Introduction
Hepatoid adenocarcinoma is a relatively rare
extrahepatic tumor with morphological features similar to
hepatocellular carcinoma (1). The
most common site of origin for hepatoid adenocarcinoma is the
stomach (83.9%) (2–4). Hepatoid carcinoma of the lung (HAL) is
rare, and its incidence accounts for 2.3% of hepatoid
adenocarcinoma cases (1). The
biological significance of HAL remains to be elucidated (4), and its clinical symptoms are generally
atypical. Although computed tomography (CT) images may provide some
indications for a diagnosis of HAL, confirmation of this diagnosis
requires morphological and immunohistochemical confirmation.
Previous studies have suggested that HAL has a poorer prognosis
compared with more common types of lung tumor (5–7). In
general, the prognosis of HAL appears poor and its invasiveness may
explain its high mortality rate (1,7). The
overwhelming majority of cases reported in the English literature
have presented with elevated serum α-fetoprotein (AFP) levels
and/or positive AFP expression on histopathological analysis, and
were commonly associated with poor prognosis (8). Furthermore, based on the present
literature review, it appears that pathological state is the most
significant prognostic factor. The present study reports a case of
HAL without AFP production in which the patient underwent radical
right upper lobectomy via single-port video assisted thoracoscopic
surgery (VATS). A description of the clinical and pathological
findings, chest CT images, the outcome following surgery, and a
review of the relevant literature are presented.
Case report
In April 2014, a 59-year-old man with a history of
mild alcohol consumption, tobacco smoking (ceased 9 years
previously) and diabetes for 8 years sought medical consultation at
Weifang People's Hospital (Weifeng, China) for a productive cough
without chest pain or dyspnea. The patient did not have alcoholic
hepatitis or any remarkable relevant family medical history.
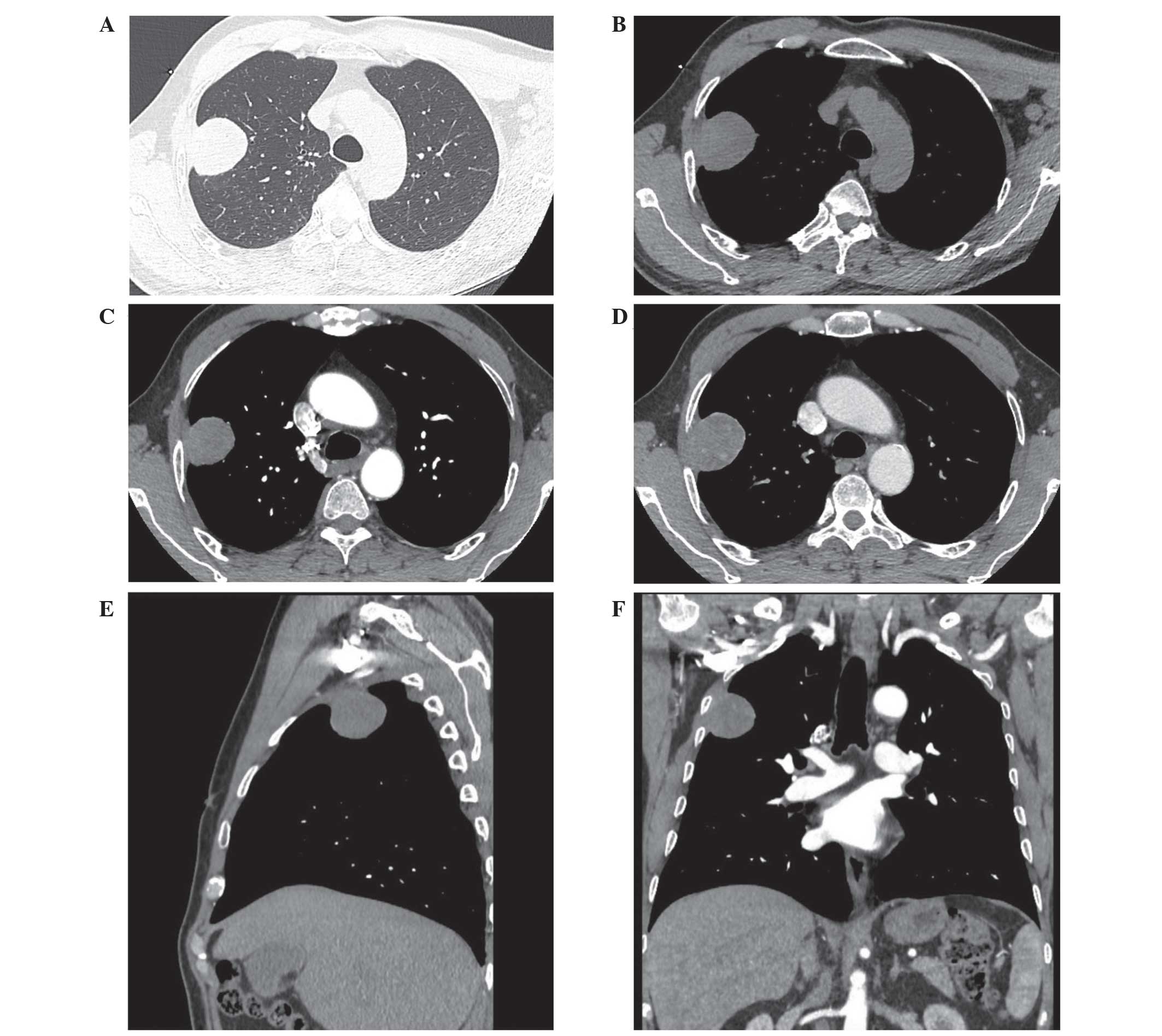
Non-contrast CT images (SOMATOM Definition AS;
Siemens Healthcare, Erlangen, Germany) revealed a well-defined
mass, of which the longest cross-sectional dimension was
4.5×3.8×3.5 cm, in the right upper lobe of the lung (Fig. 1A and B). The mass extended to the
pleura, causing thickening. Following intravenous injection of
contrast agents, the tumor appeared inhomogeneous and the majority
of the tumor exhibited mild enhancement, and moderate to
significant peripheral and patchy enhancement were found after a
delay (Fig. 1C–F). No enlarged lymph
nodes were detected in the hila or mediastinum. The patient
underwent percutaneous lung biopsy under CT guidance and routine
paraffin sectioning and hematoxylin and eosin staining were used to
detect the pathomorphological changes, which revealed
adenocarcinoma. According to the findings above, the clinical stage
of the patient was diagnosed as Ib (T2aN0M0). No abnormality was
found in the blood cell count or biochemistry. With regard to tumor
markers, carcinoembryonic antigen, CY211 and neuron-specific
enolase levels were observed to be normal. Serum AFP level was not
examined.
The patient was admitted for a pneumectomy of the
right upper lobe via single-port VATS. During the surgery, a 4×3×3
cm mass with adhesion to the chest wall in the apical segment of
right upper lobe was detected, along with enlarged subcarinal and
hilar lymph nodes. A right upper lobectomy with dissection of
multiple lymph nodes was successfully performed.
Pathological examination of the specimen revealed
that the tumor measured 4.5×3.5×3.5 cm on its largest
cross-section, and additionally exhibited extensive necrosis.
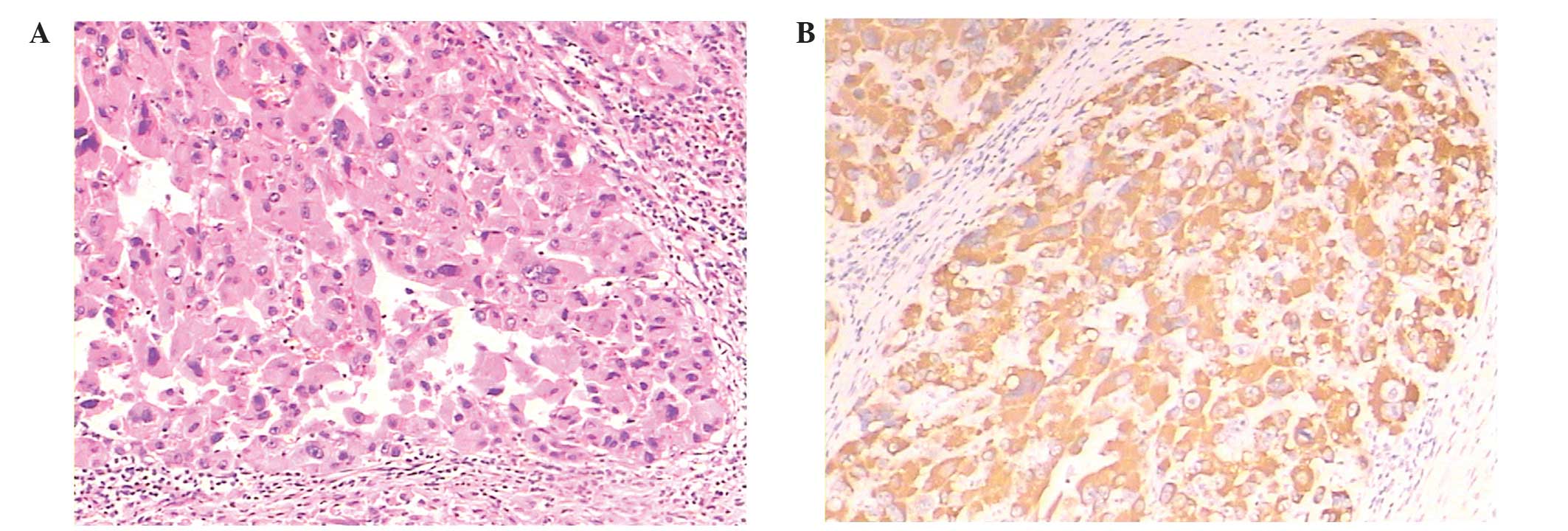
Histologically, staining with hematoxylin and eosin (Fig. 2A) of formalin-fixed paraffin-embedded
4-µm thick tumor tissues under a microscope (BX43; Olympus
Corporation, Tokyo, Japan) using a DAB Peroxidase Substrate kit
(Vector Laboratories, Inc., Burlingame, CA, USA) revealed that the
tumor was composed of poorly differentiated cancer cells with
abundant eosinophilic cytoplasm and round nuclei, resembling
hepatocellular carcinoma. The cells were arranged in trabecular and
solid mass-like growth patterns. The tissue sections were
immunostained with the following primary antibodies: Monoclonal
mouse anti-hepatocyte (clone OCH1E5; dilution, 1:200; catalog. no.,
IS62430; Dako, Glostrup, Denmark); monoclonal mouse anti-cluster of
differentiation (CD)34 (dilution, 1:200; catalog no., ab30375;
Abcam, Cambridge, MA, USA); and monoclonal rabbit anti-CD10
(dilution, 1:200; catalog no., 790-4506; Roche Diagnostics,
Indianapolis, IN, USA), overnight at 4°C. The samples were
subsequently incubated with horseradish peroxidase-conjugated
secondary antibody (goat anti-mouse; catalog no., A0216; goat
anti-rabbit; catalog no., A0208; both dilution, 1:500; both from
Beyotime Institute of Biotechnology, Haimen, China) for 30 min at
37°C. Immunohistochemical staining was positive for hepatocyte
paraffin 1 (Fig. 2B), CD10 and CD34
in the vessels; AFP, thyroid transcription factor-1, cytokeratin
8/18, CD56, chromogranin A, synaptophysin and napsin A were
negative. The Ki-67 score was observed to be 20%. The tumor had
invaded the lung capsule; however, all sampled lymph nodes were
observed to be free of tumor involvement. Consequently, the
histological type was determined to be hepatoid adenocarcinoma, and
the pathological stage was determined to be Ib (pT2aN0M0).
The patient received regular outpatient follow-up
and no local recurrence or distant metastasis was found after 23
months. The serum AFP level remained within the normal range. It is
expected that long-term survival can be expected in the present
case, although careful follow-up observations are required.
Written informed consent was obtained from the
patient for publication of the present case report and any
accompanying images. The present study was approved by the Medical
Ethics Committee of Weifang People's Hospital (Weifang, China).
Discussion
HAL is an extremely rare tumor that was first
described by Ishikura et al (3). Subsequent reports in case series or
single case reports have described the clinical manifestations and
pathological features of HAL; however, to the best of our
knowledge, little has been discussed regarding its CT findings,
with the exception of one paper (2).
Thus, the present study aimed to enrich the available information
regarding clinical findings, imaging characteristics and treatment
protocols of HAL and to ascertain their associations with
prognosis. A total of 18 cases were identified from 14 reports in
the English literature with available full texts on HAL confirmed
by histopathology. These cases, in addition to the present case,
were reviewed, and the clinical findings, imaging features and
prognosis were extracted for analysis (Table I).
 | Table I.Clinical features of previous and
present cases of hepatoid adenocarcinoma of the lung. |
Table I.
Clinical features of previous and
present cases of hepatoid adenocarcinoma of the lung.
|
|
|
| Tumor | AFP |
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Author | Age
(years)/gender | Smoker | Location | Size (cm) | Serum (ng/ml) | IHC expression | Stage | Treatment | Prognosis /
progression | Ref. |
|---|
| Wu et al | 50/M | Yes | RUL | 4.6 | 2.14 | (+) | IIa T2aN1M0 | Surgery | A, 45 months | (2) |
| Arnould et
al | 36/M | Yes | LUL | 10.0 | 6,090 | / | IV pT4N2M0 | Adjuvant chemotherapy
and surgery | Brain metastasis and
chest wall relapse; D, 7 months | (5) |
| Hiroshima et
al | 71/M | Yes | RLL | 10.5 | 7417 | (+) | IIIa pT3N1M0 | Surgery | Lung and brain
metastases; D, 1 year | (6) |
| Terracciano et
al | 44/M | / | LLL | 5.0 | 203,320 | (++) | IV cT2aN1M1b | Surgery | Liver, adrenal and
brain metastases; D, 2 months | (7) |
| Kishimoto et
al | 64/M | / | LLL | 7.0 | 673 | (+) | IIIa cT3 N0 M0 | Surgery | / | (8) |
| Papatsimpas et
al | 48/M | / | RUL | 20.0 | 39,000 | (+) | IIIa cT4N0M0 | Chemotherapy and
palliative radiotherapy | Lung metastasis; D, 6
months | (9) |
| Lin et al | 66/M | Yes | RUL | 7.3 | 8,686 | (+) | IIIa pT3N0M0 | Surgery and
chemotherapy | No progression; A, 4
years | (10) |
| Haninger et
al | 51/M | Yes | RUL | 4.2 | 1.3a | / | IIIb cT2aN3M0 | Chemoradiation and
local debulking | D, 14 months | (11) |
| Haninger et
al | 52/M | Yes | RUL | 2.5 | / | / | IV cT1bN0M1b | Surgery and
adjuvant chemoradiation | Adrenal gland and
brain metastases; A, 37 months | (11) |
| Haninger et
al | 64/M | Yes | LUL | 3.2 | 1.0a | (+) | IV cT2aN0M1b | Surgery and
adjuvant chemoradiation | C2 vertebral body
and liver metastasis; D, 10 months | (11) |
| Haninger et
al | 54/F | Yes | LUL | 1.0 | / | (−) | IV cT1aN0M1b | Chemoradiation | Lung, skull bone
and pericardium metastases; A, 9 years | (11) |
| Haninger et
al | 60/M | Yes | RUL | 11.2 | 4,410 | (+) | IV cT3N2M1b | Chemoradiation | Brain metastasis;
A, 1 month | (11) |
| Shaib et
al | 53/F | Yes | RUL | 9.5 | 37,810 | / | IIIa pT3N0M0 | Surgery and
adjuvant chemotherapy | A, 4 years | (12) |
| Che et
al | 48/M | Yes | LUL | 10.0 | 6,283 | (+) | IIIa cT4N0M0 | Chemoradiation | Lung metastases; D,
19 months | (13) |
| Fornasa | 68/F | No | LUL | 4.5 | 2.4 | / | IV T2aN0M1b | Chemotherapy | A, 15 months | (14) |
| Carlinfante et
al | 82/M | Yes | LLL | 3.5 | / | (−) | Ib pT2aN0M0 | Surgery | No progression; A,
7 years | (15) |
| Mokrim et
al | 52/M | Yes | LUL | 11.8 | 5,000 | (+) | IV cT4N0M1a | Chemotherapy | A, 2 months | (16) |
| Hayashi et
al | 55/M | Yes | RUL | 6.5 | 89a | (+) | IIa pT2bN0M0 | Surgery | No progression; A,
32 months | (17) |
| Present case | 59/M | Yes | RUL | 4.5 | / | (−) | Ib T2aN0M0 | Surgery | A, 6 months |
|
Clinically, patients with HAL typically presented
with nonspecific symptoms, including chest pain, back pain,
shooting pain in the shoulder, cough and dyspnea, asthenia,
anorexia and weight loss. The ages at diagnosis ranged from 36 to
82 years. Smoking history was available in 16 cases, of which 15
had a history of tobacco smoking. In the reviewed cases, the
incidence of HAL was markedly higher in men than in women (16 vs. 3
cases; male to female ratio, ~5.3:1); notably, no significant
gender predominance has been identified in reports on hepatoid
adenocarcinoma of the stomach (4).
The size of the HAL masses reviewed herein was variable, ranging
from 1.0 to 20.0 cm.
In the majority of cases of HAL described in the
literature (5–13), HAL was considered to be associated
with positive AFP expression on histopathology and/or elevated
serum AFP. However, not all HALs produced AFP: The serum AFP levels
of 2 cases (2,14) were within the normal ranges prior to
surgery, and immunohistochemical AFP expression was negative in 3
cases, including the present case (11,15). These
findings are consistent with the opinion of Haninger et al
(11) that AFP expression is not
requisite for diagnosis of HAL, and that the diagnosis depends on
the recognition of characteristic histological features. Therefore,
although no AFP expression was detected in present case, the
diagnosis was still established based on morphology and
immunophenotype.
In the reviewed literature, decreasing AFP level
following surgical resection was observed in 7 cases (5,6,9,12,13,16,17), and,
in 3 cases (5,9,13), the
level was elevated markedly when the patient relapsed. Thus, the
serum AFP level appears to be a reliable indicator to monitor
disease response to therapy, relapse and aggravation, and this may
be identified much earlier than any indication from imaging
findings (18).
Although CT images were only provided in 7 cases in
the literature review (2,9,11,16), in addition to the present case,
certain information was also obtained indirectly from a description
of CT features and/or pathological specimens (11 cases). These data
indicated the following findings. Firstly, the location of the
tumor was characteristic, with the majority (15/18 cases) located
in the upper lung fields, and a tendency to be adjacent to the
costal pleura (5 cases) or mediastinal pleura (6 cases); the former
often adhered to the chest wall, while paramediastinal HALs were
adjacent to blood vessels, meaning that it was easy for them to
invade the structures of the homolateral mediastinum (including the
trachea and esophagus) invasion. Secondly, whilst none of the
imaging features is considered typical enough to diagnose HAL
directly, certain findings should be regarded as concerning. HAL
tumors usually appeared inhomogeneous, and large necrotic areas may
be detected in the tumor and also observed by pathological
examination (2,5,6,9–11,15,17); this
is consistent with the report by Wu et al (2). Following contrast enhancement, the
tumors exhibited a mild to moderate inhomogeneous enhancement and
the necrotic areas appeared more clearly. In summary, imaging
evaluation serves a limited but useful role in the selection of a
therapeutic schedule for HAL, as it is able to detect lymph node or
distant metastases and help to assess the clinical stage. Knowledge
of HAL imaging characteristics is evolving and may in future
indicate associations with prognosis.
The limitations of the published literature for
establishing prognostic indicators included the limited number of
patients, short follow-up time and variable disease stages at
diagnosis. Generally, HAL is considered to be associated with a
poor prognosis (5,7,9). However,
prognosis is likely to be associated with clinical stage; as
reported by Carlinfante et al (15), one patient had a good prognosis (7
years survival) after having a tumor with small dimensions and
without extension outside of the lung (stage T2aN0M0). The
significance of staging is also indicated by the cases of stage IIa
(pT2bN0M0) and stage IIa (T2aN1M0) disease, as reported by Hayashi
et al (17) and Wu et
al (2), in which the tumors were
successfully cured by local excision and no signs of recurrence and
metastasis were observed after 32 and 45 months post surgery,
respectively. In the reviewed literature, the cases receiving
surgery and/or chemoradiation, even at an intermediate to advanced
stage, also showed favorable prognoses (10–12). These
findings suggest that clinical stage represents a significant
prognostic factor in HAL, but that curative resection and
reasonable adjuvant chemoradiation also have a substantial
influence on the prognosis of HAL at these stages (9).
It was noteworthy that a female patient with stage
IV disease (cT1aN0M1b) with negative AFP expression had the longest
survival time of 9 years out of all cases followed up, and the
metastatic lesion in this patient was controlled completely by
chemoradiation. AFP expression in the case reported by Carlinfante
et al (15) was also negative.
These two cases support the opinion of Papatsimpas et al
(9) that the patients with normal AFP
levels at presentation tended to have a better overall survival
time, even after relapse; this is likely to represent a different
subset of HAL with better biological behavior. Based on the above
analysis, we considered that long-term survival could be expected
in our case, although close follow-up was undertaken.
HAL is a rare tumor that is difficult or impossible
to distinguish from other malignant entities in the lung by imaging
alone (2,5,15,17). The number of recorded cases in the
English literature, including the present case, is small, and any
firm conclusions cannot be drawn; however, a mass in the lung
located adjacent to the costal or mediastinal pleura, with a large
necrotic region and mild to moderate inhomogeneous enhancement,
together with elevated serum AFP levels, should indicate the
possibility of HAL if there is no lesion present in the liver
(2,17).
In conclusion, the present study reported a case of
HAL without AFP production in which the patient underwent radical
right upper lobectomy via single-port VATS. The patient received
regular outpatient follow-up and no local recurrence or distant
metastasis was observed after 23 months. The serum AFP level
remained within the normal range. In general, although HAL is
usually associated with poor prognosis, for early stage HAL
patents, radical surgical resection may markedly increase the cure
rate (3,15,17,19). Even
for patients in whom lymph node or distant metastases are detected,
palliative lobectomy and adjuvant chemoradiation are considered
appropriate treatments to improve the survival time (10–12,20).
However, the optimal management of HAL is still not well defined
and further investigations are required (10–12,20). In
addition, once the diagnosis of HAL is confirmed by
immunohistochemistry, clinicians should be aware that monitoring
serum AFP levels, as well as CT findings, remains important.
References
|
1
|
Su JS, Chen YT, Wang RC, Wu CY, Lee SW and
Lee TY: Clinicopathological characteristics in the differential
diagnosis of hepatoid adenocarcinoma: A literature review. World J
Gastroenterol. 19:321–327. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wu Z, Upadhyaya M, Zhu H, Qiao Z, Chen K
and Miao F: Hepatoid adenocarcinoma: Computed tomographic imaging
findings with histopathologic correlation in 6 cases. J Comput
Assist Tomogr. 31:846–852. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ishikura H, Kanda M, Ito M, Nosaka K and
Mizuno K: Hepatoid adenocarcinoma: A distinctive histological
subtype of alpha-fetoprotein producing lung carcinoma. Virchows
Arch A Pathol Anat Histopathol. 417:73–80. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nagai E, Ueyama T, Yao T and Tsuneyoshi M:
Hepatoid adenocarcinoma of the stomach. A clinicopathologic and
immunohistochemical analysis. Cancer. 72:1827–1835. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arnould L, Drouot F, Fargeot P, Bernard A,
Foucher P, Collin F and Petrella T: Hepatoid adenocarcinoma of the
lung: Report of a case of an unusual alpha-fetoprotein-producing
lung tumor. Am J Surg Pathol. 21:1113–1118. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hiroshima K, Iyoda A, Toyozaki T, Haga Y,
Baba M, Fujisawa T, Ishikura H and Ohwada H:
Alpha-fetoprotein-producing lung carcinoma: Report of three cases.
Pathol Int. 52:46–53. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Terracciano LM, Glatz K, Mhawech P, Vasei
M, Lehmann FS, Vecchione R and Tornillo L: Hepatoid adenocarcinoma
with liver metastasis mimicking hepatocellular carcinoma: An
immunohistochemical and molecular study of eight cases. Am J Surg
Pathol. 27:1302–1312. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kishimoto T, Yano T, Hiroshima K, Inayama
Y, Kawachi K and Nakatani Y: A case of *-fetoprotein-producing
pulmonary carcinoma with restricted expression of hepatocyte
nuclear factor-4* in hepatoid foci: A case report with studies of
previous cases. Hum Pathol. 39:1115–1120. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Papatsimpas G, Kamposiorasa K, Goulab K,
Papaparaskeva K, Loukides S, Kotoulas C, Kelekis N, Xiros N,
Pectasides D and Koumarianou A: Hepatoid pancoast tumor. A case
report and review of the literature. Lung Cancer. 77:239–245. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lin SF, Hsu WH and Chou TY: Primary
pulmonary hepatoid carcinoma: Report of a case and review of the
literature. Kaohsiung J Med Sci. 29:512–516. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Haninger DM, Kloecker GH, Bousamra Ii M,
Nowacki MR and Slone SP: Hepatoid adenocarcinoma of the lung:
Report of five cases and review of the literature. 27:535–542.
2014.
|
|
12
|
Shaib W, Sharma R, Mosunjac M, Farris AB
III and El Rayes B: Hepatoid adenocarcinoma of the lung: A case
report and review of the literature. J Gastrointest Cancer.
45(Suppl 1): 99–102. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Che YQ, Wang S, Luo Y, Wang JB and Wang
LH: Hepatoid adenocarcinoma of the lung: Presenting mediastinal
metastasis without transfer to the liver. Oncol Lett. 8:105–110.
2014.PubMed/NCBI
|
|
14
|
Fornasa F: Soft-tissue localization of
hepatoid adenocarcinoma: First case report. Case Rep Oncol.
3:212–217. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carlinfante G, Foschini MP, Pasquinelli G,
Scotti R and Cavazza A: Hepatoid carcinoma of the lung: A case
report with immunohistochemical, ultrastructural and in-situ
hybridization findings. Histopathology. 37:88–89. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mokrim M, Belbaraka R, Allaoui M,
Kairaouani M, Mahassini N, Tahri A and Errihani H: Hepatoid
adenocarcinoma of the lung: A case report and literature review. J
Gastrointest Cancer. 43(Suppl 1): 125–127. 2012. View Article : Google Scholar
|
|
17
|
Hayashi Y, Takanashi Y, Ohsawa H, Ishii H
and Nakatani Y: Hepatoid adenocarcinoma in the lung. Lung Cancer.
38:211–214. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Furukawa H, Oda K, Nishie K, Miyake K, Ota
K, Nishida K, Munakata T, Ikeda H, Onaru K and Goma I: A case of
alpha-fetoprotein-producing recurrent lung adenocarcinoma
successfully treated with radiation therapy (high-grade
adenocarcinoma of fetal lung type). Gan To Kagaku Ryoho.
39:2393–2395. 2012.(In Japanese). PubMed/NCBI
|
|
19
|
Slotta JE, Jüngling B, Kim YJ, Wagner M,
Igna D and Schilling MK: Hepatoid adenocarcinoma of the transverse
colon. Int J Colorectal Dis. 27:989–991. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kitada M, Ozawa K, Sato K, Matsuda Y,
Hayashi S, Tokusashi Y, Miyokawa N and Sasajima T:
Alpha-fetoprotein-producing primary lung carcinoma: A case report.
World J Surg Oncol. 9:472011. View Article : Google Scholar : PubMed/NCBI
|