Introduction
Carcinoid tumors are a group of neuroendocrine
tumors that occur most frequently in the gastrointestinal tract as
well as in other organs comprising argyrophil cells; ~85% these
tumors occur in the digestive tract, with 10% occurring in the lung
and 5% occurring in other organs such as the testis (1) and bladder (2). The clinical manifestations of carcinoid
tumors may not be apparent, or limited to local symptoms. However,
carcinoid syndromes often have obvious systemic symptoms, such as
unexplained intermittent diarrhea, flushing, facial telangiectasia,
paroxysmal asthma or psychiatric symptoms (3). The diagnosis of carcinoid tumor is
dependent on biopsy, and surgical excision is the first treatment.
Patients without carcinoid syndrome have a better prognosis
(4).
Primary carcinoid tumor in the kidney is uncommon
and the expression of the estrogen receptor (ER) and the
progesterone receptor (PR) has not been reported. Due to the rarity
of this tumor, its clinicopathological characteristics, prognosis
and histogenesis have not been fully characterized. The current
study reports an unusual case of a carcinoid tumor of the kidney
with ER and PR expression in a 49-year-old female who presented
with a 2-year history of hypertension. Abdominal computed
tomography scans revealed a left horseshoe kidney.
Clinicopathological characteristics of primary carcinoid tumors are
also discussed by reviewing the literature. Written informed
consent was obtained from the patient for publication of this case
report and any accompanying images.
Case report
Clinical data
A 49-year-old female with a history of hypertension
for two years presented with a half-month history of painless gross
hematuria. The patient was admitted to the Department of Urological
Surgery in the Affiliated Yantai Yuhuangding Hospital (Medical
College of Qingdao University, Yantai, Shandong, China). No
abnormal physical signs were found during a physical examination.
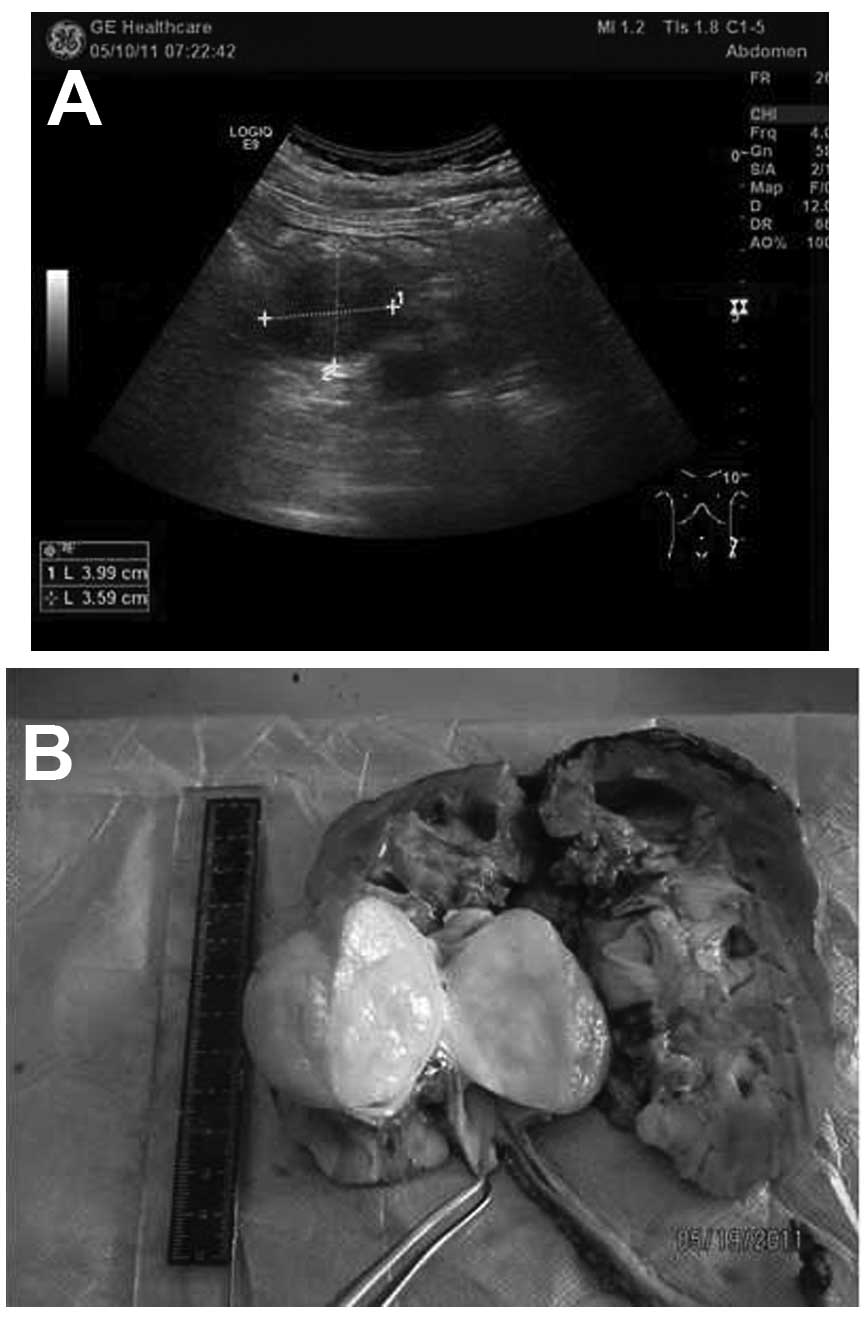
Abdominal computed tomography (CT) scans and ultrasonic testing
revealed left hydronephrosis, a horseshoe kidney and a
space-occupying lesion in the left ureter, while the right kidney
and other visceral organs were normal (Fig. 1A). The hematological findings,
endocrine index, erythrocyte sedimentation rate, blood
biochemistry, electrolytes, blood urea nitrogen and serum
creatinine levels were within the normal ranges. The surgery was
performed under general anesthesia and in a right lateral decubitus
position at 70°. The left kidney, which presented with black
coloration and a horseshoe appearance, was exposed and dissociated.
An oval tumor, ~5×4×3.6 cm, was observed under the ureter. The
boundaries of the mass were clear. The cross-section of the tumor
was faint yellow, homogeneous and pliable in quality (Fig. 1B).
Pathological findings
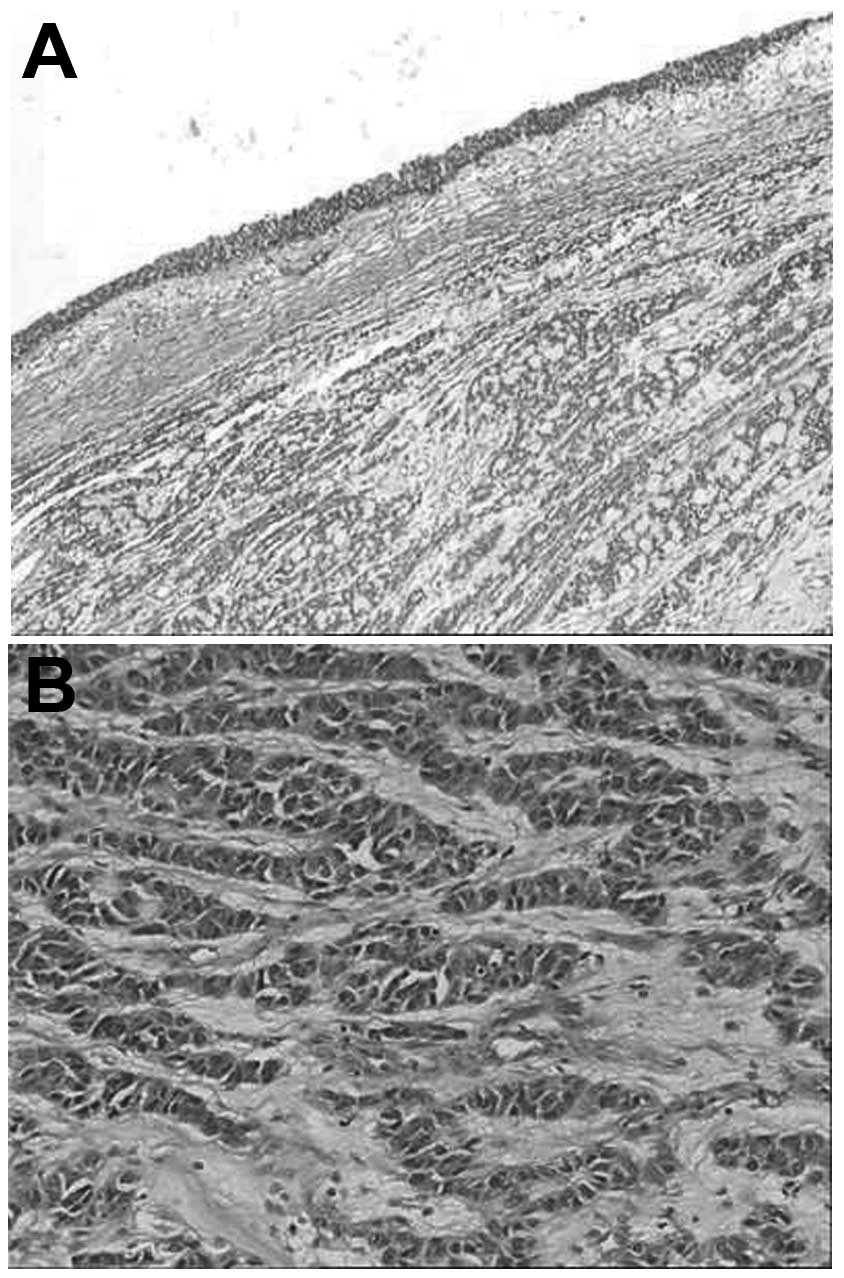
Microscopically, the tumor was located under the
mucosa of the pelvis and showed aggressive growth. The neoplasm was
composed of solid nests of cells, trabeculae, adenoid structures
and anastomosing cords in a loose and myxoid background (Fig. 2A). The tumor cells, which were
consistent in volume, exhibited centrally placed oval nuclei with
inconspicuous nucleoli, and eosinophilic finely granular cytoplasm.
The mitotic rate was <1 per 10 high-power fields (Fig. 2B).
Immunohistochemical findings
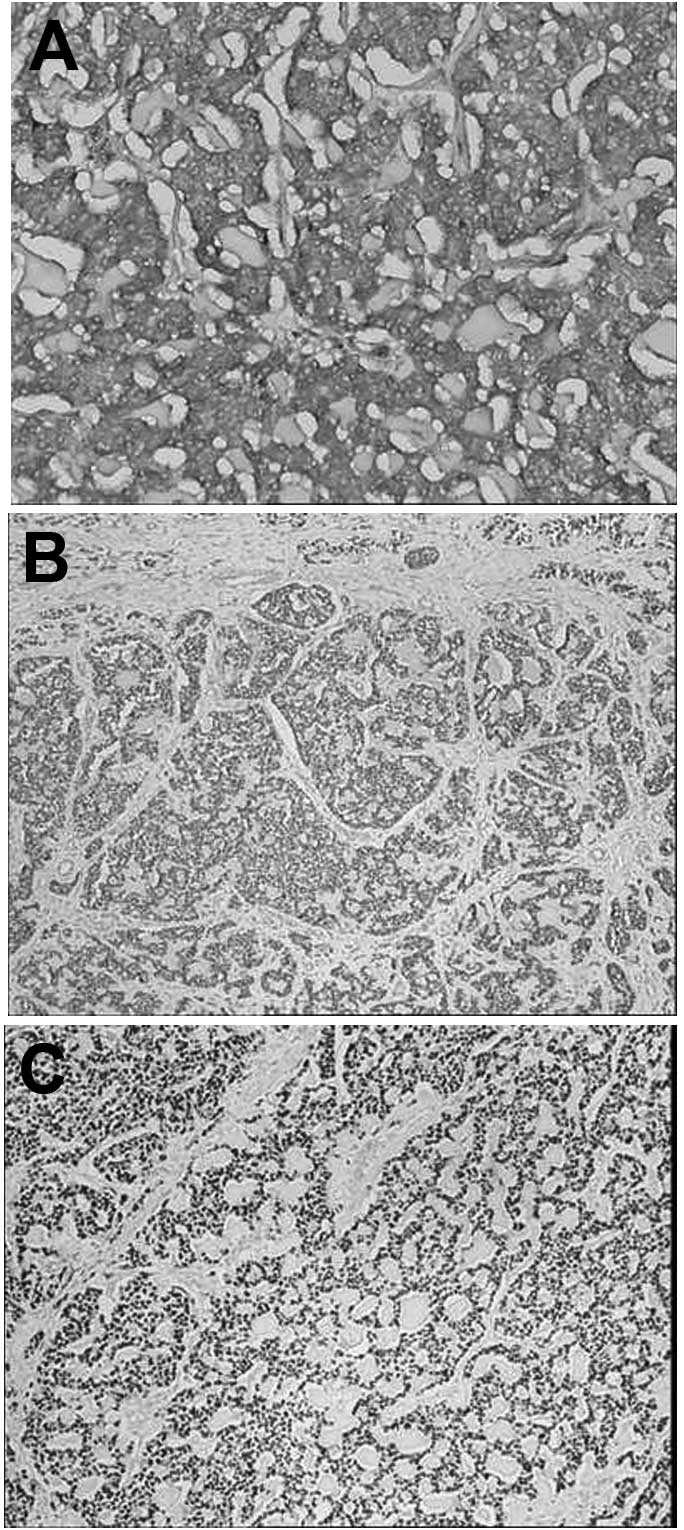
Immunohistochemical staining suggested that the
neoplastic cells were positive for AE1/AE3, vimentin, synaptophysin
(Syn; Fig. 3A), chromogranin A (CgA),
ER (Fig. 3B) and PR (Fig. 3C), while being negative for epithelial
membrane antigen, inhibin A, cluster of differentiation (CD)99,
S-100 and CD10. The cells that were positive for Ki-67 were
dispersive. All the primary antibodies used are listed in Table I. On the basis of histomorphology in
light microscopy and the presence of immunohistochemical staining,
a diagnosis of primary carcinoid tumor of the left kidney was made.
The patient did not receive further treatment. The total follow-up
period was 18 months after the surgery. Repeated CT scans and
abdominal ultrasonography every 6 months revealed no recurrence or
residual lesion.
 | Table I.Antibodies employed in the
immunohistochemistry applied for the case. |
Table I.
Antibodies employed in the
immunohistochemistry applied for the case.
| Antibody | Clone | Source | Dilution |
|---|
| Anti-S100 | 4C49 | Lab vision | 1:150 |
| Anti-cytokeratin | AE1/AE3 | Dako | 1:100 |
| Anti-vimentin | SP20 | Lab vision | 1:100 |
| Anti-Ki-67 | MIB-1 | Lab vision | 1:100 |
| Anti-CD99 | O13 | Dako | 1:100 |
| Anti-CD10 | 56C6 | Lab vision | 1:100 |
| Anti-inhibin A | R11 | Dako | 1:100 |
| Anti-EMA | E19 | Dako | 1:100 |
| Anti-ER | 1D5 | Dako | 1:100 |
| Anti-PR | EP2 | Dako | 1:100 |
| Anti-Syn | SP11 | Dako | 1:100 |
| Anti-CgA | EP38 | Dako | 1:100 |
Discussion
Carcinoid tumors of the kidney are rare. The
pathogenesis of renal carcinoid tumors remains under debate
(5–9).
Certain previous studies have attributed the genesis of this tumor
to congenital renal abnormalities, while other studies have
suggested that the tumor cells are derived from multipotential
primitive stem cells, which are induced to neuroendocrine
differentiation (10–12). Notably, in the present case, the ER
and PR sex hormone receptors were strongly expressed in the tumor
cells. ER and PR expression has previously been detected not only
in hormone target organs, such as the breast, ovaries and
endometrium, but also in the digestive tract and pancreas (13,14).
However, the expression of ER and PR in carcinoid tumors of the
kidney has not been reported. The present results may not be of use
in inferring the pathogenesis of the disease, as no relative
literature has been found by review, however, we speculate that the
ER and PR may be a potential therapeutic target in patients with
this condition (13). Further study
is required to investigate this association in the future.
Clinically, Hansel et al reported that 50% of
21 carcinoid tumor patients studied were younger than 50-years-old,
and that the tumor showed no tendencies in gender and location.
Bloody urine and pain in the lower back proved to be the most
common clinical manifestations. Horseshoe kidneys was frequently
present, while no other characteristics were known to distinguish
renal cell carcinoma on imaging. Endocrine syndrome was not found
in the blood examination (15). The
current study reports the case of a 49-year-old female who
presented with painless and gross hematuria. A horseshoe kidney on
imaging was a contributory factor for the diagnosis.
Pathological examination remains the gold standard
of diagnosis for renal carcinoid tumors (15,16). Under
the microscope, the classic histological characteristics of renal
carcinoid tumors are a band or ribbon-like pattern accompanied by
solid nests of cells and adenoid structures within a loose stroma.
Rosette structures are characteristic of these lesions, however,
this was not found in the present case. Tumor cells are similar in
size, with a granular eosinophilic cytoplasm. Round to oval nuclei
are uniform, with rare mitotic events. Used together with
histological features, neuroendocrine immunostaining would aid in
distinguishing carcinoid tumors from other diagnoses, such as small
cell carcinoma, pheochromocytoma and primitive neuroectodermal
tumor. With regard to the present case, a diagnosis of renal
carcinoid tumor may have been regarded as presumptive based on the
observation of typical morphological characteristics by light
microscopy, as this is subject to validation by positive
immunohistochemical staining of cytokeratin, vimentin and endocrine
markers (CgA, Syn or CD56 protein).
No standard therapy focusing on renal carcinoid
tumors has yet been proposed and surgical resection is currently
the only treatment (17).
Hormonotherapy may be a novel method aimed at patients with
positive ER and PR expression. Necrosis, metastasis, an age of
>50 years, a tumor diameter >4 cm and more karyokinesis are
presumed to potentially indicate an ominous prognosis. However, no
clear prognosis factors are generally accepted and further case
accumulation is required (18,19).
In conclusion, the current study presents the
clinical manifestations and pathological features of a case of
renal carcinoid tumor expressing ER and PR. The expression of ER
and PR in carcinoid tumors of the kidney is unusual, and these
molecules may be a potential therapeutic targets in such
patients.
Acknowledgements
This study was supported by the Project of
Administration of Traditional Chinese Medicine of Shandong Province
(grant no. 2009222).
References
|
1
|
Han X, Yu L, Yang S and Zheng J: Primary
neuroendocrine tumor of the testis: A study of clinicopathological
features. Int J Clin Exp Pathol. 7:1771–1776. 2014.PubMed/NCBI
|
|
2
|
Kaplan AL, Margolis DJ, Said J and Chin
AI: Primary carcinoid tumor of urinary bladder discovered on pelvic
magnetic resonance imaging. Urology. 80:e55–57. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pavel M, Hörsch D, Caplin M, et al:
Telotristat etiprate for carcinoid syndrome: A single-arm,
multicenter trial. J Clin Endocrinol Metab. 100:1511–1519. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chi Y, Du F, Zhao H, Wang JW and Cai JQ:
Characteristics and long-term prognosis of patients with rectal
neuroendocrine tumors. World J Gastroenterol. 20:16252–16257.
2014.PubMed/NCBI
|
|
5
|
Roy S, Hooda S, Huang GJ, Pantanowitz L
and Parwani AV: A novel case of concurrent renal tumors:
chromophobe renal cell carcinoma and carcinoid tumor of the kidney
with brief review of renal neuroendocrine tumors. Int J Surg
Pathol. 20:531–535. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kato Y, Nakamura K, Yamada Y, et al: A
rare case of metastatic renal carcinoid. BMC Urol. 10:222010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Litwinowicz R, Szpor J, Januś G, et al:
Primary carcinoid tumour in horseshoe kidney. Pol J Pathol.
62:72–74. 2011.PubMed/NCBI
|
|
8
|
Eble JN, Sauter G, Epstein JI and
Sesterhenn IA: Renal carcinoid tumourWorld Health Organization
Classification of Tumors. Pathology and Genetics of Tumors of the
Urinary System and Male Genital Organs. 3rd. IARC Press; Lyon,
France: pp. 812004
|
|
9
|
Raslan WF, Ro JY, Ordonez NG, et al:
Primary carcinoid of the kidney. Immunohistochemical and
ultrastructural studies of five patients. Cancer. 72:2660–2666.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Takeshima Y, Inai K and Yoneda K: Primary
carcinoid tumor of the kidney with special reference to its
histogenesis. Pathol Int. 46:894–900. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lodding P, Hugosson J and Hansson G:
Primary carcinoid tumour with ossification masquerading as calyx
stone in a horseshoe kidney. Scand J Urol Nephrol. 31:575–578.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kuroda N, Tanaka A, Ohe C, et al: Review
of renal carcinoid tumor with focus on clinical and pathobiological
aspects. Histol Histopathol. 28:15–21. 2013.PubMed/NCBI
|
|
13
|
Liang JJ, Alrawi S, Fuller GN and Tan D:
Carcinoid tumors arising in tailgut cysts may be associated with
estrogen receptor status: case report and review of the literature.
Int J Clin Exp Pathol. 1:539–543. 2008.PubMed/NCBI
|
|
14
|
Viale G, Doglioni C, Gambacorta M, Zamboni
G, Coggi G and Bordi C: Progesterone receptor immunoreactivity in
pancreatic endocrine tumors. An immunocytochemical study of 156
neuroendocrine tumors of the pancreas, gastrointestinal and
respiratory tracts, and skin. Cancer. 70:2268–2277. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hansel DE, Epstein JI, Berbescu E, Fine
SW, Young RH and Cheville JC: Renal carcinoid tumor: A
clinicopathologic study of 21 cases. Am J Surg Pathol.
31:1539–1544. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Canacci AM and MacLennan GT: Carcinoid
tumor of the kidney. J Urol. 180:21932008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kawajiri H, Onoda N, Ohira M, et al:
Carcinoid tumor of the kidney presenting as a large abdominal mass:
Report of a case. Surg Today. 34:86–89. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
McCaffrey JA, Reuter VV, Herr HW,
Macapinlac HA, Russo P and Motzer RJ: Carcinoid tumor of the
kidney. The use of somatostatin receptor scintigraphy in diagnosis
and management. Urol Oncol. 5:108–111. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Romero FR, Rais-Bahrami S, Permpongkosol
S, Fine SW, Kohanim S and Jarrett TW: Primary carcinoid tumors of
the kidney. J Urol. 176:2359–2366. 2006. View Article : Google Scholar : PubMed/NCBI
|