Introduction
The normal pineal gland secretes melatonin, which is
involved in diurnal rhythms, and is located in the supratentorial
midline, above the superior colliculi and below the splenium of the
corpus callosum and the vein of Galen (1). Pineal region neoplasms include
germinoma, teratoma, pinealocytoma and meningioma; these tumors are
infrequently occurring lesions that account for <1% of all
primary intracranial tumors in adults and 3–8% in the pediatric
population (2,3).
Inflammatory pseudotumor is a pathological term that
describes a reactive, inflammatory non-neoplastic tumor that
typically occurs in the lungs, omentum, mesentery, retroperitoneum,
orbital cavities, upper respiratory tract or genitourinary tract.
Primary intracranial involvement is extremely rare (4). The histopathology of an inflammatory
pseudotumor consists of a collagenous stroma and an inflammatory
infiltrate of mononuclear elements (5). Due to the rarity of inflammatory
pseudotumors that occur in the central nervous system, forming an
accurate diagnosis by MRI scans is challenging. According to
previous studies, surgical removal of the pseudotumor and treatment
of the forhydrocephalus were performed in the majority of cases,
and the outcomes were generally good (6,7). The
current study reports the case of a patient with an inflammatory
pseudotumor of the pineal region, and to the best of our knowledge,
it is the first reported case of an inflammatory pseudotumor in
this location.
Case report
A 53-year-old man presented to The Second Affiliated
Hospital of Zhejiang University School of Medicine (Hangzhou,
Zhejiang, China) with hearing loss that had been apparent for 1
year and blurred vision that had persisted for 10 months. The
patient was conscious and well-oriented, and normal pupil reactions
were present. The general physical examination was within normal
limits and the neurological examination indicated clear and alert
consciousness.
The routine laboratory investigations were within
normal reference ranges. Brain magnetic resonance imaging (MRI) was
performed using the 1.5T MRI scanner (Siemens Sonata, Erlangen,
Germany) prior to and following the intravenous administration of
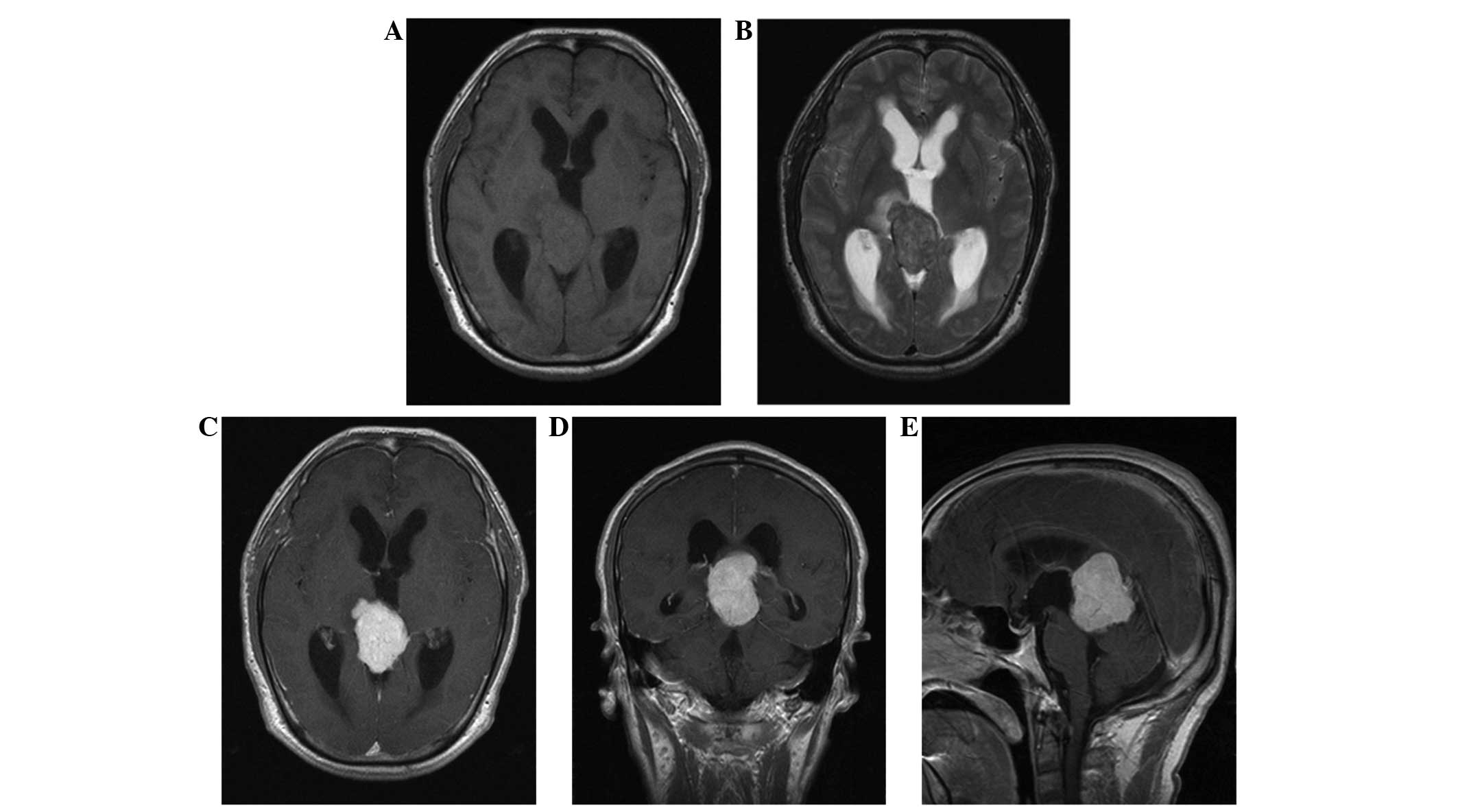
gadolinium contrast material. A well-defined mass in the pineal
region was revealed, which extended into the posterior third
ventricle and was compressing the tectal plate from above. The mass
was isointense on non-contrast T1-weighted images (Fig. 1A) and heterogeneously hyperintense on
T2-weighted images (Fig. 1B), while
homogeneous contrast enhancement of the mass lesion was observed
following administration of gadolinium (Fig. 1C–E). A provisional diagnosis of pineal
germinoma or pinealocytoma was considered.
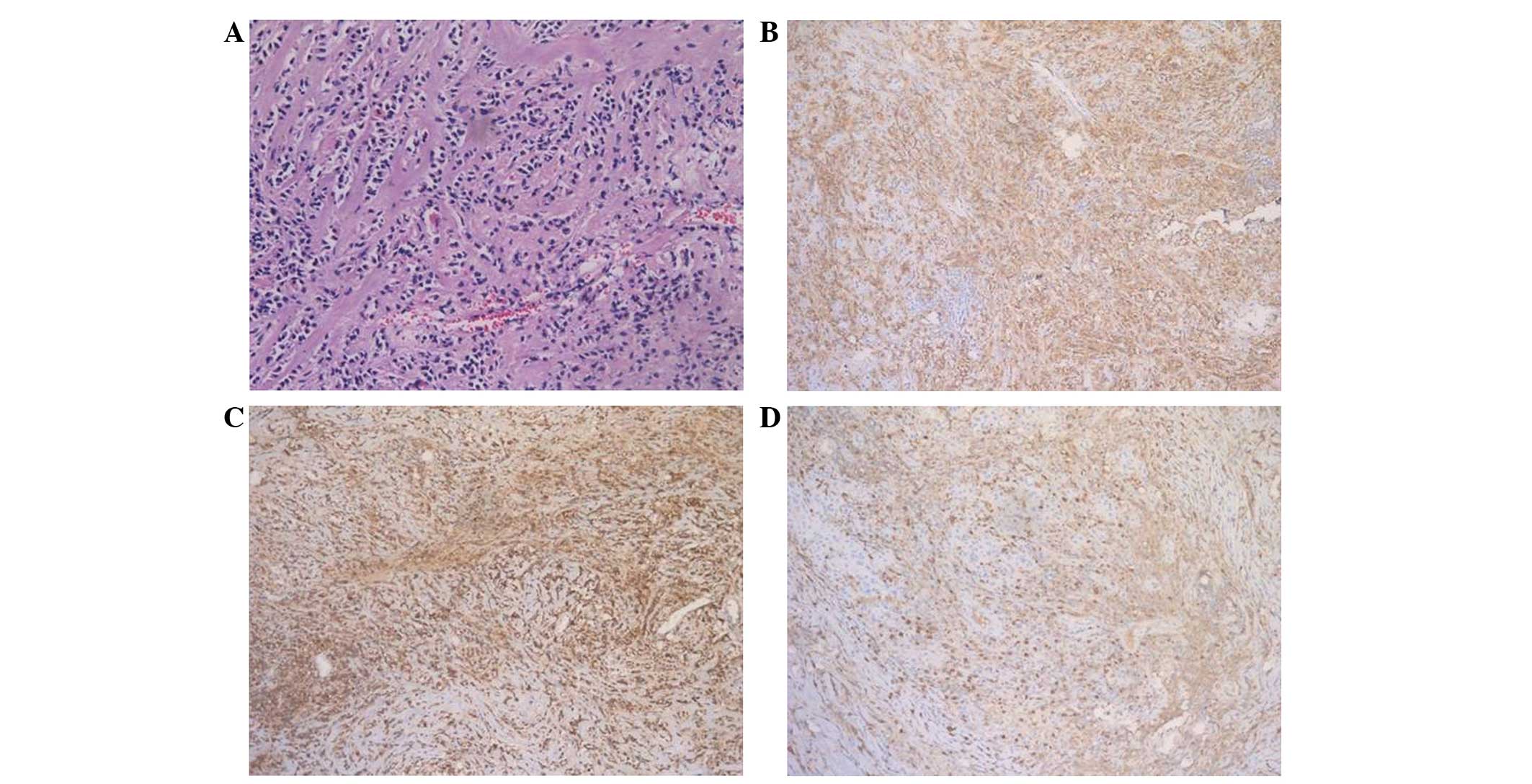
A pathological examination revealed that the lesion
was comprised predominantly of spindle cells in a collagenous
background, with dense infiltrates of small lymphocytes, plasma
cells and uninucleated histiocytes (Fig.
2A). There was no evidence of mitosis or necrosis.
Immunopositivity for cluster of differentiation (CD)138 was noted
(Fig. 2B). Specific acid-fast
bacillus staining for fungus and mycobacteria was negative.
Tumor samples were formalin-fixed and
paraffin-embedded, and cut into 4-µm thick sections that were
stained using standard hematoxylin and eosin methods.
Immunohistochemical staining was performed using a Ventana NexES
automated immunostainer (Ventana Medical Systems, Inc., Tuscon, AZ,
USA). The antibodies used included rabbit anti-human S-100 protein
polyclonal antibody (catalog no. ZA-0225; dilution, 1:500), rabbit
anti-human CD3 monoclonal antibody (catalog no., ZA-0503; dilution,
1:100), rabbit anti-human CD20 monoclonal antibody (catalog no.,
ZA-0549; dilution, 1:200), mouse anti-human CD43 monoclonal
antibody (catalog no., ZM-0048; dilution, 1:100), rabbit anti-human
CD79A monoclonal antibody (catalog no., ZA-0293; dilution, 1:150),
mouse anti-human CD138 monoclonal antibody (catalog no., ZM-0459;
dilution, 1:50), mouse anti-human Igκ monoclonal antibody (catalog
no., ZM-0160; dilution, 1:200), rabbit anti-human Igλ monoclonal
antibody (catalog no., ZM-0180; dilution, 1:200), mouse anti-human
Ki-67 monoclonal antibody (catalog no., ZM-0167; dilution, 1:100),
mouse anti-human neurofilament (NF) monoclonal antibody (catalog
no., ZM-0198; dilution, 1:200) and mouse anti-human Pit-Oct-Unc
class 5 homeobox 1 (Oct3/4) monoclonal antibody (catalog no.,
ZM-0233; dilution, 1:100). All antibodies were purchased from
Zhongshan Golden Bridge Biotechnology Co., Ltd. All tissue sections
underwent heat-induced antigen retrieval. The results showed that
the cells were immunonegative for glial fibrillary acidic protein,
S-100, placental alkaline phosphatase, NF and Oct3/4. NF
immunostaining is common in diagnostic neuropathology, and is
useful for differentiating between neurons, which express NF, and
glia, which do not express NF (8).
Oct3/4, a member of the Pit-Oct-Unc domain transcription factors
family, is normally expressed in adult and embryonic stem (ES)
cells, so may be expressed in malignant tumors (9). Increased Oct3/4 expression increases the
malignant potential of ES cell-derived tumors, whereas Oct3/4
inactivation induces the regression of the malignant component
(10).
The Ki-67 labeling index was <5%. The lymphocytic
infiltrates consisted of CD3- and CD43-positive T-cells, and CD20-
and CD79A-positive B-cells. Plasma cells displayed polytypic
reactivity for immunoglobulin κ (Fig.
2C) and λ (Fig. 2D) light
chains.
Based on the MRI, and the morphological and
immunohistochemical analysis, a final diagnosis of an inflammatory
pseudotumor was formed. In May 2014, the patient underwent surgical
resection of the tumor at The Second Affiliated Hospital of
Zhejiang University School of Medicine. Following the surgery, the
patient has not undergone any further treatment, and at 20 months
of follow-up, there is no evidence of recurrence with the patient
continuing to attend regular follow-up sessions.
Discussion
Inflammatory pseudotumors form a heterogenous
disease group with an unsettled pathogenesis (11). The tumors contain fibrosis and
inflammatory cells, with irregularly scattered infiltration by
macrophages, plasma cells and lymphocytes, and are possibly as a
result of inflammation. Furthermore, inflammatory pseudotumors may
also be caused by infections (12,13).
The radiologists in the present study could not
precisely diagnose the mass as an inflammatory pseudotumor, and the
MRI images did not provide a specific pretreatment diagnosis. On
imaging, the inflammatory pseudotumor appeared as a heterogeneously
enhancing mass originating from the pineal region. The secondary
finding of obstructive hydrocephalus was observed, similar to that
found with other masses in this location. To the best of our
knowledge, no cases of inflammatory pseudotumors developing in the
pineal region, which may have assisted in forming a diagnosis, are
recorded in the literature, and the histopathology was the mainstay
in establishing the diagnosis.
According to previous studies, surgical removal of
the pseudotumor and treatment of the forhydrocephalus were
performed in the majority of cases, and the outcomes were generally
good (6,7). Due to the rarity of inflammatory
pseudotumors that occur in the pineal region, clinical experience
of this entity remains limited and further detailed studies are
required to provide a standardization of therapy.
In conclusion, inflammatory pseudotumors occurring
in the central nervous system are extremely rare. To the best of
our knowledge, there have no previously reported cases of an
inflammatory pseudotumor originating in the pineal region. Although
rare, a diagnosis of an inflammatory pseudotumor should be
considered when a tumorous lesion is noted in the pineal region. A
correct histopathological diagnosis is required in order for an
appropriate therapeutic regimen to be selected for the lesion.
Acknowledgements
The present study was supported by the Zhejiang
Education Fund (Hangzhou, China; grant no., Y201330158).
References
|
1
|
Dahiya S and Perry A: Pineal tumors. Adv
Anat Pathol. 17:419–427. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Smith AB, Rushing EJ and Smirniotopoulos
JG: From the archives of the AFIP. Lesions of the pineal region:
Radiologic-pathologic correlation. Radiographics. 30:2001–2020.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yousem DM and Grossman RI: Neoplasms of
the brain. Neuroradiology: The Requisites (3rd). (Mosby,
Philadelphia). 94–98. 2010.
|
|
4
|
Swain RS, Tihan T, Horvai AE, et al:
Inflammatory myofibroblastic tumor of the central nervous system
and its relationship to inflammatory pseudotumor. Hum Pathol.
39:410–419. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathologic and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yavuzer D, Dalbayrak S, Oz B, Yilmaz M and
Akansel G: Intracranial inflammatory pseudotumor: Case report and
review of the literature. Clin Neuropathol. 29:151–155. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Suri V, Shukla B, Garg A, Singh M, Rishi
A, Sharma MC and Sarkar C: Intracranial inflammatory pseudotumor:
Report of a rare case. Neuropathology. 28:444–447. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lee VM and Andrews PW: Differentiation of
NTERA-2 clonal human embryonal carcinoma cells into neurons
involves the induction of all three neurofilament proteins. J
Neurosci. 6:514–521. 1986.PubMed/NCBI
|
|
9
|
Looijenga LHI, Stoop H, de Leeuw HP, de
Gouveia Brazao CA, Gillis AJ, van Roozendaal KE, van Zoelen EJ,
Weber RF, Wolffenbuttel KP, van Dekken H, et al: POU5F1 (OCT3/4)
identifies cells with pluripotent potential in human germ cell
tumors. Cancer Res. 63:2244–2250. 2003.PubMed/NCBI
|
|
10
|
Gidekel S, Pizov G, Bergman Y and Pikarsky
E: Oct-3/4 is a dose-dependent oncogenic fate determinant. Cancer
Cell. 4:361–370. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lui PC, Fan YS, Wong SS, Chan AN, Wong G,
Chau TK, Tse GM, Cheng Y, Poon WS and Ng HK: Inflammatory
pseudotumors of the central nervous system. Hum Pathol.
40:1611–1617. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fukunaga A, Yoshida K, Otani M, Ogawa Y,
Horiguchi T, Ishihara M, Toya S and Kawase T: Plasma cell granuloma
extending from the extracranial to the intracranial space
associated with Epstein-Barr virus infection. Neurol Med Chir
(Tokyo). 38:292–296. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jung TY, Jung S, Lee MC, Moon KS, Kim IY,
Kang SS and Kim SH: Hemorrhagic intracranial inflammatory
pseudotumor originating from the trigeminal nerve: A case report. J
Neurooncol. 76:139–142. 2006. View Article : Google Scholar : PubMed/NCBI
|