Introduction
Advanced non-small cell lung cancer with associated
atrial involvement is uncommon, occurring in ~10% of patients
presenting with bronchogenic carcinoma (1,2). Patients
with the disease usually possess circulatory and respiratory
symptoms, and coughing, hemoptysis, dyspnea, weight loss and an
extremely poor performance status are the typical associated
features (3). Furthermore, an
associated intra-atrial tumor thrombus is particularly rare, with
tumor thrombi potentially leading to widespread systemic
embolization and/or outflow tract obstruction (4–6). As a
result, treatment is always warranted. If there is no presentation
of distant metastasis, surgical resection is considered as the
gold-standard therapy. However, chemotherapy may also be
administered. Cases of non-small cell lung cancer with associated
intra-atrial tumor thrombi are usually diagnosed using enhanced
computed tomography (CT). Due to the rarity of this condition,
incidence and mortality rates remain unknown, however, patient
prognosis is extremely poor with an overall survival time of 4–17
months (1,7). The present study reports the case of a
patient with stage IV lung cancer with invasion into the left
atrium, for which a complete response was achieved following
treatment with stereotactic radiotherapy.
Case report
In April 2012, a 52-year-old man was admitted to the
Center of Radiation Oncology, Wujing Hospital (Shanghai, China)
presenting with a 3-month history of progressive dyspnea and
coughing. The patient also had a history of hypertension and
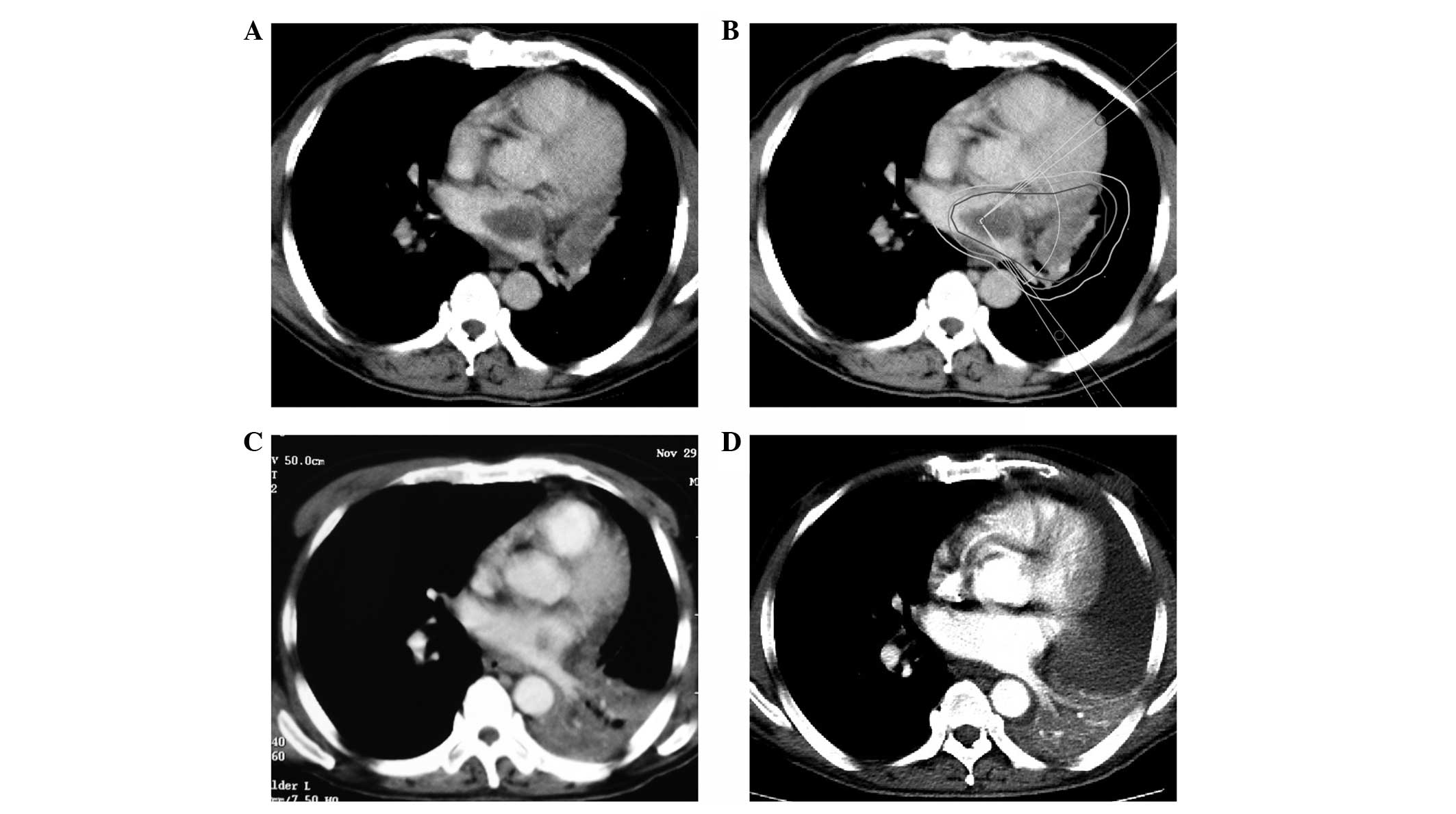
smoking. An enhanced CT scan (Optima CT660 FREEdom; GE Healthcare,
Piscataway, NJ, USA) revealed a left hilar tumor wrapped around the
left pulmonary artery and vein, along with a large mass in the left
atrium (Fig. 1A). A transbronchial
biopsy was performed. Subsequently, tissue was formalin-fixed
(Shanghai Ziyi Reagent Factory, Shanghai, China) paraffin-embedded
(Leica Microsystems, Ltd., Milton Keynes, UK) and cut into 4 µm
sections for hematoxylin and eosin (Baso Diagnostics Inc., Zhuhai,
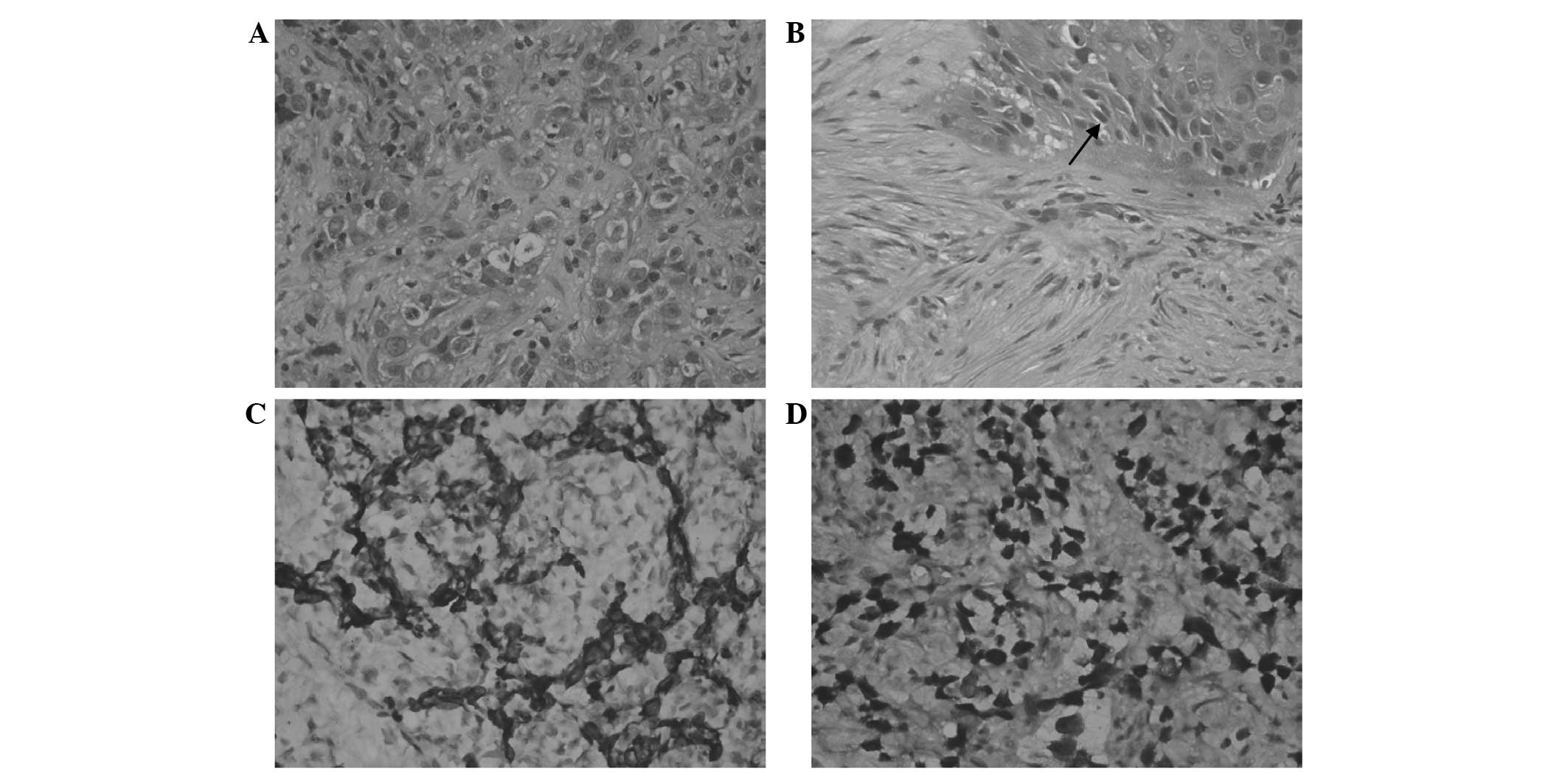
China) staining and immunohistochemistry. The biopsy revealed that
the primary site was consistent with nests and trabecula of
carcinoma cells proliferating with necrotic debris and
intercellular bridges structures (Fig. 2A
and B). For immunohistochemical analysis, the specimens were
incubated with primary antibodies for 45 min at room temperature.
Slides were then washed 4 times in Tris-Buffered Saline with Tween
20 (TBST) for 5 min. The slides were incubated with horseradish
peroxidase-conjugated polyclonal goat anti-rabbit secondary
antibody (Dako REAL™ EnVision™ kit; ready to use; cat. no. K5007;
Dako, Glostrup, Denmark) for 30 min at room temperature. The slides
were then washed 3 times with TBST for 5 min. Next, slides were
washed with Dako REAL™ substrate buffer (Dako) and incubated with
3,3′-diaminobenzidine chromogen (Dako) for 10 min at room
temperature. The slides were then washed 3 times with TBST followed
by distilled water for 1 min. Staining was visualized under a
microscope (BX41; Olympus Corporation, Tokyo, Japan).
Immunohistochemistry revealed positive staining for cytokeratin 5/6
(monoclonal anti-human mouse antibody; 1:50; cat. no. AM0101;
Ascend Biotechnology Co., Ltd., Guangzhou, China) and p40
(monoclonal anti-human mouse antibody; 1:200; cat. no. 10035N;
Ascend Biotechnology Co., Ltd.), which indicated poorly
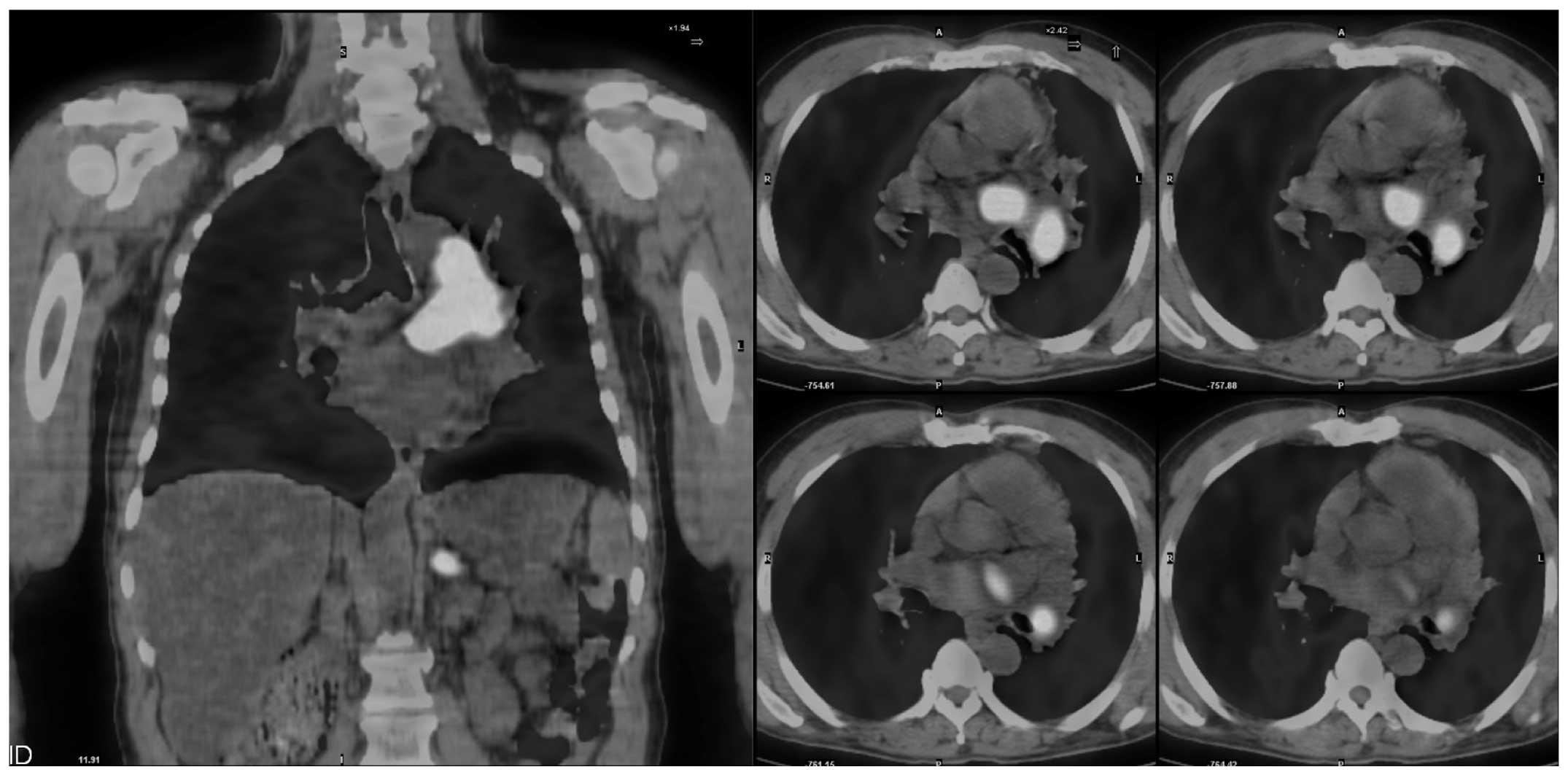
differentiated squamous cell carcinoma (Fig. 2C and D). Positron emission tomography
(PET; GE Discovery ST; GE Healthcare) exhibited intense
18F-fluorodeoxyglucose uptake in the hilar tumor and the
mass in the left atrium; additionally, a hot spot was located in
the left adrenal gland (Fig. 3). The
patient was therefore diagnosed with T4N1M1 [American Joint
Committee on Cancer stage IV (8)]
lung squamous cell carcinoma with atrial tumor thrombus.
Due to the high risks of surgical resection and a
patient history of refractory diabetes, it was agreed that
stereotactic radiotherapy, via segmented gamma-ray therapy (SGS-I,
Huiheng Medical, Shenzhen, China), would be performed on the two
lesions. An internal target volume (ITV) of the tumor was segmented
according to tumor motion based on a four-dimensional scan. A 6-mm
margin was added to the ITV to form the planning target volume
(PTV). A total dose of 40 Gy in 4-Gy fractions was delivered over 2
weeks to cover at least 95% of the PTV (Fig. 1B). The median doses for the lung and
esophagus were 6.8 and 12.6 Gy, respectively. The maximum dose
administered to the spinal cord was 5.2 Gy, and the V30
[volume (%) receiving 30 Gy] of the uninvolved heart was 20.8%.
Following a total of 2 months, a CT scan demonstrated that the left
hilar mass and the left atrial tumor thrombus had significantly
reduced in size, and the symptoms had considerably improved.
However, following a 5-month stable period, the patient was
hospitalized due to the onset of a fever and severe cough. A CT
scan revealed left lower pulmonary atelectasis and pneumonia
(Fig. 1C). Mycobacterium tuberculosis
was also detected in the sputum.
During the next 6 months, the patient received
anti-tuberculosis (300 mg isoniazid; 600 mg, rifampicin; daily) and
supportive treatment (228 mg polyene phosphatidylcholine; three
times daily). A follow-up CT scan at 1 year post-radiotherapy
demonstrated that the tumor thrombus in the left atrium had
disappeared, however, the left lower pulmonary atelectasis had not
yet been fully alleviated (Fig. 1D).
The patient exhibited no marked symptoms, and following completion
of a PET scan, there was no indication of tumor recurrence. Despite
this, 6 months later, the patient presented with progressive back
pain, and a subsequent magnetic resonance imaging scan confirmed
the presence of multiple bone metastases. The patient accepted
analgesic therapy only and succumbed 3 months later. The patient's
overall survival time was 21 months.
Written informed consent was obtained from the
family of the patient for the publication of this case report and
any accompanying images.
Discussion
Lung cancer presenting with a giant atrial tumor
thrombus is particularly rare. To the best of our knowledge, there
have only been 18 cases published in the English literature over
the last two decades. In these 18 cases, squamous cell carcinoma
was the most common pathological type and was present in 5 cases
(7,9–12),
followed by 4 neuroendocrine carcinoma cases (13–16), 3
adenocarcinoma cases (1,17,18), 3
sarcoma cases (5,6,19), 1 large
cell carcinoma case (20) and 1
neuroectodermal tumor case (21). The
pathology of a further case was reported as sarcoma mixed with
squamous carcinoma (16); although
histopathological examination demonstrated that the primary tumor
was poorly-differentiated, the cardiac and intravascular portions
of each tumor were less differentiated and more necrotic than the
primary focus in the lung (3).
The morphological style of lung cancer invasion into
the left atrium may be divided into two groups: i) Contiguous
invasion by the primary tumor from the pulmonary vein base; and ii)
direct invasion by the primary tumor, or lymph node metastasis,
into the posterior wall of the left atrium (10). The atrial wall is composed of the
epicardium, a muscle layer and the tunica intima. As a thin layer
of mesothelial cells, the epicardium is easily penetrated by tumor
cells with involvement of the muscle layer. Once the tumor cells
have invaded the atrium, this alters the hemodynamics of the body;
cancer cell-derived microparticles aggregate platelets via a tissue
factor-dependent pathway, and as a result, the tumor thrombus
rapidly increases in size (22).
Tumor thrombi may lead to widespread systemic embolization and/or
outflow tract obstruction (4–6). The incidence of embolization is ~16.7%
(3/18), and as a result, treatment is always warranted.
Lung cancer invading the left atrium or great
vessels is classified as T4 and belongs to stage IIIb of the
tumor-node-metastasis classification system (8). The prognosis for affected patients is
poor, and surgery often has an insufficient effect on the disease.
However, patients presenting with limited invasion of the left
atrium and no distant metastasis may achieve a complete surgical
resection despite having a T4 classification (23). Prior to resection of the mass, a
cardiopulmonary bypass should be performed to prevent systemic
seeding or embolization of the tumor (10,16). The
median survival time following this type of surgery has been
reported to be 10 months (24).
Radiotherapy is an important treatment for malignant
tumors. In a previous case, intensity-modulated radiotherapy (50-Gy
dose) was delivered to a lung tumor and intra-atrial lesion, with
the patient experiencing no acute side effects from the radiation
and a complete response of the intracardiac disease within 3 months
(1). Modern radiation oncology
techniques, including stereotactic and intensity-modulated
radiotherapy, have greatly reduced the risk of radiation-associated
heart disease by delivering a high dose directly to the tumor, and
a sharp dose-gradient to the adjacent normal heart and other organs
(1,25). Furthermore, due to the increased
precision of modern radiotherapy, a smaller margin is applied to
the gross tumor volume to overcome daily set-up or tumor motion
uncertainty. In particular, the risk of pericardial and coronary
artery disease is significantly limited with strategies such as a
deep inspiratory breath hold. Improved dose-delivery techniques
also increase the utility of radiation (1,25). The 18
previous cases (1,5–7,9–21) show
that surgery combined with chemotherapy is the most common
treatment for this condition, however, prognosis remains extremely
poor, with overall survival times ranging between 4 and 17 months.
In the present case, surgery was not advised due to the presence of
distant metastasis and the high risk of the surgical procedure.
However, a complete response of the tumor and the associated
thrombus was achieved using stereotactic radiotherapy alone.
However, the patient later suffered from pneumonia and tuberculosis
as a result of decreased immunity, which subsequently led to left
pulmonary atelectasis. The overall survival time of the patient was
21 months, and no radiation therapy-associated complications were
noted. Therefore, the present case demonstrates that stereotactic
radiotherapy may be a beneficial palliative treatment for patients
with stage IV lung cancer invading the left atrium.
Acknowledgements
The authors would like to thank Dr Yihong Li and Dr
Chunli Liu (Department of Nuclear Medicine, Wujing Hospital) for
providing imaging data and Dr Lina Liu (Department of Pathology,
Wujing Hospital) and Dr Yanchun Ma (Department of Pathology,
Huashan Hospital, Shanghai, China) for performing histopathological
analysis.
References
|
1
|
Lee P and Kishan AU: Radiotherapy is
effective for a primary lung cancer invading the left atrium. BMJ
Case Rep. 2012:2012.
|
|
2
|
Takahashi K, Furuse M, Hanaoka H, Yamada
T, Mineta M, Ono H, Nagasawa K and Aburano T: Pulmonary vein and
left atrial invasion by lung cancer: Assessment by breath-hold
gadolinium-enhanced three-dimensional MR angiography. J Comput
Assist Tomogr. 24:557–561. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kodama K, Doi O and Tatsuta M: Unusual
extension of lung cancer into the left atrium via the pulmonary
vein. Int Surg. 75:22–26. 1990.PubMed/NCBI
|
|
4
|
Sadat U, Noor N, See TC and Varty K:
Peripheral arterial ischemia by a primary lung tumour invading left
atrium. Lung Cancer. 57:237–239. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Koh TW: Invasion of lung mesenchymal
chondrosarcoma into the left atrium via the pulmonary vein detected
on transoesophageal echocardiography. Eur J Echocardiogr.
12:5562011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Woodring JH, Bognar B and van Wyk CS:
Metastatic chondrosarcoma to the lung with extension into the left
atrium via invasion of the pulmonary veins: Presentation as embolic
cerebral infarction. Clin Imaging. 26:338–341. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shimizu J, Ikeda C, Arano Y, Adachi I,
Morishita M, Yamaguchi S, Ishikawa N, Watanabe G and Minato H:
Advanced lung cancer invading the left atrium, treated with
pneumonectomy combined with left atrium resection under
cardiopulmonary bypass. Ann Thorac Cardiovasc Surg. 16:286–290.
2010.PubMed/NCBI
|
|
8
|
Tsim S, O'Dowd CA, Milroy R and Davidson
S: Staging of non-small cell lung cancer (NSCLC): A review. Respir
Med. 104:1767–1774. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sengül C, Sünbül A, Ozveren O and
Değertekin M: Case images: Squamous cell lung cancer metastasis in
the left atrium: An interesting case with cardiac images. Turk
Kardiyol Dern Ars. 40:6542012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ueda K, Kaneda Y, Sakano H, Tanaka T,
Saito K and Hamono K: Successful treatment of intracardiac
progression and metachronous multiple brain metastases from primary
lung cancer. Jpn J Thorac Cardiovasc Surg. 54:168–170. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim JH, Jung JY, Park Y, Hwang SI, Jung
CS, Lee SH and Yoo CW: Non-small cell lung cancer initially
presenting with intracardiac metastasis. Korean J Intern Med.
20:86–89. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Asaad K, Sadaba JR and Nair RU:
Intracardiac extension of squamous cell carcinoma of lung. Eur J
Cardiothorac Surg. 24:6402003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Costache VS, Lantuejoul S, Stoica S,
Fluttaz A, Hacini R and Brichon PY: Giant intracardiac neoplasic
thrombus of a large cell neuroendocrine carcinoma of the lung.
Cardiovasc Pathol. 19:e85–e87. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lin MT, Ku SC, Wu MZ and Yu CJ:
Intracardiac extension of lung cancer via the pulmonary vein.
Thorax. 63:11222008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brandt RR, Rubin J and Reeder GS:
Intracardiac extension of a lung tumor causing left ventricular
inflow obstruction. J Am Soc Echocardiogr. 8:930–933. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ma Q, Liu D, Liu P, Chen J, Xie Z and
D'Amico TA: Extensive invasion of the left atrium by lung cancer.
Ann Thorac Surg. 96:685–687. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Alexandrescu C, Civaia F and Dor V: Tumor
thrombus in right atrium from lung adenocarcinoma. Ann Thorac Surg.
87:e11–e12. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ucak A, Inan K, Onan B, Temizkan V, Alp I
and Yilmaz AT: Free-floating tumor thrombus in the left atrium
associated with non-small cell lung cancer. J Card Surg.
24:686–689. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dogan A, Icli A, Arslan A, Varol E and
Ozaydin M: Metastatic atrial sarcoma extending from the lung into
the left atrium via a pulmonary vein. Exp Clin Cardiol. 17:77–78.
2012.PubMed/NCBI
|
|
20
|
Khan N, Golzar J, Smith NL and Movahed A:
Intracardiac extension of a large cell undifferentiated carcinoma
of lung. Heart. 91:5122005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yokouchi H, Kodama K, Higashiyama M,
Takami K, Kobayashi T, Takami H, Nakamura S and Horai T: Successful
removal of a primitive neuroectodermal tumor in the lung with gross
extension into the left atrium. Thorac Cardiovasc Surg. 47:257–259.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Thomas GM, Panicot-Dubois L, Lacroix R,
Dignat-George F, Lombardo D and Dubois C: Cancer cell-derived
microparticles bearing P-selectin glycoprotein ligand 1 accelerate
thrombus formation in vivo. J Exp Med. 206:1913–1927. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
DiPerna CA and Wood DE: Surgical
management of T3 and T4 lung cancer. Clin Cancer Res.
11:5038s–5044s. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fukuse T, Wada H and Hitomi S: Extended
operation for non-small cell lung cancer invading great vessels and
left atrium. Eur J Cardiothorac Surg. 11:664–669. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Remouchamps VM, Vicini FA, Sharpe MB,
Kestin LL, Martinez AA and Wong JW: Significant reductions in heart
and lung doses using deep inspiration breath hold with active
breathing control and intensity-modulated radiation therapy for
patients treated with locoregional breast irradiation. Int J Radiat
Oncol Biol Phys. 55:392–406. 2003. View Article : Google Scholar : PubMed/NCBI
|