Background
Epithelial ovarian cancer is the most lethal
gynecological malignancy worldwide, with a 5-year survival rate of
<30%. Over 75% of affected women succumb to the disease
following combined first line treatment (consisting of surgery and
chemotherapy) (1).
Of all the histotypes of ovarian cancer, the most
frequent diagnosis in developed countries is high-grade serous
carcinoma (2,3), typically characterized by ubiquitous
presence of a mutation in the tumor suppressor p53 and, less
frequently, by an association with breast cancer (BRCA)1 and BRCA2
mutations (germline mutations in 13–16%; somatic mutations in ~6%
of cases) (4,5). Assuming that cancer survival is an
indicator of healthcare performance, the lethality of epithelial
ovarian cancer (EOC) may be due the common misconceptions regarding
etiology and the absence of effective screening and early
diagnostic tools (5).
Contrasting with cervical cancer, in which
preventive measures and early diagnosis of precancerous lesions has
demonstrated to be cost-effective and effective at improving cancer
mortality rates (6,7), the current management of EOC remains
poor and has been based on existing methods that are directed
against established types of cancer, rather than investigating the
mechanisms by which EOC develops (8).
Over the previous two decades, proposed EOC
screening tools have failed to demonstrate a survival benefit, most
likely due to the poor anatomical accessibility of the adnexa,
which therefore permits only indirect approaches, including
ultrasound evaluation (affected by inter-/intra-operator
variability) and serum markers assay (affected by low specificity
in precancerous and early lesion detection) (1).
Despite advances in our understanding of the
pathogenesis of EOC (8–11), the gap between actual and optimal care
in patients at increased risk for EOC emphasizes the urgent
requirement for identification of a valid screening/early
diagnostic strategy. With the aim of collaborating with worldwide
scientists and clinicians involved in the search for a novel
strategy for the screening and early diagnosis of EOC, following a
short and updated summary of the evidence regarding the recent
advances and proposals in the field of EOC treatment, the present
study proposes an innovative tool to perform screening/early
diagnosis in patients at an increased risk of EOC development.
Literature review and analysis of
evidence
Summary of novel evidence concerning the
pathogenesis of EOC. Currently, the incessant ovulation hypothesis
has been almost completely disregarded as an underlying causative
mechanism of EOC, as it appears inconsistent with the observation
that patients affected by polycystic ovarian syndrome, who
demonstrate a decreased number of ovulatory cycles, appear to
exhibit an increased risk for the development of ovarian cancer
(12). A proposed and accepted
paradigm for the development of EOC is the dualistic model, which
groups the various types of epithelial ovarian cancer into two
broad categories, designated as type I and II (8,13,14).
Type I EOC is comprised of low-grade serous,
low-grade endometrioid, mucinous and clear cell carcinomas
(15). In general, these tumors are
large cystic masses confined to one ovary with a relatively
indolent course, and are associated with mutations in Kirsten rat
sarcoma viral oncogene homolog, BRAF, phosphatase and tensin
homolog, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic
subunit, catenin (cadherin-associated protein) β 1, AT rich
interactive domain 1A and protein phosphatase 2 regulatory subunit
A α, which perturb signaling pathways (15). These molecular alterations govern the
phenotypic expression of a series of transformation events, leading
to a stepwise progression from benign, through varying degrees of
atypia (borderline tumor), to noninvasive and subsequently invasive
low-grade carcinoma (15). Type II
tumors are comprised of high-grade serous, high-grade endometrioid,
undifferentiated carcinomas and malignant-mixed mesodermal tumors
(15). These tumors are biologically
aggressive and present at an advanced stage, which contributes to
the high rate of mortality (15).
Reviews of histopathological surveys performed on
the resected fallopian tubes of BRCA mutation carriers, who
underwent risk-reducing salpingo-oophorectomy, unexpectedly
revealed the presence of occult carcinomas of the fallopian tubes
(a tissue previously thought to rarely exhibit malignancy). This
finding prompted studies which demonstrated the most accredited
theory of type II EOC development, which suggests that a large
portion of these tumors are derived from the fallopian tube
(9).
Summary of the recent evidence concerning EOC
screening and early diagnosis. Women aged >40 years or with a
family history of breast and ovarian cancer are commonly considered
at the highest risk for development of EOC, and ideally they would
be regularly screened for EOC using biomarkers able to detect the
disease in the early stages (16).
Despite the substantial efforts put forth by the
scientific community and the numerous proposals for non-invasive
EOC screening tools and biomarkers [ranging from International
Ovarian Tumor Analysis (IOTA) score assessment by highly skilled
sonographers, and the exhaled breath samples test] (17,18), there
are currently no known biomarkers or sonographic/radiological
approaches that appear sensitive or specific enough to be used as a
cost-effective tool for early-stage EOC screening and
diagnosis.
Following a systematic review of the literature, it
was identified that only a single manuscript proposed a novel
approach for the screening/early diagnosis of EOC; this study had a
positive rationale as the authors focused the proposal and pilot
study on the ‘brush cytology of the fallopian tube’ (19). Lum et al (19) proposed cytological sampling of the
fallopian tube [analogous to the Papanicolaou test (7) for the uterine cervix] to collect
endoluminal cells, allowing for discrimination between negative
samples and those containing cells suggestive of serous tubal
intraepithelial carcinoma, which may be the initial precursor of
type II EOC. In the opinion of the authors of the present study,
despite the fact that this protocol was unique in its rationale, it
may comprehensibly considered only a theoretical proposal due to
the presence of several important biases responsible for yielding
disappointing results, as well as poor feasibility and
reproducibility in a large scale population. The small number of
patients (n=10) on which the procedures were performed in addition
to the inappropriate eligibility criteria for patient selection
made the pilot study useful only for the technical validation of
procedure feasibility (all specimens had satisfactory cellularity
for interpretation without any complications linked to the
procedure), as all cases were interpreted as benign in
morphological and immunohistochemical investigations (19). Furthermore, the study failed to
demonstrate procedure feasibility due to the erroneous choice of
the cervical cytobrush for tubal cytological sampling, which
affected the study protocol for at least 3 reasons: i) The diameter
and slight flexibility of the cytobrush device does not allow
cytological sampling in the infundibulum and fimbriae (in which
precursor cells of EOC frequently originate); ii) the mechanical
trauma caused by the brush may adversely affect the subsequent
histopathological analysis of the tubal epithelium, particularly in
situations where the tumor is intraepithelial and the aggregates of
the atypical cells are few; and iii) intra-tubal traumatic sampling
may irreversibly damage the fallopian tube epithelium, causing a
negative impact on functioning (physiologically defined as the
ability to convey the products of conception to the uterus). These
facts represent a significant problem as the aim of screening is
based on maintaining tubal function in patients who have not yet
completed their reproductive program (otherwise these patients
would be candidates for prophylactic salpingectomy).
As frequently occurs during pioneering research, the
analysis of biases affecting previous studies represents a good
starting point for the improvement of subsequent protocols.
Beginning from the innovative and intuitive study by Lum et
al (19), the present study
protocol is proposed, with the aim of validating the rationale,
usefulness and feasibility of a non-invasive outpatient
hysteroscopic approach (known as ‘Tuba-check’) in the assessment of
tubal lumen cell abnormalities. This strategy may potentially be
eligible as a screening/early diagnostic tool in patients at
increased risk of EOC development.
Study proposal
In order to simplify the experimental model aimed at
evaluating the feasibility, accuracy, reproducibility and
cost-effectiveness of the proposed novel tool for the screening and
early diagnosis of EOC, the presently described protocol
intentionally focuses attention on the cohort of patients with BRCA
mutations or with a ‘BRCA-ness profile’ who have been admitted in
order to undergo risk-reducing salpingo-oophorectomy due to an
increased risk for EOC development (20). The justification for this choice is
based on the specific molecular, pathological and clinical features
of EOC detected in this cohort of women, as well as the
considerable number of prophylactic salpingo-oophorectomies
performed with the aim of reducing the risk of EOC development.
The proposed study plans to recruit 100 women with
known BRCA1/2 mutations or with a ‘BRCA-ness profile’, aged 25–75
years and spontaneously adhering to the study protocol following
adequate counseling performed in accordance with Italian privacy
laws.
Patients will be divided into 2 study groups:
Patients aged 35 and older requiring risk-reducing prophylactic
salpingo-oophorectomy will be allocated to group A, whereas those
aged <35 years who choose not to proceed with risk-reducing
prophylactic salpingo-oophorectomy for personal choice or because
they have not yet completed their reproductive lifespan, will be
allocated to group B. In addition, 100 women aged between 25–75
years, with no suspicion of BRCA1/2 mutations or ‘BRCA-ness
profile’ will be recruited, and will be divided into group C (in
the event of salpingo-oophorectomy, during hysterectomy performed
for gynecological indications different from adnexal disease) and
group D (if salpingo-oophorectomy will not performed).
Patients with a history of any neoplasia, hormonal
adjuvant/replacement treatment (including selective estrogen
receptor modulators or postmenopausal replacement therapy), adnexal
surgery (including treatment for endometriosis, ectopic pregnancy
and tubal ligation), absent tubal patency, Müllerian abnormalities,
previous cervical surgery (cervical cone or multiple loop excisions
and trachelectomy) (21,22) or abnormalities in psychological status
will be excluded from the study.
At recruitment, all patients will undergo a
gynecological physical examination and pelvic ultrasound scan. In
the event of detection of an adnexal mass, adequate
characterization will be performed in accordance with IOTA logistic
regression 2 recommendations (23).
Furthermore, all patients will undergo cancer
antigen 125 (CA125) and human epididymis secretory protein 4 (He4)
serum blood sampling with risk of ovarian malignancy algorithm
calculation according to hormonal status.
Hysteroscopy using a Bettocchi® 4.9 mm
Integrated Office hysteroscope (Bettocchi Office Hysteroscopes;
Karl Storz GmbH and Co. KG, Tuttlingen, Germany), and uterine
cavity distension using normal saline solution with an intrauterine
pressure set at approximately 35 mmHg (the balance of an irrigation
flow of approximately 200 ml/min and a vacuum of 0.2 bars), will be
performed in all eligible women aged 25–75 years old (during the
mild follicular phase of the menstrual cycle in the case of
premenopausal women).
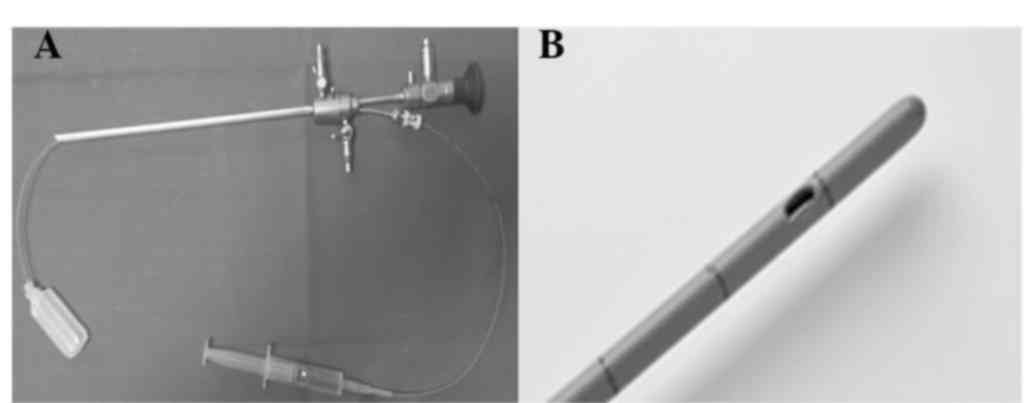
During the hysteroscopic investigation an atraumatic
4 French sterile ureteric drainage catheter (ColoplastA/S,
Humlebaek, Denmark) complete with a cylindrical metal stylet will
be introduced through the 4 French sterile ureteric drainage
catheter (Fig. 1).
At least 8 cm of the distal portion of the graduated
catheter will be introduced into the fallopian tube lumen (with the
aim of reaching the fimbriated extremity); the cylindrical metal
stylet will subsequently be removed and following instillation of 5
cc 9% Na/Cl saline sterile solution, the washing fluid containing
the end-luminal cells will be aspirated during catheter retraction.
The procedure will be performed bilaterally and the washing fluid
from the two fallopian tubes will be sent separately, in sterile
tubes, to the cytology department.
Patients in groups A and group C will undergo
hysteroscopic tubal washing and aspiration under direct
visualization through the umbilical laparoscopic port (necessary
for subsequent bilateral laparoscopic adnexectomy). The procedure
will therefore be performed under general anesthesia. By contrast,
patients admitted to group B and group D will undergo the procedure
in an outpatient setting, with routine hysteroscopic tubal
sterilization via Essure® (Bayer AG, Leverkusen,
Germany) (24).
For all patients, it is planned to collect data
concerning general epidemiological features (age, body mass index,
ethnicity), family history of breast and ovarian cancer,
oral/intrauterine contraceptive use (type and duration),
obstetrical history (parity, previous hormonal treatment for
infertility care), presence of comorbidities and associated chronic
therapy, as well as any previous history of medically treated
pelvic inflammatory disease.
Only for patients in group B and group D (outpatient
setting) will data regarding perceived pain during the
hysteroscopic procedure be collected, through a numeric rating
scale self-administered score (prior to and following the
procedure), and patient satisfaction at the end of procedure will
be assessed through a visual analogue scale with a value ranging
from 0 (no satisfaction) to 10 (complete satisfaction).
For all patients data on the following will also be
collected: Procedure failure due to technical difficulties, number
of non-diagnostic samples due to poor cellularity, number of
intraoperative complications, including bleeding or tubal
perforation, and number of postoperative complications, including
refractory pelvic pain or fever.
Additionally, data regarding preoperative ultrasound
investigation and CA125/He4 serum assays will be collected.
Finally, it is planned to collect information in cases in which
cytological anomalies are detected and, exclusively for patients in
group A and group C, data regarding histological examination of the
removed adnexa.
Study aims
The primary aim of the discussed study protocol is
to compare patients in group A and group C with those included in
group B and group D, in terms of perioperative pain, patient
satisfaction and complication rate in order to validate the safety
and technical feasibility of the procedure in an outpatient
setting.
The groups will also be compared in terms of
cellularity of the collected washing fluid, and whether this fluid
is sufficient to allow cytological diagnosis in order to validate
the potential applicability and rationale of the proposed
procedure.
The secondary aim of the discussed protocol is to
correlate the cytological investigation results from group A and
group C with definitive histology in order to validate the accuracy
of cytological tubal washing in the detection or exclusion of cases
with or without cellular abnormalities.
The tertiary aim of the discussed protocol is to
correlate preoperative epidemiological characteristics, ultrasound
features and serum biomarker values with cytological and
histological (when performed) diagnoses in order to identify
associations, if these exist.
Expected results and conclusions
As current evidence demonstrates that no diagnostic
tools or screening programs are effective or cost-effective at
improving the outcome of EOC, it is therefore imperative that the
scientific community unite its efforts in the search of a valid
screening and/or early diagnostic method for the treatment of this
lethal gynecological malignancy.
Scientific literature continues to validate
hysteroscopy as a safe routine diagnostic procedure characterized
by a short learning curve for a tubal approach (as in female
sterilization), since upon performing <50 procedures under tutor
support, generally clinicians acquire the skills required to
perform the procedure independently (24). It is therefore possible that the
hysteroscopy approach to the fallopian tube may be considered to be
the most simple, minimally-invasive and large scale reproducible
tool available. Technical difficulties are expected to arise with
the protocol discussed in this paper, however a close collaboration
with biomedical engineers should allow potential obstacles to be
overcome. For the above-mentioned reasons, the validation of
technical feasibility has been set as the primary endpoint of the
presently discussed study protocol, and determination of the
accuracy in predicting cell abnormalities has been set as the
secondary endpoint.
If the data collected by the currently summarized
study protocol will validate this approach, it is likely that in
the near future the ‘Tuba-check’ can be improved and made available
to the entire female population for the treatment of EOC, therefore
reducing the number of mortalities.
References
|
1
|
Coleman MP, Forman D, Bryant H, Butler J,
Rachet B, Maringe C, Nur U, Tracey E, Coory M, Hatcher J, et al:
ICBP Module 1 Working Group: Cancer survival in Australia, Canada,
Denmark, Norway, Sweden, and the UK, 1995–2007 (the International
Cancer Benchmarking Partnership): An analysis of population-based
cancer registry data. Lancet. 377:127–138. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
George SH and Shaw P: BRCA and early
events in the development of serous ovarian cancer. Front Oncol.
4:52014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kuhn E, Kurman RJ, Vang R, Sehdev AS, Han
G, Soslow R, Wang TL and Shih IeM: TP53 mutations in serous tubal
intraepithelial carcinoma and concurrent pelvic high-grade serous
carcinoma - evidence supporting the clonal relationship of the two
lesions. J Pathol. 226:421–426. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cancer Genome Atlas Research Network, .
Integrated genomic analyses of ovarian carcinoma. Nature.
474:609–615. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gizzo S, Noventa M and Nardelli GB:
Gardasil administration to hr-HPV-positive women and their
partners. Trends Pharmacol Sci. 34:479–480. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Saccardi C, Gizzo S, Noventa M, Anis O, Di
Gangi S, Patrelli TS, D'Antona D and Nardelli GB: High risk human
papillomavirus DNA test: Could it be useful in low-grade cervical
lesion triage? Five-year follow-up. Reprod Sci. 21:198–203. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kurman RJ: Origin and molecular
pathogenesis of ovarian high-grade serous carcinoma. Ann Oncol.
24:(Suppl 10). x16–x21. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Erickson BK, Conner MG and Landen CN Jr:
The role of the fallopian tube in the origin of ovarian cancer. Am
J Obstet Gynecol. 209:409–414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Koshiyama M, Matsumura N and Konishi I:
Recent concepts of ovarian carcinogenesis: Type I and type II.
Biomed Res Int. 2014:9342612014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li J, Abushahin N, Pang S, Xiang L,
Chambers SK, Fadare O, Kong B and Zheng W: Tubal origin of
‘ovarian’ low-grade serous carcinoma. Mod Pathol. 24:1488–1499.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schildkraut JM, Schwingl PJ, Bastos E,
Evanoff A and Hughes C: Epithelial ovarian cancer risk among women
with polycystic ovary syndrome. Obstet Gynecol. 88:554–559. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shih IeM and Kurman RJ: Ovarian
tumorigenesis: A proposed model based on morphological and
molecular genetic analysis. Am J Pathol. 164:1511–1518. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kurman RJ and Shih IeM: Molecular
pathogenesis and extraovarian origin of epithelial ovarian cancer -
shifting the paradigm. Hum Pathol. 42:918–931. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gizzo S, Berretta R, Di Gangi S, Guido M,
Zanni GC, Franceschetti I, Quaranta M, Plebani M, Nardelli GB and
Patrelli TS: Borderline ovarian tumors and diagnostic dilemma of
intraoperative diagnosis: Could preoperative He4 assay and ROMA
score assessment increase the frozen section accuracy? A
multicenter case-control study. Biomed Res Int. 2014:8035982014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lawrenson K, MhawechFauceglia P,
Worthington J, Spindler TJ, O'Brien D, Lee JM, Spain G, Sharifian
M, Wang G, Darcy KM, et al: Identification of novel candidate
biomarkers of epithelial ovarian cancer by profiling the secretomes
of three-dimensional genetic models of ovarian carcinogenesis. Int
J Cancer. 137:1806–1817. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Testa A, Kaijser J, Wynants L, Fischerova
D, Van Holsbeke C, Franchi D, Savelli L, Epstein E, Czekierdowski
A, Guerriero S, et al: Strategies to diagnose ovarian cancer: New
evidence from phase 3 of the multicentre international IOTA study.
Br J Cancer. 111:680–688. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Amal H, Shi DY, Ionescu R, Zhang W, Hua
QL, Pan YY, Tao L, Liu H and Haick H: Assessment of ovarian cancer
conditions from exhaled breath. Int J Cancer. 136:E614–E622. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lum D, Guido R, Rodriguez E, Lee T,
Mansuria S, D'Ambrosio L and Austin RM: Brush cytology of the
fallopian tube and implications in ovarian cancer screening. J
Minim Invasive Gynecol. 21:851–856. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gizzo S, Noventa M, Saccardi C, Litta P,
D'Antona D and Nardelli GB: Proposal on Raloxifene use after
prophylactic salpingo-oophorectomy in BRCA1-2: Hypothesis and
rationale. Eur J Cancer Prev. 23:514–515. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gizzo S, Ancona E, Saccardi C, Patrelli
TS, Berretta R, Anis O, Noventa M, Bertocco A, Fagherazzi S,
Longone M, et al: Radical trachelectomy: The first step of
fertility preservation in young women with cervical cancer
(Review). Oncol Rep. 30:2545–2554. 2013.PubMed/NCBI
|
|
22
|
Berretta R, Gizzo S, Dall'Asta A, Mazzone
E, Monica M, Franchi L, Peri F, Patrelli TS and Modena A Bacchi:
Risk of preterm delivery associated with prior treatment of
cervical precancerous lesion according to the depth of the cone.
Dis Markers. 35:721–726. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kaijser J, Sayasneh A, Van Hoorde K,
Ghaem-Maghami S, Bourne T, Timmerman D and Van Calster B:
Presurgical diagnosis of adnexal tumours using mathematical models
and scoring systems: A systematic review and meta-analysis. Hum
Reprod Update. 20:449–462. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gizzo S, Bertocco A, Saccardi C, Di Gangi
S, Litta PS, D'antona D and Nardelli GB: Female sterilization:
Update on clinical efficacy, side effects and contraindications.
Minim Invasive Ther Allied Technol. 23:261–270. 2014. View Article : Google Scholar : PubMed/NCBI
|