Introduction
Paraneoplastic syndromes are the manifestation of an
underlying malignancy, which may be hidden, and their pathogenesis
is complicated and largely remains to be elucidated. Manifestations
of rheumatic disease, particularly arthritis, may be an initial
presentation of a paraneoplastic phenomenon that suggests
malignancy. Leukemia cases, particularly acute lymphocytic leukemia
(ALL), frequently present with arthritic manifestations in
childhood, (1) which may lead to the
misdiagnosis of rheumatic disease. The peak incidence of ALL is in
childhood, arthritic manifestations can occur in 15–30% of ALL
cases especially in children at disease onset, when peripheral
blood changes are subtle or even absent (2). ALL frequently affects peripheral joints,
while axial spine involvement is rarely observed. Sacroiliitis is a
common manifestation of spondyloarthritis, which can be clarified
by computer tomography scan of sacroiliac joint (1). Sacroiliitis as an initial manifestation
of leukemia mimicking spondyloarthritis is rare; only one similar
case was reported in published literature before. Clinicians should
be aware that spondyloarthritis may be the onset manifestation of
ALL when atypical symptoms and laboratory results are observed.
Morphological, immunological phenotype and cytochemical examination
of bone marrow are important to identify and classify the
underlying leukemia. Chemotherapy appears to have positive effects
on arthritic symptoms in these patients. The current study presents
the case of an 18-year-old adolescent male who presented with
sacroiliitis, and who was eventually diagnosed with ALL. The
relevant literature concerning leukemic arthritis (LA) is
additionally reviewed.
Case report
An 18-year-old male presented to the Department of
Rheumatology, The First Affiliated Hospital (School of Medicine,
Zhejiang University, Hangzhou, Zhejiang, China) in January 2012
with pain in the lower back and left knee. The lower back pain had
been apparent for 4 months, and persisted day and night without
morning stiffness. Resting did not relieve the pain. The symptom
was progressive and became gradually unbearable. The patient
experienced pain in the left knee without joint swelling 1 month
prior to presenting to the hospital. There was no family history of
any arthritic disorders or any form of spondyloarthritis. Computed
tomography scans of the sacroiliac joints revealed mild bilateral
erosions (Fig. 1), and non-steroidal
anti-inflammatory drugs (NSAIDs; meloxicam, 7.5 mg twice a day)
were administered, however, the patient demonstrated no
response.
Physical examination revealed that the patient's
body temperature was 38°C and purple-red papules were scattered
throughout the anterior chest wall. Sternum tenderness was not
observed. The spleen was significantly enlarged. No swelling lymph
nodes were present. The sacroiliac joints were bilaterally tender
on palpation. The left knee was tender without swelling. Lumbar
spine motion was not decreased.
Routine blood examination revealed the following: A
hemoglobin level of 105 g/l (normal range, 131–172 g/l), a platelet
count 99×109/l (normal range, 100–300×109/l),
a white blood cell count of 5.1×109/l (normal range,
4.0–10.0×109/l), a neutrophil count of
1.1×109/l (normal range, 2.0–7.0×109/l), a
lymphocyte count of 2.1×109/l (normal range,
0.8–4.0×109/l) and a monocyte count of
1.86×109/l (normal range, 0.12–1.0×109/l),
with 22.1% neutrophils (normal range, 50.0–70.0%), 40.2%
lymphocytes (normal range, 20.0–40.0%) and 36.3% monocytes (normal
range, 3.0–10.0%, indicating a slight decrease in neutrophils,
hemoglobin and platelets, but a significant increase in monocytes.
Trace levels of urinary protein were observed. The level of serum
high-sensitivity C-reactive protein was 39.2 mg/l (normal range,
0–8.0 mg/l), and the erythrocyte sedimentation rate was 20 mm/h
(normal range, 0–15 mm/h), indicating elevation. Tests for human
leukocyte antigen (HLA)-B27, rheumatoid factor, anti-neutrophil
cytoplasmic antibody and antinuclear antibody were negative.
Abnormally decreased levels of immunoglobulin (Ig)A (35.7 mg/dl;
normal range, 90–450 mg/dl), IgG (649.0 mg/dl; normal range,
800–1,800 mg/dl) and IgM (33.2 mg/dl; normal range, 60–280 mg/dl)
revealed hypoglobulinemia. An abdominal Doppler ultrasound revealed
significant splenomegaly and kidney swelling with manifestations of
nephropathy. Abnormal cells were detected by microscopic
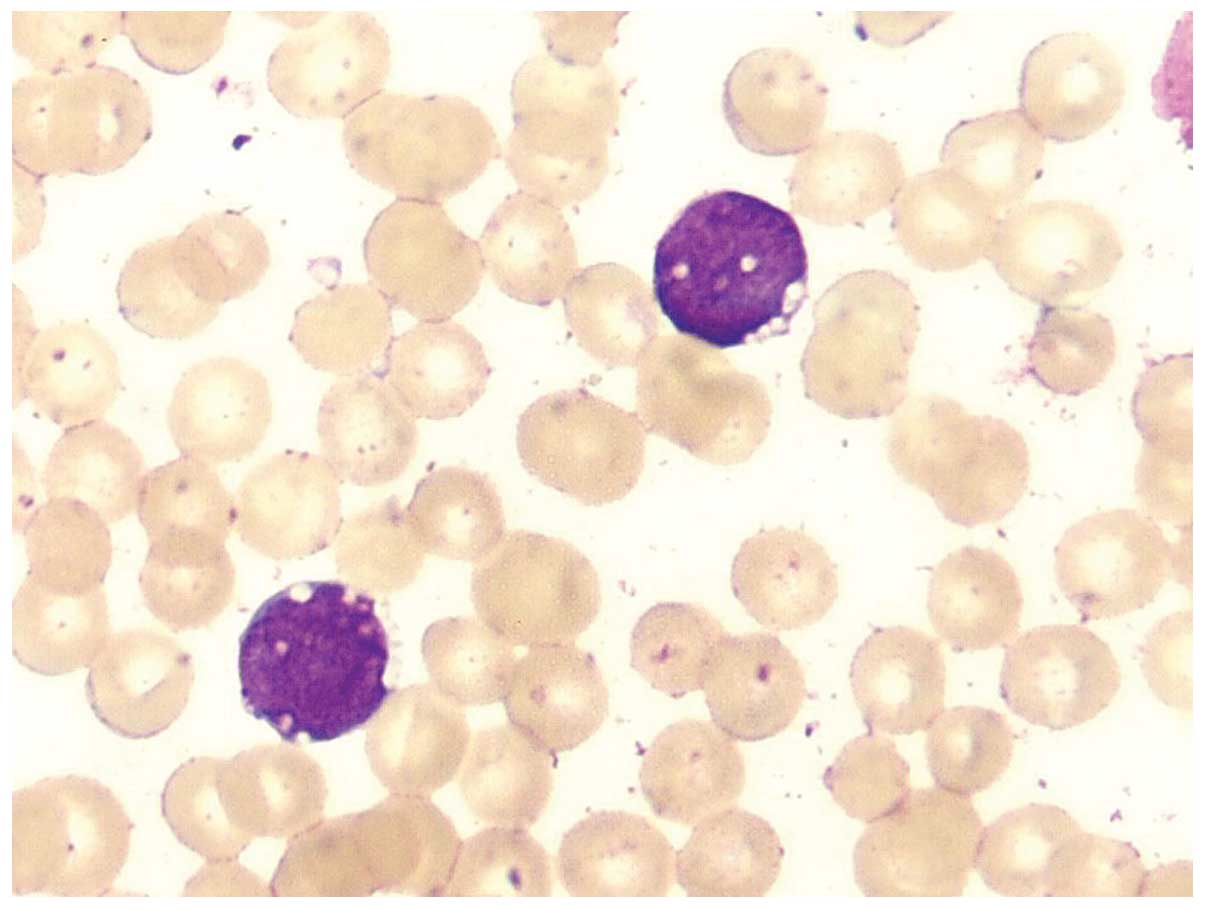
examination of peripheral blood smears. Bone marrow aspiration was
performed, revealing marked lymphocytes, including many primitive
lymphocytes and prolymphocytes (86%; Fig.
2). Immunophenotypic analysis revealed that the blasts were
positive for cluster of differentiation (CD)19, CD22, cytoplasmic
IgM and HLA-DR, and pre-B-cell ALL was indicated. The manifestation
of sacroiliitis mimicking spondyloarthritis was proven to be a
paraneoplastic phenomenon of ALL.
A total of 1 week after the administration of
chemotherapy (Idarubicin, 15 mg; cyclophosphamide, 1,200 mg;
vindesine, 4 mg; once a week), the patient's arthritic symptoms
were dramatically relieved without administration of any NSAIDs,
which further suggested that sacroiliitis was an onset presentation
of ALL in the present patient. During >2 years of follow-up, the
patient experienced a complete remission and did not develop any
lower back pain. Computed tomography scans of the sacroiliac joints
were stable compared with those performed 2 years previously.
Discussion
Paraneoplastic syndromes are the manifestation of an
underlying malignancy that may be hidden and may be caused by
various tumor effects, including substances released by tumor
cells, for example hormones, peptides and antibodies, or
immunological and other host reactions to the tumor (3). The pathogenesis of paraneoplastic
syndrome is complicated and largely remains to be elucidated.
Manifestations of rheumatic disease, including arthritis, myositis,
lupus-like syndrome and vasculitis, may be an initial presentation
of malignancy in the form of paraneoplastic syndrome. Rheumatic
symptoms may complicate diagnosis, but are significant indicators
of an underlying malignancy.
Leukemic arthritis (LA) is a major form of
paraneoplastic rheumatic syndrome, which may be defined as joint
pain and swelling associated with peripheral blood or bone marrow
leukemia, following the exclusion of alternative causes of
arthritis (4). Potential pathogenic
mechanisms for LA include hemorrhage into the joint due to
thrombocytopenia, infiltration of leukemic cells into synovial
tissue, immune complex-induced synovitis and synovial reaction to
periosteal or capsular infiltration. However, synovial infiltration
of leukemic cells appears to be the primary mechanism (5). Peripheral joints are frequently affected
in LA mimicking rheumatoid arthritis, while axial joints, including
the sacroiliac joint, are rarely affected (6,7).
Sacroiliitis as the onset symptom of malignancy is rare. To the
best of our knowledge, the present patient is only the second case
of ALL initially presenting with sacroiliitis reported in the
relevant literature.
Leukemia presenting with arthritis has been reported
in a small number of cases, while sacroiliitis at onset
presentation is rare. In the previous literature, only two cases of
leukemia initiated with sacroiliitis have been reported. In one
case report, a 28-year-old woman rapidly developed acute myeloid
leukemia 1 month after the diagnosis of myelodysplastic syndrome
with sacroiliitis (6). In another
case report, a 17-year-old male patient was admitted to hospital
due to experiencing a fever, lower back pain and knee pain for a
number of months. A complete blood count revealed pancytopenia, and
ALL was ultimately diagnosed (7). To
the best of our knowledge, the present patient is the second case
of ALL presenting with sacroiliitis reported in the relevant
literature. Spondyloarthritis is a chronic inflammatory disease,
primarily involving the axial spine and the sacroiliac joint
(8). The condition typically occurs
in young males and has a strong polygenic predisposition.
Sacroiliitis tends to be the early manifestation of
spondyloarthritis (8). The initial
symptom is typically chronic lower back pain, which is often severe
at rest, relieved by physical activity and accompanied by morning
stiffness (8). In the current study,
the patient presented with chronic lower back pain, and
sacroiliitis was indicated by imaging. Furthermore, an elevated
erythrocyte sedimentation rate and high C-reactive protein level
were observed, mimicking spondyloarthritis. Subtle abnormalities in
blood counts, an enlarged spleen and a poor response to NSAIDs were
indicators of ALL. Clinicians should consider that
spondyloarthritis may be the onset manifestation of ALL, although
this is rare.
Infiltration, including into the bone, joints,
liver, spleen or lymph nodes, is common in ALL, and ALL is prone to
complications due to paraneoplastic rheumatic syndrome,
particularly arthritic manifestations (9). As ALL typically affects children aged
3–7, and the majority of childhood leukemia cases are ALL,
childhood LA is common while adult LA is rarely observed (1) Childhood LA is liable to be misdiagnosed
as juvenile idiopathic arthritis (JIA). Marwaha et al
(10) retrospectively analyzed the
case records of 762 patients exhibiting ALL. The age of onset
ranged from 1–14 years, and 49 patients (6.4%) had an initial
presentation that mimicked JIA. This subset of ALL patients may
possess an improved prognosis and included an increased percentage
of patients opting for therapy or those with a lower total
leukocyte count, a higher platelet count and a reduced degree of
anemia. Large joints of the limbs were most commonly affected,
including the knee, ankle, hip, wrist, elbow and shoulder, while
the spine and sacroiliac joint were not mentioned (10). Although peripheral joint involvement
is common in LA, axial spinal involvement in leukemia should
additionally be considered during the differential diagnosis.
LA is associated with monocytic leukemia in adults,
potentially due to the significant role of monocytes in the
pathogenic mechanism of arthritis. Acree et al (11) initially reported the association
between adult LA and leukemia of monocytic differentiation. The
study identified that four cases investigated in their study, and
the majority of the prior reported cases of adult LA, were
monocytic leukemia, indicating that adult LA occurs in association
with leukemia of monocytic differentiation (11). Monocyte-attracting cytokines,
including tumor necrosis factor α, have a significant role in
osteoarthritis and rheumatoid arthritis via mediation of and
increasing monocyte migration into the inflamed joint space. Acree
et al (11) hypothesized that
leukemic monocytes, identical to their benign counterparts, may
migrate to sites of inflamed joints in response to
monocyte-attracting cytokines, which may be critical in the
mechanism of LA. Although the present case was not monocytic
leukemia, there were significantly increased levels of monocytes
(1.86×109/l; 36.3%). Increased monocyte levels may
additionally have had a significant role in the mechanism of LA in
the present case.
In the current relevant literature, clinical
features, including night pains, alterations in blood counts, an
absence of response to NSAID therapy and a fever, were considered
to be suspected symptoms of ALL (10,12,13). A low
platelet count and night pain that wakes a child from sleep appear
to be particularly sensitive indicators of ALL with arthritic
symptoms (12,13). For these patients, the examination of
blood smears, bone scans and bone marrow examination should be
conducted to exclude the possibility of ALL. In the present case
report, a fever, a poor response to NSAID therapy, an enlarged
spleen, anemia, a low platelet count and a low neutrophil count
indicated the underlying hematological malignancy.
In conclusion, sacroiliitis may be a rare onset
presentation of ALL. For patients exhibiting arthritic symptoms,
particularly children and adolescents, atypical clinical features
such as any subtle abnormalities in blood count and poor responses
to therapy, indicate the requirement to exclude the possibility of
acute leukemia. Early diagnosis is critical for treatment, and
chemotherapy is frequently effective for treatment of the
paraneoplastic rheumatic syndrome caused by ALL.
References
|
1
|
Usalan C, Ozarslan E, Zengin N, Büyükaýk Y
and Güllü YH: Acute lymphoblastic leukaemia presenting with
arthritis in an adult patient. Postgrad Med J. 75:425–427. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jones OY, Spencer CH, Bowyer SL, Dent PB,
Gottlieb BS and Rabinovich CE: A multicenter case control study on
predictive factors distinguishing childhood leukemia from juvenile
rheumatoid arthritis. Pediatrics. 117:e840–e844. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Andras C, Csiki Z, Ponyi A, Illés A and
Dankó K: Paraneoplastie rheumatic syndromes. Rheumatol Int.
26:376–382. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Luzar MJ and Sharma HM: Leukemia and
arthritis: Including reports on light immunofluorescent, and
electron microscopy of the synovium. J Rheumatol. 10:132–135.
1983.PubMed/NCBI
|
|
5
|
Taillan B, Leyge JF, Fuzibet JG, Nectoux
F, Ziegler G and Dujardin P: Knee arthritis revealing acute
leukemia in a patient with rheumatoid arthritis. Clin Rheumatol.
10:76–77. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hoshino T, Matsushima T, Saitoh Y, Yamane
A, Takizawa M, Irisawa H, Saitoh T, Handa H, Tsukamoto N, Karasawa
M, et al: Sacroiliitis as an initial manifestation of acute
myelogenous leukemia. Int J Hematol. 84:421–424. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Moghadam A, Talebi-Taher M and Dehghan A:
Sacroiliitis as an initial presentation of acute lymphoblastic
leukemia. Acta Clin Belg. 65:197–199. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dougados M and Baeten D:
Spondyloarthritis. Lancet. 377:2127–2137. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Appelbaum FR: The acute leukemias.
Wyngaarden JB, Smith LH and Bennett JC: Cecil Textbook of Medicine.
1:(19th). (Philadelphia, PA, USA). WB Saunders Company. 44–949.
1992.
|
|
10
|
Marwaha RK, Kulkarni KP, Bansal D and
Trehan A: Acute lymphoblastic leukemia masquerading as juvenile
rheumatoid arthritis, Diagnostic pitfall and association with
survival. Ann Hematol. 89:249–254. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Acree SC, Pullarkat ST, Quismorio FP Jr,
Mian SR and Brynes RK: Adult leukemic synovitis is associated with
leukemia of monocytic differentiation. J Clin Rheumatol.
17:130–134. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jones OY, Spencer CH, Bowyer SL, Dent PB,
Gottlieb BS and Rabinovich CE: A multicenter case-control study on
predictive factors distinguishing childhood leukemia from juvenile
rheumatoid arthritis. Pediatrics. 117:e840–e844. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gupta D, Singh S, Suri D, Ahluwalia J, Das
R and Varma N: Arthritic presentation of acute leukemia in
children, Experience from a tertiary care centre in North India.
Rheumatol Int. 30:767–770. 2010. View Article : Google Scholar : PubMed/NCBI
|