Introduction
Glomerulocystic kidneys (GCKs) are characterized by
the cystic dilatation of Bowman's space to form glomerular cysts
(GCs), and are mainly observed in infants and young children in
association with the following conditions: Hereditary polycystic
kidney disease, tuberous sclerosis, renal dysplasia and renal
ischemia, and certain medications, including lithium (1). To the best of our knowledge, only 35
cases of GCKs have been reported in adults worldwide (1–3). The
majority of these patients presented with decreased renal function
and subsequently received hemodialysis treatment, however they
eventually progressed to end-stage renal disease (2,3). However,
a few cases had normal renal function or were asymptomatic
(1–4).
GCKs are generally diagnosed by open renal biopsy. The lesion is
not generally recognized as a neoplatic mass and cases of GCKs
mimicking multilocular renal carcinoma are rare. The present study
describes the first adult case of a sporadic localized GCK that
presented as a cystic mass mimicking a neoplasm, and provides an
analysis of the features of GC. Informed consent was obtained from
the patient's family.
Case report
An asymptomatic 42-year-old male presented to
Saiseikai Senri Hospital (Osaka, Japan) was revealed to have
microscopic hematuria following a medical check-up. The patient was
revealed to have a localized nest of multilocular cysts, without
any expansile nodules, which measured 2×4 cm in diameter. The
cystic mass was detected in the lower pole of the right kidney by
abdominal ultrasonography, contrast-enhanced computed tomography
(CT) (Fig. 1A) and
gadolinium-enhanced magnetic resonance imaging (MRI) (Fig. 1B). Contrast-enhanced CT revealed
enhancement in the lesion [Bosniak classification category III
(4)]. Cystic renal cell carcinoma
could not be ruled out, therefore, a right partial nephrectomy was
performed.
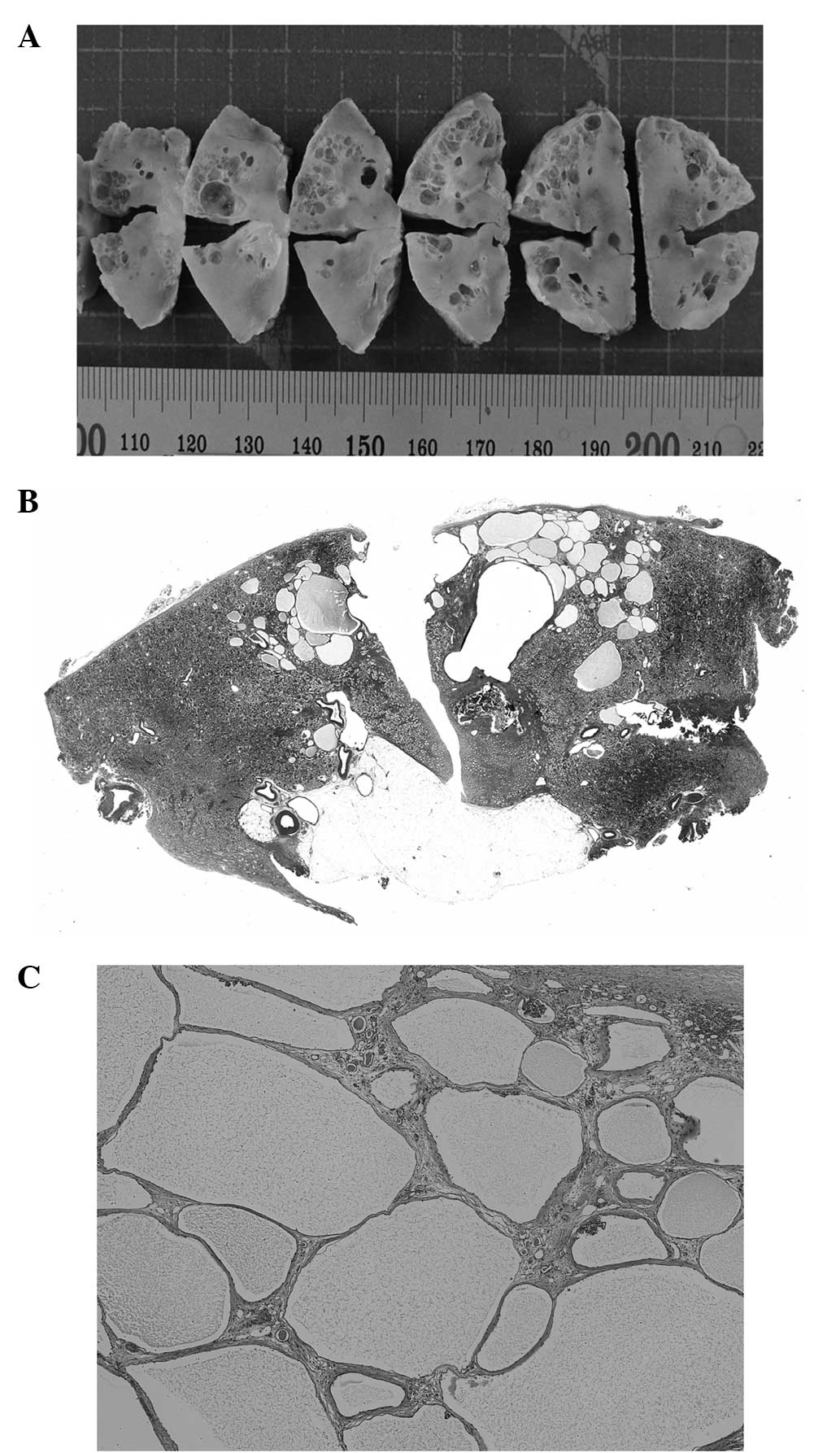
Grossly, the lesion was composed of multiple cysts
filled with serous fluid, each measuring ≤8 mm in maximum diameter,
and was distributed in the cortex of the resected kidney (Fig. 2). A small calculus measuring 2 mm in
diameter was deposited in the outer medulla directly under the
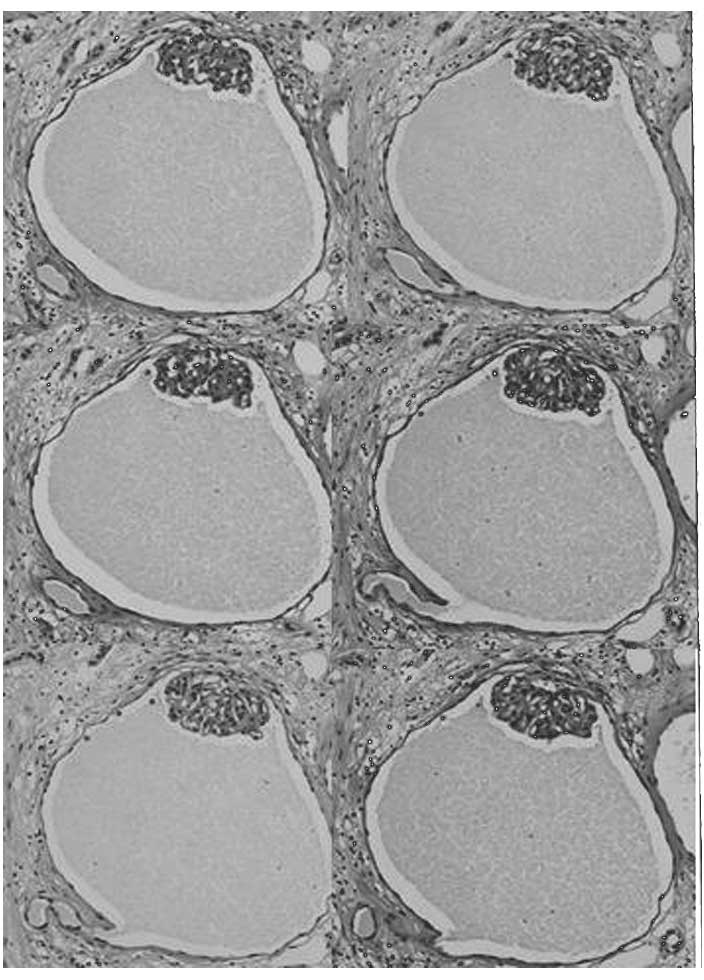
lesion. Microscopically, the majority of the cysts were lined by a
single layer of flattened epithelium and a collapsed glomerulus was
evident (Fig. 2C). In the
corticomedullary junction, a few cysts lined by epithelial membrane
antigen- and CK34βE12-positive cuboidal epithelium were suggestive
of a derivation from the distal tubule or collecting duct. This
lesion was diagnosed as a sporadic case, as no family history or
clinical history was found that was associated with GCKs.
A serial section study was performed for light
microscopy to examine the GTJ. A total of 250 4-µm thick sections
and 100 2-µm thick sections were stained with hematoxylin and eosin
(HE) and Periodic acid-Schiff (PAS), respectively. A GC was defined
as Bowman's capsule dilation of more than twice the diameter of a
normal Bowman's capsule (320 µm), as described in a previous study
(1). Each single specimen contained
50–80 cysts. Eight and six GTJs from 30 examined GCs were detected
in these HE- and PAS-stained sections, respectively. These sections
revealed a connection between the GCs and the proximal tubule,
although the connected tubule became narrow and serpiginous
(Fig. 3). The patient was lost to
follow-up.
Discussion
Generally, GCKs diffusely involve the bilateral
kidneys in infants and young children. To the best of our
knowledge, this is the first adult case of a sporadic GCK mimicking
a tumor. Retrospectively, the enhancement of this lesion that was
identified on CT was determined to be that of a residual normal
cortex. Radiologically, the lesion was almost entirely localized in
the cortex, without renal surface deformity or protrusion from the
kidney, and did not have the capsular and peritumoral change
associated with invasive or expansive growth. These findings
suggest that it was a non-neoplastic lesion. Unnecessary surgery
may be avoided in future cases by careful evaluation of the CT and
MRI, although localized GCKs are quite rare.
Obliteration at the glomerulotubular junction (GTJ)
has been assumed to be the cause of GCKs associated with several
diseases, however, the exact cause remains controversial (3,5,6). Hotta et al (5) used serial sections to demonstrate GTJ
stenosis and suggested that periglomerular fibrosis induced
stenosis of GTJ. By contrast, Liu et al (3) identified no stenosis or obstruction of
the GTJ using serial sections. In the present case, a connection
between the GCs and the proximal tubule was identified. These
findings suggested that obliteration at the GTJ was not the primary
cause of the GCs in the present case. Since this case was composed
of large GCs with non-detectable surrounding proximal tubules, it
was reasonable to assume that the GCs were composed of Bowman's
capsule and part of the proximal tubule (7). We hypothesize that proliferation of the
parietal cells and renal tubular cells, fluid accumulation and
remodeling of the nephron (6) were
the main causes of cyst development in the present case. As various
conditions are associated with the formation of GC, such as
hereditary polycystic kidney disease, tuberous sclerosis and renal
dysplasia, we hypothesize that different pathogenic mechanisms of
GC formation exist.
In summary, the present study reported an adult case
of a sporadic localized GCK that resembled a cystic renal neoplasm,
and provided analysis of its characteristic histopathological
features using serial sections.
Acknowledgements
The authors would like to thank Mr. Masaru Nishino,
Mrs. Noriko Yokozeki and Mr. Manabu Kobayashi (Department of
Central Clinical Laboratory, Saiseikai Senri Hospital, Suita,
Osaka, Japan) for their technical assistance in the serial
sectioning.
References
|
1
|
Lennerz JK, Spence DC, Iskandar SS, Dehner
LP and Liapis H: Glomerulocystic kidney: one hundred-year
perspective. Arch Pathol Lab Med. 134:583–605. 2010.PubMed/NCBI
|
|
2
|
Obata Y, Furuse A, Miyazaki M, Nishino T,
Kawazu T, Kanamoto Y, Nishikido M, Taguchi T and Kohno S:
Glomerulocystic kidney disease in an adult with enlarged kidneys: a
case report and review of the literature. Clin Nephrol. 75:158–164.
2011.PubMed/NCBI
|
|
3
|
Liu JS, Ishikawa I, Saito Y, Nakazawa T,
Tomosugi N and Ishikawa Y: Digital glomerular reconstruction in a
patient with a sporadic adult form of glomerulocystic kidney
disease. Am J Kidney Dis. 35:216–220. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bosniak MA: The Bosniak renal cyst
classification: 25 years later. Radiology. 262:781–785. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hotta O, Sato M, Furuta T and Taguma Y:
Pathogenic role of glomerulo-tubular junction stenosis in
glomerulocystic disease. Clin Nephrol. 51:177–180. 1999.PubMed/NCBI
|
|
6
|
Liu JS, Ishikawa I, Saito Y, Nakazawa T,
Tomosugi N and Ishikawa Y: Digital glomerular reconstruction in a
patient with a sporadic adult form of glomerulocystic kidney
disease. Am J Kidney Dis. 35:216–220. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kanouzawa K, Tamura H, Matsumura O,
Nagasawa R, Mitarai T, Isoda K and Yamanaka N: An adult case of
glomerulocystic kidney disease. Nihon Jinzo Gakkai Shi. 36:762–768.
1994.[(In Japanese)]. PubMed/NCBI
|