Renal cell carcinoma (RCC) is divided into
clear-cell, papillary, oncocytoma and collecting duct subtypes
which exert different invasion and metastatic potentials (1). The clear-cell carcinoma subtype
represents <85% of reported cases, according to the United
States National Centre for Health Statistics report (2). Recurrence of the disease following
surgery can be observed in one-third of the cases and one-fourth of
the patients exhibit metastatic disease at the time of a diagnosis
(1,2). RCC metastases are often regarded as
radioresistant tumors, which was observed in the present case
(2–4). For this reason, metastases are usually
treated with relatively high biologically effective doses.
Metastasis to adjacent organs and bone are common, but distant
metastases to the head and neck region are rare. Of these
previously reported cases, the facial skin area has been the most
common location. The present study demonstrates the case of rapidly
growing and radiotherapy-resistant RCC metastasis to the lower lip
and chin which was treated with surgery. The functional and
esthetic outcome was satisfactory despite the large gap generated
by the metastasis resection. This case provides evidence that
palliative surgery may achieve a higher quality of life for
end-stage oncological patients.
The current study presents the case of a 71-year-old
male patient who was diagnosed with RCC in September 2011. At that
time, the disease was at an advanced stage. The primary tumor in
the lower pool of the right kidney was infiltrating the adjacent
structures and the patient exhibited synchronous mediastinal and
pleural metastases, with the latter causing persistent pleural
effusion and markedly declining lung function. Due to the poor
performance status and risk of side effects, the patient refused to
initiate the disease-controlling sunitinib treatment and chose to
proceed to the optimum supportive care. The patient presented with
subcutaneous metastases to the lower lip and back of the neck 11
months after the diagnosis. The patient received palliative
radiotherapy (split course, 15/5 Gy) to the rapidly growing lower
lip metastasis. The tumor diameter was 1.5 cm when the treatment
was initiated. However, no clinical response to radiotherapy was
obtained, and three weeks following the treatment the tumor had
more than tripled in diameter. Thus, the patient was evaluated at
the Department of Oral and Maxillofacial Diseases (Helsinki
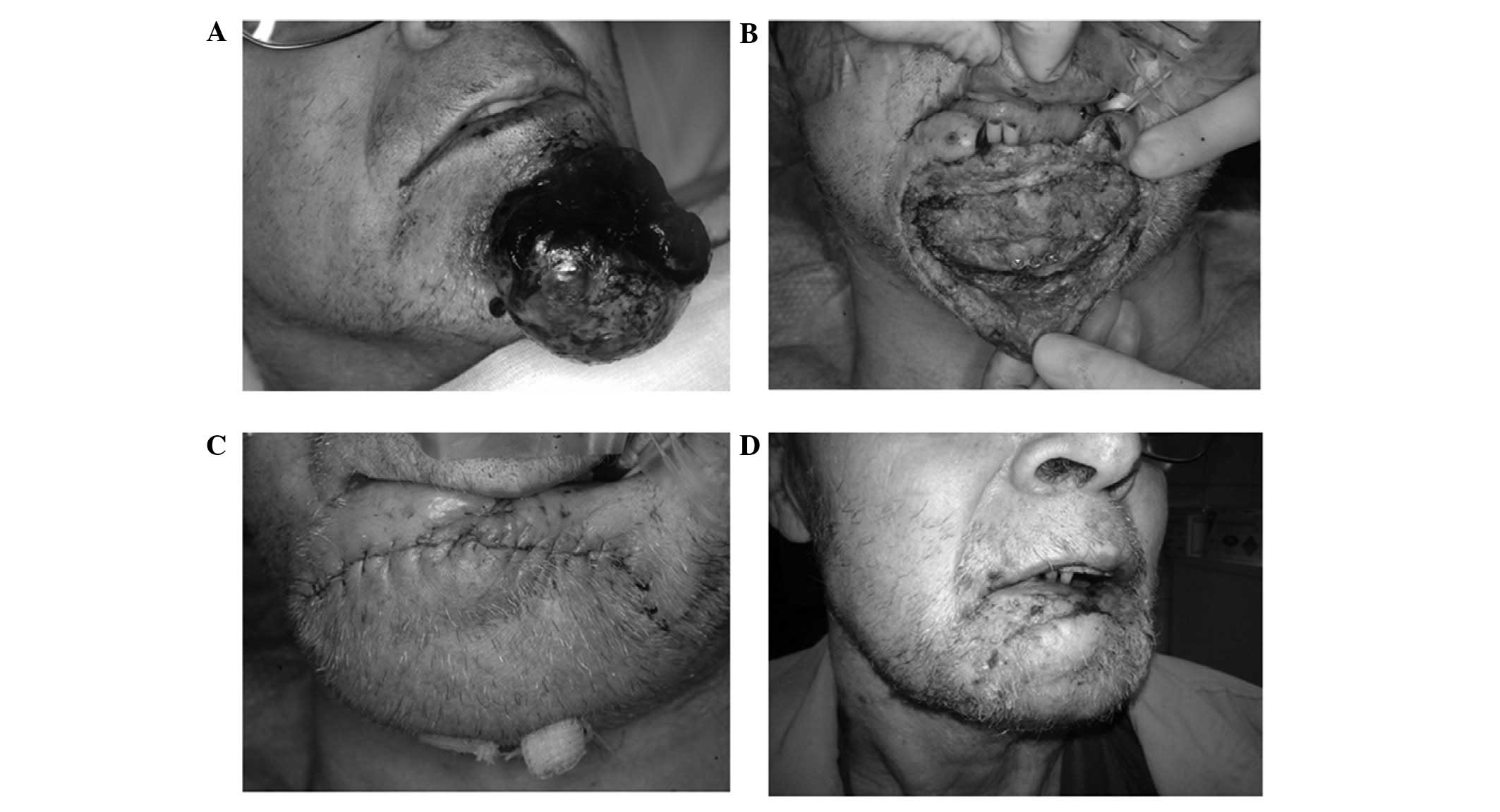
University; Helsinki, Finland). At the time of admission the
patient had a spontaneously bleeding mass (size, 60×60 mm) in the
lower lip and the anterior mandible area (Fig. 1A). In addition to this, there was a
group of smaller subcutaneous metastases located at the
subcutaneous nuchal area, which did not exhibit symptoms. Resection
of the lip metastasis was performed with 5-mm clinical margins and
for this reason, the resection was extended to the bony surface of
the mandible. The lower lip was also partially resected as the
small subcutaneous metastases had continued to spread into the lip
mucosa (Fig. 1B). To prevent wound
tension following closure, the skin was dissected subcutaneously
from the resection line to the upper neck, pulled over the chin to
cover visible bone, and resuspended with transcutaneous sutures to
the titanium plate (MatrixMFACE Plating System; Synthes Holding AG,
Solothurn, Switzerland) in the mandible (Fig. 1B and C). The patient was satisfied
with the outcome at the three-week postoperative follow-up and no
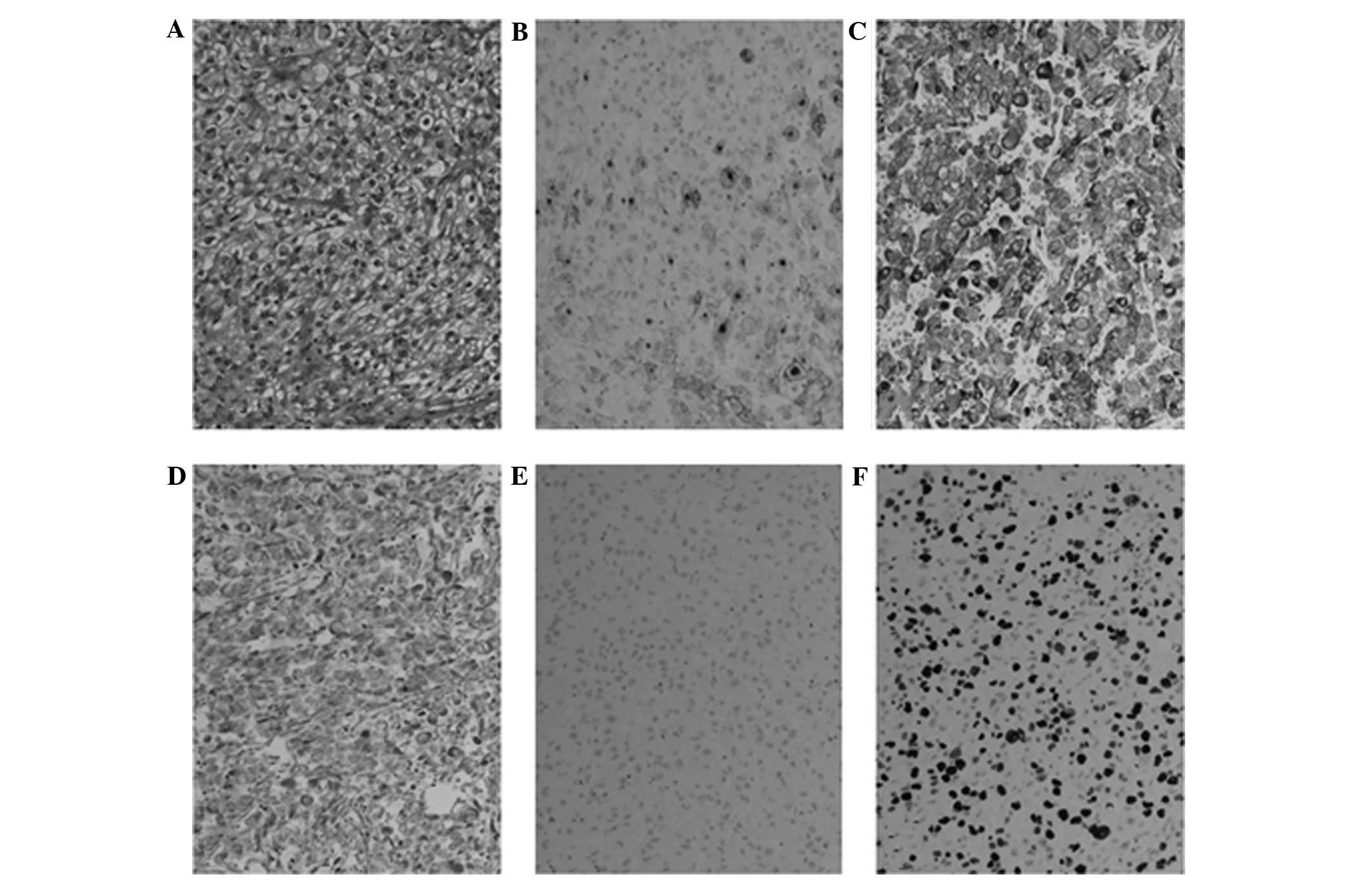
clinical sign of recurrence was observed (Fig. 1D). Histological examination via
immunohistochemical staining (Fig.
2) identified the tumor as metastatic RCC and the mass was
resected with clear lateral margins.
RCC commonly metastases to adjacent organs, and up
to one-fourth of patients have metastases present at the time of
the diagnosis (1,2). Four major subtypes of RCC exist
(clear-cell, papillary, oncocytoma and collecting duct carcinoma),
with different invasion and metastatic potentials. However, none of
them have been reported to be particularly invasive to the head and
neck region (1,2). Of the 75 previously reported cases of
metastatic RCC to the head and neck region, the majority were
already diagnosed with RCC, however, certain patients exhibited
oral metastasis as the initial manifestation of the disease. This
highlights the importance of full body imaging to identify whether
the patient has previously undergone surgery for head and neck
neoplasms, to avoid inaccurately diagnosing a newly formed
metastasis as the recurrence of a former tumor. A third of the
previously identified cases of patients with head and neck RCC
metastases have been reported on the facial skin area (4–11),
although the parotid gland, paranasal sinuses and tongue are also
common locations. In addition, single cases of nephroblastoma (also
termed, Wilms’ tumor) and renal sarcomas have been reported in the
head and neck area (12,13). According to earlier reports, none of
the RCC subtypes preferentially metastasize to the head and neck
area. The locations of previously reported metastases are listed in
Table I (4–51).
In conclusion, surgery is rarely the first option
when treating RCC patients with multiple metastases. However, it is
important to consider palliative surgery for certain patients, as
surgical management of the metastasis may provide an improved
quality of life although this type of surgery does not affect the
final outcome.
|
1
|
Cohen HT and McGovern FJ: Renal-cell
carcinoma. N Engl J Med. 353:2477–2490. 2005.
|
|
2
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J and
Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 59:225–249.
2009.
|
|
3
|
Owens RM, Friedman CD and Becker SP: Renal
cell carcinoma with metastasis to the parotid gland: case reports
and review of the literature. Head Neck. 11:174–178. 1989.
|
|
4
|
Zhang Y, Gu ZY, Tian Z, Yang C and Cai XY:
Oral metastasis from primary transitional cell carcinoma of the
renal pelvis: report of a case. Int J ORal Maxillofac Surg.
39:737–739. 2010.
|
|
5
|
Chauhan A, Ganguly M, Nath P and Chowdhary
GS: Cutaneous metastasis to face and neck as a sole manifestation
of an unsuspected renal cell carcinoma. Int J Dermatol. 50:81–84.
2011.
|
|
6
|
Chhabra P, Bhatt V and Brown AM:
Metastatic renal cell carcinoma in the neck: an unusual
presentation. Dent Update. 36:511–513. 2009.
|
|
7
|
Giuliani A, Caporale A, Borghese M, Galati
G, Di Bari M and Demoro M: Papillary renal cell carcinoma
presenting as nodal metastases to the neck. J Exp Clin Cancer Res.
18:579–582. 1999.
|
|
8
|
Langille G, Taylor SM and Bullock MJ:
Metastatic renal cell carcinoma to the head and neck: summary of 21
cases. J Otolaryngol Head Neck Surg. 37:515–521. 2008.
|
|
9
|
Mahmoudi HR, Kamyab K and Deneshpazhooh M:
Cutaneous metastasis of renal cell carcinoma: case report. Dermatol
Online J. 18:122012.
|
|
10
|
Mrena R, Leivo I, Passador-Santos F,
Hagström J and Mäkitie AA: Histopathological findings in parotid
gland metastases from renal cell carcinoma. Eur Arch
Otorhinolaryngol. 265:1005–1009. 2008.
|
|
11
|
Syryło T, Syryło A, Jurkiewicz D,
Zieliński H and Pietka T: An upper lip tumour as the presenting
symptom of metastatic renal cancer. Otolaryngol Pol. 64:318–319.
2010.
|
|
12
|
Florine BL, Simonton SC, Sane SM, Stickel
FR, Singher LJ and Dehner LP: Clear cell sarcoma of the kidney:
report of a case with mandibular metastasis simulating a benign
myxomatous tumor. Oral Surg Oral Med Oral Pathol. 65:567–574.
1988.
|
|
13
|
Jia J, Chen XM, Sun ZJ and Zhang WF:
Mandibular metastasis of nephroblastoma: a rare case. Int J Oral
Maxillofac Surg. 35:1160–1161. 2006.
|
|
14
|
Aguirre A, Rinaggio J and Diaz-Ordaz E:
Lingual metastasis of renal cell carcinoma. J Oral Maxillofac Surg.
54:344–346. 1996.
|
|
15
|
Airoldi M, Succo G, Valente G, Cavalot A,
Gabriele P and Bumma C: Head and neck metastases of renal cancer
after nephrectomy: a report of 2 cases. Tumori. 81:213–214.
1995.
|
|
16
|
Alvarez-Múgica M, Bulnez Vàzquez V, Jalón
Monzón A, Gil A, Rodríguez Robles L and Miranda Aranzubía O: Late
recurrence from a renal cell carcinoma: solitary right maxillar
mass 17 years after surgery. Arch Esp Urol. 63:147–150. 2010.
|
|
17
|
Bersani TA, Costello JJ Jr, Mango CA and
Streeten BW: Benign approach to malignant orbital tumor: metastatic
renal cell carcinoma. Ophthal Plast Reconstr Surg. 10:42–44.
1994.
|
|
18
|
Borghi L, Bianchini E, Ballotta MR and
Reale D: Metastatic renal cell carcinoma presenting as a parotid
tumor: a case report. Pathologica. 87:168–170. 1995.
|
|
19
|
Cochrane TJ, Cheng L and Crean S: Renal
cell carcinoma: A rare metastasis to the tongue - a case report.
Dent Update. 33:186–187. 2006.
|
|
20
|
Corsi A, Guerra F, Grippaudo G and Bosman
C: Oral metastasis of renal cell carcinoma. Report of case and
critical evaluation of morphologic features for differential
diagnosis. Pathologica. 86:665–669. 1994.
|
|
21
|
Dee SL, Eshghi M and Otto CS: Laryngeal
metastasis 7 years after radical nephrectomy. Arch Pathol Lab Med.
124:1833–1834. 2000.
|
|
22
|
Deeb R, Zhang Z, Kini S and Ghanem T:
Metastatic renal cell carcinoma to the parotid gland presenting 19
years after nefrectomy: case report and review of literature.
Laryngoscope. 120(Suppl 4): S1282010.
|
|
23
|
Friedlander AH and Singer R: Renal
adenocarcinoma of the kidney with metastasis to the tongue. J Am
Dent Assoc. 97:989–991. 1978.
|
|
24
|
Günbay MU, Ceryan K and Küpelíoğlu AA:
Metastatic renal carcinoma to the parotid gland. J Laryngol Otol.
103:417–418. 1989.
|
|
25
|
Hamdoon Z, Jerjes W, Upile T, Akram S and
Hopper C: Metastatic renal cell carcinoma to the orofacial region:
A novel method to alleviate symptoms and control disease
progression. Photodiagnosis Photodyn Ther. 7:246–250. 2010.
|
|
26
|
Homer JJ and Jones NS: Renal cell
carcinoma presenting as a solitary paranasal sinus metastasis. J
Laryngol Otol. 109:986–989. 1995.
|
|
27
|
Kian A and Kato SN: Renal cell carcinoma
metastatic to the base of tongue: a case report. Hinyokika Kiyo.
50:791–793. 2004.(In Japanese).
|
|
28
|
Lee HM, Kang HJ and Lee SH: Metastatic
renal cell carcinoma presenting as epistaxis. Eur Arch
Otorhinolaryngol. 262:69–71. 2005.
|
|
29
|
Maestre-Rodríguez O, González-García R,
Mateo-Arias J, Moreno-García C, Serrano-Gil H, Villanueva-Alcojol
L, Campos-de-Orellana AM and Monje-Gil F: Metastasis of renal
clear-cell carcinoma to the oral mucosa, an atypical location. Med
Oral Patol Oral Cir Bucal. 14:e601–e604. 2009.
|
|
30
|
Makos CP and Psomaderis K: A literature
review in renal carcinoma metastasis to the oral mucosa and a new
report of an epulis-like metastasis. J Oral Maxillofac Surg.
67:653–660. 2009.
|
|
31
|
Marioni G, Gaio E, Poletti A, Derosas F
and Staffieri A: Uncommon metastatic site of renal adenocarcinoma:
the oral tongue. Acta Otolaryngol. 124:197–201. 2004.
|
|
32
|
Massaccesi M, Morganti AG, Serafini G, Di
Lallo A, Deodato F, Picardi V and Scambia G: Late tonsil metastases
from renal cell cancer: a case report. Tumori. 95:521–524.
2009.
|
|
33
|
Melnick SJ, Amazon K and Dembrow V:
Metastatic renal cell carcinoma presenting as a parotid tumor: a
case report with immunohistochemical findings and a review of the
literature. Hum Pathol. 20:195–197. 1989.
|
|
34
|
Narea-Matamala G, Fernández-Toro Mde L,
Villalabeitía-Ugarte E, Landaeta-Mendoza M and Rojas-Alcayaga G:
Oral metastasis of renal cell carcinoma, presentation of a case.
Med Oral Patol Oral Cir Bucal. 13:E742–E744. 2008.
|
|
35
|
Park YW and Hlivko TJ: Parotid gland
metastasis from renal cell carcinoma. Laryngoscope. 112:453–456.
2002.
|
|
36
|
Pires FR, Azevedo RS, Ficarra G, Cardoso
AS, Carlos R, Kowalski LP and de Almeida OP: Metastatic renal cell
carcinoma to the oral cavity and clear cell mucoepidermoid
carcinoma: comparative clinicopathologic and immunohistochemical
study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
109:e22–e27. 2010.
|
|
37
|
Preechawai P, Amrith S, Yip CC and Goh KY:
Orbital metastasis of renal cell carcinoma masquerading as
cysticercosis. Orbit. 27:370–373. 2008.
|
|
38
|
Sarkis P, Bou-Malhab F and Mouaccadieh L:
Solitary laryngeal metastasis from renal cell carcinoma of the
kidney: clinical case and review of the literature. Prog Urol.
22:307–309. 2012.(In French).
|
|
39
|
Schantz JC, Miller SH and Graham WP III:
Metastatic hypernephroma to the head and neck. J Surg Oncol.
8:183–190. 1976.
|
|
40
|
Schwab B and Lee WT: Bilateral renal cell
carcinoma metastasis in the oral cavity. Am J Otolaryngol.
33:154–155. 2012.
|
|
41
|
Seijas BP, Franco FL, Sastre RM, García AA
and Lópexz-Cedrún Cembranos JL: Metastatic renal cell carcinoma
presenting as a parotid tumor. Oral Surg Oral Med Oral Pathol Oral
radiol Oral Endod. 99:554–557. 2005.
|
|
42
|
Sgouras ND, Gamatsi IE, Porfyris EA, Lekka
JA, Harkiolakis GC, Nikolopoulou SM and Valvis PJ: An unusual
presentation of a metastatic hypernephroma to the frontonasal
region. Ann Plast Surg. 34:653–656. 1995.
|
|
43
|
Shetty SC, Gupta S, Nagsubramanium S,
Hasan S and Cherry G: Mandibular metastasis from renal cell
carcinoma. A case report Indian J Dent Res. 12:77–80. 2001.
|
|
44
|
Simo R, Sykes AJ, Hargreaves SP, Axon PR,
Birzgalis AR, Slevin NJ and Farrington WT: Metastatic renal cell
carcinoma to the nose and paranasal sinuses. Head Neck. 22:722–727.
2000.
|
|
45
|
Spreafico R, Nicoletti G, Ferrario F,
Scanziani R and Grasso M: Parotid metastasis from renal cell
carcinoma: a case report and review of the literature. Acta
Otorhinolaryngol Ital. 28:266–268. 2008.
|
|
46
|
Susan LP, Daughtry JD, Stewart BH and
Straffon RA: Palatal metastases in renal cell carcinoma. Urology.
13:304–305. 1979.
|
|
47
|
Vreugde S, Duttmann R, Halama A and Deron
P: Metastasis of a renal cell carcinoma to the nose and paranasal
sinuses. Acta Otorhinolaryngol Belg. 53:129–131. 1999.
|
|
48
|
Will TA, Agarwal N and Petruzelli GJ: Oral
cavity metastasis of renal cell carcinoma: a case report. J Med
Case Rep. 2:3132008.
|
|
49
|
Yeh HC, Yang SF, Ke HL, Lee KS, Huang CH
and Wu WJ: Renal cell carcinoma presenting with skull metastasis: a
case report and literature review. Kaohsiung J Med Sci. 23:475–479.
2007.
|
|
50
|
Yiotakis J, Hantzakos A, Kostakopoulos A
and Adamopoulos G: Intramasseteric metastasis of renal cell
carcinoma. J Laryngol Otol. 115:65–67. 2001.
|
|
51
|
Yoshitomi I, Kawasaki G, Mizuno A,
Nishikido M, Hayashi T, Fujita S and Ikeda T: Lingual metastasis as
an initial presentation of renal cell carcinoma. Med Oncol.
28:1389–1394. 2011.
|