Introduction
Hepatic epithelioid angiomyolipoma (EAML), a
recently recognized subtype of AML, is very rare. At present, only
sporadic cases have been reported. It is difficult to diagnose
hepatic EAML prior to surgery, as there are no specific clinical,
laboratory or radiological signs of the disease (1,2). Recently,
the use of gadolinium ethoxybenzyl diethylenetriamine pentaacetic
acid (Gd-EOB-DTPA) as a liver-specific magnetic resonance (MR)
contrast agent has been shown to be useful for improving the
detection and characterization of hepatic lesions (3–5). In
addition, diffusion-weighted (DW) MR imaging (MRI) is increasingly
being applied as a liver imaging technique to differentiate between
benign and malignant diseases by measuring the value of the
apparent diffusion coefficient (ADC) based on extracellular water
diffusion (6,7). Although several case studies have
reported imaging findings of hepatic EMAL with ultrasonography,
computed tomography and MRI (1), to
the best of our knowledge, this is the first study to describe the
imaging findings of hepatic EMAL using Gd-EOB-DTPA-enhanced and DW
MRI. In addition, the study compared the imaging and pathological
findings of the disease. Written informed consent was obtained from
the patient for publication of this study.
Case report
On February 20, 2012, a 23-year-old female
experienced discomfort in the right upper quadrant of the abdomen
for 5 days prior to hospitalization in the Northern Jiangsu
People's Hospital (Yangzhou, Jiangsu, China). The physical
examination indicated that the abdomen was soft, but not tender.
The lower margin of the liver could be detected at approximately
three-fingers distance from the right subcostal region, and there
was no percussion pain around the hepatic area. The patient had no
medical history of hepatitis and infectious diseases, such as
schistosomiasis, and the patient did not use oral contraceptives.
The results of serum examination showed an α-fetoprotein (AFP)
level of 1.92 ng/ml (normal range, 0–7 ng/ml) and a
carcinoembryonic antigen level of 1.66 ng/ml (normal range, 0–5
ng/ml).
MRI of the upper abdomen was also performed using a
3.0-Tesla MR Scanner (Signa HDx; GE Medical Systems, Milwaukee, WI,
USA). Axial T1-weighted imaging (WI), T2WI (fat saturation), DWI (b
value, 0; 500 sec/mm2), and liver acquisition with
volume acceleration (dynamic contrast enhancement) were used after
Gd-EOB-DTPA (Primovist, Bayer-Schering, Berlin, Germany) was
injected manually at 0.025 mmol/kg body weight.
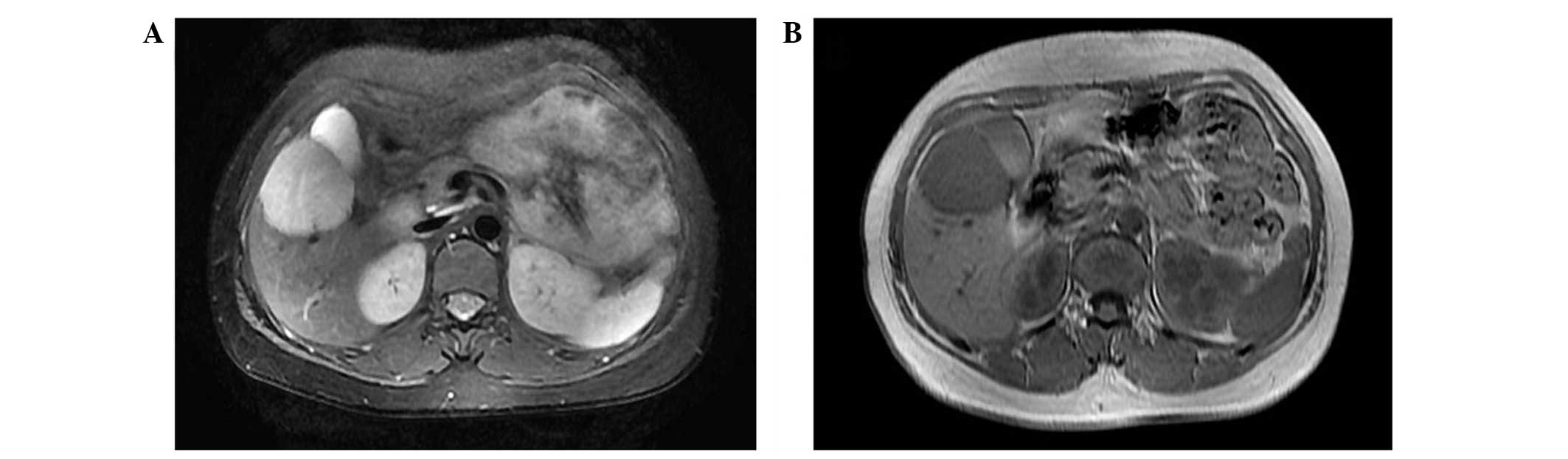
An MRI scan of the abdomen showed an ~5.6-cm,
well-defined, round tumor in segment 5 of the right hepatic lobe.
The tumor showed a heterogeneous high signal intensity on T2WI
(Fig. 1A) and a homogeneous low
signal intensity on T1WI (Fig. 1B).
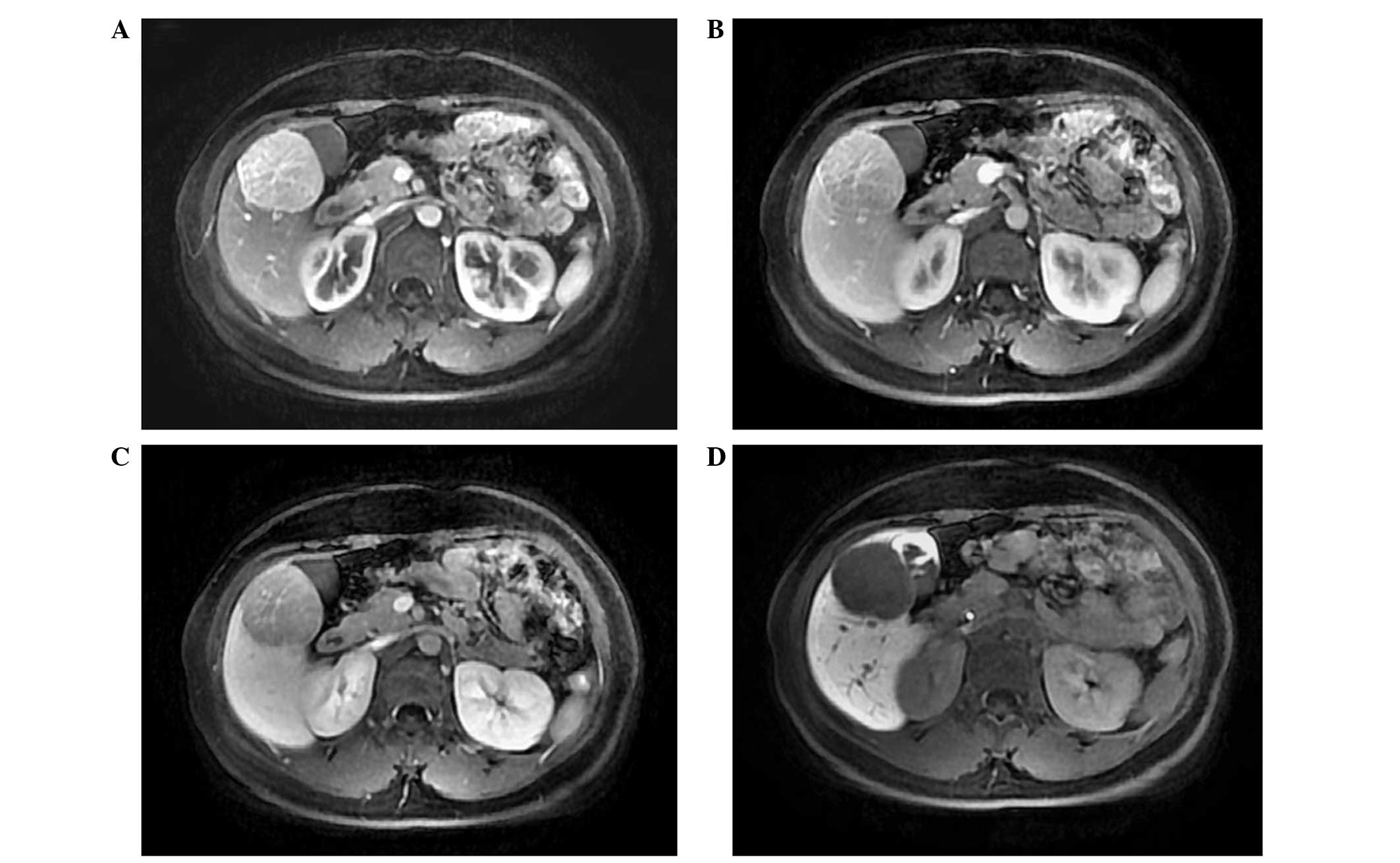
Gd-EOB-DTPA-enhanced MRI showed markedly heterogeneous enhancement
in the arterial phase, and central filiform vessels and capsule
enhancement were also observed (Fig.
2A). The signal intensity of the lesion was relatively reduced
in the portal venous phase, but remained slightly higher than the
surrounding liver parenchyma (Fig.
2B), and the enhanced signal intensity of the vascular image
was visualized within the tumor. The signal intensity of the lesion
was lower than the surrounding liver parenchyma in the delay phase
(Fig. 2C). The signal intensity of
the tumor was relatively homogeneous, but markedly lower compared
with that of the liver parenchyma, as a defect in the hepatobiliary
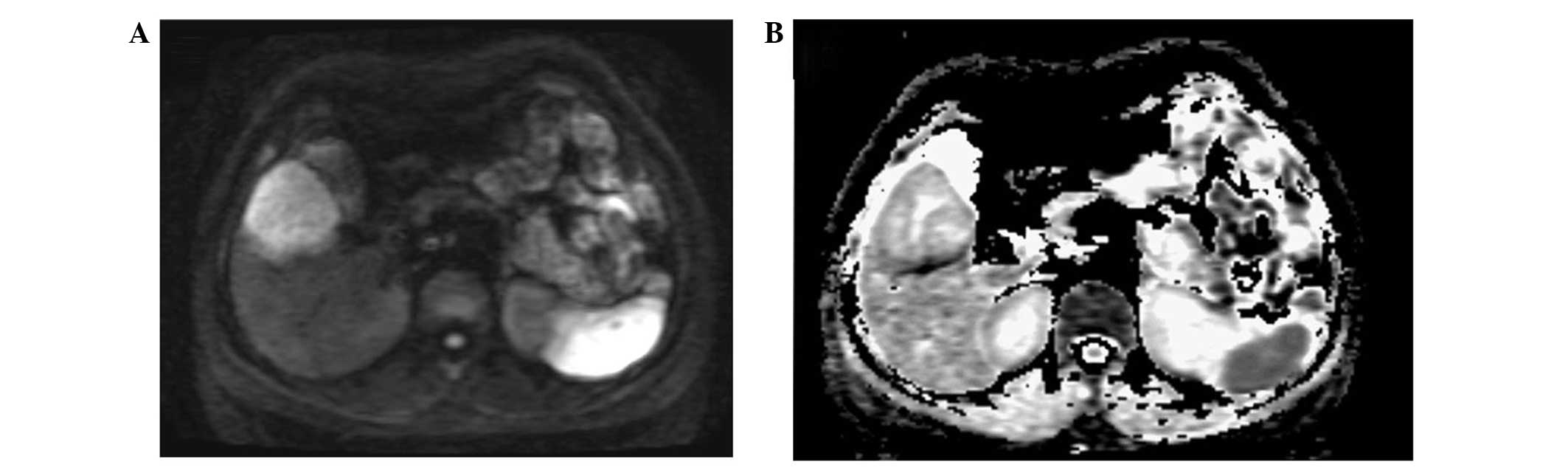
phase (Fig. 2D). Moreover, a high
signal intensity on DWI (b value, 500 sec/mm2) was
obtained for hepatic EAML (Fig. 3A),
with an average ADC value of 1.99×10−3
mm2/sec, which was higher than that of the normal liver
parenchyma (1.45×10−3 mm2/sec) (Fig. 3B).
During the surgery, it was found that the tumor was
soft with a clear margin from the surrounding, and the tumor was
delicate yellowish brown at the section, without any marked
abnormality in the surrounding liver parenchyma. The right lobe of
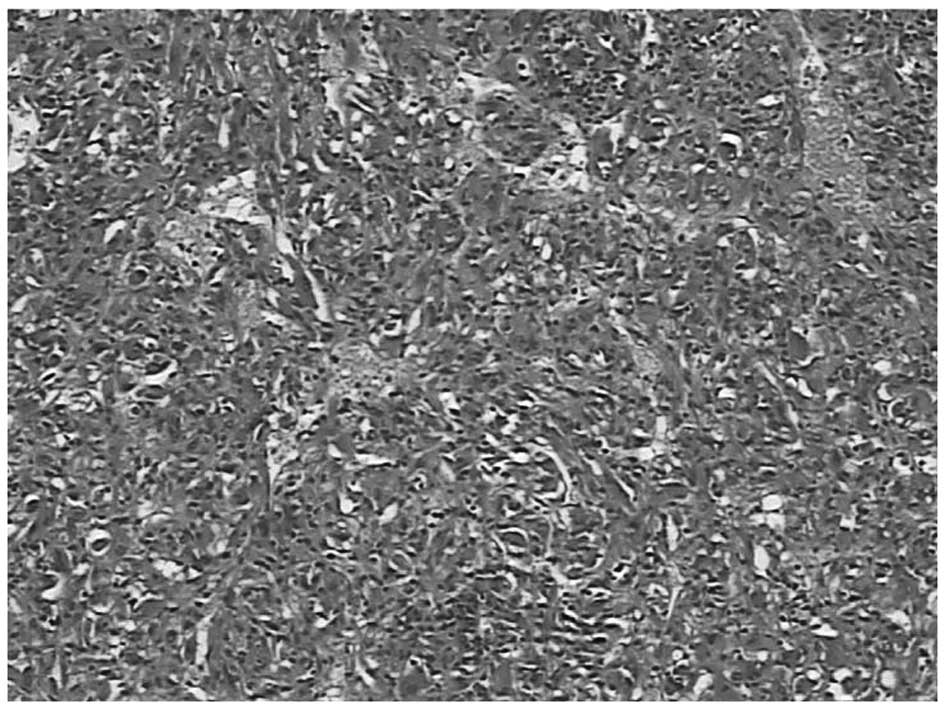
the liver was resected, and a pathological examination revealed
oval or epithelioid-like tumor cells, with abundant cytoplasm.
Vascular proliferation and a small amount of fat cells were also
found within the tumor (Fig. 4). The
immunohistochemical examination indicated that the tumor was
positive for human melanoma black 45 (HMB45), smooth muscle actin
(SMA), cluster of differentiation (CD)31 and CD34 staining, and
negative for AFP, pan-cytokeratin and S100. On the basis of these
findings, the patient was diagnosed with an EMAL of the liver. The
patient was healthy and free from recurrence at follow-up MRI
scans, which were performed at 6 months and 1 year
post-surgery.
Discussion
Hepatic EAML is a rare variant of AML that is formed
almost entirely from epithelioid cells, with a proliferation of
abnormal blood vessels and fewer or no lipocytes (8). Hepatic EAML commonly occurs in women in
the right lobe of the liver. Patients with hepatic EAML usually
have no specific clinical manifestations or physical signs,
although with an increase in tumor size, certain patients may
exhibit symptoms caused by tumor compression; however, results of
all the laboratory examinations are usually negative. The diagnosis
of EAML depends on the immunohistochemical examination (9), and the characteristic immunophenotype is
dual positive for the expression of melanoma cells and smooth
muscle cells, while the epithelial cell marker is negative. HMB45,
one of the melanocytic markers, is the most sensitive marker, and
SMA is the major marker for smooth muscle cells.
Epithelioid AML has uncertain malignant potential,
and there have been rare cases of tumor recurrence, vascular
invasion and metastases (10–12). Surgical resection should be considered
for all symptomatic patients, who should be followed up after
surgery.
The studies that previously described MRI findings
(13–15) reported that hepatic EAML commonly
occurred as a solitary lesion, which was hypointense on T1WI and
hyperintense on T2WI. The tumor was reported as moderately or
markedly enhanced, but with heterogeneous signal intensity by
Gd-DTPA dynamic scanning at the arterial phase (13–15), and
the signal intensity was higher or at least no less than the
surrounding liver parenchyma at the portal venous phase, although
the signal intensity was relatively reduced compared with the
signal intensity at the arterial phase. In general, the Gd-DTPA
dynamic scanning shows the feature of a quick wash-in and slow
wash-out. In addition, the image of the punctiform or filiform
vessels could be observed in the tumor, and the pseudocapsule was
visible as well. The Gd-EOB-DTPA-enhanced three-phase scan used in
the current study was similar to that of the Gd-DTPA-enhanced scan
reported in the literature, as Gd-EOB-DTPA shows a
vascular-interstitial distribution in the first minutes after bolus
injection, thus enabling a standard dynamic study of the liver
(3–5).
This agent is also known as gadoxetic acid disodium, and is a
hepatocyte-specific contrast agent that the urinary and biliary
systems eliminate in equal quantities. As a consequence of
hepatocyte uptake, normal liver areas exhibit T1 shortening,
whereas focal liver lesions without hepatocytes do not. Gd-EOB-DTPA
has been shown to be useful in the detection of focal malignant
liver lesions, including hepatocellular carcinoma and metastasis
(16,17). In the present patient, hepatic EAML
showed homogeneous and significantly lower signal intensity at the
hepatobiliary phase at 30 min post-Gd-EOB-DTPA injection compared
with the normal liver parenchyma. This may be due to the fact that
EAML is mainly composed of diffused epithelioid cells with diverse
morphologies, containing an abundant sinusoidal vascular network,
but lacking normal liver cells; therefore, the rate of the uptake
of Gd-EOB-DTPA is lower (8,9).
The hepatic EAML in the current study showed a high
signal intensity on DWI scans, with a higher ADC value than that of
the surrounding normal liver parenchyma. The main reason for this
was that the tumor consisted of proliferated epithelioid cells with
abundant cytoplasm and a lack of adipose tissue, which facilitated
the diffusion of water molecules within the tumor leading to the
high ADC value. In addition, EAML is a hypervascular lesion
composed of abundant sinusoid-like vessel networks and
segmentations in various sizes, which lead to increased
microperfusion and an increased ADC value (13,14).
The diagnosis of hepatic EAML must be differentiated
from that of hepatocellular carcinoma, focal nodular hyperplasia
(FNH) and hepatocellular adenoma, which are rich in blood vessels.
Hepatocellular carcinoma is usually associated with a medical
history of hepatitis B virus infection and cirrhosis, with an
increased serum AFP level; and the dynamic MRI scan demonstrates
the feature of a quick wash-in and quick wash-out. Certain
well-differentiated hepatocellular carcinoma cells maintain their
ability to uptake Gd-EOB-DTPA and present with relatively high
intensity in the liver-specific phase, while most hepatocellular
carcinoma cells show low intensity during the liver-specific phase
(5). The diffusion rate is limited in
hepatocellular carcinoma on DWI scans; therefore, the ADC value is
lower than that of the normal liver parenchyma (6,7,16). The signal intensity of an MRI scan for
FNH is close to that of the normal liver parenchyma, with star-like
scars in the middle of the lesion; it is characterized by a delayed
enhanced signal intensity during the dynamic enhanced MRI scan. FNH
could take up Gd-EOB-DTPA and induce an equivalent or higher signal
intensity compared with that of the normal liver parenchyma at the
hepatobiliary phase (17). In
addition, a higher signal intensity on the DWI scan and a higher
ADC value is also observed for FNH compared with the normal liver
parenchyma (6,7,18). Hepatic
adenoma often occurs in young and middle-aged women, who usually
have a long medical history of oral contraceptive use. The lesion
is often accompanied by an internal hemorrhage with degeneration of
the adipose tissue, and it is usually encapsulated. The MRI signal
intensity of hepatic adenoma is not homogeneous but has a clear
boundary from the surrounding tissues; the homogeneous and
persistent enhancement could be visualized during the enhanced
scanning. However, hepatic adenoma exhibits no vascular
malformation within the tumor on MRI scan. On Gd-EOB-DTPA-enhanced
hepatobiliary phase images, hepatic adenoma typically appears as
hypointense due to a lack of biliary canaliculi (19), while it has an equivalent or higher
signal intensity on DWI scan and a mildly higher ADC value than
that of the normal liver parenchyma (6,7).
In summary, the present study indicated that hepatic
EAML demonstrates specific features on dynamic Gd-EOB-DTPA-enhanced
and DWI scans, which could be used for the differential diagnosis
with other hypervascular hepatic tumors.
References
|
1
|
Xu PJ, Shan Y, Yan FH, Ji Y, Ding Y and
Zhou ML: Epithelioid angiomyolipoma of the liver: Cross-sectional
imaging findings of 10 immunohistochemically-verified cases. World
J Gastroenterol. 15:4576–4581. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lane BR, Aydin H, Danforth TL, Zhou M,
Remer EM, Novick AC and Campbell SC: Clinical correlates of renal
angiomyolipoma subtypes in 209 patients: Classic, fat poor,
tuberous sclerosis associated and epithelioid. J Urol. 180:836–843.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schuhmann-Giampieri G, Schmitt-Willich H,
Press WR, Negishi C, Weinmann HJ and Speck U: Preclinical
evaluation of Gd-EOB-DTPA as a contrast agent in MR imaging of the
hepatobiliary system. Radiology. 183:59–64. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Motosugi U, Ichikawa T, Sou H, Sano K,
Tominaga L, Muhi A and Araki T: Distinguishing hypervascular
pseudolesions of the liver from hypervascular hepatocellular
carcinomas with gadoxetic acid-enhanced MR imaging. Radiology.
256:151–158. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ahn SS, Kim MJ, Lim JS, Hong HS, Chung YE
and Choi JY: Added value of gadoxetic acid-enhanced hepatobiliary
phase MR imaging in the diagnosis of hepatocellular carcinoma.
Radiology. 255:459–466. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miller FH, Hammond N, Siddiqi AJ, Shroff
S, Khatri G, Wang Y, Merrick LB and Nikolaidis P: Utility of
diffusion-weighted MRI in distinguishing benign and malignant
hepatic lesions. J Magn Reson Imaging. 32:138–147. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Parikh T, Drew SJ, Lee VS, Wong S, Hecht
EM, Babb JS and Taouli B: Focal liver lesion detection and
characterization with diffusion-weighted MR imaging: Comparison
with standard breath-hold T2-weighted imaging. Radiology.
246:812–822. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tsui WM, Colombari R, Portmann BC, Bonetti
F, Thung SN, Ferrell LD, Nakanuma Y, Snover DC, Bioulac-Sage P and
Dhillon AP: Hepatic angiomyolipoma: A clinicopathologic study of 30
cases and delineation of unusual morphologic variants. Am J Surg
Pathol. 23:34–48. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ren N, Qin LX, Tang ZY, Wu ZQ and Fan J:
Diagnosis and treatment of hepatic angiomyolipoma in 26 cases.
World J Gastroenterol. 9:1856–1858. 2003.PubMed/NCBI
|
|
10
|
Nguyen TT, Gorman B, Shields D and Goodman
Z: Malignant hepatic angiomyolipoma: Report of a case and review of
literature. Am J Surg Pathol. 32:793–798. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Graziano A, Santangelo M and Umana DS:
Clinical evaluation of epithelioid angiomyolipoma. Ann Ital Chir.
79:135–138. 2008.PubMed/NCBI
|
|
12
|
Xie L, Jessurun J, Manivel JC and
Pambuccian SE: Hepatic epithelioid angiomyolipoma with trabecular
growth pattern: A mimic of hepatocellular carcinoma on fine needle
aspiration cytology. Diagn Cytopathol. 40:639–650. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Agaimy A, Vassos N, Croner RS, Strobel D
and Lell M: Hepatic angiomyolipoma: A series of six cases with
emphasis on pathological-radiological correlations and unusual
variants diagnosed by core needle biopsy. Int J Clin Exp Pathol.
5:512–521. 2012.PubMed/NCBI
|
|
14
|
Ji JS, Lu CY, Wang ZF, Xu M and Song JJ:
Epithelioid angiomyolipoma of the liver: CT and MRI features. Abdom
Imaging. 38:309–314. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhao Y, Ouyang H, Wang X, Ye F and Liang
J: MRI manifestations of liver epithelioid and nonepithelioid
angiomyolipoma. J Magn Reson Imaging. 39:1502–1508. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Xu PJ, Yan FH, Wang JH, Shan Y, Ji Y and
Chen CZ: Contribution of diffusion-weighted magnetic resonance
imaging in the characterization of hepatocellular carcinomas and
dysplastic nodules in cirrhotic liver. J Comput Assist Tomogr.
34:506–512. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zech CJ, Grazioli L, Breuer J, Reiser MF
and Schoenberg SO: Diagnostic performance and description of
morphological features of focal nodular hyperplasia in
Gd-EOB-DTPA-enhanced liver magnetic resonance imaging: Results of a
multicenter trial. Invest Radiol. 43:504–511. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Donati F, Boraschi P, Gigoni R, Salemi S,
Falaschi F and Bartolozzi C: Focal nodular hyperplasia of the
liver: Diffusion and perfusion MRI characteristics. Magn Reson
Imaging. 31:10–16. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Grazioli L, Morana G, Kirchin MA and
Schneider G: Accurate differentiation of focal nodular hyperplasia
from hepatic adenoma at gadobenate dimeglumine-enhanced MR imaging:
prospective study. Radiology. 236:166–177. 2005. View Article : Google Scholar : PubMed/NCBI
|