and information is important.
With regard to the factors affecting medication
adherence, nine items that had a significant effect on adherence
were observed in the present study: The number of drugs taken, the
effect of the drug, researching the medication, consulting with the
doctor or pharmacist about the drug, the understanding of the
disease, confidence in the doctor, confidence in the pharmacist, a
positive attitude and the condition of the patient. Russmann et
al (17) reported that good
relationships between patients, families and medical personnel
improved medication adherence. In the present study, similarly,
confidence in the doctor or pharmacist affected medication
adherence. However, if the guidance provided to the patient is
insufficient and the patient does not understand the supportive
care, it may lead to a decrease in the quality of life and an
increase in the frequency of doctor visits and re-hospitalization
due to improper or inadequate medication, including the use of
antiemetics in supportive care (18).
Regarding the factors associated with treatment, the
effect of the frequency, duration and number of drugs taken on
medication adherence must be considered. It has been reported that
an administration frequency of more than three times a day reduces
medication adherence significantly (19). In the present study, the majority of
the drugs were to be taken once or twice a day. Therefore, it was
assumed that the effect of the medication administration frequency
would be small. However, the patients with insufficient medication
adherence felt that they take a large number of drugs, particularly
when drugs were prescribed at the same time as the anticancer
medication. Therefore, all drugs taken, not only anticancer agents,
should be considered, as this could lead to an improved
understanding of patient-specific issues and improve the directions
offered to patients.
The attitude of a patient towards the disease and
treatment is an important factor. In the current study, patients
with good medication adherence were interested in learning about
the medicine and disease, and actively participated in their
treatment. It was also found that a positive attitude towards the
disease could affect medication adherence. If patients express a
positive attitude towards their disease, their willingness to
participate in the monitoring of side-effects may be higher.
The health of the patients also affected medication
adherence. In the present study, poor medication adherence was
associated with poor patient health. It could be hypothesized that
adherence to the treatment plan may be prevented by having poor
health.
According to the CS analysis, the items requiring
the greatest improvement were the interest in the drug, the desire
to consult about the drug and the condition of the patient. The
interest of patients in their own medication leads to the
improvement of medication adherence, which has been demonstrated to
alleviate anxiety; guiding these patients in the management of
side-effects is necessary. In addition, interventions tailored to
the condition of each patient are necessary to ensure that the
proper medication regimen is fully adhered to. Winkeljohn (20) reported that health care providers
should work with patients on intervention plans, including
discussing anxiety or answering treatment questions, providing
education about the symptoms of the disease and teaching the
management of medication side-effects. Patient education and
continuing guidance can be considered beneficial when delivered at
appropriate times using appropriate methods.
In summary, medical personnel must be aware of the
number of medications taken by the patient, the course of the
medication and the age of the patient when they instruct patients
undergoing anticancer treatments on the use of oral anticancer
agents. Future studies are necessary for an improved understanding
of the effect and necessity of drugs and their side-effects. In
addition, interventions and instructions must begin to be tailored
to the condition of each patient, as this would encourage patients
to take a greater interest in their own medication. These actions
may lead to improved medication adherence and enhance the efficacy,
safety and continuity of oral anticancer treatments.
References
|
1
|
Owashi T and Uejima K: Adherence from
compliance. Gekkan yakuji. 50:373–376. 2008.(In Japanese).
|
|
2
|
Wu EQ, Guerin A, Yu AP, et al:
Retrospective real-world comparison of medical visits, costs, and
adherence between nilotinib and dasatinib in chronic myeloid
leukaemia. Curr Med Res Opin. 26:2861–2869. 2010.
|
|
3
|
Reginster JY: Adherence and persistence:
impact on outcomes and health care resources. Bone. 38(Suppl 2):
S18–S21. 2006.
|
|
4
|
Macintosh PW, Pond GR, Pond BJ, Leung V
and Siu LL: A comparison of patient adherence and preference of
packaging method for oral anticancer agents using conventional pill
bottles versus daily pill boxes. Eur J Cancer Care (Engl).
16:380–386. 2007.
|
|
5
|
Marin D, Bazeos A, Mahon FX, et al:
Adherence is the critical factor for achieving molecular responses
in patients with chronic myeloid leukemia who achieve complete
cytogenetic responses on imatinib. J Clin Oncol. 28:2381–2388.
2010.
|
|
6
|
Nilsson JL, Andersson K, Bergkvist A, et
al: Refill adherence to repeat prescriptions of cancer drugs to
ambulatory patients. Eur J Cancer Care (Engl). 15:235–237.
2006.
|
|
7
|
Noens L, van Lierde MA, De Bock R, et al:
Prevalence, determinants, and outcomes of nonadherence to imatinib
therapy in patients with chronic myeloid leukaemia: the ADAGIO
study. Blood. 113:5401–5411. 2009.
|
|
8
|
Partridge AH, Archer L, Kornblith AB, et
al: Adherence and persistence with oral adjuvant chemotherapy in
older women with early-stage breast cancer in CALGB 49907:
adherence companion study 60104. J Clin Oncol. 28:2418–2422.
2010.
|
|
9
|
Hershman DL, Kushi LH, Shao T, et al:
Early discontinuation and nonadherence to adjuvant hormonal therapy
in a cohort of 8,769 early-stage breast cancer patients. J Clin
Oncol. 28:4120–4128. 2010.
|
|
10
|
Lebovits AH, Strain JJ, Schleifer SJ, et
al: Patient noncompliance with self-administered chemotherapy.
Cancer. 65:17–22. 1990.
|
|
11
|
Mayer EL, Partridge AH, Harris LN, et al:
Tolerability of and adherence to combination oral therapy with
gefitinib and capecitabine in metastatic breast cancer. Breast
Cancer Res Treat. 117:615–623. 2009.
|
|
12
|
McCowan C, Shearer J, Donnan PT, et al:
Cohort study examining tamoxifen adherence and its relationship to
mortality in women with breast cancer. Br J Cancer. 99:1763–1768.
2008.
|
|
13
|
Moore S: Nonadherence in patients with
breast cancer receiving oral therapies. Clin J Oncol Nurs.
14:41–47. 2010.
|
|
14
|
Hasegawa K, Kuritani Y, Adachi A, et al:
Improvement of drug compliance and pharmaceutical care - types of
drug and dosing regimens desired by patients. Iryouyakugaku.
34:800–804. 2008.(In Japanese).
|
|
15
|
Tsuboi K, Teramachi H, Kuzuya Y, et al:
Survey of the patients’ consciousness affecting medication
adherence. Iryouyakugaku. 38:522–533. 2012.(In Japanese).
|
|
16
|
Ziller V, Kyvernitakis I, Knöll D, et al:
Influence of a patient information program on adherence and
persistence with an aromatase inhibitor in breast cancer treatment
- the COMPAS study. BMC Cancer. 13:4072013.
|
|
17
|
Russmann S, Curkovic I and Huber M:
Adverse reactions and risks associated with non compliance. Ther
Umsch. 67:303–307. 2010.(In German).
|
|
18
|
Ruddy K, Mayer E and Partridge A: Patient
adherence and persistence with oral anticancer treatment. CA Cancer
J Clin. 59:56–66. 2009.
|
|
19
|
Lee CR, Nicholson PW, Souhami RL and
Deshmukh AA: Patient compliance with oral chemotherapy as assessed
by a novel electronic technique. J Clin Oncol. 10:1007–1013.
1992.
|
|
20
|
Winkeljohn D: Adherence to oral cancer
therapies: nursing interventions. Clin J Oncol Nurs. 14:461–466.
2010.
|