Introduction
Semi-invasive aspergillosis, also known as chronic
necrotizing pulmonary aspergillosis, is a form of aspergillosis
infection in which the fungus demonstrates an intermediate
phenotype between a simple saprophyte and an invasive pathogen
(1). This form of aspergillosis
infection is extremely rare in patients with normal immunity. The
major risk factor triggering invasiveness of aspergillosis is the
significant compromise of immune function due to various insults,
including underlying immunodeficiency or malignancy, cytotoxic
chemotherapies and conditioning regimens for solid organ or
hematopoietic stem cell transplantation. These insults are also
known to contribute to poor patient outcome (2,3).
Sunitinib, an indolin-2 analog that inhibits various
types of receptor tyrosine kinases (RTKs), is currently the
treatment of choice in patients with metastatic renal cell
carcinoma and imatinib-resistant gastrointestinal stromal tumors
(4,5).
Adverse effects including cytopenia, diarrhea, nausea, skin
symptoms and abnormal heart functions are reported, but
opportunistic fungal infection caused by sunitinib treatment is a
rare condition of unknown incidence and prognosis (5,6). Here, we
report a case of pulmonary aspergilloma that progressed to
semi-invasive aspergillosis following sunitinib treatment. Written
informed consent was obtained from the patient for this study.
Case report
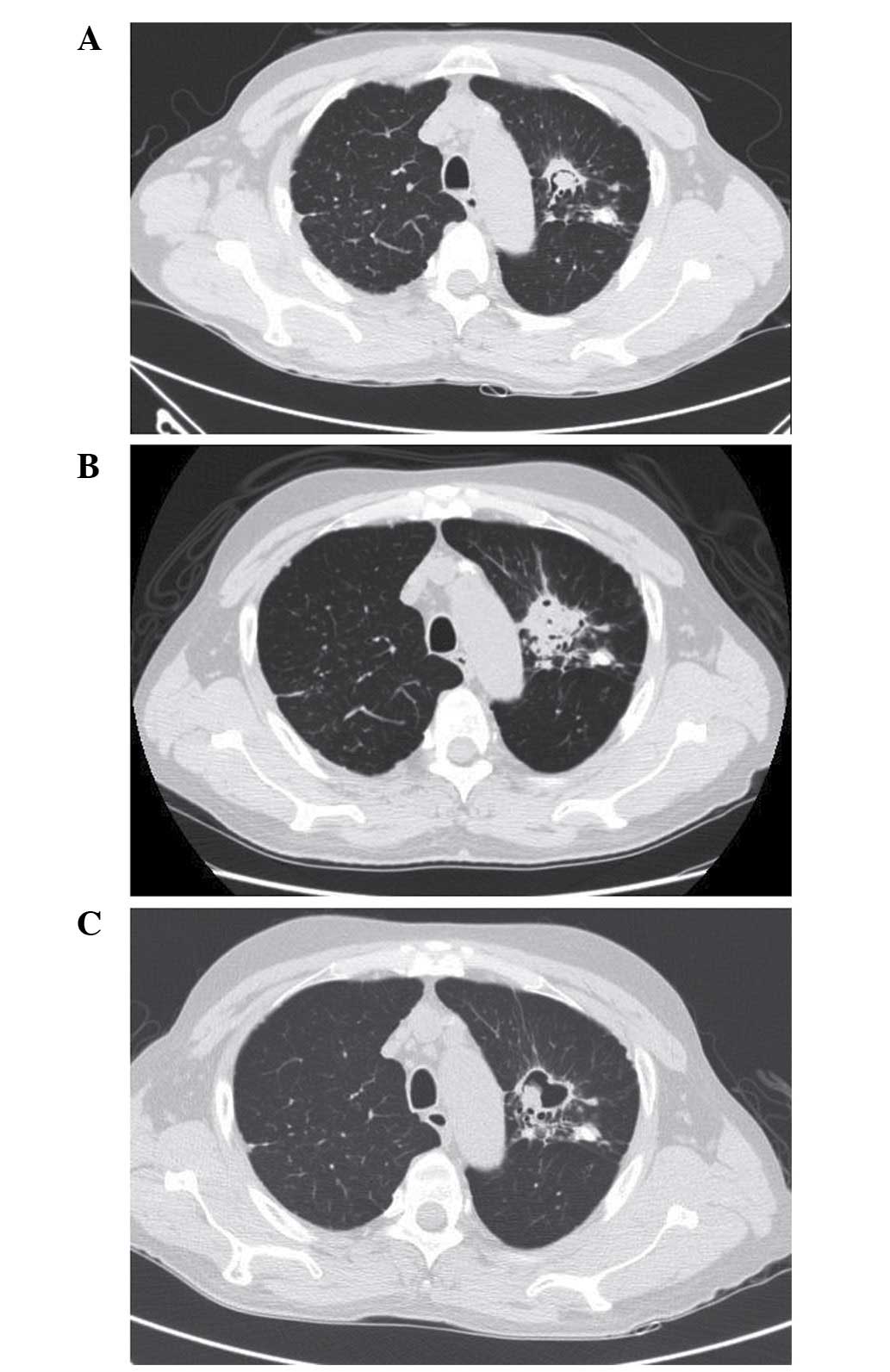
A 59-year-old male had previously been diagnosed
with stable aspergilloma in the upper lobe of the left lung and was
undergoing routine follow-up and observation of the size of the
fungal ball (Fig. 1A). After 7
months, the patient presented with chest discomfort and was
eventually diagnosed with renal cell carcinoma of the right kidney,
with distant metastasis to the left eighth rib. He underwent right
radical nephrectomy with chest wall resection. After recovering
from surgery, he started adjuvant chemotherapy with sunitinib. This
treatment was continued for 8 months.
During the ninth month of sunitinib therapy,
hemoptysis developed and reached a level of ~400 ml in the last 10
days of treatment. Physical examination revealed decreased
breathing sounds in the left upper lung. Blood tests revealed
decreased hemoglobin levels (9.9 g/dl) and increased C-reactive
protein levels (3.91 mg/dl). Prothrombin time, activated partial
thromboplastin time, fibrinogen levels and liver function tests
were all within the normal ranges. Chest computed tomography
revealed interval development of paramediastinal consolidation and
bronchial wall thickening in the left upper lobe, with an increased
soft tissue mass and air crescent sign in the underlying
aspergilloma lesion. Left bronchial artery hypertrophy was also
observed (Fig. 1B). Bronchial artery
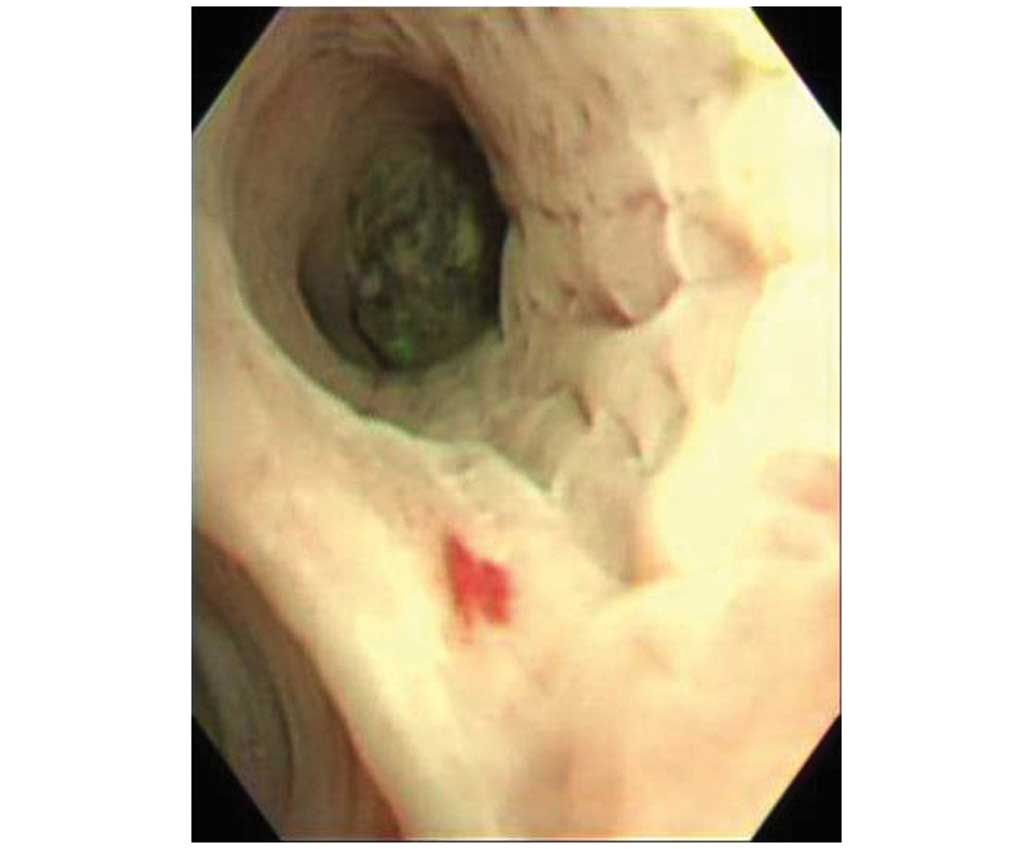
embolization was performed to control hemoptysis. Upon
bronchoscopic examination, a round, black fungal ball was noted to
be impacted in the apicoposterior segment of the upper division of
the left upper lobe (Fig. 2). An
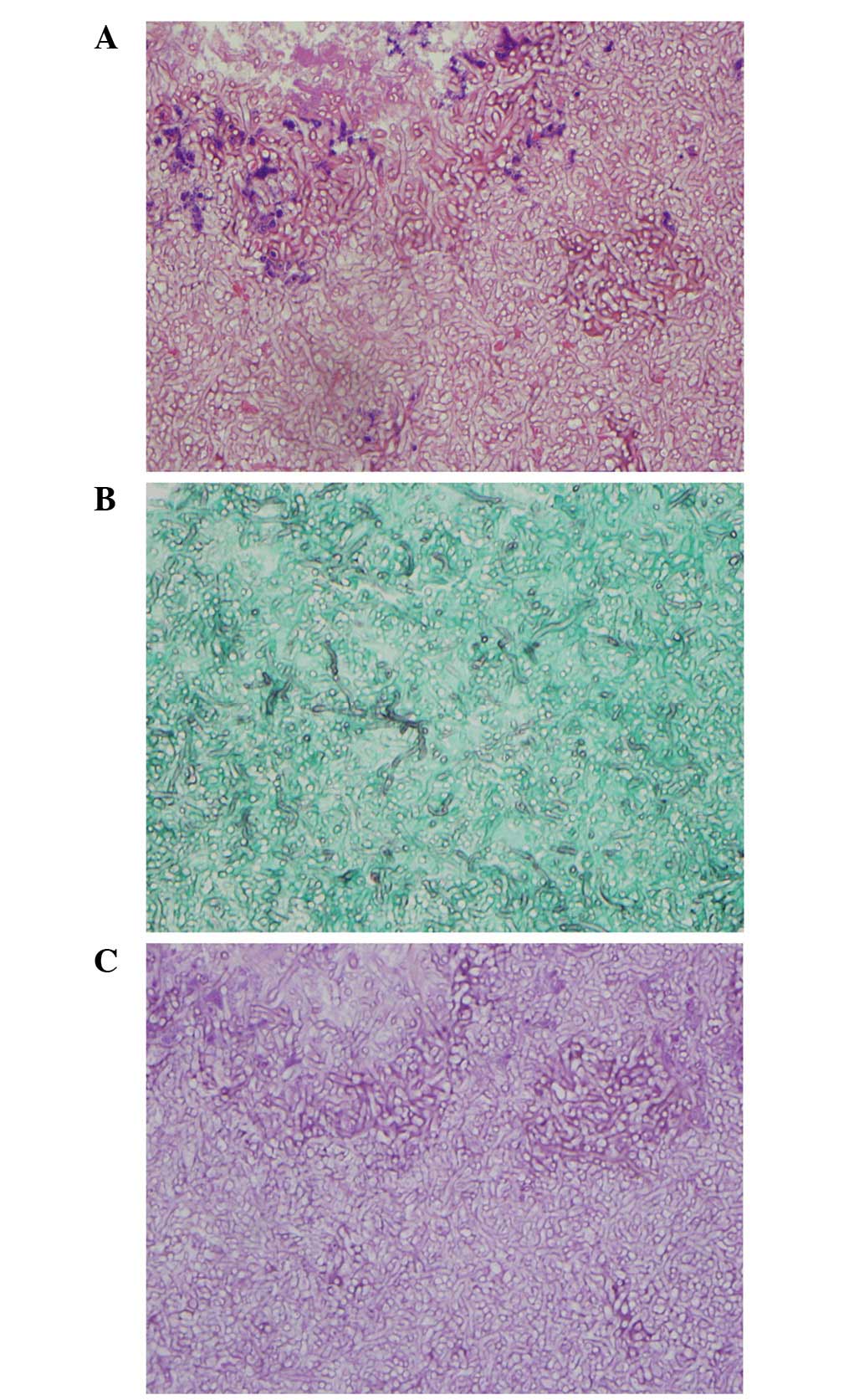
endoscopic biopsy was taken from the visible mass. Pathological
examination including Gomori methenamine silver and periodic
acid-Schiff staining revealed numerous fungal hyphae, which were
morphologically consistent with aspergillosis (Fig. 3).
Sunitinib therapy was discontinued, and the patient
was started on treatment with oral voriconazole (200 mg bid).
Treatment with voriconazole led to an improvement in his symptoms
and radiological resolution of consolidation around the
aspergilloma. A cavity remained in the left lung following
antifungal treatment (Fig. 1C).
Discussion
The typical niches of Aspergillus are air,
soil, food and decaying organic material. The conidia of
Aspergillus are easily dispersed into the air and when they
reach a permissive environment, such as the lung of an
immunosuppressed patient, they germinate into hyphae, the invasive
form of Aspergillus (7). The
virulence of aspergillosis depends on the immune status of the
host, but leads to poor outcome in patients with significantly
compromised immune function, regardless of the cause (3). Compared with the notably high incidence
and mortality of invasive aspergillosis among patients undergoing
cytotoxic regimens during hematopoietic cell transplantation,
invasive and semi-invasive forms of aspergillosis are relatively
rare in patients undergoing targeted chemotherapy with RTK
inhibitors. To date, there has been only one reported case of
invasive aspergillosis occurring following treatment with sunitinib
(5).
In the current case, the patient had underlying
stable pulmonary aspergilloma prior to the diagnosis of renal cell
carcinoma and sunitinib treatment. In the majority of patients,
stable aspergilloma does not change in size or invade the
surrounding tissue. It is reported to spontaneously resolve or
decrease in size in ~13% of cases (8). Therefore, stable aspergilloma does not
usually require active treatment. During follow-up, an increase in
size or conversion into a semi-invasive/invasive form of
aspergillosis is rare (8,9).
In the present case, stable aspergilloma progressed
and converted to semi-invasive aspergillosis after sunitinib
therapy was adopted. For the treatment of semi-invasive
aspergillosis, antifungal agents including voriconazole,
amphotericin B and itraconazole should be used promptly. Surgical
resection should be considered for patients with recurrent
hemoptysis and those intolerant or resistant to antifungal therapy
(9).
Sunitinib inhibits various RTKs including vascular
endothelial growth factor receptors 1 and 2, platelet-derived
growth factor receptors and fibroblast growth factor receptor 1,
leading to a 40–44% partial response rate in metastatic renal cell
carcinoma patients (10). Previous
studies also suggest that sunitinib inhibits the phosphorylation of
signal transducer and activator of transcription 3 (Stat3) and
Src-tyrosine kinase, suppressing the response of Th-1-type
cytokines and SYK-tyrosine kinase, which uses Stat3 as a substrate.
Th-1-type cytokine responses and SYK-dependent signals are known to
be significant in the mechanism of host defense against
Aspergillus and other fungi (5). Therefore, it is likely that inhibition
of Stat3 by sunitinib plays a key role in the development of
aspergillosis infections in patients taking this medication.
The current case suggests that clinicians should be
aware of the potential risk of opportunistic fungal infections in
patients undergoing sunitinib treatment. In particular, patients
with underlying stable aspergilloma who are planning to undergo
sunitinib therapy should be warned of the risk of conversion into
semi-invasive or invasive pulmonary aspergillosis. In such
patients, monitoring of the symptoms of invasive aspergillosis and
radiological changes in the underlying stable aspergilloma is
required.
References
|
1
|
Gefter WB, Weingrad TR, Epstein DM, Ochs
RH and Miller WT: ‘Semi-invasive’ pulmonary aspergillosis: a new
look at the spectrum of aspergillus infections of the lung.
Radiology. 140:313–321. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Salgado SM, Costa CA, Buqalho AA, Semedo
JA, Ribeiro JC and Carreiro LM: Semi-invasive aspergillosis in an
immunocompetent patient with Swyer-James-MacLeod syndrome: a case
report. J Med Case Rep. 4:1532010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Upton A, Kirby KA, Carpenter P, Boeckh M
and Marr KA: Invasive aspergillosis following hematopoietic cell
transplantation: outcomes and prognostic factors associated with
mortality. Clin Infect Dis. 44:531–540. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chow LQ and Eckhardt SG: Sunitinib: from
rational design to clinical efficacy. J Clin Oncol. 25:884–896.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Visvardis EE, Gao F, Paes MN, Duprez O and
Waxman J: Lung Aspergillosis in renal cell carcinoma patient
treated with sunitinib. QJM. 105:689–692. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hoshino Y, Hasegawa H, Ishii Y, Endo T,
Ochiai H, Okabayashi K, Kaneko G, Mikami S, Mukai M, Oya M and
Kitagawa Y: Two cases of bowel perforation associated with
sunitinib treatment for renal cell carcinoma. Int J Clin Oncol.
17:412–416. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Garcia-Vidal C, Viasus D and Carratalà J:
Pathogenesis of invasive fungal infections. Curr Opin Infect Dis.
26:270–276. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lee JK, Lee YJ, Park SS, Park JS, Cho YJ,
Park YS, Yoon HI, Lee CT and Lee JH: Clinical course and prognostic
factors of pulmonary aspergilloma. Respirology. 19:1066–1072. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cabral FC, Marchiori E, Zanetti G,
Takayassu TC and Mano CM: Semi-invasive pulmonary aspergillosis in
immunosuppressed patient: a case report. Cases J. 2:402009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Goodman VL, Rock EP, Dagher R, Ramchandani
RP, Abraham S, Gobburu JV, Booth BP, Verbois SL, Morse DE, Liang
CY, et al: Approval summary: sunitinib for the treatment of
imatinib refractory or intolerant gastrointestinal stromal tumors
and advanced renal cell carcinoma. Clin Cancer Res. 13:1367–1373.
2007. View Article : Google Scholar : PubMed/NCBI
|