Introduction
Lung cancer is one of the most common malignant
tumors to occur, worldwide. The two major subtypes are small cell
lung cancer (SCLC) and non-small cell lung cancer (NSCLC) (1). NSCLC accounts for ~85% of all lung
cancer cases (2). For early-stage or
locally advanced lung cancer, surgery is the most effective
treatment and combined chemotherapy is the standard adjuvant
approach. However, ~40% of patients with NSCLC present with
unresectable, metastatic stage IV tumors (3). The prognosis is poor, and the overall
5-year survival rate remains <15% (2). Since the effectiveness of current
standard treatment for advanced NSCLC (i.e. chemotherapy) has
reached a ceiling (4), there is a
continuous requirement for novel, more effective treatments to
further improve the outcome of patients with the disease.
Epidermal growth factor receptor (EGFR) is a
transmembrane glycoprotein that is overexpressed in numerous solid
tumors, including NSCLC (5). The
binding of a ligand, for example transforming growth factor-α or
epidermal growth factor, to EGFR triggers tyrosine kinase
phosphorylation, which in turn activates cellular pathways,
including the mitogen-activated protein kinase,
phosphatidylinositol 3′ kinase and protein kinase B pathways. The
ultimate result is cell growth and tumor progression. Therefore,
EGFR is an important therapeutic target in NSCLC (6).
Cetuximab (Erbitux®) is a chimeric
human-murine monoclonal immunoglobulin (Ig)G1 antibody. It blocks
ligand binding to EGFR, leading to a decrease in receptor
dimerisation, autophosphorylation and activation of signaling
pathways (7). Cetuximab may also act
by means of antibody-dependent cellular cytotoxicity and
complement-dependent cytotoxicity (2). In 2004, the results of a single-agent
phase II study of cetuximab in recurrent NSCLC were reported, with
29 EGFR-positive patients showing a partial response rate of 7% and
a stable disease rate of 17% (8). Two
randomized phase III trials that evaluated cetuximab in NSCLC
patients showed a small benefit in terms of overall survival for
the experimental treatment, which was considered insufficient by
the European Medicines Agency for marketing approval (1). One of the possible reasons for limited
therapeutic efficacy of cetuximab in NSCLC may be that the
increased interstitial fluid pressure inside the tumor prevents the
antibody from being delivered into the extravascular tumor tissue
(9–12).
The tumor-targeted delivery of anticancer agents is
considered as a novel strategy to traditional chemotherapy.
Tumor-targeted delivery has been proved to selectively increase the
drug concentration at the tumor site and significantly improve the
therapeutic efficacy (13).
Previously, a tumor-penetrating internalizing RGD peptide (iRGD;
amino acid sequence, CRGDK/RGPD/EC), was identified and reported to
increase vascular and tissue penetration in a tumor-specific and
neuropilin-1 (NRP-1)-dependent manner (14). The RGD tripeptide of iRGD can bind the
αvβ3 and αvβ5 integrins, the expression of which is largely
restricted to tumors, including tumor vasculature and cells
(14,15). When iRGD binds to integrins, the
peptide bond between the K and G amino acids is proteolytically
cleaved by the cell surface-associated proteases to expose the
cryptic C-end rule (CendR) motif (amino acid sequence, CRGDK/R),
which then binds to NRP-1 (14–17). The
activation of NRP-1 increases the permeability of blood vessels and
tumor tissues, which allows drugs to penetrate into the internal
tissue of the tumor much more easily (14,15,18). Thus,
when anticancer agents are modified with iRGD, the
tissue-penetrating and tumor-targeting properties can be improved.
Additionally, when iRGD was previously co-administered with drugs
or a systemic injection drug delivery system, antitumor activities
were also improved (18).
The characteristics of iRGD in solid cancers appear
to warrant further investigation; particularly, for patients with
diseases that have a dismal prognosis, such as NSCLC. However,
there have been no comprehensive in vivo studies using NSCLC
models, and the effects of iRGD used in combination with cetuximab
have not yet been tested. Therefore, the present study examined the
effectiveness of iRGD for boosting cetuximab accumulation in NSCLC
xenograft models established with the A549 cell line. The
anticancer booster effect of combination therapy with cetuximab
plus iRGD was evaluated with in vivo experiments.
Materials and methods
Cell culture
The human NSCLC-derived A549 cell line was purchased
from the Shanghai Institute of Biochemistry and Cell Biology,
Chinese Academy of Sciences (Shanghai, China), and cultured in
F-12K medium with 10% fetal bovine serum and 1%
penicillin/streptomycin (all Gibco; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA). Cells were cultured in a humidified atmosphere
containing 5% CO2 at 37°C.
Flow cytometry
A total of 1×106 A549 cells were
incubated with fluorescent-labeled antibodies diluted in 100 µl
phosphate-buffered saline (PBS) for 30 min at room temperature. The
cells were then washed, suspended and evaluated with a FACS machine
(FACSCanto II; BD Biosciences, Franklin Lakes, NJ, USA). A matched
isotype control antibody was used in all analyses. Finally, all the
data were analyzed by FlowJo 7.6.1 software (FlowJo, LLC, Ashland,
OR, USA). Integrin αvβ3 was detected using a fluorescein
isothiocyanate (FITC)-conjugated mouse anti-human integrin αvβ3
monoclonal antibody (1:100; cat. no. MAB1976; EMD Millipore,
Billerica, MA, USA), and integrin αvβ5 was detected using a
FITC-conjugated mouse anti-human integrin αvβ5 monoclonal antibody
(1:100; cat. no. MAB1961F; EMD Millipore). The matched isotype
control, FITC-conjugated mouse IgG1κ, was purchased from
eBioscience, Inc. (San Diego, CA, USA; 1:100; cat. no. 11-4714-41).
NRP-1 was detected using a phycoerythrin (PE)-conjugated mouse
anti-human NRP-1 monoclonal antibody and an isotype control (both
1:100; cat. nos. 130-098-876 and 130-098-845, respectively;
Miltenyi Biotec GmbH, Bergisch Gladbach, Germany). EGFR was
detected using a PE-conjugated mouse anti-human EGFR monoclonal
antibody and an isotype control (both 1:100; cat. nos. 555997 and
555743, respectively; BD Biosciences).
Mice and in vivo experiments
In vivo experiments involved 69 six-week-old
female BALB/C nude mice (Vital River Laboratory Animal Technology
Co., Ltd, Beijing, China), which were housed in the specific
pathogen-free animal facility of Experimental Animal Center, Xuzhou
Medical College (Xuzhou, China). Animals were housed with a 12-h
light/dark cycle, at 22±1°C, and in a 55±5% humidity-controlled
room. All mice were allowed free access to clean water and food.
All cages housed up to 6 animals and contained wood shavings and an
independent air supply system. All animal experimental protocols
were approved and reviewed by the Institutional Animal Care and Use
Committee of the Jiangsu Provincial Academy of Chinese Medicine
(approval no., SCXK 2012–0005). During in vivo experiments,
animals in all experimental groups were examined daily for physical
activity. At the end of the experiment, mice were sacrificed by
cervical dislocation.
Tumor model
The human NSCLC model was established as previously
described (19). Briefly,
1×107 A549 cells were injected into the left forelimb
armpits of 6 BALB/c nude mice. When the tumors grew to ~150
mm3, the mice were sacrificed by cervical dislocation,
and the tumors were harvested and segmented into tissue blocks (4–6
mm3 in size). Subsequently, the left forelimb armpits of
three BALB/c nude mice were inoculated subcutaneously with the
tissue blocks using a trocar. The mice were sacrificed when the
tumors grew to the desired size.
Immunofluorescence staining
Three mice were used to establish human NSCLC
models. When the tumors reached ~200 mm3, the mice were
sacrificed and the tumors were dissected and sectioned on a
cryostat. For αvβ3, αvβ5 and NRP-1 detection, the sections (n=3)
were incubated overnight at 4°C with the same anti-human αvβ3, αvβ5
and NRP-1, or isotype control antibodies, as those used in the flow
cytometry analysis. After washing, all sections were observed and
photographed with a fluorescence microscope (DS-Ri1; Nikon
Corporation, Toyko, Japan).
Tumor permeability assay
When tumors reached ~200 mm3, the mice
were divided into 4 groups (n=9/group). A total of 30 mg/kg
cetuximab (Merck Millipore, Darmstadt, Germany), 4 mg/kg iRGD
(Shanghai Apeptide Co., Ltd., Shanghai, China), 30 mg/kg
cetuximab+4 mg/kg iRGD or PBS was injected into each of the 4
groups of tumor-bearing mice via the tail vein. After 1, 3 and 9 h,
3 mice per group were anesthetized by intraperitoneal injection
with 3.5% chloral hydrate (0.2 ml/mouse; Shanghai Shifeng
Biological Technology, Co., Ltd., Shanghai, China). After 2 min,
the mice were perfused through the heart with PBS containing 1%
bovine serum albumin (Sigma-Aldrich, St. Louis, MO, USA). The
tumors were then collected and sectioned on a cryostat. The tumor
vasculature marker cluster of differentiation (CD)31 was stained
with a rabbit anti-mouse CD31 polyclonal antibody (cat. no.
ab28364; Abcam, Cambridge, MA, USA) and a DyLight 549-conjugated
goat anti-rabbit IgG (H+L) secondary antibody (cat. no. E032320;
EarthOx Life Sciences, Millbrae, CA, USA) was used for
visualization. Cetuximab was stained with the DyLight
488-conjugated goat anti-human IgG (H+L) antibody (cat. no.
109-485-003; Jackson ImmunoResearch Inc., West Grove, PA, USA). The
nuclei were stained with 4′,6-diamidino-2-phenylindole (Roche
Diagnostics GmbH, Mannheim, Germany). Imaging was performed using a
confocal microscope (OLS4100; Olympus Corporation, Tokyo, Japan).
At least 5 random visual areas were chosen in every slide. The
percentage and the integrated optical density (IOD) index of
positively stained regions were scanned and analyzed using
Image-Pro Plus (IPP) 6.0 software (Media Cybernetics Inc.,
Rockville, MD, USA). The penetration distance between the vessel
and where the fluorescence decreased to background levels was also
analyzed using the IPP software.
In vivo efficacy studies
When the tumors reached ~100 mm3, the
mice were divided into 4 groups (n=6/group). The same injections as
described for the tumor permeability assay were performed twice a
week for a total of 8 times. The volume of the tumors was measured
in two perpendicular directions with a caliper, and the weight of
the mice was calculated every 3 days. The volume of the tumor was
measured using the following formula: V=0.5x(W2xL);
where V=tumor volume, W=the smaller perpendicular diameter and
L=the larger perpendicular diameter. On day 30 following the first
injection, the mice were sacrificed and the tumors were collected
and weighed. The tumor growth inhibition ratio (TGIR) was
calculated using the formula: TGIR=(W-Wt)/Wx100; where W
is the average tumor weight of the PBS group and Wt is
the average tumor weight of the treatment group. Each tumor was cut
into two equal parts: one part was fixed in 10% neutral-buffered
formalin for immunohistochemical staining and the TdT-mediated dUTP
nick end labeling (TUNEL) assay; and the other part was snap-frozen
in liquid nitrogen for western blot analysis.
Immunohistochemical staining
The fixed tumor tissues were embedded in paraffin
and cut into 3–5 µm sections (20).
The experiment was performed on with a streptavidin-peroxidase
system (OriGene Technologies, Inc., Beijing, China). EGFR and
phosphorylated EGFR (p-EGFR) were detected with a rabbit anti-human
EGFR antibody (cat. no. ab52894; Abcam) and a rabbit anti-human
p-EGFR antibody (cat. no. 36-9700; Thermo Fisher Scientific, Inc.),
respectively. Imaging was performed by fluorescence microscopy
(DS-Ri1; Nikon Corporation). To determine the IOD indices of EGFR
and p-EGFR, 5 representative visual areas that were positive for
EGFR or p-EGFR were examined from each tumor. The EGFR and p-EGFR
indices for each selected area were analyzed using IPP 6.0
software.
Western blot analysis
Total protein was extracted using
radioimmunoprecipitation assay buffer (Beyotime Institute of
Biotechnology, Nanjing, China) containing 1 mM phenylmethylsulfonyl
fluoride (Sigma-Aldrich). Protein lysates were separated by 10%
SDS-PAGE, followed by transfer to polyvinylidene difluoride
membranes. The membranes were blocked with PBS containing 0.01%
Tween-20 (PBST) and 5% (w/v) fat-free dried milk for 1 h, followed
by incubation with anti-EGFR and anti-p-EGFR antibodies (see
above), and rabbit anti-β-actin polyclonal antibody (cat. no.
ab8227; Abcam) for 1 h. Subsequently, the membranes were washed
five times with PBST and incubated with IRDye 800CW goat
anti-rabbit IgG (H+L) antibody (cat. no. 926-32211; LI-COR
Biosciences, Lincoln, NE, USA) for 1 h. β-actin was detected as an
internal control. After washing the membranes another five times
with PBST, images were captured using an Odyssey enhanced
chemiluminescence system (LI-COR Biosciences) and the intensity of
the bands was quantified by ImageJ2x 2.1.4.7 software (Rawak
Software, Inc., Stuttgart, Germany).
TUNEL assay
The paraffin sections were prepared, as described in
the immunohistochemical staining section. The apoptotic cells were
detected using a TUNEL assay kit (cat. no. 1684809; Roche
Diagnostics), according to the manufacturer's protocol. Imaging was
performed by fluorescence microscopy (DS-Ri1). The number of
TUNEL-positive cells in 5 randomly selected fields from each tumor
was counted. The percent of TUNEL-positive cells was calculated as
the apoptotic index. A total of 100 cells were randomly selected
for each field.
Statistical analysis
SPSS version 16.0 for Windows (SPSS, Inc., Chicago,
IL, USA) was used for all analyses. Quantitative data were
presented as the mean ± standard deviation. Comparisons between two
groups were performed using independent-sample Student's t-tests,
while multiple samples were compared with one-way analysis of
variance, with α=0.05 as a level for the test. Results with a
P-value of <0.05 were considered to indicate a statistically
significant difference.
Results
Expression of ανβ3, ανβ5, NRP-1 and
EGFR in A549 cells and xenograft tissue
The tumor-penetrating ability of iRGD mainly depends
on the level of ανβ3, ανβ5 and NRP-1 in cancer cells (18,21). The
therapeutic efficacy of cetuximab mainly depends on the level of
EGFR in cancer cells (22). In order
to confirm the expression of these molecules in the human NSCLC
A549 cell line, a flow cytometry analysis was performed. As shown
in Fig. 1A, the positive expression
rates of αvβ3, αvβ5, NRP-1 and EGFR were 65.1, 32.0, 88.8 and
96.3%, respectively. This result demonstrated that the A549 cell
line may be used to establish a human NSCLC model for the study of
the combination therapy of cetuximab and iRGD. To confirm the level
of αvβ3, αvβ5, and NRP-1 in tumor tissue, a BALB/c nude mouse
xenograft model was developed with the A549 cell line. The
expression of these molecules in tumor tissue was additionally
detected by immunofluorescence staining. As shown in Fig. 1B, αvβ3 (left), αvβ5 (middle) and NRP-1
(right) were overexpressed in the xenograft tissues.
 | Figure 1.Expression of αvβ3, αvβ5, NRP-1 and
EGFR in A549 cells and xenografts. (A) αvβ3, αvβ5, NRP-1 and EGFR
expression in A549 cells was determined by flow cytometry. (B)
αvβ3, αvβ5, NRP-1 and EGFR expression in mouse xenografts was
determined by immunofluorescence staining. NRP-1, neuropilin-1;
EGFR, epidermal growth factor receptor; EG, experimental group; CG,
control group. Magnification, ×400; Scale bars=50 µm. |
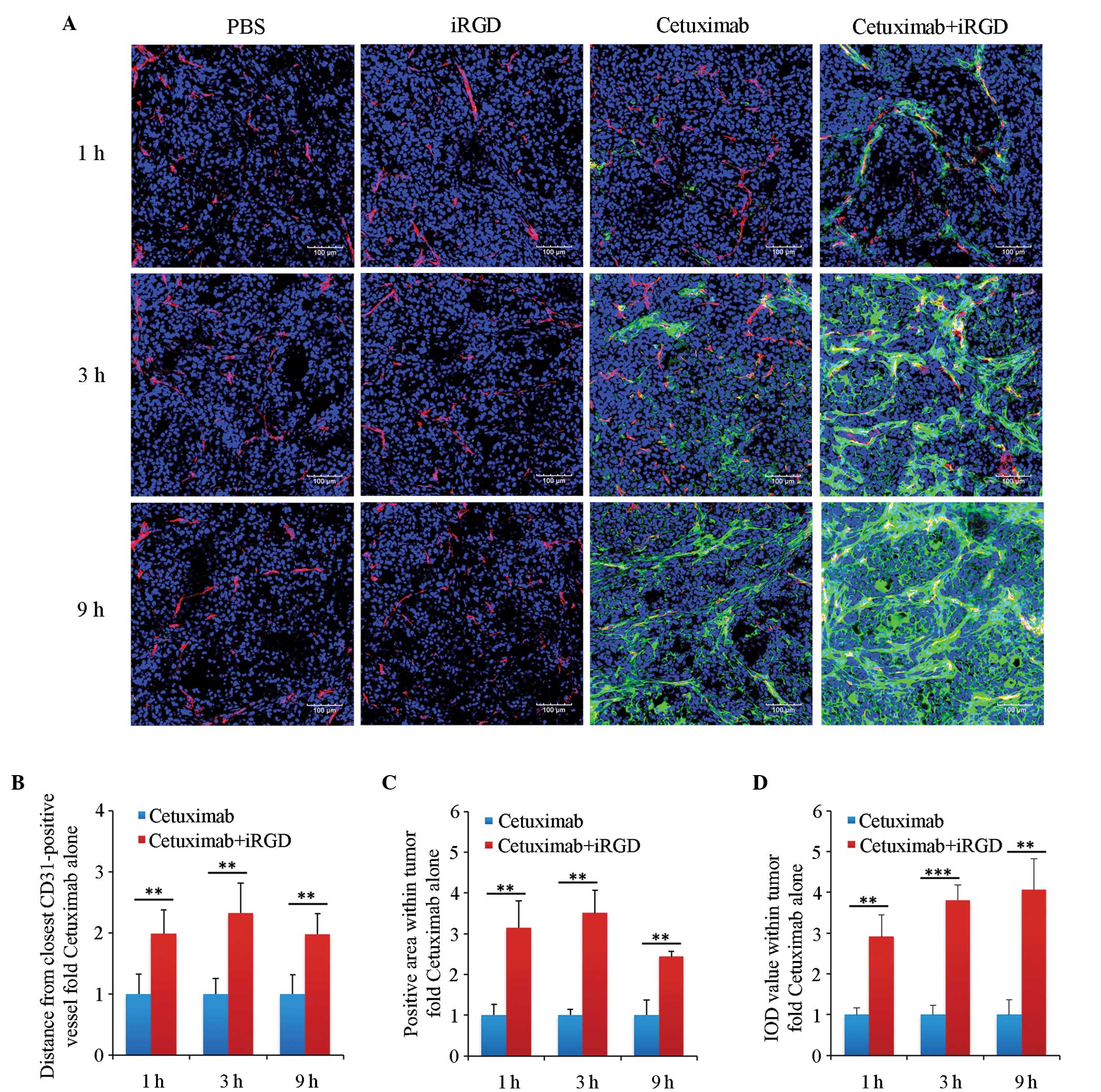
Tumor-penetrating ability of cetuximab
combined with iRGD
To determine whether iRGD can promote the
penetration of cetuximab into the human NSCLC xenograft, cetuximab
that penetrated into the tumor tissue was detected by
immunofluorescence staining. As shown in Fig. 2A, much more cetuximab could be
observed in the cetuximab+iRGD group compared with in the cetuximab
group, particularly after 3 and 9 h (Fig.
2A). The results of the quantitative analysis showed that the
penetrating depths of cetuximab into the tumors in the
cetuximab+iRGD group were 2.0, 2.3 and 2.0 times the cetuximab only
group; that the diffusing areas were 3.2, 3.5 and 2.4 times the
cetuximab only group; and the accumulated amounts were 2.9, 3.8 and
4.1 times the cetuximab only group at 1, 3 and 9 h of treatment,
respectively (Fig. 2B). These
differences were statistically significant.
Therapeutic efficacy of cetuximab
co-administered with iRGD
In order to determine an appropriate dose, at which
cetuximab efficiently inhibits tumor growth without evident side
effects, 3 doses of cetuximab (10, 30 and 90 mg/kg) were applied to
treat 3 groups of mice (n=3) via tail vain, twice per week for two
consecutive weeks. After two weeks, the mice in that 10 and 30
mg/kg groups appeared normal, but the mice in the 90 mg/kg group
showed an apparent lack of energy and loss of appetite. According
to a previous study, the A549 xenograft in mice is sensitive to
cetuximab at doses of 4 mg/kg and 40 mg/kg (22). Taking the efficacy and side effects
into consideration, the present study chose 30 mg/kg as the dose of
cetuximab in the in vivo therapeutic efficacy
experiments.
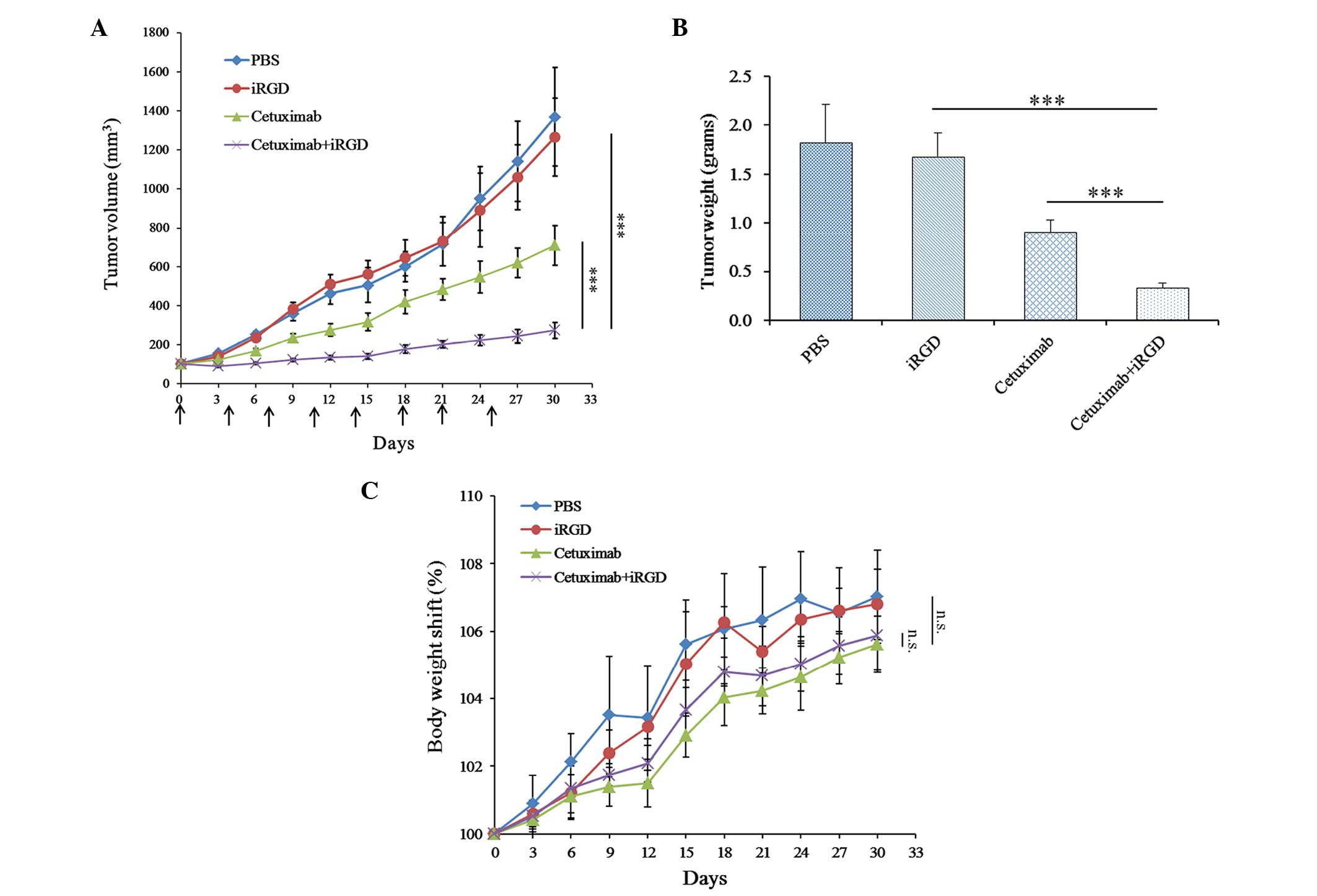
To determine whether the therapeutic efficacy of
cetuximab is enhanced when it is co-administered with iRGD,
cetuximab and iRGD were co-administered to treat the mice with A549
xenografts. As shown in Fig. 3A, the
tumors of the cetuximab+iRGD group grew more slowly compared with
the tumors in the cetuximab group, and this difference was
statistically significant. The analysis of average tumor weight
further confirmed this result (Fig.
3B). These results demonstrated that iRGD could enhance the
therapeutic efficacy of cetuximab for A549 xenografts in mice. The
body weight shift analysis of the experimental mice showed that no
significant difference was observed between the cetuximab group and
the cetuximab+iRGD group (Fig. 3C).
These results demonstrated that iRGD did not evidently exacerbate
the side effects of cetuximab.
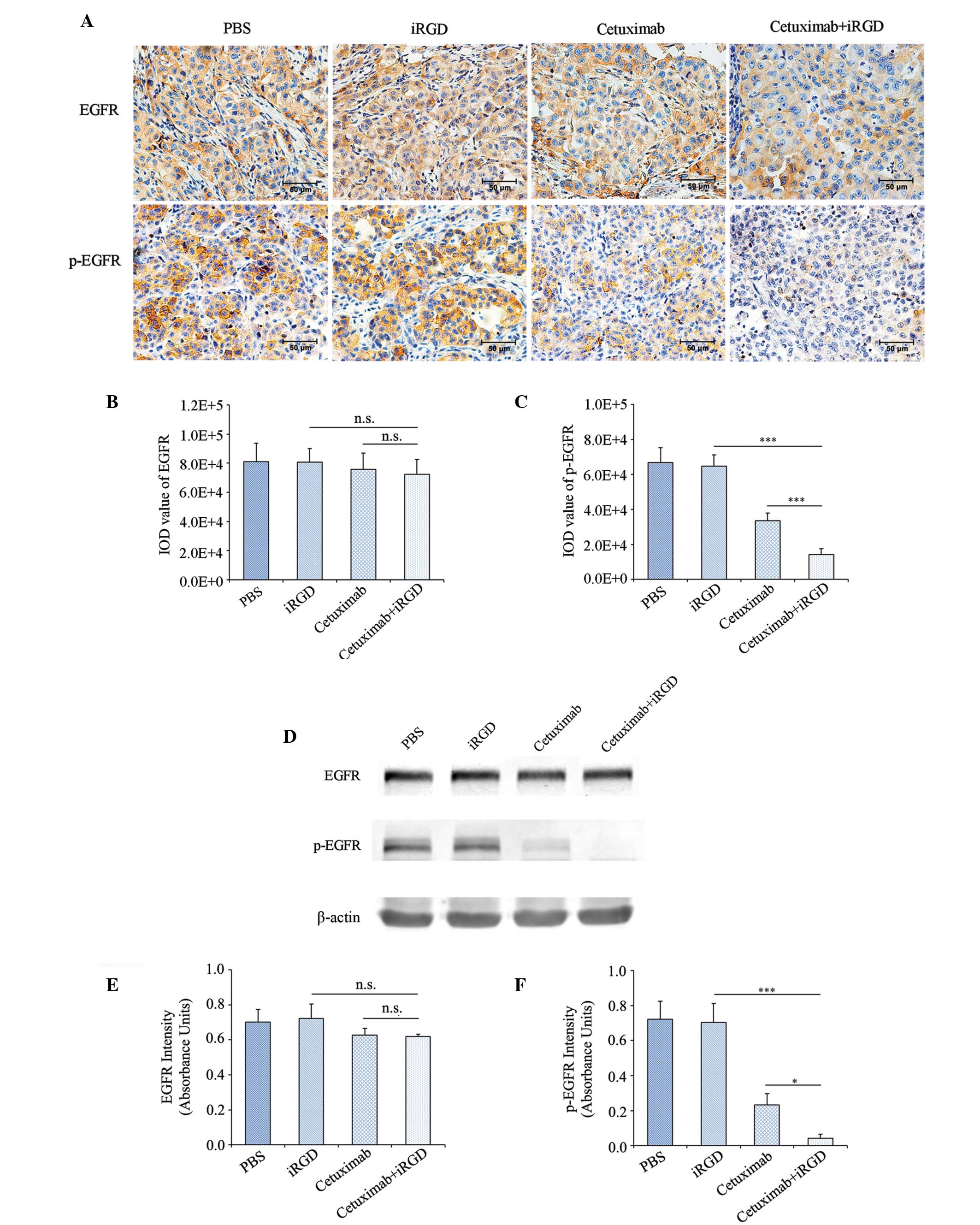
EGFR phosphorylation in the tumors
treated with cetuximab plus iRGD
With regards to the aforementioned results, iRGD
promoted the penetration of cetuximab into tumor tissue and
enhanced the therapeutic efficacy of cetuximab for the A549
xenograft. Therefore, theoretically, the co-administration of
cetuximab and iRGD could result in the increased inhibition of EGFR
phosphorylation compared with cetuximab monotherapy. In order to
confirm this speculation, the present study first detected the
phosphorylation level of EGFR in the tumor tissues by
immunohistochemical staining. The expression levels of EGFR among
the 4 groups had no significant difference (Fig. 4A and B); however, the phosphorylation
of EGFR in the cetuximab+iRGD group was reduced by 57.1% compared
with the cetuximab group, which was statistically significant
(Fig. 4A and C).
To further confirm the expression level of EGFR and
p-EGFR, the total proteins were extracted from the tumor tissues in
each group. The expression levels of EGFR and p-EGFR were detected
by western blot analysis with β-actin as an internal control. Each
strip was scanned and a quantitative analysis was performed with
ImageJ software. The expression level of EGFR in the tumor tissues
of the 4 groups had no significant difference (Fig. 4D and E); however, the expression level
of p-EGFR in the cetuximab+iRGD group was reduced by 82.6% compared
with the cetuximab group (Fig. 4D and
F). Overall, these results confirmed that the therapeutic
efficacy of cetuximab was enhanced when used in combination with
the tumor-penetrating peptide iRGD.
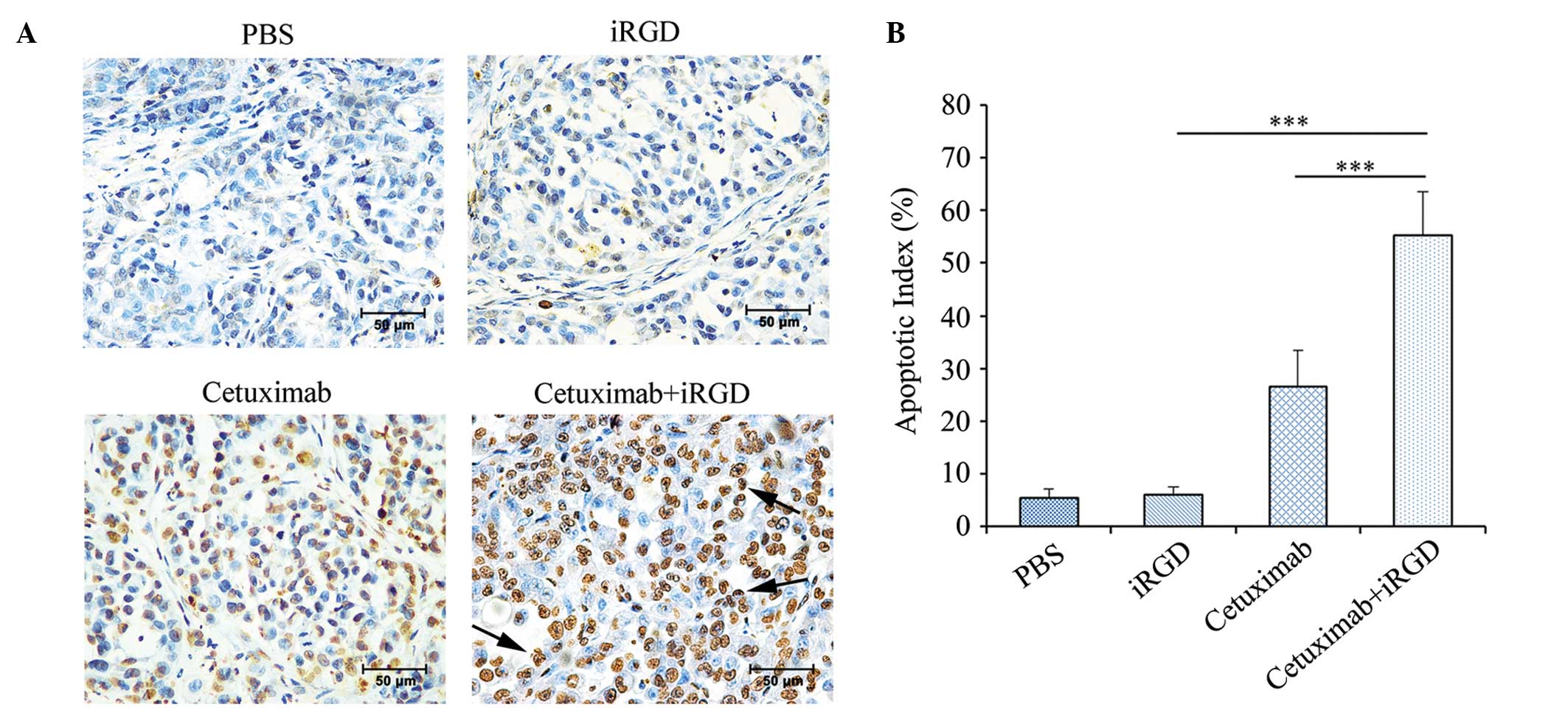
Induction of apoptosis in the tumors
treated with cetuximab plus iRGD
Previous studies have shown that cetuximab can
induce cancer cell apoptosis by competitively blocking the binding
of EGFR to its natural ligands (9,23).
Therefore, the present study detected the apoptosis of the cancer
cells in the mice treated with A549 xenografts using a TUNEL assay.
As shown in Fig. 5A, more apoptotic
cells were visible in tumors of the cetuximab+iRGD group compared
with tumors of the cetuximab group. The apoptotic index was defined
as the percentage of TUNEL-positive cells vs. the total number of
cells. According to the statistical analysis shown in Fig. 5B, the rate of apoptosis in tumors of
the cetuximab+iRGD group was 2.1 times the apoptosis rate in tumors
of the cetuximab group. These results further confirmed that iRGD
enhanced the therapeutic efficacy of cetuximab in the human NSCLC
xenograft.
Discussion
The present study was conducted to evaluate the use
of iRGD for co-administration therapy with cetuximab, and
demonstrated that iRGD boosted the accumulation of cetuximab in
human NSCLC xenograft models established with the A549 cell line.
The anticancer effects of cetuximab were also enhanced by iRGD
co-administration in this NSCLC model. To further verify the
effects of drug accumulation and anticancer, the phosphorylation of
EGFR and cell apoptosis were detected in the treated tumors.
The experiments using A549 xenograft models
confirmed the enhanced cetuximab accumulation effect and
therapeutic efficacy of iRGD. Previous reports demonstrated that
the drug accumulation effect of iRGD is dependent on the level of
ανβ3, ανβ5 and NRP-1 in the tumor tissue (14,18,24). The
results of the present study showed that these molecules are
overexpressed in A549 cells and in the xenograft tissue.
Furthermore, cetuximab accumulation was detected in tumor tissues.
The results showed that the accumulation of cetuximab in tumor
tissue is enhanced by iRGD. Theoretically, the enhanced
accumulation of cetuximab in tumor tissues could result in
decreased EGFR phosphorylation, increased cell apoptosis and
inhibited tumor growth. The results of the current study were
consistent with these theoretical speculations. Therefore, the
results confirmed that iRGD can enhance the tumor-penetration and
therapeutic efficacy of cetuximab in A549 xenograft models.
It is possible that combination with iRGD enhances
the therapeutic efficacy and decreases the side effects of
cetuximab. The results of a single-agent, phase II study in
recurrent NSCLC (n=29) showed limited therapeutic efficacy; 7% of
patients showed a partial response and 17% patients showed stable
disease (8). In one phase III trial,
cetuximab was evaluated in combination with docetaxel and
pemetrexed in patients with advanced NSCLC, and the results
indicated that cetuximab does not add any benefit to second line
chemotherapy for patients with NSCLC (25,26). The
BMS099 trial also failed to show a significant improvement in
progression-free survival (5). In the
present study, iRGD was combined with cetuximab to treat an NSCLC
xenograft model, and the results indicated that iRGD can enhance
the therapeutic efficacy of cetuximab for NSCLC without evident
side effects at dose of 30 mg/kg. Therefore, it is possible that
iRGD may add benefit to cetuximab for patients with NSCLC. However,
the efficacy of iRGD has only been examined in the A549 cell line,
so the clinical applications of these findings require careful
consideration.
The use of cetuximab and iRGD combination therapy
may have certain problems if it is applied clinically. The current
understanding of the mechanism by which iRGD enhances the
therapeutic efficacy of cetuximab for NSCLC is limited. Although no
evident side effects were observed in the present study, the safety
of this combination therapy requires additional evaluation. The
CendR motif of iRGD may also be used by viruses and microbial
toxins in order to gain entry into cells and spread within the
tissues of the body (27–29). Since EGFR is also overexpressed in
novel vessels, iRGD also may promote the uptake of cetuximab into
normal tissues that are damaged, and the tissue repair that follows
may interfere with the normal function of EGFR and cause further
damage to the body.
In summary, through a human NSCLC A549 nude mouse
xenograft model, iRGD was confirmed to promote the penetration of
cetuximab into tumor tissue and therefore enhance the therapeutic
efficacy of cetuximab in vivo. The combined application of
cetuximab and iRGD may be a novel strategy to enhance the clinical
therapeutic efficacy of cetuximab for the treatment of NSCLC.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (Beijing, China; grant no.
81301946), Natural Science Foundation of Jiangsu Province (Nanjing,
China; grant no. BK2012146), Jiangsu Provincial Office of Education
Foundation (Nanjing, China; grant no. JHB2012-34), Xuzhou Medical
College Foundation (Xuzhou, China; grant no. 2012KJZ23) and ‘Liu Da
Ren Cai Gao Feng’ Foundation of Jiangsu Province (Nanjing, China;
grant no. 53031305).
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small cell lung cancer
|
|
iRGD
|
internalizing RGD peptide
|
|
EGFR
|
epidermal growth factor receptor
|
|
p-EGFR
|
phosphorylated EGFR
|
|
CendR
|
cryptic C-end Rule
|
|
NRP-1
|
neuropilin-1
|
|
TUNEL
|
TdT-mediated dUTP nick end labeling
kit
|
References
|
1
|
Privitera G, Luca T, Musso N, Vancheri C,
Crimi N, Barresi V, Condorelli D and Castorina S: In vitro
antiproliferative effect of trastuzumab (Herceptin®)
combined with cetuximab (Erbitux®) in a model of human
non-small cell lung cancer expressing EGFR and HER2. Clin Exp Med.
2015.PubMed/NCBI
|
|
2
|
Patil N, Abba M and Allgayer H: Cetuximab
and biomarkers in non-small-cell lung carcinoma. Biologics.
6:221–231. 2012.PubMed/NCBI
|
|
3
|
Pujol JL, Pirker R, Lynch TJ, Butts CA,
Rosell R, Shepherd FA, Vansteenkiste J, O'Byrne KJ, de Blas B,
Heighway J, et al: Meta-analysis of individual patient data from
randomized trials of chemotherapy plus cetuximab as first-line
treatment for advanced non-small cell lung cancer. Lung Cancer.
83:211–218. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim SM, Kim JS, Kim JH, Yun CO, Kim EM,
Kim HK, Solca F, Choi SY and Cho BC: Acquired resistance to
cetuximab is mediated by increased PTEN instability and leads
cross-resistance to gefitinib in HCC827 NSCLC cells. Cancer Lett.
296:150–159. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pirker R, Pereira JR, von Pawel J,
Krzakowski M, Ramlau R, Park K, de Marinis F, Eberhardt WE,
Paz-Ares L, Störkel S, et al: EGFR expression as a predictor of
survival for first-line chemotherapy plus cetuximab in patients
with advanced non-small-cell lung cancer: Analysis of data from the
phase 3 FLEX study. Lancet Oncol. 13:33–42. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Douillard JY, Pirker R, O'Byrne KJ, Kerr
KM, Störkel S, von Heydebreck A, Grote HJ, Celik I and Shepherd FA:
Relationship between EGFR expression, EGFR mutation status and the
efficacy of chemotherapy plus cetuximab in FLEX study patients with
advanced non-small-cell lung cancer. J Thorac Oncol. 9:717–724.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
van den Heuvel MM, Uyterlinde W, Vincent
AD, de Jong J, Aerts J, Koppe F, Knegjens J, Codrington H, Kunst
PW, Dieleman E, et al: Additional weekly Cetuximab to concurrent
chemoradiotherapy in locally advanced non-small cell lung
carcinoma: Efficacy and safety outcomes of a randomized,
multi-center phase II study investigating. Radiother Oncol.
110:126–131. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dubey S and Schiller JH: Three emerging
new drugs for NSCLC: Pemetrexed, bortezomib and cetuximab.
Oncologist. 10:282–291. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wild R, Fager K, Flefleh C, Kan D, Inigo
I, Castaneda S, Luo FR, Camuso A, McGlinchey K and Rose WC:
Cetuximab preclinical antitumor activity (monotherapy and
combination based) is not predicted by relative total or activated
epidermal growth factor receptor tumor expression levels. Mol
Cancer Ther. 5:104–113. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yu T, Wang Z, Liu K, Wu Y, Fan J, Chen J,
Li C, Zhu G and Li L: High interstitial fluid pressure promotes
tumor progression through inducing lymphatic metastasis-related
protein expressions in oral squamous cell carcinoma. Clin Transl
Oncol. 16:539–547. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Milosevic MF, Pintilie M, Hedley DW,
Bristow RG, Wouters BG, Oza AM, Laframboise S, Hill RP and Fyles
AW: High tumor interstitial fluid pressure identifies cervical
cancer patients with improved survival from radiotherapy plus
cisplatin versus radiotherapy alone. Int J Cancer. 135:1692–1699.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Trédan O, Galmarini CM, Patel K and
Tannock IF: Drug resistance and the solid tumor microenvironment. J
Natl Cancer Inst. 99:1441–1454. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Song W, Li M, Tang Z, Li Q, Yang Y, Liu H,
Duan T, Hong H and Chen X: Methoxypoly (ethylene glycol)-block-poly
(L-glutamic acid)-loaded cisplatin and a combination with iRGD for
the treatment of non-small-cell lung cancers. Macromol Biosci.
12:1514–1523. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sugahara KN, Teesalu T, Karmali PP,
Kotamraju VR, Agemy L, Girard OM, Hanahan D, Mattrey RF and
Ruoslahti E: Tissue-penetrating delivery of compounds and
nanoparticles into tumors. Cancer Cell. 16:510–520. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Su S, Wang H, Liu X, Wu Y and Nie G:
iRGD-coupled responsive fluorescent nanogel for targeted drug
delivery. Biomaterials. 34:3523–3533. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Alberici L, Roth L, Sugahara KN, Agemy L,
Kotamraju VR, Teesalu T, Bordignon C, Traversari C, Rizzardi GP and
Ruoslahti E: De novo design of a tumor-penetrating peptide. Cancer
Res. 73:804–812. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Roth L, Agemy L, Kotamraju VR, Braun G,
Teesalu T, Sugahara KN, Hamzah J and Ruoslahti E: Transtumoral
targeting enabled by a novel neuropilin-binding peptide. Oncogene.
31:3754–3763. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sugahara KN, Teesalu T, Karmali PP,
Kotamraju VR, Agemy L, Greenwald DR and Ruoslahti E:
Coadministration of a tumor-penetrating peptide enhances the
efficacy of cancer drugs. Science. 328:1031–1035. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang Q, Liu X, Xu S, Li C, Zhang Y, Yang
J and Zheng J: Factor VII light chain-targeted lidamycin shows
intensified therapeutic efficacy for liver cancer. Cancer Biother
Radiopharm. 27:384–391. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Aizawa K, Liu C, Veeramachaneni S, Hu KQ,
Smith DE and Wang XD: Development of ferret as a human lung cancer
model by injecting
4-(Nmethyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone (NNK). Lung
Cancer. 82:390–396. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ning L, Li X, Ding X, Yin Y and Li G: An
iRGD based strategy to study electrochemically the species inside a
cell. Int J Mol Sci. 13:10424–10431. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Steiner P, Joynes C, Bassi R, Wang S,
Tonra JR, Hadari YR and Hicklin DJ: Tumor growth inhibition with
cetuximab and chemotherapy in non-small cell lung cancer xenografts
expressing wild-type and mutated epidermal growth factor receptor.
Clin Cancer Res. 13:1540–1551. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu F, Tian Y, Huang Y, Zhang LL, Guo ZZ,
Huang JJ and Lin TY: EGFR inhibitors sensitize non-small cell lung
cancer cells to TRAIL-induced apoptosis. Chin J Cancer. 30:701–711.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Akashi Y, Oda T, Ohara Y, Miyamoto R,
Kurokawa T, Hashimoto S, Enomoto T, Yamada K, Satake M and Ohkohchi
N: Anticancer effects of gemcitabine are enhanced by
co-administered iRGD peptide in murine pancreatic cancer models
that overexpressed neuropilin-1. Br J Cancer. 110:1481–1487. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Villanueva MT: Lung cancer: Cetuximab,
you're fired. Nat Rev Clin Oncol. 11:32014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rasul KI and Kerr DJ: Targeted therapies:
Cetuximab plus chemotherapy in patients with advanced NSCLC. Nat
Rev Clin Oncol. 6:499–500. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sanchez AJ, Vincent MJ, Erickson BR and
Nichol ST: Crimean-congo hemorrhagic fever virus glycoprotein
precursor is cleaved by Furin-like and SKI-1 proteases to generate
a novel 38-kilodalton glycoprotein. J Virol. 80:514–525. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wool-Lewis RJ and Bates P: Endoproteolytic
processing of the ebola virus envelope glycoprotein: Cleavage is
not required for function. J Virol. 73:1419–1426. 1999.PubMed/NCBI
|
|
29
|
Sjöberg M, Wallin M, Lindqvist B and
Garoff H: Furin cleavage potentiates the membrane
fusion-controlling intersubunit disulfide bond isomerization
activity of leukemia virus Env. J Virol. 80:5540–5551. 2006.
View Article : Google Scholar : PubMed/NCBI
|