Introduction
Colorectal cancer (CRC) is one of the most frequent
cancers in Western countries, and the disease is delineated by
local recurrence and lymphatic and hematogenous dissemination
(1,2).
The results of in vivo and in vitro studies performed
in various tumor entities indicate that tumor progression and
organ-specific metastasis is partially affected by interactions
between chemokine receptors on cancer cells and the corresponding
chemokines expressed in target organs. Therefore, chemokine
receptors direct the spread of tumor cells and affect the sites of
metastatic growth (3). Chemokines and
the corresponding G-protein-coupled receptors have previously been
reported to mediate various immunoresponses (4). The high expression of stromal cell
derived factor 1 (SDF-1), also termed C-X-C motif chemokine ligand
12 (CXCL12), in endothelial cells, biliary epithelial cells, bone
marrow stromal cells and lymph nodes results in a chemotactic
gradient that attracts lymphocytes expressing C-X-C chemokine
receptor type 4 (CXCR4) to the respective organs (4–6).
CXCR4 has become a focus of studies, as it is the
most common chemokine receptor expressed on cancer cells (3). CXCR4 has been indicated to play an
important role in tumor dissemination in colorectal, breast and
oral squamous cell carcinoma, as these tumors all commonly
metastasize to SDF-1-expressing organs (7,8). Previous
studies that analyzed the metastatic ability of CXCR4-expressing
cancer cells using murine tumor models underlined the key role of
CXCR4 in tumor cell malignancy (9–13). The
activation of CXCR4 by SDF-1α has been reported to induce the
migration, invasion and angiogenesis of cancer cells (14–17). SDF-1
proteins are found as monomers in living organisms. Six isoforms of
SDF-1 exist, consisting of SDF-1α, SDF-1β, SDF-1γ, SDF-1δ, SDF-1ε
and SDF-1θ, due to alternative splicing. All isoforms possess the
same initial three exons and then differ from exon 4 onwards
(18,19). The best-known isoforms are SDF-1α and
SDF-1β. The functional diversity and differential proteolytic
processing properties of these two isoforms has been extensively
investigated and characterized (20,21).
However, little is known about the other isoforms.
In the present study, the expression of the various
SDF-1 isoforms and SDF-1 polymorphisms in tissue specimens obtained
from CRC patients was analyzed. These results were assessed for
associations between the clinicopathological parameters and overall
survival of the patients.
Materials and methods
Tissue samples
CRC tissue samples were intraoperatively obtained
from 73 patients, according to the ethical committee of the State
Chamber of Medicine in Rhineland-Palatinate, and were derived from
30 (41%) females and 43 (59%) males, with a median age at diagnosis
of 66.5 years. Written informed consent was obtained from all
patients. The morphological classification of the carcinoma was
performed according to World Health Organization (WHO)
specifications for the tumor-node-metastasis (TNM) classification.
The patients were followed up on a regular basis, depending on the
procedure performed.
Restriction fragment length
polymorphism (RFLP) assay
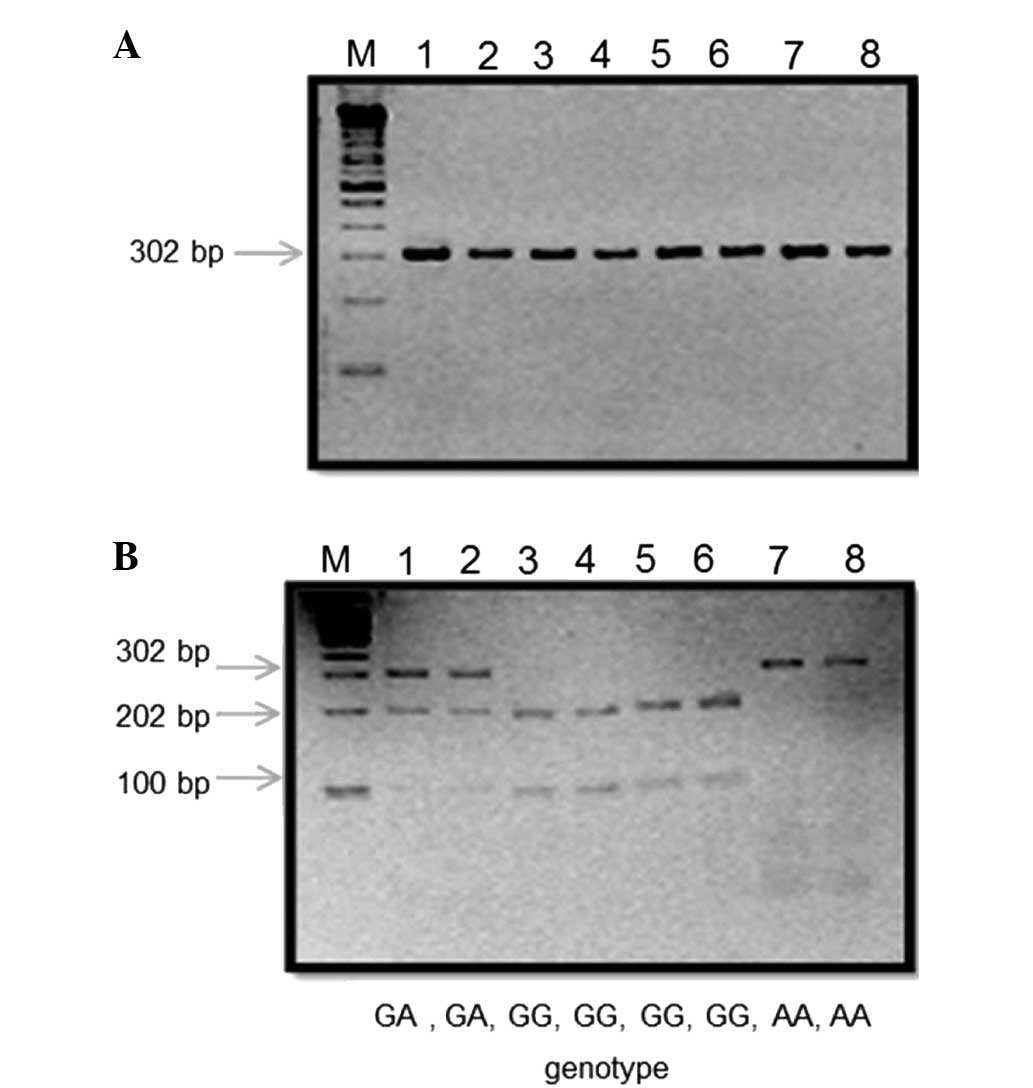
The presence of a polymorphism at codon 801 of the
SDF-1 gene was analyzed by RFLP analysis using cDNA obtained from
73 human CRC tissue specimens. Polymerase chain reaction (PCR) was
performed as described by Dimberg et al (22), using the 5′-CAGTCAACCTGGGCAAAGCC-3′
and 5′-AGCTTTGGTCCTGAGAGTCC-3′ primers (Eurofins Genomics,
Ebersberg, Germany). The resulting double-stranded DNA was then
digested using the restriction enzyme MspI. To visualize the
resulting DNA fragments, agarose gel electrophoresis was performed
(Fig. 1).
Analysis of CXCL12 splice variant
expression in human CRC and normal mucosa tissues by reverse
transcription (RT)-PCR
The expression of the CXCL12 splice variants SDF-1α,
SDF-1β, SDF-1γ, SDF-1δ, SDF-1ε and SDF-1θ was analyzed in 40 CRC
and 20 human mucosa cDNA samples obtained from a subgroup of the
aforementioned tissue samples. In order to determine the expression
patterns of the human SDF-1 isoforms in CRC and normal mucosal
tissues, PCR primers (Eurofins Genomics) that specifically detected
each SDF-1 isoform were designed as follows: SDF-1α forward,
5′-ATGAACGCCAAGGTCGTGGTC-3′ and reverse,
5′-AAGTGCTTACTTGTTTAAAGCTTTCTC-3; SDF-1β forward,
5′-ATGAACGCCAAGGTCGTGGTC-3′ and reverse,
5′-ACCCTCTCACATCTTGAACCTCTT-3′; SDF-1γ forward,
5′-ATGAACGCCAAGGTCGTGGTC-3′ and reverse,
5′-AGATAACTAGTTTTTCCTTTTCTGGGC-3′; SDF-1δ forward,
5′-ATGAACGCCAAGGTCGTGGTC-3′ and reverse,
5′-ACACCATTACACATCCCCAGGAGA-3′; SDF-1ε forward,
5′-CGCCATGAACGCCAAGGTCGTGGTCG-3′ and reverse,
5′-CTAATTACTTCAGTGGCAGATCATAC-3′; and SDF-1θ forward,
5′-CGCCATGAACGCCAAGGTCGTGGTCG-3′ and reverse,
5′-CACACTAATTACTTCAGTGGCAGATC-3′. β-actin was used as an internal
control for the tissue samples (23).
The PCR reactions were performed using an automated thermal cycler
(PTC-200; Bio Rad Laboratories GmbH, Munich, Germany).
Statistical analysis
The association between the SDF-1 G801A polymorphism
or isoform expression and the clinicopathological features of
patients was assessed using box plots and the Wilcoxon test if the
explanatory variable had 2 levels, or the Kruskal-Wallis test if
there were >2 levels of the explanatory variable. The
association between the patient age, β-actin expression and isoform
expression was determined using Pearson product-moment correlation
coefficient and reported as scatterplot matrices. P≤0.05 was
considered to indicate a statistical significant difference.
Statistical analysis was performed using SAS 9.2 software from SAS
Institute, Inc. (Cary, NC, USA).
Results
Association between SDF-1 isoforms and
clinicopathological parameters
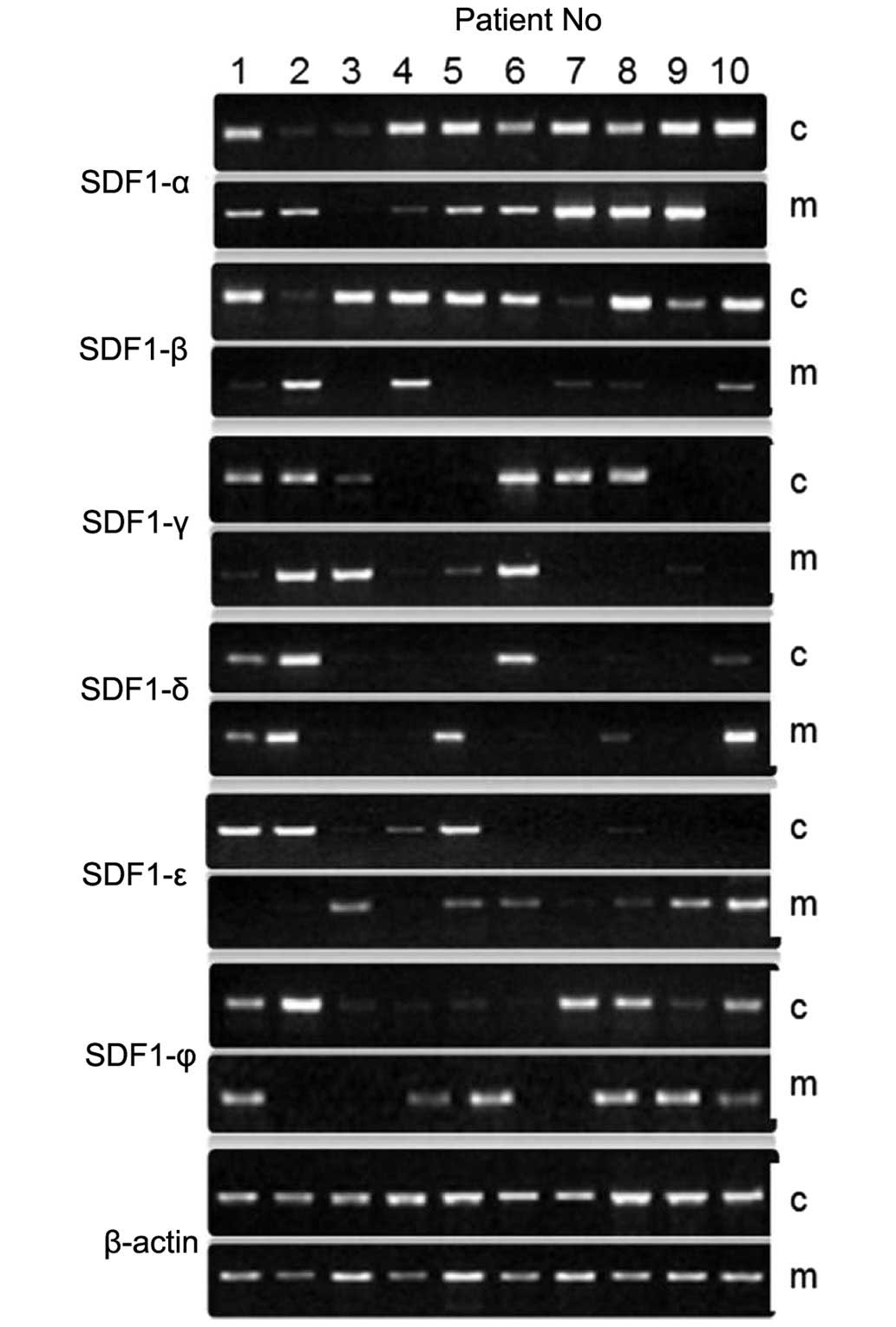
The expression of the CXCL12 splice variants SDF-1α,
SDF-1β, SDF-1γ, SDF-1δ, SDF-1ε, and SDF-1θ was evaluated in 40
established CRC and 20 normal mucosa tissue specimens. RT-PCR
analysis revealed that the mRNA of these SDF-1 splice variants was
expressed in CRC and normal mucosa tissues (Table I; Fig.
1). The expression rates of the SDF-1α, SDF-1β, SDF-1γ, SDF-1δ,
SDF-1ε and SDF-1θ splice variants were 80, 70, 50, 37.5, 30 or
32.5%, respectively. By contrast, the expression rates of the
SDF-1α, SDF-1 β, SDF-1γ, SDF-1δ, SDF-1ε or SDF-1θ splice variants
in the normal mucosa were 65, 50, 25, 40, 45 and 35%, respectively
(23).
 | Table I.Expression of SDF-1 isoforms in CRC
and normal mucosa tissues. |
Table I.
Expression of SDF-1 isoforms in CRC
and normal mucosa tissues.
| Isoform | Expression of SDF-1
isoforms in CRC tissue samples, n (%) | Expression of SDF-1
isoforms in normal mucosa tissue samples, n (%) |
|---|
| Total | 40
(100.0) | 20
(100.0) |
| SDF-1α | 32 (80.0) | 13 (65.0) |
| SDF-1β | 28 (70.0) | 10 (50.0) |
| SDF-1γ | 20 (50.0) | 5
(25.0) |
| SDF-1δ | 15 (37.5) | 8
(40.0) |
| SDF-1ε | 12 (30.0) | 9
(45.0) |
| SDF-1θ | 13 (32.5) | 7
(35.0) |
In total, 40 tumors obtained from 39 patients were
included in the present study. For 1 patient, clinical data was not
available. Out of the total 39 patients, 22 patients (56%) were
male. The analyzed tumors were located in the caecum in 3 patients
(8%), colon ascendens in 5 patients (13%), colon transversum in 1
patient (3%), colon descendens in 2 patients (5%), sigma in 13
patients (33%) and rectum in 15 patients (38%). The tumors were
stage T3 in 29 patients (74%), whereas 2 patients possessed T1
tumors (5%), 5 patients possessed T2 tumors (13%) and 3 patients
possessed T4 tumors (8%).
The median patient age was 65.7 years (standard
deviation, 10.7), with a range of 41–83 years. There was little
association between the categorical clinical parameters, such as
gender, tumor site or TNM stage and the expression of the SDF-1
isoforms, with the exception of two associations, consisting of
SDF-1β being associated with the presence of distant metastases
(P=0.0656) and SDF-1γ being significantly positively associated
with tumor size (P=0.0423) (23).
Genotype frequency
The CXCL12 splice variants were successfully
detected in all patient samples. The frequency of the GG CXCL12
allele was compared with the frequency of the GA and AA CXCL12
alleles for the patient gender, patient age and clinical
presentation (Table II). Out of the
73 patients with CRC, GG homozygosity was observed in 50 patients
with CRC (68.5%), whereas 23 CRC patients possessed the GA and AA
genotypes (31.5%; Fig. 2). With the
exception of the local progression of the primary tumor, no
significant associations were identified between the rs1801157
CXCL12 gene polymorphism and the clinicopathological parameters.
The rs1801157 CXCL12 gene polymorphism was associated with the
local progression of the primary tumor, as indicated by the T
stage. The frequency of the GG genotype was notably increased in
patients with stage 3 and 4 tumors (78.0%) compared with the
incidence of the GA or AA genotypes (69.5%; P=0.067) (23).
| Table II.Tumour characteristics in patients
expressing the CXCL12 genotypes. |
Table II.
Tumour characteristics in patients
expressing the CXCL12 genotypes.
|
| CXCL12
genotype |
|
|---|
|
|
|
|
|---|
|
Characteristics | GG, n (%) | GA or AA, n
(%) | P-value |
|---|
| Total | 50 (100.0) | 23 (100.0) |
|
| Median age,
years | 66 | 67 | 0.035 |
| Gender |
|
|
|
|
Male | 27 (54.0) | 16 (69.6) | 0.579 |
|
Female | 23 (46.0) | 7
(30.5) | NS |
| T stage |
|
|
|
|
1+2 | 11 (22.0) | 7
(30.5) | 0.067 |
|
3+4 | 39 (78.0) | 16 (69.5) |
|
| N stage |
|
|
|
| 0 | 12 (24.0) | 6
(26.0) | 0.364 |
|
1–3 | 37 (76.0) | 17 (74.0) | NS |
| M stage |
|
|
|
| 0 | 33 (66.0) | 13 (56.5) | 0.509 |
| + | 17 (34.0) | 10 (43.5) | NS |
| R status |
|
|
|
| 0 | 32 (64.0) | 11 (47.8) | 0.395 |
| + | 18 (36.0) | 12 (52.2) | NS |
| T stage |
|
|
|
|
1–3 | 39 (78.0) | 13 (56.5) | 0.214 |
| 4 | 11 (22.0) | 10 (43.5) | NS |
Discussion
SDF-1 is considered to be important for the
pathogenesis of certain diseases (24,25). The
known CXCL12 isoforms, SDF-1α, SDF-1β, SDF-1γ, SDF-1δ, SDF-1ε and
SDF-1θ result from alternative splicing events of the same gene
(26). In addition, a
single-nucleotide polymorphism (SNP), termed CXCL12-G801A or
rs1801157, was identified in the 3′-untranslated region of the
CXCL12 gene transcript.
Several studies have examined the association
between disease susceptibility and the CXCL12-G801A
polymorphism(27–33). These studies indicated that the
CXCL12-G801A polymorphism was associated with an increased risk of
HIV infection, lung cancer, breast cancer, acute leukemia, prostate
cancer, non-Hodgkin's lymphoma and oral squamous cell carcinoma
(27–34). However, only a small number of studies
focused on the presence of the CXCL12-G801A polymorphism in CRC
patients to clarify whether the CXCL12-G801A polymorphism is
associated with disease susceptibility and clinical characteristics
in CRC (31,35).
A total of 73 patients were included in the present
study, and the G/G polymorphism was identified in 50 patients with
CRC (68.5%), and the G/A and A/A genotypes were identified in 23
patients with CRC (31.5%). Comparison of the results that were
obtained in the present analysis of the CXCL12 gene polymorphism in
human CRC with results obtained previously is of importance. The
results of the present study were consistent with the results of
Dimberg et al (22), who
studied the CXCL12 gene polymorphism in 151 patients with CRC and
141 control individuals. This study reported that the frequency of
the G/G, G/A and A/A genotypes were 55.6% (84/151), 41.1% (62/151)
and 3.3% (5/151), respectively, in the patients with CRC. The
genotype distribution was not significantly different between the
CRC patients and control individuals (22).
The present study attempted to determine the
association between the presence of the CXCL12 gene polymorphism
and the development of CRC. The data in the present study revealed
that the GG genotype distribution demonstrates a strong association
with the local progression of CRC.
Previous studies have reported that the effect of
the CXCL12 gene polymorphism may contribute differentially to CRC
by mediating tumor progression, angiogenesis, metastasis and
leukocyte migration (22).
Dimberg et al (22) and Hidalgo-Pascual et al
(36) did not identify a significant
correlation between the CXCL12-AA genotype and various prognostic
markers, such as the development of metastasis and disease-free
survival time. The present data were consistent with these studies,
as the current results only identified an association between this
genotype and the presence of larger primary tumors at primary
diagnosis.
However, the study by Chang et al (37) compared the frequency of six SDF-1α
SNPs in 424 patients with primary T3 stage CRC, and reported that
the SDF-1α-G801A polymorphism was associated with lymph node
metastasis. The frequency of GA/AA genotypes was significantly
increased (54.8%) in the group of patients with lymph node
metastasis compared with the group of patients without lymph node
metastasis (40.7%). In the patients without lymph node metastasis,
the disease-free survival rate was decreased in patients with the
GA/AA genotype (74%) compared with patients with the GG genotype
(87.6%). This previous study concluded that the SDF-1α-G801A
polymorphism may increase the expression of SDF-1α mRNA and be a
predictive marker of lymph node metastasis in CRC (37). The differences observed between the
studies, including the present study, are likely to be due to a
difference in patient numbers and tumor stages.
To assess the strength of the association between
the presence of the CXCL12-G801A polymorphism and the risk of
cancer, Gong et al (38)
performed a meta-analysis of 17 studies comprising a total of 3,048
cancer patients and 4522 control individuals. The odds ratio (OR)
and 95% confidence interval (CI) were used to determine the
association. Compared with the GG genotype, the results revealed
that the variant genotypes, consisting of GA (OR, 1.38; 95% CI,
1.18–1.61) and GA/AA (OR, 1.36; 95% CI, 1.17–1.59), were associated
with a significantly increased risk of all cancer types. This
meta-analysis indicated that the CXCL12 G801A polymorphism is a
low-penetrance risk factor for cancer development (23,38).
Furthermore, the present study analyzed the
correlation between SDF-1 isoforms and clinicopathological
parameters. It was demonstrated that SDF-1β was associated with the
presence of metastases and that SDF-1γ was significantly associated
with tumor size. To the best of our knowledge, the present study is
the first to analyze the expression profile of the chemokine CXCL12
splice variants in a larger series of human CRC tissues and normal
human mucosa.
Investigation of the expression of novel CXCL12
splice variants and understanding of the potential
pathophysiological relevance of the variants under various
conditions is required. Different splice variants in certain cases
may exhibit similar functions but are active in different tissues
or physiological conditions. An improved understanding of the
functional diversity of SDF-1 splicing variants may lead to novel
therapies that target these variants, which may delay or inhibit
the metastatic process in cancer cells (23).
In the present study, SDF-1α was the most
predominant splicing variant in CRC and normal mucosa tissues,
followed by SDF-1β, whereas the other splice variants γ, δ, ε and θ
were expressed less abundantly. The present findings are consistent
with previous data from the literature (26,39,40), which
demonstrated that SDF-1α is a ubiquitously expressed splicing
variant with multiple functions in various organs. The SDF-1β
isoform appears to be involved in inter-organ communication through
blood-mediated gradients and also in the support of angiogenesis
(26,39,40).
SDF-1β was mainly found in highly vascularized organs, such as the
liver, spleen, bone marrow and kidneys, but was absent in the brain
(26,41,42).
The data obtained in the present study therefore
suggested that SDF-1α, SDF-1β and SDF-1γ may act as tumor markers,
but are not necessarily associated with the patient prognosis.
References
|
1
|
Greenlee RT, Murray T, Bolden S and Wingo
PA: Cancer statistics, 2000. CA Cancer J Clin. 50:7–33. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Weir HK, Thun MJ, Hankey BF, Ries LA, Howe
HL, Wingo PA, Jemal A, Ward E, Anderson RN and Edwards BK: Annual
report to the nation on the status of cancer, 1975–2000, featuring
the uses of surveillance data for cancer prevention and control. J
Natl Cancer Inst. 95:1276–1299. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zlotnik A: Chemokines and cancer. Int J
Cancer. 119:2026–2029. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Premack BA and Schall TJ: Chemokine
receptors: gateways to inflammation and infection. Nat Med.
2:1174–1178. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bagglioni M: Chemokines and leukocyte
traffic. Nature. 392:565–568. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bleul CC, Schultze JL and Spinger TA: B
lymphocyte chemotaxis regulated in association with microanatomic
localization, differentiation state and B cell receptor engagement.
J Exp Med. 187:753–762. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schimanski CC, Schwald S, Simiantonaki N,
Javasinghe C, et al: Effect of chemokine receptors CXCR4 and CCR7
on the metastatic behavior of human colorectal cancer. Clin Cancer
Res. 11:1743–1750. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hao L, Zhang C, Wang L, Luo Y, et al:
Recombination of CXCR4, VEGF and MMP-9 predicting lymph node
metastasis in human breast cancer. Cancer Lett. 253:34–42. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shanmugam MK, Manu KA, Ong TH,
Ramachandran L, Surana R, Bist P, Lim LH, Kumar AP, Hui KM and
Sethi G: Inhibition of CXCR4/CXCL12 signaling axis by ursolic acid
leads to suppression of metastasis in transgenic adenocarcinoma of
mouse prostate model. Int J Cancer. 129:1552–1563. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
D'Alterio C, Barbieri A, Portella L, Palma
G, Polimeno M, Riccio A, Ieranò C, Franco R, Scognamiglio G, Bryce
J, et al: Inhibition of stromal CXCR4 impairs development of lung
metastases. Cancer Immunol Immunother. 61:1713–1720. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liang Z, Yoon Y, Votaw J, Goodman MM,
Williams L and Shim H: Silencing of CXCR4 blocks breast cancer
metastasis. Cancer Res. 65:967–971. 2005.PubMed/NCBI
|
|
12
|
Smith MC, Luker KE, Garbow JR, Prior JL,
Jackson E, Piwnica-Worms D and Luker GD: CXCR4 regulates growth of
both primary and metastatic breast cancer. Cancer Res.
64:8604–8612. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Phillips RJ, Burdick MD, Lutz M, Belperio
JA, Keane MP and Strieter RM: The stromal derived
factor-1/CXCL12-CXC chemokine receptor 4 biological axis in
non-small cell lung cancer metastases. Am J Respir Crit Care Med.
167:1676–1686. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sun XS, Wei L, Chen Q and Terek RM:
CXCR4/SDF1 mediate hypoxia induced chondrosarcoma cell invasion
through ERK signaling and increased MMP1 expression. Mol Cancer.
9:172010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pan J, Mestas J, Burdick MD, Phillips RJ,
Thomas GV, Reckamp K, Belperio JA and Strieter RM: Stromal derived
factor-I (SDF-I/CXCL12) and CXCR4 in renal cell carcinoma
metastasis. Mol Cancer. 5:562006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kollmar O, Rupertus K, Scheuer C, Junker
B, et al: Stromal cell-derived factor-1 promotes cell migration and
tumor growth of colorectal metastasis. Neoplasia. 9:862–870. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mori T, Doi R, Koizumi M, Toyoda E, et al:
CXCR4 antagonist inhibits stromal cell-derived factor-1-induced
migration and invasion of human pancreatic cancer. Mol Cancer Ther.
3:29–37. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yu L, Cecil J, Peng SB, Schrementi J, et
al: Identification and expression of novel isoforms of human
stromal cell-derived factor 1. Gene. 374:174–179. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Janowski M: Functional diversity of SDF-1
splicing variants. Cell Adh Migr. 3:243–249. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lombardi L, Tavano F, Morelli F, Latiano
TP, Di Sebastiano P and Maiello E: Chemokine receptor CXCR4: Role
in gastrointestinal cancer. Crit Rev Oncol Hematol. 88:696–705.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chada S, Ramesh R and Mhashilkar AM:
Cytokine- and chemokine-based gene therapy for cancer. Curr Opin
Mol Ther. 5:463–474. 2003.PubMed/NCBI
|
|
22
|
Dimberg J, Hugander A, Löfgren S and
Wagsater D: Polymorphism and circulating levels of the chemokine
CXCL12 in colorectal cancer patients. Int J Mol Med. 19:11–15.
2007.PubMed/NCBI
|
|
23
|
Allami RH: Influence of the chemokine
CXCL12 on the progression and the signalling in colorectal cancer.
PhD dissertation. Der Johannes Gutenberg-Universität. (ArchiMed,
Mainz). 2013.
|
|
24
|
Manetti M, Liakouli V, Fatini C, Cipriani
P, Bonino C, Vettori S, Guiducci S, Montecucco C, Abbate R,
Valentini G, Matucci-Cerinic M, Giacomelli R and Ibba-Manneschi L:
Association between a stromal cell derived factor1 (SDF-1/cxcl12)
gene polymorphism and microvascular disease in systemic sclerosis.
Ann Rheum Dis. 68:408–411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu W, Zhu E, Wang R, Wang L and Liu T:
CXCL12 G801A polymorphism is associated with an increased risk of
benign salivary gland tumors in the Chinese population. Med Oncol.
29:677–681. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yu L, Cecil J, Peng SB, Schrementi J,
Kovacevic S, Paul D, Su EW and Wang J: Identification and
expression of novel isoforms of human stromal cell-derived factor
1. Gene. 374:174–179. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Winkler C, Modi W, Smith MW, Nelson GW, Wu
X, Carrington M, Dean M, Honjo T, Tashiro K, Yabe D, Buchbinder S,
Vittinghoff E, Goedert JJ, O'Brien TR, Jacobson LP, Detels R,
Donfield S, Willoughby A, Gomperts E, Vlahov D, Phair J and O'Brien
SJ: Genetic restriction of AIDS pathogenesis by an SDF-1 chemokine
gene variant variant. ALIVE Study, Hemophilia Growth and
Development Study (HGDS), Multicenter AIDS Cohort Study (MACS),
Multicenter Hemophilia Cohort Study (MHCS). San Francisco City
Cohort (SFCC) Science. 279:389–393. 1998.
|
|
28
|
Razmkhah M, Doroudchi M, Ghayumi SM,
Erfani N and Ghaderi A: Stromal cell-derived factor-1 (SDF-1) gene
and susceptibility of Iranian patients with lung cancer. Lung
Cancer. 49:311–315. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Razmkhah M, Talei AR, Doroudchi M,
Khalili-Azad T and Ghaderi A: Stromal cell-derived factor-1 (SDF-1)
alleles and susceptibility to breast carcinoma. Cancer Lett.
225:261–266. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dommange F, Cartron G, Espanel C, Gallay
N, Domenech J, Benboubker L, Ohresser M, Colombat P, Binet C,
Watier H and Herault O: GOELAMS Study Group: CXCL12 polymorphism
and malignant cell dissemination/tissue infiltration in acute
myeloid leukemia. Faseb J. 20:1913–1915. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hirata H, Hinoda Y, Kikuno N, Kawamoto K,
Dahiya AV, Suehiro Y, Tanaka Y and Dahiya R: CXCL12 G801A
polymorphism is a risk factor for sporadic prostate cancer
susceptibility. Clin Cancer Res. 13:5056–5062. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
de Oliveira KB, Oda JM, Voltarelli JC,
Nasser TF, Ono MA, Fujita TC, Matsuo T and Watanabe MA: CXCL12
rs1801157 polymorphism in patients with breast cancer, Hodgkin's
lymphoma and non-Hodgkin's lymphoma. J Clin Lab Anal. 23:387–393.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Teng YH, Liu TH, Tseng HC, Chung TT, Yeh
CM, Li YC, Ou YH, Lin LY, Tsai HT and Yang SF: Contribution of
genetic polymorphisms of stromal cell-derived factor-1 and its
receptor, CXCR4, to the susceptibility and clinicopathologic
development of oral cancer. Head Neck. 31:1282–1288. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vairaktaris E, Vylliotis A, Spyridonodou
S, Derka S, Vassiliou S, Nkenke E, Yapijakis C, Serefoglou Z,
Neukam FW and Patsouris E: A DNA polymorphism of stromal-derived
factor-1 is associated with advanced stages of oral cancer.
Anticancer Res. 28:271–275. 2008.PubMed/NCBI
|
|
35
|
Zhu K, Jiang B, Hu R, Yang Y, Miao M, Li Y
and Liu Z: The CXCL12 G801A polymorphism is associated with cancer
risk: A meta-analysis. PLoS One. 9:e1089532014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hidalgo-Pascual M, Galan JJ, Chaves-Conde
M, Ramírez-Armengol JA, Moreno C, Calvo E, Pelaez P, Crespo C, Ruiz
A and Royo JL: Analysis of CXCL12 3′UTR G>A polymorphism in
colorectal cancer. Oncol Rep. 18:1583–1587. 2007.PubMed/NCBI
|
|
37
|
Chang SC, Lin PC, Yang SH, Wang HS, Li AF
and Lin JK: SDF-1alpha G801A polymorphism predicts lymph node
metastasis in stage T3 colorectal cancer. Ann Surg Oncol.
16:2323–2330. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gong H, Tan M, Wang Y, Shen B, Liu Z,
Zhang F, Liu Y, Qiu J, Bao E and Fan Y: The CXCL12 G801A
polymorphism and cancer risk: evidence from 17 case-control
studies. Gene. 509:228–231. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Altenburg JD, Broxmeyer HE, Jin Q, Cooper
S, Basu S and Alkhatib G: A naturally occurring splice variant of
CXCL12/stromal cell-derived factor 1 is a potent human
immunodeficiency virus type 1 inhibitor with weak chemotaxis and
cell survival activities. J Virol. 81:8140–8148. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Janowski M: Functional diversity of SDF-1
splicing variants. Cell Adh Migr. 3:243–249. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sun X, Cheng G, Hao M, Zheng J, Zhou X,
Zhang J, Taichman RS, Pienta KJ and Wang J: CXCL12/CXCR4/CXCR7
chemokine axis and cancer progression. Cancer Metastasis Rev.
29:709–722. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Colobran R, Pujol-Borrell R, Armengol MP
and Juan M: The chemokine network II. On how polymorphisms and
alternative splicing increase the number of molecular species and
configure intricate patterns of disease susceptibility. Clin Exp
Immunol. 150:1–12. 2007. View Article : Google Scholar : PubMed/NCBI
|